Interesting Case - Srinakharinwirot...
61
Interesting Case Group 4 Presenting to Radiology Department: Srinakharinwirot University
Transcript of Interesting Case - Srinakharinwirot...
Interesting CaseGroup 4 Presenting to Radiology Department:
Srinakharinwirot University
Patient History:
HN: 15964-56
Social History:
A 38 year-old Married Thai Buddhist female
Career: Freelance
Allergy: No food & drug allergy
Substances: No alcohol use/ No smoking
Chief complaint:
More severe Epigastrium pain 3 day PTA
Present illness:
Intermittent Epigastrium pain
Radiate to back, no migration, with no
relationship to posture
No Fever (after 1 tab Tylenol)
Dysphagia, nausea-vomiting
Present illness:
No diarrhea, 2 days constipation
No gastric reflux and heartburn
More severity leads to hospital admission
Physical examination:
Vital sign:
BT 36.6 oC, PR 60 beat/min, RR 22/min
BP 140/80 mmHg, O2 Sat 99%
General appearance:
A Thai female, good consciousness
no jaundice
Physical examination:
HEENT :
not pale conjunctiva, clear sclera
CVS : WNL
RS : WNL
Physical examination:
Abdomen :
flat shape, no surgical scar was seen
tender at epigastrium and RUQ,
Soft, no rebound tenderness, no guarding,
Normoactive bowel sound
Physical examination:
Extremities : no rash, no petechiae ,
no pitting edema
Neuro : E4M6V5 , orientated to time place
person, motor grade V all
Murphy’s sign positive
Problem list:
Tender at epigastrium and RUQ
Murphy’s sign positive
Differential diagnosis:
Acute Cholecystitis
Choledocholithiasis CBD stone
Cholangitis
Pancreatitis
Differential diagnosis:
Acute Cholecystitis
Choledocholithiasis CBD stone
Cholangitis
Pancreatitis
Differential diagnosis:
Acute Cholecystitis
Choledocholithiasis CBD stone
Cholangitis
Pancreatitis
Differential diagnosis:
Acute Cholecystitis
Choledocholithiasis CBD stone
Cholangitis
Pancreatitis
Differential diagnosis:
Acute Cholecystitis
Choledocholithiasis CBD stone
Cholangitis
Pancreatitis
Provisional diagnosis:
Acute Cholecystitis since it is the most
common biliary tract disease which shows
fever with right upper quadrant abdominal
pain, no jaundice and Murphy’s sign positive
Lab investigation:
CBC :
Hct 13.7 Hb 37.7
WBC 9,920 N67.7% L21.9% Plt 411,000
UA:
Sp.gr. 1.010
WBC 1-2 RBC 0-1 epi 0-1
Bact. Few TB 2.65 / DB 2.38
Laboratory Evaluation
Lab investigation:
LFT:
AST 142 ALT 209 ALP 208
Amylase 79 Lipase 138
Laboratory Evaluation
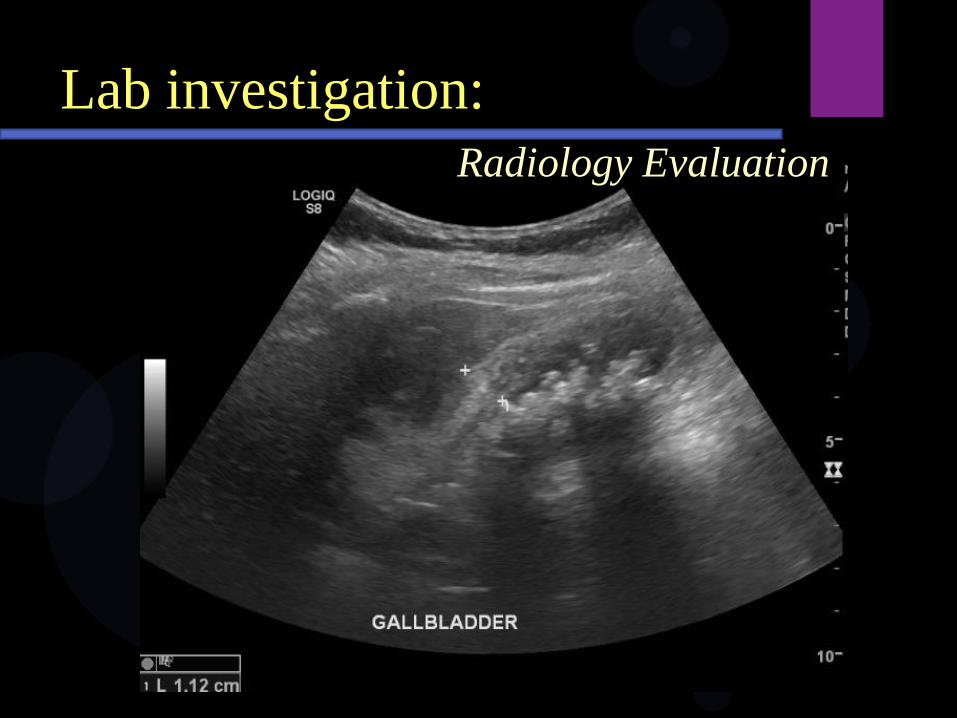
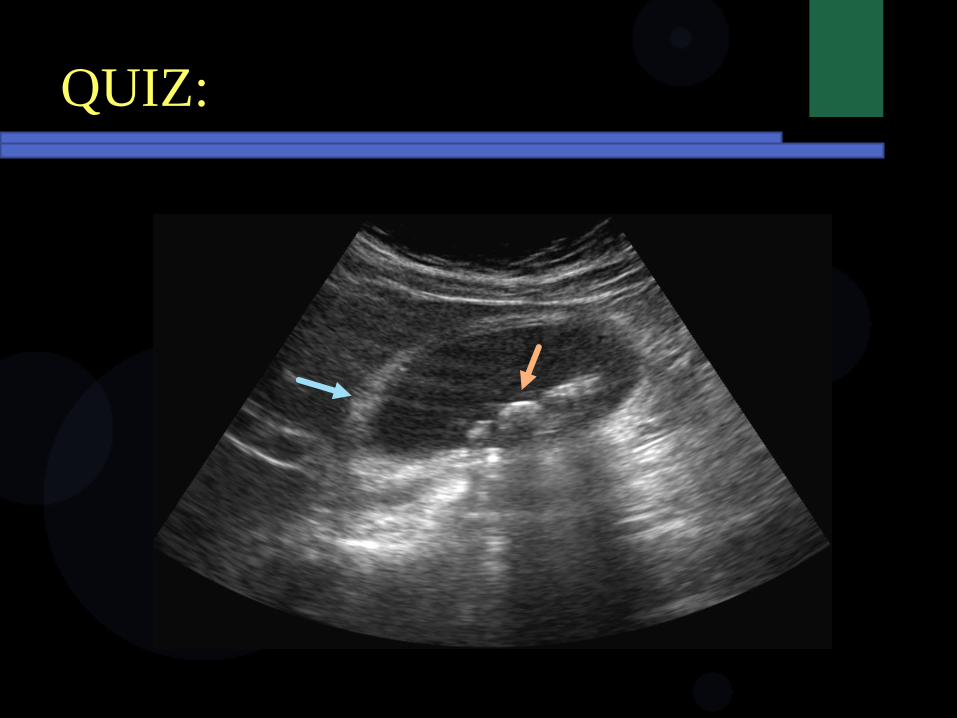
Lab investigation:
U/S upper abdomen:
Gallbladder no wall thickening
Hyperechoic with posterior acoustic shadow
Suspected gallstone
Laboratory Evaluation
Lab investigation:
Radiology Evaluation
Lab investigation:
Radiology Evaluation
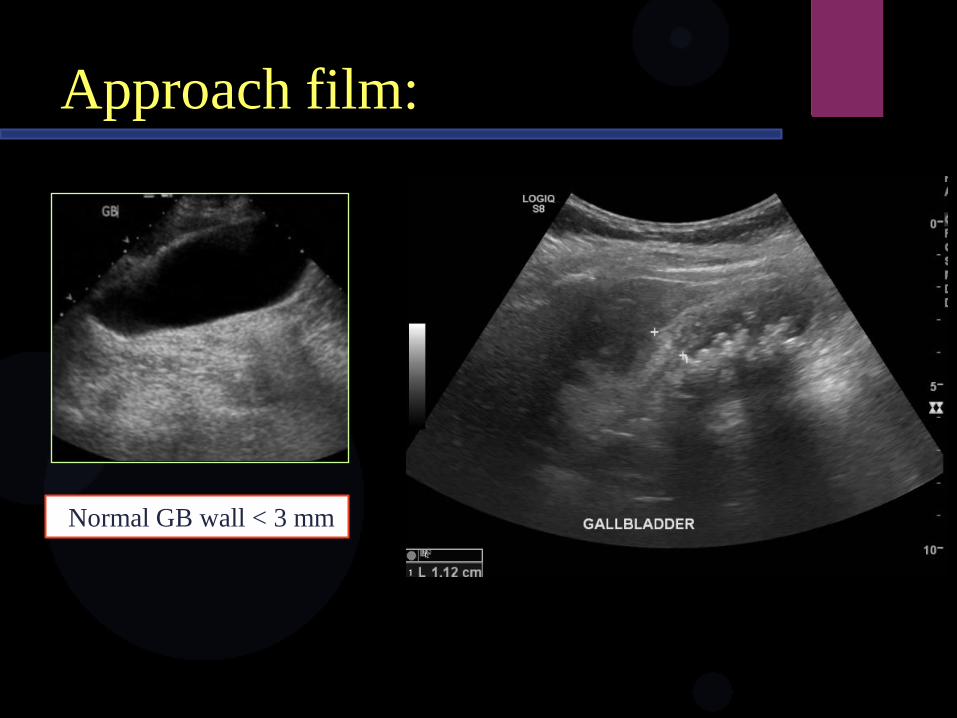
Approach film:
Normal GB wall < 3 mm
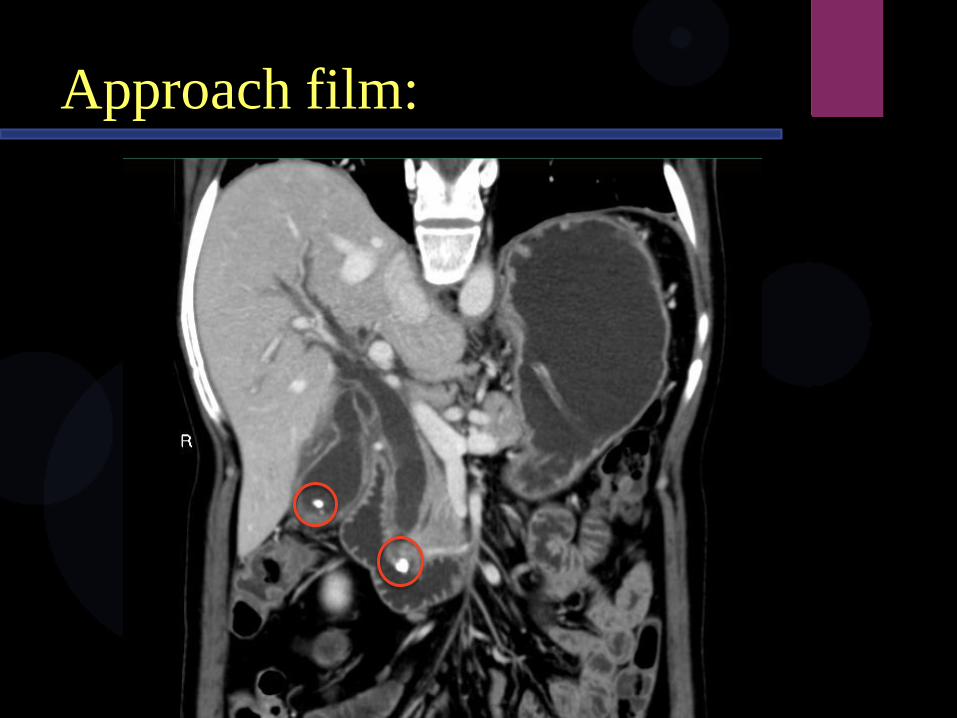
Approach film:
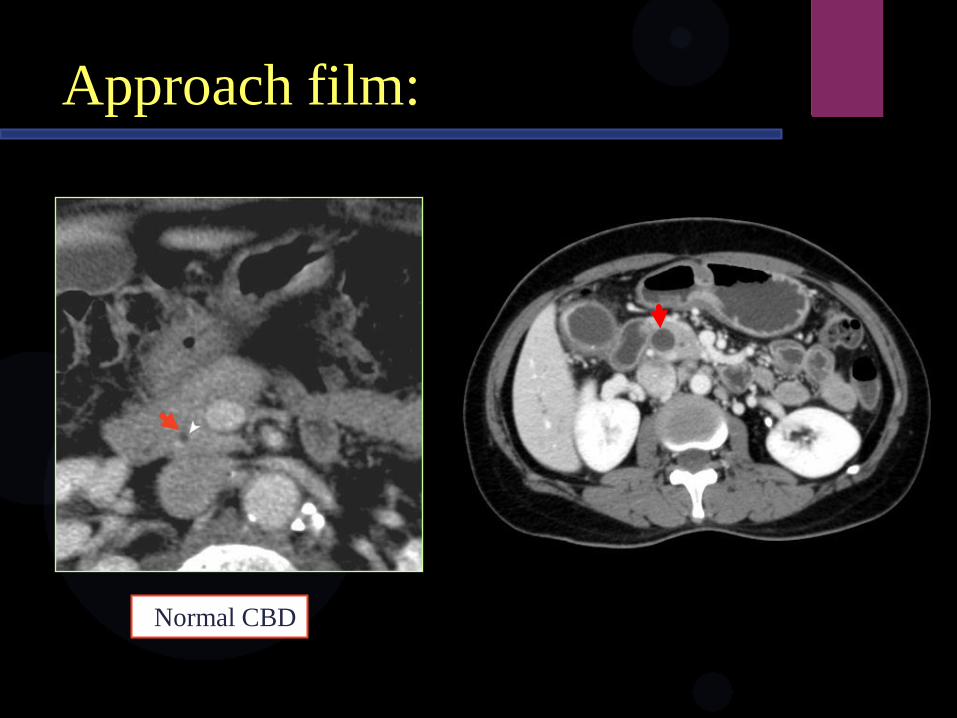
Approach film:
Normal CBD
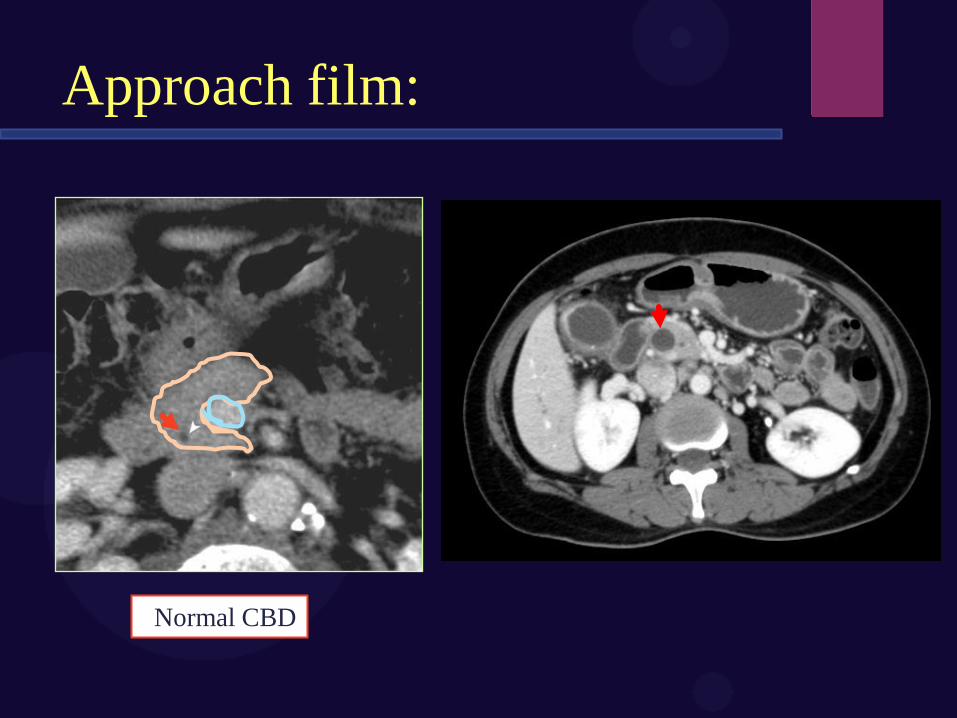
Approach film:
Normal CBD
Conclusion:
A Thai female, 38 years old presented with
epigastrium pain and Murphy’s sign positive.
US:
Gallbladder wall thickening
Hyperechoic with posterior acoustic shadow
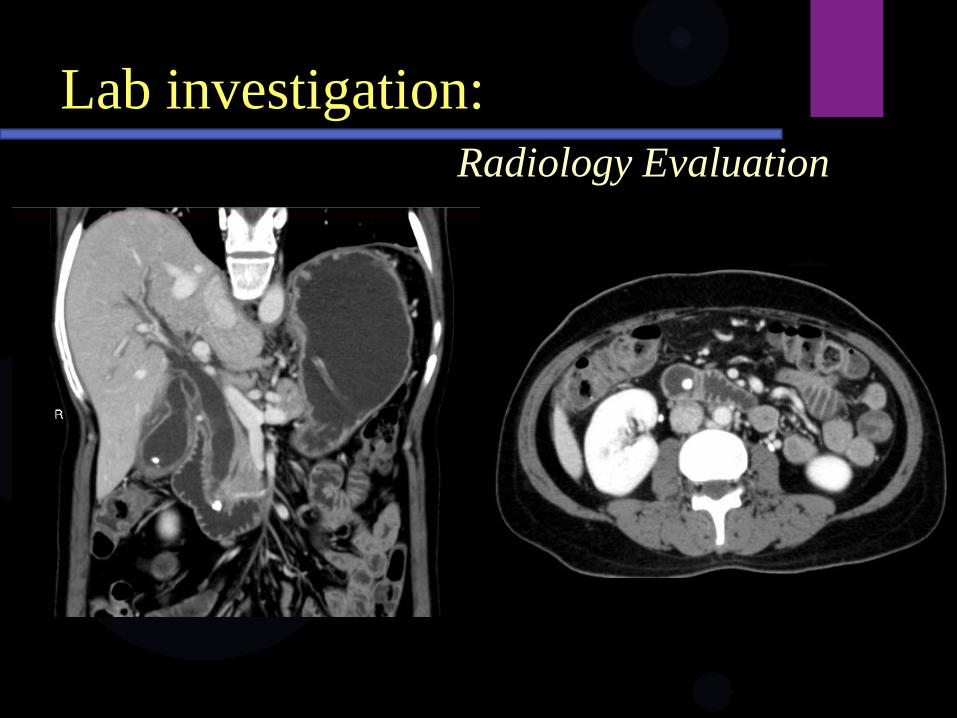
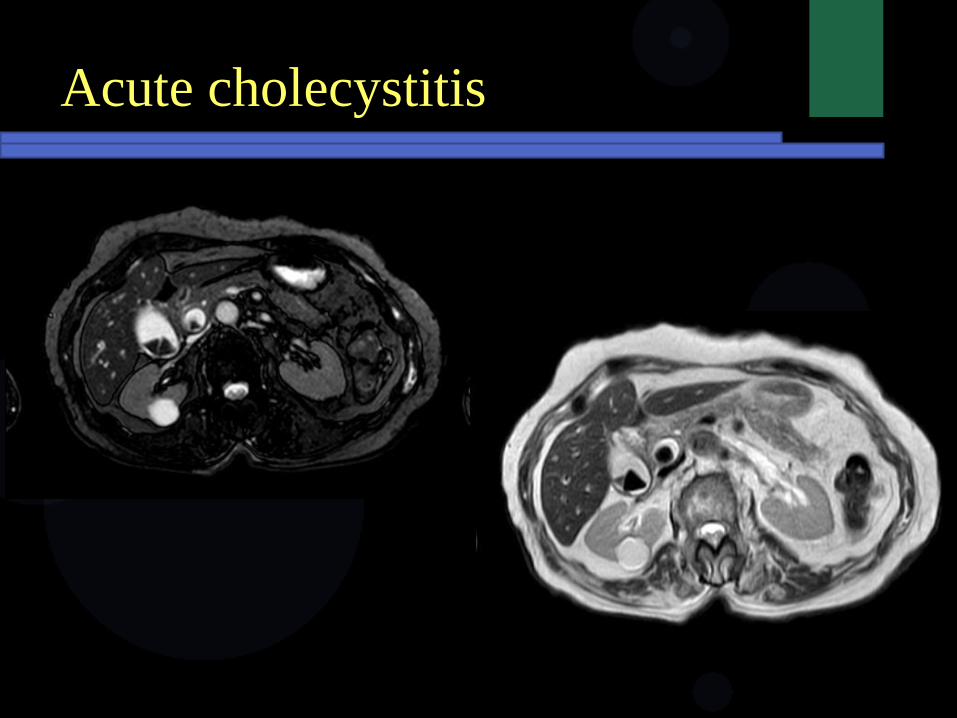
Conclusion:
CT scan:
Dense calcified stone in Gallbladder and distal
CBD
Final Diagnosis:
Acute cholecystitis with CBD stone
Treatment:
Antibiotics
• Piperacillin-tazobactam
• Ceftriaxone + Metronidazole
• Levofloxacin + Metronidazole
Cholecystectomy
• Open procedure
• Laparoscopy
Knowledge
Knowledge:
Acute Cholecytstitis
Choledocholithiasis CBD stone
Cholangitis
Acute Pancreatitis
Knowledge:
Acute Cholecytstitis
Choledocholithiasis CBD stone
Cholangitis
Acute Pancreatitis
Acute cholecystitis
90% due to calculous obstruction of
gallbladder neck or cystic duct
More common in female 90%
Acute pain in right upper quadrant
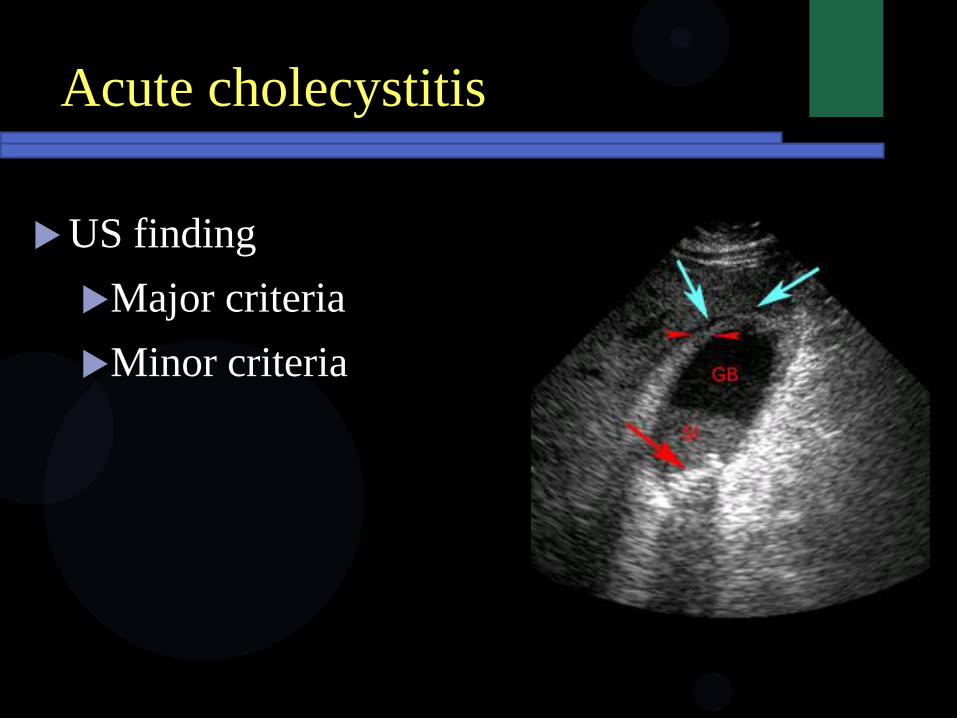
Acute cholecystitis
US finding
Major criteria
Minor criteria

Acute cholecystitis
US finding
Major criteria
Gallstone
Sonographic
Murphy’s sign
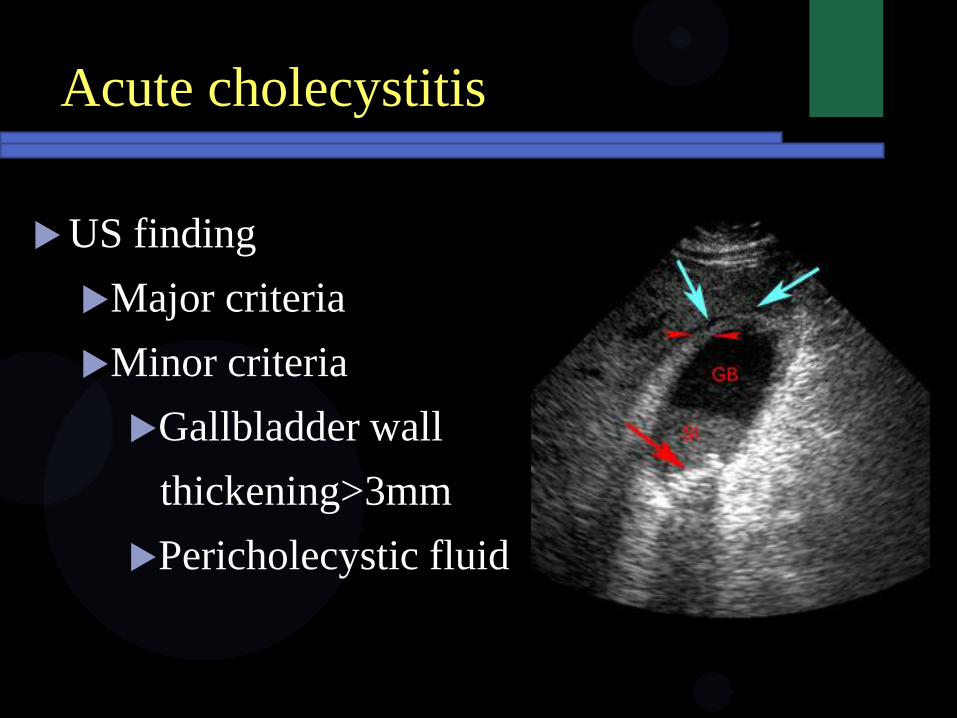
Acute cholecystitis
US finding
Major criteria
Minor criteria
Gallbladder wall
thickening>3mm
Pericholecystic fluid
Acute cholecystitis
Acute cholecystitis
QUIZ:
RANDOM _ FLASH
QUIZ:
Knowledge:
Acute Cholecytstitis
Choledocholithiasis CBD stone
Cholangitis
Acute Pancreatitis
Most common cause of biliary tract
obstruction
Mostly cause by passing gall stone
Often asymptomatic
Suspected in patients with jaundice and
biliary colic
Lab : elevated bilirubin, ALP, ALT
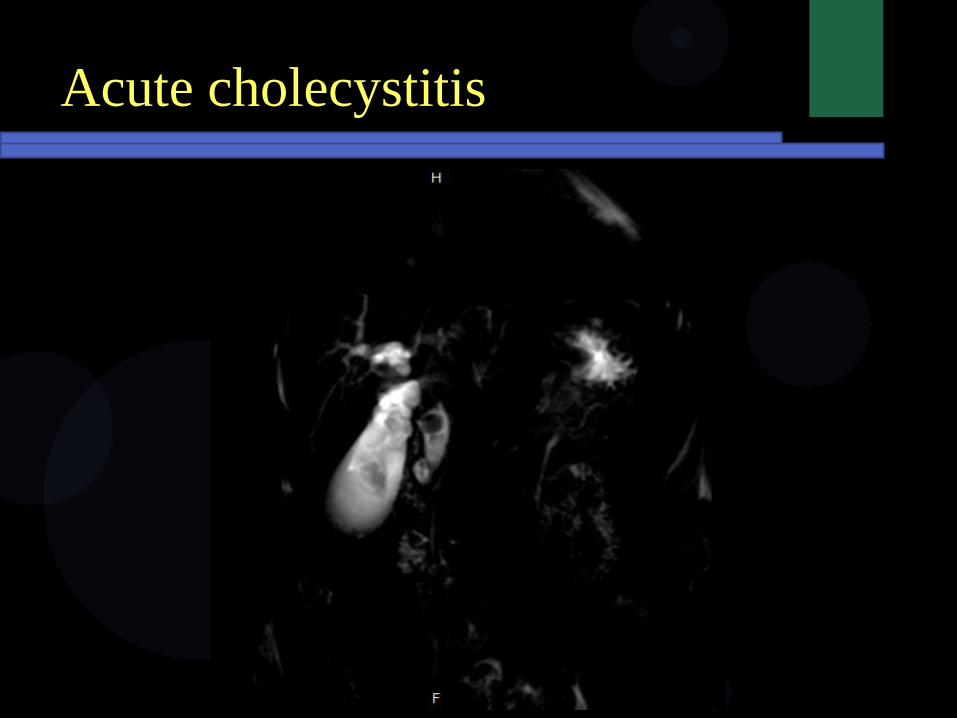
Choledocholithiasis(CBD stone)
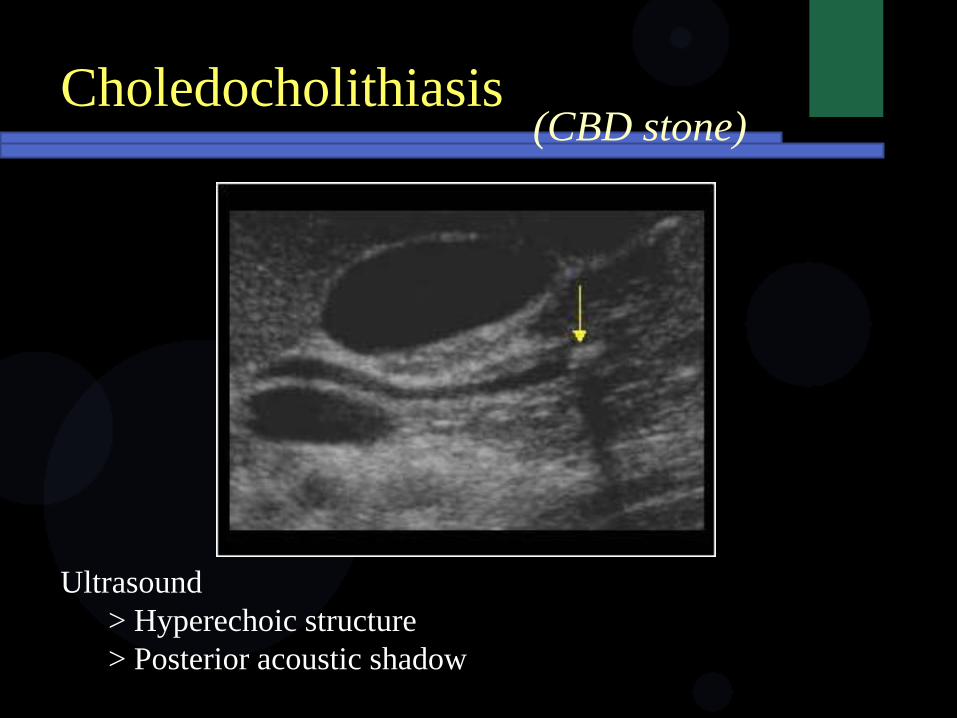
Ultrasound
> Hyperechoic structure
> Posterior acoustic shadow
Choledocholithiasis(CBD stone)
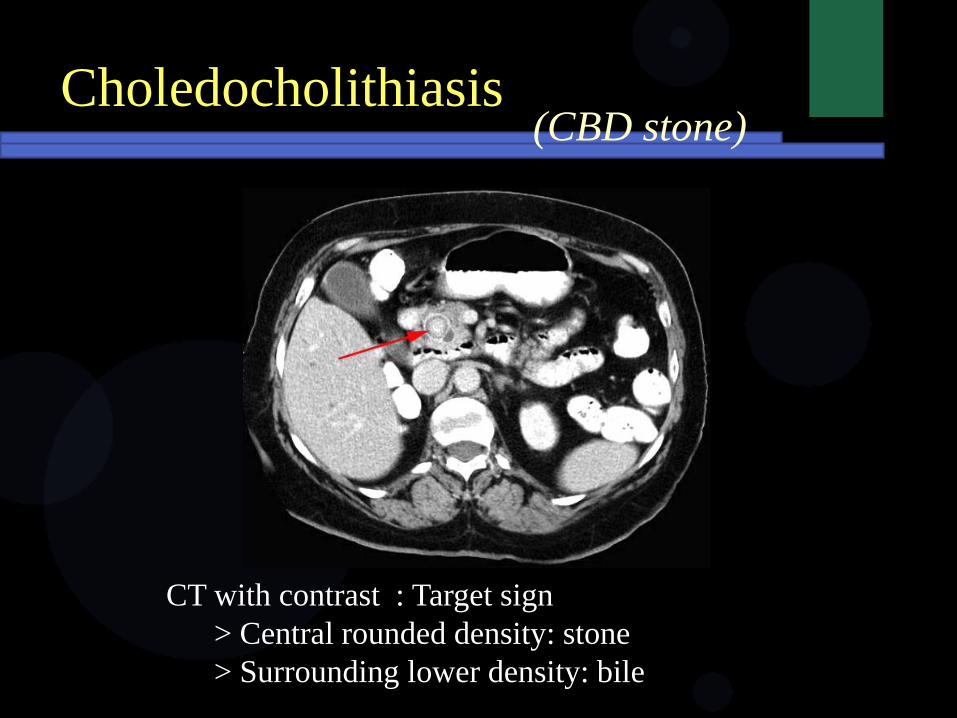
CT with contrast : Target sign
> Central rounded density: stone
> Surrounding lower density: bile
Choledocholithiasis(CBD stone)
Knowledge:
Acute Cholecytstitis
Choledocholithiasis CBD stone
Cholangitis
Acute Pancreatitis
Cholangitis
Broad descriptive term refer to
inflammation of the bile duct
Infective cholangitis : Most common
Primary sclerosing cholangitis
Chemotherapy induced cholangitis
Eosinophilic cholangitis
Acute cholangitis
Charcot’s triad : Fever, jaundice and
abdominal pain
Cause : bacterial infection in a patient with
biliary obstruction ascending from the
duodenum
E. coli 25-50% , Klebsiella 15-20% ,
Enterobacter 5-10%
Ascending cholangitis
Acute cholangitis
Laboratory test
Elevated white blood cell count
neutrophil
Elevated serum ALP, AST
Ascending cholangitis
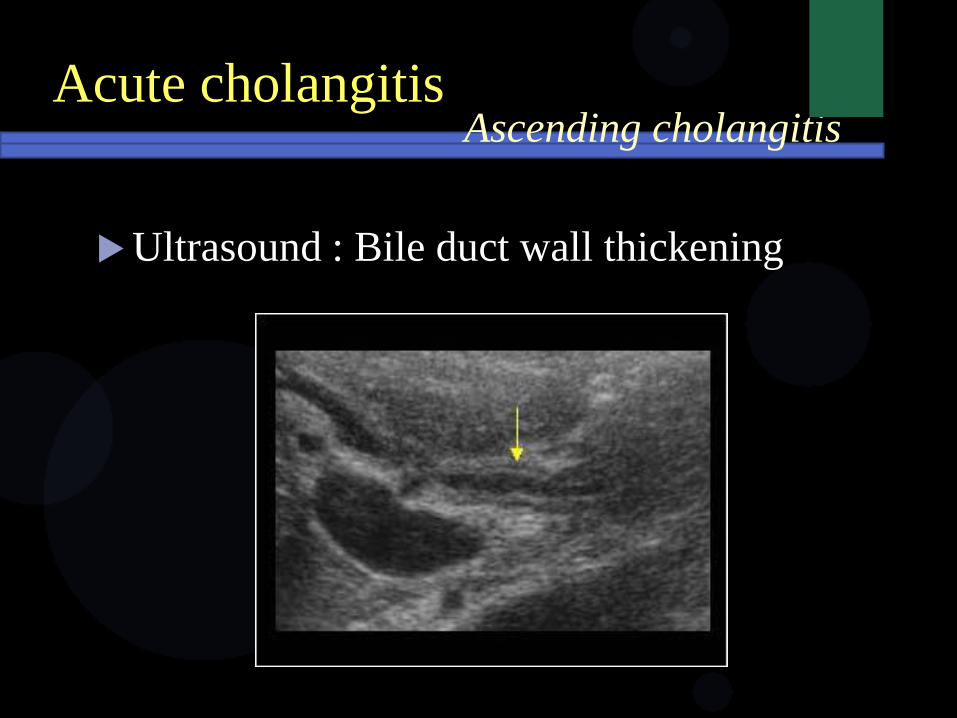
Ultrasound : Bile duct wall thickening
Acute cholangitisAscending cholangitis
Acute cholangitisAscending cholangitis
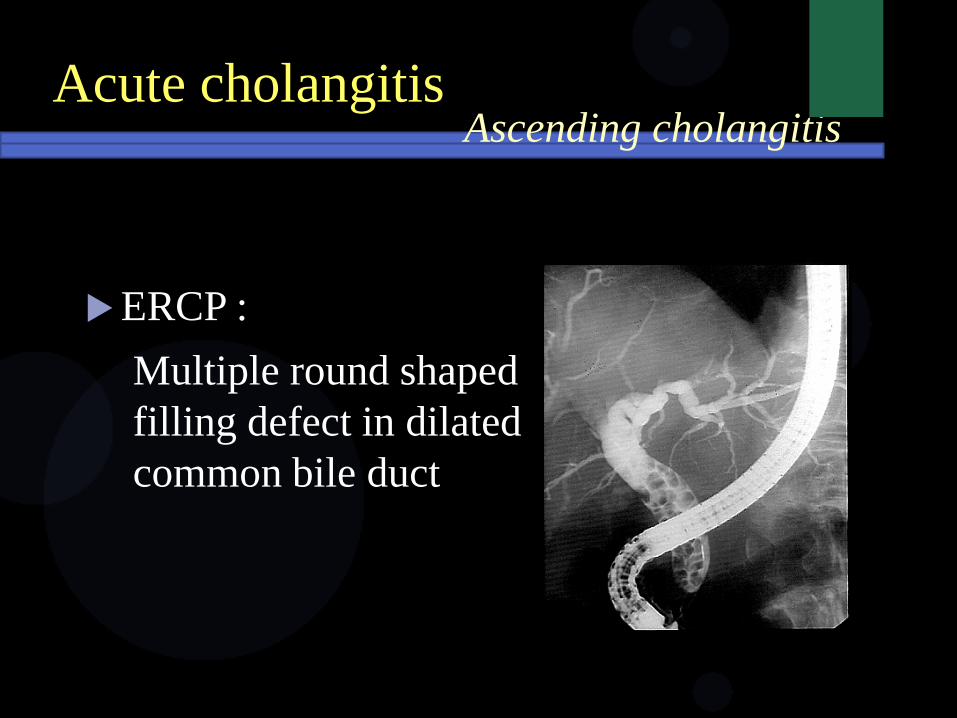
ERCP :
Multiple round shaped
filling defect in dilated
common bile duct
Most often in 30-60 years; more common
in men 70%
Idiopathic; autoimmune
Inflammation damage bile duct
scaring obstruct bile stasis & back
pressure liver damage bile lake
Primary sclerosing cholangitis
Clinical finding
Asymptomatic
Pain in upper right abdomen
diarrhea
Fever
Elevated serum ALP and AST
Primary sclerosing cholangitis
jaundice
Pruritus
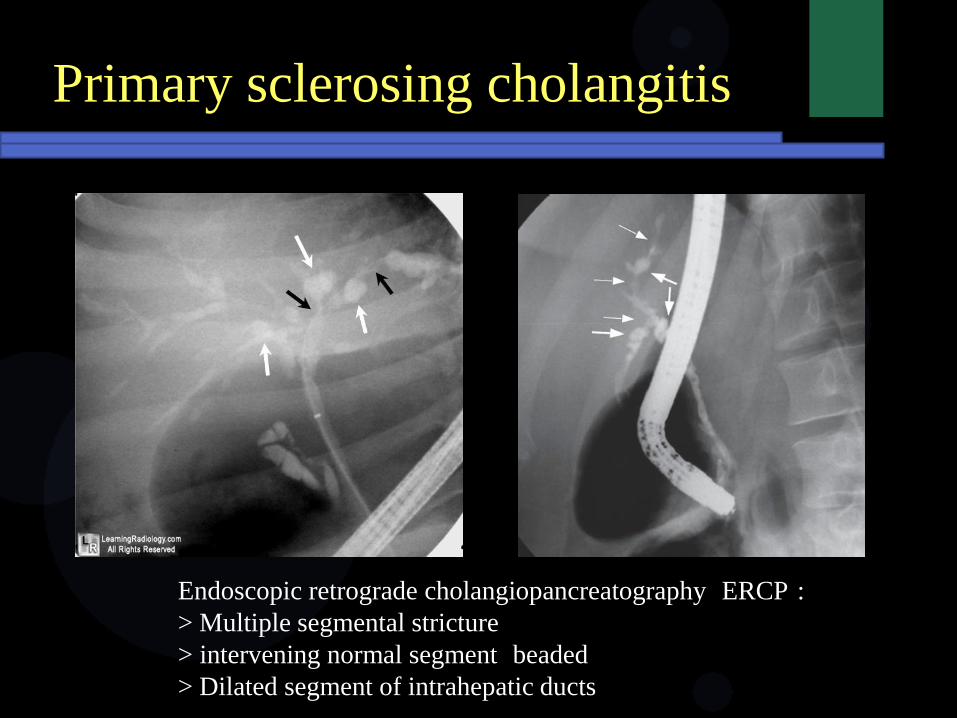
Endoscopic retrograde cholangiopancreatography ERCP :
> Multiple segmental stricture
> intervening normal segment beaded
> Dilated segment of intrahepatic ducts
Primary sclerosing cholangitis
Knowledge:
Acute Cholecytstitis
Choledocholithiasis CBD stone
Cholangitis
Acute Pancreatitis
Acute pancreatitis
Classical features
Gradual development of severe central
epigastrium pain and radiates through to the
back
Exacerbated by supine positioning
Lab
Elevated amylase and lipase enzyme
Acute pancreatitis
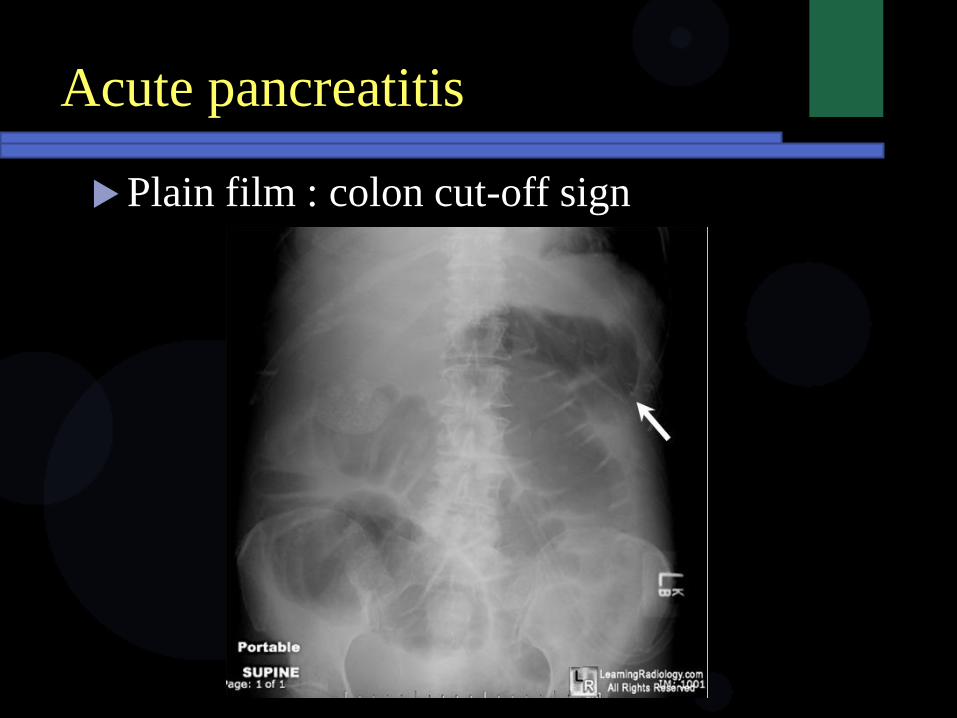
Plain film : colon cut-off sign
Acute pancreatitis
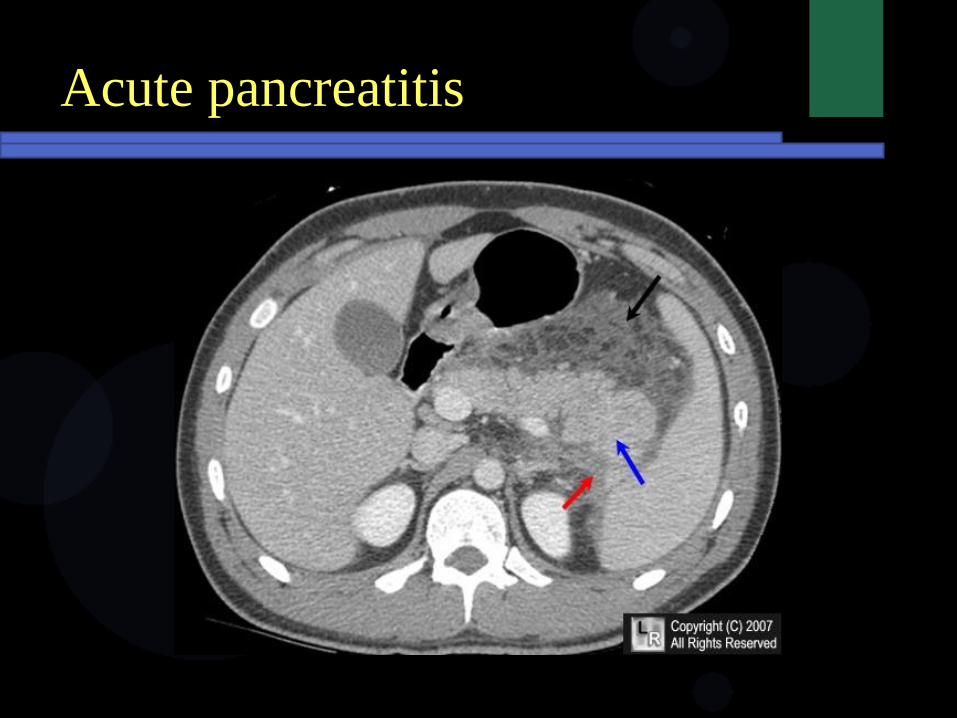
CT
Enlarged pancreas with shaggy margin
Peripancreatic fluid
Infiltration of peripancreatic fat
Acute pancreatitis
QUIZ:
1.
What is the finding of Acute Cholecystits
in Plain Film Abdomen?
Take Home Message:
Modality of choice for Acute Cholecystitis is
US
In US Triad signs suspected Acute Cholecystitis:
1. Gallbladder wall thickening (>3mm)
2. Gallstone
3. Sonographic Murphy’s sign positive
Take Home Message:
4 types of Gall stone:
• Cholesterol stone
• Pigment/Calcium bilirubinate stone
• Mixed stone
• Calcium Carbonate stone
Questions?