Integrated Health Service Plan 2016-2019 Appendices - ReCAP - FINAL.pdfthe development of the...
100
Integrated Health Service Plan 2016-2019 Appendix: B Regional Capacity Analysis and Projections (ReCAP)
Transcript of Integrated Health Service Plan 2016-2019 Appendices - ReCAP - FINAL.pdfthe development of the...

Integrated Health Service Plan 2016-2019
Appendix: B
Regional Capacity Analysis and Projections (ReCAP)

2
ABOUT THIS REPORT
This Regional Capacity Analysis and Projections (ReCAP) report was compiled by the
South East Local Health Integration Network (South East LHIN) as an environmental
scan of the region, and includes socio-demographic, health status, health system
utilization, health human resources, and health funding information. This report was
primarily developed to inform the South East LHIN’s Integrated Health Service Plan for
2016/17 to 2018/19, but can also be used as a reference tool for various regional
planning or research projects.
Data for this report was obtained from a variety of administrative and reporting
sources that are available at the regional, provincial, and federal levels. None of these
sources have endorsed or confirmed the accuracy of the analysis in this report. Many
subject matter experts were consulted to refine the analysis and provide comments on
the information in this report. However, in a few cases time did not allow for extensive
review and feedback from all sectors, particularly the hospital, primary, and long-term
care sectors. Readers with questions or comments about the content in this report are
encouraged to follow up with the South East LHIN Knowledge Management team.

3
TABLE OF CONTENTS
INTRODUCTION ............................................. 5
SOUTH EAST LHIN GEOGRAPHIC REGIONS ............ 5
POPULATION AND DEMOGRAPHIC
INFORMATION .............................................. 7
POPULATION DEMOGRAPHICS AND PROJECTED
POPULATION GROWTH .................................... 7
SOCIO-DEMOGRAPHIC CHARACTERISTICS .............. 9
Immigration and Visible Minorities ..................... 9
Language .............................................................. 9
Living Arrangements for the 65+ Population ..... 10
Education ........................................................... 10
Labour Force Activity ......................................... 11
Income ............................................................... 11
Material and Social Deprivation ........................ 11
UNIQUE POPULATIONS .................................. 12
Francophone Population ................................... 12
Indigenous Population ....................................... 13
HEALTH BEHAVIOURS, HEALTH STATUS, AND
CHRONIC DISEASE ....................................... 15
HEALTH BEHAVIOURS .................................... 15
Poor Diet ............................................................ 15
Physical Inactivity ............................................... 15
Daily Smokers ..................................................... 16
Heavy Alcohol Consumption .............................. 16
Influenza Vaccination ......................................... 16
HEALTH STATUS AND CHRONIC CONDITIONS ........ 17
Health Status ...................................................... 17
Chronic Conditions ............................................. 18
Hospitalizations for Chronic Conditions............. 22
Health Status and Chronic Conditions in the 65+
Population .......................................................... 22
BIRTHS AND DEATHS .................................... 24
BIRTHS AND MATERNAL HEALTH ....................... 24
Births and Fertility Rates ................................... 24
Birth Outcomes ................................................. 24
Maternal Health ................................................ 25
DEATHS ..................................................... 25
Overall Mortality Trends ................................... 25
Causes of Death ................................................. 26
Setting of Death................................................. 27
COMMUNITY-BASED SERVICES ...................... 28
PRIMARY CARE ............................................ 28
Types of Primary Care Provider Models ............ 28
Utilization of Core Primary Care Services .......... 33
Access to, and Satisfaction with, Primary Care . 34
COMMUNITY HEALTH CENTRES ......................... 35
Client Characteristics ......................................... 36
Individual encounters with CHC providers ........ 36
Group Encounters with CHC providers ............. 38
COMMUNITY SUPPORT SERVICES ...................... 39
General Data Notes ........................................... 39
General Observations ........................................ 40
Home Support Services ..................................... 41
Hospice Services ................................................ 42
Specialized Services ........................................... 42
Alzheimer Societies ........................................... 43
COMMUNITY ADDICTIONS AND MENTAL HEALTH ... 44
Overview of the Addictions and Mental Health
Redesign ............................................................ 44
General Data Notes ........................................... 45
Utilization of Community AMH Services ........... 46
Community Addictions Services ........................ 48
Community Mental Health Services .................. 50
HOME CARE ................................................ 53

4
HOSPITAL-BASED SERVICES .......................... 54
HOSPITALS IN THE SOUTH EAST LHIN ................ 54
EMERGENCY DEPARTMENT ............................. 55
Overall Utilization .............................................. 55
Utilization by Hospital ........................................ 56
Time of Day ........................................................ 56
Lengths of Stay ................................................... 57
SAME DAY SURGERY ..................................... 57
ACUTE INPATIENT ........................................ 59
Overall Utilization .............................................. 59
Alternate Level of Care (ALC) ............................. 60
Services and Programs ....................................... 61
SURGICAL AND DIAGNOSTIC WAIT TIMES AND
VOLUMES .................................................. 62
Completed Cases................................................ 62
Open Surgical Cases ........................................... 64
INPATIENT MENTAL HEALTH ........................... 66
CRITICAL CARE ............................................ 66
Overall Volume and Distribution of Services ..... 66
Source of Admission .......................................... 67
Patient Demographic and Clinical
Characteristics .................................................... 68
Interventions ...................................................... 69
Discharge Information ....................................... 69
Average Lengths of Stay ..................................... 69
Occupancy Rates ................................................ 70
Avoidable Days ................................................... 70
Readmissions ..................................................... 70
Mortality Rates .................................................. 70
POST ACUTE CARE ....................................... 71
Complex Continuing Care .................................. 71
Inpatient Rehabilitation ..................................... 71
LONG-TERM CARE ........................................ 73
Bed Supply ......................................................... 73
Wait List and Demand ....................................... 74
Resident Characteristics .................................... 75
HOSPICE PALLIATIVE CARE ............................ 76
Hospital-Based Services - Acute Inpatient ........ 76
Community-Based Services ............................... 79
HEALTH LINKS .............................................. 80
Overview of the Health Links Initiative ............. 80
Describing the Health Links Target Population . 80
HEALTH HUMAN RESOURCES ......................... 83
PHYSICIANS ................................................ 83
Overall Trends by Specialty ............................... 83
Family Physicians ............................................... 83
ALLIED HEALTH PROFESSIONALS ....................... 86
FUNDING .................................................... 89
OVERVIEW OF HEALTH SYSTEM FUNDING REFORM . 89
Why Change is Necessary .................................. 89
Shifting from the Historic Funding Approach .... 89
Components of Health System Funding
Reform ............................................................... 89
HSFR Funding Implications ................................ 91
OVERALL FUNDING BY SECTOR ......................... 94
HEALTH SYSTEM PERFORMANCE .................... 95
MLAA INDICATOR RESULTS ............................. 95
Performance Indicators ..................................... 95
Monitoring Indicators ........................................ 97
APPENDIX A – GLOSSARY OF TERMS .............. 99

5
INTRODUCTION
This Regional Capacity Analysis and Projections
(ReCAP) report is intended to provide data analysis at
the local level to support recommendations related to
the development of the Integrated Health Service Plan
(IHSP). For this third iteration of ReCAP, the analysis is
in support of IHSP4 for the fiscal year 2016/17 to
2018/19 period.
The guiding principle behind this effort is that if
programs/services are to meet the needs of the
population, then greater emphasis has to be placed on
the evidence behind local planning and be supported
by the collection and analysis of available data and
projections at the local level. Information in this
analysis was obtained in part from the IHSP
Environmental Scan from the Health Analytics Branch
at the Ministry of Health and Long-Term Care
(MOHLTC), and more detailed and local analyses were
accomplished using a number of data sources available
to the South East Local Health Integration Network
(South East LHIN).
The ReCAP analysis has been divided into a variety of
components, including sections on the South East LHIN
population (socio-demographic characteristics, health
status and behaviours, births, and deaths), utilization
profiles of different health system sectors and services
within the South East LHIN, information on Health
Links and their target population, a summary of health
human resources, and information on Health System
Funding Reform (HSFR) and its implications for the
health system. Because the results are quite extensive,
only a bulleted summary of the key findings are
presented in this report.
In most cases, annual information is summarized based
on the fiscal year, which is defined as the period
between April 1 and March 31. The type of annual
information used (e.g. calendar or fiscal year) is noted
at the start of each section.
South East LHIN Geographic Regions
Historically, ReCAP analyses have been based on the
SubLHIN geographies, along with other geographic
groups that make up the LHIN. However, with the
introduction of the Health Links initiative in the South
East LHIN in 2013, analysis and planning efforts have
been focused on these new geographic regions.
A map with the seven South East LHIN Health Link
geographies is shown in Figure 1. Maps for the other
geographic regions commonly used for planning
purposes (Public Health Units, SubLHINs, and
municipalities) are also included.

6
Figure 1: South East LHIN Geographies: (1) Health Links; (2) Public Health Units; (3) SubLHINs; (4) Municipalities.
(2) (1)
(3) (4)

7
POPULATION AND
DEMOGRAPHIC
INFORMATION
Population Demographics and Projected Population Growth
Population estimates and projections were obtained
from the Ontario Ministry of Finance. Detailed
projections by SubLHIN and Health Link were computed
by the South East LHIN using a cohort component
methodology that incorporates factors such as deaths,
births, and migration. A detailed explanation for the
projections methodology can be found here.
• As of 2014, the South East LHIN was home to
almost 495,000 people. This accounts for 3.6% of
the population of Ontario, making the South East
LHIN the second smallest LHIN based on total
population.
• A quarter of the population lives in a large urban
centre, while 45% live in a rural area, making the
South East LHIN the most rural LHIN population in
Ontario.
• Just over half of the population lives in the
municipalities of Kingston, Belleville, Quinte West,
Prince Edward County, and Brockville. Kingston is
the only municipality with a population greater
than 100,000; all other areas have a population of
about 50,000 or less.
• Between 2009 and 2013, the LHIN population
increased by only 1.5%, which was much lower
than the Ontario growth rate of 3.5%.
• By 2017, there will be more people aged 70 and
over than those aged 15 and below in the South
East LHIN.
• As of 2013, one in five South East LHIN residents
were 65+ years of age. This percentage has
increased from 16.6% in 2006 and is projected to
continue increasing as the “boomer” generation
(approximately those 45-64 years of age) ages. By
2016, those aged 65+ will account for 22% of the
LHIN’s population, and by 2026, this proportion
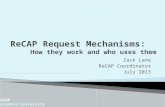
will rise to 28% (Figure 2). In all of these years, the
South East LHIN is expected to have the highest
proportion aged 65+ compared to all the LHINs.
The 65+ age group is projected to grow in all
regions of the South East LHIN with average
annual growth between 3.0% and 3.8% between
2011 and 2026.
• The 65+ age group is the only age group growing
dramatically in the South East LHIN, with
projected negative average annual growth rates
for younger age groups. The 75+ population is
projected to increase by 50% by 2025 and double
in size by 2033.
• By 2018 (in the time frame of this IHSP), 10% of
South East LHIN residents will be 75 years of age
and over. By 2025, this will increase to 13%.
• The 65-74 and 75+ age groups are projected to
grow in all Health Links between 2016 and 2021
(Table 1). The highest annual growth rate for
those 65-74 is projected to be in Salmon River
Figure 2: Population Pyramid for the South East LHIN, 2011, 2016, 2021, and 2026.
Population
Count

8
(3.5% annual growth), and the highest rate for
those 75+ is in Salmon River and Rural Kingston
(both 4.8%).
• The younger age groups will generally experience
negative growth in each Health Link, except for
the Kingston Health Link where there will be
minimal growth (just over 1% annually) in the 0-
19 and 20-44 year age groups (Table 1).
• The Rideau-Tay and Rural Hastings Health Links
are projected to have the highest percentage of
the population aged 65+ in 2016 (25.9% and
25.4%, respectively) (Figure 3). By 2021, the
population aged 65+ is expected to account for
about 30% of the population in both of these
areas.
• In terms of absolute numbers, the Quinte and
Kingston Health Links are projected to have the
highest number of residents aged 65+ in 2016
(30,538 and 24,172, respectively).
• The aging population in the South East LHIN will
have implications for various health issues,
programs, and sectors, which will be explored
further in later sections of the ReCAP analysis.
00-19 20-44 45-64 65-74 75+
Rural Hastings -0.1% -0.4% -1.2% 2.7% 4.3% 0.4%
Quinte -0.1% -0.4% -0.8% 2.7% 3.1% 0.3%
Salmon River -0.2% 0.0% 0.4% 3.5% 4.8% 1.0%
Rural Kingston -0.7% -0.1% -0.7% 2.1% 4.8% 0.3%
Kingston 1.3% 1.1% -0.6% 2.5% 3.0% 1.0%
Rideau-Tay -0.7% -0.6% -2.2% 2.9% 4.2% 0.0%
Thousand Islands -1.7% -1.1% -1.2% 2.0% 3.7% -0.2%
South East LHIN 0.0% 0.1% -0.9% 2.5% 3.6% 0.5%
Age GroupHealth Link Total
Table 1: Projected Average Annual Population Growth between 2016-2021 by Health Link and Age Group.
Figure 3: Population Pyramid by Health Link, South East LHIN, 2011, 2016, 2021, and 2026.

9
Socio-Demographic Characteristics
Examining socio-demographic characteristics is a
means for understanding the population at a
general level, but it is also important for
identifying possible variation in social factors
known to be associated with health status and
health outcomes.
Information in this section was obtained from the
Statistics Canada 2011 Census and National Household
Survey (NHS). Due to high non-response rates for
certain areas for the NHS, data for certain
municipalities were not released by Statistics Canada
due to data quality concerns. As a result, the South East
LHIN could not use NHS information to produce socio-
demographic information at the Health Link level. LHIN
level-estimates were released by the MOHLTC and
were deemed to have acceptable data quality. Also
note that changes in data collection methods between
the NHS and previous census years impaired the ability
to interpret trends over time for NHS indicators.
Definitions for these indicators, as well as additional
details about the Census and NHS, can be found here.
IMMIGRATION AND VISIBLE MINORITIES
• The South East LHIN has a relatively low
proportion of immigrants and visible minorities. In
2011, 8.5% of the population were immigrants
(compared to 28.5% provincially) and less than 1%
were recent immigrants (arriving in Canada
between 2006 and 2011) (Figure 4). The highest
proportion of immigrants were in the
municipalities of Kingston and Brighton (~13% of
the population).
• Just 3.4% of South East LHIN residents were
visible minorities (compared to 25.9%
provincially). There were larger visible minority
populations in the municipalities of Kingston
(7.4%) and Belleville (4.9%).
• The majority (79%) of South East LHIN residents
were born in Ontario, followed by other places in
Canada (12%), Europe (5%), and the USA,
Caribbean/Central & South America, and
Asia/Middle East (~ 1% each).
• Certain areas of the South East LHIN had a higher
proportion of residents born in other countries
(e.g., Asia and the Middle East in Kingston – 3.4%
of the population).
LANGUAGE
• About 9 in 10 people in the South East LHIN
(91.9%) reported English as their mother tongue
in 2011, which was substantially higher than the
provincial rate (70.4%) and highest of all the
LHINs (Figure 4).
• About 3% of the South East LHIN population (or
about 13,800 people) reported French as their
mother tongue in 2011. Only 0.2% had no
knowledge of neither English nor French.
• The proportion of the South East LHIN population
with French as mother tongue has increased
slightly over time (was 2.4% in 1996).
• The proportion of the population with French as a
mother tongue was highest in the Kingston
(3.6%), Rideau-Tay (3.3%), and Thousand Islands
(2.9%) Health Links. Rates were higher when
looking at smaller areas of geography, in
particular municipalities in the eastern part of the
LHIN (Merrickville-Wolford,
Edwardsburgh/Cardinal, and Montague, all >4%)
and larger municipalities including Kingston and
Quinte West (both ~4%).

10
• Nearly all (96.8%) South East
LHIN residents reported
speaking English most often
at home.
• The proportion of the South
East LHIN population with
French or other languages
as mother tongue increased
with increasing age.
LIVING ARRANGEMENTS FOR THE 65+ POPULATION
• In 2011, the majority
(67.4%) of the population
aged 65 and over in the
South East LHIN lived with
relatives in a private
dwelling (Figure 4).
• The proportion of the 65+
population living alone in the South East LHIN
(24.1%) was slightly higher than for the province
as a whole (22.8%).
• Females aged 65+ were more likely to live alone
than males (31.8% versus 15.0%).
• Across the LHIN the population aged 65+ living
alone was highest in the Kingston and Thousand
Islands Health Links (28.1% and 26.5%,
respectively) and lowest in the Rural Kingston
Health Link (19.4%).
• The proportion living alone has either remained
the same or declined over time in all areas of the
LHIN (was 27.1% in 1996 for the South East LHIN
overall).
EDUCATION
• In 2011, 12.5% of South East LHIN residents
between 25 and 64 years of age had less than a
high school education (Figure 4). This rate was
slightly higher than the province as a whole
(11.0%) and has declined over time. The
percentage of those with less than a high school
education was highest in the municipalities of
Tudor and Cashel, Faraday, and Tyendinaga
Mohawk Territory (all higher than 27%).
• In 2011, 59.9% of South East LHIN residents
between 25 and 64 years of age had completed
some form of postsecondary education. This
proportion was lower than the province as a
whole (64.8%).
Figure 4: Select socio-demographic characteristics, South East LHIN and Ontario, 2011.
Note: Number in brackets indicates the LHIN rank (out of the 14) for each indicator.

11
LABOUR FORCE ACTIVITY
• Labour force participation rates in 2011 were
lower for the South East LHIN compared to the
province as a whole (61.0% versus 65.5%, Figure
4), which is likely due to the relative size of the
65+ population in the LHIN.
• Labour force participation rates were higher for
males compared to females.
• Certain areas of the LHIN have lower labour force
participation rates; however, most are areas with
a relatively larger population over 65 years of age
(e.g., Tudor and Cashel, Limerick, and Faraday).
• Unemployment rates in 2011 were similar
between the South East LHIN and the province as
a whole (8.0% versus 8.3%).
• Certain areas of the LHIN have relatively low
unemployment rates (e.g., Centre Hastings
(2.8%), Westport (3.4%), and Frontenac Islands
(3.7%)).
• Unemployment rates have increased between
2006 and 2011 in most areas.
INCOME
• Fourteen percent of the South East LHIN
population were living in low income in 2011,
which was similar to the province overall (Figure
4).
• There was a marked difference in the percent of
population living in low income across the LHIN,
ranging from 3.0% in Frontenac Islands to 39.7%
in Tudor and Cashel.
MATERIAL AND SOCIAL DEPRIVATION
The deprivation index information presented below
was produced using the methodology developed by
Pampalon et al. (see details here). Calculation of the
deprivation index for 2011 has not been completed due
to the data quality issues associated with the NHS.
• Based on data from 2006, certain rural areas of
the LHIN were noted to have higher levels of
material deprivation including Addington
North/Central (N/C) Frontenac and North
Hastings SubLHIN areas (Table 2). Conversely,
more urban areas tended to be more socially
deprived, particularly in Kingston & Islands and
Belleville. Looking at the combined material and
social deprivation measure, Addington N/C
Frontenac, North Hastings, and Belleville were
noted to be most deprived.
Table 2: Deprivation index rankings (using quintile levels 1 = less deprived to 5 = more deprived) by type (material, social, and combined) and SubLHIN area, 2006.
SubLHIN Material Social Combined
Addington N/C Frontenac 5 2 5
Belleville 2 5 4
Brockville 2 4 3
Central Hastings 3 2 4
Gananoque Leeds 1 3 2
Kingston and Islands 1 5 3
North Hastings 4 3 5
Prince Edward County 1 2 2
Quinte West 2 2 3
Rideau Lakes 1 2 2
SE Leeds Grenville 2 2 3
Smiths Falls, Perth, Lanark 2 4 4
South Frontenac 1 1 1
Stone Mills Loyalist 1 1 2
Tyendinaga Napanee 3 2 3

12
Unique Populations
Certain populations within the South East LHIN
have different health needs or require different
approaches to service provision. The Francophone
and Indigenous populations are two such groups
that the South East LHIN works with to ensure
optimal health outcomes and equitable access to
services.
Currently, there are no comprehensive, routine
sources of information on the health and health
system utilization of the Francophone and
Indigenous populations in the South East LHIN.
Routine collection of population health and
service utilization information for these
populations is required in order to better plan for
the health service needs of these groups.
Information in this section was obtained from the
Statistics Canada 2011 Census and National Household
Survey (NHS). See the previous section for additional
data notes and limitations.
FRANCOPHONE POPULATI ON
Demographic Characteristics
• According to the 2011 Census, 3.0% of the South
East LHIN population (or about 14,100 people)
were Francophones, based on the inclusive
definition of the Francophone population (IDF)
adopted by the Ontario government in 2009. This
definition typically results in higher estimates of
the Francophone population compared to the
French as mother tongue definition as it also
includes “those whose mother tongue is neither
French nor English but have a particular
knowledge of French as an Official Language and
use French at home”. The impact of the change of
definition in the South East LHIN is minimal
(~0.1%) compared to the province overall as the
additional inclusion criterion is typically
associated with immigrants to Canada, of which
the South East LHIN has a relatively low
proportion.
• Additional information on the population
reporting French as their mother tongue can be
found in the Socio-Demographic Characteristics
section of this document.
Health Status and Health Service
Utilization
• The Champlain and South East LHINs have
identified a need for data on Francophone’s
utilization of health services and health status in
order to plan, fund, and integrate health services
in accordance with the needs of the Francophone
populations in their geographies. A pilot project is
underway which will examine the feasibility of
collecting information about a patient’s linguistic
profile at the time of registration with hospitals.
In addition, it will examine the feasibility of
making this information available to the LHINs in
a format that is useful for planning purposes. The
planned completion date for this project is end of
fiscal year 16/17.
Community Engagement
• As part of the Health Care Tomorrow initiative, a
project championed by the South East LHIN that
aims to redefine the health care system across
our region, a web-based community engagement
survey was used to collect information on health
system priorities, as well as opinions on what
currently works well or does not work well in the
health system. As part of this survey, respondents
were asked to identify their mother tongue.
Responses from those who identified French as
their mother tongue were analyzed to understand
the priorities and needs identified by the
Francophone population.

13
• Generally, responses from Francophones
mirrored those of non-Francophones in terms of
health system priorities, importance of select
services, concerns about services being moved
from a community, and issues with seeking
specialist treatment.
• Three key themes emerged from the feedback
from Francophone respondents:
o Communication: Need for clinical staff who
can communicate in French (or availability of
an interpreter), coordination between
different levels of care, and increased respect
for patients who do not understand English
o Access: Need for reduction of wait times for
select services, availability of local service,
and a listing of French speaking health service
providers.
o Quality of care: Shifting care to the
community, use of multidisciplinary teams,
and holistic approaches to care.
INDIGENOUS POPULATION
Demographic Characteristics
• We have used the term Indigenous as an inclusive
term to describe individuals and collectives who
consider themselves as being related to and/or
having historical continuity with “First Peoples”.
By using this term, individuals and communities
will be supported in self-defining what it means to
them. However, NHS data presented below uses
other terms as it reflects how questions are asked
of respondents.
• About 3.9% of the South East LHIN population
reported an Aboriginal identity in 2011 compared
to 2.4% for Ontario as a whole, with larger
populations in certain areas of the LHIN (e.g., the
municipalities of Tyendinaga Mohawk Territory,
Tudor and Cashel, Limerick, and Bancroft). In the
South East LHIN, 2.6% of the population identified
as a First Nations person, 1.0% as Métis, and 0.2%
as having multiple and/or other Aboriginal
identities.
• Due to suppression of NHS data in certain areas of
the LHIN (e.g., Deseronto and Wollaston) and
other challenges associated with the collection of
Aboriginal population data, the LHIN estimate of
the population with an Aboriginal identity is likely
an underestimate of the true value. These
limitations surrounding current data on
Indigenous populations have been recognized at
the provincial level and avenues to enhance our
understanding of these populations are being
explored.
• Despite the likely undercounting of those with an
Aboriginal identity, the proportion of the
population reporting an Aboriginal identity has
increased since 1996, both locally and provincially
(both were 1.3% in 1996). Statistics Canada has
noted that in addition to natural increases (e.g.,
births and migration), the increase in the
population reporting an Aboriginal identity is
likely in part due to ethnic mobility (i.e., changes
in self-reporting of cultural affiliation).
Health Status and Health Service
Utilization
• In terms of available information on the health
status of the Indigenous population in the South
East LHIN, a previous provincial survey of the
Métis population identified issues in the South
East LHIN regarding the health status, as well as
the service utilization and access, of this
population group. A summary of this information
can be found in the previous ReCAP report.
• The South East LHIN will continue to work with
the different Indigenous groups across the region
to better understand their population health
status and health care needs.

14
Mohawks of the Bay of Quinte
• The Mohawks of the Bay of Quinte First Nation is
one Indigenous group within the South East LHIN.
As of February 2015, the registered population
with the Mohawks of the Bay of Quinte was
8,099, of whom 24% live on the Tyendinaga
Mohawk Territory reserve. The Mohawks of the
Bay of Quinte population is generally younger
than the overall South East LHIN population,
particularly those living on reserve.
• The Community Wellbeing group of the Mohawks
of the Bay of Quinte delivers health and social
services using a unique approach to holistic
services to help meet the emotional, intellectual,
physical, and spiritual needs of the community.
Health programs delivered by this group include
home support, community health, home and
community care, and diabetes education.
• Health priorities identified by the Mohawks of the
Bay of Quinte include:
o Addictions and Aftercare
o Mental Health
o Heart Disease
o Fetal Alcohol Spectrum Disorders
o Assisted Living
o Cancer Screening and Care
o Diabetes
o Chronic Disease Management and Prevention

15
HEALTH BEHAVIOURS,
HEALTH STATUS, AND
CHRONIC DISEASE
Health Behaviours
Unhealthy behaviours can lead to the
development of various health issues, which in
turn decrease quality of life and increase health
system utilization. An understanding of the
current state of these behaviours in the South
East LHIN can inform planning for future care
needs of the population, as well as identify needs
related to health promotion activities completed
by partner sectors such as public health.
Information on health behaviours is captured through
the Canadian Community Health Survey. Information is
collected from the population 12 years of age and over
for two-year calendar periods as of 2007-08. Prior to
2007, the CCHS collected data every two years over a
12-month period. Further information on the CCHS and
definitions and data notes for these indicators can be
found here.
POOR DIET
Low consumption of fruits and vegetables is
associated with an increased risk of
cardiovascular disease, stroke, functional declines
associated with aging, and possible increased risk
of certain types of cancer.
• The majority (60.0%, 95% Confidence Interval (CI)
57.2%-62.9%) of the population in the South East
LHIN reported consuming fruits and vegetables
fewer than five times per day in calendar years
2013-14 (Figure 5). This rate has increased since
2005 and was similar to the 2013-14 provincial
rate of 61.2% (95% CI 60.3%-62.1%). Rates were
significantly higher in males compared to females
and were similar across all age groups. Rates in
those aged 65+ have significantly increased since
2005, with nearly a 20% difference. By region,
rates have increased in the Leeds, Grenville and
Lanark District and Hasting Prince Edward Public
Health Units.
PHYSICAL INACTIVITY
Physical activity reduces the risk of premature
morbidity and mortality, particularly in relation to
cardiovascular disease, hypertension, cancer, and
osteoporosis. It is also associated with positive
mental health and is an important risk factor for
overweight and obesity.
• In 2013-14, nearly half (45.6%, 95% CI 42.5%-
48.8%) of the population in the South East LHIN
were classified as inactive in their leisure time
(Figure 5). Rates of physical inactivity in the South
East LHIN declined between 2001 and 11/12 but
appear to have increased in 2013-14, bringing the
South East LHIN rate closer to the provincial rate
(46.3%, 95% CI 45.4%-47.3%).
Figure 5: Self-reported prevalence of various health behaviors, South East LHIN and Ontario, calendar years 2013-2014.

16
• Rates of physical inactivity increased with
increasing age and were similar for both sexes, as
well as across the three South East LHIN public
health units in 2013-14.
DAILY SMOKERS
Smoking tobacco is the most important
preventable cause of lung cancer. It can also
contribute to the development of leukemia and
cancers of the bladder, stomach, kidney,
pancreas, and cervix. It is also associated with
Chronic Obstructive Pulmonary Disorder (COPD)
and cardiovascular diseases.
• About one in five (19.5%, 95% CI 16.6% - 22.3%)
South East LHIN residents report being daily
smokers, which was significantly higher than
provincial levels in 2013-14 (13.1%, 95% CI 12.5%-
13.6%) (Figure 5). While rates for the province
have steadily declined over time, rates in the
South East LHIN have not changed significantly
over the past ten years.
• Rates were highest in the 18-44 and 45-64 year
age groups. While not significantly different, rates
appear to be higher for males and in the western
and eastern part of the LHIN.
HEAVY ALCOHOL CONSUM PTION
Health problems associated with heavy alcohol
consumption over time include diseases of the
liver, pancreas, and nervous system, as well as
certain cancers (e.g., upper respiratory system,
digestive system, and breast).
• About one in five (18.6%, 95% CI 16%-21.1%)
South East LHIN residents were classified as heavy
drinkers in 2013-14 (Figure 5). This rate was not
significantly higher than the provincial rate of
16.6% (95% CI 15.9%-17.2%). Rates in both areas
have remained relatively consistent over the past
ten years.
• In South East LHIN, rates of heavy alcohol
consumption were higher for males and among
those 18-44 years of age. Rates were similar
across the three South East LHIN public health
unit regions.
INFLUENZA VACCINATION
Influenza vaccination can prevent infection and
reduce the morbidity, mortality, and health
system utilization associated with this illness,
particularly in vulnerable populations such as the
elderly.
• In 2013-14, only 41.7% of South East LHIN
residents reported receiving an influenza
vaccination within the last year. This rate has
remained relatively constant over time and has
remained consistently higher than the provincial
rate (which was 33.5% in 2013-14). Rates were
significantly higher for females, as well as higher
in the 46-64 and 65+ year age groups. In 2013-14,
about four in five South East LHIN residents aged
65+ reported receiving an influenza vaccination
within the last year. Rates were relatively
constant across the three public health unit
regions in the South East LHIN.
• About three-quarters (74.0%, 95% CI 71.1%-
76.8%) of the South East LHIN population
reported ever receiving an influenza vaccine as of
2013-14. Again, this was higher than the
provincial rate of 64.1%. Rates have increased
over time for both sexes, all age groups, and in
the three public health unit regions within the
LHIN.
• Of note, nearly all (90.6%) of those aged 65+
reported ever receiving an influenza vaccination.

17
Health Status and Chronic Conditions
Information on the health status and chronic conditions
of the South East LHIN population is captured through
the Canadian Community Health Survey (see the
previous section for additional information about the
survey). For chronic conditions, people aged 12 and
over are asked to self-report if they have one of these
“long-term conditions” that are expected to last or
have already lasted 6 months or more, and that have
been diagnosed by a health professional. The chronic
disease indicators are presented in order of descending
prevalence.
Note that diabetes prevalence is determined using a
validated algorithm that incorporates data from
various administrative sources (see the MOHLTC Key
Performance Measures for the Ontario Diabetes
Strategy report for details). Also, the incidence of
various types of cancers was obtained from the Ontario
Cancer Registry (2012 for SEER*Stat Release 9 Nov.
2012, Cancer Care Ontario).
HEALTH STATUS
Self-Perceived Health
This indicator can serve as a proxy of general
health in the population; health means not only
the absence of disease or injury but also physical,
mental, and social wellbeing.
• About three-fifths of the South East LHIN
population (59.8%, 95% Confidence Interval (CI)
56.7%-63%) reported that their health was very
good/excellent in calendar years 2013-14. This
was similar to the provincial rate of 59.5% (95% CI
58.7%-60.4%). However, about one in ten South
East LHIN residents (13.5%, 95% CI 11.5%-15.6%)
reported that their health was fair/poor. Rates for
both indicators have been relatively consistent
over time for the South East LHIN and Ontario.
• Rates of reported very good/excellent health and
fair/poor health were similar between the sexes.
• With increasing age, a lower proportion of the
population reported very good/excellent health
and a higher proportion reported fair/poor
health. While rates over time were fairly stable
within most age groups, it appears that the
proportion of those aged 65+ reporting fair/poor
health has decreased over time. Differences in
rates over time were significant for the province
overall but not for the South East LHIN. In 2013-
14, 23.2% (95% CI 19.2%-27.2%) of those aged
65+ reported fair/poor health, compared to
28.0% (95% CI 23.3%-32.8%) in 2001. Similarly,
the proportion of those aged 65+ reporting very
good/excellent health has increased over time.
• For both indicators, rates were generally more
favorable in the Kingston, Frontenac and Lennox
& Addington Health Unit compared to the other
South East LHIN regions.
Self-Perceived Mental Health
Perceived mental health is a general indication of
the number of people in the population suffering
from some form of mental disorder, mental or
emotional problems, or distress, and is not
necessarily reflected in self-perceived health.
• In 2013-14, 69.2% (95% CI 66.3%-72.1%) of the
South East LHIN population reported that their
mental health status was very good/excellent.
This was similar to the provincial rate of 70.6%
(95% CI 69.8%-71.5%). Rates in both areas have
declined over time (from 73.9% (95% CI 71.8%-
76.1%) in the South East LHIN in 2003). While a
much lower rate overall, it appears that the
proportion of the population reporting that they
have fair/poor mental health has increased
slightly over time. In the South East LHIN, rates
increased from 4.8% (95% CI 3.8%-5.7%) in 2005
to 8.4% (95% CI 6.7%-10%) in 2013-14.

18
• While high variability in the rates for South East
LHIN impair comparisons between sub-groups,
provincially, rates of fair/poor self-perceived
mental health were higher in females and those
45-64 years of age.
• Rates of very good/excellent self-perceived
mental health were relatively consistent over
time in all South East LHIN regions except for the
Hastings Prince Edward Public Health Unit, where
rates appear to have decreased in the last 10
years (from 74.3% (95% CI 70.6%-77.9%) in 2003
to 64.1% (95% CI 58.8%-69.4%) in 2013-14).
Self-Perceived Life Stress
The emotions produced by stress can modify
immune response and influence the onset and
progression of physical illness; stress may also
trigger negative changes in health behaviours as
individuals try to cope.
• About a quarter of the South East LHIN
population (24.0%, 95% CI 20.8%-27.2%) reported
that most days in their life were quite a bit or
extremely stressful in 2013-14. This rate has
remained relatively consistent over the last eight
years and was similar to the provincial rate of
22.7% (95% CI 21.8%-23.5%).
• Females and adults aged 15-64 generally reported
experiencing higher stress levels compared to
other groups. Rates were similar across the three
South East LHIN public health unit regions.
Obesity
Health problems associated with obesity can
include type 2 diabetes, dyslipidemia,
hypertension, coronary heart disease, gallbladder
disease, obstructive sleep apnea, and certain
cancers.
• A quarter of the adult population in the South
East LHIN (25.7%, 95% CI 22.9%-28.6%) was
classified as obese in 2013-14. This rate has
steadily increased over time and was significantly
higher than the provincial rate of 19.2% (95% CI
18.5%-19.9%) in 2013-14. The difference between
the South East LHIN and Ontario rates has been
increasing in recent years.
• Rates in 2013-14 were similar between males and
females. Provincially, rates were highest for those
45-64 years of age. This difference between age
groups appears to be consistent for the South
East LHIN; however, rates by age group were not
significantly different.
• Across the South East LHIN, rates have increased
between 2005 and 2013 for Kingston, Frontenac
and Lennox & Addington Public Health Unit and
Leeds, Grenville and Lanark District Health Unit,
while remaining constant for the Hastings Prince
Edward Public Health Unit.
CHRONIC CONDITIONS
Defined broadly as "illnesses that are prolonged,
do not resolve spontaneously, and are rarely
cured completely”, chronic diseases account for a
substantial burden of illness due to their
associated morbidity and mortality.
Arthritis
• A quarter of the South East LHIN population
(24.3%, 95% CI 22%-26.5%) reported having
arthritis in calendar years 2013-14 (Figure 6).
Arthritis prevalence rates have continued to be
significantly higher in the South East LHIN
compared to the province overall (17.9%, 95% CI
17.3%-18.5%), even after standardizing rates by
age. Rates have remained relatively constant over
time.
• Within the South East LHIN, arthritis appears to
be more common among females (although not
significantly higher than males in 2013-14 due to

19
high variability in rates) and with increasing age.
About half of the population aged 65+ reported
having arthritis, compared to about 30% of those
aged 45-64 and less than 10% of those aged 15-44
years of age.
• Across the South East LHIN, rates were highest in
the Leeds, Grenville and Lanark District Health
Unit (27.0% in 2013-14, 95% CI 23.1%-30.8%),
which is in part due to the relatively older
population in this region.
High Blood Pressure
• Nearly a quarter (22.8%, 95% CI 20.7%-25%) of
the population in the South East LHIN reported
having high blood pressure in 2013-14. Rates have
steadily increased over the last 10 years, both
within the South East LHIN and in the province
overall. The 2013-14 South East LHIN rate was
significantly higher than the provincial rate of
18.5% (95% CI 17.9%-19.1%). Part of this
difference in rates can be attributed to the older
population within the South East LHIN, as rates
between the two areas were more similar after
adjusting for age.
• Rates of high blood pressure were similar
between males and females, and increased
significantly with age. Nearly thirty percent
(28.2%, 95% CI 23.3%-33.1%) of the population
aged 45-64 years and nearly half (46.8%, 95% CI
43.1%-50.5%) of the population aged 65+
reported having high blood pressure in 2013-14.
• Across the South East LHIN, rates were highest in
the Hastings Prince Edward Public Health Unit
(24.0%, 95% CI 20.7%-27.3%) and the Leeds,
Grenville and Lanark District Health Unit (24.6%,
95% CI 21%-28.3%).
Mood Disorders
Includes conditions such as depression, bipolar
disorder, mania or dysthymia.
• The prevalence of mood disorders in the South
East LHIN has steadily increased over the last ten
years, from 6.8% (95% CI 5.6%-7.9%) in 2003 to
13.2% (95% CI 11%-15.4%) in 2013-14. Rates for
Ontario have also increased but not as much as
the South East LHIN rate. While rates between
the two areas were similar in 2003, the South East
LHIN rate in 2013-14 was significantly higher than
the provincial rate of 8.5% (95% CI 8%-9%).
• Rates were significantly higher in females
compared to males (15.9% (95% CI 12.6%-19.1%)
versus 10.3% (95% CI 9.6%-11%), respectively). By
age, rates were highest in those between 18 and
64 years of age. Rates appear to be increasing for
both sexes, all age groups, and in all regions of
the South East LHIN.
Figure 6: Self-reported prevalence of various chronic conditions, South East LHIN and Ontario, calendar years 2013-2014.
Notes: Data with asterisk: Interpret estimate with caution due to high sampling variability. Diabetes prevalence is as of April 2013.

20
Anxiety Disorders
Includes anxiety disorders such as phobias, obsessive-
compulsive disorder, or a panic disorder.
• In both the South East LHIN and Ontario, rates of
anxiety disorders have increased over time. In
2013-14, about one in ten (11.0% (95% CI 9.1%-
13%) South East LHIN residents reported having
been diagnosed with an anxiety disorder. This
rate was significantly higher than the provincial
rate of 7.6% (95% CI 7.1%-8.1%). Rates in 2013-14
were similar across the South East LHIN region.
• While not significantly different for the South East
LHIN, as is the case for Ontario, rates of anxiety
disorders appeared higher for females compared
to males. While high variability in the rates for the
South East LHIN impair comparison between age
groups, provincially, rates appeared lowest in the
65+ age group.
Diabetes
• The prevalence of diabetes (types 1 and 2) in the
South East LHIN was 12.4% among those 18+
years of age as of April 2013. This was similar to
the provincial rate of 11.9% and has increased
slightly over time, from 10.6% in April 2009.
• The prevalence of diabetes increased with
increasing age, ranging from 3.8% in those 18-49
years of age to 29.9% in those 80+ years. The
prevalence within each age group has increased
over time, with minimal increases in those under
60 years of age (<1% difference in rates compared
to April 2009) and greater increases in the 60-69
(2.1%), 70-79 (3.0%), and 80+ (5.2%) year age
groups.
• The prevalence of diabetes ranged across the
South East LHIN region, from 6.9% of the
population aged 18+ in the Rideau Lakes SubLHIN
area (as of April 2012) to 15.7% in the North
Hastings SubLHIN.
Asthma
• About one in ten (9.8%, 95% CI 8%-11.6%) South
East LHIN residents reported having asthma in
2013-14. This rate continues to be significantly
higher than the provincial rate of 7.6% (95% CI
7.2%-8%).
• Rates have remained relatively consistent over
time and appeared to be higher for females and
for younger age groups (although differences
were not statistically significant for the South East
LHIN).
Heart Disease
• In the South East LHIN, 6.4% (95% CI 5.4%-7.4%)
of the population in 2013-14 reported having
been diagnosed with heart disease. This rate has
declined slightly over the past decade, and while
not significantly different, the South East LHIN
rate appears higher than the provincial rate of
4.9% (95% CI 4.6%-5.3%). However, after
adjusting the rate for age, there was little
difference between the South East LHIN and
provincial rates.
• While not significantly different, rates of heart
disease appeared higher among South East LHIN
males (7.3%, 95% CI 5.9%-8.7%) compared to
females (4.0%, 95% CI 3.6%-4.4%).
• Rates of heart disease were significantly higher in
older age groups. One-fifth (20.1%, 95% CI 16.7%-
23.5%) of South East LHIN residents 65+ years of
age reported having heart disease.
• Across the South East LHIN, rates of heart disease
were highest in the Hastings Prince Edward Public
Health Unit (8.1%, 95% CI 6.3%-9.8%) and lowest
in the Kingston Frontenac and Lennox &
Addington Public Health Unit (4.7%, 95% CI 3%-
6.4%).

21
Chronic Obstructive Pulmonary Disease
(COPD)
• In 2013-14, the rate of COPD in the South East
LHIN (6.4%, 95% CI 4.9%-7.9%) was significantly
higher than the provincial rate (4.0%, 95% CI
3.6%-4.3%). This difference remained significantly
higher even after accounting for the older
population in the South East LHIN using age
standardization.
• Provincially, rates of COPD were higher for
females, as well as with increasing age. A similar
trend was observed for the South East LHIN;
however, these differences were not significant
due to high variability in the rates.
• Rates in the Hastings Prince Edward Public Health
Unit (8.2%, 95% CI 6%-10.4%) were significantly
higher than the provincial rate in 2013-14.
Cancer
The incidence of cancer in a region can be
influenced by a variety of factors including
prevalence of risk and protective factors, uptake
of cancer screening, and population composition
in the region (such as proportion of immigrants in
a region).
• In 2009, there were 3,031 new cases of cancer
diagnosed in the South East LHIN; 1,532 of those
diagnosed were male and 1,499 were female. The
most common types of cancers in males were
prostate (21% of all male cancer diagnoses), lung
(17%), and colon and rectum (14%). All other
types each accounted for less than 5% of
diagnoses. For females, breast (26%), lung (12%),
and colon and rectum (12%) were the most
common cancer diagnoses, with all other causes
each accounting for 6% or less.
• The 2009 age-standardized incidence rate for all
cancers in males was similar between the South
East LHIN and the province as a whole (445.3
cases per 100,000 population for the South East
LHIN), with notably lower rates of prostate cancer
in the South East LHIN (90.1 versus 122.6
provincially) and higher rates of lung cancer (74.5
versus 58.2 provincially).
• For females, the 2009 age-standardized incidence
rate for all cancers was highest in the South East
LHIN compared to all other LHINS (400.0 cases per
100,000 population for the South East LHIN
compared to 373.0 provincially). South East LHIN
rates were also higher for the three most
common types of cancers in females.
Intestinal or Stomach Ulcers
• A relatively low proportion of the South East LHIN
population (2.8%, 95% CI 1.7%-3.9%) reported
having intestinal and stomach ulcers as of 2013-
14. Rates were similar to the province overall and
have remained relatively consistent over time in
both areas.
Stroke
• Just under 2% (1.6%, 95% CI 1.1%-2.1%) of the
South East LHIN population reported suffering
from the effects of a stroke in 2013-14. This crude
rate appeared higher than the provincial rate of
1.2% (95% CI 1%-1.3%); however, this difference
is in part due to higher prevalence in older age
groups and the older age structure of the South
East LHIN population, as the rates were more
similar after adjusting for age.

22
HOSPITALIZATIONS FOR CHRONIC CONDITIONS
Information was obtained from the Canadian Institute
for Health information’s (CIHI) Discharge Abstract
Database (DAD). Hospitalizations for chronic
conditions were identified based on the most
responsible diagnosis noted on the hospitalization
record.
• Hospitalizations due to chronic conditions
account for a sizable proportion of acute inpatient
hospital use in the South East LHIN. In fiscal year
2013/14, there were about 11,300
hospitalizations due to chronic conditions
(including arthritis & related conditions, asthma,
cancer, CHF, COPD, diabetes, hypertension,
ischemic heart disease (IHD), and stroke), which
accounted for a quarter of all hospitalizations in
the South East LHIN and about 27% of all hospital
days. The conditions accounting for the highest
number of hospitalizations and hospital days were
arthritis and related conditions, cancer, and IHD.
• Compared to other LHINs, the South East LHIN
had the second-highest proportion of
hospitalizations and hospital days for chronic
conditions, which could be due in part to the
older population in the South East LHIN and the
higher prevalence of chronic conditions. In
particular, the South East LHIN had relatively high
hospitalization and hospital day rates per capita
for arthritis and related conditions, cancer, COPD,
and IHD.
HEALTH STATUS AND CHRONIC CONDITIONS IN THE 65+ POPULATION
• As previously highlighted, the prevalence of
chronic conditions generally increases with
increasing age in the South East LHIN, with the
exception of mood disorders, anxiety disorders,
and asthma, which all have slightly lower
prevalence in those 45-64 and 65+ years of age
compared to those 18-44 years of age (Figure 7).
• With increasing age, South East LHIN residents
were more likely to report fair/poor self-
perceived health and less likely to report very
good/excellent health. In terms of self-perceived
mental health, there is less of a difference by age
Figure 7: Self-reported prevalence of various chronic conditions in the 65+ population, South East LHIN and Ontario, calendar years 2013-2014.
Notes: Data with asterisk: Interpret estimate with caution due to high sampling variability.

23
group in those reporting very good/excellent
mental health. Those aged 65+ also reported
significantly lower levels of self-perceived life
stress compared to younger age groups.
• Older adults in the South East LHIN often
reported being limited in certain activities
because of a physical condition, mental condition,
or health problem which has lasted or is expected
to last 6 months or longer. In calendar years
2013-14, just under a half of those aged 45-64
reported sometimes or often having an activity
limitation and just over half of those aged 65+
reported the same. The rate in those aged 45-64
was significantly higher than the provincial rate
(36.4%, 95% CI 34.8%-37.9%).
• A sizeable proportion of the older adult
population in the South East LHIN were classified
as having moderate to poor functional health
based on measures from eight dimensions of
functioning (vision, hearing, speech, mobility,
dexterity, feelings, cognition and pain). In 2013-
14, about a quarter of those aged 45-64 were
noted to have moderate to poor functional health
and about 35% of those aged 65+ were classified
as such. These rates were similar to the provincial
rate.
• Given the aging population in the South East
LHIN, there will be a larger number of people
living with chronic conditions and limitations
resulting from these conditions in the coming
years if all factors related to disease risk,
diagnosis, and survival remain constant. However,
increasing rates of certain risk factors for chronic
disease (e.g., obesity or heavy drinking) in those
under 65 years of age may entail that a greater
proportion of the population will be developing
chronic conditions, resulting in higher disease
prevalence for those over age 65 in the coming
years.

24
BIRTHS AND DEATHS
Births and Maternal Health
Understanding trends in births and maternal
health is important for planning obstetrical
services in the South East LHIN, as well as planning
for other community and hospital services that
support healthy pregnancies.
Vital Statistics information on births was obtained from
the Office of the Registrar General (ORG),
ServiceOntario via the Ministry of Health and Long-
Term Care’s IntelliHEALTH system. Information on
maternal health and some of the obstetric indicators
were obtained from various reports from Better
Outcomes Registry & Network (BORN) Ontario.
BIRTHS AND FERTILITY RATES
• In 2011, there were about 2,400 births in the
South East LHIN, a rate of 8.6 births per 1,000
population. This is the lowest rate out of all the
LHINs, which is in part due to the older population
distribution in the LHIN and, in turn, the lower
proportion of females within childbearing age.
The number of births has remained relatively
constant over the last 10 years. The highest
number of births in 2011 were in the Kingston
(1,386) and Quinte (1,162) Health Links. All other
Health Links had less than 520 births in that year.
• Among females 15-49 years of age, the fertility
rate in the South East LHIN has increased over the
last 10 years, as it has for the province as a whole.
While the fertility rate in the South East LHIN was
more similar to the other LHINs compared to the
crude birth rate, the rate in 2011 (39.5 births per
1,000 females aged 15-49) was still the lowest of
all the LHINs.
• Within the South East LHIN, total fertility rates
have generally increased in all Health Links except
Thousand Islands. The highest rates in 2011 were
in Salmon River, Rural Hastings, and Rideau Tay
(all above 41.5 births per 1,000 females aged 15-
49).
• In the South East LHIN, fertility rates were highest
in the 25-29 year age group (100.9 births per
1,000 females), followed by the 30-34 and 20-24
year age groups (91.7 and 52.5 births per 1,000
females, respectively). Fertility rates appear to be
higher for the younger age groups in the South
East LHIN compared to the province as a whole.
Rates in the South East LHIN have increased over
time for those above 30 years of age and have
either remained the same or have declined
slightly for the younger age groups. Birth rates for
teenagers in the South East LHIN continue to be
higher than the provincial rate.
• Within the South East LHIN, fertility rates in those
under 25 years of age were highest in the Rural
Hastings, Quinte, and Salmon River Health Links;
rates for those above 35 were highest in the
Kingston Health Link.
• If current fertility rates remain constant, the
number of births in the South East LHIN is
projected to remain relatively unchanged by 2026
due to the projected stability in the size of the
population in childbearing age. By Health Link, the
number of births is projected to decrease in all
areas except for the Kingston Health Link, which is
expected to see a small increase in the number of
births (about 150 extra births or a 10% increase
from 2010).
BIRTH OUTCOMES
• Similar to the province overall, rates of low birth
weight births in the South East LHIN have
increased over time (to 6.5% of births in 2011 for
both South East LHIN and Ontario), while rates of

25
high birth weight births have decreased (to 2.3%
in South East LHIN compared to 1.6% in Ontario).
Low birth weight rates were particularly high in
the Salmon River (8.9%), Rural Hastings (7.5%),
and Quinte (7.7%) Health Links.
• The preterm birth rate has varied in the South
East LHIN over the past 10 years and was similar
to the provincial rate in 2011 (7.8% of all live
births in the South East LHIN compared to 7.7%
for the province). Rates by Health Link also varied
considerably over time, with rates generally
increasing in all areas except the Kingston and
Rideau-Tay Health Links. Preterm birth rates were
highest in the Rural Hastings Health Link (10.0% of
all births).
• The multiple birth rate has varied in the South
East LHIN over the past 10 years and was lower
than the provincial rate in 2011 (2.9% of all live
births in the South East LHIN compared to 3.6%
for the province). This difference in rates may be
due to the increased incidence of multiple births
with increasing age, as the provincial fertility rates
are higher for older age groups compared to the
South East LHIN. Variation in multiple birth rates
over time by Health Link is high due to the low
number of multiple births in each area.
• The rate of Caesarean deliveries in the South East
LHIN in 2011/12 (27.5% of births) was similar to
the provincial average (28.4%).
MATERNAL HEALTH
• In terms of maternal health behaviors during
pregnancy, the South East LHIN has markedly
higher rates of smoking at the time of delivery
(18.4% versus 8.5% provincially); however,
smoking rates did decrease by 2.7% between the
first prenatal visit and the time of birth.
• The South East LHIN also had higher rates of
maternal drug and substance use (3.8% versus
2.0% provincially), as well as alcohol use (2.3%
versus 1.6% provincially) in fiscal year 2013/14.
• Rates of exclusive breastfeeding on discharge
from hospital have increased over time for South
East LHIN mothers (from 56.4% in 2009/10 to
61.1% in 2011/12), with the 2011/12 rate slightly
lower than the provincial rate of 63.2%.
• Similar to the province as a whole, most hospital
births in the South East LHIN in 2011/12 were
attended by an obstetrician (82.9%), followed by
family physicians (12.3%), and midwives (3.1%).
The percentage of hospital births attended by
midwives was the second lowest of all the LHINs.
The percent of South East LHIN obstetric patients
readmitted to hospital within 30 days of discharge
has decreased slightly over time and was similar
to the provincial rate in 2013/14 (1.6% in South
East LHIN versus 1.8% provincially).
Deaths
This analysis was based on Vital Statistics data
obtained from the Office of the Registrar General
(ORG), ServiceOntario via the MOHLTC IntelliHEALTH
system. Information on setting of death was compiled
by MOHLTC using data from several administrative
sources (see details here).
OVERALL MORTALITY TRENDS
• In 2010, there were about 4,750 deaths in the
South East LHIN, a rate of 970 deaths per 100,000
population. This is the highest rate out of all the
LHINs, which is in part due to the older population
distribution in the LHIN. The South East LHIN also
had the highest mortality rate out of all LHINs for
the population aged 65+.
• Within the South East LHIN, the highest number
of deaths in 2010 were in the Quinte (1,260),

26
Kingston (1,229), and Thousand Islands (741)
Health Links (Figure 8). Crude mortality rates
were highest in Salmon River (1,103 deaths per
100,000 population) and lowest in Rural Kingston
(742 deaths per 100,000 population). By age
group, the highest mortality rates for the 1-19
and 20-44 year age groups were in Rural Hastings,
while the highest rates for the older age groups
(65-74, 75-84, 85+) were in the Salmon River,
Quinte, and Thousand Islands Health Links.
• If the status quo remains (i.e., no changes in age-
specific mortality rates), the number of deaths
occurring in the South East LHIN is projected to
increase by just over 40% between 2014 and 2026
as the population in the region ages (Figure 8).
This would result in approximately 2,200
additional deaths among South East LHIN
residents. An increase in the number of deaths is
projected for all Health Links, with all areas having
at least a 35% increase in the number of deaths
over this time period.
• Overall life expectancy in the region is 79.6 years
(3rd lowest in province) and 19.0 years for those
aged 65 (2nd lowest in the province) based on
mortality data from 2007 to 2009. Similar to the
province overall, life expectancy for females in
the South East LHIN is higher than for males (82.0
years versus 77.1, respectively). While life
expectancy is a traditional measure for
understanding population health, it is also
important to consider disease burden and quality
of life as the population reaches end of life.
• By sex, males had a higher proportion of deaths
under 75 years of age in 2010 (44.5% of deaths
for males versus 29.9% for females). Deaths
occurring in those younger than 75 years are
considered premature. Premature deaths
accounted for 27,275 years of potential life lost
(PYLL) for LHIN residents in 2010.
• The PYLL rate was 6,080 per 100,000 population
aged less than 75 years for South East LHIN
residents, which was greater than the PYLL rate
for Ontario residents (4,532). Although the South
East LHIN PYLL rate has decreased over time, it is
the third highest rate among the LHINs. Within
the South East LHIN, the PYLL rate was highest in
Rural Hastings (7,144) and lowest in Kingston
(5,390). All Health Link-specific rates were higher
than the provincial rate.
CAUSES OF DEATH
• The leading causes of death for residents in the
South East LHIN between 2010 and 2011 were
ischaemic heart disease, cancer of lung and
bronchus, dementia/Alzheimer’s disease,
cerebrovascular diseases, and chronic lower
respiratory diseases. These causes accounted for
42.2% of all deaths in the South East LHIN. The
South East LHIN had higher mortality rates for
these leading causes of death compared to
provincial rates, which is in part due to the older
age distribution in the LHIN. The top leading
causes of death were similar across the South
East LHIN Health Links.
Figure 8: Actual and projected number of deaths by Health Link and calendar year, calendar years 2010 to 2026.
Notes: Crude projections are based on 5-year age- and sex-specific mortality rates in calendar years 2009 and 2010 and projected population growth. These crude projections assume that mortality rates by age group remain constant in the projected time period. Projected values rounded to nearest hundred.

27
• Looking at the overall lead cause of death groups,
over half of all deaths in the South East LHIN
between 2010 and 2011 fell under the malignant
neoplasms (28% of deaths) and circulatory system
(27% of deaths) groups (Figure 9). Deaths related
to the respiratory system (9%), nervous system
(9%), injuries (5%), blood forming/endocrine
system (4%), and digestive system (2%) were the
other main cause of death groups. The
distribution of deaths across these lead cause
groups was similar across the Health Links, with
the exception of slightly higher proportions of
malignant neoplasm deaths in Rural Kingston
(31% of deaths) and circulatory system-related
deaths in Thousand Islands (31%).
• By age group, deaths for most cancers, cirrhosis
and other liver diseases, unintentional injuries,
and intentional self-harm were more common
among those under 75 years of age.
SETTING OF DEATH
• In fiscal year 2012/13, deaths among South East
LHIN residents occurred most often in acute care
settings (41% of deaths), followed by private
homes and select residential settings (such as
hospices and retirement homes, 23%),
long-term care facilities (21%), complex
continuing care facilities (9%), and
emergency departments (6%) (Figure 10).
This distribution of death settings was
similar to the province as a whole.
• An increasing proportion of deaths in our
region are occurring in private homes, with
fewer occurring in hospital-based settings
(including acute care, complex continuing
care, and emergency departments) (Figure
10). The proportion of deaths occurring at
home has increased from 19% in 2010/11
to 23% in 2012/13. This proportion also
increased provincially over the same time
period (from 22% to 24%). The proportion
of deaths in hospital settings have decreased
from 60% in 2008/09 to 56% in 2012/13.
• If the current proportion of people dying at home
remains constant, there will be a need to provide
in-home palliative and end of life care for an
estimated 500 additional people by 2026
compared to 2014 - a 41% increase.
• Planning for services must consider patient choice
regarding setting of death along with evidence-
based guidelines and models of care.
Figure 9: Distribution of deaths by lead cause of death, South East LHIN residents, calendar years 2010 and 2011.
Figure 10: Number of deaths by setting of death and fiscal year, South East LHIN, fiscal years 2008/09 to 2012/13.
Note: Home with/without support and long-term care deaths grouped in 2008/09 and 2009/10 due to incomplete LTC reporting.

28
COMMUNITY-BASED
SERVICES
Primary Care
Understanding primary care availability and
utilization is important not only for performance
management, planning (including human
resources planning), and accountability of primary
care agencies and organizations currently
associated within the Ministry-LHIN
Accountability Agreement (MLAA) structure, but
also for the purposes of overall health system
planning and understanding population health in
its broadest sense.
TYPES OF PRIMARY CARE PROVIDER MODELS
Patient Enrolment Models
Information on the number of enrolled patients is
based on data from the MOHLTC Client Agency
Program Enrolment Database. Information on the
number of physicians is based on data from
HealthForceOntario and the MOHLTC Corporate
Providers Database (CPDB). Physician locations were
classified based on their reported primary practice
address. This information may not be current in the
above databases, resulting in misclassification of
Name Description
Comprehensive Care
Model (CCM)
Designed for solo physicians. Patient enrolment is strongly encouraged. Have standard office hours
with one additional 3-hour session of extended hours on weekday evenings and/or weekends.
Funding is provided by fee-for-service, plus incentives for services to enrolled patients.
Community
Sponsored
Agreement (CSA)
Physicians are salaried employees of Community or Mixed Governance Family Health Teams. Salary is
based on the number of enrolled patients, plus benefits and bonuses.
Family Health Group
(FHG)
Comprised of three or more physicians practicing together. Patient enrolment is strongly encouraged.
Have standard office hours with 3-5 additional three hour (minimum) sessions of extended hours on
weekday evenings and/or weekends. Office is also staffed with nurses and an after-hours telephone
health advisory service. Funding is provided by fee-for-service, plus incentives for services to enrolled
patients.
Family Health
Network (FHN)
Similar to FHG in terms of number of physicians, nursing staff, after-hours availability, and telephone
health advisory service. Different from FHGs in that FHNs commit to enrolling patients. Funding is
provided through a blended capitation model (e.g. age- and sex-adjusted base rate remuneration plus
incentives).
Family Health
Organization (FHO)
Similar to FHN in terms of number of physicians, nursing staff, after-hours availability, telephone
health advisory service, and funding scheme. FHOs have a larger basket of services included in
capitation compared to FHNs.
Southeastern
Ontario Academic
Medical Organization
(SMO)
A large interdisciplinary organization in the South East comprised of over 300 physicians. Family
physicians that enroll patients are a subset of the organization and are funded through an Alternative
Funding Plan (AFP). While very similar to FHOs in terms of capitation and services offered, the SMO
model offers a salary-based funding to family physicians for academic activities (i.e. teaching and
research).
Table 3: Primary care Patient Enrolment Models (PEMs) in the South East LHIN.

29
practice locations and physician involvement in Family
Health Teams as determined by South East LHIN staff
based on reported primary practice address.
• Patient Enrolment Models (PEMs) are primary
care physician remuneration models that
generally share common features of patient
enrolment (rostering), group practice,
performance-based incentives, and after-hours
care commitments. The types of PEMs in the
South East LHIN are listed in Table 3.
• The majority (81%) of South East LHIN residents
were enrolled in a PEM as of May 2015, with most
enrolled with Family Health Organizations (FHOs).
• Out of a total of 127 locations where PEM
physicians offer services in the South East LHIN,
69% were FHOs, 13% were FHGs, 9% were CCMs,
5% were FHNs, 3% were CSAs, and <1% was SMO
(Figure 11).
• There were 338 physicians in the South East LHIN
practicing in PEMs as of January 2015.
Approximately 73% of the physicians were part of
a FHO, 12% were part of a FHG, 4% were part of
each FHN, SMO, and CCM, and 3% were part of a
CSA (Figure 11).
• While the total number of PEM locations and
physicians varied across the Health Links in the
South East LHIN, each Health Link had more FHO
locations and physicians than any other model
type (Table 4). Kingston Health Link had the
largest number of PEM locations and physicians
overall, as well as the largest variety of models
(including all but CSAs), which is in part due to the
larger population in this area. Information on the
overall number of family physicians per capita can
be found in the Human Resources section of this
document.
Family Health Teams
• Family Health Teams (FHTs, captured under a
number of PEM types) are interdisciplinary
practices of health professionals (e.g., nurses,
physicians, pharmacists, social workers, and
dieticians) that are established based on
community needs and that focus on preventive
Figure 11: Primary Care Patient Enrollment Models (PEM) in the South East LHIN, January 2015.

30
care, health promotion, and chronic disease
management.
• Just over 40% of South East LHIN residents were
enrolled in a FHT at the end of fiscal year
2013/14, the second-highest rate among all the
LHINs. Provincially, about 23% of Ontario
residents were enrolled in a FHT.
• Of the approximately 650 family physicians in
the South East LHIN as of January 2015, 197
(30%) were part of a FHT. The largest
representation of physicians was at Queen’s
FHT, followed by Maple FHT and Upper Canada
FHT (Figure 12).
• Kingston Health Link had the highest number of
physicians working with FHTs in the South East
LHIN as of January 2015, which again is in part
due to the larger population in this area.
Information on the overall number of family
physicians per capita can be found in the Human
Resources section of this document.
Non-Patient Enrolment Models
• Non-PEM primary care models include other
group-based models and solo fee-for-service
physicians
• Types of non-PEM group models include
Community Health Centres (CHCs), Nurse
Practitioner-Led Clinics (NPLCs), midwifery group
practices, and Aboriginal Health Access Centres
(AHACs). These models typically serve a particular
population (e.g., marginalized communities,
healthy pregnant women, and newborns), may
include health promotion and community
development, and may offer comprehensive,
interdisciplinary care (i.e., various types of health
professionals).
• CHCs are the only type of primary care model that
is LHIN-funded. In fiscal year 2014/15, there were
22,556 clients registered at South East LHIN CHCs.
Additional information on client characteristics
and CHC utilization can be found in the CHC
section of this report.
• The distribution of non-PEM family physician
locations is illustrated in Figure 13. There were
150 non-PEM family physician locations in the
South East LHIN as of January 2015.
Approximately 47% were located in Kingston
Health Link, 19% in Quinte Health Link, 11% in
Thousand Islands Health Link, 10% in Rideau-Tay
Health Link, 4% in each Rural Kingston and
Salmon River Health Links, and 1% in Rural
Hastings Health Link.
Table 4: Number of family physicians by Patient Enrolment Model (PEM) type and Health Link, South East LHIN, January 2015.
CCM CSA FHG FHN FHO SMO
Rural Hastings 7 2 1 1 6 14 31
Quinte 58 3 86 147
Salmon River 12 2 11 25
Rural Kingston 10 14 24
Kingston 157 7 35 8 65 15 287
Rideau-Tay 34 1 1 2 21 59
Thousand Islands 33 7 36 76
Total 311 13 9 40 14 247 15 649
Non-PEM
PEM
Health Link Total

31
Figure 12: Family Health Team (FHT) main sites in the South East LHIN, January 2015.

32
Figure 13: Non-Patient Enrolment Model (PEM) physician locations in the South East LHIN, January 2015.

33
UTILIZATION OF CORE PRIMARY CARE SERVICES
Information was obtained from the MOHLTC’s Medical
Services database, which contains Ontario Health
Insurance Plan (OHIP) approved claims data. A core
primary care visit was defined as one or more billings
occurring for the same patient, on the same day for
select billing codes (see here for details).
Note that since medical service data sources contain
only fee‐for‐service provider activity, visits at providers
that are salaried or paid through alternative payment
programs (e.g., some community health centres,
academic institutions, etc.) would not be included if the
provider does not submit "shadow-billed" claims (i.e.,
claims submitted for recording purposes but not for
payment purposes). As well, there are known data
quality issues with the place of residence noted for
some patients in the medical services database due to
outdated address information associated with the ‘red
and white’ health cards.
• In fiscal year 2013/14, there was a rate of 2.6 core
primary care visits per population in the South
East LHIN. This was slightly lower than the
provincial rate of 3.1 and was mid-range
compared to other LHINs (ranging from 1.3 in
Toronto Central to 5.4 in Central and Central
West). Overall utilization of core primary care
services is likely higher given that not all providers
submit OHIP billing claims and will vary between
areas based on the distribution of primary care
models and shadow-billing practices within each
area.
• The utilization rate of core primary care visits in
the South East LHIN increased with increasing
age, from 1.4 visits per population under 20 years
of age to 5.0 visits per population 85 years of age
and over (Figure 14). By sex, rates were higher for
females in all age groups, with the exception of
those aged 85+ (4.6 visits per female compared to
5.8 visits per male). Increased frequency of
utilization within the older age groups will have
implications for future demands on services due
to the aging South East LHIN population.
• Sixty-five percent of the South East LHIN
population had a core primary care visit in
2013/14. This proportion increased with
increasing age, from 56% among those under 20
years of age to 84% among those 85 years of age
and over.
• Across the South East LHIN, core primary care
utilization rates were highest in Rural Hastings
(2.9 visits per population, 75% of the population
accessing these services) and lowest in Rideau-
Tay (1.9 visits per population, 57% of the
population accessing these services). Again,
variation between areas may be in part due to the
distribution of primary care models; a relatively
high proportion of the population in Rideau-Tay
accessed CHC primary care services compared to
other Health Links in 2014/15 (13% versus <8%
for all other areas).
Figure 14: Age-and sex-specific rates of core primary care visits, South East LHIN, fiscal year 2013/14.

34
ACCESS TO, AND SATISFACTION WITH, PRIMARY CARE
The information presented below is based on results
from the Health Care Experience Survey conducted by
the MOHLTC from January-December 2014 (estimates
for patient attachment and same/next day access are
for April 2014-March 2015). Includes adults aged 16
and older.
• The South East LHIN performed well on a number
of measures related to access to, and satisfaction
with, primary care. The South East LHIN continues
to have the highest level of primary care
attachment among all the LHINs. Between July
2014 and June 2015, 97.5% of adults (95%
Confidence Interval (CI) 96.3-98.6%) in the South
East LHIN reported having a primary care
provider, compared to 94.0% (95% CI 93.4-94.5%)
provincially (Figure 15). As well, in 2014, over 90%
of adults (91.8%, 95% CI 89.6-94.0%) reported
that their primary care provider always or often
gives them the opportunity to ask questions, and
86.9% (95% CI 84.3-89.6%) reported that their
provider always or often spends enough time with
them – both of which were the highest
proportions among the LHINs.
• However, some challenges exist related to
accessing primary care on the same day or next
day, as well as accessing after-hours primary care.
About 40% of adults (40.3%, 95% CI 34.6-45.9%)
in the South East LHIN reported being able to see
a primary care provider on the same day or next
day, which was slightly lower than the percentage
for the province overall (43.7%, 95% CI 42.1-
45.3%) (Figure 15). Also, almost 60% of adults
(59.6%, 95% CI 54.8-64.3%) reported difficulty
accessing after-hours care without going to an
emergency department, one of the highest rates
across the LHINs.
• Health Care Connect is a MOHLTC program that
refers Ontarians who don't have a physician to a
family health care provider who may be accepting
new patients. According to Health Care Connect,
as of December 2015, there were about 3,000
patients within the South East LHIN Health Links
registered with Health Care Connect who had not
yet been matched with a primary care provider.
Figure 15: Selected indicators from the Health Care Experience Survey, adults aged 16 years and older, South East LHIN and Ontario, January to December 2014 (unless otherwise noted).

35
Community Health Centres
Community Health Centres (CHCs) are non-profit
organizations that provide primary care and
health promotion programs to individuals,
families, and communities using an
interdisciplinary, team-based approach. CHCs
prioritize improving the health and well -being of
populations who have traditionally faced barriers
accessing health services. Each CHC is unique in
the types of services offered as they are tailored
to the needs within the community served.
Data on CHC clients and their individual encounters
with CHC providers were extracted from each South
East LHIN CHC’s Electronic Medical Record. Data on
group encounters from fiscal year 2014/15 were
obtained from the OHRS/MIS system. Additional details
on the types of groups offered were provided by each
CHC.
Figure 16: South East LHIN Community Health Centre (CHC) locations (including satellites).

36
CLIENT CHARACTERISTICS
• CHC clients in the South East LHIN have more
complex conditions than what is expected based
on the complexity of primary care provided to the
Ontario population. The Standardized ACG
Morbidity Index (SAMI) is an index used to
measure client complexity by examining
differential morbidity at the primary care practice
level. Compared to the average Ontarian, all
South East LHIN CHCs have more complex clients,
especially those served by the Kingston CHC
Street Health Centre.
• Belleville Quinte West CHC and Kingston CHC
serve a relatively younger client population (47%
and 54% of clients accessing services in fiscal year
2014/15 were under 45 years of age,
respectively), while the other CHCs had an older
client population (with each having about 30% of
clients over 65 years of age).
• Certain South East LHIN CHCs appear to have a
relatively high proportion of clients with lower
income levels, education levels, single parent
households, and lone person households
compared to the South East LHIN overall.
However, this information was not available for a
relatively high proportion of clients at most CHCs.
• For a given CHC, the majority of the clients
accessing services in 2014/15 were from one
Health Link region. Belleville and Quinte West
CHC had nearly 90% of clients coming from the
Quinte Health Link, Gateway CHC had 80% from
the Rural Hastings Health Link, Kingston CHC had
68% from the Kingston Health Link and 20% from
Salmon River (the location of the Napanee and
Area CHC), and both Country Roads CHC and
Rideau CHS had the majority of their clients
coming from the Rideau-Tay Health Link (86% and
74% of clients, respectively).
INDIVIDUAL ENCOUNTERS WITH CHC PROVIDERS
• In 2014/15, the South East LHIN CHCs saw just
over 20,000 clients, with a total of nearly 200,000
individual encounters to primary care and allied
health providers.
• The number of clients accessing services in
2014/15 varied by CHC, ranging from about 3,200
clients at both Country Roads CHC and Gateway
CHC to about 5,800 clients at Rideau CHS.
• There were 21 different types of primary care and
allied health providers across the South East LHIN
CHCs, reflecting the interdisciplinary nature of
this primary care model. Across CHCs, the
majority (81%-87%) of encounters in 2014/15
were with primary care-related providers. Among
the allied health-related specialties, encounters
with social workers, dietician/nutritionists,
counselors, chiropodists, and community health
workers were most common across the South
East LHIN CHCs.
• The number of clients accessing services in a
given year across the South East LHIN CHCs has
increased over time, with a 12% increase between
2012/13 and 2014/15. The number of encounters
also increased but not to the same extent, with a
3.2% increase during the same period.
• By CHC, overall encounter volumes have varied
over time (Figure 17). Belleville and Quinte West
CHC has seen continuously increasing volumes
with the establishment of service provision at
their CHC. Overall encounter volumes at Gateway
CHC, Kingston CHC, and Country Roads CHC have
remained relatively constant over the last three
years, and volumes at Rideau CHS increased in
fiscal year 2013/14 and decreased the following
year. Note that variation in utilization rates
between CHCs, as well as in volumes over time for
a given CHC, may result from differences in client
characteristics, provider complement and staffing

37
counts, service availability, or
charting and coding practices. As
well, migrations to a new
electronic medical record (EMR)
system over the last three years
were also noted to affect
encounter volumes.
• Looking at interdisciplinary
teamwork rates, nearly four-
fifths (78%) of all CHC clients in
the South East LHIN received
care from more than one
provider over a two-year period.
Rates ranged from 69% at
Kingston CHC to 86% at Gateway
CHC. More than half of the clients (56%) saw
three or more providers, and a third (32%) saw
four or more.
• There was diversity in the mode of contact for
encounters across CHCs and by provider type. The
majority of encounters for each CHC and provider
type took place in person with the client at the
CHC. At Kingston CHC and Rideau CHS, phone
contact with third parties on behalf of the client
was common for a number of provider types
(physicians, nurses, nurse practitioners,
accounting for 15-25% of encounters with these
providers). Registered nurses at Gateway CHC had
a relatively high (~30%) proportion of encounters
at outreach locations. For all CHCs, encounters
with allied health professionals were generally
more diverse in terms of the mode of contact
(i.e., higher proportion of outreach and home
visits).
• No shows for appointments can be a challenge for
providers working with marginalized populations.
The no-show rate for appointments (excluding
cancelled appointments) varied across the South
East LHIN CHCs and by provider type. No-show
rates were higher for encounters with allied
health providers compared to the primary care-
related providers (23% versus 10% overall for the
South East LHIN CHCs). No-show rates for both
allied health and primary care providers were
highest for Kingston CHC (34% and 19%,
respectively), and were lowest at Gateway CHC
(<1% and 6%).
• Across the CHCs, the average number of
encounters with the various primary care-related
provider types increased with increasing age. The
one exception was at Kingston CHC, where the
average number of encounters in the 20-44 and
45-64 year age groups were often as high, or
higher than, encounter rates for those aged 65+.
Increased frequency of utilization within the older
age groups will have implications for future
demands on services due to the aging South East
LHIN population.
• Based on utilization patterns for 2014/15 and
projected population growth, the number of
encounters with primary care providers is
projected to grow at each CHC. LHIN-wide,
between 2014/15 and 2018/19, the projected
average annual growth in the number of
encounters is 1.3% for physicians, 1.5% for
registered practical nurses, 1.1% for registered
nurses, and 0.5% for nurse practitioners.
Figure 17: Number of encounters by provider type, CHC and fiscal year, 2012/13-2014/15.

38
GROUP ENCOUNTERS WITH CHC PROVIDERS
• The South East LHIN CHCs held just over 3,000
group sessions in fiscal year 2014/15, with about
35,000 participants in these groups. The number
and type of group sessions offered varied by CHC.
Kingston CHC and Rideau CHS each held about
800 group sessions, Belleville and Quinte West
CHC held 621, Gateway CHC held 479, and
Country Roads CHC held 384.
• Looking at specific group programs, there were
about 130 different types of group sessions run by
all the CHCs, reflecting the diversity of
programming offered by the CHCs. By category,
the greatest variety in program types was for
nutrition, with just over 40 programs offered
across the CHCs (including programs related to
the Good Food Box and community
kitchens/cooking demonstrations), followed by
diabetes education (just under 40 types, including
foot care, pre-diabetes, and exercise programs,
with most being offered by the Rideau CHS
Diabetes Education Program), and health
promotion/education/ community development
(about 25 types, including living well, walking, and
gardening programs).

39
Community Support Services
Community Support Services (CSS) are a range of
programs and services intended for seniors or
people with disabilities who prefer to stay at
home. Services can be offered at the client’s home
or in the community and are provided by a
number of different agencies across our region.
Data on CSS clients and their encounters with CSS
providers was obtained from each CSS agency’s data
collection system (NesdaTrak and other data
management systems). The LHIN-level analysis of CSS
client and service volumes is based on data from the
MOHLTC Management Information System (MIS).
GENERAL DATA NOTES
• Variation in volumes between agencies may result
in part from differences in the interpretation and
application of service coding across agencies
within the LHIN and across the province. Also,
volunteer activity and services provided by self-
raised funds, may impact the perspective on LHIN
funding return on investment.
• Two of the 28 CSS organizations (Brockville and
District Hospice Palliative Care Service and
Canadian National Institute for the Blind -
Kingston) did not report client or encounter
information in time for inclusion in this report.
The CSS organizations are listed in Table 5.
• The availability of client age, sex, and location of
residence in the data has improved over time at
the LHIN level, to 92%, 97%, and 96% in 2014/15,
respectively.
• The number of events is based on face-to-face
contact and does not include phone contact. The
only exception is for Security & Reassurance
where phone contact is included in the service
event count.
Acronym Organization Name
ASBH Alzheimer Society Belleville Hastings Quinte
ASK Alzheimer Society Kingston
ASLC ALZ Lanark County
BGH Brockville and District Hospice Palliative Care
Service
CCCH Community Care for Central Hastings
CCNH Community Care North Hastings
CCSH Community Care for South Hastings
CH Cheshire Homes (Hastings-Prince Edward)
CHS Canadian Hearing Society
CHSLC Community Home Support Lanark County
CNIBK Canadian National Institute for the Blind –
Kingston
CPHC Community & Primary Health Care - Lanark,
Leeds & Grenville
HHH The Heart of Hastings Hospice
HK Hospice Kingston
HLA Hospice Lennox & Addington
HPE Hospice Prince Edward
HQ The Regional Hospice of Quinte Inc.
LASOS Lennox and Addington Seniors Outreach
Services (SOS)
LOCS Land O’Lakes Community Services
MBQ Mohawks of the Bay of Quinte
MOD March of Dimes (Rehab. Foundation for the
Disabled)
NFCS Northern Frontenac Community Services
PCBIS Providence Care – Reg. Comm. Brain Injury
Services
PCHC Providence Care – Hildegard Centre & ACOP
PECCCS PEC Community Care for Seniors
PTI Pathways to Independence
SFCS Southern Frontenac Community Services
VON VON Canada –
Hastings/Northumberland/Prince Edward
Table 5: List of Community Support Services Organizations in the South East LHIN.

40
• Data from the Mohawks of the Bay of Quinte is
only represented on regional level and not
reflected in per agency analysis.
• Rates per 1,000 population calculated at the
LHIN-level are based on the total LHIN population.
Given the relatively older population in the South
East LHIN and the fact that most CSS services are
targeted towards the older age groups, overall
utilization rates for the South East LHIN may
appear higher than other areas due in part to this
difference in the age structure of the population.
Further investigation of age-specific or age-
standardized rates would help illuminate
differences in utilization between areas that is not
related to differences in the age structure of the
population.
GENERAL OBSERVATIONS
• CSS agencies are located across all of the South
East LHIN Health Links (Figure 18).
• In fiscal year 2014/15 and compared to other
LHINs in Ontario, the South East LHIN CSS
agencies served a relatively high number of
individuals (per capita) for the following (with an
asterisk indicating the highest rate in the
province):
Figure 18: South East LHIN Community Support Service locations. Symbols indicate the primary service provided by the organization.

41
o General geriatric health promotion*
o Case management*
o Crisis intervention
o Day services
o Deaf, Deafened Services
o Foot Care*
o Hospice Visiting*
o Meals delivery*
o Respite*
o Transportation
o Vision Impaired care
o Social and safety visiting
• In contrast, the South East LHIN had the lowest
utilization rates for Assisted Living services among
all the LHINs.
HOME SUPPORT SERVICES
• In total, the number of clients served increased
year over year in all age groups (Figure 19). The
observations described below are for 2012/13 to
2014/15, unless denoted otherwise. Rates per
1,000 population are calculated for 2014/15.
• The number of clients served per capita is the
lowest in Kingston and Quinte West SubLHINs and
highest in Addington N/C Frontenac and
Tyendinaga Napanee SubLHINs.
• Adult Day services were provided by 5 agencies,
predominantly by VON and CPHC (Community &
Primary Health Care – Lanark, Leeds and
Grenville). All SubLHINs are served, with Central
Hastings having the fewest number of clients per
capita served.
• Congregate Dining services were provided by 9
agencies and showed variance across SubLHINs in
terms of clients served per capita with Kingston,
North Hastings, and Quinte West relatively
underserved. Addington N/C Frontenac had the
highest rate per 1,000 population served in
2014/15.
• Care Giving and Home Help (includes Home
Maintenance and Home Making) service was
provided by 9 agencies. There was variance across
SubLHINs (clients served per capita) with
Kingston, Stone Mills Loyalist, North Hastings, and
Quinte West SubLHINs being relatively
underserved. Addington N/C Frontenac had the
highest rate per 1,000 population served in
2014/15.
• Foot Care service was provided by 9 agencies and
5 agencies served significantly more clients than
others. There was variance across SubLHINs
(clients served per capita) with Kingston,
Belleville, and Quinte West SubLHINs relatively
underserved. North Hastings had the highest rate
per 1,000 population served in 2014/15.
• Meals delivery (meals on wheels and frozen
meals) service was provided by 11 agencies, and 4
agencies served significantly more clients than
others. The ratio of meals to clients seems to be
consistent among these agencies. There was
Figure 19: Number of CSS clients served by Fiscal Year, service category, and age group, South East LHIN.

42
variance across SubLHINs (clients served per
capita) with Kingston, Stone Mills Loyalist, and
Quinte West SubLHINs relatively underserved.
Tyendinaga Napanee had the highest rate per
1,000 population served.
• Friendly Visiting (includes Grand Friends and
Good Fellowship) service was provided by 8
agencies. Kingston, Quinte West, and North
Hastings SubLHINs were relatively underserved.
• Respite services were provided by only 6
agencies. The four western SubLHINs have
received relatively more services per 1,000
population.
• Socialization and Activation service was provided
by 7 agencies and LASOS (Lennox and Addington
Seniors Outreach) provided significantly more
services than any other agency. There was
variance across SubLHINs (clients served per
capita), with 8 out of 15 SubLHINs relatively
underserved. Tyendinaga Napanee had the
highest rate per 1,000 population served.
• Security & Reassurance service was provided by 6
agencies. There was variance in the service/client
ratio among agencies and CHSLC (Community
Home Support Lanark County) served the most
clients. There was variance across SubLHINs
(clients served per capita) with 7 out of 15
SubLHINs relatively underserved. Smiths Falls
Perth and North Hastings had the highest rate per
1,000 population served.
• Transportation service was provided by 11
agencies. There was variance across SubLHINs
(clients served per capita), with Kingston and
Quinte West relatively underserved. Tyendinaga
Napanee and Addington N/C Frontenac had the
highest rate per 1,000 population served.
HOSPICE SERVICES
• The rate per 1,000 population of clients who
received hospice visiting was the highest amongst
other LHINs in 2014/15.
• Hospice Quinte and Hospice Kingston experienced
a higher number of services year-over-year and
delivered the bulk of hospice visiting services in
the region. Although no data was received from
Hospice Brockville, Addington and Smiths Falls
SubLHINs were well served with hospice and
bereavement support services.
SPECIALIZED SERVICES
• The rate per 1,000 population of clients who
received vision impaired care and hearing care
was above average compared to other LHINs in
2014/15.
• The per capita services for Acquired Brain Injury
(ABI) including Assisted Living, Day Services and
Personal Support were at the provincial average.
ABI intake served clients from all SubLHINs.
• Deaf support services (clients per 1,000
population) were highest in Kingston and
Belleville, with very low rates in the other western
SubLHINs.
• The Seniors Managing Independent Living Easily
(SMILE) program is run by the VON. The number
of clients served increased from 847 in 2011 to
2004 in 2014. A diverse range of services were
provided of which house hold management had
the highest volume of services.
• Supportive Living services for physically disabled
adult persons were concentrated in the western
SubLHINs only.

43
ALZHEIMER SOCIETIES
• Residents from only 5 out of 15 SubLHINs
received services from Alzheimer societies
• The number of public education services dropped
by almost 50% in 2014 (from 2013). This might be
attributable to data quality issues post-
amalgamation of agencies.

44
Community Addictions and Mental Health
OVERVIEW OF THE ADDI CTIONS AND MENTAL HEALTH REDESIGN
The South East LHIN Addictions and Mental Health
Redesign was initiated in 2013 and aims to ensure that
our addictions and mental health system meets the
needs of clients and their caregivers. This goal is
articulated through the Ideal Individual Experience,
which describes the end state vision of the client
journey throughout his or her life and throughout the
continuum of care. This vision was developed with
input from clients, their families and from providers,
and has been endorsed by providers across the region.
The adoption of this Ideal Individual Experience across
the region will not only help establish a consistent
approach to care, but it will also mean that clients will
be able to travel across the system and know exactly
what to expect from one care provider to the next.
Activities within the Addictions and Mental Health
Redesign include the development and
implementation of a common basket of services across
the South East LHIN region, a regional back office
integration plan, and a common training and capacity
plan.
For more information on the Addictions and Mental
Health Redesign, see the South East LHIN website.
Region Acronym Organization Name
Hastings and
Prince Edward
(HPE)
AMHS-HPE Addictions and Mental Health Services - Hastings
Prince Edward
QHC Quinte Healthcare Corporation
SACQ Sexual Assault Centre for Quinte and District
YHQ Youth Habilitation Quinte
Kingston,
Frontenac,
Lennox &
Addington
(KFLA)
AMHS-KFLA Addiction & Mental Health Services – Kingston,
Frontenac, Lennox & Addington
HDH Hotel Dieu Hospital
KGH Kingston General Hospital
PC Providence Care
SAHL Salvation Army Kingston Harbour Light
SACK Sexual Assault Centre Kingston
Lanark, Leeds,
Grenville (LLG)
LLGAMH Lanark, Leeds and Grenville Addictions and Mental
Health
BGH Brockville General Hospital
CMHALG CMHA Leeds and Grenville Branch
(No longer funded by South East LHIN as of fall 2015)
LCMH Lanark County Mental Health
DSLG Developmental Services of Leeds and Grenville
(No longer funded by South East LHIN as of fall 2015)
Regional PSSEO Peer Support South East Ontario
Table 6: South East LHIN Community Addictions and Mental Health Organizations.

45
GENERAL DATA NOTES
For all data sources used in this section, variation in
volumes between organizations, as well as over time
for a given organization, can result in part from
differences in the interpretation and application of
service codes and data collection practices. As well,
transitions between information systems at some
organizations has also impacted data quality.
As part of the Addictions and Mental Health Redesign,
the South East LHIN will work together with
community addictions and mental health (AMH)
agencies to investigate opportunities to standardize
data collection and reporting procedures across
organizations. As well, processes for routine collation
and analysis of LHIN-wide data should be developed to
better understand community mental health services
in the South East LHIN by important client
characteristics such as age, sex, and place of residence.
This will be essential to ensure that service gaps and
areas of future need for community mental health
services within our region can be identified and
addressed. The implementation of a common client
record will greatly increase data quality and
standardization.
Figure 20: South East LHIN Community Addictions and Mental Health Service Locations. Symbols indicate the primary service provided by the organization.

46
UTILIZATION OF COMMUNITY AMH SERVICES
Information is based on OHRS Trial Balance
Submissions for provincial sector code=323 (CMH&A)
for Fund Types 2 and 3. Note that two hospitals
providing community AMH services (KGH, BGH) do not
report client activity statistics using this sector code
and as a result are not reflected in the information
below. Also note that the number of clients served
metric does not reflect “not uniquely identified service
recipients”. Such clients are more commonly served by
organizations providing anonymous or phone-based
services.
• In fiscal year 2014/15, there were 23,196 clients
served by South East LHIN community AMH
organizations. These clients had about 364,000
individual visits/interactions and attended 9,300
group sessions. The South East LHIN community
AMH organizations received about 12,000 new
referrals to their programs in that year, and
provided about 158,000 days of
inpatient/resident care in supportive housing and
crisis beds. The number of visits, group sessions,
and inpatient/resident days have increased over
the last three years, while the number of
individuals served by the organizations and the
number of new referrals have either varied or
decreased over the same time period.
• Compared to other LHINs, the South East LHIN
had the fourth or fifth highest utilization rates per
capita for the number of visits, new referrals,
inpatient/resident days, and individuals served by
community AMH organizations in 2014/15. Rates
of group participants and group sessions per
capita were lower, with the South East LHIN
having the ninth and tenth highest rates,
respectively.
Figure 21: Distribution of South East LHIN community addictions and mental health clients, visits/interactions, and resident days by service type, fiscal year 2014/15.

47
Figure 22: Distribution of community addictions and mental health clients by organization and service type, fiscal years 2012/13 – 2014/15.
Note: All reported client activity for Peer Support South East Ontario (PSSEO) in the OHRS Trial Balance submission was for not uniquely identified clients. Information on the number of unique individuals served was provided by PSSEO and is presented in the figure.

48
• The majority (just under 80%) of community AMH
clients in 2014/15 were accessing mental health
services (Figure 21). By program type, the most
common types of mental health services accessed
by clients were for crisis intervention (5,454
clients), counseling and treatment (5,265 clients),
and case management (4,368 clients). For
addictions, the most common type of service
utilized was treatment for substance abuse (3,150
clients), followed by residential addiction
withdrawal management centres (1,088 clients)
and case management (383 clients).
• In terms of the number of visits/interactions for
mental health services, the highest number of
visits/interactions were for case management
(75,226), crisis intervention (53,245), and
assertive community treatment (ACT) teams
(54,704) (Figure 21). For addictions services,
treatment for substance abuse had the highest
number of visits/interactions (16,044).
• For residential-based services, there were
138,902 resident days (7,049 crisis bed days)
associated with mental health services and 18,718
resident days for addictions services (Figure 21).
• Across organizations, the number of clients
served has either remained generally consistent
or has increased over time, particularly at
Providence Care (Figure 22). The number of
visits/interactions, group sessions, and resident
days generally mirrored these trends. Note that
variation in number of clients served by
organization, as well as in clients served over time
for a given organization, may result from
differences in client characteristics, staffing levels,
and service offerings (e.g., long-stay residential
programs would generally have fewer clients
compared to case management services).
• Certain programs are only offered by one or two
organizations in the region, such as programs for
eating disorders, withdrawal management/detox,
and child/adolescent services.
COMMUNITY ADDICTIONS SERVICES
Information is based on data from the provincial Drug
and Alcohol Treatment Information System (DATIS).
DATIS collects data from publically funded agencies
(excluding acute care or psychiatric hospitals) that
provide one or more specialty programs for substance
abuse and/or problem gambling. The information
below reflects all South East LHIN residents accessing
services, regardless of where the agency was located
(i.e., includes out of LHIN agencies).
Note that Lennox and Addington Addiction Services
(now part of Addiction & Mental Health Services –
Kingston, Frontenac, Lennox & Addington) did not
report data into DATIS for fiscal year 2014/15, resulting
in overall lower volumes for some services in that year
(see notes below).
Substance Abuse
Overall Trends in Utilization
• Compared to other LHINs in the province, the
South East LHIN had the third or fourth highest
rate per capita for substance abuse open (new or
carry over from a previous year) admissions
between fiscal years 2007/08 and 2012/13. This
ranking remained consistent despite a slight
decline in overall service utilization during the 6
year period. In 2012/13, there were
approximately 85 open admissions per 10,000
population for substance abuse services in the
South East LHIN.
• The two most utilized substance abuse services in
the South East LHIN between 2012/13 and
2014/15 were community treatment (1-2 hour
sessions in group or individual format, typically
once a week or less often, while the client resides
in the community) and residential withdrawal
management (for individuals who volunteer to
withdraw from alcohol and other substances).

49
• In terms of community treatment, there were
almost 1,650 new admissions in 2014/15, a 33%
increase compared to the previous two years. This
resulted in part from changes to reporting
procedures, as new admissions for initial
assessment treatment planning services were
reported under this category as of 2014/15.
Carryover admissions for community treatment
declined notably (>20%) from just over 1,050 to
less than 825 during this three-year period, due in
part to the absence of data for Lennox and
Addington Addiction Services (now part of
Addiction & Mental Health Services – Kingston,
Frontenac, Lennox & Addington).
• For residential withdrawal management,
utilization decreased from about 730 new
admissions in both 2012/13 and 2013/14 to just
under 620 cases in 2014/15. There were no
carryover admissions for this service.
• Other substance abuse services with relatively
high utilization in the LHIN included:
o Case management experienced a notable
decrease in carryover admissions (>180 to <
120, due in part to the absence of data for
Lennox and Addington Addiction Services) but
a sizeable increase in new admissions (115 to
>140) over the 3 year
period.
o Residential treatment
(a structured,
scheduled program of
treatment and/or
rehabilitation activities
provided while the
client resides in-house)
saw a slight decrease in
new admissions (from
183 to 170) but a
corresponding increase
in carryover admissions
(from 45 to 63).
o Support within housing (a range of services
provided in the client’s residence) saw an
increasing number of both new (from less
than 5 to 30) and carryover (from 10 to 29)
admissions
o Residential support (housing and related
recovery/support services such as lifestyle
counselling, coaching for activities of daily
living, community reintegration, vocational
counselling, and mutual aid) remained at 18-
20 new and 5-6 carryover admission during
the three-year period.
• Across service types in 2014/15, between 8% and
15% of admissions had an associated mental
health hospitalization within the last year; higher
rates tended to be related to admissions for
residential services.
Client Characteristics
• Overall, nearly all (85%) of admissions for
substance abuse services in 2014/15 were for
those between 16 and 54 years of age.
• Two out of every three admissions for Community
Treatment were from clients aged 25-54, with the
majority being in the 35-54 year age group (Figure
Figure 23: Number of admissions (new and carryover) for substance abuse services by age group and fiscal year, South East LHIN residents, fiscal years 2012/13 to 2014/15.

50
23). About 1 in 5 of admissions were for those
younger than 25 years of age and 10% were for
those 55 years or older.
• Residential substance abuse services were most
commonly utilized by clients 35-54 years of age
(>40%) and 25-34 years of age (>30%), with
relatively lower utilization for those 55 years or
older (>12%) or younger than 25 (<10%) (Figure
23).
• About half of admissions for case management
were for clients 25-34 years of age, followed by
about a quarter of clients 35-54 years of age and a
fifth of those younger than 25 years (Figure 23).
• With the exception of case management, the
majority (between 60% and 80%) of substance
abuse admissions across service types were for
male clients. For case management, about 80% of
admissions for case management in 2014/15
were for female clients, though just 2 years prior
more males utilized this service.
• For most substance abuse services, about half of
admissions were for clients who reported being
single (i.e. never married).
• Overall, utilization of substance abuse services
was highest for residents of the Kingston &
Islands SubLHIN (accounting for about 35% of
admissions), followed by Smiths
Falls/Perth/Lanark, Belleville, and Brockville (each
about 10% of admissions). This is in part reflective
of the larger overall population in some of these
areas; however, relative rates of utilization per
population were notably high in Smiths
Falls/Perth/Lanark
• Of note, residents of the Kingston & Islands
SubLHIN had relatively higher utilization of
residential withdrawal and case management
compared to other service types, accounting for
about half of all admissions for these service
categories (compared to about one third of
admissions for other services)
Problem Gambling
• Provincially, with the exception of the North West
LHIN, admissions for problem gambling generally
did not surpass 5 cases per 10,000 population
over the last six years. Overall, the South East
LHIN had between 2 and 4 open admissions per
10,000 population between 2007/08 and
2012/13, with the highest reported levels of
utilization occurring in the middle of this period
• In the South East LHIN, reported volumes of
problem gambling services varied considerably
over the last three years, as well as by service
type. The most commonly reported services were
community treatment and community
day/evening treatment services.
• Further understanding and improvement of data
quality issues will enable a more in-depth analysis
and understanding of service utilization for
problem gambling services.
COMMUNITY MENTAL HEALTH SERVICES
Information is based on data extracts from each
organization’s client information management system.
Not all organizations collect record-level data for all
clients due to the nature of services provided, or were
not able to provide data in a format that allows for a
systematic and consistent analysis of client and service
characteristics across organizations. As a result, the
following information does not reflect all South East
LHIN community mental health organizations, all
services within a particular organization, and all clients
accessing services within an organization.
Clients by Age Group
• Across the organizations and services with data
available for analysis, the majority of clients
accessing community mental health services in

51
2014/15 were between 20 and 64 years of age.
Organizations that provide services tailored to
certain age groups saw relatively more clients in
the younger and older age groups, including
Youth Habilitation Quinte (half of all clients under
20 years of age and all clients under 45 years of
age) and Providence Care (43% of clients were 65
years of age and over).
• Some services were accessed more frequently by
clients in certain age groups. In 2014/15, early
intervention services were provided solely to
clients under 45 years of age, with 30% of these
clients under the age of 20. Services for eating
disorders, the intensive transitional treatment
program (ITTP), and diversion and court support
were also primarily provided to those under 45
years of age. Looking at the older client
population, abuse services, wellness programs,
and social rehabilitation and recreation were
primarily provided to those 45 years of age and
over.
Clients by Sex
• There appeared to be some
variation in the distribution of
clients by sex across the CMH
organizations. Relatively equal
numbers of male and female
clients accessed services at
Quinte Healthcare Corporation,
Addiction & Mental Health
Services – Kingston, Frontenac,
Lennox & Addington, Hotel Dieu
Hospital, and Lanark, Leeds and
Grenville Addictions and Mental
Health. The other organizations
saw a higher proportion of
female clients, from 59%
females at Addictions and
Mental Health Services -
Hastings Prince Edward to 67%
at Youth Habilitation Quinte and Kingston General
Hospital.
• By service type, nearly all (>94%) clients accessing
eating disorders, abuse services, and family
initiatives services were female. Child/adolescent,
ITTP, and counselling and treatment services were
also more commonly accessed by females. Males
were more likely to access short term crisis
support beds, early intervention, diversion and
court support, psychogeriatric, and support within
housing services.
Clients by Place of Residence
• The CMH organizations within the HPE and LLG
regions primarily served clients from the one or
two closest Health Link regions (Figure 24).
Organizations within the KFLA region had the
majority of their clients coming from the Kingston
Health Link, but also saw clients from a range of
other Health Link regions. Out of LHIN clients
Figure 24: Distribution of community mental health clients by organization and Health Link of Residence, South East LHIN, fiscal year 2014/15.
Note: Information on client Health Link of residence was not available for SACQ, SACK, LCMH, BGH, and PSSEO. Note that not all services within each organization are reflected for fiscal year 2014/15. As a result of this, the distribution of clients by place of residence are is not reflective of all clients served by these organizations. Clients may be counted more than once if they access multiple service types within or across organizations.

52
accounted for about 5% or less of the client
population at each organization.
• A full understanding of CMH utilization rates by
Health Link is not possible due to the absence of
information on client place of residence for all
organizations. Understanding possible geographic
areas of need for CMH services should also
consider population health status and need for
services in addition to utilization rates.
Client-Identified Unmet Needs
Understanding the needs of consumers of
community mental health services can help to
guide service planning to address the areas of
greatest unmet needs. Research has
demonstrated that focusing on addressing client-
identified unmet needs can lead to better
outcomes in quality of life.
Information on client-identified unmet needs is
captured using the Ontario Common Assessment of
Need (OCAN), which is completed as part of community
mental health service provision across the South East
LHIN. Information from these assessments can be
shared across organizations using the Integrated
Assessment Record (IAR) to assist with planning and
delivery of services. Unmet needs are defined as areas
that remain a serious problem for the client, despite
any help that is provided.
Preliminary data is available in the IAR from 6 South
East LHIN service providers. Information is available for
clients with an assessment completed in the 12 month
period ending August 26, 2015. The data reflect only
assessments uploaded into the IAR and where the
client has granted consent to share their information.
Note that each individual organization has more
complete assessment information for their clients since
not all assessments are uploaded into the IAR.
• Across the mental health functional centers with
the greatest number of assessments, the life
domains where clients have identified the most
unmet needs are psychological distress, company,
daytime activities, physical health, money, and
intimate relationships.
• Further investigation and discussion is required to
better understand the assessment data contained
in the IAR and how representative it is of the
community mental health client population across
the South East LHIN. As well, methods for
obtaining more complete assessment data should
be investigated, either through encouraging use
of the IAR or by working with each organization
directly to understand information about the
assessments not included in the IAR. With this
understanding, further analysis can be conducted
to understand unmet client needs overall, as well
as by organization and by the type of service
provided.

53
Home Care
Data on utilization of home care was obtained from the
MOHLTCs Home Care Database (HCDB), which
captures information on clients receiving services from
Community Care Access Centres (CCACs).
• The South East LHIN had the highest rate of active
home care clients per 1,000 population in fiscal
year 2013/14 (62.2 for the South East LHIN versus
a provincial average of 45.8). There were over
30,600 active clients in this year.
• The South East LHIN had the fourth highest rate
of service visits at 793 per 1,000 population
(compared to a provincial average of 648). The
rate of service visits was highest for nursing visits
(557 visits per 1,000 population – 65% of all visits)
and the rate of visits for occupational therapy (55
visits per 1,000 population compared to the
provincial average of 36) and social work visits
(10.2 vs 3.9) were the highest across the 14 LHINs.
• The utilization rate of home care services
increased with increasing age across most service
recipient categories – an important consideration
as the baby-boomer population ages. (i.e., those
currently between 50 and 70 years of age).
• In-home maintenance, in-home support and long-
term care placement services are utilized at a
higher rate by older age groups. The In-home
maintenance and long-term support categories
accounted for a large volume of service – over
86% of the total hours of service provided by the
CCAC in 2014/15.
• Younger age groups comprised a large percentage
of the in-home rehabilitation service recipient
category with children (0-9 years) accounting for
11% of these visits in 2014/15.
• In 2014/15, over 6,000 CCAC admissions were
referred as hospital inpatients (36.7% of the total
admissions). Community social services or other
individuals accounted for 15% of admissions, and
self-referrals accounted for just under 4% of
admissions. Just under 19% were referred as
hospital outpatients and just under 17% were
referred by general practitioners.
• The number of ‘high needs’ clients being
supported with home care services in the
community has increased substantially over the
past few years. The number of these clients has
more than doubled between 2011/12 and
2014/15, with approximately 1,900 clients in April
2010/11 and over 4,000 in the first quarter of
2015/16.
• The projected increase in the number of seniors
in the South East LHIN as the baby-boomer
generation ages will result in a large increase in
demand for many CCAC services. Without any
changes in the way services are currently
delivered, there will be increased utilization of
these services by 2041:
o Acute (in-home) services would increase by
38%
o Rehabilitation (in-home) services would
increase by 64%
o Long-Term supportive (in-home) services
would increase by 77%
o In-home maintenance services would double
(an increase of 103%)

54
HOSPITAL-BASED
SERVICES
Hospitals in the South East LHIN
There are seven hospital corporations with thirteen
hospital sites in the South East LHIN (Figure 25).
Together these sites provide the population with the
broad mix of acute care, post-acute and outpatient
services to meet their needs. The local hospital system
Perth Smiths Falls
District Hospital – Perth
site 24,670 ER Visits 47 Acute beds
(43 Medical/Surgical, 4 ICU)
Perth Smiths Falls District
Hospital – Smiths Falls site 20,440 ER Visits 38 Acute beds
(30 Medical/Surgical, 4 ICU, 4 Obstetric)
4 Bassinets
1 CT machine
Brockville General
Hospital 25,885 ER Visits 77 Acute beds
22 Mental Health Beds (55 Medical/Surgical, 9 ICU,
12 Obstetric, 1 Paediatric)
42 Chronic beds
5 Rehab beds 10 Bassinets
1 CT machine
Kingston General Hospital 56,607 ER Visits 390 Acute beds
37 Mental Health beds
46 Bassinets
1 MRI, 2 CT machines
Providence Care Centre
120 Mental Health beds
98 Chronic beds
46 Rehab beds
Lennox & Addington
County General
Hospital 25,867 ER Visits 30 Acute beds
(26 Medical/Surgical, 4 ICU)
22 Convalescent Care Beds
Quinte Health Care – Belleville site 38,218 ER Visits 108 Acute beds
(74 Medical/Surgical, 14 ICU, 14 Obstetric)
24 Mental Health beds
18 Chronic beds
44 Rehab beds
22 Bassinets
1 MRI, 1 CT machine
Quinte Health Care –
Bancroft site 12,996 ER Visits
6 Acute beds
Quinte Health Care –
Picton site 17,987 ER Visits 12 Acute beds
Quinte Health Care –
Trenton site 31,345 ER Visits 24 Acute beds
1 CT machine
Hotel Dieu Hospital 49,489 ER Visits
1 CT machine
Figure 25: South East LHIN Hospitals and their ED visit volumes (for fiscal year 2014/15), bed counts, and MRI and CT machine counts (as of December 2015).

55
includes an academic health science centre in Kingston
– meeting a range of the highly-specialized care needs
of the local population. Information on overall ED
volumes (from NACRS), overall bed counts (from the
MOHLTC Bed Census Summary), and MRI and CT
machines by site are noted in Figure 25.
Note that the South East LHIN hospitals do not have
any formally designated addiction and crisis unit beds
within the mental health bed type category. As well,
Perth & Smiths Falls District Hospital has no formally
designated rehab beds, but some acute beds are
informally being used for this purpose. Additional
rehab beds are under development at Brockville
General Hospital.
There is also one MRI machine being operated by an
Independent Health Facility in Kingston.
Emergency Department
Data on utilization of emergency departments (EDs)
was obtained from the Canadian Institute for Health
Information’s (CIHI’s) National Ambulatory Care
Reporting System (NACRS).
The acuity level of ED visits is classified using the
Canadian Triage & Acuity Scale (CTAS). High-acuity is
defined as CTAS levels I, II, and III (Resuscitation,
Emergent, and Urgent), and low-acuity is defined as
CTAS levels IV and V (Less Urgent/Semi Urgent and Non
Urgent).
OVERALL UTILIZATION
• After a steady decline in emergency department
(ED) volumes, from 304,589 in 2011 to 293,466 in
fiscal year 2013/14, the number of ED visits
increased to 303,824 in 2014/15.
• The rate of emergency department visits for non-
admitted low-acuity patients was highest among
younger age groups. For non-admitted high-acuity
visits, the rate was highest among the oldest age
groups. As with inpatient utilization, the rate of
ED visits that resulted in admission increased
exponentially with increasing age.
• The proportion of ED visits that resulted in an
admission was over one fifth for patients 75+
years of age, and increased with successively
older cohorts. The proportion of non-admitted
high-acuity visits also increased with increasing
age, although not as dramatically. The percentage
of ED visits for low-acuity conditions decreased
with older cohorts.
• South East LHIN residents had the third highest
rate of ED utilization after only the two Northern
LHINs. The crude rate of 600 visits per 1,000
population in 2013/14 was 40% higher than the
provincial rate. Higher rates are evident across
the more rural LHINs in Southern Ontario with a
higher percentage of these visits being for low-
acuity purposes.
• Low-acuity ED visits are often examined for health
system planning purposes as a portion of these
visits could potentially be addressed in other non-
urgent health care settings. In the South East
LHIN, over 46% of ED visits in 2014/15 were low-
acuity. The South East LHIN is among a group of
LHINs (South West, Erie St. Clair, North Simcoe
Muskoka, and the Northern LHINs) that have
relatively high proportions (over 40%) of low-
acuity visits.
• Scheduled visits are were virtually non-existent in
2014/15. Across all South East LHIN hospitals
there were a total of 24 scheduled visits – down
from over 900 in 2009/10.
• The volume of ER visits by South East LHIN
residents is projected to be slightly below 305,000
in 2016/17 and increase by 2.9% between
2016/17 and 2021/22 (Figure 26) (projected
volumes are based on age/sex-specific rates for 5

56
year age groups computed from
two years of data combined. These
rates are then applied to future
population projections based on
the same 5-year age groups).
UTILIZATION BY HOSPITAL
• The highest volumes of ED visits in
the South East LHIN were at KGH
(with an increase from 46,800 ED
visits in 2009/10 to 56,600 in
2014/15 – a 20% increase over
these 5 years) and HDH (an Urgent
Care Centre (UCC) with just under
49,500 visits in 2014/15), followed by QHC-
Belleville (38,200) and QHC-Trenton (31,300).
• As an UCC, HDH saw a high volume of non-
admitted patients, specifically low-acuity non-
admitted patients (accounting for over 70% of ED
visits at HDH).
• KGH saw relatively few non-admitted low-acuity
patients (23% of the hospitals total ER visits in
2014/15 –compared to the average of 45% across
the SE LHIN hospitals) and had the highest
percentage of admitted patients (20%) and non-
admitted high-acuity patients (57%).
• Non-admitted low-acuity patients accounted for
55% of ED visits at both PSFDH sites in 2014/15 –
a major reduction from 65% in the year previous
and 72% in 2012/13.
• Higher percentages of low-acuity patients were
also evident at other smaller rural hospitals across
the LHIN (QHC-Bancroft, QHC-Picton, and LACGH).
• The proportion of patients that left prior to the
completion of treatment was highest at QHC-
Belleville (8%), followed by BGH and LACGH (5%
at both sites).
• There was pronounced seasonal variation in the
number of ED visits at QHC-Picton, QHC-Bancroft,
and PSFDH-Perth, with notably higher summer
volumes at these sites.
TIME OF DAY
• The time of day at which patients register in the
ED was relatively consistent across sites in
2014/15 (consistent with historical patterns). The
number of registrations increased after 6 AM to a
peak between 10 AM and 11 AM, followed by a
slow gradual decline throughout the remainder of
the day (Figure 27).
• Low volumes of ED visits are seen overnight at the
smaller hospitals in the region. LACGH, both
PSFDH sites, and the Bancroft and Picton sites of
QHC each saw on average less than 5 patients per
night between midnight and 6 AM.
Figure 26: Actual and projected emergency department visits, South East LHIN residents, 2009/10 to 2021/22.
The dotted lines indicates
projected ER volumes if we
continued to use ER’s at the same
rate across age/sex categories
The actual number of ER
visits varies from this line…
other factors (i.e. more than
age and sex groups) were
impacting our use of ERs

57
LENGTHS OF STAY
Note that in other reports, ED visit wait times
are usually defined as the 90th percentile
length of stay (i.e. 1 in 10 had an ED visit that
lasted past that point). The information
below reflects the total time that patients
spend in the ED (i.e. time from registration or
triage (whichever is first) to the time the
patient leaves the ED), which will be lower
than the 90th percentile statistics.
• Across South East LHIN hospitals in
2014/15, just under 75% of patients had
an ED LOS that was less than 4 hours.
The notable exceptions were at KGH
and QHC-Belleville, where
approximately 55% of patients had a
LOS that was less than 4 hours. Across
South East LHIN hospitals, the entire ED
visit ended within 8 hours for 93% of patients.
• At KGH, 4.6% of patients had an ED LOS longer
than 24 hours in 2014/15. At QHC-Belleville 1.7%
of patients in the ED stayed longer than 24 hours
in the ED.
• The average length of stay (LOS) for ED visits was
much higher for admitted patients. Across all age
groups in 2014/15, non-admitted low-acuity
patients averaged a 2.2 hour ED LOS, non-
admitted high-acuity patients averaged 3.6 hours
and admitted patients averaged 13 hours. For
each of the three patient categories, there is a
trend toward longer ED LOS among older age
groups.
Same Day Surgery
Data on utilization of same day surgery was obtained
from the Canadian Institute for Health Information’s
(CIHI’s) National Ambulatory Care Reporting System
(NACRS).
• The South East LHIN rate of day surgery visits
remained second highest across the LHINs in fiscal
year 2014/15, at 131 visits per 1,000 population.
This rate is considerably higher than the provincial
rate of 88 visits per 1,000 population.
• The number of day surgery visits at South East
LHIN hospitals has remained relatively constant
over time, with a very slight decline over the past
3 years (from 61,441 in 2012/13 to 61,033 in
2014/15).
• Endoscopic interventions on the digestive tract
(inspections and biopsies) accounted for the
highest number of day surgery events followed by
cataract procedures and minor digestive
interventions.
Figure 27: Average daily number of patients registering in the ER across South East LHIN hospitals by time of day, fiscal year 2014/15.

58
• The number of cardiac catheterizations has
increased from 2,645 in 2012/13 to 3,022 in
2014/15. These procedures are performed only at
KGH.
• There is a steady increase in the rate of non-
emergency outpatient procedures across older
age groups – including day surgery cases, renal
dialysis visits, oncology visits, and cardiac
catheterization visits. There is a general steady
increase in the rate of visits for each of these
ambulatory case types as the population ages.
The rates peak among the population in their 70’s
(though the rate of renal dialysis visits continues
to increase into the 90+ age group).
• Oncology visits increased by 19% over the past
three years, from 31,007 in 2012/13 to 36,823 in
2014/15. The bulk of these visits were to KGH
(over 91% of the total volume).

59
Acute Inpatient
Data on utilization of acute inpatient services was
obtained from CIHI’s Discharge Abstract Database
(DAD). Unless otherwise stated, the statistics quoted
below exclude newborn and stillborn cases. Note that
the fiscal year reflects the year the patient was
discharged from hospital.
OVERALL UTILIZATION
• As a LHIN, the number of acute inpatient
separations across our hospitals has continued to
increase, from 36,101 in fiscal year 2009/10 to
39,504 in 2014/15.
• Residents of the South East LHIN had a relatively
high rate of inpatient separations compared to
the province as a whole in 2013/14 (83.8
separations per 1,000 South East LHIN residents
compared to the provincial rate of 73.2). The
Northern LHINs had a much higher rate of
inpatient utilization (over 110 separations per
1,000). South East LHIN was part of a group of 5
relatively rural LHINs in Southern Ontario (South
East, Erie St. Clair, South West, Hamilton
Niagara Haldimand Brant, North Simcoe
Muskoka) with crude separations rates
hovering around 80 per 1,000 population.
The more urban LHINs had a lower rate of
inpatient separations.
• The rate of acute inpatient utilization in
the South East LHIN was highest in the first
year of life and among older age groups
(Figure 28).
• For females, there is an increase in acute
inpatient utilization, primarily related to
obstetrics, for those within child-bearing
age (i.e. 20-39 years of age).
• The increasing rate of acute inpatient
utilization across older cohorts begins to
increase noticeably at approximately 50 years of
age, and increases exponentially with older age
groups.
• Health Based Allocation Model (HBAM) Inpatient
Grouper (HIG) weights are relative values that
describe the expected acute inpatient resource
use of an average patient within specified clinical
groups and with certain demographic and clinical
characteristics. Higher HBAM HIG weights reflect
relatively higher resource use. The average HBAM
HIG weight per separation for South East LHIN
residents (1.62) in 2013/14 was highest across the
LHINs and was higher than the provincial average
(1.50). An older population may account for a
portion of the higher relative resources required
per inpatient event.
• The average acute length of stay (LOS) for
hospitals in the South East LHIN (5.4 days in
2014/15) has reduced over the past several years
(from 5.8 days in 2011/12 and 6.1 days in
2008/09) and was equal to the provincial average.
• The South East LHIN displayed a similar pattern
compared to most other LHINs in terms of the
rate of inflow (i.e. out of LHIN residents coming to
South East LHIN hospitals) and outflow (i.e. South
Figure 28: Bed days per year and rate of acute inpatient visits, South East LHIN residents, average of fiscal years 2013/14 and 2014/15 combined.

60
East LHIN residents going to out of
LHIN hospitalist), with a higher
percentage of outflow from the
South East LHIN (6.4% inflow vs
12.3% outflow).
• The volume of acute inpatient
discharges by South East LHIN
residents is projected to be 46,900
in 2016/17 and is projected to
increase to approximately 50,750 in
2021/22 (Figure 29).
• If utilization of acute inpatient beds
continued at current rates the
number of bed days would be
projected to increase by 57% by
2041 as the population increases
and ages.
• The acute LOS at QHC-Belleville (3.8 days) was
shorter than other South East LHIN hospitals
(aside from the specialized inpatient programs at
HDH, which had a 2 day average acute LOS).
Conversely, the acute LOS was highest at PSFDH-
Perth (6.7 days) and LACGH (6.7 days).
ALTERNATE LEVEL OF CARE (ALC)
Alternate Level of Care (ALC) is a designation given by
a physician to a patient who is occupying a bed in a
hospital while not requiring the intensity of resources
or services provided in that particular care setting.
• The average ALC LOS in the South East LHIN had
dropped considerably over time, from 26.8 days
in 2008/09 (third highest across the LHINs) to as
low as 16 days in 2011/12 (seventh highest across
LHINs). The numbers reflect the average number
of days these ALC patients (i.e. those with 1 or
more ALC days as part of their hospital stay) spent
after being designated ALC. The average ALC LOS
increased over the past 2 years to just under 25
days in 2014/15 for patients with an ALC
component of their stay.
• Patients awaiting alternate placement accounted
for 46,299 acute inpatient days in 2008/09 (127
beds at 100% occupancy). This count decreased to
a low of 31,968 in 2013/14 (87 beds) but has
increased to 39,184 for patients discharged in
2014/15 (107 beds) (Figure 30).
Figure 29: Actual and projected acute inpatient discharges, South East LHIN residents, fiscal years 2009/10 to 2021/22.
Figure 30: Acute and Alternate Level of Care (ALC) days of care at South East LHIN acute inpatient hospitals, fiscal years 2009/10 to 2014/15.

61
SERVICES AND PROGRAM S
• Medical cases (i.e. cases not
requiring surgical
intervention, not related to
a mental health diagnosis,
and not related to childbirth
issues) across the South East
LHIN accounted for
approximately 51% of acute
inpatient separations and
over 57% of total days in
2014/15 (Figure 31). These
cases represented 74% of all
ALC days. The volume of
medical separations is
highest in the 75 years and
over age group.
• Surgical cases had higher
average resource use,
accounting for 27% of
separations in 2014/15 but
40% of weighted cases.
• Obstetrics and Neonatology
each accounted for just over
10% of total separations
across South East LHIN
hospitals in 2014/15 (Figure
32). KGH, QHC-Belleville,
and BGH collectively
accounted for
approximately 77% of
medical separations and
over 90% of surgical,
obstetric, and neonatal
separations.
• The volume of Mental Health discharges appears
small in Figures 31 and 32. However, these figures
account for patients discharged from acute
inpatient beds in 2014/15 and do not include
patients who were admitted to inpatient mental
health beds over the year.
Figure 32: Distribution of acute inpatient separations by service category at South East LHIN Hospitals, average of fiscal years2013/14 and 2014/15 combined.
Figure 31: Number of acute inpatient separations by service category at South East LHIN Hospitals, average of fiscal years 2013/14 and 2014/15 combined.

62
Surgical and Diagnostic Wait Times and Volumes
Surgical and diagnostic wait times and volumes for
completed and open cases were obtained from the
MOHLTC Wait Time Information System (WTIS) hosted
through the Cancer Care Ontario (CCO) iPort reporting
system. Information is presented for priority levels 2, 3
and 4 combined.
COMPLETED CASES
Wait times for completed cases are measured using an
indicator derived by CCO that shows the percent of
cases that were completed within the access target, as
set by the MOHLTC. The access targets differ based on
procedure as well as priority level.
Table 7: Summary of surgical and diagnostic wait times for completed and open cases by South East LHIN hospital, fiscal
year 2014/15.
Note: The first number and underlying bar indicates the percent of cases completed within access target, and the number in brackets
indicates the percent of open cases that have been on the wait list for a duration greater than the access target. Open case information
was not available for CT and MRI scans.
Hospital
General
Surgery
Gynaeco-
logic
Surgery
Neuro-
surgery
Oncology
Procedures
Ophthal-
mic Surgery
Oral and
Maxillo-
facial
Surgery and
Dentistry
Ortho-
paedic
Surgery
Otolaryngic
Surgery
Plastic and
Recon-
structive
Surgery
Thoracic
Surgery
Urologic
Surgery
Vascular
Surgery
QHC - - - -
LACGH - - - - -
KGH -
KMRI - - - - - - - - - - - -
HDH - - - - - -
PSFDH - - - - - -
BGH - - - -
SELHIN
Ontario
Adult Surgical Procedures
99 (LV) 97 (4) 92 92 (3) 100 81 (3) 83 (10) 96 (LV)
98 (26) 97 98 85 (30) 100 (LV) 100
76 (19) 82 (17) 54 (33) 88 (5) 68 (LV) 55 (25) 90 (LV) 87 (43) 97 74 (30) 74 (LV)
86 (14) 86 (7) 82 (15) 52 (31) 57 (37) 82 (39)
99 (LV) 94 (LV) 97 89 (13) 75 (31) 100
94 (4) 79 (12) 58 99 (5) 100 36 (31) 81 (22) 61 (12)
94 (11) 91 (10) 54 (33) 89 (4) 90 (6) 95 (5) 63 (24) 69 (29) 85 (39) 97 89 (13) 74 (10)
95 (18) 91 (19) 83 (22) 88 (15) 91 (11) 85 (21) 83 (24) 88 (28) 92 (24) 94 (35) 96 (18) 83 (19)
Hospital
Paediatric
Dental/
Oral/
Maxillo-
facial
Surgery
Paediatric
General
Surgery
Paediatric
Gynaeco-
logic
Surgery
Paediatric
Neuro-
surgery
Paediatric
Ophthal-
mic Surgery
Paediatric
Ortho-
paedic
Surgery
Paediatric
Otolaryngic
Surgery
Paediatric
Plastic and
Recon-
structive
Surgery
Paediatric
Urologic
Surgery CT Scan MRI Scan
QHC - -
LACGH - - - - - - -
KGH - -
KMRI - - - - - - - - - -
HDH - -
PSFDH - - - - - - - - - -
BGH - - - - - - - -
SELHIN
Ontario
Paediatric Surgical Procedures Diagnostic Procedures
94 100 LV LV 82 95 (8) 100 83 50
LV LV LV LV
LV 96 (LV) 100 LV 73 (15) 65 (LV) 19 (59) 79 51
16
34 (32) 98 87 (LV) 71 (16) 65 (11) 95 (LV) 74 LV
78
100 33 (20) 95
68 (25) 97 (4) 100 50 87 (8) 73 (14) 75 (11) 81 (20) 72 (50) 80 36
70 (30) 92 (11) 92 (16) 92 (7) 86 (22) 81 (16) 85 (19) 88 (16) 82 (21) 67 39
LV: Low Volumes – procedures with less than five occurrences were excluded from the analysis.

63
Surgical
• The South East LHIN completed a total of 27,830
surgical cases in fiscal year 2014/15, with an
average of 81% completed within access target.
This was below the provincial average of 89%.
In the South East LHIN, 12 out of 21 surgical
procedures were completed within the provincial
access target at a rate of 80% or greater in
2014/15 (Table 7). Furthermore, 7 of 21 surgical
procedures were completed with a rate of 90% or
greater.
• The South East LHIN was lower than the provincial
rate of cases completed within the access target
for 14 out of 21 surgical procedures; however,
many were within only a 5-10% difference (Table
7). Notable differences were observed with
neurosurgery and paediatric neurosurgery cases
(29% and 42% difference, respectively).
• Ophthalmic and orthopaedic surgeries had the
largest volume of completed surgical cases in the
South East LHIN from 2012/13 to 2014/15 (Figure
33). Provincially, these procedures also had the
highest volume of completed surgical cases.
• Ophthalmic surgery had one of the largest
volumes of completed surgical cases in the South
East LHIN and has also maintained a high rate of
cases that were completed within target, at 90%
in 2014/15 (down from 94% in 2012/13).
• Overall, there has been a decrease in the number
of orthopaedic surgery cases completed within
access target over time in the South East LHIN,
from 67% in 2012/13 to 63% in 2014/15. LACGH
and QHC are the only facilities in the South East
LHIN that noted an increase in cases completed
within target during this time (24% and 17%
increases, respectively).
Figure 33: Number of completed surgical and diagnostic cases, South East LHIN, fiscal year 2014/15.

64
Diagnostic
• The South East LHIN completed a total of 63,224
diagnostic cases in 2014/15 with an average of
58% completed within the access target. This was
slightly higher than the provincial average of 56%.
• In 2014/15, the majority of diagnostic cases were
completed at QHC (18,837), followed by KGH
(13,625), HDH (12,263), and KMRI (an
Independent Health Facility, 10,240). BGH and
PSFDH completed 4,184 and 4,095 cases,
respectively. LACGH did not complete any case as
they do not operate CT or MRI scanners on site.
• Overall, the South East LHIN completed a higher
percentage of CT scans within target compared to
the province from 2012/13 to 2014/15. HDH, with
the majority of CT volumes, as well as KGH and
QHC, have seen an increase in cases completed
within the access target from 2012/13 to
2014/15. BGH has remained consistent at 95%
over the same period, and PSFDH saw a decrease
from 90% to 78%.
• Between 2012/13 and 2014/15, the volume of
MRI scans completed in the South East LHIN has
nearly doubled. The increase in volume has been
accompanied by a decrease in the number of
cases completed within target, from 58% in
2012/13 to 36% in 2014/15. Kingston MRI
maintains the largest volume of MRI procedures
and saw the largest decrease in completed cases
within target from 47% in 2013/14 to 16% in
2014/15 (note: KMRI had zero cases in 2012/13).
• Data for 2015/16 Q3 show a decrease in percent
of cases completed within access target for CT
scans in the South East LHIN. For MRI scans, the
South East LHIN overall shows a slight increase
from 36 to 37% cases completed within access
target; HDH maintained 100%, while KGH and
QHC saw increases, however, KMRI has dropped
to 6% for cases completed within access target.
OPEN SURGICAL CASES
Open cases (i.e. cases that are still on the wait list, yet
to be completed), are similarly measured using a CCO
indicator that shows the percent of cases that have
been on the wait list for a duration that has already
exceeded the access target.
• The South East LHIN had approximately 15.8% of
open cases on the wait list for a duration that
exceeded the access target in 2014/15. This has
decreased from 17.7% in 2012/13.
• The procedures that maintained the largest
volume of open cases on the wait list in the South
East LHIN at year end from 2012/13 to 2014/15
were ophthalmic and orthopaedic surgery (Table
7 and Figure 34). These procedures also had the
largest volume of open cases that had been on
the wait list for a duration that exceeded the
access target; however, this only accounted for
6% for ophthalmic surgery compared to 24% for
othropaedic surgery.
• Excluding procedures with less than five open
cases, plastic and reconstructive surgery, as well
as neurosurgery, had the highest percentage of
open cases that had been on the wait list for a
duration that exceeded the access target in the
South East LHIN in 2014/15. This was an increase
for both procedures from 2012/13.
• The largest volume of open cases on the wait list
in the South East LHIN from 2012/13 to 2014/15
was observed at HDH and QHC, with the majority
being ophthalmic and orthopaedic surgeries (39%
and 24% of open cases at HDH; 27% and 21% of
open cases at QHC, respectively). While HDH
averaged 19% of open cases on the wait list for a
duration greater than the access target in
2014/15, QHC only averaged 2% - the lowest in
the South East LHIN.
• For orthopaedic surgeries in the South East LHIN,
KGH and HDH had the largest volume of open
cases on the wait list. These volumes have

65
increased overall from 2012/13 to 2014/15
(increase of 120 and 92, respectively). Both
facilities saw a peak in the number of open cases
on the wait list for a duration greater than the
access target in 2013/14, however, the number
decreased again in 2014/15.
• For ophthalmic surgeries in the South East LHIN,
HDH maintained the majority of open cases on
the wait list from 2012/13 to 2014/15, with a
notable increase in 2014/15 by approximately 200
cases.
• The percent of open cases on the wait list for a
duration that exceeded the access target was only
7% in 2014/15, a decrease from a peak of 14% in
2013/14.
Figure 34: Number of open surgical cases (at year end), South East LHIN hospitals, fiscal year 2014/15.

66
Inpatient Mental Health
Data on utilization of inpatient mental health acute
inpatient services was obtained from CIHI’s Ontario
Mental Health Reporting System (OMHRS).
• The crude rate of mental health inpatient active
cases for South East LHIN residents in fiscal year
2013/14 (466 per 100,000 population aged 15 and
over) was below the provincial average (523 per
100,000 population). The average length of stay,
however, was much higher (56 days) at South East
LHIN hospitals than compared to other areas of
the province (the next highest LHINs are at 36
days).
• The number of acute mental health inpatient
admissions has decreased substantially at QHC-
Belleville, from approximately 500 in 2010/11 to
261 in 2014/15.
• The largest number of admissions in 2014/15 was
at KGH (825), followed by BGH (566) and QHC-
Belleville (548). These sites provide acute mental
health inpatient services and have shorter lengths
of stay (in 2014/15 the average length of stay at
KGH was 16.5 days, BGH 13.2 days, QHC-Belleville
10.5 days).
• Providence Care provides long-stay inpatient and
forensic mental health services. The 276
admissions at Providence Care in 2014/15
accounted for 11.4% of the total admissions
across the South East LHIN but 40% of the total
bed days. Patients discharged from long stay
mental health beds and forensic mental health
beds at Providence Care in 2014/15 had an
average length of stay of 231 days.
Critical Care
Data on utilization of Intensive Care Unit (ICU) beds
were obtained from Ontario’s Critical Care Information
System (CCIS). Six hospital sites in the South East have
ICU beds and report into the CCIS:
Hospital Site
Number
of Level 2
Beds
Number
of Level 3
Beds
Total
ICU
Beds
QHC – Belleville 5 9 14
LACGH 4 0 4
KGH 32 33 65
PSFDH – Perth 4 0 4
PSFDH – Smiths Falls 4 0 4
BGH 6 3 9
South East LHIN 55 45 100
Information reported for fiscal year 2015/16 reflects all
data reported into CCIS as of February 15, 2016 (i.e.
does not reflect the complete fiscal year).
Note that variation between hospitals can result in part
from differences in data quality and entry into the CCIS
system, as well as due to how ICU beds are utilized in
each hospital.
OVERALL VOLUME AND DISTRIBUTION OF SERVICES
• As of December 2015, there were 100 ICU beds in
the South East LHIN region (Table 8). The majority
(65) of these beds were located at KGH, followed
by QHC – Belleville (14), BGH (9), and four each at
LACGH and at both PSFDH sites.
• Level 3 beds are capable of providing the highest
level of service, including the ability to
mechanically ventilate patients for more than 48
Table 8: Number of ICU beds by South East LHIN hospital site as of December 2015.

67
hours. Three hospitals in the South East LHIN have
Level 3 beds, with the majority (33) of the beds
located at KGH. QHC – Belleville had nine, and
BGH had three.
• In fiscal year 2014/15, there were 7,866 patients
admitted to ICUs in the South East LHIN. The
annual count of ICU admissions has declined over
time (was 8,030 in fiscal year 2011/12).
• The total number of ICU beds in the region have
also declined in this time period, from 108 to 100
(as of December 2015). This resulted from an
increase in one bed at QHC – Belleville, and a
decrease of nine beds at KGH.
• Mirroring the distribution of ICU beds, the highest
number of ICU admissions was at KGH (61% of all
ICU admissions), followed by BGH (12%), QHC –
Belleville (11%), LACGH (6%), PSFDH – Perth (5%),
and PSFDH – Smiths Falls (5%) (Figure 35).
SOURCE OF ADMISSION
• At most hospitals, the majority of ICU patients
were admitted from the ED in the same hospital.
For the South East LHIN as a whole, 50% were
admitted from the ED in 2015/16. Other common
sources of admission include the operating room
or post-anesthesia care unit (OR/PACU, 21% of
South East LHIN admissions) and units/wards
(14% of admissions) within the same hospital.
• There was a lower proportion of patients
admitted from the ED and a higher proportion
admitted from the OR/PACU and Level 2/Step
Down and Level 3 (Medical/Surgical or Specialty
Unit) critical care units at KGH.
• Only 1% of South East LHIN ICU admissions were
from out of LHIN, with nearly all out of LHIN
patients being admitted to QHC – Belleville and
KGH. Compared to the centrally located LHINs,
the South East had a relatively lower proportion
of ICU admissions from outside of the LHIN
(provincial rate is 3%).
Figure 35: Number of ICU admissions, average length of stay, and occupancy rates by hospital and quarter, South East LHIN, fiscal year 2014/15 - 2015/16 (to February 15, 2016).
Note: Occupancy rate not available for 2014/15.

68
PATIENT DEMOGRAPHIC AND CLINICAL CHARACTERIS TICS
Age Group
• Nearly all (89%) ICU admissions in the South East
LHIN were for those 40 years of age and over, and
about half were for those between 60 and 79
years of age.
• This distribution was similar across the South East
LHIN hospitals, as well as provincially; however,
there was a higher proportion of admissions for
youth (i.e., those under 18 years of age) at KGH
(accounting for 5% of admissions) and a higher
proportion of admissions for those aged 60+ at
both PSFDH sites.
Admitting Diagnosis
• In the South East LHIN, patients were most
commonly admitted to the ICU with
cardiovascular/cardiac/vascular diagnoses (34% of
all South East LHIN admissions in 2015/16), which
was higher than the provincial percentage of 42%.
The proportion of admissions with this diagnosis
varied across hospitals, from 28% at QHC-
Belleville to 53% at PSFDH – Perth. Other
common admission diagnoses included
respiratory (20% of South East LHIN admissions,
with a relatively higher (40%) proportion at QHC –
Belleville), neurological (8% of South East LHIN
admissions, with slightly higher proportions at
QHC – Belleville and KGH), and gastrointestinal
(6% of South East LHIN admissions, with a
relatively higher proportion (22%) at LACGH).
• By age group, admissions for Trauma and
Metabolic/Endocrine diagnoses were relatively
more common among those under 40 years of
age compared to the other diagnosis groups.
Those under 40 years accounted for 42% and 33%
of admissions for these diagnoses, respectively.
Nine Equivalents of Nursing Manpower
Use Score (NEMS)
• The nine equivalents of nursing manpower use
score (NEMS) is frequently used to quantify,
evaluate and allocate nursing workload at the ICU
level.
• The mean NEMS score for ICU admissions in the
South East LHIN was relatively lower compared to
other LHINs and the province as a whole (mean of
20.3 for the South East versus 21.9 for the
province overall).
• Within the South East LHIN, NEMS scores were
highest at QHC – Belleville (mean of 26.1 in the
most recent quarter), BGH (20.9), and KGH (19.5).
Mean NEMS scores appeared to be increasing
over time at BGH (was 17.6 in Q1 of fiscal year
2014/15).
Multiple Organ Dysfunction Score (MODS)
• The Multiple Organ Dysfunction Score (MODS)
provides an objective scale to measure the
severity of the multiple organ dysfunction
syndrome as an outcome in critical illness.
• The mean MODS score for ICU admissions in the
South East LHIN was similar to the province as a
whole (3.0 versus 2.8, respectively).
• Within the South East LHIN, mean MODS scores
were highest at KGH (3.6 in the most recent
quarter) and QHC – Belleville (3.4). Scores appear
to be generally increasing at most South East LHIN
hospitals over the last two years. Data on MODS
scores from BGH were only reported for Q4 of
2015/16.

69
INTERVENTIONS
• In the South East LHIN, just over 70% of ICU
patient days were spent on ventilation, 40% were
spent on central venous lines, about 25% were
spent on arterial lines, about 20% were spent on
intravenous vasoactive/inotropic medication, and
less than 5% were spent on dialysis or intracranial
pressure monitors in fiscal year 2015/16. These
percentages of ICU days spent on life support
interventions were relatively lower compared to
the province overall. The percentage of ICU
intervention days spent on ventilation, central
venous, and arterial lines was highest at QHC –
Belleville, followed by KGH.
• The ventilator occupancy rate, defined as the
number of patient days with mechanical invasive
ventilation divided by the total ventilated bed
days, provides an approximation of utilization of
ventilator capacity. The ventilator occupancy rate
in the South East LHIN in fiscal year 2015/16
(48%) was similar to the provincial rate (50%). By
hospital, QHC – Belleville had the highest
ventilator occupancy rate (70%) in the most
recent quarter, followed by KGH (47%) and BGH
(7%). All three hospitals had some quarterly
variation in rates. LACGH and PSFDH are not able
to accommodate ventilated patients for any
length of time and, therefore, no ventilated bed
days were reported for these two hospitals.
DISCHARGE INFORMATION
• The majority (65%) of South East LHIN patients
discharged from the ICU in fiscal year 2015/16
continued to be treated in the same hospital, with
most of these patients going to a unit/ward.
About 20% were discharged home, 7% died while
in the ICU, and 4% were transferred to another
hospital within the LHIN.
• Trends in discharge destination are influenced by
the acuity level of patients seen at each hospital.
Information on discharges by bed type (i.e., Level
2 and 3) would provide a more fulsome
understanding of these trends; however, this
breakdown is not currently available in the CCIS
standard reports.
• Compared to the province overall, a higher
proportion of South East LHIN patients were
transferred to a unit/ward (61% in the South East
versus 54% provincially) or to home (22% versus
17%), and fewer were transferred to a Level
2/Step Down and Level 3 (Medical/Surgical or
Specialty Unit) critical care units (4% versus 13%).
• By hospital, a higher proportion of patients were
discharged to another hospital within the LHIN or
to home from LACGH, PSFDH – Smiths Falls, BGH,
and PSFDH – Perth, as would be expected based
on the lower acuity level of patients treated at
these hospitals. A higher proportion of discharged
patients stayed within the hospital or were
deceased at QHC – Belleville and KGH.
• ICU discharges occurring at night (defined in this
analysis as between the hours of 10:00 PM and
7:00 AM) have been associated with an increased
risk of mortality post-discharge and readmission.
The night time discharge rate from ICUs in South
East LHIN in fiscal year 2015/16 was similar to the
provincial rate (both about 8%). By hospital, the
night time discharge rates were highest at PSFDH
- Smiths Falls (13%), LACGH (11%), and QHC –
Belleville (10%), however, low numbers at some
of the smaller hospitals may result in higher
variability in rates.
AVERAGE LENGTHS OF STAY
• On average, ICU patients in South East LHIN
hospitals were admitted for about 4 days in fiscal
year 2015/16, which is similar to the provincial
ICU average LOS.
• At the hospital level, patients stayed slightly
longer at KGH and QHC – Belleville (average LOS

70
of 4.7 and 4 days in the most recent quarter,
respectively), with several spikes in quarterly
average length of stay at QHC – Belleville over the
last two years (Figure 35).
• Higher LOS can result from higher patient acuity
levels and can also be influenced by patient flow
issues
OCCUPANCY RATES
• The ICU occupancy rate for the South East LHIN
was 78% in fiscal year 2015/16, which is slightly
lower than the provincial rate of 81%.
• By hospital, ICU occupancy rates often varied
considerably by quarter (~30% difference in
occupancy rates between quarters at QHC –
Belleville and LACGH) (Figure 35). In the most
recent quarter, occupancy rates ranged from 65%
at LACGH to 96% at QHC – Belleville.
AVOIDABLE DAYS
• The avoidable days rate, defined as the number of
delayed transfer days divided by the total ICU
patient days, reflects the percent of time that
patients spend occupying an ICU bed when they
have been deemed ready for transfer by the most
responsible physician and no longer require the
intensity of care provided in the ICU. Delays in
transfer can result from capacity issues in other
health care settings and other patient flow
considerations.
• The avoidable days rate for the South East LHIN in
fiscal year 2015/16 was slightly higher than the
provincial rate (8.7% versus 7.9%, respectively).
• Rates by South East LHIN hospital were variable
by quarter but generally were highest at KGH and
PSFDH – Perth over the last two years (was 13.1%
and 11.7% in the most recent quarter,
respectively). Rates over this time period appear
to be decreasing at QHC – Belleville and
increasing at KGH.
• Note that variation by hospital may be in part due
to differences in methods for identifying patients
who are ready for transfer.
READMISSIONS
• The ICU readmission rate is defined as the
number of readmissions within 48 hours from
non-ICU locations divided by the number of live
ICU discharges. Readmissions are associated with
poorer patient outcomes and can result from
early and/or inappropriate transfers out of the
ICU.
• Rates of ICU readmissions within 48 hours were
similar between the South East LHIN and the
province overall in fiscal year 2015/16 (1.7%
versus 1.8%, respectively).
• Within the South East LHIN in 2015/16, ICU
readmission rates were highest at LACGH (4.9%).
The low number of readmissions at some of the
smaller hospitals may result in higher variability in
rates. There were no readmissions within 48
hours reported at PSFDH – Smiths Falls during this
time period.
MORTALITY RATES
• The ICU mortality rate in the South East LHIN was
relatively lower compared to other LHINs and was
slightly lower than the provincial rate in fiscal year
2015/16 (6.6% for the South East versus 7.1% for
the province overall).
• By hospital, rates were variable by quarter but
were generally highest at QHC – Belleville and
KGH (15% and 10% in the most recent quarter,
respectively).

71
Post Acute Care
COMPLEX CONTINUING CARE
Data on utilization of complex continuing care services
was obtained from CIHI’s Continuing Care Reporting
System (CCRS).
• The rate of complex continuing care (CCC) active
cases for South East LHIN residents in fiscal year
2013/14 was the fourth highest across the LHINs
(at 289 admissions per 100,000 population,
compared to the provincial average of 216).
• The rate and number of CCC bed days increases
dramatically with increasing patient age:
o In the South East LHIN, the rate of CCC bed
days increases from 99 per 1,000 population
aged 45-64 to over 2,775 bed days per 1,000
population in the 85+ age group.
o Just under 20% of the total beds days in
2014/15 were associated with patients under
the age of 65. This increases to over 40% of
the total bed days for the population aged 85
and over.
o 20% of CCC admissions were for patients
under the age of 65, while approximately 60%
were for patients aged 75 or older.
• The number of admissions (and discharges) to
CCC institutions in the South East LHIN declined
slightly in 2013/14 and 2014/15 to approximately
1,145 per year. In the three previous years, the
average number of admissions (1,284) and
discharges (1,277) were slightly higher.
• Total bed days have declined substantially from
over 73,000 in 2008/09, to 60,000 by 2012/13,
and to 51,705 in 2014/15.
• There has been a reduction in the number of CCC
beds in the past three years, from 200 in 2012/13
to 160 in the subsequent year. This results from a
reduction in CCC beds at QHC and LACGH (LACGH
currently has 22 convalescent care beds to better
meet the needs of the patient population).
• Crude assessments of differential access or
utilization of CCC beds is complicated by the large
component of Alternate Level of Care (ALC)
patients in CCC beds. The pressures of the ALC
population are felt across CCC beds at all sites but
are particularly pronounced at BGH, where
between 40% and 50% of CCC bed days are ALC.
• As the population ages and if the rates of
admission to CCC beds continues as per current
practice the number of admissions to CCC beds is
projected to almost double by 2041.
INPATIENT REHABILITATION
Data on utilization of inpatient rehabilitation was
obtained from CIHI’s National Rehabilitation System
(NRS).
• The South East LHIN inpatient rehabilitation
admission rate of 213 admissions per 100,000
population aged 18 and over in fiscal year
2014/15 was below the provincial rate of 286.
• There was a total of 76 inpatient rehabilitation
beds across the South East LHIN in 2014/15, with
46 at Providence Care, 25 at QHC-Belleville, and 5
at BGH. In terms of current and future bed
counts, the number of beds increased at QHC-
Belleville to 44 in 2015/16, and BGH will have 17
inpatient rehabilitation beds as of 2017/18 to
address the historic deficiencies in inpatient
rehabilitation resources in the area. The increase
in inpatient rehabilitation beds at QHC-Belleville
was targeted at clients of the new Behavioural
Support Services Transition Unit (BSSTU)
established at QHC-Belleville.
• Over 15% of inpatient rehabilitation admissions
for South East LHIN residents in 2014/15 were to
hospitals outside the South East LHIN. Patient

72
outflow was split between hospitals in the
Champlain LHIN (5.4%) with smaller percentages
of patients going to institutions in the Toronto
Central LHIN (3.9%) and the Central East LHIN
(3.7%).
• There is much less ‘inflow’ of patients from out of
the LHIN coming to South East LHIN hospitals, as
5.6% of admissions to South East LHIN institutions
in 2013/14 were for residents from outside the
area.
• The number of inpatient rehabilitation admissions
has stabilized over the past few years, fluctuating
around 700 admissions per year (with a high of
740 admissions in 2014/15). Volumes have
increased from a low of less than 550 admissions
in 2008/09.
• The number of inpatient rehabilitation bed days
has remained relatively stable, averaging around
20,500 bed days per year. The 2014/15 fiscal year
had the lowest number of bed days over the last 5
years, at 19,755.
• There has been a general decline in bed days at
BGH and Providence Care over the past 5 years
but an increase in bed days at QHC-Belleville. The
increase at QHC-Belleville relates to an increased
number of beds, from 18 in 2012/13 to 25 in
2014/15. This has increased further to 44 beds in
2015/16 with the addition of the BSSTU.
• Providence Care had the highest volume of beds
days in the South East LHIN (10,528 bed days in
2014/15, accounting for 53% of the total bed days
across the LHIN). Bed days at this site and the
percentage of total bed days across the LHIN they
accounted for have declined since 2011/12
(12,882 bed days, accounting for 61% of total bad
days in the LHIN).
• The volume of bed days has also declined at BGH
from over 2,000 in 2011/12 to 1,452 in 2014/15.
• The reduction in bed days at both Providence
Care and BGH are mirrored by reduced
rehabilitation average lengths of stay (LOS). The
average LOS at the three South East LHIN
inpatient rehabilitation sites ranged from 21.5 to
23.5 days in 2014/15. In 2011/12, the average
rehabilitation LOS were 38.4 days at BGH, 32.8
days at Providence Care, and 24.1 days at QHC-
Belleville.
• Projected rehabilitation volumes are complicated
by the current low utilization rate relative to
provincial norms. This lower utilization is
reflective of a lower number of rehabilitation
beds than other areas – particularly in the Lanark
Leeds and Grenville area. Past analysis to
estimate rehabilitation be requirements utilized
two years of provincial data to construct age/sex-
specific rates of inpatient bed days. These
provincial rates were applied to local population
projections with adjustments for anticipated
market share and desired occupancy levels to
highlight a need for 17 inpatient rehabilitation
beds in the Leeds and Grenville area. The
implementation of these beds at Brockville
General will occur in 2019 to address regional
inequity.

73
LONG-TERM CARE
Long-Term Care Homes provide 24/7 support for
nursing and personal care. Residents have access
to health professionals and receive an individual
care plan which is reviewed every three months.
The home provides meals, accommodation,
personal supplies, medical/clinical supplies,
assistance with activities of daily living, and access
to social and recreational programs.
BED SUPPLY
Information is based on the Long Term Home Care
System Report (LTHCSR) and reflects information as of
March 2015 (unless otherwise noted).
• The South East LHIN had a total of 37 long-term
care homes as of December 2015 (Figure 36). This
includes the Convalescent Care beds at LACGH.
• In total, there were 4,050 long-term care beds in
the South East LHIN as of March 2015. Just under
half (47%) of these were basic beds, 30% were
private beds, and 24% were semi-private beds.
Figure 36: South East LHIN Long-Term Care Home (LTCH) Locations. Symbols indicate the LTCH funding type.

74
• Twenty eight of the long-term care homes in the
South East LHIN had 128 beds or less. Eighteen
had less than 100 beds, and ten had 60 or fewer
beds.
• The number of beds in the South East LHIN had
decreased by 56 since 2012, resulting in marginal
growth since 2009 of 7% (over 5 years).
• The long-term care bed supply rate (per 1,000
population, age 75+) in the South East LHIN was
higher than the provincial rate (Figure 37)
• The majority of beds were located at for-profit
long-term care homes (56%), followed by non-
profit (11%) and municipal (34%) homes.
• Approximately 1,976 of the beds (49% of the
South East LHIN total) across 25 long-term care
homes need to be redeveloped. Redevelopment
includes refurbishing of homes to meet new
standards and requires capital investment. In
some cases, upgrades may result in a temporary
disruption of service or relocation of the home.
• Monthly utilization rates for basic and private bed
types had been consistently above 99%, with
semi-private beds above
97.5%.
• The South East LHIN has
a relatively higher supply
of LTC beds for those 75
and over compared the
province overall (Figure
37). However, this ratio
will decrease annually as
more baby-boomers (i.e.,
those currently between
50 and 70 years of age)
move into the 75 and
over age group. Given
the projected increase in
the size of this age group
(50% increase in the 75+
population by 2025 and a
doubling of this
population by 2033), the demand for long-term
care beds is also expected to increase.
• Approximately 1,976 of the beds (49% of the
South East LHIN total) across 25 long-term care
homes need to be redeveloped. Redevelopment
includes refurbishing of homes to meet new
standards and requires capital investment. In
some cases, upgrades may result in a temporary
disruption of service or relocation of the home.
WAIT LIST AND DEMAND
Information by LHIN is based on data from the MOHLTC
Management Information System (MIS). Detailed
information for the South East LHIN was obtained from
the Long Term Home Care System Report (LTHCSR) and
reflects information as of March 2015.
• Compared with the province overall, the South
East LHIN had a lower median time to placement
(84 days) but had higher rates (per 1000 of the
population) for long-term care residents and long-
term care demand as of March 31, 2015 (Figure
LTC beds
waitlist
Erie St. Clair 87.6 83.9 12.4 96.4 99 56 107
South West 97.4 94.6 16.8 111.3 60 34 68
Waterloo Wellington 81.4 79.3 19.6 98.9 79 45 82
HNHB 88.6 86.3 15.3 101.6 81 86 84
Central West 81.3 79 10.3 89.3 74 50 76
Mississauga Halton 62.3 60.9 20.2 81.2 189 197 189
Toronto Central 73.1 71.3 24.2 95.5 199 57 243
Central 62.9 60.3 23.9 84.2 157 130 161
Central East 82.9 80.2 37.7 118 138 96 147
South East 92.2 90 17.7 107.7 84 64 84
Champlain 87.5 84 24.7 108.7 111 64 135
North Simcoe Muskoka 82.3 78.1 32.4 110.5 152 124 160
North East 104.6 100 25 124.9 58 53 50
North West 99.1 95.8 37 132.8 169 93 187
Ontario 82.6 79.7 22.7 102.4 108 69 116
Median
TTP (days)
From
Acute
Care
Median TTP
(days) From
Community
LTC supply, residents, waitlist and demand
per 1,000 population age 75+Median
TTP (days)
OverallLHIN LTC Supply LTC Residents LTC demand
Figure 37: Long-term care (LTC) supply and demand by LHIN as of March 31, 2015.

75
37). The South East LHIN also had a higher long-
term care supply rate than Ontario.
• Relative to Ontario, the South East LHIN had a
lower median time to placement (TTP) overall and
for clients from both acute and community
settings. The overall median TTP for the South
East LHIN was 24 days shorter than the provincial
median.
• The majority (54%) of clients waiting for
placement in the South East LHIN as of March
2015 were females aged 75 or over. Overall, 79%
of wait list clients were aged 75 years or over.
• The wait list for long stay clients within the South
East LHIN decreased from 1,494 in January 2013
to 1,319 in December 2014.
• The majority (64%) of long-term care wait list
clients requested basic beds. However, basic beds
made up 47% of the total bed supply.
• Wait times for placement were not significantly
different amongst client choice (1st, 2nd and 3rd
choice of home).
• By South East LHIN SubLHIN area, the highest
median wait time (as of March 2015) was in North
Hastings (257 days), though with a relatively low
23 clients from that area waiting for a long-term
care bed.
• In Kingston (including South Frontenac & the
Islands), Belleville (including Quinte West), and
the Napanee area (including Tyendinaga, Stone
Mills and Loyalist), the median wait time for
residents in the community awaiting placement
was greater than 150 days, with substantial
volumes of clients awaiting placement (331, 278,
and 129 clients respectively).
• The northern, more rural SubLHINs had a higher
utilization of long-term care per 1,000 population
compared to other areas of the LHIN. South
Frontenac had a particularly low utilization rate.
RESIDENT CHARACTERISTICS
Information is based on data from the Canadian
Institute for Health Information’s (CIHI’s) Continuing
Care Reporting System (CCRS).
• Overall, 70% of South East LHIN long-term care
home residents as of March 31, 2015 were
female, and 77% were aged 75+ (with 45% aged
85+).
• The top 5 most common conditions captured on
resident’s most recent assessments in 2014/15
were dementia, depression, diabetes,
gastrointestinal disorders, and cerebrovascular
accident. This is a slight change from 2010/11,
where the top 5 conditions were dementia,
hypertension, depression, diabetes, and arthritis.
• The average length of stay (LOS) for long-term
care residents in the South East LHIN was 2.9
years in 2014/15, which was the same as the
provincial rate. The average length of stay has
increased over time, from 2.7 years in 2012 to 2.9
years in 2014.

76
HOSPICE PALLIATIVE
CARE
Hospice palliative care aims to relieve suffering
and improve the quality of living and dying. The
vision for hospice palliative care in the South East
Region is that residents and their families will
have access to exemplary hospice palliative care
when needed. Care will be provided in the most
appropriate setting through an interdisciplinary
program of care which focuses on quality of life,
control of pain and symptoms and attends to the
psychological, spiritual experiences of individuals
and their families in adapting to illness, preparing
for death and bereavement.
Planning for hospice palliative care is guided by
the 2011 Declaration of Partnership and
Commitment to Action for advancing high quality,
high value palliative care in Ontario. The
Declaration contains further information on
definitions of hospice palliative care and details
about models of care.
This analysis uses “hospice palliative care” as an
inclusive term to mean hospice, palliative and end of
life care. Various definitions are used to identify
patients receiving palliative and end of life care based
on the data source being used. Defections are noted in
each section below. Note that these definitions may not
capture all patients receiving palliative and end of life
care who are accessing services in these various
settings.
Information on deaths in the South East LHIN is
important to consider when planning for hospice
palliative care services. A summary of this information,
including trends in setting of death, can be found in the
Mortality section of this document.
System indicators for palliative care are currently being
developed at the provincial level. Results for a number
of the draft indicators are presented in the Acute
Inpatient section below.
HOSPITAL-BASED SERVICES - ACUTE INPATIENT
Patients receiving palliative and end-of-life care
often access services within hospital-based
settings, including emergency departments, acute
inpatient, and complex continuing care. While
there are no officially designated palliative care
units in the South East LHIN, each hospital may
informally designate beds for the purpose of
providing palliative care.
A summary of overall utilization within acute
inpatient settings is provided below.
Acute inpatient discharges were classified as being
related to palliative care if the hospitalization record
contained an International Statistical Classification of
Diseases (ICD)-10-CA diagnosis code of Z51.5 (Palliative
care) in any diagnosis field (e.g. most responsible,
secondary, pre-admit comorbidity, etc.), or if the main
patient service was noted to be palliative care (058). As
previously noted, not all patients receiving palliative
care may be coded as such on their hospitalization
record. As a result, this information likely
underestimates the number of people receiving
palliative care that are also accessing acute inpatient
services.
Overall Acute Inpatient Utilization and
Trends Over Time
• The number of palliative care-related
hospitalizations for South East LHIN residents has
steadily increased over time, with an average
annual growth rate of 4% between 2008/09 and
2014/15.

77
• The number of palliative-related hospitalizations
has increased in all Health Links, with Rural
Hastings and Thousand Islands having the highest
utilization rates in 2014/15 (about 5.5 palliative
care discharges per 1,000 population in each of
these Health Links) (Figure 38).
• Nearly all hospitalizations related to palliative
care were for those over 50 years of age. Looking
at hospitalization rates within this group, the rate
of hospitalizations increased with increasing age
(from 1.9 hospitalizations per 1,000 population
aged 50-54 to 44.0 per 1,000 population aged 85+
in 2014/15). Rates in each age group increased
minimally between 2008/09 and 2014/15, with
the exception of a more notable increase among
those 85+. These relatively minor increases in
age-specific rates suggests that overall increases
in the number of hospitalizations are due in part
to population aging.
• Given the aging population within the LHIN, the
number of palliative care-related hospitalizations
is expected to grow in the coming years. If the
status quo remains (i.e., Trends in acute care
utilization and the need for palliative services by
age group remains constant), the number of
hospitalizations related to palliative care is
projected to increase by 41% by 2026/27. This
would result in approximately 900 additional
hospitalizations for South East LHIN residents.
• By Health Link, the highest rate of growth for
palliative-related hospitalizations is projected to
be in Salmon River (a 55% increase by 2026/27,
resulting in about 70 additional hospitalizations),
and the highest absolute increase in the number
of hospitalizations will be in Quinte (about 240
additional hospitalizations by 2026/27, a 38%
increase).
Time Spent in Acute Inpatient Beds and
ALC Days
• In 2014/15, patients with a palliative care-related
hospitalization on average stayed in hospital for
13.4 days. This rate was slightly lower than the
provincial average of 14.9 days. Compared to all
hospital discharges in the South East LHIN,
patients with a palliative care-related
hospitalization had on average longer hospital
stays (average LOS for all discharges was 6.1
days).
• The percentage of palliative care-related inpatient
days where the patient was waiting for ALC in the
South East LHIN was fourth highest among all
LHINS (26.5%, versus 20.9% provincially). By
Health Link, this rate was highest in Quinte and
Rideau Tay (both about 40%). Compared to all
hospital discharges overall, there was a higher
percentage of ALC days for patients with a
palliative care-related hospitalization (% ALC was
14.2% for all discharges).
Figure 38: Actual and projected number of acute inpatient hospitalizations related to palliative care by Health Link, South East LHIN, fiscal years 2008/09-2014/15 (actual) and 2018/19, 2021/22, and 2026/27 (projected).
Notes: Crude projections are based on age- and sex-specific utilization rates for fiscal years 2013/14-2014/15 and projected population growth. These crude projections assume that all factors related to acute care utilization, need for palliative care by age group, and diagnosis coding remain constant. Projected values rounded to nearest hundred.

78
Deaths in Hospital and Discharge
Destination
• The majority (~60%) of South East LHIN residents
with a palliative-related acute inpatient
hospitalization in 2014/15 ended up dying in
hospital. Those who were discharged were either
transferred to another facility (e.g., complex
continuing care, long-term care) or discharged
home, with each of these categories accounting
for about 20% of hospitalizations.
• The proportion of palliative care-related
hospitalizations where the patient died in hospital
was highest in the Salmon River Health Link (72%
of hospitalizations in 2014/15) and lowest in the
Thousand Islands Health Link (41% of
hospitalizations)
Palliative Care Hospital Discharges with
the Status ‘Home with Support’
Patients who are identified as needing palliative
care while in hospital should be offered support
in the community so they are able to sustain good
quality of life and prevent/delay readmission and
institutionalization. ‘Home with support’ can be
interpreted to mean anything from Meals on
Wheels to comprehensive home care.
• Between 2009/10 and 2013/14 in the South East
LHIN, there was variable but generally increasing
rates of palliative care-related discharges to home
with the discharge status ‘home with support’
(from 76% in 2009/10 to 81% in 2013/14). This
was also true for Ontario as a whole (from 65% in
2009/10 to 79% in 2013/14).
• By Health Link, a lower proportion of patients
discharged home to Salmon River and Rideau-Tay
were noted to be receiving support (60% and
68%, respectively). In contrast, 90% of those
discharged home to the Thousands Islands were
discharged with support.
• In addition to variation in practices for identifying
need for community-based support services,
variation in this indicator between areas may also
result due to differences in hospital coding
practices.
Palliative Care Patients Discharged from
Hospital and Readmitted within 30 Days
Readmission to an acute care setting may indicate
poor discharge planning and follow-up. As well,
readmissions can occur when a patient’s
symptoms are not well managed, or if they do not
want to die at home. Further investigation is
required to better understand reasons for
hospital readmission.
• In the South East LHIN, 30 day hospital
readmission rates for palliative care patients were
fairly consistent between 2009/10 and 2013/14
(22% in 2009/10 and 20% in 2013/14) and were
similar to the provincial rate, which has declined
over time (from 22% to 18% in the same time
period).
Palliative Care Patients Discharged from
Hospital who Visited the ED within 30
Days
Visiting the ED soon after being discharged from
hospital setting may indicate poor quality of care
coordination. While not all ED visits may be
avoided, palliative care may be effective in
reducing ED visits.
• Between 2009 and 2013, there was a gradual
increase in the rate of unscheduled ED visits for
palliative care patients within 30 days of
discharge in the South East LHIN (from 32% in
2009 to 36% in 2013). South East LHIN rates were
higher than the provincial rate, which only varied
slightly over the same time period (was 28% in
both 2009 and 2013).

79
COMMUNITY-BASED SERVICES
Hospice Services
Information on South East LHIN hospice services can be
found in the Community Support Services section of
this document.
Home Care (CCAC) Services
This information reflects CCAC clients who were noted
to be receiving end of life services (service recipient
code = 95). These services are intended to provide
complex support to alleviate symptoms and reduce
pain for clients in the last stages of their illness.
• In fiscal year 2014/15, there were about 950
South East LHIN clients receiving end-of-life home
care services. These clients received about 96,600
hours of service through approximately 70,300
service encounters during this time period.
• Nearly all (98%) South East LHIN clients receiving
end-of-life home care in 2014/15 were 65+ years
of age. About half were aged 75+, and 22% were
85+.
• The number of end-of-life home care clients,
service encounters, and hours of service have
increased slightly over the last three years (a 4%,
2%, and 1% increase, respectively).
• Utilization of end-of-life home care services
among those 65+ years of age varied across the
LHIN in fiscal year 2014/15, with the highest
utilization in the Rural Hastings and Quinte Health
Links (Figure 39). This was true for both client and
service volume rates. Utilization rates were
lowest in the Rideau-Tay, Rural Kingston, Salmon
River, and Thousand Islands Health Links.
• Compared to other LHINs, the South East LHIN
has some of the lowest utilization rates of end-of-
life home care services. Among those 65+ in the
South East LHIN, there were 7.3 clients per 1,000
population using end-of-life home care services,
compared to 9.6 per 1,000 for the province as a
whole (Figure 39). Looking at hours of service,
there were 753 hours of end-of-life home care
services provided per 1,000 South East LHIN
residents 65+ years of age, which was the lowest
rate of all the LHINs. Provincially, there were
1,064 hours of service per 1,000 population.
Variation in modes of home care service delivery
and availability of other end-of-life services need
to be considered when comparing rates of service
hours between areas.
Figure 39: Utilization rates of end-of-life home care services by Health Link of residence, South East LHIN clients aged 65+, fiscal year 2014/15.
ClientsService
Encounters
Hours of
ServiceRural Hastings 15.0 1,071.5 1,717.4
Quinte 9.7 863.1 1,081.7
Salmon River 3.8 239.5 421.3
Rural Kingston 5.2 295.7 457.8
Kingston 6.4 608.5 698.8
Rideau-Tay 4.1 209.9 331.0
Thousand Islands 4.9 229.2 320.4
South East LHIN 7.3 572.6 752.7
Ontario 9.6 792.1 1,063.7
Rate per 1,000 population aged 65+Health Link

80
HEALTH LINKS
OVERVIEW OF THE HEALTH LINKS INITIATIVE
Health Links were established as a key commitment in
the Ontario Ministry of Health and Long Term Care’s
(MOHLTC) Patients First: Action Plan for Health Care to
improve the delivery and coordination of care,
enhance the experience, and improve the quality of
care at lower cost for patients with complex health and
social needs. These goals will be achieved through a
mutually beneficial and accountable collaboration with
providers across the continuum of care.
The MOHLTC identified that 5% of patients account for
two-thirds of health care costs (called high cost users).
These are most often patients with multiple, complex
conditions who may benefit from the care
coordination provided by Health Links initiative.
In the South East LHIN, Health Links are collaborative
networks that include a diverse group of health and
social services organizations, where providers come
together to meet the Health Link objectives of
improved care coordination and transitions between
services for patients with complex needs.
In the South East LHIN, there are seven Health Links
that jointly cover the entire region. A map of the Health
Links are provided on Page 7. Each Health Link in the
South East LHIN has a primary care lead organization.
Five of the Health Links launched in 2013 and two
began operations in 2014.
For more information on the Health Links initiative, see
the South East LHIN website.
DESCRIBING THE HEALTH LINKS TARGET POPULATION
Currently, all levels (provincial, regional, and local) use
a standard definition developed by the MOHLTC and
the Measurement and Performance Sub-Committee of
the Health Links Advisory Table. This definition
identifies the target population as those with four or
more high needs and/or complex conditions from a
defined list of conditions. This definition takes into
account the following:
• The number of people identified as the target
population is close to 5% of the Ontario
population
• The target population overlaps substantially with
high cost users recognizing that:
o Not all high cost users are high needs patients
in the community (e.g., some patients
received inpatient care for the entire fiscal
year)
o Not all high needs/complex patients are
currently high cost users (patients with
multiple physician or ED visits, patients
receiving frequent home care services)
Consideration of socio-economic factors and a focus
on individuals living with mental health and addictions,
hospice palliative patients, and the frail elderly is also
strongly encouraged as part of target population
identification.
Various methods for identifying the Health Links target
population have been developed based on available
data and how the target population information will be
used. The MOHLTC and South East LHIN use this
information to help inform planning purposes. Each
individual Health Link can also apply further criteria
and clinical judgment to help identify and prioritize
their Health Link patients.

81
Further refinement of definitions
and methods to approaches used
at each level will be made to
account for new data sources,
tools, and any changes in the focus
of the Health Links initiative.
The information presented below
summarizes analyses conducted at
the provincial and regional levels;
however, it is important to note
that analytic work is ongoing
within Health Link to characterize
their patient population and
monitor and evaluate patient
outcomes.
MOHLTC Analysis
The target population of those with documentation of
four or more chronic and/or high cost conditions is
identified by the MOHLTC using information on
encounters in a given year from a variety of health care
sectors, including acute care, day surgery, emergency,
ambulatory oncology, ambulatory dialysis, inpatient
mental health, inpatient rehabilitation, complex
continuing care (CCC), home care, long-term care (LTC),
or physician services.
• The MOHLTC identified that the size of the South
East LHIN Health Links target population was
about 30,000, based on health system utilization
in fiscal year 2011/12.
• A higher percentage of the South East LHIN
population were identified as being part of the
target population compared to the province
overall (7.2% versus 5.9%, respectively). This is
likely due in part to the relatively older population
in the South East LHIN, as those in older age
groups were more likely to be identified as part of
the target population.
• Among the South East LHIN target population,
about half were noted to also be high cost users
of the system.
• By Health Link, the largest target populations
were in the Kingston and Quinte Health Links
(8,360 and 7,815, respectively) (Figure 40). The
target populations in the Rural Hastings and
Salmon River Health Links accounted for a
relatively large proportion of their overall patient
population (i.e., those accessing any type of
health service in that year - both 8.1%).
South East LHIN Analysis
The South East LHIN analyses conducted to date have
identified the target population based on
documentation of four or more chronic and/or high
cost conditions in a given year based on acute inpatient
discharges and/or emergency department visits only.
This more focused approach was used to align with the
current regional focus on patients with complex needs
who have high utilization of hospital services, or who
are at risk of hospitalization. The resulting target
Figure 40: Number and relative size of the Health Links target population by South East LHIN Health Link, based on the MOHLTC analysis of utilization in fiscal year 2011/12.

82
population sizes presented below are lower than those
identified by the MOHLTC.
• In fiscal year 2014/15, there were about 7,000
target population patients identified across the
South East LHIN Health Links using acute inpatient
discharges and/or emergency department visit
data. This corresponds to about 1.4% of the
population across the Health Links. The
proportion of the population identified in each
Health Link varied, from 1.0% in Rural Kingston to
1.7% in both Rural Hastings and Thousand Islands.
• Of those identified as having complex needs, the
majority (73%) were 65+ years of age and 48%
were female (Figure 41). Across the South East
LHIN Health Links, patients with complex needs
had an average of 4.7 emergency department
visits or hospitalizations in the one-year period.
• Given the aging population in the South East LHIN
and the fact that complex needs patients are
generally older, the size of this population and in
turn the amount of services and care coordination
required for this population will increase in the
coming years if all factors remain constant.
• The most common diagnoses associated with the
patients with complex needs were diabetes (8%
of patients), hypertension (8%), cardiac
arrhythmias (6%), pneumonia (6%), ischaemic
heart disease (6%), renal failure (6%), chronic
obstructive pulmonary disease (5%), and
congestive heart failure (5%).
Figure 41: Number in Health Links target population by age group and sex, South East LHIN Health Links, based on the South East LHIN analysis of utilization in fiscal year 2014/15.

83
HEALTH HUMAN
RESOURCES
Describing and quantifying health human
resources is essential for understanding both
current and potential future areas of need with
respect to this workforce.
Physicians
Information on physicians was obtained from the
Ontario Physician Human Resources Data Centre
(OPHRDC). Physicians were classified geographically
based on the location of their primary practice. Further
details can be found here.
OVERALL TRENDS BY SPECIALTY
• Compared to Ontario as a whole, the number of
physicians per capita in calendar year 2013 was
actually higher in the South East LHIN for most
specialties, particularly those that are less
specialized (Figure 42).
• Examining the age of physicians, particularly for
the older age groups that are closer to retirement
age, can provide some indication of where there
may be physician staffing needs in the coming
years. More than 10% of physicians were 65 years
of age or older for a notable number of
specialties, including family physicians,
psychiatrists, diagnostic radiologists and
cardiologists. Even more of the specialties had a
substantial portion of physicians 55 to 64 years of
age (Figure 42).
• Between 2010 and 2013, there was an increase in
the number of physicians for certain specialties
(with the greatest increase for family medicine,
internal medicine, psychiatry, emergency
medicine, and anesthesiology – all 8 or more),
and a decrease for others (greatest decrease for
the Family/Emergency Medicine combination (5
fewer) and General Pathology (4 fewer)). Small
absolute increases or decreases are also
important to consider for specialties with a low
number of physicians
• With the exception of anesthesiology and internal
medicine, the number of physicians entering the
health care system were typically much lower
than those who were departing.
• While the age of retirement varies depending on
the specialty, results are pointing to a reduction in
the number of physicians for many specialties in
the next 10 to 15 years if the current trends are
maintained.
FAMILY PHYSICIANS
Family Physicians Per Capita
• Relative to the province overall, the South East
LHIN has more family physicians per population,
with over 100 physicians per 100,000 population
in the South East LHIN compared to 86 for Ontario
in 2013 (Figure 42).
• Within the LHIN, there is substantial variation in
the family physician rate across the Health Link
geographies (Figure 43). Rates were highest in the
Kingston Health Link (just under 150 physicians
per 100,000 population in 2013) and lowest in the
Rural Hastings and Rural Kingston Health Links
(both just under 50 physicians per 100,000
population).

84
Physicians
All Ages
# # % # % SELHIN Ontario
Family Medicine 498 134 27% 75 15% 22 101.0 86.3
Psychiatry 90 30 33% 18 20% 8 18.2 15.2
Anesthesiology 57 13 23% 4 7% 7 11.6 9.2
Diagnostic Radiology 37 9 24% 4 11% 1 7.5 7.1
F.M./Emergency Medicine 35 4 11% 1 3% -5 7.1 7.0
Emergency Medicine 31 9 29% 1 3% 8 6.3 2.2
Cardiology 29 8 28% 7 24% 2 5.9 4.4
Internal Medicine 28 5 18% 2 7% 10 5.7 5.9
Obstetrics & Gynecology 27 4 15% 3 11% -2 5.5 5.4
Orthopedic Surgery 25 5 20% 1 4% 3 5.1 3.8
General Surgery 24 7 29% 0 0% 0 4.9 4.6
Ophthalmology 20 3 15% 1 5% -1 4.1 3.2
Anatomical Pathology 15 3 20% 0 0% 4 3.0 2.9
Medical Oncology 15 3 20% 1 7% 0 3.0 1.7
Urology 14 3 21% 2 14% 2 2.8 1.8
Gastroenterology 13 4 31% 2 15% 1 2.6 2.3
Neurology 12 1 8% 3 25% 2 2.4 2.4
Radiation Oncology 12 2 17% 1 8% 1 2.4 1.5
Respirology 10 3 30% 2 20% -3 2.0 1.9
Nephrology 9 1 11% 0 0% 1 1.8 1.7
Otolaryngology - Head & Neck Surgery 9 3 33% 3 33% 1 1.8 1.9
Physical Medicine & Rehab. 8 3 38% 1 13% -1 1.6 1.4
Hematology 7 4 57% 0 0% -1 1.4 1.3
Rheumatology 7 1 14% 1 14% 1 1.4 1.3
Critical Care Medicine 6 0 0% 0 0% 2 1.2 1.2
General Pathology 6 1 17% 1 17% -4 1.2 0.7
Neurosurgery 6 3 50% 1 17% 3 1.2 0.7
Cardiac Surgery 4 0 0% 0 0% 0 0.8 0.7
Infectious Diseases 4 1 25% 0 0% 0 0.8 0.9
Nuclear Medicine 4 1 25% 0 0% 0 0.8 0.6
Plastic Surgery 4 2 50% 0 0% 0 0.8 1.6
Public Health & Preventive Medicine 4 3 75% 0 0% 1 0.8 0.7
Clinical Immunology & Allergy 3 0 0% 0 0% 0 0.6 0.5
Endocrinology & Metabolism 3 1 33% 0 0% 0 0.6 1.5
Geriatric Medicine 3 2 67% 0 0% 0 0.6 0.9
Hematological Pathology 3 0 0% 1 33% 1 0.6 0.2
Medical Genetics 3 0 0% 0 0% -1 0.6 0.3
Dermatology 2 0 0% 1 50% 0 0.4 1.5
Gynecologic Oncology 2 1 50% 0 0% 0 0.4 0.2
Vascular Surgery 2 2 100% 0 0% 0 0.4 0.5
Adolescent Medicine 1 0 0% 1 100% 0 0.2 0.0
Forensic Pathology 1 0 0% 0 0% 1 0.2 0.1
Medical Microbiology 1 1 100% 0 0% 0 0.2 0.3
Neuropathology 1 0 0% 0 0% 0 0.2 0.1
Psychiatry - Forensic 1 0 0% 0 0% 1 0.2 0.0
Thoracic Surgery 1 1 100% 0 0% 0 0.2 0.4
Pediatrics 28 7 25% 4 14% 3 5.7 6.8
Gastroenterology - Pediatric 2 0 0% 0 0% 1 0.4 0.2
Cardiology - Pediatric 1 1 100% 0 0% 0 0.2 0.3
Neurology - Pediatric 1 1 100% 0 0% 0 0.2 0.2
Pediatric Surgery 1 1 100% 0 0% 0 0.2 0.1
Difference in
# physicians
2010-2013
Physicians
55-64 years
Physicians
65+ years
Physicians per
100,000 populationSpeciality
Figure 42: Number of physicians, distribution by age, change in number from 2010, and rate per population for each physician specialty, South East LHIN, 2013.

85
Areas of High Physician Need
To help improve access to family physicians in
communities that have a high need for their services,
the Ministry of Health and Long-Term Care (MOHLTC)
uses a Managed Entry process to identify current areas
of high physician need that could be supported by new
family physicians.
This list of current areas of high physician need is
reviewed and updated on an ongoing basis by the
MOHLTC, in collaboration with the LHINs. Currently,
several factors are considered when identifying high
needs communities:
• The Rurality Index for Ontario (RIO) score
• The family physician to population ratio
• Local demographics, socioeconomic status,
population health needs, and access
considerations
Table 9 shows the municipalities in the South East LHIN
that have been identified as current areas of high
family physician need.
New criteria have been developed to help guide the
identification and prioritization of areas of high
physician need. Recommended considerations for
identifying high need areas include:
• Areas where patients have to travel at least 30
minutes and/or 30 kilometres to access a primary
care physician
• Areas with a population of 30,000 or less
• Areas with a small number of primary care
physicians, and/or physicians with large patient
rosters, and/or physicians who contribute to
emergency department or after hours coverage
• Patient demographics and socio-economic
factors, including areas with a high numbers of
unattached patients, medically complex patients,
or seniors
Table 9: Current areas of high family physician need in the South East LHIN.
Figure 43: Rate of family physicians per 100,000 population by fiscal year and Health Link, South East LHIN, calendar years 2009 to 2013.

86
Recommendations on prioritizing areas of high
physician need include using the following categories:
• Critical need – Areas with an urgent and
unexpected need due to physician death or
unexpected departure, which immediately
impedes patient’s access to primary care.
• Urgent need –Areas where a significant number of
patients currently do not have access to a
physician or will not have access within six
months.
• Future need – Areas with declared and/or
anticipated retirements (e.g. a high percentage of
physicians who are aged 70+).
Some additional considerations for future recruitment
of family physicians noted by the South
East/Champlain Regional Advisor for
HealthForceOntario include:
• Family physicians are one of the specialties that
tend to practice longer than many others, though
anecdotally it seems that the physicians of the
“baby boomer” generation (i.e., those currently
between 50 and 70 years of age) are retiring at
younger ages compared to their predecessors
• There may be future recruitment challenges in
the more rural areas of the LHIN due to the
anticipated retirement of solo, fee-for-service
physicians given that new physicians are typically
not as interested in starting or maintaining a solo
practice compared to the past
Allied Health Professionals
Information on allied health professionals was
obtained from the Health Professions Database
(HPDB), 2013 Submission. The HPDB captures the
number of ‘active’ health professionals who are
registered by their respective regulatory College to
practice in their profession in full or any one capacity
(clinical, research, teaching health promotion, etc.).
Members may or may not be working in the profession.
This data does not include members who hold
educational registrations. Health professionals were
classified geographically based on the location of the
first practice site listed in the HPDB. Further details can
be found here.
• While the number of allied health professionals
approaching retirement age appears to be
relatively low across almost all professions in
2013, the proportion of professionals who are
between 55 to 64 years of age was markedly high
in a few cases (Figure 44). This could develop into
a human resource capacity issue in the next 10 to
15 years if the rate of professionals entering the
system is lower than the rate of those retiring.
• There were a number of professions with
substantially lower rates per population in the
South East LHIN compared to the province as a
whole (Figure 44). The lowest rates were
observed for dentists, with a rate of 5 per 100,000
population in the South East LHIN compared to
just under 70 per 100,000 for Ontario overall in
2013.
• Similar to the trend observed for physicians, the
rate of allied health professionals per population
by Health Link was lowest for most professions in
Rural Kingston and Rural Hastings, and highest in
Kingston, Quinte, and Rideau-Tay (Figure 45).

87
Professionals
All Ages
# # % # % SELHIN Ontario
Audiologists 16 1 6% 0 0% 0 3.3 4.8
Chiropodists 11 1 9% 0 0% 1 2.2 4.3
Chiropractors 108 17 16% 8 7% 10 21.9 33.3
Dental Hygienists 388 31 8% 3 1% 22 78.8 97.9
Dental Technologists 15 5 33% 2 13% 3 3.0 3.8
Dentists 25 4 16% 2 8% 3 5.1 66.8
Denturists 19 4 21% 0 0% 1 3.9 4.1
Dietitians 121 17 14% 3 2% 14 24.6 26.2
Massage Therapists 258 16 6% 4 2% 258 52.4 74.2
Medical Laboratory Technologists 269 74 28% 6 2% -19 54.6 47.3
Medical Radiation Technologists 259 61 24% 6 2% 43 52.6 49.1
Midwives 17 0 0% 0 0% 0 3.5 4.5
Nurse Practitioners 127 19 15% 2 2% 38 25.8 15.9
Occupational Therapists 199 29 15% 5 3% 23 40.4 36.1
Opticians 66 15 23% 6 9% 8 13.4 18.8
Optometrists 72 10 14% 6 8% 13 14.6 16.0
Pharmacists 400 78 20% 35 9% 38 81.3 93.2
Pharmacy Technicians 54 3 6% 0 0% 54 11.0 13.5
Physiotherapists 268 42 16% 8 3% 9 54.4 50.9
Psychologists 163 47 29% 29 18% 12 33.1 27.2
Registered Nurses 4,562 1,113 24% 243 5% 249 926.8 709.5
Registered Practical Nurses 2,067 385 19% 63 3% 282 419.9 277.4
Respiratory Therapists 102 13 13% 0 0% 12 20.7 23.1
Speech-Language Pathologists 81 17 21% 1 1% 6 16.5 22.2
Allied Health Professions
Professionals
55-64 years
Professionals
65+ years
Professionals per
100,000 population
Difference in #
Professionals
2010-2013
Figure 44: Number of allied health professionals, distribution by age, change in number from 2010, and rate per population for each allied health profession, South East LHIN, 2013.

88
Rural
HastingsQuinte
Salmon
RiverKingston
Rural
Kingston
Rideau-
Tay
Thousand
Islands
South East
LHIN
Audiologists 1 3 2 9 0 1 0 16
Chiropodists 0 5 0 4 0 1 1 11
Chiropractors 11 32 5 30 2 14 14 108
Dental Hygienists 26 123 20 128 9 26 56 388
Dental Technologists 0 4 0 8 0 3 0 15
Dentists 0 5 2 13 0 1 4 25
Denturists 2 6 0 7 0 1 3 19
Dietitians 5 27 7 51 1 16 14 121
Massage Therapists 20 67 9 84 9 33 36 258
Med Laboratory Technologists 7 70 9 146 0 13 24 269
Med Radiation Technologists 11 64 8 145 0 13 18 259
Midwives 0 5 0 8 1 0 3 17
Nurse Practitioners 13 20 2 60 4 11 17 127
Occupational Therapists 1 46 2 133 1 4 12 199
Opticians 1 25 2 34 0 0 4 66
Optometrists 4 25 4 22 1 8 8 72
Pharmacists 26 96 21 170 13 30 44 400
Pharmacy Technicians 4 26 3 17 0 3 1 54
Physiotherapists 8 66 10 149 0 16 19 268
Psychologists 3 17 1 121 2 4 15 163
Registered Nurses 189 1,004 107 2,376 29 307 550 4,562
Registered Practical Nurses 116 469 96 830 14 197 345 2,067
Respiratory Therapists 0 25 1 67 1 3 5 102
Speech-Language Pathologists 0 21 2 43 0 6 9 81
Allied Health Professions
Rate per 100,000 Population
Figure 45: Rate of allied health professionals per 100,000 population by profession and Health Link, South East LHIN, 2013.

89
FUNDING
The South East LHIN allocates funds to Health
Service Providers across the region to support
services in hospitals, the community, and in long
term care. Each Health Service Provider (HSP)
enters into a Service Accountability Agreement
with the LHIN, whose role is to manage and
monitor service delivery and its efficiency. In
addition to LHIN funding, some HSPs do
community fundraising to expand their scope and
volume of services.
Overview of Health System Funding Reform
WHY CHANGE IS NECESS ARY
Ontario’s health care system is facing significant
challenges over the next few years:
• Fiscal Challenge: Historic levels of investment
growth are not seen to be sustainable
• Demographic Challenge: The cost of care for a
senior is 3x higher than for the average person.
Changing demographics will result in a higher cost
to the system
• Complex Health Challenge: A small number of
patients use a disproportionate amount of
resources .Making better use of our health care
resources so people get the most appropriate
care.
• Unhealthy Lifestyle Challenge: Unhealthy eating,
lack of activity and smoking levels may lead to
increased chronic disease
SHIFTING FROM THE HISTORIC FUNDING APPROACH
Previously, Ontario used a global provider-focused
funding model. Hospitals, on average, received about
75-90% of their funding from global budgets. The
majority of the funding was in the form of base
annualized funding and new incremental funding, and
the remaining funding was acquired from other
sources (i.e. preferred accommodation, alternative
revenue, etc.).
Ontario is moving from this provider-focused model to
one that revolves around the patient. Under this new
model, hospitals, Community Care Access Centres, and
long-term care homes are compensated based on:
• Best available evidence and best practices
• Needs of the population served
• Services delivered
• Number of patients
This Health System Funding Reform was initiated by
Ontario's Action Plan for Health Care in 2012 and is
enabled by The Excellent Care for All Act (ECFAA),
which sets out principles and levers to embed a culture
of quality and accountability in the delivery of patient-
centred health care services.
COMPONENTS OF HEALTH SYSTEM FUNDING REFORM
There are two key components to HSFR:
• Organizational-level funding, which will comprise
approximately 40 per cent of hospital funding.
Funding is allocated to hospitals using the Health
Based Allocation Model (HBAM).
• Quality-Based Procedures, which will comprise
approximately 30 per cent of hospital funding.
Funding is allocated to specific procedures based
on a "price X volume" approach. This involves
providing evidence-based allocations to targeted

90
clinical groups. The price is structured to provide
an incentive and adequately reimburse providers
for delivering high-quality care.
As of 2015/2016, HSFR will comprise 70 per cent of the
funding envelope provided to hospitals with the
remaining 30 per cent based on global funding.
Health Based Allocation Model (HBAM)
HBAM is both a funding allocation methodology and a
management tool for strategic decision-making. The
primary objective of HBAM is to enable government to
equitably allocate funding to the LHINs for local health
services. Currently, HBAM is designed to allocate
funding for the hospital and home care sectors.
HBAM estimates future expenses based on past
service levels and efficiency, as well as population and
health information (e.g. age, gender, population
growth rates, diagnosis and procedures).
Key things to note about HBAM:
• HBAM is a ‘pie-sharing’ model where the pie is
the sum of all expected expenses in the province.
• Approximately 37% of total hospital base funding
is distributed based on each HSP’s percentage of
the pie (which was $5.15B in fiscal year 2015/16).
• An HSP’s share of the pie is impacted by:
o An HSP’s own expected results, including
year-over-year changes in expected results;
and
o The expected results of all other HSPs within
each of the HBAM Care Types.
Quality-Based Procedures (QBPs)
QBPs are clusters of patients with clinically related
diagnoses/ treatments and functional need that are
identified by an evidence-based framework. QBPs
provide opportunity for:
• Aligning incentives to facilitate adoption of best
clinical practices
• Appropriately reducing variation in costs and
practice while improving outcomes
• Using set prices and volumes
QBP Funding
Hospitals are funded for QBPs on a Price X Volume X
Acuity approach:
• At the individual hospital level, QBPs were carved
out from hospital base funding at the time of QBP
introduction.
• At the provincial level, the sum of all HSP QBP
carve outs (from QBP Introduction) +/- Volumes &
Pricing results in the QBP funding pot
• The HSP’s QBP funding allocation is equal to the
Provincial Price X Volume X the HSP’s Acuity Level
QBP Roadmap
As QBPs are developed across the continuum of care,
different approaches will be required for addressing
the varying needs of patient/ client populations:
• Acute Inpatient: Initial QBP focus is on acute-
impatient episodes of care.
• Outpatient Clinics & Emergency Departments
(ED): Incorporating ED care that incents
appropriate quality care. Both ED and Outpatient
clinics serve as key transition points along the
continuum of care.
• Transition: Work is underway to develop QBPs for
the post-acute phase, including the short stay
population.
• Community: The future goal is to define QBPs for
clients requiring assistance with their activities of
daily living (i.e. long stay population).

91
QBP Performance
A detailed overview of QBP performance was
compiled jointly by LHIN staff across the province. The
report includes both a provincial context and LHIN-
specific results. The LHIN-specific results for the South
East LHIN are presented in Figures 46a and 46b.
Highlights from the provincial overview include:
• The South East LHIN had a much lower acute
length of stay in comparison to the expected
length of stay for most QBPs
• The South East LHIN demonstrated a relatively
high percentage of discharges to Home Care across
a range of QBPs – for example 27.6% of Hip
Fracture QBP cases were discharged to Home Care
(second among LHINs and compared to a
provincial average of 15.9%). However, the
readmission rate for Hip Fractures was highest
among the LHINs at 9.7% (compared to the
provincial average of 7.3%).
• In contrast to most QBPs, the South East LHIN had
the lowest percentage of non-cardiac vascular –
aortic aneurysm patients discharged to home care
in 2013/14 (at 3.8% - compared to the provincial
rate of 27%)
• The highest average weight (HBAM inpatient
grouper (HIG) weights are indicative of resource
requirements for a case) were for non-cardiac
vascular aortic aneurysm cases (average HIG
weight of 3.67 in 2013/14) followed by
hemorrhagic stroke cases (2.83).
• The South East LHIN had the lowest readmission
rate in 2013/14 for COPD QBP cases at 17.5% -
compared to a provincial rate of 19.6%. The
average acute LOS was 5.9 days – consistently
lower than the expected length of stay.
• The South East LHIN had the lowest average acute
length of stay for pneumonia cases in 2013/14 at
5.4 days (other LHINs average acute length of stay
ranged from 5.6 to 7.0 days).
• Best practice for acute inpatient stroke care
includes admission to an acute stroke unit where
specialized and dedicated care results in better
patient outcomes. It is recommended that to
accrue the benefits of care in an acute stroke unit
requires a minimum of 165 (ischemic) stroke
patients per year. In the eastern portion of the
LHIN, consolidated stroke care at Brockville
General is under development to improve patient
outcomes. Stroke care continues to strive for best
practice across the South East.
• The Tonsillectomy QBP includes both day surgery
and inpatient cases. The South East LHIN had the
highest proportion of day surgery cases at 97.3% in
2013/14 (by comparison the lowest LHIN had
41.4% of Tonsillectomy QBPs as day surgery cases)
HSFR FUNDING IMPLICATIONS
• Comparisons of healthcare spending indicate the
South East LHIN is a high spender when compared
to other LHINs, and actual costs exceeds expected
costs.
• HSFR will increasingly impact the hospitals in the
South East LHIN. This year (2015/16), hospitals in
the South East LHIN experienced a $16.8 million
reduction in funding through the application of
the HBAM as a consequence of the hospitals,
collectively, performing at a higher than expected
cost. Hospitals expect that the continued
application of HBAM will further reduce revenues
in the future.
• Achieving critical mass and bringing actual costs in
line with expected will be necessary in order to
stabilize South East LHIN HBAM share.
• The hospitals in the South East LHIN have a
significant opportunity to improve service delivery
that will result in improved quality, access, patient
experience, and will lower costs.

92
Figure46a: South East LHIN QBP volumes and performance measures for non-elective procedures by fiscal year, 2011/12 to 2013/14.

93
Figure 46b: South East LHIN QBP volumes and performance measures for elective procedures by fiscal year, 2011/12 to 2013/14.

94
• Hospitals in the South East LHIN will
continue to face increasing pressures:
the hospitals, collectively, within the
South East LHIN are inefficient when
compared to provincial peers - this will
result in a reduction in revenue through
HBAM; hospitals, collectively, will face
inflationary pressures on cost and
increasing demand through
demographic changes; and, hospitals in
the short-term will still need to balance
their budgets, take efforts to improve
their individual efficiency and make
investments to build capacity to invest
in the future together.
Overall Funding by Sector
• Hospitals received 59.2% of all LHIN-
allocated funds in fiscal year 2015/16 –
(Figure 47 presents estimated totals for
2015/16).This is a decrease from 65.7% in
2011/12.
o This was in part a result of a transfer
of funding for Addiction and Mental
Health services to community agencies
in 2013/14
o More recent changes in hospital funding are
largely a result of Health System Funding
Reform and the relative share of funding
allocation to South East LHIN hospitals given
the volume and relative resource needs for
patients.
• Funding increased for all community sectors
(Figure 48). The highest growth in funding
occurred in the Addiction and Mental Health
sector –funding increased by 78% between
2011/12 and 2015/16 (again the transfer of
funding from hospitals into the community
accounts for the bulk of this increase) followed by
Acquired Brain Injury (ABI) Agencies (42%), and
Community Health Centres (30%).
• LHIN funding increased by 3% over the past five
years to a total of $1,102.5 million in 2015/16.
Funding to community agencies increased by 35%
over this time period.
Figure 47: Distribution (in Millions and percentage) of South East LHIN funding by sector, fiscal year 2015/16.
Figure 48: Change in funding over time (relative to fiscal year 2011/12) by sector, South East LHIN, 2011/12 to 2015/16.

95
HEALTH SYSTEM
PERFORMANCE
In the South East LHIN, the performance of our health
system is monitored using various performance
indicators. Indicators are developed and included in
the Accountability Agreements detailing the
commitments of the LHIN and our Health Service
Providers. The LHIN also has an Accountability
Agreement with the Ministry of Health and Long-Term
Care (the Ministry-LHIN Accountability Agreement
(MLAA)) with a range of indicators designed to track
how well various elements of our local health system
function. Indicators across these agreements can be
used to compare the performance of our system or
individual Health Service Providers (i.e. a hospital or a
community service provider) to other areas in the
province. In most cases there is a linkage between
indicators for individual programs and higher level
indicators to monitor or evaluate performance at
sector or system levels (i.e., across sectors).
The indicators in the Ministry-LHIN Accountability
Agreement (MLAA) are the ‘highest level’ of indicators
intended to assess priority areas or system level
performance. There are 14 performance indicators.
Province-wide targets are set for each of the
performance indicators and are used to assess
progress across LHINs toward desired levels of health
system performance and outcomes. Indicators are
reported on a regular basis to enable monitoring of
performance over time. This is important to ensure
that any performance issues can be identified, and
strategies to address these issues can be implemented
in a timely way.
MLAA Indicator Results
Data for MLAA indicators was obtained from the
MOHLTC (quarterly MLAA supplementary reports),
Access to Care Analytics (CCO) (monthly and quarterly
data), and Cardiac Care Network. The definitions and
methodology for calculating the MLAA indicators can
be found here.
PERFORMANCE INDICATORS
The South East LHIN performance on the 14 MLAA
performance metrics are displayed in Figure 49. Across
the LHIN, only one performance metric is currently
meeting or exceeding the provincial target. The
potential for progress toward the provincial targets
varies across the indicators. Some indicators require
simple process monitoring or moderate interventions,
while others require more detailed operational
changes or system-level interventions:
• Progress on the ‘Home and Community Care’
indicators has remained relatively static. The
South East LHIN has historically performed well
on the 90th percentile wait time for first in-home
service for clients admitted from the community.
The two indicators that are beyond the provincial
target (percentage of clients receiving personal
support or nursing service within 5 days) are close
to the target. With concerted effort to
understand the systemic barriers and routine
monitoring of results, it is expected that the
targets will be achieved in 2016/17.
• The Emergency Room Length of Stay (ER LOS)
indicators are symptomatic of systemic patient
flow issues that have proven a more difficult fix.
There has been progress as a LHIN, and selected
hospitals do meet the targets. However, the
highest-volume Emergency Departments struggle
to meet the targets. The ‘admitted patient’
population is a subset of the ‘complex patients’
with particularly long ER lengths of stay. The wait

96
time for the 10% of admitted patients with the
longest wait times (i.e. 90% wait below this time
frame) may routinely pass 20 hours in the largest
hospitals, and occasionally in the smaller
hospitals, where the pressures for inpatient beds
can be high.
• The percentage of patients receiving diagnostic
procedures (computed tomography (CT) and
Magnetic Resonance Imaging (MRI)) within
expected clinical timeframes varies across the two
domains. While performance on the percentage
of CT cases performed within target is slightly
below target (and anticipated to improve), the
performance on MRI wait times remains well
below expected targets – despite being the
highest-performing LHIN in the province. To meet
the provincial target requires the ability of
providers to perform higher volumes of lower
priority MRI procedures (the procedures that can
wait longer periods of time) – and the required
funding to perform these diagnostic procedures.
Figure 49: Ministry – LHIN Accountability Agreement (MLAA) performance indicators by fiscal quarter, Quarter 1 2014/15 to Quarter 2 2015/16.

97
• LHIN-wide performance on the orthopedic
performance indicators (percentages of Hip and
Knee replacements performed within targeted
wait times) highlights a fundamental systemic
difference in the way procedures are prioritized in
the South East, with a vast under-reporting of
priority 4 procedures (those that can wait the
longest time) relative to other LHINs across the
province. Performance on this indicator cannot be
reasonably assessed until these discrepancies are
corrected.
• The Alternate Level of Care (ALC) situation across
the South East LHIN remains an on-going pressure
with patients waiting in hospital beds for services
elsewhere in the system. This is a broad system
issue complicated by a lack of assisted living in the
South East LHIN. Broader patient flow initiatives
are underway under the direction of the South
East CCAC and Hospitals Executive Forum
(SECHEF).
• Past performance on the Repeat Unscheduled
Emergency Visits for Mental Health and
Substance Abuse indicators is indicative of the
need for system redesign in the Addiction and
Mental Health System to improve client
outcomes. The sector continues to move forward
in a comprehensive redesign with a goal of
improving client care and outcomes.
MONITORING INDICATORS
Some MLAA indicators are defined as monitoring
indicators (Figure 50). These indicators are used to
monitor trends for additional explanatory factors or for
past performance indicators. These monitoring
indicators have no set targets.
• Wait times to be assessed for Long Term Care
Home placement were relatively consistent over
time, with the median number of days ranging
from 13 to 15 days for those in the community
and from 5 to 8 days for those in acute care
settings. The provincial median in the second
quarter of 2015/16 was 14 and 8 days,
respectively.
• The percent of cases completed within access
targets for cancer surgery and cataract surgery
(priority levels 2 to 4) both fluctuated between
83% and 94% between the first quarter of
2014/15 and the second quarter of 2015/16.
• The percent of cases completed within access
targets for cardiac bypass surgery (priority levels 2
to 4) was either close to, or at 100% in the first
two quarters of 2015/16.
• The rate of patients who visited the emergency
department for conditions that could be treated
in alternative primary care settings (also known as
conditions best managed elsewhere, or CBME)
ranged from 7.8 to 11.5 visits per 1,000
Figure 50: Ministry – LHIN Accountability Agreement (MLAA) monitoring indicators by fiscal quarter, Quarter 1 2014/15 to Quarter 2 2015/16.

98
population. These rates were lower than the
overall provincial rate of 3.8 from the second
quarter of 2015/16.
• The rate of hospitalizations for ambulatory care
sensitive conditions (ACSC) ranged from 108.7 to
122.2 hospitalizations per 100,000 population and
was well above the provincial rate of 72.2
hospitalizations per 100,000 population from the
second quarter of 2015/16. The highest
performing LHIN had a rate 41.4 hospitalizations
per 100,000 population.
• The percentage of patients who had a physician
follow-up visit within 7 days of hospital discharge
(where that hospital stay was for one of 8
specified conditions), ranged between 48.8 % and
41.5 % without any specific trend (2013 Q3 –
2015 Q1). The provincial average is 47.5% with
the best performing LHIN at 57.6% (2015 Q1).

99
APPENDIX A – GLOSSARY OF TERMS
ABI Acquired Brain Injury
ACSC Ambulatory Care Sensitive Conditions
ACT Assertive Community Treatment
ADL Activities of Daily Living
ALC Alternate Level of Care
ALOS Average Length of Stay
AMH Addictions & Mental Health
AMI Acute Myocardial Infarction
BGH Brockville General Hospital
BORN Better Outcomes Registry & Network
BSSTU Behavioural Support Services Transition
Unit
CACS Comprehensive Ambulatory Classification
System
CCAC Community Care Access Centre
CCC Complex Continuing Care
CCHS Canadian Community Health Survey
CCIS Critical Care Information System
CCM Comprehensive Care Model
CCO Cancer Care Ontario
CCRS Continuing Care Reporting System
CHC Community Health Centre
CHF Congestive Heart Failure
CIHI Canadian Institute for Health Information
CMG Case Mix Group
CMH&A Community Mental Health & Addictions
COPD Chronic Obstructive Pulmonary Disease
CPDB Corporate Providers Database
CSA Community Sponsored Agreement
CSS Community Support Services
CTAS Canadian Triage and Acuity Scale
DAD Discharge Abstract Database
DATIS Drug and Alcohol Treatment Information
System
DI Diagnostic Imaging
ED Emergency Department
ELOS Expected Length of Stay
EMR Electronic Medical Record
FHG Family Health Groups
FHN Family Health Network
FHO Family Health Organizations
FHT Family Health Teams
HAB Health Analytics Branch
HBAM Health-Based Allocation Model
HCDB Home Care Database
HDH Hotel Dieu Hospital
HHR Health Human Resources
HIG HBAM Inpatient Grouper
HPDB Health Professions Database
HPE Hastings Prince Edward
HQO Health Quality Ontario
HSAA Hospital Service Accountability Agreement
HSFR Health System Funding Reform
HSP Health Service Provider
IADL Instrumental Activities of Daily Living
IAR Integrated Assessment Record
ICD-10-CA International Statistical Classification of
Diseases and Related Health Problems,
10th Revision, with Canadian
Enhancements
ICES Institute for Clinical Evaluative Sciences
ICU Intensive Care Unit
IDF Inclusive Definition of Francophone
IHD Ischemic Heart Disease
IHF Independent Health Facilities
IHSP Integrated Health Service Plan
InterRAI International Resident Assessment
Instruments
InterRAI-
CHA
InterRAI – Community Health Assessment
InterRAI-
HC
InterRAI – Home Care

100
InterRAI-
LTCF
InterRAI – Long Term Care Facility
IP Inpatient
ITTP Intensive Transitional Treatment Program
KFL&A Kingston Frontenac Lennox & Addington
KGH Kingston General Hospital
LACGH Lennox & Addington County General
Hospital
LGL Leeds, Grenville, Lanark
LOS Length of Stay
LSAA Long-Term Care Home Service
Accountability Agreement
LTC Long Term Care
LTCH Long Term Care Home
MCC Major Clinical Category
MLAA Ministry LHIN Accountability Agreement
MODS Multiple Organ Dysfunction Score
MOHLTC Ministry of Health and Long Term Care
MRI Magnetic Resonance Imaging
MSAA Multi Sector Accountability Agreement
NACRS National Ambulatory Care Reporting
System
NEMS Nine Equivalents of Nursing Manpower
Use Score
NHS National Household Survey
NRS National Rehabilitation System
OCAN Ontario Common Assessment of Need
OCDM Ontario Cost Distribution Methodology
OHIP Ontario Health Insurance Plan
OHRS/MIS Ontario Healthcare Reporting Standards/
Management Information System
OMHRS Ontario Mental Health Reporting System
OPHRDC Ontario Physician Human Resources Data
Centre
OR Operating Room
ORG Office of the Registrar General
PACU Post-Anaesthetic Care Unit
PC Providence Care
PCC Program Cluster Category (Grouping of
CMGs)
PEM Patient Enrolment Model
PHU Public Health Unit
PSFDH Perth Smith Falls District Hospital
PSFDH -
Perth
Perth and Smiths Falls District Hospital–
Perth Site
PSFDH -
Smiths
Falls
Perth and Smiths Falls District Hospital–
Smiths Falls Site
PYLL Potential Years of Life Lost
QHC Quinte Health Care
QHC -
Bancroft
Quinte Healthcare Corporation-Bancroft
Site
QHC -
Belleville
Quinte Healthcare Corporation-Belleville
Site
QHC -
Picton
Quinte Healthcare Corporation-Picton Site
QHC-
Trenton
Quinte Healthcare Corporation-Trenton
Site
QIP Quality Improvement Plan
ReCAP Regional Capacity Assessment and
Projections
RIW Resource Intensity Weight
RUG Resource Utilization Group
SAA Service Accountability Agreement
SAMI Standardized ACG (Adjusted Clinical
Group) Morbidity Index
SMILE Seniors Managing Independent Living
Easily
SMO South East Ontario Academic Medical
Organization
South East
LHIN
South East Local Health Integration
Network
Sp Special Programs
TTP Time To Placement
UCC Urgent Care Centre
VON Victorian Order of Nurses
WTIS Wait Time Information System