Parity Violating Electron Scattering in Resonance region (Res-Parity)
Upload
karen-reedCategory
view
213download
0
Influence of Age and Parity on the Emotional Care Given to Women Experiencing Miscarriages Karen Reed
Obstetrical nurses (N = 309) participated in a study of the hypothetical injuence of patients’ age and parity status on nurses’ emotional care fm women who had experienced miscam’age. Vignettes in which age and parity were varied were mailed to the sample along with a questionnaire. AJier factor analysis, three measures of emotional care were used as the dependent variabb: emotional seriousness, F’ority of care, and emotional support. Analysis of variance showed that the parity status of the woman was a significant variable in the nurses’ perupions of emotional sa’ousness and parity of care, but did not affect the nurses’ perceptions of the need fm emotional support. Age was not a significant variabh in the three measures of emotional care.
* * *
U nexpected or involuntary pregnancy losses occur frequently to women during the reproductive years. Conservative predictions place the rate of miscarriage at about 20 percent of confirmed
pregnancies (Friedman & Gradstein, 1982). Others (Oakley, 1986) place the rate of miscarriages closer to the 50 percent mark. There is also some evidence that the rates have in- creased in the past 20 years (Cohen, Zilka, Middleton & O’Donnohue, 1978 Knuppel, 1985).
Although the experience of miscarriage is fairly common and not potentially life-threatening, miscarriages can have emotional repercussions for the women who experience them. For many women, a miscarriage has a profound em@ tional effect that can last for an extended period.
A search of the literature revealed that women who ex- perience miscarriages perceive health care professionals- particularly physicians and nurses-to be cold and indifferent to their situation (Hutti, 1984; bvell, 1983). The reasons for or factors contributing to the patients’ perceptions of indif- ference of nurses and physicians have not as yet been iden- tified. The purpose of this study was to determine whether or not certain factors, namely, the age of the patient and her parity status, would affect the emotional care given to women who experience miscarriages.
Review of the Literature It was not until the early 1970s that the subject of preg-
nancy loss was considered in the professional literature. The focus of the early literature was on the emotional impact of stillbirths and perinatal death. Reporting research done in the late 196Os, Wolff, Nielson and Schiller (1970) focused on the emotional reactions ofwomen following the loss of a baby at birth. They followed 50 from 1 to 3 years after their baby’s death. The researchers found that all the women were depressed initially following the death and that a majority of the women exhibited a grief reaction to the event. Of the 50
women, 22 refused to discuss their attitudes about doctors and nurses. This resistance was surprising to the authors because of the womens’ willingness to discuss the events surrounding the death of the baby. Of the remaining 28 women in the sample, 13 found their doctors to be warm, 10 felt they were cold, and 5 felt they were neutral. The women rated nurses in much the same manner: 10 women felt the nurses had been warm to them, 11 felt the nurses had been cold, and 7 felt they were neutral.
Kennell, Slyter and Klaus (1970) reported on the reactions of women to tactile contact with their babies who later died. This study has since been regarded as the classic study of the emotional impact of stillbirth. Before this study, contact with an infant who might die was considered to be detrimental to the emotional health of the mother. Contact with the infant was prohibited so that bonding would not occur. It was thought that this would decrease the emotional trauma the woman would go through at the death of the infant. In this study, women who lost a baby through early perinatal death were divided into two groups-those who were allowed to touch their infant and those who were not. Interviews were held to ascertain the effect of tactile contact; contact seems not to have had any detrimental effects.
In 1982, the study of miscarriages as a separate entity first appeared in the professional literature. In an editorial, Stephany (1982) made this statement:
The grief of an early miscarriage is not easily resolved. Unlike the patient who loses a child later in pregnancy, there is no concrete image of the child to say goodbye to. This patient has no formed baby to see or hold. She walks into the hospital pregnant and leaves nonpregnant, often only a few hours later. (p. 89)
There were differences of opinion expressed in the early literature on how to treat a woman who had a miscarriage. Wetzel (1982), a clinical nurse specialist, advocated that time be spent acknowledging the miscarriage and letting the mother discuss the experience. The message given to emer- gency room physicians however, was quite different:
Anything that will minimize the magnitude of the miscarriage for the woman should be exploited.. . .I think the emergency physician should examine a women right away to confirm that she is having an inevitable or incomplete miscarriage and then go ahead with the suction curet- tage. That way you rapidly stop the bleeding and minimize the physical
KAREN S. REED, R.N., Ph.D., Delta Omega, is Associate Professor a t The university of Akron. The research reported here was sup- ported by a Post Baccalaureate Faculty FellOWShlp, Department of Health and Human Services. correspondence to College of NUrS- Ing, university @Akron, Akron, OH 44325.
Accepted for publication August 24.1989.
Volume 22, Number 2, Spring 1990 89

Influence of Age and Parity on the Emotional Care Gwen to Women Experiencing Miscarriages
and emotional discomfort and get the woman back to normal with a small, empty uterus. (“Treating Early Miscarriage,” 1983, p. 148)
Most clinical literature took the position that miscarriages should be treated in the same manner as any other type of perinatal loss (Estok & Lehman, 1983; Stack, 1984). Miscar- riages represent several types of loss. One is the loss of the fantasized child. Rubin (1967) and others indicated that the beginnings of bonding occur between the mother and her fantasy child. It is during the pregnancy that most mothers and fathers begin to plan a hture as a family around the addition of a child. A miscarriage prevents those plans from coming to fruition. A second loss concerns the self-concept of the woman. Many women see their inability to stay pregnant as an inability to fulfill a basic requirement of womanhood-the bearing of offspring. The damage to the selfconcept may lead to the woman’s questioning of her own self-worth, especially if the pregnancy was planned (@irk, 1979).
One consistent point in the literature is that the involun- tary loss of any pregnancy is perceived by the woman as a significant event in her life-one that was difficult for the woman to handle. Miscarriages are perhaps especially dif- ficuIt to deal with because the loss is rather ambiguous. Often there is no tangible evidence of the pregnancy to mourn. And in Western cultures, there are no rituals or societal customs that provide a socially acceptable means to grieve the miscarriage.
As with other types of involuntary pregnancy loss, some authors reported that women who experience miscarriages perceive physicians and nurses as being cold and indifferent to their situation (Hutti, 1984; Lovell, 1983). Wall-Haas (1985) and Oakley (1986) suggested that the indifferent behavior of nurses may be based on the medical perception of a miscarriage as a simple, nonthreatening physical condi- tion. Therefore, the nurses may infer that the nonserious physical situation has little emotional impact.
There are physical attributes that increase the serious consequences for miscarriage. Menning (1982) noted that an increase in age decreases a woman’s ability to conceive or carry a child to full term. Likewise, the chances of a successful pregnancy also decrease if miscarriage occurs often. Women are labeled “habitual aborters” if three or more consecu- tive pregnancies terminate in miscarriage (Friedman & Gradstein, 1982).
If nurses were caring for women whose age and parity status placed them into the “serious miscarriage”situation, would they give more attention to the emotional impact of the experience? This study was designed to survey the responses of nurses to the emotional impact of miscarriage in situations where the age and parity status of the women varied.
Methods The responses of nurses to miscarriage were explored
through the use of a survey that utilized vignettes to repre- sent a typical, yet fictional, situation of miscarriage. Each nurse received one of nine vignettes about women of dif- ferent ages and parity who experience miscarriage. The nurses were then asked to respond to a series of questions regarding the vignette.
Sample A list of 3,000 names and addresses of obstetrical-
gynecological nurses was obtained through the North
Carolina Board of Nursing. After the list was numbered consecutively, a computer program generated a random number list. The projected sample size was 400 to give ade- quate leeway for nonresponse. Since itwas preferable to have equal numbers of subjects receiving each of the nine vignettes, the number of subjects was reduced to 396, which is divisible by nine.
Instruments The subjects were asked to respond to one of nine
vignettes that described a case of miscarriage during the third pregnancy. In each vignette, age and parity status were systematically combined to represent different situations. Three levels each of age (20, 29,38) and parity status (0 , 1 , 2) were used to create the nine different vignettes. The nurses were asked to respond to the situation presented to them as if it had occurred on a typical day in their clinical setting, and as if they were responsible for the patient’s care.
The questionnaire consisted of 14 items that measured various aspects of emotional care. The respondents were instructed to read the vignette and circle the number, from 1 to 7, that described how they would respond to the patient in the vignette situation. They were told that there was no one correct answer. The items were constructed so that item scores at the high end of the scale indicated a greater likelihood of emotional care in the situation. A standardized Cronbach’s alpha of .82 was obtained for the scale items.
Procedure The data were collected using a mailed questionnaire sent
to the home address of the subjects. A series of three mailings was used to obtain the highest response rate possible. At the end of the data collection period, the response rate was 335 (84%) with 309 (78%) of the questionnaires usable.
Results Most of the nurses were married (82%) and were between
the ages of 25 and 40 (69%). Most had worked full-time (71 %) in obstetrics for less than 10 years (55%). Most (78%) were employed in a hospital and were staff nurses (59%); most were educated at the Associate Degree or Diploma level (67%). Most (73%) of the respondents had not experienced a miscarriage themselves. The nine different vignettes were evenly represented. Each vignette accounted for a p proximately 10 percent of the return data, with cell sizes ranging from 29 to 38.
To validate that the instrument did in fact measure a concept known as emotional care, a factor analysis was per- formed. Using avarimax rotation, the factor analysis retained four factors in the solution before reaching the eigenvalue limit of one. The emergence of four factors suggested that the instrument measured more than one concept. This brought into question whether or not scores from the instru- ment could be summed for a measure of emotional care. In additional testing of construct validity, the four factors were treated as subscales. A series of correlations-item to scale, item to subscale, subscale to scale, and subscale to subscale- were used to measure the instrument. Throughout the cor- relations, two questions consistently did not meet the criteria for acceptance. Since these questions made up the fourth factor, there was reason to doubt that the fourth factor was
90 IMAGE: Journal of Nuning Scholanhip

Influence of Age and Parity on the Emotional Care Given to Women Experiencing Miscarriages
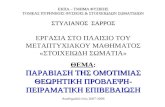
Factor 1: Emotional Seriousness -low do you think the miscarriage will affect Ms. Smith’s ifestyle in the next few weeks? (.83)
How much emotional distress do you think Ms. Smith will sxperience as a result of the miscarriage? (.83)
How long do you think it will take Ms. Smith to recover from her experience emotionally? (.62)
How much of an emotional reaction do you expect Ms. Smith to have in this situation? (.68)
How much assistance do you think Ms. Smith may need in anticipating what to say to family and friends? (54)
Factor 2 Priority of Care Compared to the other patients you are taking care of, how much time will you need to care for Ms. Smith? (.81)
What priority would Ms. Smith’s nursing care receive, compared to the other patients you ordinarily have? (.78)
How necessary do you think it is for you to keep in contact with Ms. Smith after she goes home? (.61)
Factor 3 Emotional Support How much would you encourage Ms. Smith’s significant others to stay with her i f she asks for them? (.80)
How willing would you be to take the initiative to refer Ms. Smith to a perinatal death support group? (54)
How empathetic do you think you could be to Ms. Smith in this situation? (.62)
NOTE: Loadings of the items on the factors in parentheses.
IGURE 1. Factors within the emotional care instrument.
a measurement of emotional care. Thus factor four was eliminated (see the 11 items in Fig. 1).
Factor loadings for the items ranged from .54 to 33, indicating a good fit of the items to factors (see Fig. 1). No items loaded on more than one factor. Factor 1 consisted of items measuring the nurses’ perceptions of the impact that the miscarriage would have on the woman. Factor 2 consisted of items measuring the priority that the miscarriage patient would have in the nurses’ regular caseloads. Factor 3 con- sisted of items measuring the nurse’s perception of the woman’s need for emotional support,
A two-factor analysis of variance (ANOVA) was used to test for main and interaction effects of age and parity status on the three measures of emotional care. It was expected that as age increased, the nurses’ rating of emotional seriousness would rise. Further, it was expected that as the parity level went down, perceived seriousness would increase. The results of the analysis are summarized in Table 1.
Parity status, however, affected significantly the nurses’ ratings of the emotional seriousness of the situation. The mean scores of the nurses on the emotional seriousness of a miscarriage was 5.83 for a woman with no children; this decreased to 5.32 if the woman had one living child and decreased further if the woman had two living children (5.18). A subsequent Tukey’s Honestly Significant Dif- ference (HSD) test suggested that nurses rated the present miscarriage as being less emotionally serious if the woman had at least one living child.
Priority of care It was expected that as the age of the woman having a
miscarriage increased, her priority for the nurses’ time would increase. Also, as the parity level went down, the priority of care would rise. Again, age did not alter significantly the nurses’ views of the priority of care given in the situation, and there were no interaction effects. The woman’s parity status, however, did affect the nurses’ ratings of priority of care.
The mean score for priority of care was 4.83 for a woman with no children. If the woman had at least one living child, this decreased to 4.46 and if she had two living children, it remained approximately the same (4.47). Again, a Tukey’s HSD confirmed that the nurses rated a woman who had at least one living child as having a lower priority of care than one who had no living children.
Need for Emotional Support It was expected that the nurses would rate an older woman
as needing more emotional support than a younger woman and would rate a woman with fewer living children as needing more emotional support. However, neither age nor parity level had a significant effect on nurses’ perception of need. The mean scores for older women were higher than were those of younger women, indicating that the nurses may have taken into account the woman’s age in rating the need for emotional support.
Discussion Overall, the mean scores of emotional care were higher
than anticipated, given that the literature reported nurses to be cold and indifferent in all miscarriage situations. The high mean scores across situations seem to indicate that the emo- tional care of a miscarriage patient was important.
Of the three measures, the mean scores on priority of care were the lowest (in the 4.0 range). In comparison to the other two measures, the lower scores may indicate that, though the nurses may see the emotional care of miscarriage patients as being important, they may not be able to convey the concern in a direct manner (i.e., through spending time with the patient). If nurses do not spend time with the miscarriage patient, it may help explain how patients have interpreted
TABLE 1. Effects of Age and Parity Status on Nurses’ Percep tion of the Setlousnoso of the Miacarrtrw
Source 88 df MS Fvalue D
Emotional Seriousness The woman’s age had no significant effect on the nurses’
ratings of the emotional seriousness of the situation. There was no interaction effect of age and parity status on the ratings of emotional seriousness.
Main effects Woman’s age 2.84 2 1.42 2.20 .113 Parity 25.70 2 12.85 19.88 .0001
Interaction 1.25 4 .31 .a .74a Error 188.10 291 .65 Total 218.41 299 .73
Volume 22, Number 2, Spring 1990 91

Innuence of Age and Parity on the Emotional Cam Given to Women Experiencing Miscarriages
92 IMAGE: Journal of Nursing Scholarship
the nurse’s attitude as one of indifference. Nurses consis- tently stated in anecdotal remarks that priority care in an obstetrical unit is given to the woman who is in active labor or in physical danger. Those who are physically stable are often not given as much time as they need simply because of the demands of the work place. Several of the nurses recog- nized the problem of giving the miscarriage patient the emotional care she needs. One nurse put it very succinctly:
In [labor and delivery] a pregnant mother with aviable fetus will always have priority overa stable miscarriage mother. On a busy day emotional support is the f irs t thing dropped by the wayside. I am reduced to running from patient to patient evaluating Mom and fetus, praying the fetal monitor does not show the baby has been in distress while I was with someone else. Forgotten are perinatal death, support groups, her feelings on future babies, or contact after discharge. That’s life!
The mean scores on emotional support were the highest of the three scores (in the 6.0 range). The emotional support items dealt with the need for others to provide emotional support, not the nurse. Thus the nurses may be aware of the need for support, but may feel that the support could be given by someone other than themselves.
The women’s age did not predict emotional seriousness or priority of care, and only approached significance as a predic- tor of emotional support. Nurses may have not responded to the age of the women as a significant factor in emotional care simply because nurses see a greater range of ages in their patients than in the past.
Parity status affected significantly the nurses’ responses to the vignettes. In the vignettes, the woman had experienced three pregnancies which resulted in either no living children or one or two living children. The situation of three pregnancies and no live births is a clear indication that the woman may have an infertility problem. The nurses may have had an increased awareness of the emotional seriousness of the situation. Further study of the effect of parity status needs to be done using differing gravida para combinations. Nurses might react quite differently to a first pregnancy that ends in miscarriage.
Conclusions The results of this study do not support the idea that nurses
are indifferent to miscarriage patients. Nurses’ ratings of emotional care for miscarriage patients were high, regardless of parity status or age of the woman. Parity status became a factor only in deciding which women needed more emo- tional care than others.
The findings of this study would support the idea that nurses do in fact perceive the need for emotional care to women with miscarriages. It may be that the women’s per- ceptions of the situation are not clear. In a crisis situation such as miscarriage, persons tend to have difficulty in per- ceiving their surroundings. The emotional upheaval of mis- carriage may make women feel depressed or anxious. Both states can lead to misinterpretations of the environment and of others within the environment.
Because the findings of this study are based on self-report to hypothetical situations, the idea that nurses are not s u p portive cannot be ruled out. It may be that nurses do in fact regard women with a miscarriage as needing less emotional care than do other obstetrical patients. The wish of nurses to be seen as providing high levels of emotional care may have influenced their responses; that is, nurses may have responded to the questionnaire as they thought they
“should” have, rather than as they normally would react. Further, in the situation presented in the vignettes, no men- tion was made of the number of other patients the nurse would be caring for, or what the situation at work might be. A more detailed description of the work load might have led the nurses to rate differently their ability to give emotional care. Clearly, further study is needed in the actual clinical situation to determine nurses’ resDonses.
The anecdotal responses indicated that the topics of emo- tional care and miscarriage are of interest to nurses working in the obstetrical field. More than half of the respondents took the time to add comments concerning their feelings about miscarriage patients. Many chose to describe personal accounts of what had happened in their practice or private lives. Most felt that the research topic was timely. Based on the results of the study and the anecdotal comments, the following recommendation is made.
Because a miscarriage patient is admitted into a hospital only briefly, if at all, there needs to be some method of providing follow-up care that focuses on both the emotional and physical needs of the family. None of the nurses reported that their institutions had an established protocol for the care of miscar- riage patients. In fact, quite a few nurses felt that it was not part of their job to contact the miscarriage patient after she went home. Common responses were “[I] separate my home and work life,” ‘This is not the role of a staff nurse in the hospital,” and “Although I feel it is very important [to stay in touch], I must admit this isn’t done at our institution.”
A protocol similar to those used in other types of perinatal death may be in order. If the staff nurses who are in contact with the patients are not able or willing to provide the emotional care needed, then there needs to be some mechanism for referring patients to others who can provide the emotional care as well as information about available supports before they leave the health care setting.
References
Cohen, L., Zilka, S.. Middleton, J., & O’Donnohue, N. (1978). Perinatal mortality: Assisting parental affirmation. American Journal of Orthopsychiahy, 48,727-731.
Estok, P., & Lehman. A. (1983). Perinatal death: Grief support for families. Birth, 10, 17-25.
Friedman, R., & Gradstein, B. (1982). Suwivingpregnancy loss. Boston: Little, Brown and Company.
Hutti, M. (1984).An examination ofperinatal death literature: Implicationsfor nursing practice and research. Health Care for Women International, 5,387-400.
Kennell, J., Slyter. H., & Klaus, M. (1970). The mourning response of parents to the death of a newborn infant. The New England Journal of Medicine, 283,344 -349.
Knuppel, R (1985). Ectopic pregnancy. Perinatal PreSq 9(1), 21. Lovell, A. (1983). Women’s reactions to late miscarriage, stillbirth and perinatal death. Health Vitor, 56,325-327.
Menning, B. (1982). The psychosocial impact of infertility. Nursing Clinics of Nortb America, 17, 155-163.
Oakley, A. (1986). Miscarriage and its implications. Midwife Health Visitor and Com- munity Nurse, 22,123-126.
Quirk, T. (1979). Crisis theory, grief theory, and related psychosocial factors: The framework for intervention. J o d of Nurse Midwifery, 24,1?-19.
Rubin. R. (1967). Attainment of the maternal role. Nlwing Research, 16, 237-245. Stack, J. (1984). The psychodynamics of spontaneous abortion. American Journal of
Stephany, T. ( 1982). Early miscarriage: Are we too quick to dismiss the pain? RN, 45.89. Treating early miscarriage in the E.D. (1983). Emergency Medicine, 15,148-152. Wall-Haas, C. (1985). Women’s perceptions of first trimester spontaneous abortions.
Werzel, S. (1982). Are we ignoring the needs of the woman with a spontaneous
Wolff, J.. Nielson, P.. & Schiller, P. (1970). The emotional reaction to a stillbirth.
Orthopsychiatry, 54, 162-167.
Journal of Obstetric, Gynecologic, and Neonatal Nursing, 14.50-53.
abortion? American Journal of Maternal Child Nursing, 7,258459.
American Journal of Obstetrics and Gynecology, 108,73-77.