Part 3 Cholinoceptor Antagonists. A Muscarinic receptor antagonists.
Upload
michael-j-hickeyCategory
view
216download
2
INFLUENCE OF POSTISCHEMIC ADMINISTRATION OFOXYRADICAL ANTAGONISTS ON ISCHEMIC INJURY TO RABBITSKELETAL MUSCLE
MICHAEL J. HICKEY, Ph.D., KENNETH R. KNIGHT, Ph.D.,*
DIANA A. LEPORE, M.Sc., JOHN V. HURLEY, M.D., B.S., Ph.D.,
and WAYNE A. MORRISON, M.D., B.S.
The aim of this study was to determine whether the admin-istration of free radical antagonists, immediately before andduring the early minutes of reperfusion, improves muscle sur-vival 24 hr after a period of ischemia. Rabbit rectus femorismuscles were isolated, made ischemic for 31⁄2 hr and treatedwith either desferrioxamine (DFX), an Fe3+ chelator, super-oxide dismutase and catalase (SOD & CAT), which quenchsuperoxide and hydrogen peroxide, or allopurinol, an inhibi-tor of xanthine oxidase (XO). After 24 hr reperfusion, muscleviability (±s.e.m.), measured by the nitro blue tetrazolium(NBT) vital staining technique, was 41.6 ± 11.3% for saline-treated ischemic controls, 30.6 ± 7.6% for DFX-treated, 46.7± 10.3% for SOD & CAT-treated, and 43.3 ± 9.5% for allo-purinol-treated muscles. None of the treated groups differed
significantly from the ischemic control group. Tissue my-eloperoxidase, ATP and reduced glutathione levels, andplasma lactate dehydrogenase (LDH) and aspartate trans-aminase (AST) levels were increased by ischemia and reper-fusion in all groups, but the changes did not differ betweenthe treatment groups. Levels of XO in the rabbit muscle weredetermined and found to be very low in both normal andpostischemic muscle. As XO is the target enzyme of allopu-rinol, its absence provides a basis for the lack of effect of thisagent. However, it is not clear why DFX and SOD & CAT hadno protective effect.
© 1997 Wiley-Liss, Inc.MICROSURGERY 17:517–523 1996
Reperfusion of tissue after a period of ischemia leads togeneration of highly reactive oxygen-derived free radicals(oxyradicals) whose toxic effects amplify the tissue injurycaused by the ischemia.1,2 However, attempts to salvagepostischemic tissue either by inhibiting free radical produc-tion or by scavenging existing free radicals have had mixedsuccess, particularly in skeletal muscle. Some studies usingthis approach have claimed beneficial effects such as at-tenuation of postischemic increases in vascular permeabil-ity,3 preservation of transmembrane potentials,4 reductionof no-reflow,5 and preservation of muscle function.6 How-ever, many other studies using similar treatments havefailed to detect any beneficial effect.7–13 Diversity of spe-cies used, times of drug administration, and end points ex-amined may have contributed to these conflicting findings.
In reconstructive surgery, the administration of oxygen-free radical antagonists is most likely to be useful duringreplantation of traumatically amputated digits and limbs. Insuch cases, the earliest possible time for drug intervention is
at the end of ischemia, just before blood flow is re-established following vascular anastomosis. The present pa-per describes the effect on the viability of the rabbit rectusfemoris muscle after ischemic injury of three types of anti-free radical treatment administered immediately before res-toration of blood flow and in the early stages of reperfusion.The treatments examined were: (1) desferrioxamine (DFX),an Fe3+ chelator that may prevent oxyradical production viathe Fenton reaction, (2) a combination of superoxide dis-mutase (SOD) and catalase (CAT), which quench O2
− andH2O2, respectively, and (3) allopurinol, an inhibitor of xan-thine oxidase (XO).
MATERIALS AND METHODS
Animal Model and Operative Procedure
Thirty-eight New Zealand white rabbits of both sexes,weighing 2.0–2.5 kg, were used. For all operative proce-dures, anesthesia was induced by intravenous injection ofpentobarbitone sodium (30 mg/kg) and maintained by inha-lation of oxygen (2 L/min) and 2% halothane. Sterile tech-nique was used for all procedures and only one muscle wasisolated per rabbit. Animals were cared for in accordancewith the National Health and Medical Research Council(Australia) guidelines for the care and use of laboratory
Bernard O’Brien Institute of Microsurgery, St. Vincent’s Hospital, Fitzroy, Vic-toria 3065, Australia.
Contract grant sponsor: National Health and Medical Research Council, Aus-tralia.
*Correspondence to: Kenneth R. Knight, Bernard O’Brien Institute of Micro-surgery, St. Vincent’s Hospital, 42 Fitzroy Street, Fitzroy, Victoria 3065, Aus-tralia. E-mail: [email protected]
© 1997 Wiley-Liss, Inc.

animals. Chemicals were purchased from Sigma ChemicalCo., St. Louis, MO, unless stated otherwise.Surgical isolation of rectus femoris muscle. Themethod of surgical isolation of the rabbit rectus femorismuscle has been described previously.14 Briefly, a skin in-cision is made on the medial thigh from the inguinal liga-ment to the knee, the rectus femoris approached by dividingthe aponeurosis between the vasti muscles and isolated fromthe surrounding tissues by blunt dissection. The distal ten-dinous insertion is divided and several small arterial andvenous perforators at the proximal end of the muscle iso-lated and cauterized. The neurovascular pedicle and the ad-jacent femoral vessels are then dissected free, the femoralartery ligated distal to the origin of the artery supplying themuscle, and the muscle divided as proximally as possible.To induce ischemia, vascular clamps are placed on thefemoral artery proximal to the branch supplying the muscle,and on the vein draining the muscle. The muscle is replacedin position and fixed distally with a stay suture. The skin isclosed with sutures and the animal allowed to wake up. Themuscles underwent 31⁄2 hr of ischemia, a period that hasbeen shown previously to cause a reproducible, but incom-plete and potentially reversible, degree of muscle necro-sis.14 Nearing the end of ischemia, the rabbits are re-anesthetized using nitrous oxide/oxygen only.Treatment groups examined. Five groups of animalswere examined.
1. Ischemic Control-Infused group:A catheter was intro-duced into the femoral artery just distal to the branchsupplying the muscle, the venous clamp removed, andinfusion at 0.1 mL/min of the intra-arterial drug vehicle(0.9% NaCl containing 300 mg/mL papaverine HCl)commenced 10 min before the end of ischemia. Thearterial clamp was removed to commence reperfusion,and the infusion continued for a further 10 min, afterwhich the femoral artery was ligated, the skin closed, andthe rabbit allowed to wake up (n4 6).
2. DFX-treated group:Desferrioxamine (Desferal, Ciba-Geigy, Pendle Hill, NSW, Australia) (100 mg/kg, 10% inH2O), was injected as an i.v. bolus immediately beforethe end of ischemia. This drug was not given by i.a.infusion because the volume required, especially in thelarger rabbits, was greater than that infused in the stan-dard infusion protocol (n4 8).
3. SOD & CAT-treated group:Superoxide dismutase(20,000 U) and catalase (Calbiochem Corp, San Diego,CA) (40,000 U) were dissolved in 2 mL of the infusionvehicle and infused using the same protocol as the Isch-emic Control-Infused group (n4 8).
4. Allopurinol-treated group:Allopurinol [50 mg/kg, 6.8%(w/v) in 0.01 M NaOH] was given by slow i.v. injectionover several minutes via an ear vein, commencing 10min before the end of ischemia. This treatment was not
given via i.a. infusion because the high pH of the solu-tion required to dissolve allopurinol would damage thearterial vasculature of the infused muscle (n4 8).
5. Normal Muscle Control group:Unoperated rabbits wereused to provide baseline levels for biochemical studies (n4 8).
The doses of all agents used were chosen to fall into theeffective dose ranges as determined in previously publishedstudies: DFX,12,15 SOD & CAT,6,8 and allopurinol.16,17
Evaluation of Ischemia-Reperfusion Injury
In all groups, the rabbits were re-anesthetized 24 hr afterthe start of reperfusion, a venous blood sample removedfrom a lateral ear vein and the rabbits sacrificed by sodiumpentobarbitone overdose. The rectus femoris muscle wasremoved, cross-sectioned rapidly at 5 mm intervals and al-ternate slices either snap frozen in liquid nitrogen for sub-sequent biochemical analysis, or incubated in Nitro BlueTetrazolium (NBT) to stain viable tissue.14
Muscle viability. Every second serial slice of the musclewas incubated for 25 min at room temperature in 0.1 Mphosphate buffer containing 0.033% NBT and 0.13%NADH, then washed and fixed in 10% formalin. The per-centage of viable (labelled) muscle was calculated by mea-suring the total area and the viable area on either side ofeach slice using computerized image analysis (Video Pro32, Leading Edge, Pty. Ltd., Hove, South Australia). Fromthe proportional area of viable tissue and the weight of eachslice, the percentage of viable tissue for the whole musclewas calculated.Biochemical analysis. A frozen slice from each musclewas thawed at 4°C and weighed portions prepared for analy-sis. The techniques used for the biochemical analyses havebeen described previously.18 Myeloperoxidase (MPO) re-sults were expressed as U/g wet weight where 1 U of ac-tivity was defined as the change in absorbance of 1.0/min at655 nm and 37°C. Acid soluble sulfhydryl or reduced glu-tathione (GSH) results were expressed asmmol/g wetweight, and tissue ATP levels were expressed asmmolATP/g wet weight.Xanthine oxidase. For analysis of XO levels in rabbitmuscle, samples were taken of unoperated muscle and ofmuscle that had undergone ischemia and 24 hr of reperfu-sion. To compare the XO content of rabbit muscle with thatof tissue known to contain high XO levels, samples of nor-mal rat gastrocnemius muscle prior to ischemia (n4 6), andof that muscle following 2 hr of tourniquet ischemia at 36°Cand 24 hr of reperfusion (n4 6), were obtained. Allsamples were rapidly frozen as already described andthawed immediately prior to analysis.
Tissue levels of XO were determined using a modifica-tion of the method described by Im et al.19 Tissue samples(10–25 mg) were homogenized in 1 mL of 0.05 M Tris
518 Hickey et al.

buffer at pH 7.5 and 4°C. Standard solutions of isoxanthop-terine were prepared in the range 0–200 pmol. The XOassay reaction mixture was prepared in 0.05 M Tris buffer(pH 7.5) and contained pterine (2-amino-4-hydroxypteri-dine) (20 mM), EDTA (1 mM), dithiothreitol (10 mM), andphenylmethyl sulfonyl fluoride (1 mM). Equal volumes oftissue homogenate (or standards) and reaction mixture weremixed and incubated in a 37°C shaking water bath for 30min. The reaction was stopped by placing the tubes in boil-ing water. The sample was diluted with 0.1 M sodium ac-etate buffer at pH 5.4 and centrifuged at 3,000 rpm for 15min. The fluorescence of the samples was read in a fluo-rimeter (Hitachi F-2000 Fluorescence Spectrophotometer,Tokyo, Japan) set at 347 nm excitation and 405 nm emis-sion. XO activity was calculated from the standard curveand expressed as pmol isoxanthopterine/hour/10 mg dryweight of tissue.
As a reference for conversion from pmol/g/hr to Inter-national Units (IU), XO from a stock solution known tocontain 20 IU/mL (Boehringer Mannheim GmBh, Mann-heim, Germany) was diluted either 1:1,000 or 1:10,000 andthe aliquots assayed at the same time as the muscle biopsies.For conversion to IU: 1 IU4 1 pmol uric acid/minute at25°C. Using this equation and the XO stock solution ofknown activity in the assay used in these experiments, 1.0pmol/hr was found to be equivalent to 7.92 × 10−8 IU.Blood biochemistry. Blood samples taken via an earvein just before sacrifice were placed in lithium heparintubes and centrifuged to isolate the plasma fraction. Levelsof lactate dehydrogenase (LDH) and aspartate aminotrans-ferase (AST) were measured using an Olympus AU5000autoanalyser (Integrated Sciences, Melbourne, Australia).Statistical analysis. Muscle viability data were ana-lysed following arcsine transformation by one-way analysisof variance and the Student-Newman-Keuls multiple com-parison procedure. Biochemical data were analysed in asimilar manner without transformation. The Kruskal-Wallisnon-parametric multiple comparison procedure was used forthe blood enzyme data.
RESULTS
Muscle Viability
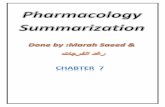
The percentage of muscle viability after 31⁄2 hours ofischemia and 24 hr of reperfusion in the Ischemic Control-Infused group and in the three groups of muscles treatedwith free radical antagonists is shown in Figure 1. It can beseen that there is no significant difference between the vi-ability of the Ischemic Control-Infused group (41.6 ± 11.3%viable) and that of the other three treated groups.
Muscle Biochemistry
The results of the various biochemical analyses areshown in Table 1.
The MPO level in untreated muscle was 0.340 ± 0.039U/g and this increased to 0.619 ± 0.026 U/g 24 hr afterischemia (P < 0.01). Ischemic muscle treated with each ofthe free radical antagonists showed elevated postischemicMPO levels, which were not significantly different fromthat of Ischemic Control-Infused muscle.
Ischemia and reperfusion caused a 49.8% reduction inreduced GSH levels compared with normal tissue levels (P< 0.01). GSH levels in the treated groups were also lowerthan in normal muscle (DFX, 35.8% reduction; SOD &CAT, 33.7% reduction; allopurinol, 13.8% reduction) butnot significantly different from levels in the Ischemic Con-trol-Infused group.
Following ischemia and reperfusion, the ATP levels inthe Ischemic Control-Infused group fell to 0.443 ± 0.074mmol/g compared to a level of 1.171 ± 0.130mmol/g inuntreated muscle (P < 0.01). Slightly smaller decreaseswere observed in postischemic muscle after treatment withDFX, SOD & CAT, and allopurinol but the levels were notsignificantly different from that of Ischemic Control-Infused muscle.
Blood Biochemistry
Blood levels of LDH and AST after 31⁄2 hours ischemiaand 24 hr reperfusion are listed in Table 2. Basal levels were281 ± 44 and 37 ± 7 U/L for LDH and AST, respectively.Levels in all postischemic groups were significantly higherthan in basal levels. However, no significant differencesbetween the Ischemic Control-Infused group and any of thetreatment groups were observed. In all groups, results weresubject to wide intra-group variation and the blood enzyme
Figure 1. Percentage viabilities of rabbit rectus femoris muscles fol-lowing 31⁄2 hr of ischemia, treatment with various free radical antago-nists, and 24 hr reperfusion. There are no significant differencesbetween the treatment groups. Results are shown as mean ± s.e.m.
Oxyradical Antagonists and Ischemia-Reperfusion 519

levels correlated poorly with the degree of necrosis shownby NBT staining.
Xanthine Oxidase Levels in Rabbit and Rat Muscle
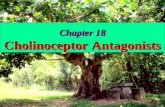
The results of the analysis of XO levels in both unop-erated and postischemic rabbit and rat muscle are shown inFigure 2. In both unoperated and postischemic rabbitmuscle, XO was barely detectable. Ischemia increased XOactivity in rat muscle approximately threefold to a levelsignificantly greater than that of all other groups examined(P < 0.05 by one-way ANOVA and Tukey’s test for mul-tiple comparisons). By contrast, rabbit muscle contains onlyminimal amounts of XO, which is not increased by a periodof ischemia and reperfusion.
DISCUSSION
To be of clinical value in combating IRI following re-plantation of a traumatically amputated part, free radicalantagonists must be effective when administered at the endof the ischemic interval and immediately before the com-mencement of reperfusion. The aim of the present study wasto determine whether administration of three specific freeradical antagonists immediately before and during the startof reperfusion protects skeletal muscle against IRI. Viabilitywas assessed after 24 hr reperfusion to provide an accuratemeasurement of long-term muscle survival.14 In many pre-vious studies, the effects of free radical antagonists havebeen assessed after less than 6 hr of reperfusion, but find-ings at such an early stage may not give an accurate pre-diction of long-term muscle survival.20 The biochemicalparameters measured were chosen to reflect different as-pects of IRI: GSH as an important tissue antioxidant, whichis depleted when free radical production increases; MPO asan index of neutrophil infiltration, neutrophils (MPO) beingone of the sources of free radicals in postischemic tissue;and ATP as an index of the energetic state of the tissue.
It is convenient to discuss the effects of each form oftreatment separately.
Desferrioxamine
The effect of DFX on IRI has been examined in severaltissues. In cardiac muscle, DFX appears to be protectivewhen given at the start of reperfusion.21–24 In skin flaps,some studies have shown beneficial effects15,25,26but othersfound no protection.12,27 In skeletal muscle, Morris et al.15
reported increased postischemic survival of the pig latissi-mus dorsi, but only if administration of the drug began 2days before injury and was continued during the period ofreperfusion. When DFX administration is limited to theclinically relevant period, immediately prior to or at the startof reperfusion, the drug appears to have little, if any, pro-tective effect on skeletal muscle viability. There are reportsof slight diminution of the postischemic rise in compartmentpressure,17 of reduced depletion of cellular antioxidants,28
and of reduced lipid peroxidation and lessened membranedysfunction29 postischemia. DFX has no effect on increasedvascular permeability in postischemic rat muscle30 and, inthe present study in rabbits, postischemic administrationhad no effect on muscle necrosis at 24 hr or on the conse-quential changes in muscle or blood biochemistry. It seemsthat if DFX is to reduce IRI in skeletal muscle it must begiven well before the ischemic insult and maintainedthrough ischemia and reperfusion. If so, this drug has littleclinical value as a postischemic treatment for IRI.
Table 2. Mean Plasma Levels of LDH and AST (U/L) inUnoperated Rabbits and in Rabbits Following 31⁄2 Hr of Ischemia,
Treatment With Various Free Radical Antagonists, and24 Hr Reperfusiona
TreatmentLDH(U/L)
AST(U/L)
Untreated 281 ± 44 37 ± 7Ischemic Control infusion 1,261 ± 307* 172 ± 33.8*DFX 583 ± 91* 87.9 ± 17.5*SOD & CAT 1,047 ± 624* 110 ± 51.3*Allopurinol 674 ± 109* 102 ± 20.9*
aResults are expressed as mean ± s.e.m. of at least 6 animals per group.*The levels of the two enzymes measured were increased significantly in allpostischemic groups relative to untreated animals.
Table 1. Tissue Levels of Myeloperoxidase (MPO), Reduced Glutathione (GSH),and ATP in Untreated Muscle and in Muscle Following 31⁄2 Hr of Ischemia, Various
Treatments, and 24 Hr of Reperfusiona
TreatmentMPO(U/g)
GSH(µmol/g)
ATP(µmol/g)
Untreated 0.340 ± 0.039 0.689 ± 0.032 1.171 ± 0.130Ischemic Control infusion 0.619 ± 0.026* 0.346 ± 0.051* 0.443 ± 0.074*DFX 0.730 ± 0.204* 0.442 ± 0.097* 0.569 ± 0.134*SOD & CAT 0.638 ± 0.112* 0.457 ± 0.059* 0.686 ± 0.203*Allopurinol 0.500 ± 0.102* 0.594 ± 0.225* 0.745 ± 0.273*
aResults are expressed as mean ± s.e.m. of at least 6 animals per group. MPO results arereported in U/g wet weight, GSH levels are expressed in µmol/g wet weight, and ATP levels areexpressed as µmol/g wet weight.*For each parameter examined, the only statistically significant change was the increase (MPO)or decrease (GSH, ATP) in all postischemic groups relative to untreated muscle (P < 0.01). Noneof the treatments was significantly different from the Ischemic Control-Infused group.
520 Hickey et al.

Superoxide Dismutase and Catalase
Several studies have shown beneficial effects of post-ischemic treatment of skeletal muscle with SOD and/orCAT in the first few hours of reperfusion of ischemic skel-etal muscle3,4,15,28,31,32and inhibition of neutrophil adhe-sion and attenuation of no-reflow have been proposed as theresponsible mechanisms.33,34However, studies with cardiacmuscle suggest that changes observed in the early stages ofreperfusion may not be an accurate guide to the protectiveeffect of SOD and CAT on muscle injury 24 hr or morelater.20 SOD and CAT may merely delay the injury by ab-lating the initial burst of superoxide production that pro-
vokes early neutrophil immigration.11 However, chemotac-tic factors are released continuously during reperfusion andstimulate neutrophils to enter the injured tissue and act as asource of superoxide for much longer than the tissue half-life of SOD (<30 min).20,35 In support of this hypothesis,Ricci et al.,32 examining the effects of SOD administrationin a canine compartment syndrome model, demonstrateddecreased technetium pyrophosphate uptake after 1 hr ofreperfusion, but found no effect on muscle function after 17hr reperfusion.
Only two early non-quantitative studies in rats haveshown long-term benefits of SOD administration on isch-emic skeletal muscle.5,6 In the present study, SOD & CAThad no effect on either muscle necrosis or biochemicalchanges after 24 hr reperfusion.
In addition to the short half-life of SOD in tissues andplasma, other factors may contribute to these negative find-ings. The two main sources of superoxide production inpostischemic muscle are endothelial XO and infiltratingneutrophils. Our findings show that, unlike rat muscle, rab-bit skeletal muscle contains only minimal amounts of XOand recent studies in the rabbit rectus femoris model showthat inhibition of neutrophil influx into postischemic musclehas no effect on muscle survival at 24 hr reperfusion.36
Taken together, these findings suggest that superoxide pro-duction does not contribute significantly to IRI in thismodel.
Alternatively, the lack of protective effect may havebeen due to the short half-lives of SOD and CAT as theseenzymes are removed from the blood within 30 min ofadministration.37 In ischemic reperfused muscle, it is likelythat oxy-radicals are produced for several hours after thestart of reperfusion, especially as neutrophils do not accu-mulate in large numbers for at least 6 hr. The treatmentsused in the present experiments would not persist longenough to quench superoxide generated in the later hours ofreperfusion. The survival of SOD and CAT in the blood canbe increased by up to 9 hr by conjugation with polyethyleneglycol.31 Polyoxyethylene-conjugated SOD has been shownto preserve the function of sarcoplasmic reticulum after 19hr reperfusion35 and to prevent lipid peroxidation and ATPdepletion in postischemic rat muscle.38 The use of long-lasting conjugates of SOD and CAT may prove to be a moreeffective protection against IRI.
Allopurinol
In both rat and canine skeletal muscle, allopurinol hasbeen shown to reduce IRI if given before the onset of isch-emia.3,31,39 The protective effect is thought to be due toreduced production of XO-derived superoxide.33,34
Allopurinol given at the start of reperfusion has beenless successful. Concannon et al.16 reported improved mac-roscopic survival of replanted limbs in rats, but did notconfirm this histologically. In rabbit muscle, Perler et al.17
Figure 2. Results of measurement of XO in rabbit and rat muscle, inboth unoperated muscle and in muscle following ischemia and 24 hrof reperfusion. In rabbit muscle, XO activity was barely detectable inboth normal and postischemic samples. In the rat muscle followingischemia and reperfusion, XO activity was significantly elevated rela-tive to all other groups examined. Results are shown as mean ±s.e.m. of six animals per group.
Oxyradical Antagonists and Ischemia-Reperfusion 521

found small, but significant, reduction in blood flow andcompartment pressure after 2 hr reperfusion, but Feller etal.6 found muscle function 5 weeks after ischemia was notpreserved. In the canine gracilis model, neither tissue ATPlevels nor O2 consumption after 1 hr of reperfusion wasimproved by postischemic administration.9 In the presentstudy, no beneficial effect on any of the parameters exam-ined was seen after 24 hr reperfusion.
The main reason for the failure of allopurinol to protectischemic rabbit muscle is its minimal content of XO, thetarget enzyme for allopurinol. XO content varies widely indifferent species.40 Results in rat tissue, which has high XOcontent, will not reflect the effect on either rabbits or hu-mans where muscle contains only minimal amounts of XOand allopurinol has little, if any, value in the clinical man-agement of IRI in skeletal muscle.41
A further limitation of allopurinol is that the transfor-mation to its active metabolite, oxypurinol, the effectiveinhibitor of XO, takes several hours.42 Hence, if given at thestart of reperfusion, allopurinol cannot affect free radicalproduction in the vital early hours of reperfusion.
Summary
In summary, the present study shows that a single post-ischemic infusion of DFX, SOD & CAT, or allopurinol hasno protective effect on the viability of rabbit skeletal musclefollowing 31⁄2 hr ischemia and 24 hr reperfusion. It may bethat free radicals are not important in this type of injury orthat the free radical scavengers used did not achieve a pro-tective concentration during the critical period of the isch-emic injury. Inhibitors targeted more specifically to the oxi-dants produced within the postischemic muscle or longer-acting free radical scavengers might provide more effectiveprotection.
ACKNOWLEDGMENTS
This study was supported by a project grant from theNational Health and Medical Research Council, Canberra,Australia.
REFERENCES
1. Freeman BA, Crapo JD: Biology of disease. Free radicals and tissueinjury. Lab Invest47:412–426, 1982.
2. Powell SR, Tortolani AJ: Recent advances in the role of reactiveoxygen intermediates in ischemic injury. I. Evidence demonstratingpresence of reactive oxygen intermediates; II. Role of metals in site-specific formation of radicals.J Surg Res53:417–429, 1992.
3. Korthuis RJ, Granger DN, Townsley MI, Taylor AE: The role ofoxygen-derived free radicals in ischemia-induced increases in canineskeletal muscle vascular permeability.Circ Res57:599–609, 1985.
4. Perry MO, Fantini GA: Ischemia: Profile of an enemy. Reperfusioninjury of skeletal muscle.J Vasc Surg6:231–234, 1987.
5. Weiss APC, Carey LA, Randolph MA, Moore JR, Weiland AJ: Oxy-gen radical scavengers improve vascular patency and bone-muscle cell
survival in an ischemic extremity replant model.Plast Reconstr Surg84:117–123, 1989.
6. Feller AM, Roth AC, Russell AC, Eagleton B, Suchy H, Debs N:Experimental evaluation of oxygen free radical scavengers in the pre-vention of reperfusion injury to skeletal muscle.Ann Plast Surg22:321–331, 1989.
7. Belkin M, La Morte WL, Wright JG, Hobson RW II: The role ofleukocytes in the pathophysiology of skeletal muscle ischemic injury.J Vasc Surg10:14–19, 1989.
8. Downey JM, Miura T, Eddy LJ, Chambers DE, Mllert T, Hearse DJ,Yellon DM: Xanthine oxidase is not a source of free radicals in theischemic rabbit heart.J Mol Cell Cardiol 19:1053–1060, 1987.
9. Faust KB, Chiantella V, Vinten-Johansen J, Meredith JH: Oxygen-derived free radical scavengers and skeletal muscle ischemic/reperfusion injury.Am J Surg54:709–719, 1988.
10. Hawkes JS, Young CMA, Cleland LG: Ischaemia reperfusion injury inpedicle skin flaps in the pig: Lack of protective effect of SOD andallopurinol.Br J Plast Surg42:668–674, 1989.
11. Messmer K, Sack FU, Menger MD, Bartlett R, Barker JH, HammersenF: White cell-endothelium interaction during postischemic reperfusionof skin and skeletal muscle.Adv Exp Med Biol242:95–98, 1988.
12. Nishikawa H, Manek S, Fryer PR, Green CJ: Reperfusion injury in ratadipomusculocutaneous flaps: An ultrastructural and microangio-graphic study.Br J Plast Surg44:500–505, 1991.
13. Smith A, Hayes G, Romaschin A, Walker P: The role of extracellularcalcium in ischemia/reperfusion injury.J Surg Res49:153–156, 1990.
14. Hickey MJ, Hurley JV, Angel MF, O’Brien BMcC: The response ofthe rabbit rectus femoris muscle to ischemia and reperfusion.J SurgRes53:369–377, 1992.
15. Morris SF, Pang CY, Lofchy NM, Davidson G, Lindsay WK, ZukerRM, Boyd B: Deferoxamine attenuates ischemia-induced reperfusioninjury in the skin and muscle of myocutaneous flaps in the pig.PlastReconstr Surg92:120–132, 1993.
16. Concannon MJ, Dooley TW, Puckett CL: Improved survival in a re-plantation model containing ischemic muscle.Microsurgery12:18–22,1991.
17. Perler BA, Tohmeh AG, Bulkley GB: Inhibition of the compartmentsyndrome by the ablation of free radical-mediated injury.Surgery108:40–47, 1990.
18. Kohout M, Lepore DA, Knight KR, Van Gelder J, O’Brien BMcC,Stewart AG, Morrison WA: Cool perfusion solutions for skin flaps: Anew mixture of pharmacological agents which improves skin flap vi-ability. Br J Plast Surg48:132–144, 1995.
19. Im MJ, Shen W-H, Pak CJ, Manson PN, Bulkley GB, Hoopes JE:Effect of allopurinol on the survival of hyperemic island skin flaps.Plast Reconstr Surg73:276–278, 1984.
20. Engler R, Gilpin E: Can superoxide dismutase alter myocardial infarctsize?Circulation 79:1137–1142, 1989.
21. Ambrosio G, Zweier JL, Jacobus WE, Weisfeldt ML, Flaherty JT:Improvement of postischemic myocardial function and metabolisminduced by administration of deferoxamine at the time of reflow: Therole of iron in the pathogenesis of reperfusion injury.Circulation76:906–915, 1987.
22. Bolli R, Patel BS, Jeroudi MO, Li X-Y, Triana JF, Lai EK, McCay PB:Iron-mediated radical reactions upon reperfusion contribute to myo-cardial ‘‘stunning.’’ Am J Physiol259:H1901–H1911, 1990.
23. Reddy BR, Kloner RA, Przyklenk K: Early treatment with deferox-amine limits myocardial ischemic/reperfusion injury.Free RadicalsBiol Med 7:45–52, 1989.
24. Qayumi AK, Jamieson WR, Poostizadeh A, Germann E, Gillespie KD:Comparison of new iron chelating agents in the prevention of isch-emia/reperfusion injury: A swine model of heart-lung transplantation.J Invest Surg5:115–127, 1992.
25. Angel MF, Narayanan K, Swartz WM, Ramasastry SS, Kuhns DB,Basford RE, Futrell JW: Deferoxamine increases skin flap survival:Additional evidence of free radical involvement in ischemic flap sur-gery.Br J Plast Surg39:469–472, 1986.
26. Yoon JO, Im MJ, Manson PN, Bulkley GB, Hoopes JE: The role ofmetal ions in ischemia/reperfusion injury in skin flaps.J Surg Res46:163–165, 1989.
27. Nishikawa H, Gower JD, Fryer PR, Charlett A, Manek S, Green CJ:
522 Hickey et al.

Ultrastructural changes and lipid peroxidation in rat adipomusculocu-taneous flap isotransplants after normothermic storage and reperfu-sion.Transplantation54:795–801, 1992.
28. Purucker E, Egri L, Hamar H, Augustin AJ, Lutz J: Differences inglutathione status and lipid peroxidation following ischemia and reper-fusion.Res Exp Med191:209–217, 1991.
29. Fantini GA, Yoshioka T: Deferoxamine prevents lipid peroxidationand attenuates reoxygenation injury in postischemic skeletal muscle.Am J Physiol264:H1953–H1959, 1993.
30. Grossfield S, Firrell JC: The effect of deferoxamine on ischemicchanges in rat skeletal muscle: A preliminary study.J Invest Surg5:375–381, 1992.
31. Punch J, Rees R, Cashmer B, Wilkins E, Smith DJ, Till GO: Xanthineoxidase: Its role in the no-reflow phenomenon.Surgery11:169–176,1992.
32. Ricci MA, Graham AM, Corbisiero R, Baffour R, Mohamed F, SymesJF: Are free radical scavengers beneficial in the treatment of compart-ment syndrome after acute arterial ischemia?J Vasc Surg9:244–250,1989.
33. Suzuki M, Grisham MB, Granger DN: Leukocyte-endothelial cell ad-hesive interactions: Role of xanthine oxidase-derived oxidants.J Leu-koc Biol 50:488–494, 1991.
34. Menger MD, Steiner D, Messmer K: Microvascular ischemia-reperfusion injury in striated muscle: Significance of ‘‘no-reflow.’’AmJ Physiol263:H1892–H1900, 1992.
35. Lee KR, Cronenwett JL, Shlafer M, Corpron C, Zelenock GB: Effect
of superoxide dismutase plus catalase on Ca2+ transport in ischemicand reperfused skeletal muscle.J Surg Res42:24–32, 1987.
36. Breidahl AF, Hickey MJ, Stewart AG, Hayward PG, Morrison WA:Effects of low dose intra-arterial monoclonal antibodies to ICAM-1and CD11/CD18 on local and systemic consequences of ischaemia/reperfusion injury in skeletal muscle.Br J Plast Surg49:202–209,1996.
37. Turrens JF, Crapo JD, Freeman BA: Protection against oxygen toxicityby intravenous injection of liposome-entrapped catalase and superox-ide dismutase.J Clin Invest73:87–95, 1984.
38. Kawasaki S, Sugiyama S, Ishiguro N, Ozawa T, Miura T: Implicationof superoxide radicals on ischemia-reperfusion-induced skeletalmuscle injury in rats.Eur Surg Res25:129–136, 1993.
39. McCutchan HJ, Schwappach JR, Enquist EG, Walden DL, Terada LS,Reiss OK, Leff JA, Repine JE: Xanthine oxidase-derived H2O2 con-tributes to reperfusion injury of ischemic skeletal muscle.Am J Physiol258:H1415–H1419, 1990.
40. Picard-Ami LA Jr, MacKay A, Kerrigan CL: Pathophysiology of isch-emic skin flaps: Differences in xanthine oxidase levels among rats,pigs and humans.Plast Reconstr Surg87:750–755, 1991.
41. Dorion D, Zhong A, Chiu C, Forrest CR, Boyd B, Pang CY: Role ofxanthine oxidase in reperfusion injury of ischemic skeletal muscles inpig and the human.J Appl Physiol75:246–255, 1993.
42. Spector T: Oxypurinol as an inhibitor of xanthine oxidase-catalyzedproduction of superoxide radical.Biochem Pharmacol37:349–352,1988.
Oxyradical Antagonists and Ischemia-Reperfusion 523