
Interactive Case Presentation #2: Autoimmune Liver and ... · Interactive Case Presentation #2:...
45
Interactive Case Presentation #2: Autoimmune Liver and Biliary Diseases Moderator: Rebekah Hamner, MSN, RN, AGCNS-BC Texas Liver Institute Austin, Texas
-
Upload
truongtram -
Category
Documents
-
view
223 -
download
0
Transcript of Interactive Case Presentation #2: Autoimmune Liver and ... · Interactive Case Presentation #2:...
InteractiveCasePresentation#2:AutoimmuneLiverandBiliary
Diseases
Moderator:RebekahHamner,MSN,RN,AGCNS-BC
TexasLiverInstituteAustin,Texas
ThePatient:T.H.(June10,2016)
HPI:52yo Caucasianfemalew/historyofelevatedliverenzymes,firstnotedApril2016.• 5/12/16:AST/ALT100s-200s,ALP180,Tbili 0.9,Albumin4.4,
Plts 280• 6/4/16:AST/ALTinthe1000s,ALP380,Tbili 1.1,Albumin3.4,
Plts 299• VS:145/92,75,16,97.6,Weight:154,BMI28
Meds:• ASA81mg,Multivit,Lipitor20mg,levothyroxine100mcg• Tooknitrofurantoin x12weeksforrecurrentUTIs lastfall

ThePatient:T.H.PMH/PSH:• Hyperlipidemia• UTIs• Anxiety• HTN• Hypothyroidism• PrediabetesFMH:• M-hypothyroidism,Sjogren
syndrome• D-Alzheimer’s,HTN• Deniesfamilyhistoryofliver
disease
Social:• Married• Nonsmoker• ETOH:2-4perweekwithdinner• IllicitDrugs:Denies• Bloodtransfusionbefore1992:Denies
• Tattoos:1fromtattooparlor10yearsago

ThePatient:T.H.ROS: PE:• +anxiety• +vagueRUQdiscomfort• +fatigue• +mildpruritus• +arthralgia
• +centraladiposity,otherwiseunremarkable
• Unabletoelicitabdtenderness
• Nohepatosplenomegaly• Nosignsofdecompensatedliverdisease
DifferentialDiagnosis• NAFLD
+Metabolicsyndromefeatures:overweight,centraladiposity,prediabetes,hyperlipidemia,HTN- LiverenzymestooelevatedforNAFLD
• HepatitisC+TailendofBabyBoomergeneration,greatestriskofhavingHCV,tattoo- Nootherriskfactors
• AutoimmuneHepatitis(AIH)+Personalhx hypothyroidism,familyhx autoimmunedisease,tookmedsbelievedtobepossibletriggersforAIH,oftenseeveryhighAST/ALT- UsuallyALPisnotelevated
• PrimaryBiliaryCholangitis(PBC)orPrimarySclerosingCholangitis(PSC)
+Middleagedfemale,fatigue,ALPiselevated,pruritus• DrugInducedLiverInjury(DILI)
+NitrofurantoinknowntocauseDILI
WorkupRecommendationLabs
• CBC,CMP,pt/INR,GGT• ImmunoglobulinsA,G,M• Viralserologies,acuteandchronic:Hep CAb,Hep BandHep A,EBV,HSV
• Geneticliverdiseases:ceruloplasmin,iron%,alpha1antitrypsin
• Autoimmune:AMAM2,ASMA,ANA
ImagingandStagingLiverDisease
• AbdominalUS• Elastography orFibroscan
Holdoffonliverbiopsyatthistimeuntillabresultsarein.

AnOverviewofPrimaryBiliaryCholangitis&PrimarySclerosing Cholangitis
EmmaPham,MPAS,PA-CTexasLiverInstitute
TransplantHepatologyUniversityofTexasHealthScienceCenter
SanAntonio,Texas

NormalHepatobiliary Anatomy
http://hb.surgery.ucsf.edu/media/2907208/UCSF045_ExtrahepaticBileDuctAnatomy

PrimaryBiliaryCholangitis(PBC)• Formerly Primary Biliary
Cirrhosis • Autoimmune progressive,
cholestatic disease which may extend over many decades
• Combination of genetic predisposition and environmental triggers
• Destruction of intrahepatic bile ducts
1. CareyEJ,etal.Lancet. 2015;386(10003):1565-1575.2. Primarybiliarycirrhosis(PBC).PathPedia website.
http://www.pathpedia.com/education/eatlas/histopathology/liver_and_bile_ducts/primary_biliary_cirrhosis_(pbc).aspx.AccessedFebruary17,2016.
3. 1. Kumagi T, Heathcote EJ. Orphanet J Rare Dis. 2008;3:1.
Presenceoflymphocytes,plasmacells,macrophages,polymorphonuclear cells

ImportantTidbitstoRemember
• 95% affected are women• After HCV, second most common reason
for transplant in women• Elevated alkaline phosphatase is main lab
feature• Symptoms may be absent early in disease• Untreated, most will progress to advanced
disease over 15 years
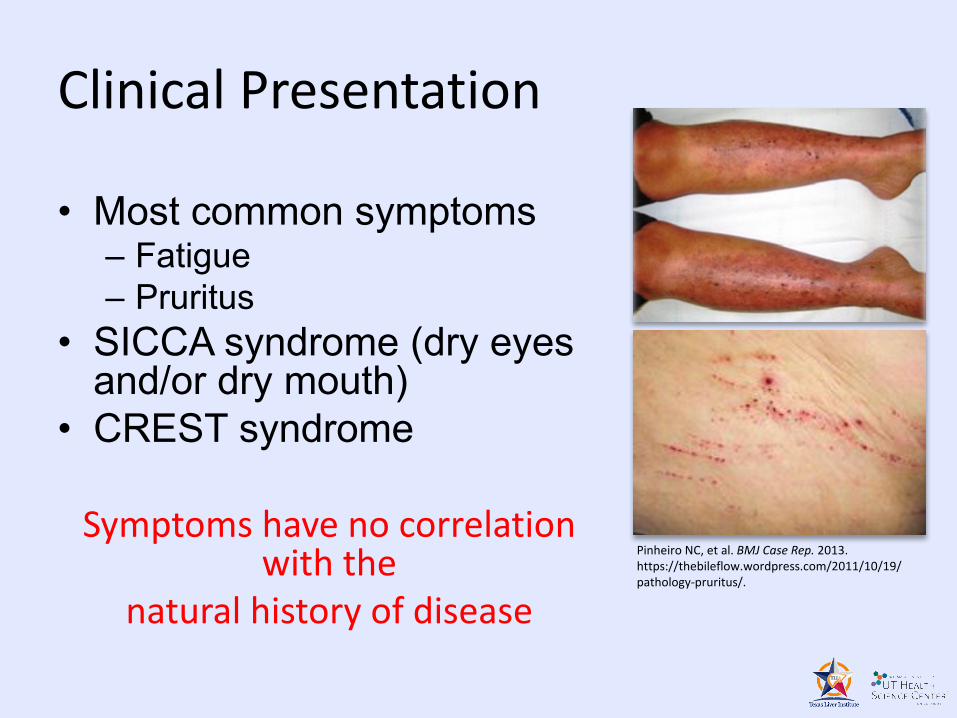
ClinicalPresentation
• Most common symptoms– Fatigue– Pruritus
• SICCA syndrome (dry eyes and/or dry mouth)
• CREST syndrome
Symptomshavenocorrelationwiththe
naturalhistoryofdisease
PinheiroNC,etal. BMJCaseRep. 2013.https://thebileflow.wordpress.com/2011/10/19/pathology-pruritus/.

Calcinosis Raynaud’s
Sclerodactyly Telangiectasias
CREST
Esophagealdysmotility
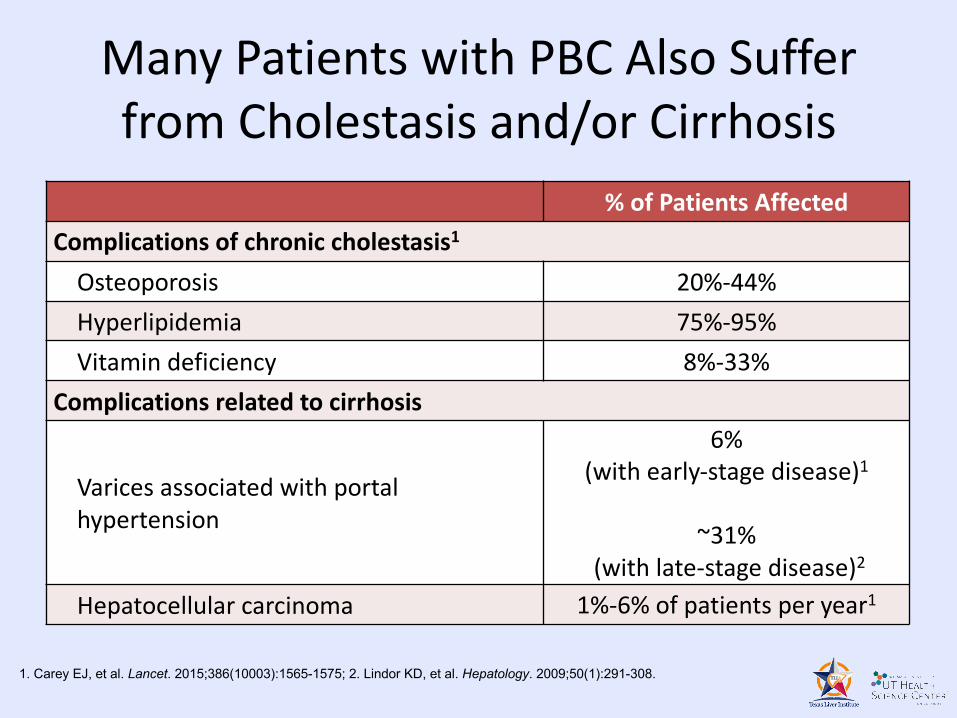
ManyPatientswithPBCAlsoSufferfromCholestasisand/orCirrhosis
%ofPatientsAffectedComplicationsofchroniccholestasis1
Osteoporosis 20%-44%Hyperlipidemia 75%-95%Vitamindeficiency 8%-33%
Complicationsrelatedtocirrhosis
Varices associatedwithportalhypertension
6%(withearly-stagedisease)1
~31%(withlate-stagedisease)2
Hepatocellularcarcinoma 1%-6%ofpatientsperyear1
1. Carey EJ, et al. Lancet. 2015;386(10003):1565-1575; 2. Lindor KD, et al. Hepatology. 2009;50(1):291-308.
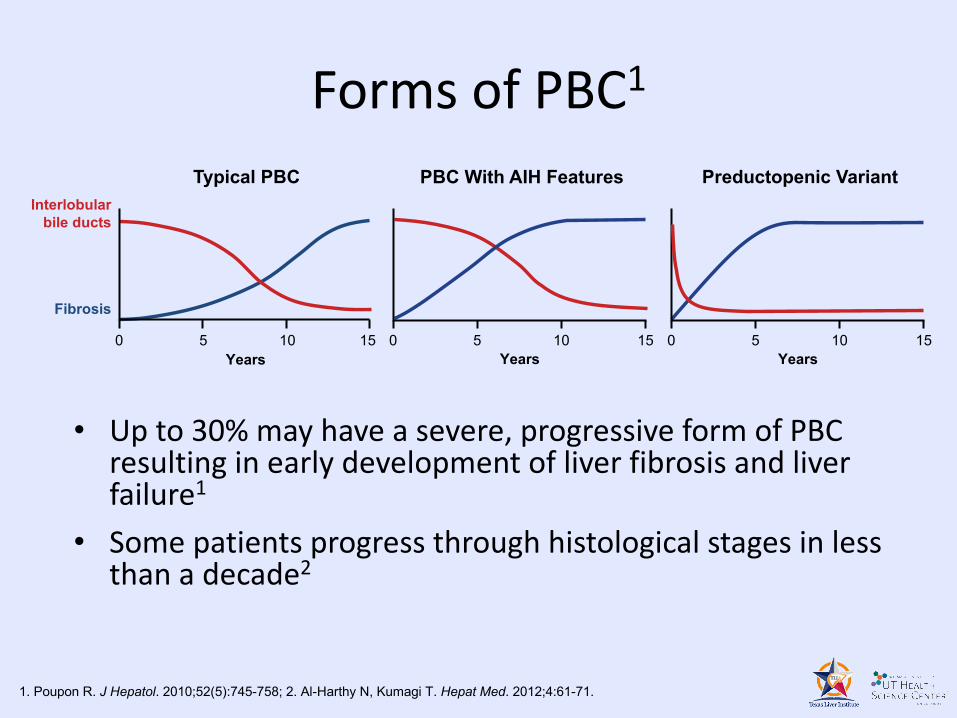
FormsofPBC1
• Upto30%mayhaveasevere,progressiveformofPBCresultinginearlydevelopmentofliverfibrosisandliverfailure1
• Somepatientsprogressthroughhistologicalstagesinlessthanadecade2
PBC With AIH Features
0 5 10 15Years
Preductopenic Variant
0 5 10 15Years
Typical PBC
Fibrosis
Interlobularbile ducts
0 5 10Years
15
1. Poupon R. J Hepatol. 2010;52(5):745-758; 2. Al-Harthy N, Kumagi T. Hepat Med. 2012;4:61-71.
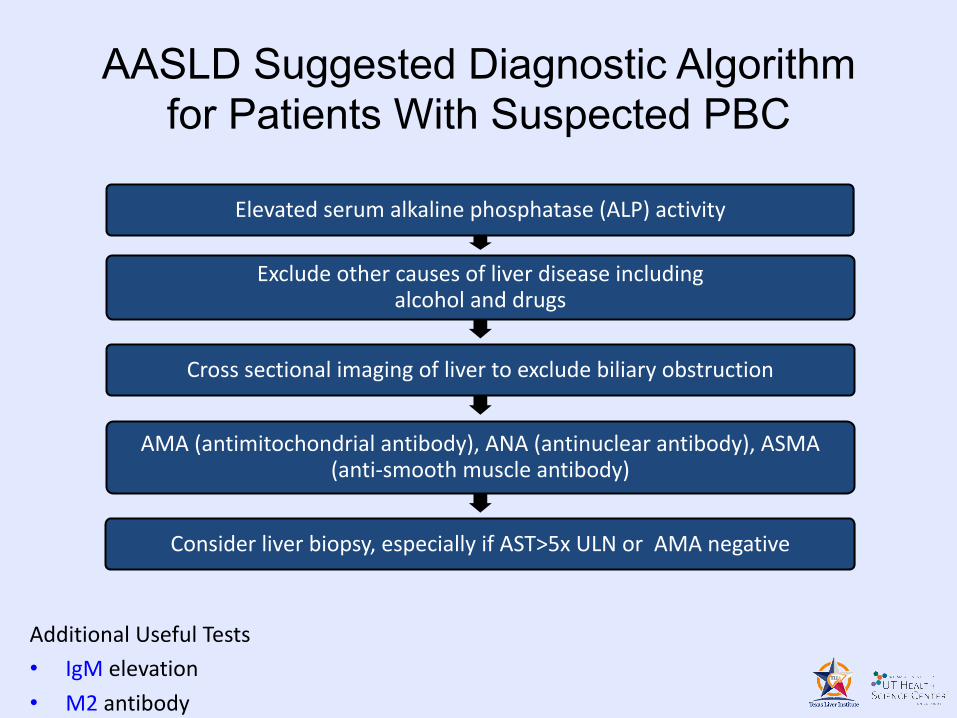
AASLD Suggested Diagnostic Algorithm for Patients With Suspected PBC
Elevatedserumalkalinephosphatase(ALP)activity
Excludeothercausesofliverdiseaseincludingalcoholanddrugs
Crosssectionalimagingoflivertoexcludebiliaryobstruction
AMA(antimitochondrial antibody),ANA(antinuclearantibody),ASMA(anti-smoothmuscleantibody)
Considerliverbiopsy,especiallyifAST>5xULNorAMAnegative
AdditionalUsefulTests• IgM elevation• M2 antibody
Ursodeoxycholic Acid (UDCA)• Orally administered nontoxic
bile acid • Balances the bile acid ratio
normally produced by the liver, some of which are more toxic to the liver
• UDCA in a dose of 13-15 mg/kg/day
• UDCA is initiated gradually and given BID
AASLD Guidance Document
Ursodeoxycholic Acid (UDCA)
• Improvement in liver tests will be seen within a few weeks and 90% of the improvement usually occurs within 6-9 months
• Safe, may improve clinical symptoms, delay progression of disease and survival, and improve QOL
• However, up to 40% of PBC patients treated with UDCA have a suboptimal response
Pares A, Gastroenterology, 2006; Marschall HU, Gastroenterology, 2005.
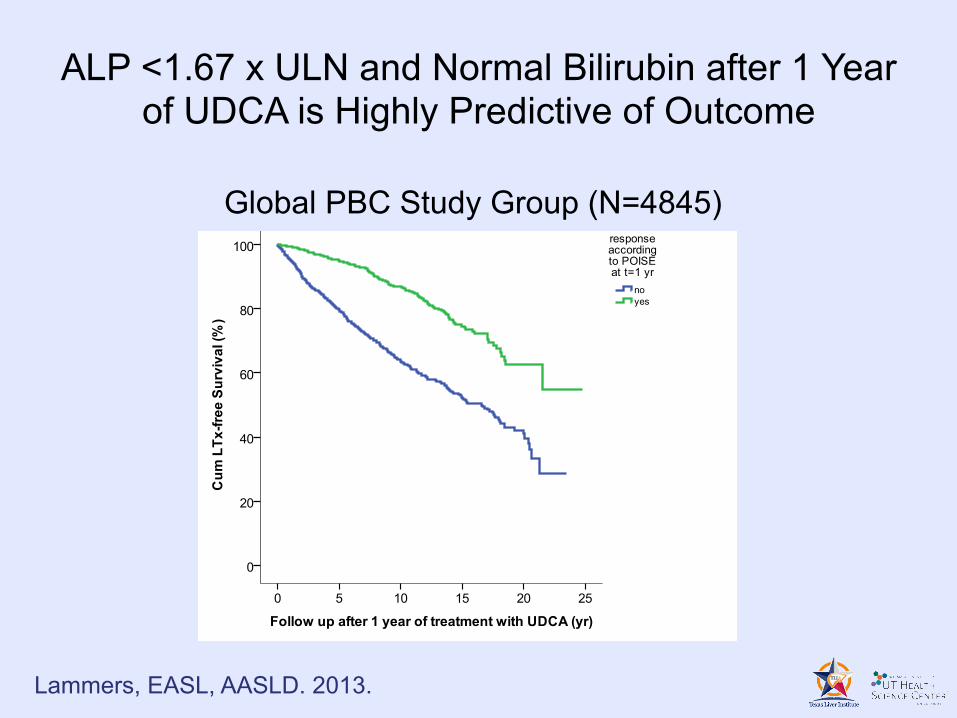
ALP <1.67 x ULN and Normal Bilirubin after 1 Year of UDCA is Highly Predictive of Outcome
Global PBC Study Group (N=4845)
Lammers, EASL, AASLD. 2013.

Obeticholic Acid (OCA)
• A modified bile acid and FXR agonist
• OCA given to individuals with PBC with an inadequate response to or unable to tolerate UDCA
• Produced a significant clinically meaningful improvement in liver biochemistry
• Approved by FDA on May 27, 2016 (Ocaliva)

Long-term Management of Patients with PBC (AASLD Guidance)
• Liver tests every 3-6 months• Thyroid status (TSH) annually• Bone mineral densitometry every 2-4 years• Vitamins A, D, K annually if bilirubin >2.0• Upper endoscopy every 1-3 years if cirrhotic
or Mayo risk score >4.1• Ultrasound ± AFP every 6 months in patients
with known or suspected cirrhosis

PBCPrognosisUsingMayoRiskScore

PBCPrognosisUsingMayoRiskScore

Livertransplantation(LT)• Indicatedfor
– Patientsprogressingtodecompensatedcirrhosis
• Patientswithlatediagnosis• NoresponsetoUDCA(30-40%)
• MELD> 15• HCCmeetingtransplantcriteria
– Patientswithintractablepruritus

PBCSummary• PBCischroniccholestaticdiseaseresultingindestructionofintrahepaticbileducts
• MostcommonsymptomsofPBCisfatigueandprofoundpruritus
• ElevatedALPwithpositiveAMAishighlydisease-specific
• MajorityofpatientsrespondtoUDCA• OCAcanbeusedasadjuncttherapyforpatientsthatarenon-responderorpartialresponderstoUDCA
• Livertransplantationisanoptionforpatientswhoaredecompensatedorhaverefractorypruritus

WhatisPSC?:PrimarySclerosingCholangitis
• Chronicprogressiveinflammatorydiseasethanaffectsextraand/orintrahepaticbileducts–biliarystricturing andfibrosis
– “chainoflakes”oncholangiogram
Bileductstricturing=“chainoflakes”
ERCP:endoscopicretrogradecholangio-pancreatography

Epidemiology,NaturalHistory&Prognosis
• Prevalence6-8/100,000• Usuallydiagnosedin20sand30s• Malepredominance~3:1• 80%haveIBD- usuallyulcerativecolitis(UC)90%
– 4%withUCgetPSC• ~44%asymptomaticatdiagnosis• Mediansurvival~12years• 4th leadingdiagnosisleadingtoLTinNorthAmerica• Associatedwithcancer
– Cholangiocarcinoma– HCC(withcirrhosis)– ColonCancer(ifIBDpresent)
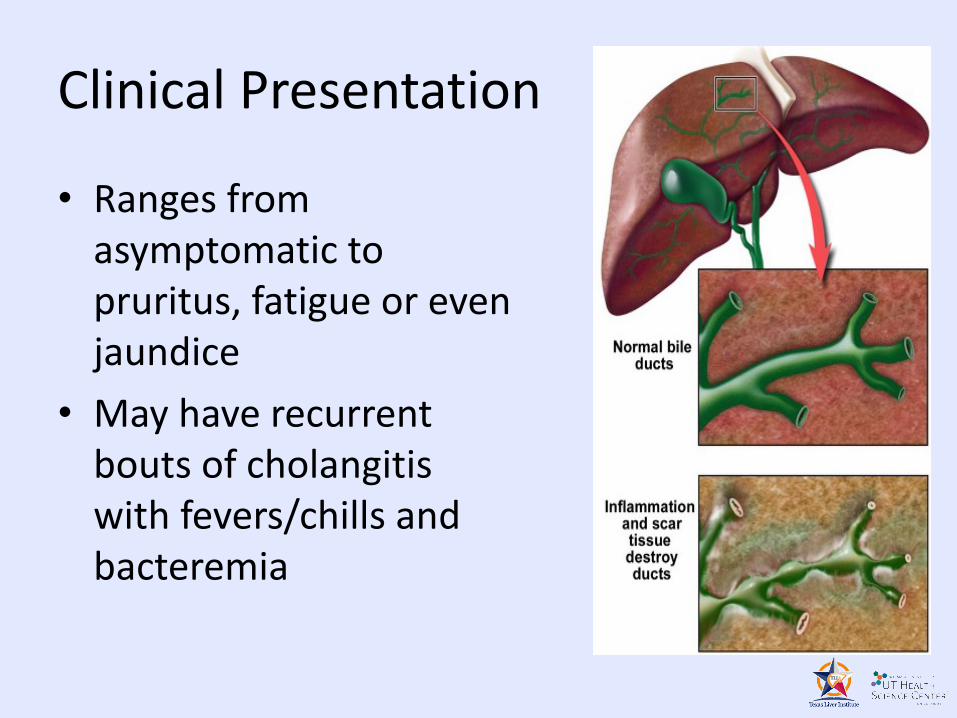
ClinicalPresentation
• Rangesfromasymptomatictopruritus,fatigueorevenjaundice
• Mayhaverecurrentboutsofcholangitiswithfevers/chillsandbacteremia

9%
31%
50%
2% 5%
10%
10Years 20Years 25Years
Ris
k %
PSC/CUC CUC
Broome U, Lofberg R, Veress B, et al. Primary sclerosing cholangitis and ulcerative colitis: Evidence for increased neoplastic potential. Hepatology. 1995;22(5):1404-8
ColonCancerRiskwithIBD/PSC

DiagnosisofPSC• CholestaticLiverTests(elevatedALPandGGT)
• Cholangiography(MRCPorERCP)
• Exclusionofsecondarysclerosing cholangitis
• 95%atleastoneautoantibody– 85%+ pANCA– 50%+ ANA– 25%+ SMA
HistologicFeaturesofPSC
Eaton JE, Talwalkar JA, Lazaridis KN, et al. Pathogenesis of Primary Sclerosing Cholangitis and Advances in Diagnosis and Management. Gastroenterology. 2013;145:521-536.
pANCA isperinuclear antineutrophil cytoplasmicantibody

Treatment
• Medical management– Ursodeoxycholic acid (20-25 mg/kg)
• Uncertain benefit but should not use high dose– Pruritus: cholestyramine, rifampicin, opioid antagonist
• Endoscopic therapy– Balloon dilation and stenting
• Dilation recommended due to decreased risk of infection
• Follow bili and alk phos for treatment improvement• Cholangiocarcinoma (CCA) and HCC
surveillance

LiverTransplantation
• Indicatedfor– Patientsprogressingtodecompensatedcirrhosis
• MELD> 15• HCCmeetingtransplantcriteria
– Patientswithintractablepruritus,recurrentbacterialcholangitis,orcholangiocarcinoma
• EventuallymostpatientswillrequireLTasthereisnoeffectivetreatment
PSCSummary
• Chronicprogressiveinflammatorydiseaseaffectextra- and/orintrahepaticbileducts
• Noestablishedtherapy,howeverursodiol canbeused
• Riskofbiliarycancersandcoloncancer
• Livertransplantationisoftentheonlytreatmentoption

SimilaritiesandDifferencesPrimaryBiliary Cholangitis PrimarySclerosing Cholangitis
EtiologyUnclear EtiologyUnclear
EffectsIntrahepaticbileducts Caneffectextra-intrahepaticbileducts
Vanishingbileducts
Presencelymphocytes,plasmacells,macrophages,andPMNsonbiopsy
Stricturing ofbileducts
Absencesofinflammatorycellsonbiopsy
AssociatedwithSICCAorCRESTsyndrome AssociatedwithUC
UDCAhelpsinmajorityofpatients;OCA recentlyapproved
Newdrugtherapiesareinclinicaldevelopment;ingeneralPSCleads
tolivertransplantation

Lab/ImagingResults(June10,2016)• Labs:
–Alb4.4,Tbili 0.5,Alk Phos 200,AST91,ALT110,IgMandIgGelevated,ferritin444,GGT72,WBC5.9,Hgb 13.1,HCT40.7,Plt 280
–EBVPCRneg,HSVPCRneg,HAVIgMneg,HBVsurfaceAGneg,HBVcoreIgMABneg,HCVABneg
–ANA1:160(pos),AMAM2+,SMA+•AbdominalUS
• Liver:mildfattyliverwithnofocallesions,spleen:normal•Elastography
• 8.2kPa• Moderate fibrosis?
•BiopsyperformedandconfirmedPBCandAIH

AutoimmuneHepatitis(AIH)
ChristyRosas,MPAS,PA-CTexasLiverInstituteSanAntonio,Texas
AIH:ClinicalPresentation
• 30%presentwithcirrhosis
• Upto50%maypresentwithjaundice
• Asymptomatic(35-45%)withabnormalenzymes– Oftendiscoveredduringevaluationforotherautoimmuneconditions

AIH: DemographicsandEpidemiology
• Afflicts~200,000inU.S.A.• Incidence1.9per105peryear
• Prevalence16.9per105
• Afflictsbothchildrenandadults• Femaletomaleratio=4:1
• Bimodalagedistribution:10-20vs.45-75yrs• 6%livertransplantsinUS

AIHPathogenesis
• Geneticfactors– Antigenpresentation/immunocyte activation– DRB1encodesforMHCIIantigenbindinggrooves(antigenpresentationtoTcells)
• Triggeringfactors– Infections(HCV,HDV)– Medications
-Minocycline,Nitrofurantoin,Methyldopa,Atorvastatin,Diclofenac,Augmentin,Isoniazid,Infliximab
Czaja etal.Hepatology 2002;36:479Krawitt. N Engl J Med 2006;354:54
Manns et al. Hepatology 2006;14:S132
Diagnosis
• Serology– PositiveANA,SMAorLKM
– ElevatedserumIgG totwicenormallevels
– 5%haveseronegativedisease
• Histology– BiopsyrequiredfordiagnosisALWAYS
– Sometimesatypicalfeatures
– Overlapsyndromes(PBC/PSC)

GoalsfortreatmentofAIH
• NormalizationofALTandIgG
• Normalizationofhistology
• Regressionoffibrosis
• Preventionofcirrhosis
• Minimizationofsideeffects

AIH: CriteriaforTreatment
• Symptomaticdiseaseandeither–AST>10-foldnormal
–AST5-10foldnormaland>2-foldelevationofIgG
• Presenceoffibrosis
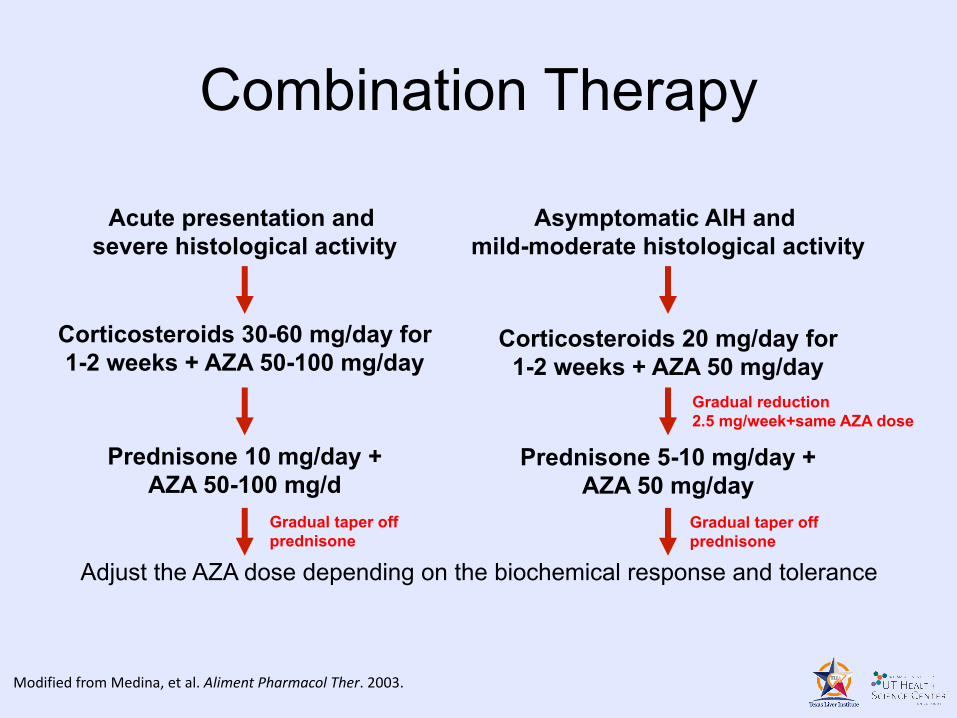
Acute presentation and severe histological activity
Asymptomatic AIH and mild-moderate histological activity
Corticosteroids 30-60 mg/day for 1-2 weeks + AZA 50-100 mg/day
Corticosteroids 20 mg/day for1-2 weeks + AZA 50 mg/day
Adjust the AZA dose depending on the biochemical response and tolerance
Prednisone 10 mg/day +AZA 50-100 mg/d
Prednisone 5-10 mg/day +AZA 50 mg/day
Gradual taper offprednisone
Gradual reduction2.5 mg/week+same AZA dose
Gradual taper offprednisone
ModifiedfromMedina,etal.AlimentPharmacolTher.2003.
Combination Therapy

AIHTreatmentSideEffects
• Longtermprednisone– Osteoporosisandfractures– Diabetes– Obesity– CVdisease
• Cytopenias• AZA-inducedpancreatitis• Longtermlymphomaandskincancerrisks

AIH: TakeHomePoints
• Chronichepatocellulardiseaseingeneticallypredisposedpatientsofuncleartrigger
• Diagnosisbaseduponliverenzymes,serology,gammaglobulins,andhistology
• Immunosuppressivetherapyisthemainstayoftreatmentandislongtermfornearlyallpatients
• Tailortherapybasedupontreatmentendpoints
PatientT.H.:TreatmentPlan
• PBC–Ursodiol–Obeticholic acidifnoresponse
• AIH–Treatwithazathioprineandprednisone,weaningthelatteroffinfewmonths


















