Interferon alpha is an effective therapy for congenital dyserythropoietic anaemia type I
3
Case Report Interferon alpha is an effective therapy for congenital dyserythropoietic anaemia type I Shamseddine A, Taher A, Jaafar H, Haidar JH, Nasr R, Arzoumanian V, Salem Z, Bazarbachi A. Interferon alpha is an effective therapy for congenital dyserythropoietic anaemia type I. Eur J Haematol 2000: 65: 207–209. # Munksgaard 2000. Abstract: The efficacy of interferon-alpha (IFN) was reported in three patients with congenital dyserythropoietic anaemia (CDA) type I. We describe two additional cases treated with IFN, which normalized the haemoglobin level in both patients with a dramatic decrease in the size of the spleen in one. Haemoglobin remained stable more than 6 months after discontinuation of treatment. IFN induced more than 50% decrease in the number of BFU-E in both patients’ bone marrow cultures, suggesting an indirect effect of IFN on erythropoiesis in vivo. We conclude that a trial of IFN therapy should be considered in patients with CDA type I. Ali Shamseddine 1 , Ali Taher 1 , Hassan Jaafar 1 , Joud H. Haidar 2 , Rihab Nasr 1,3 , Varant Arzoumanian 1 , Ziad Salem 1 , Ali Bazarbachi 1,3 Departments of 1 Internal Medicine, 2 Pathology and Laboratory Medicine, and 3 Biochemistry, American University of Beirut, Beirut, Lebanon Key words: congenital dyserythropoietic anaemia; interferon; BFU-E Correspondence: Ali Bazarbachi, MD, PhD, Department of Internal Medicine, American University of Beirut, PO Box 113 6044, Beirut, Lebanon Tel: +961-3-612434 Fax: +961-1-345325 e-mail: [email protected] Accepted for publication 2 May 2000 Congenital dyserythropoietic anaemia (CDA) is a rare inherited haematological disorder with mild to moderate anaemia, splenomegaly, ineffective erythropoiesis and morphological abnormality of mature red blood cells and their precursors (1, 2). The diagnosis is usually done in early childhood. CDA consists of three major types with a number of variants. CDA type I is an autosomal recessive disease with macrocytic mild to moderate macrocytic anaemia. Bone marrow abnormalities consist of megaloblas- tic erythropoiesis with an irregular nuclear segmen- tation, binucleated cells and pairs of erythroblasts connected by thin chromatin bridges. The acid lysis test and sugar test are negative. CDA type II is an autosomal recessive disease characterized by nor- mocytic moderate to severe anaemia and by the presence of the unique HEMPAS antigen on red blood cells. Bone marrow abnormalities consist of more abnormal erythroblasts. CDA type III is an autosomal dominant disease characterized by macrocytosis in peripheral blood and bone marrow erythroblasts with up to 12 nuclei, and prominent basophilic stippling. Currently, the management of CDA type I relies on blood transfusion with preventive measures for secondary hemochromatosis. Splenectomy may be of benefit in some cases. Recent reports showed the efficacy of alpha interferon (IFN) in three patients with CDA type I (3–5). One patient showed a substantial reduction in the extent of ineffective erythropoiesis (5). In this manuscript, we report two additional cases of CDA type I who showed excellent in vivo haematologic response to IFN with in vitro IFN suppression of BFU-E. Results Case 1 A 31-yr-old Lebanese man presented with anaemia since early childhood that required multiple trans- fusions. The family history revealed two other siblings with chronic anaemia. Physical examina- Eur J Haematol 2000: 65: 207–209 Printed in UK. All rights reserved Copyright # Munksgaard 2000 EUROPEAN JOURNAL OF HAEMATOLOGY ISSN 0902-4441 207
-
Upload
ali-shamseddine -
Category
Documents
-
view
213 -
download
0
Transcript of Interferon alpha is an effective therapy for congenital dyserythropoietic anaemia type I

Case Report
Interferon alpha is an effective therapy forcongenital dyserythropoietic anaemia type I
Shamseddine A, Taher A, Jaafar H, Haidar JH, Nasr R, ArzoumanianV, Salem Z, Bazarbachi A. Interferon alpha is an effective therapy forcongenital dyserythropoietic anaemia type I.Eur J Haematol 2000: 65: 207±209. # Munksgaard 2000.
Abstract: The ef®cacy of interferon-alpha (IFN) was reported in threepatients with congenital dyserythropoietic anaemia (CDA) type I. Wedescribe two additional cases treated with IFN, which normalized thehaemoglobin level in both patients with a dramatic decrease in the size ofthe spleen in one. Haemoglobin remained stable more than 6 monthsafter discontinuation of treatment. IFN induced more than 50% decreasein the number of BFU-E in both patients' bone marrow cultures,suggesting an indirect effect of IFN on erythropoiesis in vivo. Weconclude that a trial of IFN therapy should be considered in patientswith CDA type I.
Ali Shamseddine1, Ali Taher1,Hassan Jaafar1, Joud H. Haidar2,Rihab Nasr1,3,Varant Arzoumanian1, Ziad Salem1,Ali Bazarbachi1,3
Departments of1Internal Medicine,
2Pathology and
Laboratory Medicine, and3Biochemistry, American
University of Beirut, Beirut, Lebanon
Key words: congenital dyserythropoietic anaemia;
interferon; BFU-E
Correspondence: Ali Bazarbachi, MD, PhD, Department
of Internal Medicine, American University of Beirut,
PO Box 113 6044, Beirut, Lebanon
Tel: +961-3-612434
Fax: +961-1-345325
e-mail: [email protected]
Accepted for publication 2 May 2000
Congenital dyserythropoietic anaemia (CDA) is arare inherited haematological disorder with mildto moderate anaemia, splenomegaly, ineffectiveerythropoiesis and morphological abnormality ofmature red blood cells and their precursors (1, 2).The diagnosis is usually done in early childhood.CDA consists of three major types with a number ofvariants.
CDA type I is an autosomal recessive disease withmacrocytic mild to moderate macrocytic anaemia.Bone marrow abnormalities consist of megaloblas-tic erythropoiesis with an irregular nuclear segmen-tation, binucleated cells and pairs of erythroblastsconnected by thin chromatin bridges. The acid lysistest and sugar test are negative. CDA type II is anautosomal recessive disease characterized by nor-mocytic moderate to severe anaemia and by thepresence of the unique HEMPAS antigen on redblood cells. Bone marrow abnormalities consistof more abnormal erythroblasts. CDA type IIIis an autosomal dominant disease characterizedby macrocytosis in peripheral blood and bone
marrow erythroblasts with up to 12 nuclei, andprominent basophilic stippling.
Currently, the management of CDA type I relieson blood transfusion with preventive measures forsecondary hemochromatosis. Splenectomy may beof bene®t in some cases.
Recent reports showed the ef®cacy of alphainterferon (IFN) in three patients with CDA type I(3±5). One patient showed a substantial reduction inthe extent of ineffective erythropoiesis (5). In thismanuscript, we report two additional cases of CDAtype I who showed excellent in vivo haematologicresponse to IFN with in vitro IFN suppression ofBFU-E.
Results
Case 1
A 31-yr-old Lebanese man presented with anaemiasince early childhood that required multiple trans-fusions. The family history revealed two othersiblings with chronic anaemia. Physical examina-
Eur J Haematol 2000: 65: 207±209Printed in UK. All rights reserved
Copyright # Munksgaard 2000
EUROPEANJOURNAL OF HAEMATOLOGY
ISSN 0902-4441
207

tion showed icteric sclera and splenomegaly at12 cm below costal margin (bcm). The haemoglobinlevel was 84 g/l (MCV, 77; reticulocyte, 6.5%) andthe WBC and platelet counts were normal. Aperipheral blood smear showed anisocytosis andpolychromasia.
Laboratory studies revealed high LDH, raisedindirect serum bilirubin levels, and absent hapto-globin suggestive of either haemolysis or more likelyineffective erythropoiesis with death of nucleatedred cell precursors in the marrow. Creatinin andliver function tests were normal. Direct Coombsand acid lysis tests were negative. The iron pro®lewas normal. G6PD and pyruvate kinase levels,osmotic fragility and haemoglobin electrophoresiswere normal with a haemoglobin A2 of 1.9%.The bone marrow aspirate showed a hypercellularmarrow with evidence of megaloblastoid and grossdyserythropoiesis features with binucleation, inter-nuclear bridges and lobulated nuclei con®rming thediagnosis of CDA type I.
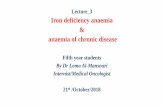
The patient was started on IFN [3r106 IUsubcutaneously (SC) thrice weekly]. The haemoglo-bin level started to improve after 1 month oftreatment and reached a borderline normal value of120 g/dl after 4 months of treatment (Fig. 1). Thiswas associated with normalization of the haemo-lysis markers and a dramatic decrease in the size ofthe spleen to 3 cm bcm. Despite the absence of anysigni®cant side effects of IFN therapy, the patientthen spontaneously stopped his treatment. Hishaemoglobin remained stable for more than 6months and then gradually dropped to the pre-treatment level after 9 months (Fig. 1). Thesplenomegaly returned to pretreatment size of12 cm bcm at the same time. Bone marrow aspiratewas not repeated.
Case 2
A 64-yr-old Lebanese woman presented to ourhospital because of anaemia that had started earlyin her childhood. The family history was negative.She underwent splenectomy because of splenome-galy at the age of 22 yr.
Her haemoglobin level was 88 g/l with an MCV of85; the WBC count and differential were normal. Aperipheral smear showed anisocytosis, polychroma-sia and basophilic stippling. Laboratory studiesrevealed high LDH, raised indirect serum bilirubinlevels, and absent haptoglobin suggestive of eitherhemolysis or more likely ineffective erythropoiesiswith death of nucleated red cell precursors in themarrow. Her iron pro®le was normal. Acid lysistest, G6PD level and haemoglobin electrophoresiswere normal with a haemoglobin A2 of 1.7%.The bone marrow aspirate showed a hypercellularmarrow with evidence of megaloblastoid and grossdyserythropoiesis features with binucleation andlobulated nuclei suggestive of CDA type I. How-ever, no typical inter-nuclear bridges were noted.Myeloid precursors were normal.
The patient was started on IFN therapy (3r106
IU SC three times weekly). The haemoglobin levelstarted to improve after 1 month and reached aborderline normal value of 110 g/l after 3 months(Fig. 1). Minimal side effects were noted, mostlymyalgia and mild nausea. IFN discontinuationresulted in a progressive drop of haemoglobin toreturn to pretreatment level after 7 months (Fig. 1).
Colony-forming unit assay
Bone marrow mononuclear cells (MNC) werecollected from the 2 patients before starting IFN
Fig. 1. Haemoglobin levels in response to IFN (3r106 IUSC, 3r weekly) treatment in 2 patients with CDA type I.
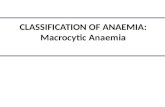
Fig. 2. Interferon effects (100 IU/ml) on bone marrowcultures from one normal subject and two patients withCDA type I. Numbers of colonies at day 14 are presented asa percentage of untreated cultures.
Shamseddine et al.
208

therapy, as well as from one healthy individual afterinformed consent. These MNC were cultured inMethocult2 GF H4434 (Stem Cell Technologies,Vancouver, BC, Canada) semisolid methylcellulosemedium which contains a combination of variouscolony-stimulating factors (rh stem cell factor; rhGM-CSF; rh IL3 and rh erythropoietin). Cells wereplated in triplicate at a concentration of 1r105/mlin 35 mm gridded Petri dishes (Stem Cell Tech-nologies) and incubated at 37 uC, 5% CO2, 100%humidity for 14 d. Non-haemoglobinized aggreg-ates containing more than 50 cells [colony-formingunit±granulocyte macrophage (CFU-GM)] andhaemoglobinized aggregates containing more than50 cells [burst-forming-units erythroid (BFU-E)]were counted using an inverted microscope. To testthe effect of IFN on CFU-GM and BFU-E growth,100 U/ml of IFN (Roferon1, Roche, Switzerland)was added to dishes on day 1. This dose of 100 U/mlof IFN corresponds to plasma levels achievable invivo.
As expected, in the normal control, IFN resultedin a moderate decrease in the number of CFU-GMand a more signi®cant decrease in the number ofBFU-E (Fig. 2) which was associated with a smallersize of the BFU-E colonies. These results are con-sistent with the previously described inhibitoryeffect of IFN on erythropoiesis (6). Interestingly,similar results were observed with the 2 patientswith CDA type I who responded in vivo to IFNtherapy (Fig. 2).
Discussion
The ef®cacy of IFN was previously reported in threepatients with CDA type I. We describe twoadditional cases treated with IFN, which normal-ized the haemoglobin level in both patients with adramatic decrease in the size of the spleen in one.Haemoglobin remained stable more than 6 monthsafter discontinuation of treatment. IFN inducedmore than 50% decrease in the number of BFU-E inboth patients' bone marrow cultures. This fall in
BFU-E numbers in the face of a rise in haemoglobinis strongly suggestive of reduced ineffective ery-thropoiesis caused by IFN, although improvedsurvival of peripheral blood red cells may also be afactor. The indirect effect of IFN through cytokinemodulation should also be examined. Recently,impaired lymphocyte production of IFN wasdocumented in 7 patients with CDA type I (7).Our results recon®rm the ef®cacy and tolerance ofIFN therapy in patients with CDA type I. Noclinical results are currently available on the useof IFN in other types of CDA. The stability ofhaemoglobin levels for more than 6 months afterdiscontinuation of IFN treatment permits inter-mittent maintenance therapy with low dose of IFN.
Acknowledgement
We thank Dr Marwan E. El-Sabban for his valuable input.
References
1. HEIMPEL H, FORTEZA-VILA J, QUEISSER W, SPEIRTZ E. Electronand light microscopic study of the erythroblasts of patientswith congenital dyserythropoietic anaemia. Blood 1971;37:299±310.
2. LEWIS SM, NELSON DA, PITCHER CS. Clinical and ultra-structural aspects of congenital dyserythropoietic anaemiatype I. Br J Haematol 1972;23:113±119.
3. LAVABRE-BERTRAND T, BLANC P, NAVARRO R, et al. Alpha-interferon therapy for congenital dyserythropoiesis type I. BrJ Haematol 1995;89:929±932.
4. VIRJEC S, HATTON C. Congenital dyserythropoiesis type I andalpha interferon therapy. Br J Hematol 1996;94:581±582.
5. WICKRAMASINGHE SN. Response of congenital dyserythropoi-esis anaemia type I to alpha interferon. Eur J Hematol1997;58:121±123.
6. CASTELLO G, MELA G, CERRUTI A, MENCOBONI M, LERZA R.Azidothymidine and interferon-a in vitro effects on hemato-poiesis: Protective in vitro activity of IL1 and GM-CSF(Unpublished work).
7. WICKRAMASINGHE SN, HASAN R, SMYTHE J. Reduced inter-feron-alpha production by Epstein±Barr virus transformedB-lymphoblastoid cell lines and lectin-stimulated lympho-cytes in congenital dyserythropoietic anaemia type I. Br JHaematol 1997;98:295±298.
IFN therapy for CDA type I
209