Influenza A(H5N1) in Humans: Outbreak Investigation in an International Setting Case Study 2: Part 1...
60
Influenza A(H5N1) in Humans: Outbreak Investigation in an International Setting Case Study 2: Part 1 1 1
-
date post
20-Dec-2015 -
Category
Documents
-
view
215 -
download
1
Transcript of Influenza A(H5N1) in Humans: Outbreak Investigation in an International Setting Case Study 2: Part 1...

Influenza A(H5N1) in Humans: Outbreak Investigation in an
International Setting
Case Study 2: Part 1
11

Learning Objectives
• Describe key outbreak management issues that need to be addressed related to supplies, team composition, WHO policy and epidemiologic data management during an internationally located A(H5N1) outbreak investigation.
• Identify critical coordination priorities involving the interface between animal and human health sectors, key stakeholders such as WHO, CDC and Ministries of Health and communication processes between CDC field staff, CDC Headquarters and relevant subject matter experts. 22

Learning Objectives (cont.)
• List appropriate practices and procedures for: Specimen collection and transport Epidemiologic investigation Identification of transmission mechanismsContact tracing Isolation/quarantine policyTreatment/control policy Risk communication prioritiesRecommended laboratory specimen protocols methodsEthical considerations
3

Outline
• Review of the preparation for an outbreak investigation
• Description of the situation and available details on the case, surrounding events/history and environment
• Engage in outbreak investigation activities: Case definition Clinical / laboratory findings, samples, recommendations Line listing Contract Tracing Treatment options/ recommendations
Principles are applicable to outbreaks from other known or newly emerging pathogens
44

Introduction
Be sure to have materials needed to take notes and create a line list
5

Republic of Pegu: Setting
• Developing country
• Southeast Asia
• 21 provinces
• Population: 50 million
66

Epidemiologic Setting
• Mass deaths in chicken, geese, and waterfowl flocksFive months ago (March) Southeastern region
• Ministry of Agriculture (MOA) reported 3 test results “weakly positive” for avian influenza A(H5N1)Came from three dead chickens sent to national lab in
Anawrahta (April)
• No systemic surveillance exists for H5N1 in poultry, wild bird or animal populations
7

Question 1
To respond to trigger event #1, you need to put together a Rapid Response Team (RRT) - Which of the following skills or persons should be represented in this RRT?
Team Leader Epidemiologist Veterinary Liaison Respiratory Therapist Medical Officer / Clinician Data Manager Marketing Assistant Laboratorian or Lab tech Logistician Communications Specialist
8

Question 2
Match who should be notified about the investigation on the left with the reason they should be notified on the right.
1. Veterinary Health Authority
2. Healthcare personnel
3. The community
4. Non-governmental organizations
5. The laboratory
a. So they can raise concerns and be aware of possible cases
b. To be ready for samples that will be coming
c. So they can undertake enhanced surveillance for sick or dying poultry
d. So they know you are coming to investigate, can have medical records ready to review, and have appropriate staff available
e. So they can leverage resources such as medical supplies or additional staff
9

Question 2 Answers
Answer:1. Veterinary health = c. Evaluate diseased poultry
2. Healthcare personnel = d. Knowledge that you will investigate
3. Community = a. Can raise concerns
4. NGOs = e. Medical personnel/supplies and resources
5. Laboratory = b. Prepare for incoming samples
10

Question 3
Below are 6 categories of supplies needed when you go to the field. Match the list of supplies to the general category.
Categories: Epidemiological, Medical, Laboratory, Educational & Communications, PPE, Decontamination
a. Case definitionsb. Antiviral medicationc. Gogglesd. Glovese. Graph paperf. Solution for decontaminating
homes or hospital roomg. Transportation containersh. Pensi. Gown and capj. Reporting forms
k. Specimen collection materials
l. Icem. Guidelines for contacts,
family members, and healthcare workers
n. Notebook/laptopo. Portable GIS unitp. Viral transport mediaq. Simple messages r. Respirators
11

Question 3 Answers
Answer:
• Epidemiological: a. Case definitions, j. reporting forms, n. notebook/laptop, h. Pens, e. graph paper, o. portable GIS unit
• Medical: b. Antiviral medication
• Laboratory: k. Specimen collection materials, g. Transportation containers, l. Ice, p. Viral transport media
• Educational materials: q. Simple messages, m. Guidelines for contacts, family members, and healthcare workers
• Personal Protective Equipment (PPE): r. Respirators, d. gloves, i. gown and cap, c. goggles
• Decontamination: f. Solution for decontaminating homes or hospital rooms
12

Trigger Event
July 15th
• Dava Ghar hospital has admitted 2 patients with SARI Reported to District Health Office They suspect avian influenza due to poultry
outbreaks in area
• Patients are related 65 year old grandmother (JAM) 10 year old grandson (AAJ)
JULY 15
13

Character Details
• 65 year old grandmother = JAMChronically illCaretaker of grandson
starting July 11
• 10 year old grandson = AAJOnset July 10
• Uncle = JRO
• Grandfather = AWM
• Mother = NJC Caretaker of son (AAJ)
Setting: Small, mountain village in Pelu Jaghai
province
JULY 15
14

Exposure & Onset Details
• AAJ, NJC, & JRO attended live-market (“Murg Market”)
Murg Market in Pelu Jaghai: Local market with live animals and location of A(H5N1) confirmed poultry outbreaks
July 8th
• July 13th AAJ brought to hospital with: fever (38.7), cough, diarrhea and shortness of breath
• AAJ becomes ill on July 10th
• JAM cares for him starting July 11th
Dava Ghar hospital: 60 km away from village
July
13th
JULY 15
15

AAJ Clinical Presentation and Further Evidence
• Arrived in unstable condition on the night of 13th
• Admitted early on 14th
• Rapidly deteriorated
Respiratory distress led to endotracheal intubation and ventilatory support
Cefriaxone treatment started
10 year old child (AAJ) CXR on Admission
JULY 15
16
Caretaker Health Status at Hospital
• Mother (NJC) and grandfather (AWM) are asymptomatic or deny symptoms
• Grandmother (JAM) reports respiratory condition suddenly worsened on about July 9th JAM symptoms: fever, cough
and dyspnea = SARI JAM admitted to hospital
on July 14th
JAM denied contact with Murg Market or poultry
JULY 15
17

Rumor Surveillance Update from Local Health Authorities
• May be additional sick persons with respiratory symptoms in Pelu Jaghai
• May continue to be wide-spread chicken deaths
JULY 15
18

Question 4
How would you classify AAJ into the WHO influenza A(H5N1) case definition? Information on AAJ is given for your reference.
a. Under investigation
b. Suspected
c. Probable
d. Confirmed
Answer: The Chest X-ray and clinical deterioration extend the ‘suspected A(H5N1) status’ to C, a probable case designation.
Clinical: Fever, cough, diarrhea and
shortness of breath, Chest x-ray
positive for pneumonia
Epidemiological: Exposure to live-
market on July 8th where influenza
A(H5N1) infections in animals were
confirmed in the last month.
Laboratory: No lab specimens
available.
19

Question 5
How does patient JAM fit into the WHO influenza A(H5N1) case definition?
a. Under investigation
b. Suspected
c. Probable
d. Confirmed
Answer: The above information is supportive of a designation of a. person under investigation
Clinical: Fever, cough, and shortness of breath
Epidemiological: Close contact (within 1 meter) with a person who is a suspected, probable, or confirmed H5N1 case. Close contact with probable case occurred 2 days after “onset of symptoms”.
Laboratory: No lab specimens collected at time of questioning.
20
Create a Line List
ID Age Gender
What variables should be included?
• ID #• Demographics: (age, gender,
patient contact)• Possible exposure to infected
animals within 7 days of symptoms
• Possible contacts with suspect or confirmed human case within 7 days
• Occupation• Symptom onset• Date of onset• Hospital test results• H5 Laboratory diagnosis• Antivirial treatment• Status (Case or Contact)• Disposition (Hospitalized,
deceased, etc)21

Suggested Line List Format
22
ID #
Initials Vill-age
Age Sex Possible exposures and date
EPI relation
Syx Onset date- July
Lab
Status
Case status
Outcome

Update the Line List
Update the line list with the cases as of July 15th mid-dayID #
Initials Vill-age
Age Sex Possible exposures and date
EPI relation Syx Onset date- July
1 AAJ DG 10 M Live Mkt: July 8th
Grandmother: July9th
Child (exposed at live market)
F,C,S 10
2 JAM DG 65 F Caretaker of #1
Timing unknown
Grandmother of #1 (AAJ)
F,C,S 9
ID #
Initials Lab
Status
Case status definition
(Case v. Contact)
Outcome
1 AAJ No lab specimen Probable Case Hospitalized on ventilator, pneumonia, respiratory failure
2 JAM Pending Person under invest. Hospitalized
F: Fever; C: Cough; D: Diarrhea; S: Shortness of breath; M: Myalgias; URI – upper respiratory syxDG: Dava GharPJ: Pelu Jaghai
JULY 15
23

Question 6
Which of the following would be considered contacts of AAJ?
a. JAM
b. A teacher who last spoke to him 2 weeks ago
c. A tuk-tuk driver who drove him to a friends home on the 6th
d. A neighbor who walked by AAJ but didn’t say anything to him on the 10th
Answer: a.
24

Question 7
Note whether the following statements used to define who is a close contact of this probable case are true or false.
1. Anyone who came within 1 meter of the case patient
2. Anyone who had shared space within 1 meter of the case patient
3. Close contact 1 day before through 14 days after onset of symptoms
4. Close contact 7 days before through 14 days after the onset of symptoms
5. Someone who kissed, embraced or shared utensils with the case patient
6. Someone who spoke with or touched the case patient
25
Answers:
False
True
True
False
True
True

Review: Identifying Contacts
• Potential contactsHousehold membersFriendsHealthcare providersPharmacistsTraditional healersWorkplace contacts
• Contact tracing activitiesPrioritize high
probability of influenza A(H5N1) case patients
Prioritize contacts by duration, proximity, and intensity of exposure to the case patient
26

Question 8
Assuming that neuraminidase inhibitors are available:
1.Should AAJ be given anti-viral treatment?
2.Should JAM be given anti-viral treatment?
Answer: 1.Yes2.Maybe
Hint: If antiviral drugs are available, treatment doses should be provided to suspected, probable and confirmed cases as classified according to the WHO case definition.
27

Question 9
1. Should JAM receive anti-viral prophylaxis?
2. Should asympomatic close contacts of AAJ be given anti-viral prophylaxis?
3. Should close contacts of JAM receive antiviral prophylaxis?
Answer:
1. Yes
2. Yes
3. No
Hint: The WHO Rapid Advice Guidelines on pharmacological management of humans infected with avian influenza A (H5N1) virus suggests that prophylaxis doses should be provided to all identified close contacts of confirmed cases, and if resources allow, to close contacts of “strongly suspected” cases as well.
28
Question 10If there are not enough antiviral resources for everyone, persons in the community should be prioritized for antiviral prophylaxis. Match the Risk Group on the left with the description on the right.
1. High Risk
2. Moderate Risk
3. Low Risk
a. Personnel culling likely non-infected animalsb. Personnel handling sick animals or decontaminating
environments using insufficient PPE c. Personnel handling sick animals or decontaminating
environments using adequate PPE d. Unprotected close/direct exposure to H5N1 infected
animalse. Healthcare or laboratory personnel in close contact with
strongly suspected or confirmed patients or their samples with insufficient PPE
f. Healthcare workers not in close contactg. Healthcare workers with close contact using adequate
PPEh. Close household contact of strongly suspected or
confirmed patients 29
Question 10 AnswersHigh and Moderate Risk Groups
High risk exposure groups
h. Household or close family contacts of a strongly suspected or confirmed H5N1 patient
Moderate risk exposure
b. Personnel involved in handling sick animals or decontaminating affected environments
d. Individuals with unprotected and very close direct exposure to sick or dead animals infected with the H5N1 virus
e. Health care or laboratory personnel with unprotected close contact with strongly suspected or confirmed H5N1 patients or their clinical samples 30

Question 10 Answers:Low Risk Groups
Low risk exposure groups
f. Health care workers not in close contact
g. Health care workers using adequate PPE
a. Personnel involved in culling non-infected or likely non-
infected animal populations
c. Personnel involved in handling sick animals or
decontaminating affected environments using adequate PPE
Explain (tactfully!) to contacts the scarcity of antivirals, and that they will be
monitored.
NOTE: Drug allocation plans for treatment and prophylaxis should be made in
advance 31

Update: July 16th
The RRT arrives at Dava Ghar
AAJ Update
• Admission Fever 39 °C Heart rate 120 34 breaths/minute Blood pressure 90/60 O2 saturation 88%
• Outcome Intubated Jul 14 Hypotensive with renal failure Died on the 16th Respiratory and sputum samples
of poor quality
JAM Update
• Admission Temperature 38.5 °C 28 breaths/minute Blood pressure 160/95 O2 saturation 90%
• Initial laboratory findings High lymphocyte count High leukocyte count
JULY 16
32
Specimens Needed
• You will need to quickly determine whether you’re dealing with H5N1 or some other communicable pathogen
• You send respiratory specimens from the grandmother to the National laboratory for testing.
JULY 16
33

Question 11What specimen type is the top priority to be collected from JAM for laboratory testing for influenza?
a.Endotracheal fluidb.Broncho-alveolar lavagec.Throat swab (oropharyngeal) d.Nasal swab (nasopharyngeal) e. Blood
Answer :c. Throat swabComment: Nasal swabs should be collected to rule out seasonal influenza. In general, collect multiple samples on multiple days.
Remember! It is vital to use proper safety equipment including eye protection and PPE for the protection of the individual(s) carrying out the procedure(s). Treat all clinical samples as though they are potentially infected with avian influenza!!!
34
Question 12Which of the following statements about specimen collection is NOT true?
a.It should begin as soon as possible after symptoms begin
b.It should begin before antiviral medications are administered (but treatment should not be delayed for specimen collection)
c.Sample should be collected even if symptoms began more than one week ago
d.Multiple samples should be collected on multiple days if possible
e.None of the above (all statements are true)
Answer: e.
Remember – it is better to collect too many specimens than not enough 35

Specimen Collection Kit
Collection vials with VTM
Polyester fiber-tipped applicators
Sterile saline which is 0.85% NaCl
A sputum or mucus trap
Tongue depressors
Specimen collection cups or Petri dishes
Transfer pipettesA secondary
containerIce pack
Items for collection of blood
Personal Protective Equipment (PPE)
Field collection forms
A pen or marker for labeling samples
JULY 15
36

Question 13
• Done appropriate PPE
• Slowly remove the swab while slightly rotating ; the patient should try to resist gagging and closing the mouth
• Swab oropharyngeal area behind tonsils
• Have the patient open his/her mouth wide open
• Put tip of swab into vial containing VTM, breaking/cutting applicator’s stick
Put the following steps for collecting an oropharyngeal specimens in the proper orderAnswers
1.
3.
4.
2.
5.
37

Question 14Here is an image of a properly packed specimen. Label the packaging using the answer choices given.
1) 3 layers of _________
2) Absorbent _________
5) Specimen______
6) _______ label
4) Itemized list of ______
3) Labeling of the _________ as UN3373 diagnostic specimens
Answer choices:a.contentsb.packing materialc.identificationd.outer packagee.packagingf.biohazard 38

Question 15Here is an image of a properly packed specimen. Label the packaging using the answer choices given.
1) 3 layers of e. packaging.
2) Absorbent b. packing material
5) Specimen c. identification
6) f. Biohazard label
4) Itemized list of a. contents
3) Labeling of the d. outer package as UN3373 diagnostic specimens
39

Question 16
Determine whether the following statements about storing specimens in VTM are true or false.
1.Specimens can be stored at 4 °C within 48 hours of collection both before and during transportation.
2.Store specimens at -70 °C beyond 48 hours (if you will not be able to immediately transport specimen to laboratory)
3.Never store specimens on dry ice
4.Specimens may be stored in standard freezer
40
Avoid freeze – thaw cycles. It is better to keep a sample on ice even for a week, than to allow the sample to freeze and thaw multiple times.
Answers:
True
True
False
False

Question 17
When transporting specimens from potential human cases of influenza A(H5N1) infection from the field to the laboratory, you should follow which sets of regulations?
a. WHO guidelines for safe transport of infectious substances and diagnostic specimens
b. Local regulations on the transportation of infectious material
c. Neither a nor b
d. Both a and b
Answer: d.
41
Epidemiologic and Specimen Tracking for
Transportation• Documents to include
Itemized list of specimens with identification numbers Instructions for the laboratory
• Information to maintain Identification numbers, linking to epidemiologic data forms Case demographics When and where a specimen was collected Type of specimen
Coordinate shipment with the laboratory so they are prepared when the specimens arrive 42
JULY 16

Contact Identification
• You have finished collecting patient specimens and have sent them off to the national laboratory
• You want to identify all potentially exposed individuals who have had contact with the probable case (AAJ)
• You determine that close contacts areMother (NJC) Uncle (JRO),Grandparents (JAM & AWM)
JULY 16
43
Update the Line List
44
ID #
Initials Vill-age
Age Sex Possible exposures and date
EPI relation Syx Onset date
Lab
Status
Case status
Outcome
1 AAJ DG 10 M Live Mkt: July 8th
Grandmother: July9th
Index case F,C,S
Jul 10 No lab specimen
Probable Case
Hospitalized on ventilator, pneumonia, respiratory failure
2 JAM DG 65 F Caretaker of #1
Timing - ?
Grandmother of #1 (AAJ)
F,C,S
Jul 9 Pending Person under invest.
Hospitalized
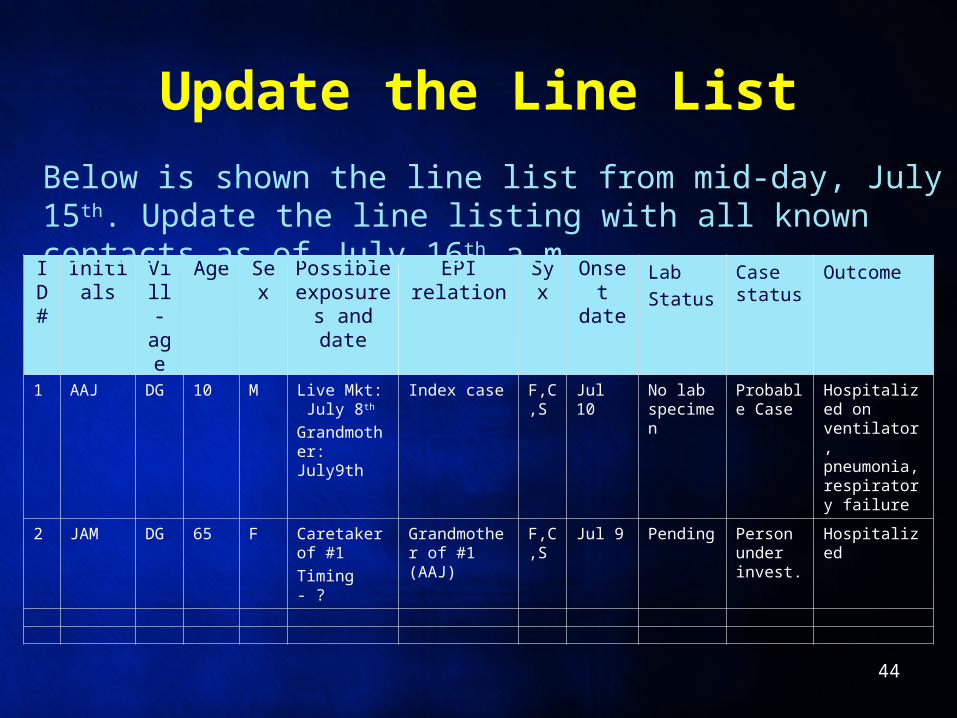
Below is shown the line list from mid-day, July 15th. Update the line listing with all known contacts as of July 16th a.m.

Line List as of July 16th a.m.
F: Fever; C: Cough; D: Diarrhea; S: Shortness of breath; M: Myalgias; URI – upper respiratory syxDG: Dava GharPJ: Pelu Jaghai
ID #
Initials Vill-age
Age Sex Possible exposures and date
EPI relation
Syx Onset date
Lab
Status
Case status
Outcome
1 AAJ DG 10 M Live-Mkt: July 8
‘index’ case
F, C, D, S
10 No lab specime
n
ProbableCASE
Died (7/16)
2 JAM DG 65 F Caretaker of # 1
Grandmother (# 1)
F, C, S
9 Pending PUI/Contact
Hospitalized
3 AWM DG 70 M Caretaker of # 1
Grandfather (# 1)
Contact
4 NJC DG 36 F Caretaker of # 1; Live-Mkt: July 8
Mother (# 1)
Contact
5 JRO DG 27 M Live-Mkt: July 8
Uncle (# 1)
Contact
45

Beyond the Given Scenario
Also think beyond the nuclear familyVillage health workersTraditional healersTaxi drivers Other people that may have had close contact with
the case during the infectious period
46

Question 18
You want to know whether there are more contacts that you should be concerned about. Which of the following places would NOT be one that you would visit at this point to determine if there are more cases and/or contacts?
a.Health care facilities (hospitals, clinics, traditional healers)b.Patient (or family proxy)c.Patient’s village/neighborhoodd.Patient’s school/workplacee.None of the above
Answer: e. Depending on the places visited by a case, any of these places could be important places to undertake additional contact tracing activities
47

Question 19Which of the following scenarios does NOT list the appropriate PPE measure?
1. You will interview a symptomatic person that could be infected with influenza A(H5N1): Interview from more than 1-2 meters away and wear no PPE
2. You will be within 1-2 meters of a symptomatic person that could be infected with influenza
A(H5N1) Wear a fit tested respirator and eye protection
3. You physically examine a person that could be infected with influenza A(H5N1) You need to wear droplet and contact precautions
4. You are entering an environment where poultry products or feces may be contaminated, Wear droplet and contact precautions including boots and undertake appropriate
biosecurity/decontamination measures before leaving the premises
Answer: Scenario 2. Respirators are used for aerosol-generating procedures.48

Question 20
1. Hospital or other medical facility
2. Patient (or proxy)
3. Patients home and village
a. Administer case finding questionnaire to determine if the interviewee knows of anyone else who is sick, to ask about possible exposures, and to ask about possible contacts
b. Retrace the steps of the patient in the facility and try to determine if there were any close contacts without adequate PPE
c. Find out more details about suspected exposures, conduct an environmental survey, and determine if there are any outbreaks among animals. Look for additional cases
Match the information source on the left with the contract tracing activities that should be conducted there on the right.
Answer: 1. b 2. a 3. c 49
Question 21
Questions to ask the case patient/case patient’s family regarding potential H5N1 exposures should cover which of the following?
Contact with confirmed , suspect, or probable human H5 cases
Exposure to sick or dying animals, wild birds, other animals, or their environment
Exposure to environments that may be contaminated with influenza A (H5N1)
Exposure to cooked chicken products
Handling/preparation of raw poultry and other animal products 50

Question 22
Questions to as the case patient/case patient’s family regarding additional case finding/H5N1 circulation in the community include which of the following?
Awareness of additional cases of severe respiratory illness in family, friends and co-workers
Awareness of H5N1 outbreaks occurring outside of the country
Awareness of illness or deaths in birds, cats, swine, or other animals in the household and neighboring area
51

Question 23
When in a patient’s home or their village, what are important contextual factors to observe?
Poultry in and around the houseConstruction material of the homeMapped location or photograph of house and surroundingsPossible unique and culturally-specific mechanisms of exposureAnnual community festival daysLive bird markets or other occupationally related exposures
52

Case Finding Results
• Child with unexplained respiratory illness reported in nearby province, Pelu Jaghai
• Director of Epidemiology orders your team to meet the Ministry of Health field workers there and make site visits to hospitals and villages
JULY 16
53

New Case and Contact
• 11-year-old boy, TMUFever, cough shortness of breath , date of onset July 12Admitted July 15Critically ill, not intubated
You and your team don PPE, evaluate the patient, review medical chart, and interview available family members
• Mother (ACM)Reports boy visited Murg market on July 8
54
JULY 16

Update the line list with the current information as of the afternoon of
July 16.
55

Line List as of July 16th p.m.
56
F: Fever; C: Cough; D: Diarrhea; S: Shortness of breath; M: Myalgias; URI – upper respiratory syxDG: Dava GharPJ: Pelu Jaghai
ID #
Initials Vill-age
Age Sex Possible exposures and date
EPI relation Syx Onset date
Lab
Status
Case status
Outcome
1 AAJ DG 10 M Live-Mkt: July 8
‘index’ case F, C, D, S
10 No lab specimen
ProbableCASE
Died (7/16)
2 JAM DG 65 F Caretaker of # 1
Grandmother (# 1)
F, C, S
9 Pending PUI/Contact
Hospitalized
3 AWM DG 70 M Caretaker of # 1
Grandfather (# 1)
Contact
4 NJC DG 36 F Caretaker of # 1; Live-Mkt: July 8
Mother (# 1) Contact
5 JRO DG 27 M Live-Mkt: July 8
Uncle (# 1) Contact
6 TMU PJ 11 M Live-Mkt: July 8
Playmate (# 1)
F, C, D, M
12 Pending SuspectCASE
Hospitalized
7 AMC PJ 29 F Caretaker of # 6
Mother of # 6 Contact

Differential DiagnosesHuman influenza
• Commonly an upper respiratory infection
• Fever, headache, cough, sore throat
• Muscle ache, exhaustion
• Other respiratory symptoms
• Recovery: 2-7 days
• Can progress to pneumonia and respiratory failure in some cases
Influenza A(H5N1)• Commonly a lower respiratory
infection• Fever, headache, cough, sore
throat• Muscle ache, exhaustion• Difficulty breathing,
respiratory distress• Crackling on inhalation• Leukopenia, lymphopenia• Increased respiratory rate• Sputum production, possibly
with blood• Limited data: diarrhea
57
An animal virus that is adapting to humans may have a mixed picture of clinical presentations.

Non-Influenza Differential Diagnoses
Viral
• Human influenza viruses
• Parainfluenza viruses
• Respiratory syncytial virus
• Adenovirus
• Rhinovirus
• Flaviviruses (e.g. Dengue)
• Coronaviruses (including SARS-CoV)
• Human metapneumovirus
• Hantavirus
• New / emerging viruses, such as bocavirus
Bacterial
• Mycobacteria tuberculosis
• Yersinia pestis (pneumonic plague)
• Streptococcus pneumoniae
• Staphylococcus aureus
• Hemophilus influenzae
• Burkholderia pseudomallei
• Legionella spp.
• Chlamydia pneumoniae
• Mycoplasma pneumoniae
• Coxiella burnetii(Q fever) 58
59
Clinical signs and symptoms alone cannot distinguish the severe
complications of seasonal influenza from
influenza A (H5N1) infection in humans:
Examine the epidemiology and collect
specimens!

Move on to Outbreak Investigation, Part 2
60