Inhalation Therapy for Stable COPD: 20 Years of GOLD ReportsInhalation Therapy for Stable COPD: 20...
17
REVIEW Inhalation Therapy for Stable COPD: 20 Years of GOLD Reports Paul D. Terry . Rajiv Dhand Received: February 8, 2020 / Published online: April 3, 2020 Ó The Author(s) 2020 ABSTRACT The Global Initiative for Chronic Obstructive Lung Disease (GOLD) was formed in the late 1990s to spread awareness of chronic obstruc- tive pulmonary disease (COPD) as a major public health problem and facilitate its preven- tion and treatment. GOLD has since become internationally recognized for the development of evidence-based strategy documents, most notably the annual GOLD Reports, for COPD diagnosis, management, and prevention. The GOLD Reports incorporate the latest evidence and expert consensus to guide the management and prevention of COPD on a global level. Since the first GOLD Report in 2001, profound inno- vations have taken place regarding inhaler device options, available pharmaceuticals, knowledge regarding effective dosages and potential side effects, and the various combi- nations of drugs used to relieve symptoms. Concomitantly, an evolution of expert opinion on how best to apply these innovations to the care of patients with COPD has also taken place, an evolution that is nowhere more detailed or definitive than in the 20 years of annual GOLD Reports. We summarize key features and trends in inhalation therapy for stable COPD in these Reports. Keywords: COPD; GOLD reports; Inhalation therapy Enhanced Digital Features To view enhanced digital features for this article go to https://doi.org/10.6084/ m9.figshare.11940423. P. D. Terry Á R. Dhand (&) Department of Medicine, Graduate School of Medicine, University of Tennessee Medical Center, Knoxville, TN, USA e-mail: [email protected]; [email protected] Adv Ther (2020) 37:1812–1828 https://doi.org/10.1007/s12325-020-01289-y
Transcript of Inhalation Therapy for Stable COPD: 20 Years of GOLD ReportsInhalation Therapy for Stable COPD: 20...

REVIEW
Inhalation Therapy for Stable COPD: 20 Yearsof GOLD Reports
Paul D. Terry . Rajiv Dhand
Received: February 8, 2020 / Published online: April 3, 2020� The Author(s) 2020
ABSTRACT
The Global Initiative for Chronic ObstructiveLung Disease (GOLD) was formed in the late1990s to spread awareness of chronic obstruc-tive pulmonary disease (COPD) as a majorpublic health problem and facilitate its preven-tion and treatment. GOLD has since becomeinternationally recognized for the developmentof evidence-based strategy documents, mostnotably the annual GOLD Reports, for COPDdiagnosis, management, and prevention. TheGOLD Reports incorporate the latest evidence
and expert consensus to guide the managementand prevention of COPD on a global level. Sincethe first GOLD Report in 2001, profound inno-vations have taken place regarding inhalerdevice options, available pharmaceuticals,knowledge regarding effective dosages andpotential side effects, and the various combi-nations of drugs used to relieve symptoms.Concomitantly, an evolution of expert opinionon how best to apply these innovations to thecare of patients with COPD has also taken place,an evolution that is nowhere more detailed ordefinitive than in the 20 years of annual GOLDReports. We summarize key features and trendsin inhalation therapy for stable COPD in theseReports.
Keywords: COPD; GOLD reports; Inhalationtherapy
Enhanced Digital Features To view enhanced digitalfeatures for this article go to https://doi.org/10.6084/m9.figshare.11940423.
P. D. Terry � R. Dhand (&)Department of Medicine, Graduate School ofMedicine, University of Tennessee Medical Center,Knoxville, TN, USAe-mail: [email protected]; [email protected]
Adv Ther (2020) 37:1812–1828
https://doi.org/10.1007/s12325-020-01289-y

Key Summary Points
The Global Initiative for ChronicObstructive Lung Disease (GOLD) isinternationally recognized for thedevelopment of evidence-based strategydocuments, most notably the annualGOLD Reports
The GOLD Reports incorporate the latestevidence and expert consensus to guidethe management and prevention of COPDon a global level
The 20 years during which GOLDpublished their annual Reports has been aperiod of remarkable innovation andrefinement of inhalation therapy forCOPD
The GOLD Reports document profoundevolutions in the armamentarium ofinhaled drugs in all categories ofinhalation devices; the use of long-acting,combination, and triple therapies;algorithms for initial and follow-uptreatment; the acceptance of nebulizers inregular maintenance therapy; and theemphasis on inhalation device choice,technique, and adherence, all of which aredesigned to optimize outcomes in COPDmanagement
We summarize key features and trends ininhalation therapy for stable COPD inthese Reports
INTRODUCTION
The GOLD Expert Panel, a distinguishedgroup of health professionals from thefields of respiratory medicine, epidemiol-ogy, socioeconomics, public health, andhealth education, reviewed existing COPDguidelines, as well as new information onpathogenic mechanisms of COPD as theydeveloped a consensus document. Many
recommendations will require additionalstudy and evaluation as the GOLD pro-gram is implemented.–Claude Lenfant, MD, Director, NationalHeart, Lung, and Blood Insti-tute,1982–2003 [1].
The Global Initiative for Chronic ObstructiveLung Disease (GOLD) has its origins as aNational Heart, Lung, and Blood Institute- andWorld Health Organization-sponsored ‘‘thinktank,’’ formed in the late 1990s to spreadawareness of chronic obstructive pulmonarydisease (COPD) as a major public health prob-lem and facilitate its prevention and treatment[2]. GOLD has since become internationallyrecognized for the development of evidence-based strategy documents, most notably theannual GOLD Reports, for COPD diagnosis,management, and prevention. The GOLDReports incorporate the latest evidence andexpert consensus to guide the management andprevention of COPD on a global level [3].
The first annual GOLDReport, Global Strategyfor Diagnosis, Management and Prevention ofCOPD was issued in 2001. The GOLD ScienceCommittee, comprising recognized leaders inCOPD research and clinical practice, was estab-lished shortly thereafter to review publishedresearch findings and evaluate their impact onrecommendations in the subsequent GOLD doc-uments. The evaluation of science and method-ology behind each of the annual Gold Reportrevisions involves, at a minimum, review anddiscussion of literature twice a year by the ScienceCommittee, as well as rewriting and updatingcontent as it relates to the literature review. Therewas no annual Report issued by GOLD in 2002 or2012. Thus, the most recent GOLD Report, for2020, made available in December 2019 (https://goldcopd.org), marks the 18th report to havecontributed substantially towards meetingGOLD’s founding goals ‘‘to increase awareness ofCOPD and help the thousands of patients whosuffer from this disease and die prematurely fromCOPD or its complications [2].’’
Patients with COPD rely heavily on inhaledbronchodilators and inhaled corticosteroids(ICS) to control symptoms, maximize theirquality of life, and avoid exacerbations and
Adv Ther (2020) 37:1812–1828 1813

costly hospitalizations. Since the first GOLDReport in 2001, profound innovations havetaken place regarding inhaler device options,available pharmaceuticals, knowledge regardingeffective dosages and potential side effects, andthe various combinations of drugs used torelieve symptoms. Concomitantly, an evolutionof expert opinion on how best to apply theseinnovations to the care of patients with COPDhas also taken place, an evolution that isnowhere more detailed or definitive than in the20 years of annual GOLD Reports.
Oral therapies considered in the GOLDReports include methylxanthines (amino-phylline, theophylline), phosphodiesterase 4inhibitors (roflumilast), and mucolytic agents(erdosteine, carbocysteine, N-acetylcysteine).Our focus is on inhaled therapies, however,which are faster in onset than oral therapies,have less side effects, are more commonly used,and are often considered more effective in thelong-term management of symptoms inpatients with stable COPD.
Our aim here is not to distill GOLD’s treat-ment recommendations for clinical use. Rather,because the collective GOLD Reports providecontext and perspective on the ever-expandingtreatment choices facing patients and theirproviders, we summarize key features andtrends in inhalation therapy for stable COPD inthese Reports. This article is based on previouslyconducted studies and does not contain anystudies with human participants or animalsperformed by any of the authors.
A NOTE ON METHODSAND THE GOLD REPORTS FORMAT
Relevant Chapters
The first GOLD Report (2001) comprised sixchapters: (1) Definition; (2) Burden of COPD;(3) Risk Factors; (4) Pathogenesis, Pathology andPathophysiology; (5) Management of COPD;and (6) Future Directions. Chapter 5, Manage-ment of COPD, comprised four components: (1)Assess and Monitor Disease; (2) Reduce RiskFactors; (3) Manage Stable COPD; and (4)Manage Exacerbations. In this report, our
primary focus is on the pharmacological treat-ments discussed in the third component of thischapter: ‘‘Manage Stable COPD.’’ In 2011, a newchapter, ‘‘Therapeutic Options,’’ was added,which then contained the specific informationon pharmacological therapies; the chapter wasretitled ‘‘Evidence Supporting Prevention andMaintenance Therapy’’ in 2017.
Levels of Evidence
At various places in each Report, the GOLDScience Committee qualifies the level of evi-dence supporting COPD management recom-mendations hierarchically from ‘‘A’’ (highest) to‘‘D’’ (lowest). We refer to these levels of evidencewhen highlighting certain GOLD recommen-dations in our discussion. Levels of evidence aredefined by GOLD on the basis of the followingdata sources:
A Large, well-designed randomized controlledtrials (RCTs) with no perceived importantsource of bias
B RCTs with limited numbers of patients,limited duration of follow-up, limitedconsistency of study results, and/or withperceived methodological weaknesses
C Non-randomized trials and observationalstudies
D Panel consensus judgment based on clinicalexperience or knowledge that does notmeet the above criteria; the availableclinical literature is insufficient
COPD Severity of Airflow Limitationand Pharmacological ManagementClassifications
The first GOLD Report (2001) used the follow-ing severity of airflow designation for patientswith COPD based on spirometric assessment: 0.At Risk; (1) Mild; (2) Moderate; (3) Severe. In2003, a fourth category was added: (4) VerySevere. In 2006, the category ‘‘At Risk’’ was nolonger used. The four remaining categories havebeen used in GOLD Reports through 2020. Inthe 2011 Report, GOLD stated: ‘‘In previousversions of the GOLD Report, COPD treatment
1814 Adv Ther (2020) 37:1812–1828

recommendations were based on spirometryonly. This is in keeping with the fact that mostof the clinical trial evidence about treatmentefficacy in COPD is oriented around baselineFEV1 (forced expiratory volume in one second).However, FEV1 alone is a poor descriptor ofdisease status and for this reason the treatmentstrategy for stable COPD should also consideran individual patient’s symptoms and futurerisk of exacerbations.’’ With this, GOLD pre-sented a new model for the initiation of phar-macological management of COPD accordingto both the spirometric classification and theindividualized assessment of symptoms andexacerbation risk:
Group A Less symptoms, low riskGroup B More symptoms, low riskGroup C Less symptoms, high riskGroup D More symptoms, high risk
A refined version of the ABCD AssessmentTool is presented in the GOLD 2020 Report(Fig. 1).
Formulations and Typical Doses of COPDMedications
A table in the 2001 GOLD Report ‘‘CommonlyUsed Formulations of Bronchodilator Drugs’’listed the generic drug name, the inhaler type—or nebulizer—used to deliver the drug, thecommon dose or dose range for each, and theexpected duration of action. A footnote to thetable noted that not all formulations and dosesare available or typical in all countries. Thistable exists in all GOLD Reports to date, albeitwith modifications within each of the cate-gories over time in accordance with the avail-able scientific evidence. In 2010, the title of thetable changed to ‘‘Formulations and TypicalDoses of COPD Medications,’’ and in 2017 to‘‘Commonly Used Maintenance Medications inCOPD.’’ Starting in 2019, typical doses of listeddrugs were no longer provided. Whereas weselectively cite information from these tables inour discussion, we do not reiterate GOLD’s jus-tification for including or excluding specificdrugs (Tables 1, 2, 3, 4).
INHALED PHARMACOLOGICALTHERAPY IN GOLD
Inhaled Bronchodilators
Inhaled bronchodilators are central tosymptom management and commonlygiven on a regular basis to prevent orreduce symptoms. Bronchodilators act byaltering airway smooth muscle tone andthe improvements in expiratory flowreflect widening of the airways rather thanchanges in lung elastic recoil. Bron-chodilators tend to reduce dynamichyperinflation at rest and during exerciseand improve exercise performance.–GOLD Report, 2020
As noted by GOLD, inhaled bronchodilatorsare used to prevent and control symptoms,reduce the frequency and severity of exacerba-tions, improve health status, and improveexercise tolerance. GOLD Reports consistentlynote, however, that no drug or combination ofdrugs has been shown conclusively to decreasethe rate of patients’ long-term decline in lungfunction. The 2009 and 2010 GOLD Reportsnoted limited evidence (Evidence B) that regu-lar treatment with long-acting b2-agonists(LABAs), inhaled corticosteroids (ICS), and/ortheir combination can decrease the rate ofdecline of lung function. However, subsequentevidence has not supported this suggestion andthe association was not noted in subsequentReports. The most recent GOLD Report (GOLD,2020), however, cites evidence to suggest thattriple inhaled therapy, specifically triple com-binations of a LABA, a long-acting muscarinicantagonist (LAMA), and an ICS, may reducemortality among patients with the most severestages of COPD (see ‘‘Triple Therapy’’).
Discussion of inhaled bronchodilators isfound in all GOLD Reports under four mainheadings: b2-Agonists; Anticholinergics (orAntimuscarinics or Muscarinic antagonists);Inhaled corticosteroids; and Combinationbronchodilator therapy. We address each ofthese four treatment categories below, focusingmore on drug effectiveness than side effects.
Adv Ther (2020) 37:1812–1828 1815

b2-Agonists
The principal action of beta2-agonists is torelax airway smooth muscle by stimulatingbeta2-adrenergic receptors, which increa-ses cyclic AMP and produces functionalantagonism to bronchoconstriction. Thereare short-acting (SABA) and long-acting(LABA) beta2-agonists. The effect of SABAsusually wears off within 4 to 6 h.–GOLD Report, 2020
The first GOLD Report (2001) listed five b2-agonists (in the table ‘‘Commonly Used For-mulations of Bronchodilator Drugs’’): SABAsfenoterol, albuterol, terbutaline, and LABAsformoterol, and salmeterol (Table 1). Typicaldoses for pressurized metered-dose inhaler(pMDI)-delivered and nebulizer-delivered drugs
were provided; dry powder inhaler (DPI)-speci-fic dose information was added in 2003.Henceforth divided under ‘‘short-acting’’ and‘‘long-acting’’ headings, this list grew to includeSABA levalbuterol (2007), and LABAs arfor-moterol (2009), indacaterol (2010), vilanterol(2014, in combination with umeclidinium), andolodaterol (2016). Changes in the typical dosesof these drugs occurred over successive reports,including the discontinuation of nebulizedterbutaline after 2001 and pMDI-delivered for-moterol after 2016.
Anticholinergics/Antimuscarinics/Muscarinic Antagonists
Antimuscarinic drugs block the bron-choconstrictor effects of acetylcholine onM3 muscarinic receptors expressed in
THE REFINED ABCD ASSESSMENT TOOL
FIGURE 2.4
SpirometricallyConfirmed Diagnosis
Assessment ofsymptoms/riskAssessment of
Post-bronchodilatorFEV₁/FVC < 0.7
Moderate or Severe
≥2 or≥ 1 leadingto hospitaladmission
0 or 1(not leadingto hospitaladmission)
C D
A B
Symptoms
mMRC 0-1CAT < 10
mMRC ≥ 2CAT ≥ 10
FEV₁(% predicted)
GOLD 1 ≥ 80
GOLD 2 50-79
GOLD 3 30-49
GOLD 4 < 30
Grade
Fig. 1 The refined ABCD assessment tool
1816 Adv Ther (2020) 37:1812–1828

airway smooth muscle. Short-actingantimuscarinics (SAMAs), namely iprat-ropium and oxitropium, also block theinhibitory neuronal receptor M2, whichpotentially can cause vagally inducedbronchoconstriction. Long-acting mus-carinic antagonists (LAMAs), such as tio-tropium, aclidinium, glycopyrroniumbromide and umeclidinium have pro-longed binding to M3 muscarinic recep-tors, with faster dissociation from M2
muscarinic receptors, thus prolonging theduration of bronchodilator effect.–GOLD Report, 2020
The initial GOLD Report (2001) listed twoanticholinergics in common use at that time,both short-acting: ipratropium bromide andoxitropium bromide (Table 2). These two drugsremain the only SAMAs listed in the 2020 Report.Several LAMAs were subsequently added: tio-tropium in 2003; aclidinium bromide and gly-copyrronium bromide in 2013; umeclidinium in
Table 1 b2-Agonists devices and doses for treating patients with stable COPD in the GOLD Reports, 2001–2020
b2-Agonists Inhaler (lg) Solution for nebulizer (mg/ml)
Duration of action (h)
Short actinga,b
Fenoterol 100–200 (pMDI) 0.5–2.0 to 1c 4–6
Albuterol
(salbutamol)
100–200 (pMDI and DPI) 2.5–5.0 to 5d 4–6
Terbutaline 250–500 to 400–500e (DPI) 5–10f 4–6
Levalbuterolg 45–90 (pMDI) 0.6, 1.25 to 0.21, 0.42g 6–8
Long actinga,b
Formoterol 12–24 to 4.5–12h (pMDI and DPI)i 12
Salmeterol 50–100 to 25–50j (pMDI and DPI) 12
Arformoterolk 0.0075 12
Indacateroll 150–300 to 75–300 (DPI)m 24
Olodateroln 5 (SMI) 24
Specific doses were no longer shown in ‘‘Commonly Used Maintenance Medications in COPD’’ after 2018a Short- vs. long-acting formulations were separated into categories in 2003b DPI-specific dose information was added in 2003; the 2001 Report listed pMDI doses onlyc Nebulized solution dose for fenoterol changed from 0.5–2.0 to 1 mg/ml in 2003d Nebulized solution dose for albuterol changed from 2.5–5.0 to 5 mg/ml in 2003e pMDI dose for terbutaline changed from 250–500 lg to 400–500 lg in 2003f Nebulized solution of terbutaline was discontinued after 2001g Nebulized solution of levalbuterol was added in 2007 and changed from 0.63 or 1.25 to 0.21 or 0.42 mg/ml; levalbutrolpMDI was added in 2008h pMDI dose for formoterol changed from 12–24 lg to 4.5–12 lg (pMDI and DPI) in 2003i pMDI formulation of formoterol was discontinued after 2016; DPI dose changed to 4.5–9 lg in 2017j pMDI dose for salmeterol changed from 50–100 lg to 25–50 lg in 2003k Arformoterol was added in 2008l Indacaterol was added in 2010m DPI dose of Indacaterol was changed in 2011 to 75–300 lgn Olodaterol was added in 2016
Adv Ther (2020) 37:1812–1828 1817

2016; glycopyrrolate and revefenacin in 2020.Other changes over time include those related tospecific doses of drugs, and additions and dis-continuations of a delivery device for a specificdrug, such as the addition (2003) and subsequentdiscontinuation (2017) of a nebulized solution ofoxitropium bromide.
Inhaled Corticosteroids (ICS)
In vitro evidence suggests that COPD-as-sociated inflammation has limited
responsiveness to corticosteroids. More-over, some drugs including b2-agonists…may partially facilitate corticosteroid sen-sitivity in COPD. The clinical relevance ofthis effect has not yet been fullyestablished.–GOLD Report, 2020
In 2001, GOLD suggested that regular treat-ment with ICS was only appropriate for symp-tomatic patients with COPD and a documentedspirometric response to ICS. In 2003, thisstatement was clarified to exclude all but
Table 2 Anticholinergics, devices, and doses for treating patients with stable COPD in the GOLD Reports, 2001–2020
Anticholinergics Inhaler (lg) Solution for nebulizer (mg/ml) Duration of action (h)
Short actinga,b
Ipratropium bromide 40–80 to 20, 40c (pMDI) 0.25–0.5 6–8
Oxitropium bromide 200 to 100d (pMDI) 1.5e 7–9
Long actinga
Tiotropiumf 18 (DPI) 24
5 (SMI)g 24
pMDI
Aclidinium bromideh 322 to 400 DPI, 400 pMDIi 12
Glycopyrronium bromidej 44 (DPI) 24 to 12–24k
Umeclidiniuml 62.5 (DPI) 24
Glycopyrrolatem 12
Revefenacinn 24
Specific doses were no longer shown in ‘‘Commonly Used Maintenance Medications in COPD’’ after 2018a Short- vs. long-acting formulations were separated into categories in 2003b DPI-specific dose information was added in 2003; the 2001 Report listed pMDI doses onlyc Ipratropium dose changed from 40–80 to 20 or 40 lg in 2003d Oxitropium dose changed from 200 to 100 lg in 2003e Oxitropium solution for nebulizer was added in 2003; it was discontinued in 2017f Tiotropium was added in 2003; pMDI formulation was added in 2020g Soft mist inhaler (SMI) formulation for tiotropium was added in 2009h Aclidinium bromide was added in 2013i Aclidinium dose (DPI) changed from 322 to 400 lg in 2017; pMDI dose of 400 lg was added in 2017j Glycopyrronium bromide was added in 2013k Glycopyrronium dose was changed to 15.6 and 50 lg (DPI) and duration of action was changed from 24 to 12–24 h in2017l Umeclidinium was added in 2015m Glycopyrrolate was added in 2020 as a nebulizer solutionn Revefenacin was added in 2020 as a nebulizer solution
1818 Adv Ther (2020) 37:1812–1828

symptomatic patients with COPD and an FEV1
of less than 50% predicted and repeated exac-erbations (Evidence A). The 2003 Report alsonoted the results of a few studies suggesting thatregular treatment with ICS reduces all-causemortality. As mentioned earlier, later GOLDReports did not find sufficient evidence toclearly support this hypothesis.
The initial GOLD Report (2001) listed fourICS as potential treatments for patients withstable COPD: Beclomethasone, Budesonide,Fluticasone, Triamcinolone (Table 3). Fluticas-one was discontinued after 2006. Later GOLDReports noted that ICS are less effective alonethan in combination with a LABA in improvinglung function and health status in patients withexacerbations and moderate to very severeCOPD (Evidence A). It was also noted that moststudies found that regular treatment with ICSalone did not modify long-term decline of FEV1
or mortality in patients with COPD. The 2011Report stated, ‘‘Long-term monotherapy withinhaled corticosteroids is not recommended inCOPD because it is less effective than the com-bination of inhaled corticosteroids with LABAs(Evidence A).’’ After 2016, ICS were listed in‘‘Commonly Used Maintenance Medications inCOPD’’ only in combination with drugs of otherclasses; ICS as a discrete therapy was no longerlisted. Notwithstanding, the 2019 Report notedthe results of a study that found fluticasonefuroate alone was associated with slower declinein FEV1 compared with placebo or vilanterolalone in moderate COPD.
Effect Modification by Blood Eosinophil LevelIn 2017, GOLD noted that high blood eosino-phil levels may be a useful biomarker to predictefficacy of ICS, and hence inform treatmentdecisions. The Report cited evidence thatshowed a reduction of exacerbations from aLABA/ICS combination versus only a LABA oronly a LAMA was greater in patients with higherblood eosinophil counts; however, further evi-dence was needed. By 2019, GOLD noted addi-tional evidence that blood eosinophil countspredict the magnitude of the effect of ICS,added on top of regular maintenance bron-chodilator treatment, in preventing futureexacerbations. GOLD further noted: ‘‘There is acontinuous relationship between blood eosino-phil counts and ICS effects; no and/or smalleffects are observed at lower eosinophil counts,with incrementally increasing effects observedat higher eosinophil counts. Data modellingindicates that ICS-containing regimens havelittle or no effect at a blood eosinophilcount\100 cells/lL, therefore this thresholdcan be used to identify patients with a lowlikelihood of treatment benefit with ICS. Thethreshold of a blood eosinophilcount[300 cells/lL identifies the top of thecontinuous relationship between eosinophilsand ICS, and can be used to identify patientswith the greatest likelihood of treatment benefitwith ICS.’’ However, by 2020, GOLD still cau-tioned that: ‘‘There is insufficient evidence torecommend that blood eosinophils should beused to predict future exacerbation risk on anindividual basis in COPD patients.’’
Table 3 Inhaled corticosteroids, devices, and doses for treating patients with stable COPD in the GOLD Reports,2001–2020
ICSa Inhaler (lg) Solution for nebulizer (mg/ml)
Beclomethasone 50–400 (pMDI and DPI) 0.2–0.4
Budesonide 100, 200, 400 (DPI) 0.20, 0.25, 0.5
Fluticasone 50–500 (pMDI and DPI)
Triamcinoloneb 100 (pMDI) 40
a Inhaled corticosteroids were only listed in combination with other drugs after 2016 (see Table 4)b Triamcinolone was discontinued after 2009
Adv Ther (2020) 37:1812–1828 1819

Table 4 Drug combinations, devices, and doses for treating patients with stable COPD in the GOLD Reports, 2001–2020
Drug Inhaler (lg) Solution for nebulizer(mg/ml)
Duration of action(h)
Combination short-acting b2-agonists plus anticholinergic in one inhaler
Fenoterol/ipratropiuma 200/80 (pMDI) 1.25/0.5 in 4 ml 6–8
Albuterol/ipratropiuma 75/15 (pMDI)b 0.75/4.5 to 0.5, 2.5 in 3 mlc 6–8
100/20 (SMI)d 6–8
Combination long-acting b2-agonists plus anticholinergic in one inhaler
Indacaterol/glycopyrroniume 85/43 (DPI) 24
Vilanterol/umeclidiniumf 25/62.5 (DPI) 24
Formoterol/aclidiniumg 12/340 (DPI) 12
Olodaterol/tiotropiumh 5/5 (SMI) 24
Formoterol/glycopyrroniumi 9.6/14.4 to 9.6/18
(pMDI)
12
Formoterol/glycopyrrolatej 4.8/9 12
Combination long-acting b2-agonists plus glucocorticosteroids in one inhaler
Formoterol/budesonidek 4.5/160 (pMDI
9/320 (DPI)
Formoterol/mometasonel 10/200, 10/400
(pMDI)
Salmeterol/fluticasonem 50/100, 250, 500
(DPI)
25/50, 125, 250
(pMDI)
Vilanterol/fluticasone furoaten 25/100 (DPI)
Formoterol/beclomethasoneo 6/100 (pMDI & DPI)
Triple combination in one device (LABA/LAMA/ICS)p
Fluticasone/umeclidinium/vilanterolq
(DPI)
Beclometasone/formoterol/glycopyrroniumr
(pMDI)
1820 Adv Ther (2020) 37:1812–1828

Effect Modification by Exacerbation HistoryA statement that the treatment effect of ICS-containing regimens is higher in patients withhigh exacerbation risk first appeared in GOLD’s2019 Report, which concluded: ‘‘The use ofblood eosinophil counts to predict ICS effectsshould always be combined with clinicalassessment of exacerbation risk (as indicated bythe previous history of exacerbations).’’
Combination Therapy
Combining bronchodilators with differentmechanisms and durations of action mayincrease the degree of bronchodilationwith a lower risk of side effects comparedto increasing the dose of a singlebronchodilator.–GOLD Report, 2020
Since 2001, several combinations of inhaleddrugs used to treat COPD have been added to
GOLD’s ‘‘Commonly Used Maintenance Medi-cations in COPD’’ (Table 4). The combinationsof drugs listed in the table of each Report arethose available in one inhaler device. Not listedin the tables are combinations involving the useof more than one inhaler device. For example,although not listed in the table, the 2017 Reportnoted that treatment with formoterol and tio-tropium (LABA/LAMA) in separate inhalers wasshown to have a greater impact on FEV1 thaneither component alone.
SABA/SAMAThe first GOLD Report (2001) noted that acombination of a SABA and ipratropium(SAMA) in stable COPD produced greater andmore sustained improvements in FEV1 thaneither drug alone (Evidence A). By 2003, thisstatement was expanded more generally toSABA/SAMA combinations and by 2011 to alsoimproving symptoms. Combinations of
Table 4 continued
Drug Inhaler (lg) Solution for nebulizer(mg/ml)
Duration of action(h)
Specific doses were no longer shown in ‘‘Commonly Used Maintenance Medications in COPD’’ after 2018a Combination added in 2003b pMDI formulation for albuterol/ipratropium combination was discontinued after 2013c Albuterol/ipratropium combination solution for nebulizer was changed to 0.75/0.5 in 2010, discontinued in 2013, andadded back as 0.5, 0.25 mg/ml in 2017d A soft mist inhaler (SMI) formulation for albuterol/ipratropium combination (100/20 lg) was added in 2014e Indacaterol/glycopyrronium combination was added in 2014f Vilanterol/umeclidinium combination was added in 2014g Formoterol/aclidinium combination was added in 2015h Olodaterol/tiotropium combination was added in 2017i Formoterol/glycopyrronium combination was added in 2017; dose was changed to 9.6/18 in 2018j Formoterol/glycopyrrolate combination was added in 2018k Formoterol/budesonide combination was added in 2003l Formoterol/mometasone combination was added in 2013m Salmeterol/fluticasone combination was added in 2003n Vilanterol/fluticasone combination was added in 2014o Formoterol/beclomethasone combination was added in 2015 for pMDI; DPI formulation was added in 2016p Triple therapy was added to GOLD’s ‘‘Commonly Used Maintenance Medications in COPD’’ table in the 2019 Reportq Fluticasone/umeclidinium/vilanterol combination was added in 2019 (doses and devices were not specified)r Beclometasone/formoterol/glycopyrronium combination was added in 2019 (doses and devices were not specified)
Adv Ther (2020) 37:1812–1828 1821

fenoterol/ipratropium and albuterol/iprat-ropium in one inhaler were first listed in the2003 Report.
SABA/LABA or LAMAThe 2011 Report noted that regular and as-needed use of SABAs improves FEV1 and symp-toms (Evidence B), but that the use of highdoses of SABAs on an as-needed basis in patientsalready treated with long-acting bronchodila-tors is not supported by evidence and cannot berecommended. However, the 2017 and laterReports state that LABAs do not preclude addi-tional benefit from as-needed SABA therapy.
LABA/LAMAAs mentioned above, the 2017 Report notedthat treatment with formoterol and tiotropiumin separate inhalers was shown to have a greaterimpact on FEV1 than either component alone.The possibility that this LABA/LAMA combina-tion improves lung function more effectivelythan monotherapy was first noted in the 2011Report (Evidence B). In 2014, GOLD noted thatLABA/LAMA combinations have shown a sig-nificant increase in lung function whereas theimpact on patient-reported outcomes was stilllimited. The Report also noted that there wasstill too little evidence to determine if a com-bination of long-acting bronchodilators is moreeffective than a LABA alone for preventingexacerbations. In the 2017 Report, it was moredefinitively stated that a ‘‘combination treat-ment with a LABA and LAMA increases FEV1
and reduces symptoms and exacerbationscompared to monotherapy (Evidence A).’’ TheReport also noted that a lower dose, twice dailyregimen for a LABA/LAMA was shown toimprove symptoms and health status inpatients with COPD.
LABA/LAMA by Exacerbation HistoryThe 2017 Report noted that most studies withLABA/LAMA combinations have been per-formed in patients with a low rate of exacerba-tions, but a study in patients with a history ofexacerbations found that a combination oflong-acting bronchodilators was more effectivethan long-acting bronchodilator monotherapy
for preventing exacerbations. (A similar effectmodification by exacerbation history was men-tioned earlier for ICS.) Additional evidenceregarding effect modification by exacerbationhistory was available in 2019, when GOLDnoted that several (but not all) studies sup-ported greater benefits from LABA/LAMA com-binations compared with long-actingbronchodilator monotherapy among patientswith a history of exacerbations. Although notspecific to exacerbations, the 2018 GOLDReport noted the results of a clinical trial thatfound LABA/LAMA treatment had the greatestimprovement in quality of life, compared withits individual bronchodilator components, inpatients with the highest baseline symptomburden.
LABA/ICSThe GOLD 2017 Report noted beneficial effectsof LABA/ICS over LABA alone on exacerbationrate. For patients with persistent dyspnea,exercise limitation, or exacerbations on LABA/ICS treatment, the Report suggested that aLAMA can be added to escalate to triple therapy.In 2019, GOLD noted that initial therapy withLABA/ICS has the greatest likelihood of reduc-ing exacerbations in patients with blood eosi-nophil counts of 300 cells/lL or higher, andperhaps also in patients with both COPD and ahistory of asthma. The Report further notedthat de-escalating from LABA/ICS to LABA/LAMA should be considered if the originalindication for ICS was not appropriate, giventhe increased risk of side effects with ICS, suchas pneumonia.
Triple TherapyThe 2011 Report first mentioned ‘‘triple ther-apy’’ when stating that the addition of a LABA/ICS combination to tiotropium improves lungfunction and quality of life and may furtherreduce exacerbations (Evidence B). The Reportemphasized that more studies of triple therapywere needed. In the 2013 Report, GOLD recog-nized that a few patients with newly diagnosedvery severe COPD may benefit from tripletherapy, and further noted the importance ofvalidating the effects of individual drugs before
1822 Adv Ther (2020) 37:1812–1828

using a combination. Most of the studies GOLDcited examined triple therapy in a single inha-ler. In the 2017 Report, possible benefits of tri-ple therapy were discussed more generally, nolonger referring specifically to newly diagnosedpatients. At that time, GOLD still cautionedthat more evidence was needed before firmconclusions could be drawn regarding tripletherapy. In the 2019 Report, GOLD cited addi-tional evidence from double-blind RCTs sup-porting benefits from triple therapy, includingimproved lung function, better patient-reportedoutcomes, and reduced risk of exacerbations.Triple therapy was added to GOLD’s ‘‘Com-monly Used Maintenance Medications inCOPD’’ table in the 2019 Report.
As noted consistently in GOLD Reports todate, no single drug or combination of drugshas been shown conclusively to decrease therate of patients’ long-term decline in lungfunction. However, the 2020 GOLD Reportcited evidence from RCTs showing that triplecombinations of LABA/LAMA/ICS reducedmortality compared with a LAMA, LABA/LAMA,or LABA/ICS. Although still relatively few innumber, these trials targeted patients mostlikely to show such an effect, namely, severelysymptomatic patients with moderate to verysevere airflow obstruction and a history of fre-quent and/or severe exacerbations; previousstudies did not specifically target such patients.GOLD also noted methodological reasons tointerpret the results of these studies cautiously.
Studies comparing combinations of drugs intheir effects on various objective and patient-reported outcomes, and especially how thoseeffects may be modified by other factors, are fewin number, limited in scope, and hence aredifficult to interpret. Nonetheless, such studiesare necessary steps in the refinement and per-sonalization of treatment for COPD.
INHALATION DEVICECONSIDERATIONS
Randomized controlled trials have notidentified superiority of one device/for-mulation. However, patients included in
these trials are usually those who masterinhalation technique and receive propereducation and follow-up regarding thisissue, and therefore may not be reflectiveof normal clinical practice.–GOLD Report, 2020
Besides the choice of inhaled drugs, keyaspects influencing effectiveness of treatmentare the choice of the most appropriate aerosoldelivery device, proper education, device train-ing, and adherence. Inhaled bronchodilatorsand ICS are typically delivered by inhalers,either pMDIs (sometimes referred to in GOLDReports as MDIs), DPIs, or soft mist inhalers(SMIs), or by nebulizers. Each device hasadvantages and disadvantages. Regarding inha-lers, GOLD (2017) noted that the main errors indelivery device use relate to problems withinspiratory flow, inhalation duration, coordi-nation, dose preparation, exhalation maneuverprior to inhalation, and breath-holding follow-ing dose inhalation. Poor adherence to inhala-tion therapy further compounds the problem ofdevice misuse.
GOLD has noted the importance of properinhaler use since their first (2001) Report. In2017, GOLD significantly expanded their dis-cussion on inhaler use to ‘‘attempt to improvetherapeutic outcomes.’’ The 2017 and subse-quent Reports more clearly emphasized that: (1)Education and training in inhaler device tech-nique cannot be overemphasized; (2) Choice ofdevice must be individually tailored dependingon access, cost, prescriber, and most impor-tantly, patient’s ability and preference; (3)Clinicians should instruct, demonstrate,recheck, and ensure proper inhalation tech-nique when prescribing a device, and follow upat each visit; (4) Inhaler technique and adher-ence should be assessed before concluding thatcurrent therapy is insufficient. This appears tomark GOLD’s first distinct emphasis of theimportance of choosing an appropriate inhala-tion device to optimize outcomes in COPDmanagement.
GOLD’s conclusions regarding regular use ofnebulizers have evolved as well. In the 2001Report, and all subsequent Reports until 2010,GOLD stated that ‘‘Nebulizers are not
Adv Ther (2020) 37:1812–1828 1823

recommended for regular treatment because theyare more expensive and require appropriatemaintenance.’’ In the 2006 Report, GOLD firstopened the door to the possibility of recom-mending regular use of nebulizers in somepatients by stating: ‘‘In general, nebulized therapyfor a stable patient is not appropriate unless it hasbeen shown to be better than conventional dosetherapy.’’ In 2010, GOLD no longer stated directlythat nebulizers were inappropriate for patientswith stable COPD, but recommendations for theiruse were still cautious: ‘‘Many drugs are availableas nebulizer solutions and for patients who areseverely overinflated and consequently may havevery low inspiratory flow rates, there may betheoretical advantages of nebulizers. However,there is little randomized trial evidence for benefitcompared to the use of other devices and use ofnebulizers will often depend on local preference,availability and price. Benefit should be judgedsymptomatically, since changes in lung functionmay be small and within the limits of repeata-bility. Nebulized treatment should only be con-tinued if the patients report clear symptomaticbenefit that cannot be achieved by simpler,cheaper, and more portable alternatives.’’ Theevolution towards accepting nebulizers as a stan-dard inhalation delivery device in patients withstable COPD continued, and the caveats notedabove were removed from the GOLD Reports in2017.
CHOOSING AND MANAGINGTHERAPY
In order to adjust therapy appropriately asthe disease progresses, each follow-up visitshould Include a discussion of the currenttherapeutic regimen. Monitoring shouldfocus on: Dosages of prescribed medica-tions; Adherence to the regimen; Inhalertechnique; Effectiveness of the currentregime; Side effects.–GOLD Report, 2020
GOLD’s most fundamental and consistentrecommendation for managing therapy is thatthe choice of drug, or combination therapy,depends on the availability of the drug, its cost,
and the individual response in terms of symptomrelief and side effects. In 2017, GOLD revised thisrecommendation to include patient preferenceand ability to use various drug delivery devices:‘‘Each pharmacological treatment regimenshould be individualized and guided by theseverity of symptoms, risk of exacerbations, sideeffects, comorbidities, drug availability and cost,and the patient’s response, preference and abilityto use various drug delivery devices.’’
Treatment Considerations Accordingto Drug Class
Long-Acting vs. Short-Acting BronchodilatorsEarly GOLD Reports noted that long-actinginhaled bronchodilators were more convenientthan short-acting bronchodilators but were alsomore expensive. In 2003, for ‘‘moderate’’ to‘‘very severe’’ disease, GOLD recommendedregular treatment with long-acting bron-chodilators, including tiotropium, rather thanshort-acting bronchodilators (Evidence A). In2004, it was noted more generally that long-acting inhaled bronchodilators were moreeffective. In 2009, it was further noted that thisalso applied to nebulized formulations. In 2017,the Reports began to address long-acting vs.short-acting bronchodilators within specificGOLD Groups (see ‘‘A Model for Initial Phar-macological Treatment’’ below). In brief, eitherclass of drug was recommended for patientswith the mildest disease, whereas long-actingdrugs were preferred at more advanced stages.
SABA vs. SAMABetween 2001 and 2016, GOLD Reports statedthat the bronchodilating effect of SAMAs lastslonger than that of short-acting b2-agonists. The2017 Report cited specific evidence that iprat-ropium, a SAMA, alone provided small benefitsover SABAs in terms of lung function, healthstatus, and requirement for oral steroids.
LABA vs. LAMAFrom the 2017 Report to present, GOLD statedthat LAMAs have a greater effect on exacerba-tion reduction compared with LABAs (Evi-dence A) and decrease hospitalizations
1824 Adv Ther (2020) 37:1812–1828

(Evidence B). Since 2011, GOLD has also notedthat a LAMA (tiotropium) may improve theeffectiveness of pulmonary rehabilitation.
LABA/LAMA vs. LABA/ICSEvidence presented in the 2019 Report suggeststhe possibility that the effectiveness of a LABA/LAMA combination compared with a LABA/ICScombination depends on the presence orabsence of other factors. That Report noted astudy in patients with a history of exacerbationsthat found a combination LABA/LAMAdecreased exacerbations to a greater extent thana LABA/ICS combination. Consistent with whatwas noted above for ICS, however, GOLD citedanother study in a population with high exac-erbation risk that reported that LABA/ICSdecreased exacerbations to a greater extent thana LABA/LAMA combination at higher (greaterthan 150 cells/lL) blood eosinophil concentra-tions. Although convincing data on these asso-ciations are lacking, a history of exacerbationsmay favor LABA/LAMA treatment, except wheneosinophil levels are high, in which case LABA/ICS treatment may be more effective in reduc-ing exacerbations.
Triple Therapy vs. Dual or Single TherapyAccumulating evidence cited in GOLD Reportsfrom 2011 to 2020 supports the recent GOLD
recommendations regarding triple therapy, e.g.,to add a LAMA in patients already on LABA/ICStherapy who still have persistent dyspnea,exercise limitation, or exacerbations. Recom-mendations concerning triple therapy areproblematical, however, when consideringpotential effect modification by exacerbationhistory and/or eosinophil concentrations,given: (i) sparse data from studies exploringeffect modification; (ii) no known biologicalmechanism to explain the modifying effects;and (iii) contrasting effect modificationsobserved with different components of tripletherapy (noted in the previous section).
A Model for Initial PharmacologicalTreatment
Rescue short-acting bronchodilatorsshould be prescribed to all patients forimmediate symptom relief.–GOLD Report, 2020
As mentioned above, in 2017, the GOLDReports began to address recommendations forinitial treatment within specific GOLD Groups(Fig. 2). For Group A patients, either short-actingor long-acting bronchodilators were recom-mended according to individual effectivenessand preference. For Group B patients, ‘‘Initialtherapy should consist of a long-acting
≥ 2 moderate≥ 1
leading to
mMRC 0-1, CAT < 10 mMRC ≥ 2, CAT ≥ 10
LAMA
A Bronchodilator(LABA or LAMA)
LAMA orLAMA + LABA* orICS + LABA**
0 or 1 moderate
(not leading tohospital admission)
INITIAL PHARMACOLOGICAL TREATMENT
Group C
Group A
Group D
Group B
> 20)**Consider if eos ≥ 300
FIGURE 4.2
Fig. 2 A model for initial pharmacological treatment
Adv Ther (2020) 37:1812–1828 1825
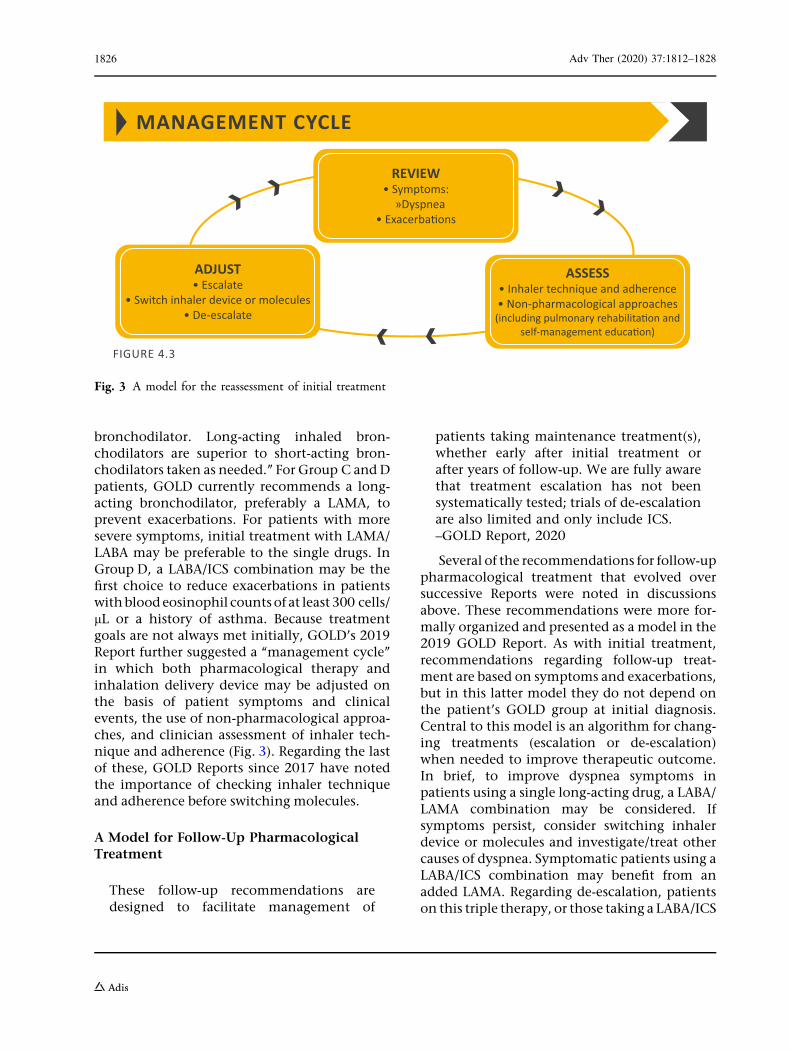
bronchodilator. Long-acting inhaled bron-chodilators are superior to short-acting bron-chodilators taken as needed.’’ For Group C andDpatients, GOLD currently recommends a long-acting bronchodilator, preferably a LAMA, toprevent exacerbations. For patients with moresevere symptoms, initial treatment with LAMA/LABA may be preferable to the single drugs. InGroup D, a LABA/ICS combination may be thefirst choice to reduce exacerbations in patientswithbloodeosinophil counts of at least 300 cells/lL or a history of asthma. Because treatmentgoals are not always met initially, GOLD’s 2019Report further suggested a ‘‘management cycle’’in which both pharmacological therapy andinhalation delivery device may be adjusted onthe basis of patient symptoms and clinicalevents, the use of non-pharmacological approa-ches, and clinician assessment of inhaler tech-nique and adherence (Fig. 3). Regarding the lastof these, GOLD Reports since 2017 have notedthe importance of checking inhaler techniqueand adherence before switching molecules.
A Model for Follow-Up PharmacologicalTreatment
These follow-up recommendations aredesigned to facilitate management of
patients taking maintenance treatment(s),whether early after initial treatment orafter years of follow-up. We are fully awarethat treatment escalation has not beensystematically tested; trials of de-escalationare also limited and only include ICS.–GOLD Report, 2020
Several of the recommendations for follow-uppharmacological treatment that evolved oversuccessive Reports were noted in discussionsabove. These recommendations were more for-mally organized and presented as a model in the2019 GOLD Report. As with initial treatment,recommendations regarding follow-up treat-ment are based on symptoms and exacerbations,but in this latter model they do not depend onthe patient’s GOLD group at initial diagnosis.Central to this model is an algorithm for chang-ing treatments (escalation or de-escalation)when needed to improve therapeutic outcome.In brief, to improve dyspnea symptoms inpatients using a single long-acting drug, a LABA/LAMA combination may be considered. Ifsymptoms persist, consider switching inhalerdevice or molecules and investigate/treat othercauses of dyspnea. Symptomatic patients using aLABA/ICS combination may benefit from anadded LAMA. Regarding de-escalation, patientson this triple therapy, or those taking a LABA/ICS
FIGURE 4.3
MANAGEMENT CYCLE
ASSESS• Inhaler technique and adherence• Non-pharmacological approaches
REVIEW• Symptoms: »Dyspnea
ADJUST• Escalate
• Switch inhaler device or molecules• De-escalate
Fig. 3 A model for the reassessment of initial treatment
1826 Adv Ther (2020) 37:1812–1828

combination, who are experiencing side effects,may stop taking ICS and try (or revert to) a LABA/LAMA combination. A separate model for esca-lating and de-escalating treatment during exac-erbations was also present in the 2019 Report.
CONCLUSION
The fundamental original idea behindGOLD is to provide a strategy for thediagnosis and the management of COPDresulting in a worldwide document and,for this reason alone, the GOLD docu-ments cannot be regarded as a standardclinical guideline per se… GOLD has madea great contribution to capture the globalCOPD landscape and its very significantchanges experienced over the last twodecades.–Roberto Rodriquez-Roisin, MD, Chair,GOLD Board of Directors, 2008–2011 [2].
The 20 years during which GOLD publishedtheir annual Reports has been a period ofremarkable innovation and refinement ofinhalation therapy for COPD. The GOLD Reportsdocument profound evolutions in the arma-mentarium of inhaled drugs in all categories ofinhalation devices; the use of long-acting, com-bination, and triple therapies; algorithms forinitial and follow-up treatment; the acceptanceof nebulizers in regular maintenance therapy;and the emphasis on inhalation device choice,technique, and adherence, all of which aredesigned to optimize outcomes in COPD man-agement. At one time, COPD was considered tobe an untreatable and progressive disease. As ouranalysis shows, the GOLD Reports manifest thesteady, important advancements made over thelast 20 years by researchers, clinicians, organiza-tions, and COPD community members, toward amore positive and organized approach to thetreatment of this widely prevalent disease.
ACKNOWLEDGEMENTS
The authors thank Ms. Katie Langefeld, ProjectManager of the Global Initiative for Chronic
Obstructive Lung Disease (GOLD), and theGOLD organization, for providing access to allof the GOLD Reports.
Funding. No funding or sponsorship wasreceived for this study or publication of thisarticle.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole, and have given theirapproval for this version to be published.
Disclosures. Dr. Terry and Dr. Dhand havenothing to disclose.
Compliance with Ethics Guidelines. Thisarticle is based on previously conducted studiesand does not contain any studies with humanparticipants or animals performed by any of theauthors.
Data Availability. Data sharing is notapplicable to this article as no datasets weregenerated or analyzed during the current study.
Open Access. This article is licensed under aCreative Commons Attribution-NonCommer-cial 4.0 International License, which permitsany non-commercial use, sharing, adaptation,distribution and reproduction in any mediumor format, as long as you give appropriate creditto the original author(s) and the source, providea link to the Creative Commons licence, andindicate if changes were made. The images orother third party material in this article areincluded in the article’s Creative Commonslicence, unless indicated otherwise in a creditline to the material. If material is not includedin the article’s Creative Commons licence andyour intended use is not permitted by statutoryregulation or exceeds the permitted use, youwill need to obtain permission directly from thecopyright holder. To view a copy of this licence,visit http://creativecommons.org/licenses/by-nc/4.0/.
Adv Ther (2020) 37:1812–1828 1827

REFERENCES
1. Lenfant C. Preface to the 2001 GOLD Report. In:Pauwels RA, Buist AS, Calverley PM, Jenkins CR, HurdSS. Global strategy for the diagnosis, management,and prevention of chronic pulmonary disease.NHLBI/WEHO Global Initiative for Chronic Obstruc-tive Lung Disease (GOLD) Workshop summary. Am JRespir Crit Care Med 2001;163:1256–76.
2. Rodriquez-Roisin R. Twenty years of GOLD(1997–2017). The origins. https://goldcopd.org/wp-content/uploads/2019/03/GOLD-Origins-Final-Version-mar19.pdf. Accessed 19 Mar 2020.
3. Mirza S, Clay RD, Koslow MA, Scanlon PD. COPDguidelines: a review of the 2018 GOLD report. MayoClin Proc. 2018;93:1488–502.
1828 Adv Ther (2020) 37:1812–1828