Insulin Resistance Syndrome in Indians A. Misra*, … · Insulin Resistance Syndrome in Indians A....
4
Insulin Resistance Syndrome in Indians A. Misra*, J.S. Wasir**, N.K. Vikram*** atrics, 56, 508-520,1975a 28. Rush D., Stein Z. & Susser M.: A randomized controlled trial of prenatal nutritional supplementa- tion in New York city. Pediatrics, 65,688-697,1980 29. Prentice A.M., Cole J.J., Foord FA, Lamb W.H. & Whitehead R.G.: Increased birth weight after prenatal dietary supplementation of rural African women Am J Clin Nutr, 46, 912-925,1987 30. Ghafoorunissa, Fat and fatty acid contents of cereals and pulses and their relevance to Indian diets. Eur J Clin Nutr 43:275-283,1989 31. Gopalan S., Patnaik R.and Ganesh K.: Feasible strategies to combat low birth weight and intra- uterine growth retardation, Journal of Pediatric Gastroenterology and Nutrition, Vol 39(1), S37, 2004 32. Olsen S.F., Sorensen J.D., Secher N.J., Hildegaard M, Henriksen T.B., Hansen H.S. & Grant, A.: Ran- domized controlled effect of fish oil supplementa- tion on pregnancy duration. Lancet 339(8800), 1003- 1007,1992 33. Rice R.: Fish and healthy pregnancy: more than a red herring! Professional care of mother and child 6(6). 171-173,1996 34. Hales, C.N. and Barker D.,J., P.: Type 2 (non insulin dependent) diabetes mellitus; the thrifty phenotype hypothesis, Diabetologia, 35;1019-1022, 1992 35. Hales C.N., Barker D.J., Clark, P.M., Cox L.J., Fall C., Osmond C. et al.: Fetal and infant growth and impaired glucose intolerance at age 64, BMJ ;303; 1019-22,1991 36. Yajnik, C.S.: Life cycle effects of nutrition and body size on adult adiposity, diabetes and cardio- vascular disease, Obes. Rev, 3:217-224,2002 37. Bhargava S.K., Sachdev H.S., Fall C., Osmond C., Lakshmy R., Barker D.J., Biswas S.K.D., Ramji S., Prabhakaran D. and Reddy K.S.: Relation of serial changes in childhood body mass index to impaired glucose intolerance in young adulthood. The New Eng J of medicine; 350(9): 865-875, 2004 38. Prader A. Catch-up growth. Postgrad Med J: 54:133-43,1978 39. Cooper E.S., Duff E.M., Howell S. and Bundy D.A.: Catch-up growth velocities after treatment for Trichuris dysentery syndrome. Trans Soc Trop Med Hyg, 89(6)-653, 1995 40. Callend J., Walker S.,·Granthan M.G.S., Cooper E.: Growth and development four years after treat- ment for the Trichuris dysentery syndrome, Acta Paediatrica, Vol 87, No 12(3):1247-1249,1998 41. Keet M.P., Moodie D.O., Wittmann W., Hansen J.D.L.: Kwashirokar: a prospective ten year follow- up study. S Afr Med J: 45:1427-29,1971 42. Satyanarayana K., Prasanna K.T., Narasinga Rao B.S.: Effect of early chiidhood undernturition and child labour on grow1h and adult nutrition status of rural Indian boys around Hyderabad. Hum Clin Nutr, 40 C: 131-40, 1986 43. Martorell R., Rivera J., Kaplowitz H. "Conse- quences of stunting in early childhood for adult body size in rural Guatemala." Annales Nestle 48:85- 92,1990a 44. Waterlow J.S.: Recent Trends in nutrition Chap- ter 2: Reflections on stunting, 18-34, 1993 45. Proos L.A.: Growth and development of Indian children adopted in Sweden. Acta Universities Upasaliensis, Upasala University, 363,1992 46. Stewart R.J.C., Shephard H.G., Preece R.F. and Waterlow J.C.: The effect of rehabilitation at different stages of development of rats marginally malnourished for ten to twelve generations, Br J. Nutr, 403-412,1980 Type 2 diabetes mellitus (T2DM) and coronary heart disease (CHD) are important non-communicable diseases (NCDs) in developed as well as devel- oping countries. Migrant South Asians have an unusually high predisposi- tion to develop both the NCDs'. Rapid nutritional transition and urbanization have resulted in an alarming increase in NCDs in India, while the communi- cable diseases are showing a down- ward trend. During the previous three decades, the prevalence ofT2DM has doubled in both rural and urban areas of India2. INSULIN RESISTANCE Resistance to the insulin-medi- ated glucose uptake in liver, adipose tissue and muscle is the central fea- ture of insulin resistance syndrome (IRS)3, recently also termed as meta- bolic syndrome. The pancreas secretes excessive insulin, thereby, causing hyperinsulinemia, which finally leads to hyperglycemia. The excessive flux of non-esterified free fatty acids from the excess adipose tissues and he- patic overproduction of very-low den- sity lipoprotein cholesterol are key metabolic events resulting in dyslipidemia. The clinical definition of meta- bolic syndrome has been derived from data from Caucasians based on the presence of abdominal obesity, dyslipidemia, hypertension and glu- cose intolerance4• The cut-offs laid down for the definition of the meta- bolic syndrome, however, may not be applicable to Indians5. Migrant Indians:Features of metabolic syndrome were shown in migrant South Asians in the UK nearly a decade ago'. These studies involved people whose ancestral origins were from various South Asian countries, in particular India and Bangladesh. Subsequently, several other investi- gators in the UK have shown that South Asians have a higher magni- tude of insulin resistance than white Caucasians6. Hyperinsulinemia and dyslipidemia have also been shown in South Asian children6. Further, South Asians also have significant procoagulant tendency signified by 5 high plasminogen activator inhibitor- 1 and plasma fibrinogen concentra- tions6,7 . Research on migrant Indians in the USA is recent. Furthermore, most of this research is based on case- control and convenience samples and are not population-based studies. A study of healthy Indian physicians and their relatives residing in the USA, showed higher prevalence of T2DM, hypertriglyceridemia and lower levels of HDL-C. However, the prevalence of obesity was much lower as compared to Caucasians. This study was not population-based, and the investiga- tors did not measure abdominal obe- sityB. Raji et al. 9 indicated that healthy Indian migrants exhibit fasting hyperinsulinemia, higher glucose and insulin levels during the oral glucose tolerance test, and reduced glucose disposal rates as compared to Cau- casians, despite similar fasting plasma glucose levels. Similar data have been reported from other parts of the USA. Indians residing in India: Diet and physical activity profiles of Indi- ans residing in India are extremely heterogeneous. People in the rural areas are physically active farmers or labourers and consume frugal diets. However, increasing affluence, mecha- nization and dietary transition to 'en- ergy-dense' diets is seen in a stepwise manner from smaller cities to metro- politan mega cities. The prevalence rates of obesity and T2DM in the rural populations are low, but these rates show an increasing trend from smaller to larger cities, peaking in the metro- politan cities. Nearly 10-20% of urban people have metabolic syndrome10. A more worrisome feature is highly preva- lent insulin resistance in children and young adults who seem to be under- going 'lifestyle transitions' more rap- idly (Figure)11. People belonging to low socio- economic strata (SES) are generally leaner and have less T2DM than those with high SES. However, rural-to-ur- ban migrants who belong to low SES are adversely affected and show several features of metabolic syndrome and multiple cardiovascular risk factors12-15.
Transcript of Insulin Resistance Syndrome in Indians A. Misra*, … · Insulin Resistance Syndrome in Indians A....

Insulin Resistance Syndrome in IndiansA. Misra*, J.S. Wasir**, N.K. Vikram***
atrics, 56, 508-520,1975a
28. Rush D., Stein Z. & Susser M.: A randomizedcontrolled trial of prenatal nutritional supplementation in New York city. Pediatrics, 65,688-697,1980
29. Prentice A.M., Cole J.J., Foord FA, Lamb W.H.& Whitehead R.G.: Increased birth weight afterprenatal dietary supplementation of rural Africanwomen Am J Clin Nutr, 46, 912-925,1987
30. Ghafoorunissa, Fat and fatty acid contents ofcereals and pulses and their relevance to Indiandiets. Eur J Clin Nutr 43:275-283,1989
31. Gopalan S., Patnaik R.and Ganesh K.: Feasiblestrategies to combat low birth weight and intrauterine growth retardation, Journal of Pediatric
Gastroenterology and Nutrition, Vol 39(1), S37, 2004
32. OlsenS.F., Sorensen J.D., Secher N.J.,HildegaardM, Henriksen T.B., Hansen H.S. & Grant, A.: Randomized controlled effect of fish oil supplementation on pregnancy duration. Lancet 339(8800), 10031007,1992
33. Rice R.: Fish and healthy pregnancy: more thana red herring! Professional care of mother and child
6(6). 171-173,1996
34. Hales, C.N. and Barker D.,J., P.: Type 2 (noninsulin dependent) diabetes mellitus; the thriftyphenotype hypothesis, Diabetologia, 35;1019-1022,1992
35. Hales C.N., Barker D.J., Clark, P.M., Cox L.J.,Fall C., Osmond C. et al.: Fetal and infant growthand impaired glucose intolerance at age 64,BMJ;303; 1019-22,1991
36. Yajnik, C.S.: Life cycle effects of nutrition andbody size on adult adiposity, diabetes and cardiovascular disease, Obes. Rev, 3:217-224,2002
37. Bhargava S.K., Sachdev H.S., Fall C., OsmondC., Lakshmy R., Barker D.J., Biswas S.K.D., RamjiS., Prabhakaran D. and Reddy K.S.: Relation ofserial changes in childhood body mass index toimpaired glucose intolerance in young adulthood.The New Eng J of medicine; 350(9): 865-875, 2004
38. Prader A. Catch-up growth. Postgrad Med J:54:133-43,1978
39. Cooper E.S., Duff E.M., Howell S. and BundyD.A.: Catch-up growth velocities after treatment forTrichuris dysentery syndrome. Trans Soc Trop MedHyg, 89(6)-653, 1995
40. Callend J., Walker S.,·Granthan M.G.S., CooperE.: Growth and development four years after treatment for the Trichuris dysentery syndrome, Acta
Paediatrica, Vol 87, No 12(3):1247-1249,1998
41. Keet M.P., Moodie D.O., Wittmann W., HansenJ.D.L.: Kwashirokar: a prospective ten year followup study. S Afr Med J: 45:1427-29,1971
42. Satyanarayana K., Prasanna K.T., NarasingaRao B.S.: Effect of early chiidhood undernturitionand child labour on grow1h and adult nutritionstatus of rural Indian boys around Hyderabad. HumClin Nutr, 40 C: 131-40, 1986
43. Martorell R., Rivera J., Kaplowitz H. "Consequences of stunting in early childhood for adultbody size in rural Guatemala." Annales Nestle 48:8592,1990a
44. Waterlow J.S.: Recent Trends in nutrition Chapter 2: Reflections on stunting, 18-34, 1993
45. Proos L.A.: Growth and development of Indianchildren adopted in Sweden. Acta UniversitiesUpasaliensis, Upasala University, 363,1992
46. Stewart R.J.C., Shephard H.G., Preece R.F.and Waterlow J.C.: The effect of rehabilitation at
different stages of development of rats marginallymalnourished for ten to twelve generations, Br J.Nutr, 403-412,1980
Type 2 diabetes mellitus (T2DM)and coronary heart disease (CHD) areimportant non-communicable diseases(NCDs) in developed as well as developing countries. Migrant South Asianshave an unusually high predisposition to develop both the NCDs'. Rapidnutritional transition and urbanizationhave resulted in an alarming increasein NCDs in India, while the communicable diseases are showing a downward trend. During the previous threedecades, the prevalence ofT2DM hasdoubled in both rural and urban areasof India2.
INSULIN RESISTANCE
Resistance to the insulin-mediated glucose uptake in liver, adiposetissue and muscle is the central feature of insulin resistance syndrome(IRS)3, recently also termed as metabolic syndrome. The pancreas secretesexcessive insulin, thereby, causinghyperinsulinemia, which finally leadsto hyperglycemia. The excessive fluxof non-esterified free fatty acids fromthe excess adipose tissues and hepatic overproduction of very-low density lipoprotein cholesterol are keymetabolic events resulting indyslipidemia.
The clinical definition of metabolic syndrome has been derived fromdata from Caucasians based on thepresence of abdominal obesity,dyslipidemia, hypertension and glucose intolerance4• The cut-offs laiddown for the definition of the metabolic syndrome, however, may not beapplicable to Indians5.
Migrant Indians:Features ofmetabolic syndrome were shown inmigrant South Asians in the UK nearlya decade ago'. These studies involvedpeople whose ancestral origins werefrom various South Asian countries,in particular India and Bangladesh.Subsequently, several other investigators in the UK have shown thatSouth Asians have a higher magnitude of insulin resistance than whiteCaucasians6. Hyperinsulinemia anddyslipidemia have also been shownin South Asian children6. Further, SouthAsians also have significantprocoagulant tendency signified by
5
high plasminogen activator inhibitor1 and plasma fibrinogen concentrations6,7 .
Research on migrant Indians inthe USA is recent. Furthermore, mostof this research is based on casecontrol and convenience samples andare not population-based studies. Astudy of healthy Indian physicians andtheir relatives residing in the USA,showed higher prevalence of T2DM,hypertriglyceridemia and lower levelsof HDL-C. However, the prevalence ofobesity was much lower as comparedto Caucasians. This study was notpopulation-based, and the investigators did not measure abdominal obesityB. Raji et al. 9 indicated that healthyIndian migrants exhibit fastinghyperinsulinemia, higher glucose andinsulin levels during the oral glucosetolerance test, and reduced glucosedisposal rates as compared to Caucasians, despite similar fasting plasmaglucose levels. Similar data have beenreported from other parts of the USA.
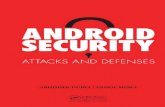
Indians residing in India: Dietand physical activity profiles of Indians residing in India are extremelyheterogeneous. People in the ruralareas are physically active farmers orlabourers and consume frugal diets.However, increasing affluence, mechanization and dietary transition to 'energy-dense' diets is seen in a stepwisemanner from smaller cities to metropolitan mega cities. The prevalencerates of obesity and T2DM in the ruralpopulations are low, but these ratesshow an increasing trend from smallerto larger cities, peaking in the metropolitan cities. Nearly 10-20% of urbanpeople have metabolic syndrome10. Amore worrisome feature is highly prevalent insulin resistance in children andyoung adults who seem to be undergoing 'lifestyle transitions' more rapidly (Figure)11.
People belonging to low socioeconomic strata (SES) are generallyleaner and have less T2DM than thosewith high SES. However, rural-to-urban migrants who belong to low SESare adversely affected and showseveral features of metabolic syndromeand multiple cardiovascular riskfactors12-15.

FIGURE: Prevalence of high HOMA-IR values in post-pubertalAsian Indian children (n=396) residing in India
66.7
HOMA-IR: Insulin resistance estimated by homeostatic model assessment,BMI: Body mass index, BF: Body fat
4. A4. Executive Summary of the Third Report ofthe National Cholesterol Education Program (NCEP)Expert Panel on Detection, Evaluation, and Treat-
3. Reaven G.M.: Banting lecture 1988. Role ofinsulin resistance in human disease. Diabetes.
1988;37(12): 1595-607.
2, Gupta A., Gupta R., Sarna M" Rastogi S., GuptaV,P" Kothari K.: Prevalence of diabetes, impairedfasting glucose and insulin resistance syndrome inan urban Indian population. Diabetes Res Clin Pract.
2003;61 (1):69-76.
References:
protective against adiposity anddyslipidemia, Additionally, fibre intakemay be lower and homocysteine levels may be high in vegetarian Indians,contributing further to cardiovascularrisk24. Dietary acculturation of migrantIndians to the 'Westernized diets' maylead to further unfavourable metabolicchanges,
Physical inactivity: Physicallyinactive lifestyles are consistently seenin South Asians, particularly in women25.The important determinants includeurbanization, affluence and increasing mechanization26. Recent reportsalso indicate substantial physical inactivity in adolescents and youngadults27. Physical inactivity in Indianshas been linked to adiposity,dyslipidemia, and hypertension. Although only a limited number of investigative studies are available, itappears that physical inactivity is acritical determinant of obesity and insulin resistance in Indians.
Genetic predisposition: The factthat Indians in disparate countries andlocations uniformly show a higher tendency to have insulin resistance bespeaks of underlying genetic predispositions. Further, insulin sensitivityis reduced even when the role of adi
posity is nullified in lean Indians ascompared with other ethnic groups2S.However, this issue has not been investigated in any detail. The role ofcandidate genes lipoprotein lipase,plasminogen activator inhibitor-1,adiponectin, angiotensinogen andperoxisome proliferator activator receptor-gamma remain to be investigated in insulin resistant Indians.
1, McKeigue P.M., Marmot M,G" SyndercombeCourt Y.D., Cottier D.E., Rahman S., RiemersmaR.A.: Diabetes, hyperinsulinaemia, and coronaryrisk factors in Bangladeshis in east London. Br
Heart J. 1988;60(5) :390-6
Authors: 'Professor "Pool Officer "'Asst Prof.
Deptt of Medicine, AI/MS, New Delhi
High BF
58.2
• Females
Normal BF
as well as children21. Importantly, theCRP levels in Indians are consistentlyhigher than in Caucasians22. The highCRP levels could be explained by excessabdominal adiposity, since the predominant source of these cytokinesis abdominal adipose tissue. Indeed,high CRP levels in Indians were stronglyassociated with obesity, abdominalobesity, and excess subcutaneousbody faF3.
Whereas the relationship betweeninsulin resistance and sub-clinical inflammation continues to be debated,CRP levels in Indians also correlate toinsulin resistance21, Finally, althoughCRP levels have predicted an increasedrisk of developing of CHD22 prospective data are needed.
Diet: The link between Indian dietsand insulin resistance has been suspected but remains inadequately investigated. In general, consumptionof saturated fat has increased in Indiain line with 'dietary Westernization',and this might be linked to overall aswell as abdominal adiposity. The highcarbohydrate content of Indian dietsmay cause hypertriglyceridemia andhyperinsulinemia. The vegetarian dietary habits of Indians may not be
LIFESTYLE ANDGENETIC FACTORS
High BMI
o Males
Normal BMI
80
7060
Q)
() 50c ~ro> 40Q) '-D...
~30
0
20100
BODY FAT DISTRIBUTION
As compared to Caucasians inthe developed countries, the prevalence of obesity is less in Indians. Anincreasing trend in obesity in Indianchildren and adolescents, however,has been recently reported16,17.
The paradox of high predisposition to developing T2DM and CHD ata relatively lower average level of bodymass index (8MI) is not easily explained; however, several peculiarfeatures in the body composition ofIndians have been noticed. It appearsthat migrant and urban Indians of bothsexes have excess of body fat, truncalsubcutaneous fat, and intraabdominalfat12,14,15,1S-20.Data showing a higherprevalence of abdominal adiposity,as defined by high ratio of waist-tohip circumference, have been consistently recorded in migrant Indians irrespective of their geographical habitat. It is generally believed by manyinvestigators that excess regionaladiposity as seen in Indians is the keydeterminant to the development ofinsulin resistance.
Subclinical inflammation: Sub
clinical inflammation denoted by highC-reactive protein (CRP) concentrations, an important indicator of cardiovascular risk, has been recordedto be widely present in Indians, adults

ment of High Blood Cholesterol in Adults (AdultTreatment Panel III). JAMA. 2001; 285(19) :24862497.
5. Misra A., Wasir J.S., Pandey A.M.: An evaluation of candidate definitions of the metabolic syndrome in adult Asian Indians. Diabetes Care.
2005;28(2):398-403.
6. Whincup P.H., Gilg J.A., Papacosta 0., et al.Early evidence of ethnic differences in cardiovascular risk: cross sectional comparison of BritishSouth Asian and white children. BMJ.
2002;324(7338):635.
7. Kain K., Catto A.J., Grant P.J.: Impaired fibrinolysis and increased fibrinogen levels in SouthAsian subjects. Atherosclerosis. 2001 ;156(2):45761.
8. Enas E.A., Garg A., Davidson M.A., Nair V.M.,Huet B.A., Yusuf S.: Coronary heart disease and itsrisk factors in first-generation immigrant Asian Indians to the United States of America. Indian Heart J.
1996;48(4) :343-53.
9. Raji A., Seely EW., Arky R.A., Simonson D.C.:Body fat distribution and insulin resistance in healthyAsian Indians and Caucasians. J Clin Endocrinol
Metab. 2001 ;86(11):5366-71.
10. Misra A., Vikram N.K.: Insulin resistance syndrome (metabolic syndrome) and Asian Indians.Curr Sci. 2002;83:1483-1496 (available at h11QJL
teias. serc. iisc. erne!. in/- cu rrsell.
11. Arya S., Misra A., Vikram N.K., et al. Fastinghyperinsulinemia and its relationship to measuresof obesity and lipid profile in urban adolescentsand young adults in north India. Diabetes Metab.2003;29:4S118-119.
12. Misra A., Chaudhary D., Vikram N.K., et a/.
Insulin resistance and clustering of atherogenicrisk factors in women belonging to low socio-economic strata in urban slums of North India. Diabe
tes Res Clin Pract. 2002;56(1) :73-5.
13. Misra A., Pandey R.M., Sharma R.: Non-communicable diseases (diabetes, obesity andhyperlipidaemia) in urban slums. Natl Med J India.2002; 15(4) :242-4.
14. Misra A., Pandey R.M., Devi J.R., Sharma R.,Vikram N.K., Khanna N.: High prevalence of diabetes, obesity and dyslipidaemia in urban slum population in northern India. Int JObes Relat Metab
Disord. 2001 ;25(11):1722-9.
15. Misra A., Sharma R., Pandey R.M., Khanna N.:Adverse profile of dietary nutrients, anthropometryand lipids in urban slum dwellers of northern India.Eur J Clin Nutr. 2001 ;55(9):727-34.
16. Kapil U., Singh P., Pathak P., Dwivedi S.N.,Bhasin S.: Prevalence of obesity amongst affluentadolescent school children in delhi. Indian Pediatr.
2002;39(5) :449-52.
17. Guleria R., Dhingra V., Chatterjee A., et al.Anthropometric profile in urban adolescents andyoung adults. J Assoc Physicians India. 2003;50:.1521.
18. Banerji M.A., Faridi N., Alturi R., Chaiken R.L.,Lebovitz H.E.: Body composition, visceral fat, leptinand insulin resistance in Asian Indian men. J Clin
Endocrinol Metab. 1999;84:137-144.
19. Dudeja V., Misra A., Pandey R.M., Devina G.,Kumar G., Vikram N.K.: BMI does not accuratelypredict overweight in Asian Indians in northernIndia. Br J Nutr. 2001 ;86(1):105-12.
20. Misra A., Athiko D., Sharma R., Pandey R.M.,Khanna N.: Non-obese hyperlipidemic Asian northern Indian males have adverse anthropometricprofile. Nutr Metab Cardiovasc Dis. 2002;12(4):178-83.
21. Chambers J.C., Eda S., Bassett P., et al. Creactive protein, insulin resistance, central obesity,and coronary heart disease risk in Indian Asiansfrom the United Kingdom compared with Europeanwhites. Circulation. 2001;104(2):145-50.
22. Forouhi N.G., Sattar N., McKeigue P.M.: Relation of C-reactive protein to body fat distributionand features of the metabolic syndrome in Europeans and South Asians. Int JObes Relat Metab
Disord. 2001 ;25(9):1327-31.
23. Vikram N.K., Misra A., Dwivedi M., et al. Correlations of C-reactive protein levels with anthropometric profile, percentage of body fat and lipids inhealthy adolescents and young adults in urbanNorth India. Atherosclerosis. 2003;168(2):305-13.
24. Vikram N.K., Pandev R.M., Sharma R., Misra A.:Hyperhomocysteinemia in healthy Asian Indians.Am J Hematol. 2003;72(2):151-2.
25. Kamath S.K., Hussain E.A., Amin D., et al. Cardiovascular disease risk factors in 2 distinct ethnic
groups: Indian and Pakistani compared with American premenopausal women. Am J Clin Nutr.
1999;69(4):621-31.
26. Misra A.: Body composition and the metabolicsyndrome in Asian Indians: a saga of multipleadversities. Natl Med J India. 2003;16(1):3-7.
27. Dhingra V., Chatterjee A., Guleria R., et al.
Adverse physical activity pattern in urban adolescents. J Assoc Physicians India. 2002;50: 1521.
28. Dickinson S, Colagiuri S, Faramus E, Petocz P,Brand-Miller JC. Postprandial hyperglycemiaand insulin sensitivity differ among lean youngadults ofdifferent ethnicities. J Nutr. 2002;132(9):25742579.
FOUNDATIONNEWS
• Meeting on Food and NutritionSecurity in South Asia: (March 7 9,2005)
The Nutrition Foundation of India, with the cooperation of the Government of India and the United StatesDepartment of Agriculture, organizeda three-day meeting on Food andNutrition Security in South Asia.
DrC. Rangarajan, Chairman, Economic Advisory Council to the PrimeMinister, Government of India, delivered the inaugural address.' An excerpt from the address appears elsewhere in this Bulletin.
Delegates from seven countriesof South Asia, namely, Bangladesh,Bhutan, India, Maldives, Nepal, Pakistan and Sri Lanka, participated in the
meeting.
In the first session, delegatesdescribed the experiences of theirrespective countries in promotingnutrition security through appropriate nutrition orientation to food production policies.
The second session dealt withpolicies and strategies to acceleratepoverty reduction.
The third session was devotedto discussions on ongoing programmesfor improving access to food. Thedelegates presented their experiencesin ensuring targeting and good coverage under these programmes, andevaluated the impact ofthe programmeson the prevalence of undernutrition.
In the fourth session, the healthconsequences of under/overnutritionand country programmes for combating these problems were discussed.
The rapporteurs presented summaries of the presentations in eachsession, and presented similarities andcontrasts between the countries. Theyalso summarized the recommendations regarding policies, strategies andprogrammes for improving nutritionsecurity and the nutritional status ofthe populations of South Asian nations.
The report of the meeting is being edited by Ms Malini Sheshadri.
The delegates to the meetingwere:
Bangladesh: Mr M.A. Hussain; Dr M.Hossain; Dr H.H. Akhter; Dr F. Naher
Bhutan: Ms C.P Wangdi; Dr D. Kinlay
India: Dr B.N. Yugandhar; Dr A. Sen;Dr V. Prakash; Dr P. Ramachandran
Maldives: Ms Shazla Mohamed; DrM. Shareef; Dr. A.S. Mohamed
Nepal: Dr S. Acharya; Mr A. Talukder;Prof B. Pyakural; Dr D. Paudyal
Pakistan: Dr Naeem I. Hashmi; DrM.A. Khan; Prof F.M. Anjum
Sri Lanka: Dr P. Soysa; Dr S.Weerasena; Dr R.M.K. Ratnayake; DrC. Piyasena
Resource Persons: Mr Chad R. Russel;Mr. David Kincaid; Dr C. Bantilan; DrB. Nandi; Dr M. Ali; Dr S. Babu; Dr C.Jackson
Rappoteurs: Dr M. Bamji; Dr K.Krishnaswamy; Dr N. Singh; Dr A.N.Kapoor

• Course in Practical PaediatricNutrition
Dr Sarath Gopalan and DrAnupamSibal, the Course Directors conductedthe Fifth Course in Practical Paediatric Nutrition on March 5th and 6th 2005at Indraprastha Apollo Hospital, NewDelhi.
• Nutrition in the Philippines: ThePast for its Template, Red for itsColor
Recently the Philippines Presslaunched a book "Nutrition in the Philippines: The Past for its Template,Red for its Color", authored by DrCecilia A Florencio. The book describes and analyses the advancesand shortfalls in the country's thinking and efforts to address the longstanding, widespread, and layeredproblem of malnutrition in infants,children, adolescents, pregnant andlactating women, adults, and the elderly. The author puts forward recommendations for reflection and action,on specific and broad fronts, and whilerecognizing the reality of an increasingly borderless world; she calls forthe country to address its nutritionalsituation with the national interest andpriorities first. And yet, in a generalsense, the book is as much aboutmany other countries in both the Eastand West as it is about the Philippines. In the global community, it isestimated that 800 million people arefood insecure and 170 million youngchildren suffer from undernourishment.Copies of the book can be orderedfrom [email protected] [email protected] (website:www.uppress.org).
• Mid-day Meal Programme in DelhiSchools
NFl has been collaborating withthe Municipal Corporation of Delhi(MCD) in the implementation of theMid Day Meal programme in Delhischools. A meeting to discuss futurecollaborations with MCD was held onJanuary 31st, 2005. The meeting wasattended by Mr Rakesh Mehta, Commissioner, MCD, officials of MCD associated with the NFI-MCD collaborative projects, and the NFl team.
NUTRITIONNEWS
Focusing on direct nutritionintervention programmes toaddress the needs of vulnerable groups.
Countries of South Asia havea common heritage. They were allunder colonial rule till the middleof the last century. Newly independent, they face similar problems. Ensuring food and nutritionsecurity is one such problem. Allthe countries in this region haveaddressed this problem in similarways. We need to know whichprogrammes have been successful and which have not. This meetingwill enable you to make an assessment.
All programmes aimed at ensuring food and nutrition securityinvolve heavy expenditure byGovernments. The conventionalbudget exercises focus on allocation of resources to differentheads without assessing how theseexpenditures get translated intooutputs and outcomes. Outputsare the direct result of government expenditure and outcomesare the final results. For example,in the context of education, opening a new school or appointing anew teacher is an output and raising literacy ratio is the outcome.
The emphasis must, therefore, be on output and outcomerather than allocation. Public expenditures must be guided by thecriterion of economy, efficiencyand effectiveness.
These are particularly important in the case of programmesaimed at improving the nutritionstatus of the population, since theexpenditures are large and goalsare specific.
partment of Medicine, AIIMS, New Delhi)spoke on Metabolic syndrome in Indians: Trials and Tribulations.
• National Academy of Medical Sciences (NAMS)
Dr Prema Ramachandran, DirectorNFl has been elected as the VicePresident of NAMS. She will hold theoffice for two years.
Excerpts from the Inaugural Address byDr C Rangarajan
(d)Food security in India hasessentially meant food grain security for meeting the requirementsof energy and protein. For nutrition security, food productionshould ensure availability of diverse foods, which can enhancethe nutritional content, includingmicronutrients. Nutrition securityis thus a broader term. It includeswithin it food grain security butgoes beyond it.
Undernourishment has a deleterious effect on the life of people.Malnourished children grow up tobecome adults unable to operateat full potential. Developmenteconomists and policy makers needto take into account the effects ofnutritional and health care deprivation on human productivity. Thelinks between nutritional statusand the capacity for work havenot so far been adequately incorporated in growth models. Poornutrition and under nourishmentresult in low productivity leadingto low wages which, in turn, results in poor nutrition intake. Thusa vicious cycle is set in motion.One writer has described this asthe 'poverty trap'.
Ensuring nutrition securityrequires attention to programmesaimed at-
(a) Enhancing food grain production with a nutritional orientation;
(b) Improving the food distribution system so that the poorhave access to food grain ataffordable costs;
(c) Augmenting the purchasingpower of the poor throughspecial schemes in times ofstress and vulnerability; and
• Study Circle MeetingsJanuary 18th, 2005.Dr Siddharth Ramji (Professor &
Head, Department of Neonatology,MAMC, New Delhi) delivered a talk on"Neonatal Feeding: Long Term HealthOutcomes" .
February 16th, 2005Dr Anoop Misra, (Professor, De-
Edited by Mrs Anshu Sharma for the Nutrition Foundation of India, C-13, Qutab Institutional Area, New Delhi 110 016. website: www.nutritionfoundationofindia.orge-mail: [email protected] Designed and produced by Media Workshop India Pvl Ltd. e-mail: [email protected]