



Innovative Surgical Management in the Treatment of Rectal ...€¦ · Innovative Surgical...
57
Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch Division Associate Professor of Surgery Johns Hopkins University Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond
Transcript of Innovative Surgical Management in the Treatment of Rectal ...€¦ · Innovative Surgical...
Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch Division Associate Professor of Surgery Johns Hopkins University
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond
Overview • Current Standard of Care
– Staging – Neoadjuvant Therapy – Technique
• MIS techniques • TEM/TAMMIS • Robotic Approach • Watch and Wait
Staging Determine extent of local
disease • History and physical exam
– pain • Digital rectal examination • Vaginal examination • Endoscopy • Imaging Studies
Imaging of Body
• CT Abdomen/Pelvis/Chest • CXR • MRI • US • ? PET scan
Current Neoadjuvant Recommendations in United States
• T3, NO or any T, N1 or 2 • Middle or Distal Rectum • Circumferential Margin • Long Course Therapy • Surgery 8-10 weeks
– Possibly 12 weeks
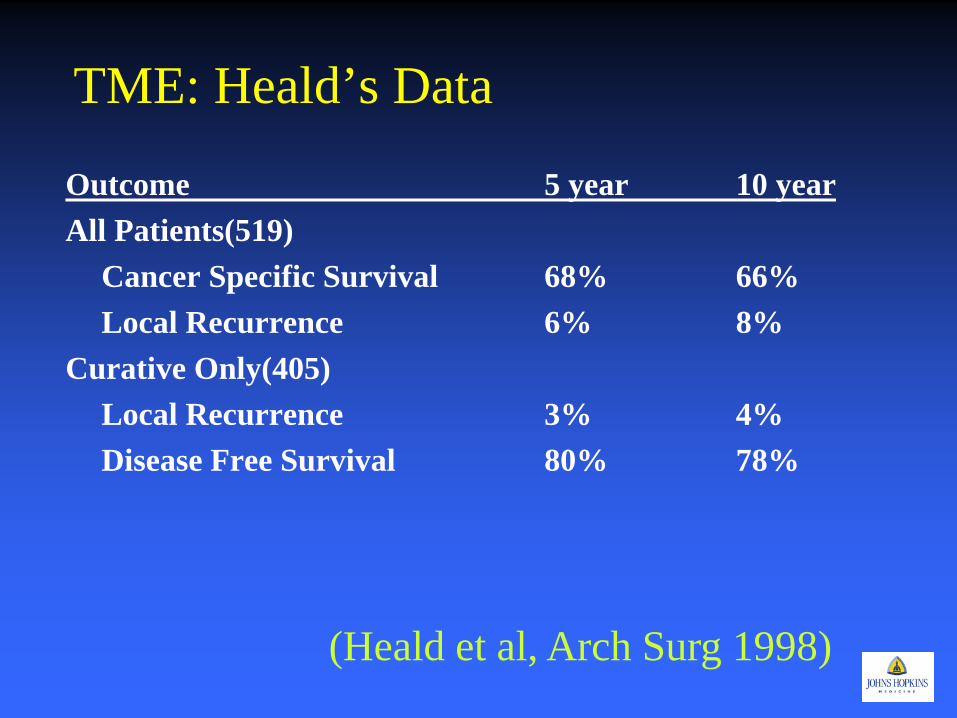
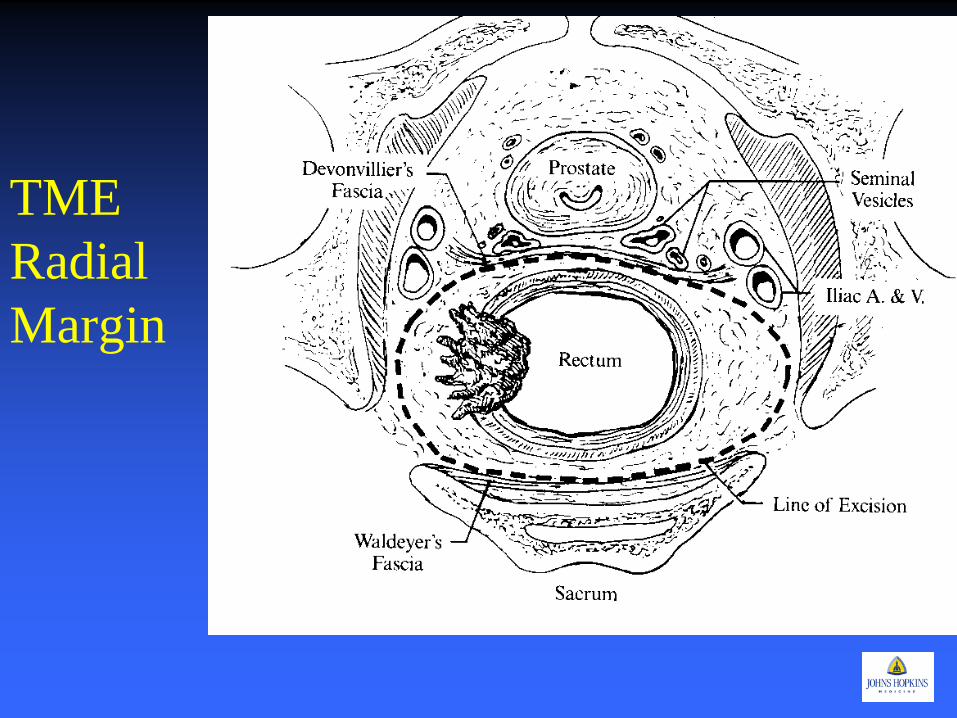
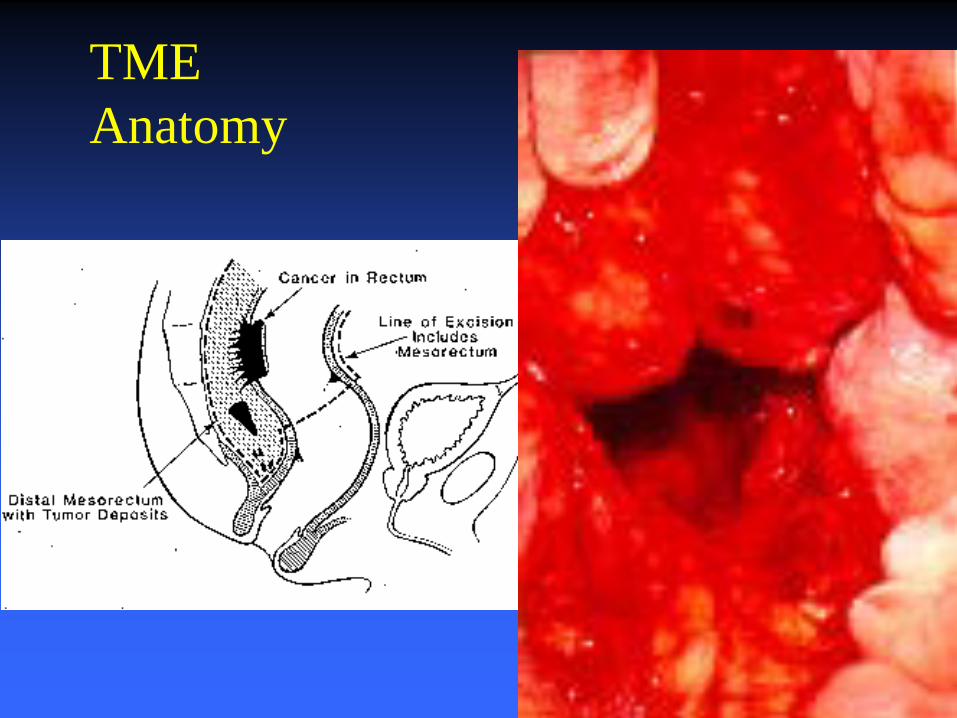
TME: Heald’s Data
Outcome 5 year 10 year All Patients(519) Cancer Specific Survival 68% 66% Local Recurrence 6% 8% Curative Only(405) Local Recurrence 3% 4% Disease Free Survival 80% 78%
(Heald et al, Arch Surg 1998)
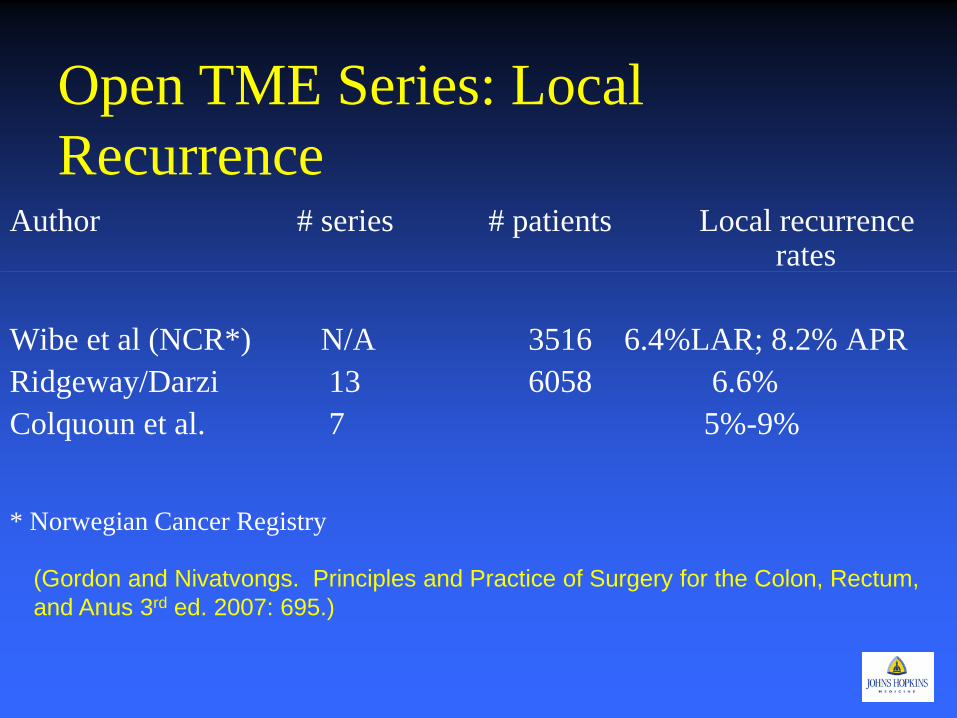
Open TME Series: Local Recurrence
Author # series # patients Local recurrence rates
Wibe et al (NCR*) N/A 3516 6.4%LAR; 8.2% APR Ridgeway/Darzi 13 6058 6.6% Colquoun et al. 7 5%-9%
* Norwegian Cancer Registry (Gordon and Nivatvongs. Principles and Practice of Surgery for the Colon, Rectum, and Anus 3rd ed. 2007: 695.)
Definitions: MIS Surgery • Laparoscopic assisted proctectomy with TME
– Laparoscopic colonic mobilization with open proctectomy
– Laparoscopic colonic and rectal resection with laparoscopic TME and double stapled coloanal
– Laparoscopic colonic and rectal resection with TME and intersphincteric dissection and hand sewn coloanal anastamosis.
– Laparoscopic Abdominoperineal resection – SILS – Robotic
• Hand assisted proctectomy with TME
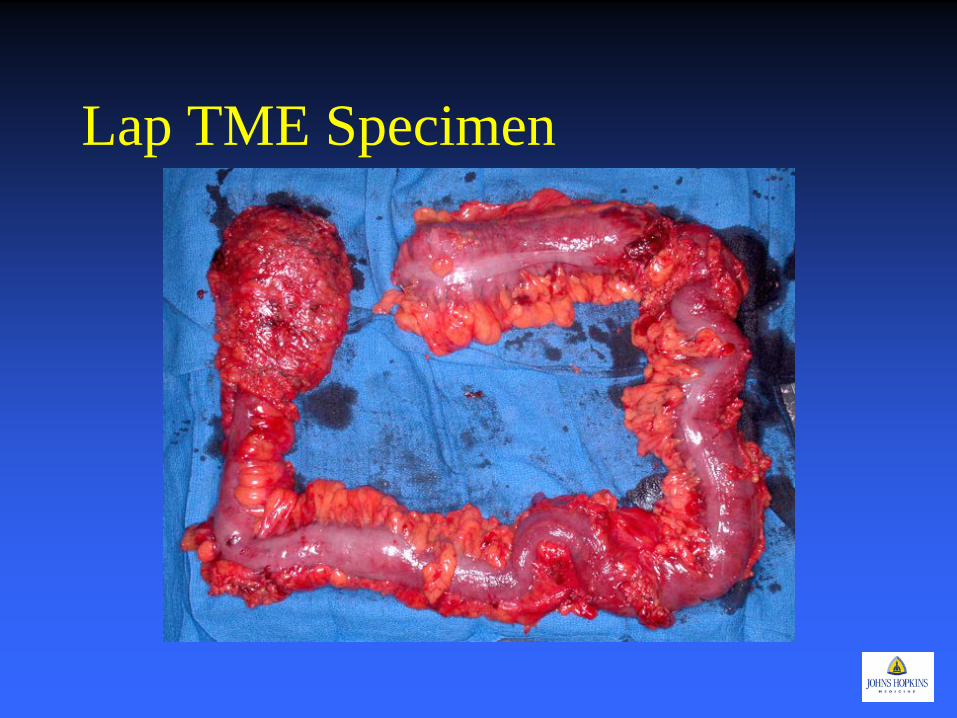
Measures of Quality and Outcome
• Short Term Complications – Mortality – Morbidity
• Pathological Assessment – TME specimen, circumferential margins – Lymph nodes
• Long Term Complications • Recurrence • Survival
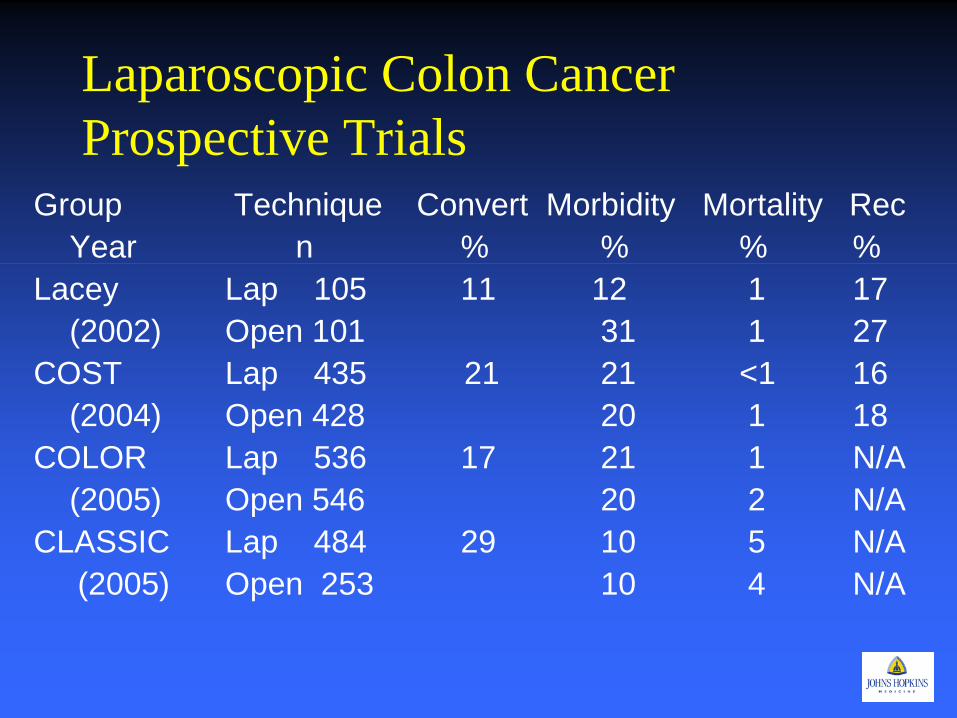
Laparoscopic Colon Cancer Prospective Trials
Group Technique Convert Morbidity Mortality Rec Year n % % % % Lacey Lap 105 11 12 1 17 (2002) Open 101 31 1 27 COST Lap 435 21 21 <1 16 (2004) Open 428 20 1 18 COLOR Lap 536 17 21 1 N/A (2005) Open 546 20 2 N/A CLASSIC Lap 484 29 10 5 N/A (2005) Open 253 10 4 N/A
MIS Surgery for Rectal Cancer
• Is MIS Total Mesorectal Excision possible? • How does the physiology of
pnuemoperitoneum and laparoscopic surgery effect the tumor biology? – It Doesn’t
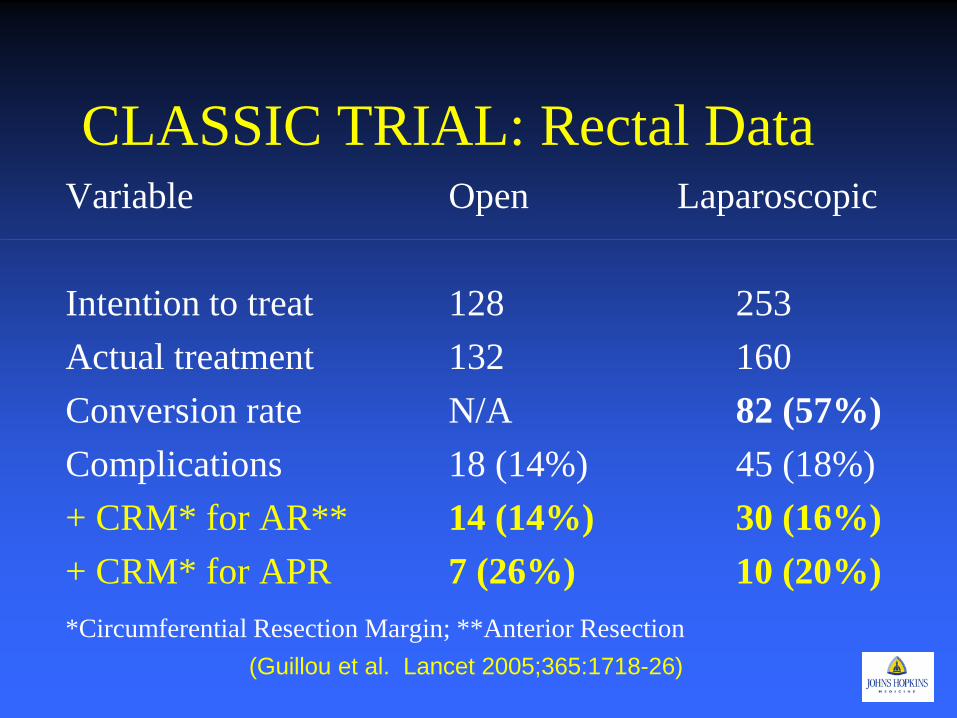
CLASSIC TRIAL: Rectal Data Variable Open Laparoscopic Intention to treat 128 253 Actual treatment 132 160 Conversion rate N/A 82 (57%) Complications 18 (14%) 45 (18%) + CRM* for AR** 14 (14%) 30 (16%) + CRM* for APR 7 (26%) 10 (20%) *Circumferential Resection Margin; **Anterior Resection (Guillou et al. Lancet 2005;365:1718-26)
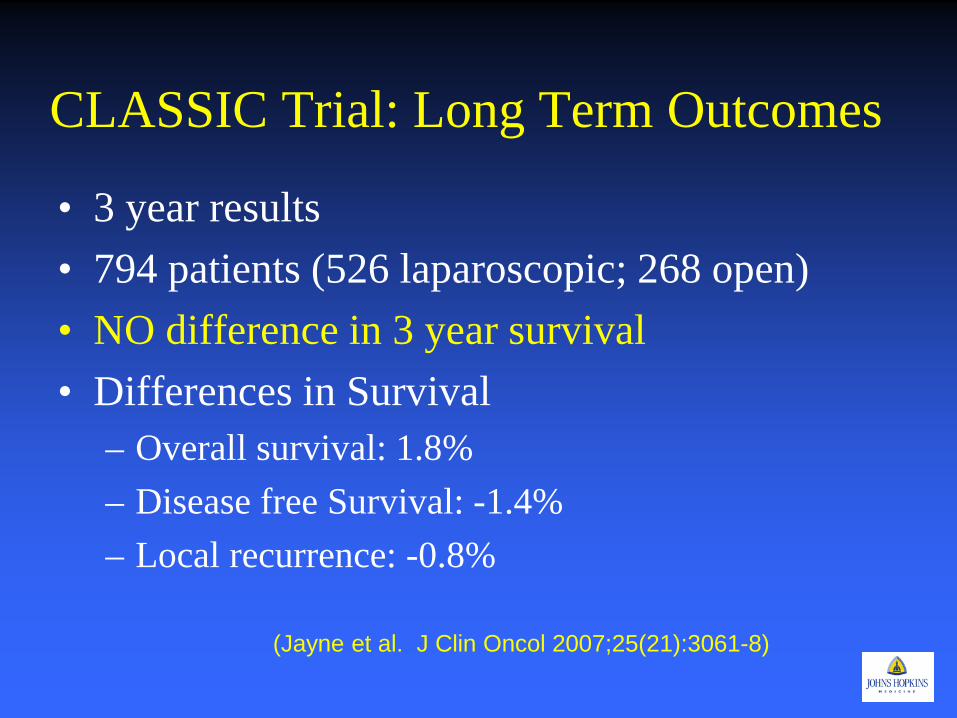
CLASSIC Trial: Long Term Outcomes
• 3 year results • 794 patients (526 laparoscopic; 268 open) • NO difference in 3 year survival • Differences in Survival
– Overall survival: 1.8% – Disease free Survival: -1.4% – Local recurrence: -0.8%
(Jayne et al. J Clin Oncol 2007;25(21):3061-8)
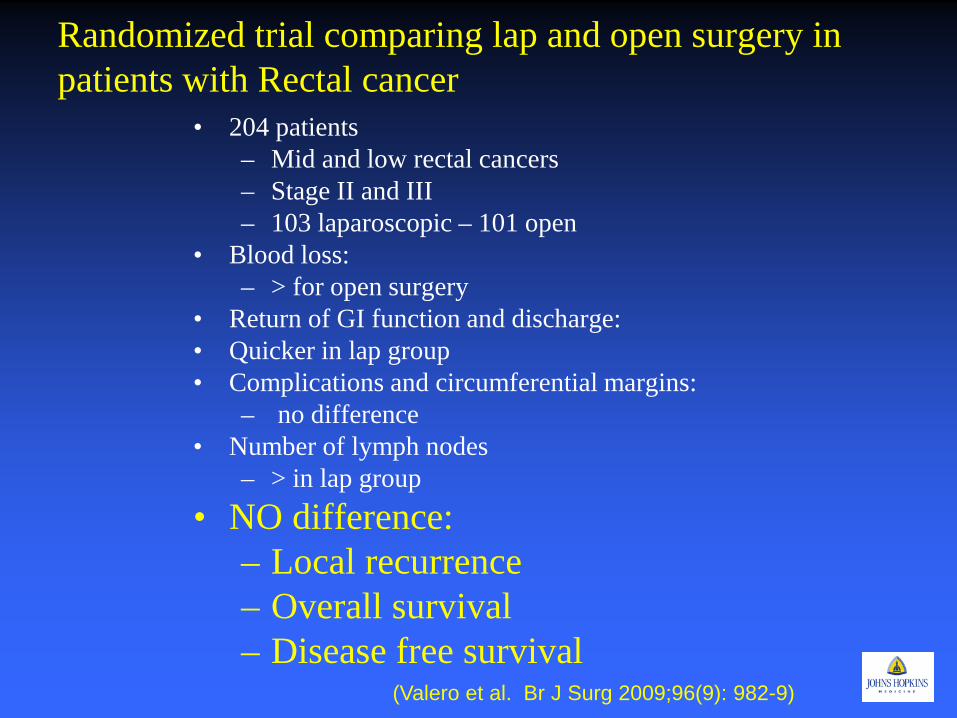
Randomized trial comparing lap and open surgery in patients with Rectal cancer
• 204 patients – Mid and low rectal cancers – Stage II and III – 103 laparoscopic – 101 open
• Blood loss: – > for open surgery
• Return of GI function and discharge: • Quicker in lap group • Complications and circumferential margins:
– no difference • Number of lymph nodes
– > in lap group • NO difference:
– Local recurrence – Overall survival – Disease free survival
(Valero et al. Br J Surg 2009;96(9): 982-9)
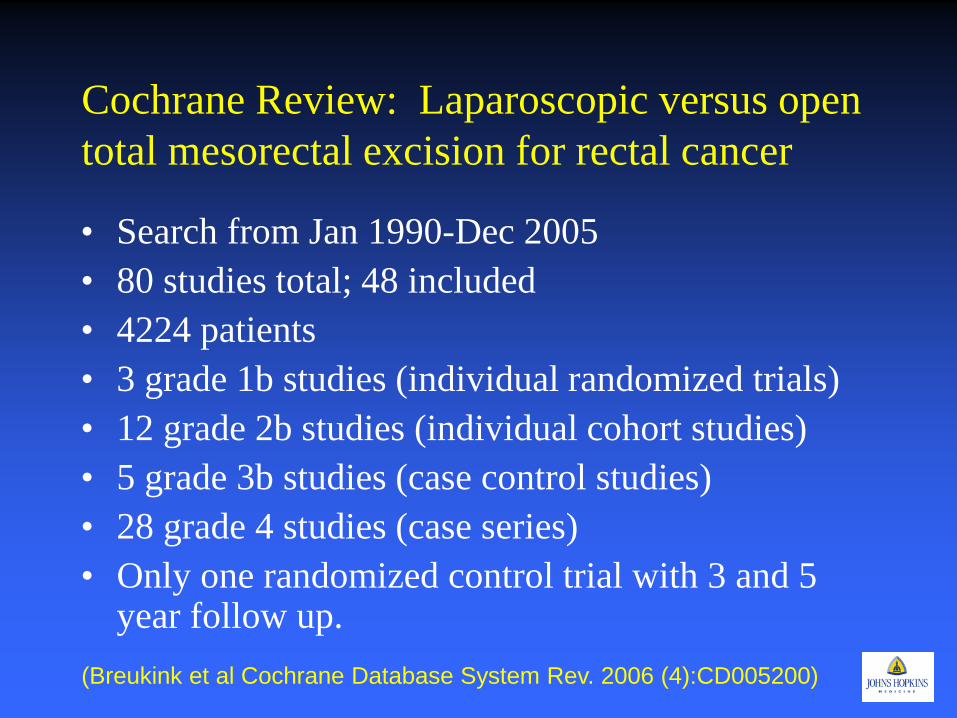
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Search from Jan 1990-Dec 2005 • 80 studies total; 48 included • 4224 patients • 3 grade 1b studies (individual randomized trials) • 12 grade 2b studies (individual cohort studies) • 5 grade 3b studies (case control studies) • 28 grade 4 studies (case series) • Only one randomized control trial with 3 and 5
year follow up. (Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
Laparoscopic Resection of Rectosigmoid Cancer
• Prospective randomized study • 1993-2002 • 5 year follow up • 403 patients randomized • Conversion rate 23.2%
(Leung et al. Lancet 2004;363:1187-92)
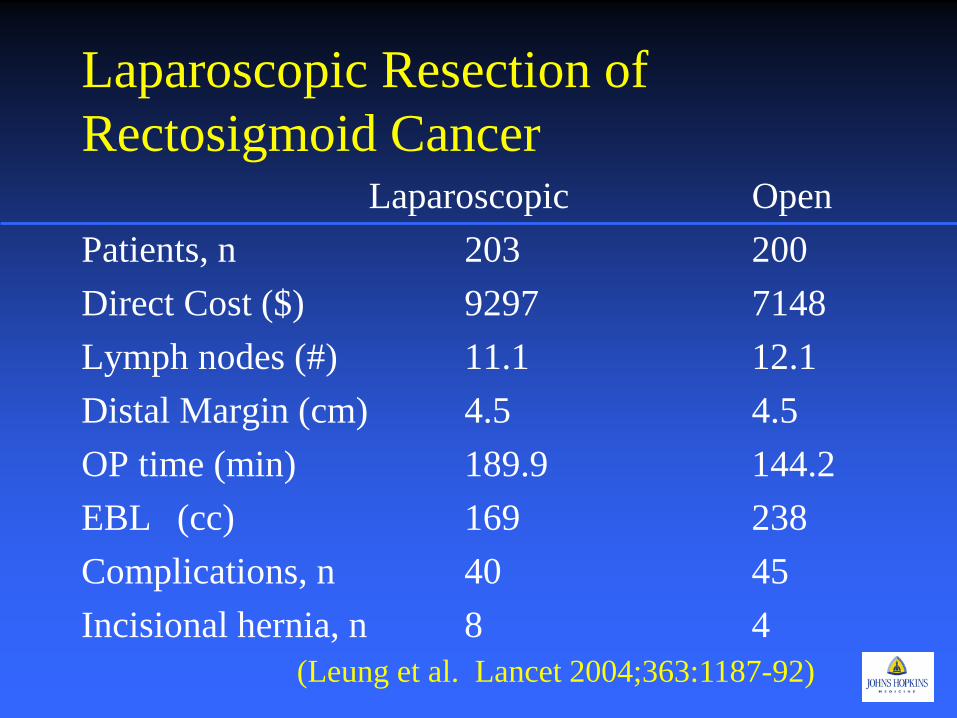
Laparoscopic Resection of Rectosigmoid Cancer Laparoscopic Open Patients, n 203 200 Direct Cost ($) 9297 7148 Lymph nodes (#) 11.1 12.1 Distal Margin (cm) 4.5 4.5 OP time (min) 189.9 144.2 EBL (cc) 169 238 Complications, n 40 45 Incisional hernia, n 8 4
(Leung et al. Lancet 2004;363:1187-92)
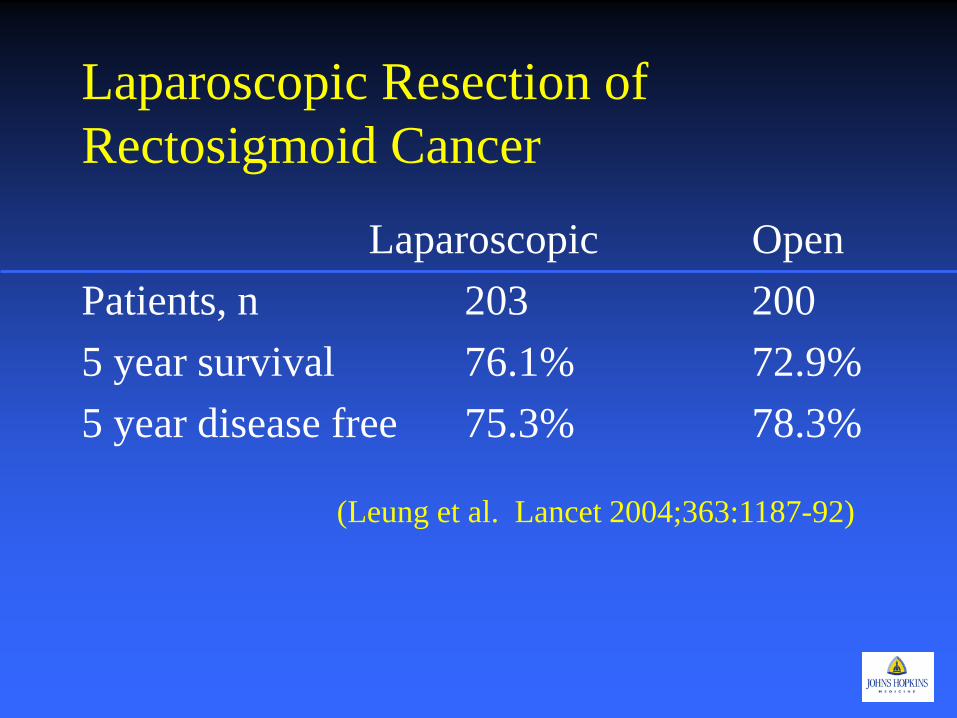
Laparoscopic Resection of Rectosigmoid Cancer
Laparoscopic Open Patients, n 203 200 5 year survival 76.1% 72.9% 5 year disease free 75.3% 78.3%
(Leung et al. Lancet 2004;363:1187-92)
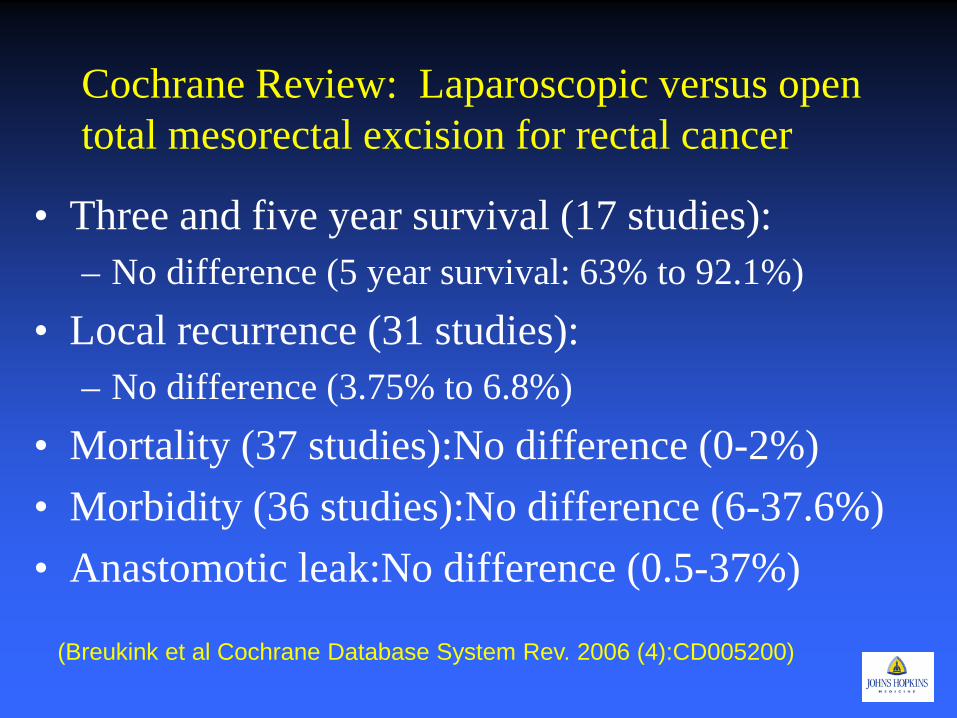
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Three and five year survival (17 studies): – No difference (5 year survival: 63% to 92.1%)
• Local recurrence (31 studies): – No difference (3.75% to 6.8%)
• Mortality (37 studies):No difference (0-2%) • Morbidity (36 studies):No difference (6-37.6%) • Anastomotic leak:No difference (0.5-37%)
(Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Laparoscopic TME had significant benefit in: – Blood loss – GI recovery rate – Post operative pain score – Postoperative analgesia – Immunological response – Length of stay
(Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Open TME had significant benefit in: – Duration of surgery – Cost (only one study)
(Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
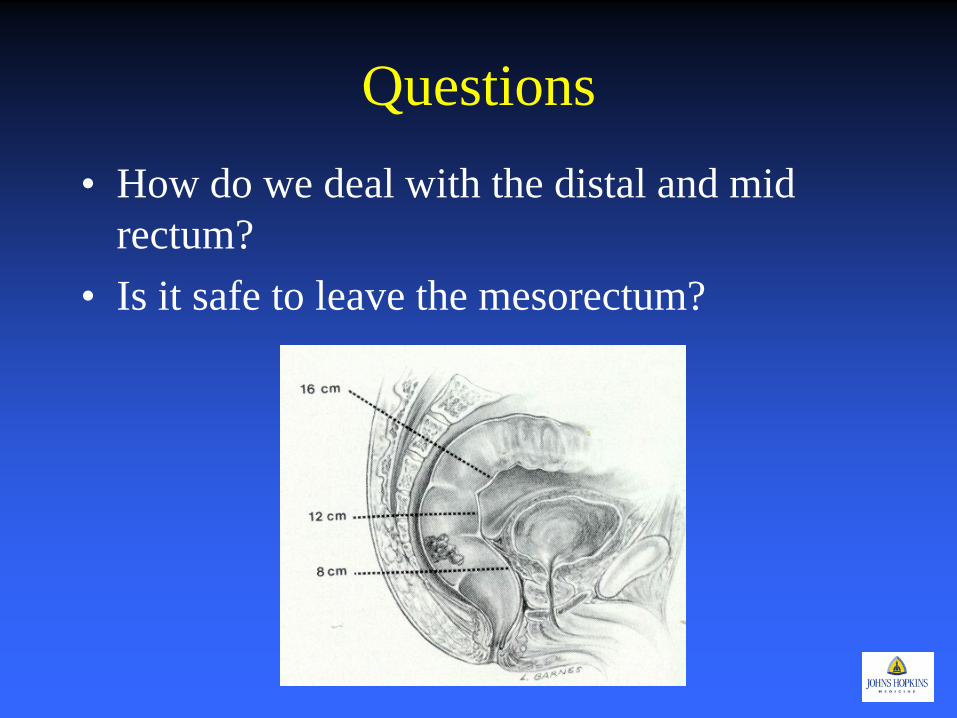
Questions • How do we deal with the distal and mid
rectum? • Is it safe to leave the mesorectum?
Laparoscopic TATA: Laparoscopic Transanal Transabdominal Approach
• 79/102 patients • 1998-2008 • Excluded:
– Stage IV – Tumors 3 cm from the anorectal ring – No neoadjuvant therapy
• Mean follow up: 34.2 months • Conversion rateL: 2.5% • Morbidity:
– Major: 11% – Minor:19%
• Local Recurrence: 2.5% • Distant Recurrence: 10.1%
(Marks J et al. Surg Endosc 2010 Nov 24(11):2700-7)
Transanal Endoscopic Microsurgery/TAMIS
• Trans anal excision – TEM superior to standard – ? TAMIS Equivalent
• Risk of lymph node metastasis – Recurrence
• T stage – T1 lesions – T2 lesions – T2 after neoadjuvant therapy
Transanal Endoscopic Microsurgery vs. Laparoscopic Total Mesorectal Excision for T2N0 Rectal Cancer.
• 78 patients – T2N0 tumors – Median follow up 70 months
• Morbidity less in TEM (p=0.001 TEM TEM+RT Laparoscopic n 32 11 35 Recurrence 26% 0% 9%
( Allax ME et al. J Gastrointest Surg 2012 Oct 16 epub)
TAMIS: Feasibility of transanal minimally invasive surgery for mid-rectal lesions.
• 16 patients – 3 T1 – 8 S/P neoadjuvant therapy – 4 neuroendocrine – 1 mucocele
• TAMIS technique • 7.5 cm from the anal verge (4-10cm) • No morbidity or mortality • LOS: 3 days
(Lim SB et al. Surg Endosc Nov 2012;26(11):3127-32)
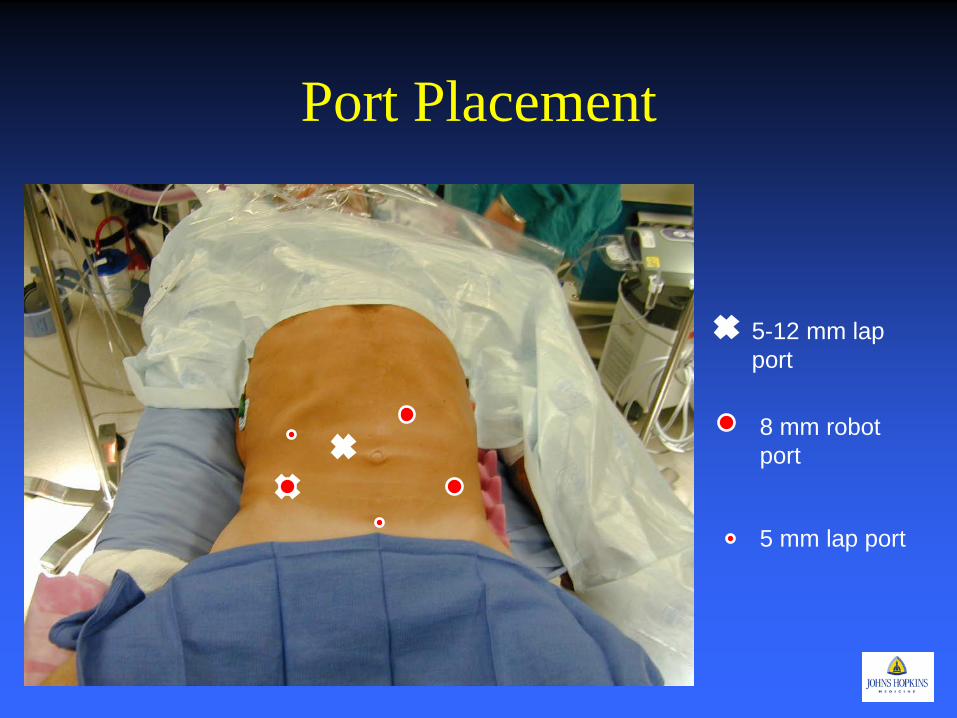
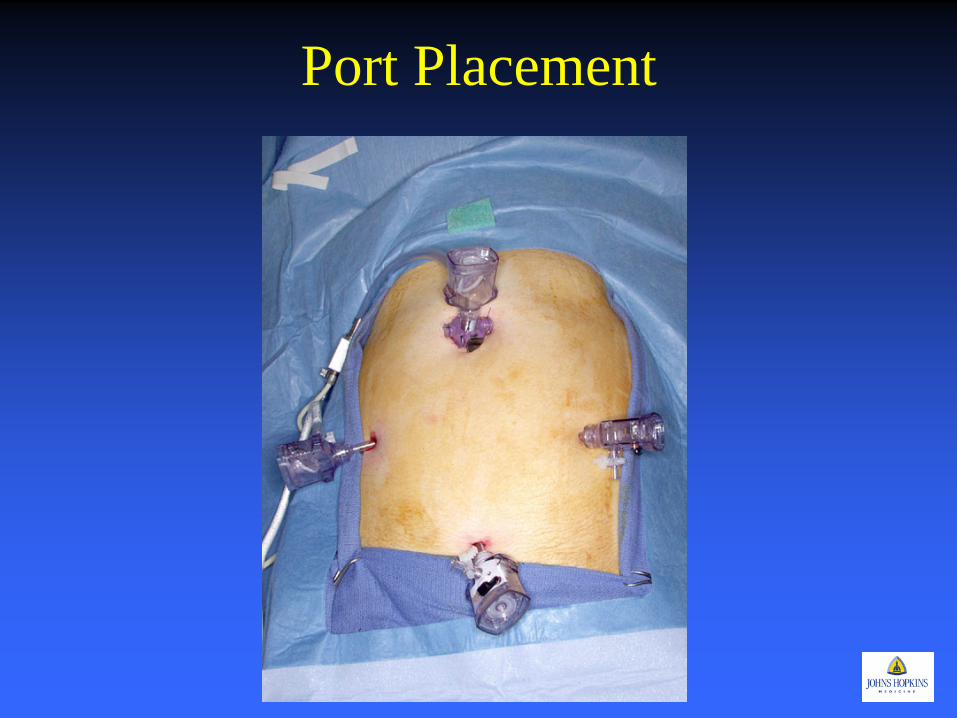
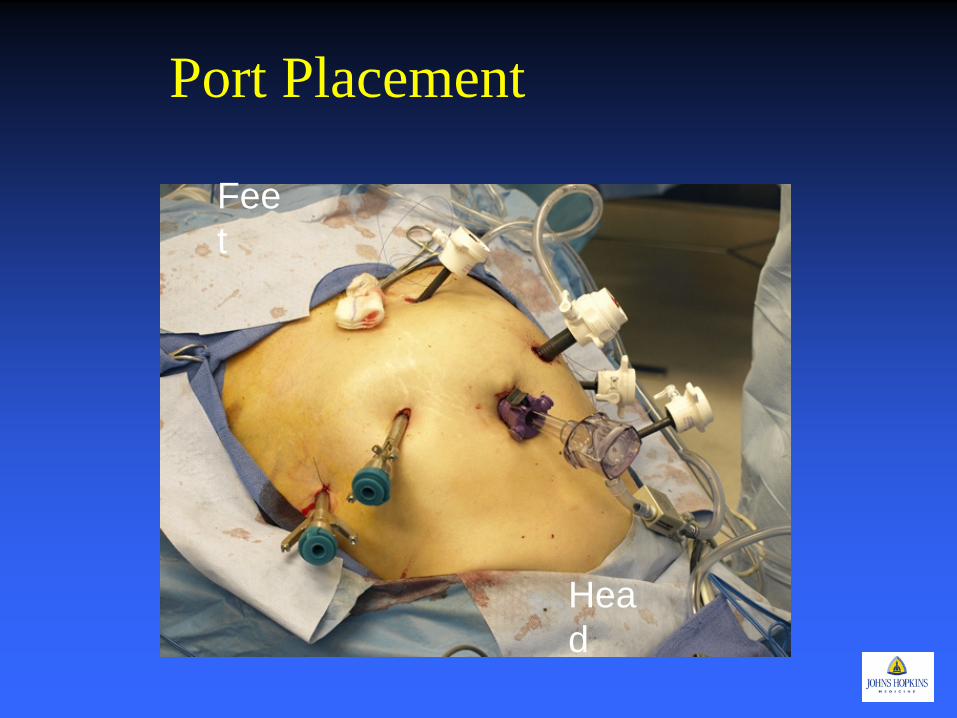
Port Placement
5-12 mm lap port
8 mm robot port
5 mm lap port
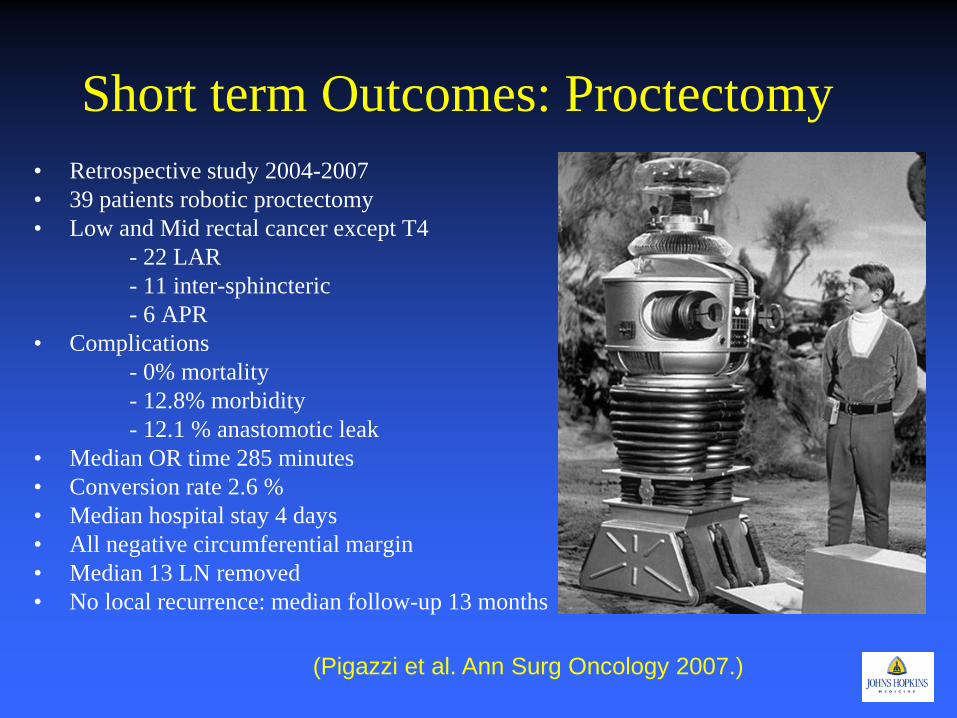
Short term Outcomes: Proctectomy • Retrospective study 2004-2007 • 39 patients robotic proctectomy • Low and Mid rectal cancer except T4 - 22 LAR - 11 inter-sphincteric - 6 APR • Complications - 0% mortality - 12.8% morbidity - 12.1 % anastomotic leak • Median OR time 285 minutes • Conversion rate 2.6 % • Median hospital stay 4 days • All negative circumferential margin • Median 13 LN removed • No local recurrence: median follow-up 13 months
(Pigazzi et al. Ann Surg Oncology 2007.)
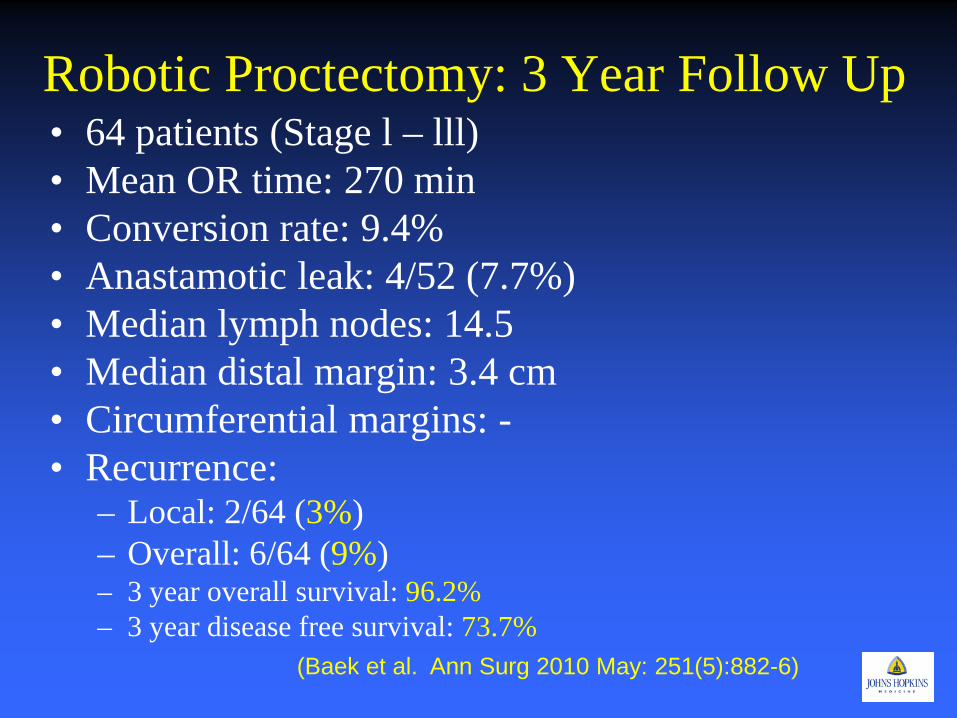
Robotic Proctectomy: 3 Year Follow Up • 64 patients (Stage l – lll) • Mean OR time: 270 min • Conversion rate: 9.4% • Anastamotic leak: 4/52 (7.7%) • Median lymph nodes: 14.5 • Median distal margin: 3.4 cm • Circumferential margins: - • Recurrence:
– Local: 2/64 (3%) – Overall: 6/64 (9%) – 3 year overall survival: 96.2% – 3 year disease free survival: 73.7%
(Baek et al. Ann Surg 2010 May: 251(5):882-6)
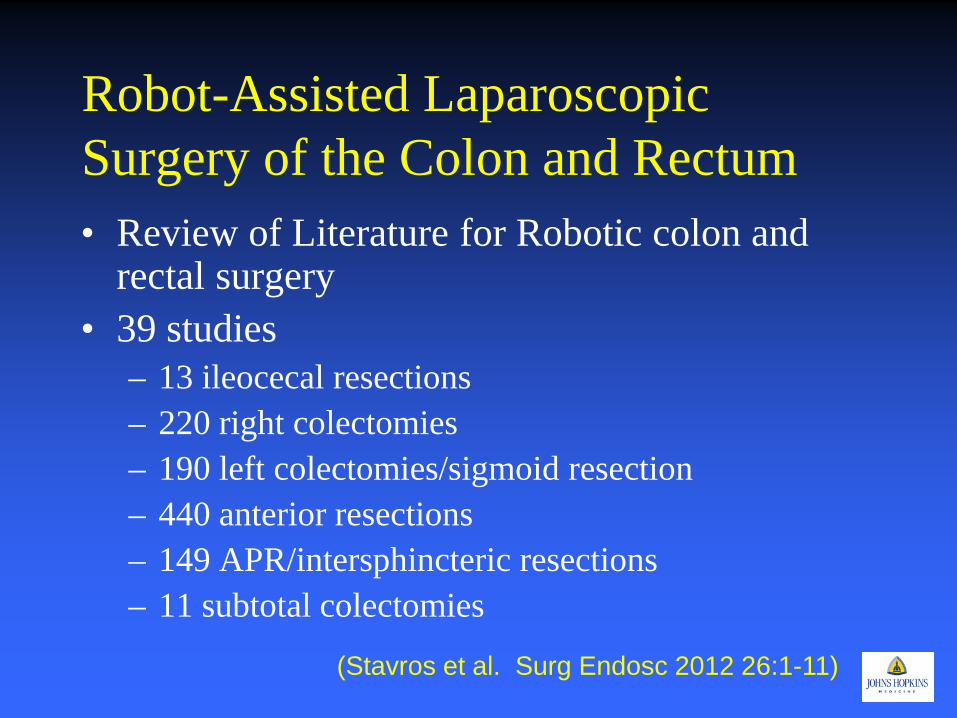
Robot-Assisted Laparoscopic Surgery of the Colon and Rectum • Review of Literature for Robotic colon and
rectal surgery • 39 studies
– 13 ileocecal resections – 220 right colectomies – 190 left colectomies/sigmoid resection – 440 anterior resections – 149 APR/intersphincteric resections – 11 subtotal colectomies
(Stavros et al. Surg Endosc 2012 26:1-11)
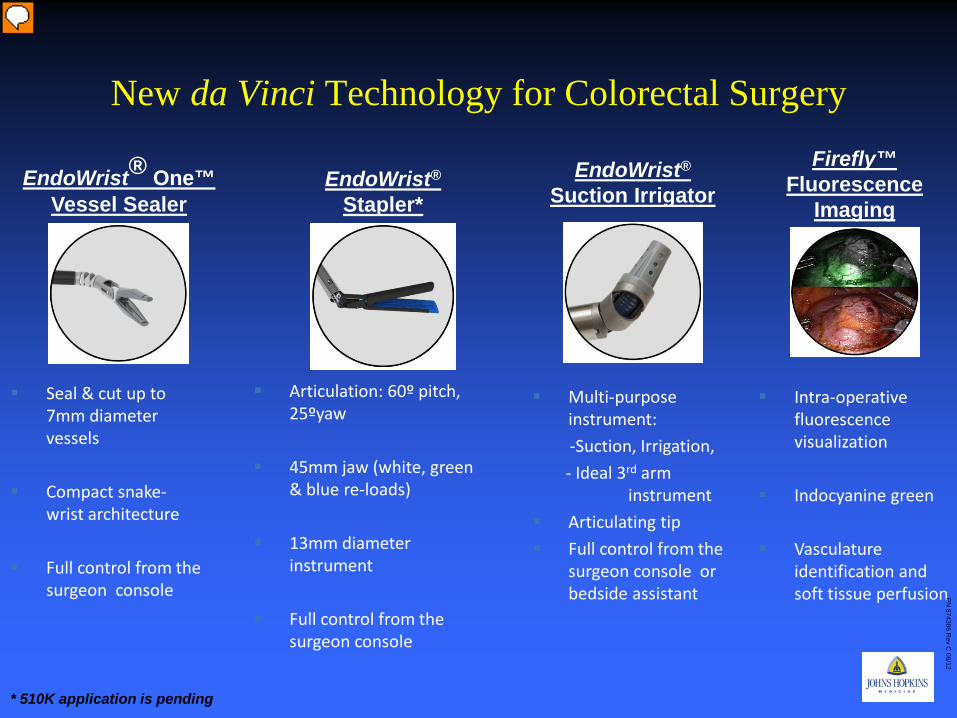
New da Vinci Technology for Colorectal Surgery
Seal & cut up to 7mm diameter vessels
Compact snake-wrist architecture
Full control from the surgeon console
Articulation: 60º pitch, 25ºyaw
45mm jaw (white, green & blue re-loads)
13mm diameter instrument
Full control from the surgeon console
EndoWrist® One™ Vessel Sealer
EndoWrist® Stapler*
* 510K application is pending
EndoWrist® Suction Irrigator
Multi-purpose instrument:
-Suction, Irrigation, - Ideal 3rd arm
instrument Articulating tip Full control from the
surgeon console or bedside assistant
Firefly™ Fluorescence
Imaging
Intra-operative fluorescence visualization
Indocyanine green
Vasculature identification and soft tissue perfusion
PN
874386 Rev C
06/12
Presenter
Presentation Notes
Script: Overall, we are very excited about the new products we recently launched and a few others that are in our development pipeline. We believe these instruments will further improve patient outcomes due to the precision and dexterity they will provide to the console surgeon. These instruments will also reduce the OR times even further and will further reduce the skill level needed at the bedside The EndoWrist Vessel Sealer will be able to seal and cut up to 7 mm vessels, and will be fully controlled by the console surgeon. The EndoWrist Stapler will be a game changing instrument and will overcome surgical challenges that surgeons currently experience in both lap and open surgery. The instrument offers: precision, surgeon control, articulation to allow access deep in the pelvis or around critical anatomy, and intelligent tip sensing to ensure appropriate tissue gap prior to firing the stapler. The new da Vinci Suction/Irrigator– already FDA-approved – will also enable the console surgeon to clear his operating field on his own - providing full autonomy. Firefly technology will provide additional intraoperative value in assessing vasculature identification and perfusion. Probing Questions: What are your thoughts on the impact of these instruments on the wider adoption of da Vinci in colorectal surgery? Do you think the features of these product may improve the surgical outcomes such as leakage, or conversion?
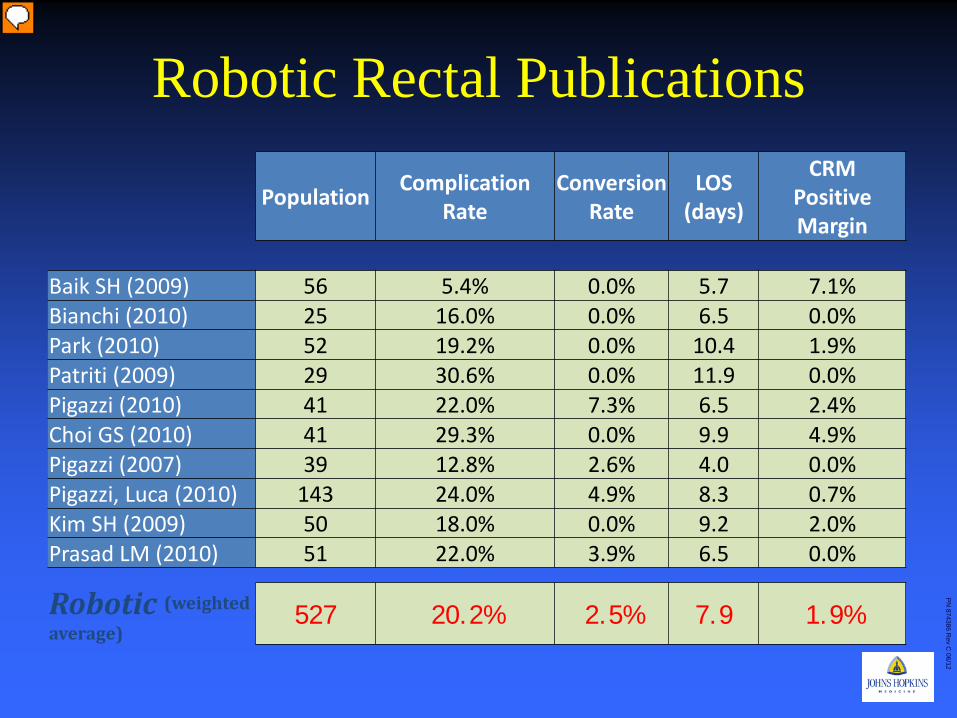
Robotic Rectal Publications
Population Complication Rate
Conversion Rate
LOS (days)
CRM Positive Margin
Baik SH (2009) 56 5.4% 0.0% 5.7 7.1% Bianchi (2010) 25 16.0% 0.0% 6.5 0.0% Park (2010) 52 19.2% 0.0% 10.4 1.9% Patriti (2009) 29 30.6% 0.0% 11.9 0.0% Pigazzi (2010) 41 22.0% 7.3% 6.5 2.4% Choi GS (2010) 41 29.3% 0.0% 9.9 4.9% Pigazzi (2007) 39 12.8% 2.6% 4.0 0.0% Pigazzi, Luca (2010) 143 24.0% 4.9% 8.3 0.7% Kim SH (2009) 50 18.0% 0.0% 9.2 2.0% Prasad LM (2010) 51 22.0% 3.9% 6.5 0.0%
Robotic (weighted average)
527 20.2% 2.5% 7.9 1.9%
Population Complication Rate
Conversion Rate
LOS (days)
CRM Positive Margin
PN
874386 Rev C
06/12
Presenter
Presentation Notes
Script: And, a more broad analysis of robotic rectal cancer publications reveal very promising outcomes. An internal analysis by taking a weighted average of these publications compared the outcomes published in MRC Classic randomized trial (2005). <Note> MRC stands for Medical Research Council, it’s an entity in the UK and funds a variety of large trials. The MRC randomized trial on colorectal cancer (patient accrual completed in 2002, results published in 2005) revealed less-than-expected outcomes for laparoscopic colorectal surgery compared to open. This study is widely and globally respected and referenced due to its randomized nature, however it’s also thought to hamper the adoption of laparoscopy in colorectal surgery. And although this comparison is not apples-to-apples, it still highlights quiet a difference between these three different modalities from positive margin rates to conversions, from complication rate to length of stay.
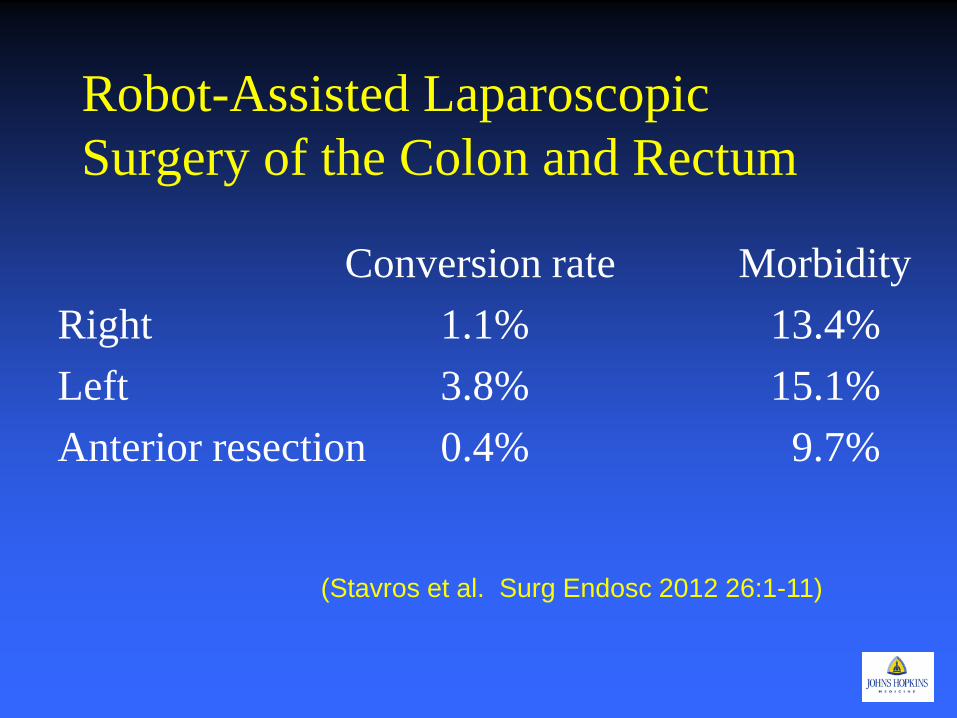
Robot-Assisted Laparoscopic Surgery of the Colon and Rectum
Conversion rate Morbidity Right 1.1% 13.4% Left 3.8% 15.1% Anterior resection 0.4% 9.7%
(Stavros et al. Surg Endosc 2012 26:1-11)
SILS
• Minimal data • Retrospective small series and case reports • No definitive benefit over other MIS
techniques • Most data on Right colectomies for colon
cancer
© 2012 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
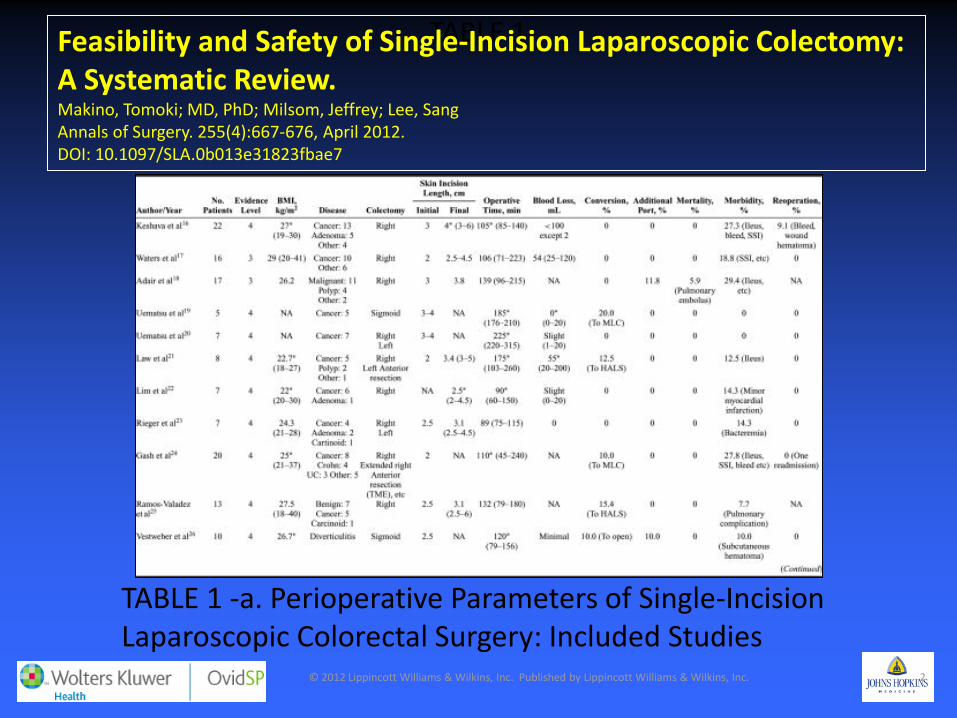
TABLE 1 Feasibility and Safety of Single-Incision Laparoscopic Colectomy: A Systematic Review. Makino, Tomoki; MD, PhD; Milsom, Jeffrey; Lee, Sang Annals of Surgery. 255(4):667-676, April 2012. DOI: 10.1097/SLA.0b013e31823fbae7
TABLE 1 -a. Perioperative Parameters of Single-Incision Laparoscopic Colorectal Surgery: Included Studies
© 2012 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
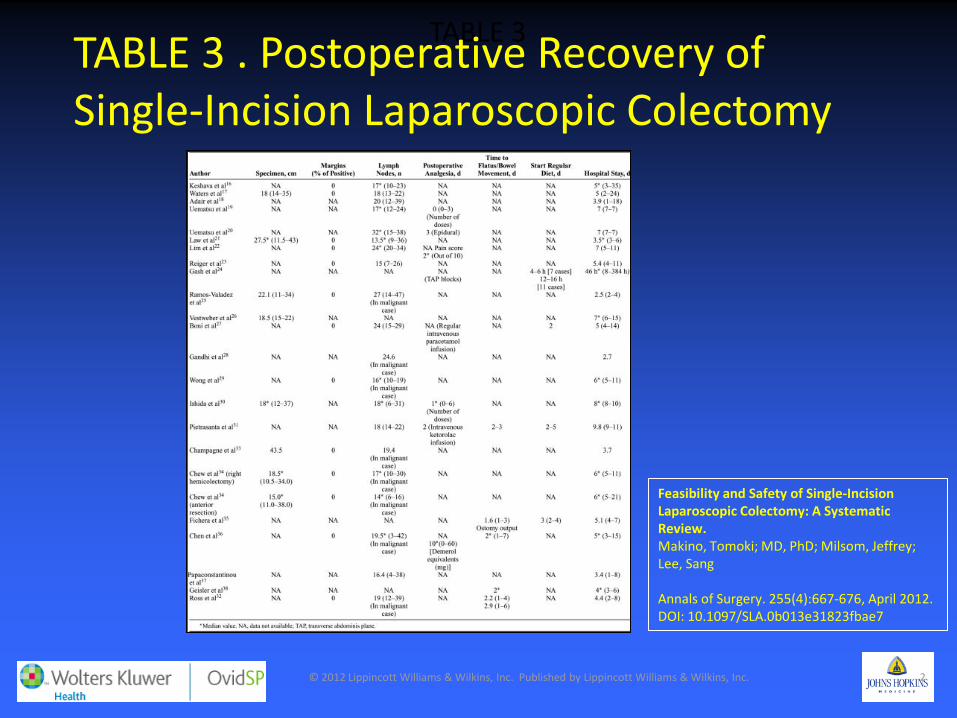
TABLE 3
Feasibility and Safety of Single-Incision Laparoscopic Colectomy: A Systematic Review. Makino, Tomoki; MD, PhD; Milsom, Jeffrey; Lee, Sang Annals of Surgery. 255(4):667-676, April 2012. DOI: 10.1097/SLA.0b013e31823fbae7
TABLE 3 . Postoperative Recovery of Single-Incision Laparoscopic Colectomy
The Future “To boldly go where no man has gone before”
Captain James T. Kirk
“Steel isn’t the answer to a systemic biological disease”
Gershon Efron MD
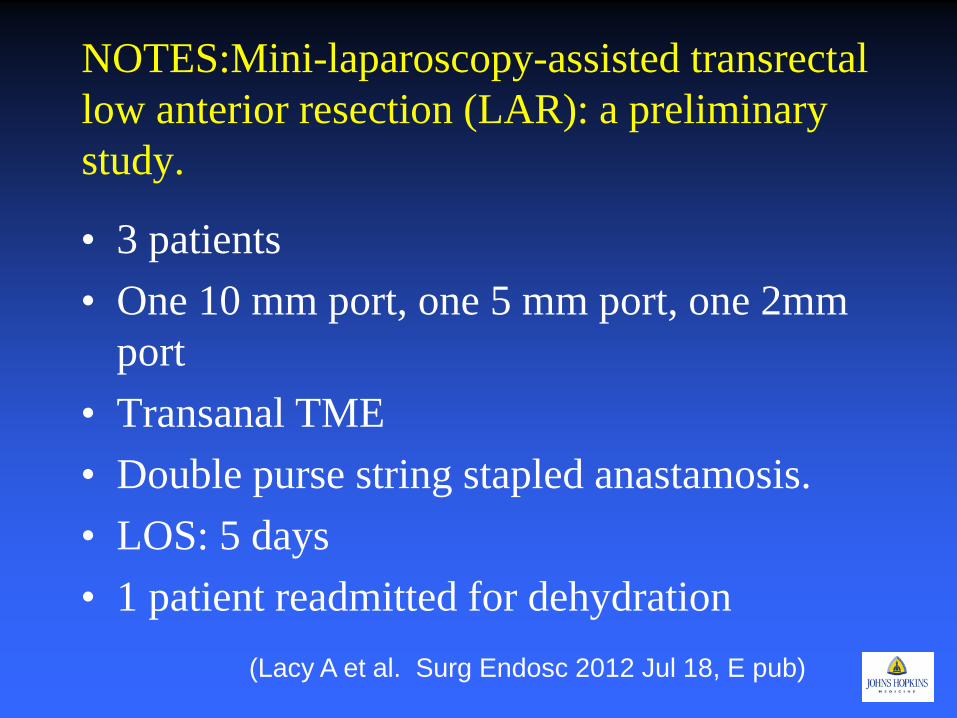
NOTES:Mini-laparoscopy-assisted transrectal low anterior resection (LAR): a preliminary study.
• 3 patients • One 10 mm port, one 5 mm port, one 2mm
port • Transanal TME • Double purse string stapled anastamosis. • LOS: 5 days • 1 patient readmitted for dehydration
(Lacy A et al. Surg Endosc 2012 Jul 18, E pub)
Incisionless: No Surgery • Predictors of complete response
– Tumor markers – Inflammatory markers – Treatment regimine
• Adequate post treatment assessment: determine cpr – MRI – PET/CT – Endoscopy
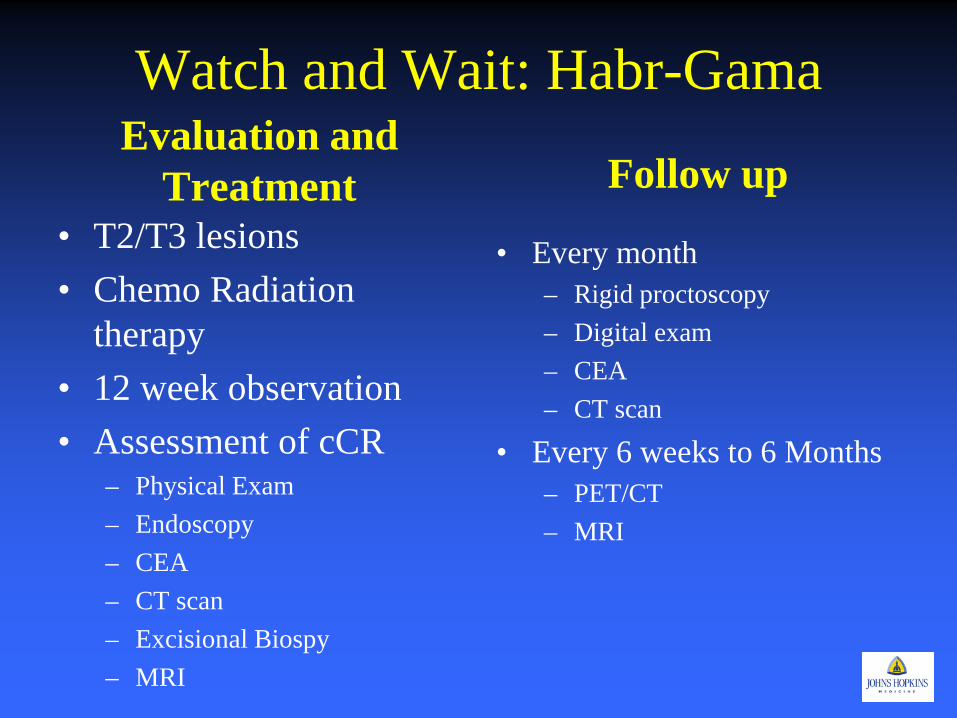
Watch and Wait: Habr-Gama Evaluation and
Treatment • T2/T3 lesions • Chemo Radiation
therapy • 12 week observation • Assessment of cCR
– Physical Exam – Endoscopy – CEA – CT scan – Excisional Biospy – MRI
Follow up
• Every month – Rigid proctoscopy – Digital exam – CEA – CT scan
• Every 6 weeks to 6 Months – PET/CT – MRI
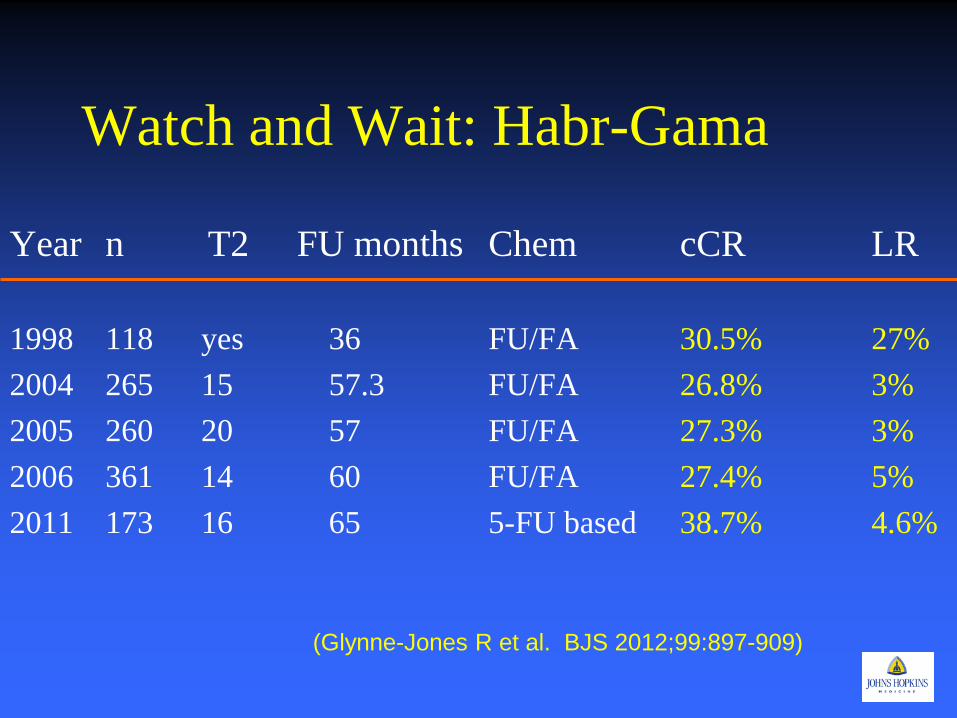
Watch and Wait: Habr-Gama
Year n T2 FU months Chem cCR LR 1998 118 yes 36 FU/FA 30.5% 27% 2004 265 15 57.3 FU/FA 26.8% 3% 2005 260 20 57 FU/FA 27.3% 3% 2006 361 14 60 FU/FA 27.4% 5% 2011 173 16 65 5-FU based 38.7% 4.6%
(Glynne-Jones R et al. BJS 2012;99:897-909)
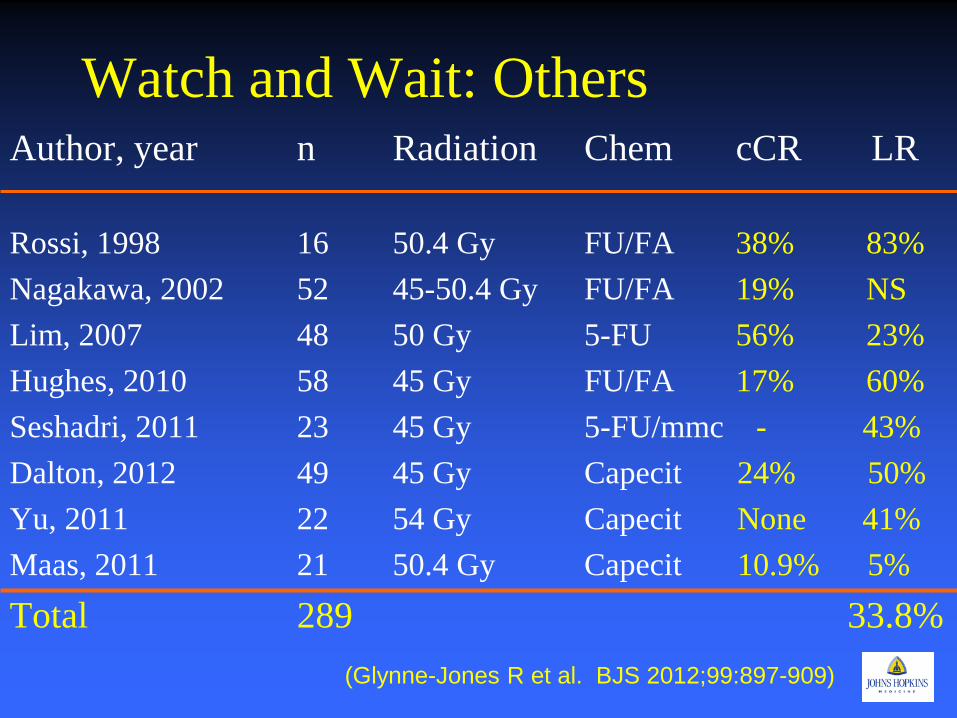
Watch and Wait: Others Author, year n Radiation Chem cCR LR Rossi, 1998 16 50.4 Gy FU/FA 38% 83% Nagakawa, 2002 52 45-50.4 Gy FU/FA 19% NS Lim, 2007 48 50 Gy 5-FU 56% 23% Hughes, 2010 58 45 Gy FU/FA 17% 60% Seshadri, 2011 23 45 Gy 5-FU/mmc - 43% Dalton, 2012 49 45 Gy Capecit 24% 50% Yu, 2011 22 54 Gy Capecit None 41% Maas, 2011 21 50.4 Gy Capecit 10.9% 5% Total 289 33.8%
(Glynne-Jones R et al. BJS 2012;99:897-909)
Where we stand • Some evidence to suggest similar oncological
results when comparing MIS to open TME. • Evidence to show benefits seen with other MIS
colectomy procedures. • Guidelines for laparoscopic colectomies for cancer
should be extrapolated • Possibly avoid in obese patients or those with
large bulky tumors. • Requires advance laparoscopic and colorectal
experience • Preliminary Data on Watch and Wait
– Needs Replication
Where are we going? • Need randomized trials to confirm suspicions. • Japan: JCOG 0404
– Randomized trial comparing lap and open colon and rectal cancer
• Color II – International randomized trial comparing lap and open
rectal cancer • US ACOSOG funded trial
– 500 patient randomized trial comparing lap and open rectal resections
• Multicenter Prospective Data Base on Watch and Wait Patients
• Robotic Prospective Trials – International/Korea
December 19, 2012 57
Johns Hopkins Hospital: New Clinical Buildings
Opened April 30, 2012
Johns Hopkins Hospital Opened 1883


















