![GLICK I Judge Gfitbe]t · 2017-11-16 · Glick also obtained the power of attomey or otherwise had control over bank accounts with significant deposits. 3. Glick and his companies,](https://static.fdocuments.net/doc/165x107/5f4fb49b064cf52aed0d63c8/glick-i-judge-gfitbet-2017-11-16-glick-also-obtained-the-power-of-attomey-or.jpg)
Inflammatory Bowel Disease Sarah R. Glick and Ryan S ... · Inflammatory Bowel Disease Sarah R....
14
DOI: 10.1542/pir.32-1-14 2011;32;14 Pediatrics in Review Sarah R. Glick and Ryan S. Carvalho Inflammatory Bowel Disease http://pedsinreview.aappublications.org/content/32/1/14 located on the World Wide Web at: The online version of this article, along with updated information and services, is Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly by Rachel Boykan on November 9, 2011 http://pedsinreview.aappublications.org/ Downloaded from
Transcript of Inflammatory Bowel Disease Sarah R. Glick and Ryan S ... · Inflammatory Bowel Disease Sarah R....

DOI: 10.1542/pir.32-1-142011;32;14Pediatrics in Review
Sarah R. Glick and Ryan S. CarvalhoInflammatory Bowel Disease
http://pedsinreview.aappublications.org/content/32/1/14located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from
Inflammatory Bowel DiseaseSarah R. Glick, MD,*
Ryan S. Carvalho, MD†
Author Disclosure
Drs Glick and
Carvalho have
disclosed no financial
relationships relevant
to this article. This
commentary does
contain a discussion
of an unapproved/
investigative use of a
commercial
product/device.
Objectives After completing this article, readers should be able to:
1. Develop a differential diagnosis and plan an initial evaluation for the child oradolescent who presents with bloody diarrhea and abdominal pain.
2. Recognize that growth failure and pubertal delay may be an initial presentation ofCrohn disease.
3. List the extraintestinal manifestations of inflammatory bowel disease (IBD).4. Discuss the genetic advances in understanding the pathogenesis of IBD.5. Describe the current treatments for IBD and the common adverse effects.
IntroductionIBD is a complex, multifactorial disease characterized by chronic inflammation in theintestinal tract of a genetically predisposed host. The spectrum of IBD in children primarilyincludes ulcerative colitis (UC) and Crohn disease (CD). With pediatric patients nowaccounting for 20% to 25% of newly diagnosed cases, it is becoming increasingly importantfor pediatricians to recognize the symptoms of IBD. (1) In this review, we discuss theepidemiology, clinical presentation, diagnosis, and complications of IBD, with specificemphasis on growth failure and pubertal delay because these are unique manifestations inchildren. We also describe newer, less invasive diagnostic techniques and current trends inmanagement and advances in the pharmacologic treatment of affected children.
Epidemiology and DemographicsThe epidemiologic patterns of pediatric IBD have evolved over the past few decades, withsignificant increases in both incidence and prevalence. The current incidence is 5 to 11 per100,000 children, with a recent statewide survey from Wisconsin reporting the annualrate of diagnosis as 4.56 per 100,000 for CD and 2.14 per 100,000 for UC. (2) Canadian
studies have reported an acceleration in new diagnoses from9.5 per 100,000 in 1994 to 11.4 per 100,000 in 2005. Themost significant increases were among the younger agegroups, with the incidence rising 5% annually in childrenyounger than 4 years of age and 7.6% annually in childrenages 5 to 9 years. (3)
The mean age at diagnosis of pediatric IBD in the UnitedStates is 12.5 years, (2) with 20% of children diagnosedbefore the age of 10 years and fewer than 5% diagnosedbefore age 5 years. Males seem overrepresented in new casesof pediatric CD, although an equal number of males andfemales receive a UC diagnosis. (4)
Many risk factors have been associated with IBD, includ-ing family history, ethnicity, and tobacco use. Up to 25% ofchildren who develop IBD have a positive family history ofIBD. (5) Children who have a first-degree relative affectedby either UC or CD have a 10 to 13 times higher risk fordeveloping IBD. (5) Monozygotic twin concordance is ap-proximately 50% for CD and nearly 20% for UC. (6)
In the United States, population-based studies histori-
*Wright State University Boonshoft School of Medicine, Children’s Medical Center of Dayton, Dayton OH.†The Ohio State University College of Medicine, Nationwide Children’s Hospital, Columbus, OH.
Abbreviations5-ASA: 5-aminosalicylatesCD: Crohn diseaseEN: erythema nodosumESR: erythrocyte sedimentation rateFC: calprotectinFL: lactoferrinIBD: inflammatory bowel diseaseIGF-1: insulin-like growth factor-1MRI: magnetic resonance imagingPG: pyoderma gangrenosumPSC: primary sclerosing cholangitisSNP: single-nucleotide polymorphismTNF: tumor necrosis factorUC: ulcerative colitisVCE: video capsule endoscopy
Article gastrointestinal
14 Pediatrics in Review Vol.32 No.1 January 2011
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

cally have shown a higher prevalence of IBD in patientsof European or African descent than in patients of His-panic or Asian descent. (7) Notably, Jewish ancestry(Ashkenazi more than Sephardic) is a significant riskfactor for the development of IBD. However, morerecent pediatric-specific population studies detected nodifferences in IBD frequency between ethnic groups. (2)
The prevalence of IBD is highest in the industrializedworld, including North America, northern Europe, andthe United Kingdom. However, with progressive mod-ernization, the prevalence is now increasing in the devel-oping world. Tobacco use is linked closely with an in-creased risk of IBD. In smokers, the probability ofdeveloping CD is twice as high as for nonsmokers. (7)Passive exposure to smoking may be influential as well. (8)
GeneticsA genetic predisposition to IBD has been hypothesizedfor decades because of the strong familial pattern ofdisease. Linkage analyses and genome-wide associationstudies have identified numerous IBD candidate genes.Many share a connection to the immune, inflammatory,or bacterial recognition pathways, which are fundamen-tal mechanisms in the pathogenesis of IBD.
In 2001, the NOD2/CARD15 gene, located on chro-mosome 16q in the IBD1 susceptibility locus, was asso-ciated with CD. Three high-risk single nucleotide poly-morphisms (SNPs) are suggested to alter recognitionof bacterial peptidoglycans in monocytes, macrophages,gut epithelial cells, and Paneth cells. NOD2 mutationscan impair the degradation of gut bacteria, leading to anaccumulation of bacterial antigens and predisposing tomucosal T-cell activation.
Nearly 40% of white patients who have CD carry oneof these NOD2 SNPs compared with 20% of controls. (9)These allelic variants also have phenotypic implicationsfor those who have CD, with earlier age of onset, stric-turing disease, and ileal involvement occurring morefrequently.
The IBD5 locus on chromosome 5q31 is associatedwith a higher susceptibility toward CD. Patients whohave CD and IBD5 locus polymorphisms may have moreperianal disease, colonic disease, and importantly in pe-diatric patients, decreased weight and height at diagno-sis. (10) There also has been a weak association of theIBD5 locus with UC.
The IBD3 locus on chromosome 6 contains themajor histocompatibility complex genes, which also maycontribute toward IBD predisposition. The DRB1*1502gene has been associated with UC, and the DRB1*07gene has been associated with CD, particularly in patients
who have ileal disease without a high-risk NOD2 poly-morphism. The DRB1*0103 allele has been linked toUC and colonic CD. Patients who have UC and thisvariant seem to have a greater predisposition towardmore extensive and severe colonic involvement. Therealso seems to be an association between IBD3 locusvariants and the extraintestinal manifestations of uveitisand peripheral arthropathy. (9)
The field of IBD genetics is continuously expanding,but genetic testing is currently limited to research. In thefuture, children who have IBD may undergo genetictesting to quantify disease risk in family members or topredict phenotypic expression.
CausesThe precise causes of IBD remain unknown, but thecurrent understanding involves a genetic predispositioncombined with a dysregulation between the immunesystem and the antigenic environment in the gastrointes-tinal tract, leading to inflammation and damage. (11)The major pathogenic mechanism underlying CD is anexcessive Th1 immune response, whereby CD4! T cellsbecome upregulated and markedly resistant to apoptosis.(12) An excessive Th2 immune response has been impli-cated in patients who have UC. (13)
Defective gastrointestinal mucosal integrity may leadto enhanced uptake of luminal bacteria, causing thenormally protective mucosal immune system to be over-whelmed. This derangement may be a result of toler-ance to luminal antigens, a hyperreactive cell-mediatedimmune system, or specific gene mutations (such asNOD2).
It has been postulated that the unchecked intestinalimmune response to ubiquitous bacterial and entericantigens could lead to the pathologic gross tissue injurycharacteristic of IBD. Activated immune cells secretea variety of soluble mediators of inflammation, includ-ing cytokines (tumor necrosis factor [TNF]-alpha,interferon-gamma, transforming growth factor-beta, andinterleukin-2, -5, -6, -12, and -18), arachidonic acidmetabolites, reactive oxygen intermediates, streptolysins,and growth factors. (12) Activated neutrophils and mac-rophages may also release metalloproteinases, which di-gest collagen in the lamina propria and basement mem-brane and are markedly elevated in the fistulous tracts ofthose who have CD.
The most persuasive argument for a pathogenic roleof enteric flora comes from murine studies of IBD.(14)(15) The gut inflammation seen in mouse models ofIBD depends on the presence of bacterial flora. No singleinfectious agent has been reproducibly associated with
gastrointestinal inflammatory bowel disease
Pediatrics in Review Vol.32 No.1 January 2011 15
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from
IBD, but several bacterial species, including Salmonella,Helicobacter, toxigenic Escherichia coli, Listeria, andCampylobacter, have been suggested to play a role inpathogenesis. Mycobacterium paratuberculosis has beenstrongly suspected in IBD development. (16) Viral the-ories have been proposed, including the potential formeasles virus to cause a granulomatous vasculitis. (17)Another antigenic hypothesis in the development of IBDincludes the phenomenon of dysbiosis, which is an al-tered balance between protective bacteria, such as Lacto-bacillus and Bifidobacterium, and aggressive organisms,including Bacteroides, Enterococcus, and invasive E coli.(18)
Clinical PresentationUC and CD can have varied yet overlapping presenta-tions. The cardinal symptoms of UC are diarrhea, rectalbleeding, and abdominal pain. Most children presentwith an insidious history of diarrhea without systemicsigns of fever or weight loss. One third present withmoderate symptoms, including hematochezia, abdomi-nal cramping associated with fecal urgency, malaise, low-grade or intermittent fevers, anorexia with weight loss,mild anemia, and hypoalbuminemia. Only 10% of pa-tients present with severe colitis, characterized by five ormore bloody stools per day; more profound anemia andhypoalbuminemia; fever; tachycardia; and a diffusely ten-der or distended abdomen. (19)(20) Children who haveUC may develop symptoms of reflux or dyspepsia asso-ciated with inflammation of the upper gastrointestinaltract. (21)
The classic presentation of ab-dominal pain, diarrhea, and weightloss occurs in most children whohave CD. Abdominal pain typicallyis crampy and can be diffuse or lo-calized to the right lower quadrant.(22) Stools can appear nonbloodyor melanotic or can contain frankred blood. Chronic perianal disease,including tags, fissures, fistulae, andabscesses, may be present. (23) Re-current aphthous-stomatitis can alsosuggest the diagnosis. A decrease inheight velocity may precede overt ab-dominal symptoms by 5 years, andgrowth failure may be the only sign ofillness in 5% of children who receivethe diagnosis of CD. (24) Poor appe-tite, fevers, and iron deficiency ane-mia are also commonly noted at ini-
tial presentation in children who have CD. Decreased bonedensity is seen in 25% of newly diagnosed children, evenbefore initiation of corticosteroid therapy. (25)
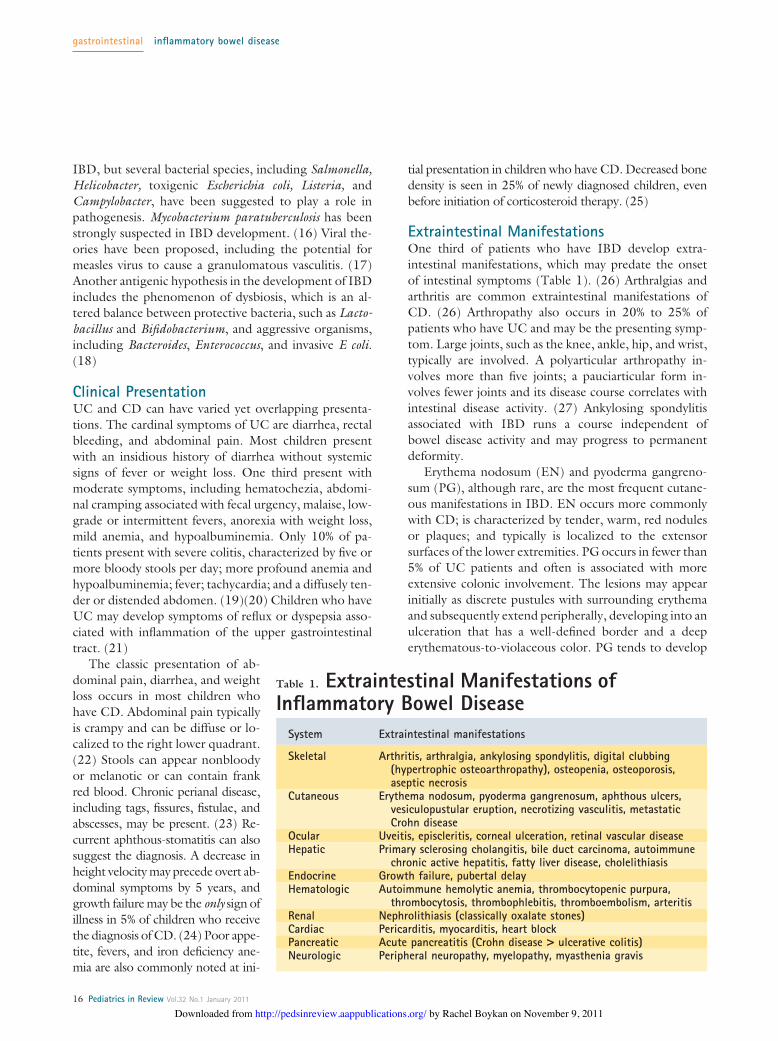
Extraintestinal ManifestationsOne third of patients who have IBD develop extra-intestinal manifestations, which may predate the onsetof intestinal symptoms (Table 1). (26) Arthralgias andarthritis are common extraintestinal manifestations ofCD. (26) Arthropathy also occurs in 20% to 25% ofpatients who have UC and may be the presenting symp-tom. Large joints, such as the knee, ankle, hip, and wrist,typically are involved. A polyarticular arthropathy in-volves more than five joints; a pauciarticular form in-volves fewer joints and its disease course correlates withintestinal disease activity. (27) Ankylosing spondylitisassociated with IBD runs a course independent ofbowel disease activity and may progress to permanentdeformity.
Erythema nodosum (EN) and pyoderma gangreno-sum (PG), although rare, are the most frequent cutane-ous manifestations in IBD. EN occurs more commonlywith CD; is characterized by tender, warm, red nodulesor plaques; and typically is localized to the extensorsurfaces of the lower extremities. PG occurs in fewer than5% of UC patients and often is associated with moreextensive colonic involvement. The lesions may appearinitially as discrete pustules with surrounding erythemaand subsequently extend peripherally, developing into anulceration that has a well-defined border and a deeperythematous-to-violaceous color. PG tends to develop
Table 1. Extraintestinal Manifestations ofInflammatory Bowel Disease
System Extraintestinal manifestations
Skeletal Arthritis, arthralgia, ankylosing spondylitis, digital clubbing(hypertrophic osteoarthropathy), osteopenia, osteoporosis,aseptic necrosis
Cutaneous Erythema nodosum, pyoderma gangrenosum, aphthous ulcers,vesiculopustular eruption, necrotizing vasculitis, metastaticCrohn disease
Ocular Uveitis, episcleritis, corneal ulceration, retinal vascular diseaseHepatic Primary sclerosing cholangitis, bile duct carcinoma, autoimmune
chronic active hepatitis, fatty liver disease, cholelithiasisEndocrine Growth failure, pubertal delayHematologic Autoimmune hemolytic anemia, thrombocytopenic purpura,
thrombocytosis, thrombophlebitis, thromboembolism, arteritisRenal Nephrolithiasis (classically oxalate stones)Cardiac Pericarditis, myocarditis, heart blockPancreatic Acute pancreatitis (Crohn disease > ulcerative colitis)Neurologic Peripheral neuropathy, myelopathy, myasthenia gravis
gastrointestinal inflammatory bowel disease
16 Pediatrics in Review Vol.32 No.1 January 2011
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

around sites of trauma and surgical scars. Although theemergence of EN usually follows intestinal disease activ-ity, PG runs an independent course, often necessitatingpotent therapy.
Transient transaminase elevation occurs in some chil-dren who have IBD and may be related to medicationsor disease activity. Persistent elevations suggest the pres-ence of primary sclerosing cholangitis (PSC) or auto-immune hepatitis. PSC is more commonly associatedwith UC and can predate the onset of intestinal symp-toms in 50% of patients. (28) Typical symptoms in-clude chronic fatigue, anorexia, pruritus, and jaundice,although children may be asymptomatic. Elevated gamma-glutamyltranspeptidase and alkaline phosphatase valuesalong with results of cholangiography and liver biopsyhelp confirm the diagnosis. (29)
Nutritional ConsiderationsGrowth failure occurs in 15% to 40% of children whohave IBD and is more frequent in CD than UC. TheZ-score (or standard deviation score) is used as an objec-tive measurement of growth. The mean height Z-scoreat diagnosis of pediatric CD is "0.54, and a delay indiagnosis or presence of jejunal disease is negativelycorrelated with the Z-score. (4) Poor weight gain alsomay precede a diagnosis of IBD. Mean weight Z-score atdiagnosis of pediatric CD is "1.06, with almost 30%of patients having weight Z-scores below the 3rd per-centile. In comparison, mean weight Z-score at diagnosisof UC is "0.32, with only 9% of patients falling belowthe 3rd percentile for age. (4)
The cause of growth failure in IBD is multifactorial.Patients often experience abdominal pain and diarrhearelated to eating, leading to food avoidance behaviorsand a decrease in total energy intake. Elevated concen-trations of proinflammatory cytokines contribute to an-orexia and can cause growth hormone resistance, withinhibition of insulin-like growth factor-1 (IGF-1) pro-duction. (30) In CD, active inflammation in the smallintestine can decrease the absorptive surface area, result-ing in a protein-losing enteropathy. Fat malabsorptioncontributes to the general energy-deficient state and maycause deficiencies in fat-soluble vitamins. Disease com-plications such as the presence of internal fistulae, surgi-cal bowel resections, or diverting ostomies can decreasenutrient absorption further.
Differential DiagnosisThe differential diagnosis for a child or adolescent pre-senting with abdominal pain and bloody diarrhea isbroad. Infectious enterocolitis, pseudomembranous
colitis, lymphocytic colitis, eosinophilic enterocolitis,Henoch-Schonlein purpura, and hemolytic-uremic syn-drome should be considered in addition to IBD. Intesti-nal malignancies such as non-Hodgkin lymphoma alsoshould be considered. The periodic fevers syndromes,including TRAPS (TNF receptor-associated periodicsyndrome) and PFAPA (periodic fever, aphthous stoma-titis, pharyngitis, and cervical adenitis), are rare but havesome clinical overlap with IBD. Rheumatologic disor-ders, such as juvenile idiopathic arthritis, ankylosingspondylitis, and systemic lupus erythematosus, sharemany characteristics with pediatric IBD, specifically,weight loss, malaise, recurrent fevers, and joint involve-ment. Finally, intestinal tuberculosis and CD have similarclinical, radiographic, and endoscopic features and canbe remarkably hard to differentiate. Intestinal tuberculo-sis typically involves the ileocolonic region, and the ul-cerative form is most common. A patient who has riskfactors for tuberculosis should have a tuberculin skin testplaced.
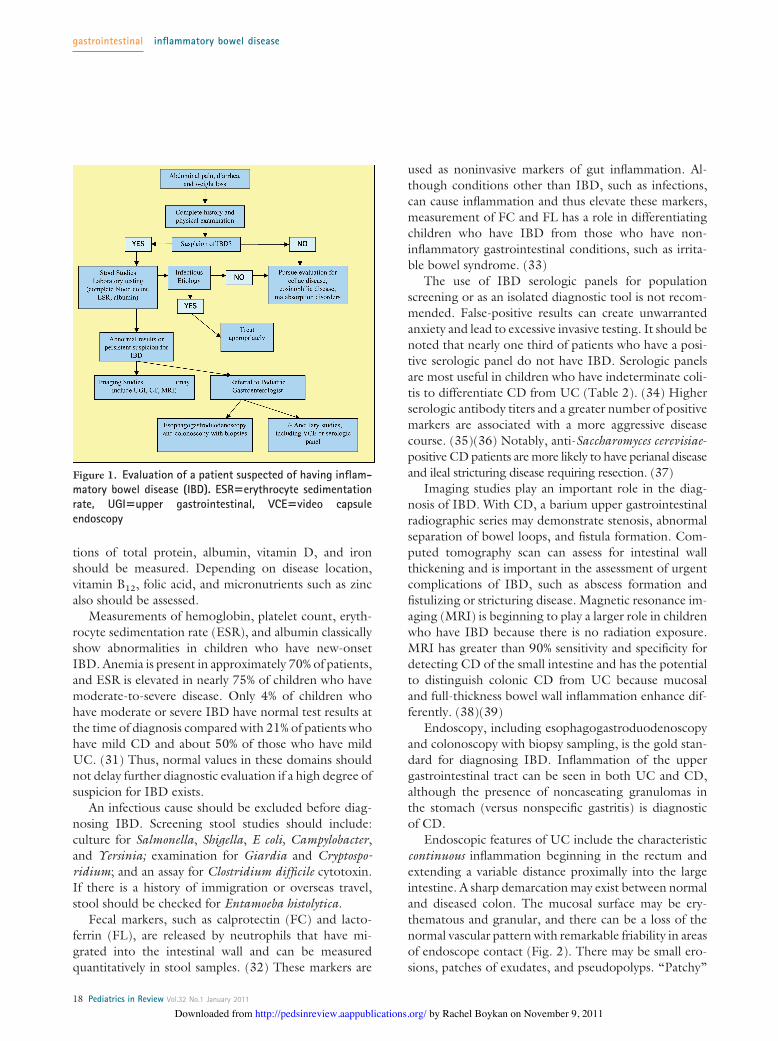
DiagnosisA new diagnosis of IBD often is suggested by the clinicalhistory and findings on physical examination (Fig. 1).The history should focus on the nature and duration ofsymptoms; location and quality of abdominal symptoms;frequency and consistency of bowel movements; pres-ence of blood in stools; urgency, tenesmus, and night-time awakening for bowel movements; and perianal,systemic (weight loss, fevers, fatigue), and extraintestinalsymptoms (aphthous ulcers, skin lesions, joint pains, eyesymptoms). A family history of IBD is of critical impor-tance.
The physical examination should include measure-ments of height and weight as well as Sexual MaturityRating staging. A complete evaluation includes examin-ing the mouth for aphthous lesions and performing athorough abdominal examination. Physical findings mayinclude abdominal tenderness, right lower quadrant massor fullness, pallor, and digital clubbing. A benign abdom-inal examination does not exclude the diagnosis of IBD.A rectal examination is mandatory, and the perianal areamust be checked for skin tags, fistulae, and fissures.
Nutritional assessment should include measurementsof growth velocity, height and weight Z-scores, and acomparison of absolute height with predicted mid-parental height. A bone age radiograph can be obtainedif there is concern for significant growth delay. A dietaryhistory should be obtained, with calculation of protein,carbohydrate, fat, vitamin, and mineral intake and com-parison to recommended daily values. Serum concentra-
gastrointestinal inflammatory bowel disease
Pediatrics in Review Vol.32 No.1 January 2011 17
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from
tions of total protein, albumin, vitamin D, and ironshould be measured. Depending on disease location,vitamin B12, folic acid, and micronutrients such as zincalso should be assessed.
Measurements of hemoglobin, platelet count, eryth-rocyte sedimentation rate (ESR), and albumin classicallyshow abnormalities in children who have new-onsetIBD. Anemia is present in approximately 70% of patients,and ESR is elevated in nearly 75% of children who havemoderate-to-severe disease. Only 4% of children whohave moderate or severe IBD have normal test results atthe time of diagnosis compared with 21% of patients whohave mild CD and about 50% of those who have mildUC. (31) Thus, normal values in these domains shouldnot delay further diagnostic evaluation if a high degree ofsuspicion for IBD exists.
An infectious cause should be excluded before diag-nosing IBD. Screening stool studies should include:culture for Salmonella, Shigella, E coli, Campylobacter,and Yersinia; examination for Giardia and Cryptospo-ridium; and an assay for Clostridium difficile cytotoxin.If there is a history of immigration or overseas travel,stool should be checked for Entamoeba histolytica.
Fecal markers, such as calprotectin (FC) and lacto-ferrin (FL), are released by neutrophils that have mi-grated into the intestinal wall and can be measuredquantitatively in stool samples. (32) These markers are
used as noninvasive markers of gut inflammation. Al-though conditions other than IBD, such as infections,can cause inflammation and thus elevate these markers,measurement of FC and FL has a role in differentiatingchildren who have IBD from those who have non-inflammatory gastrointestinal conditions, such as irrita-ble bowel syndrome. (33)
The use of IBD serologic panels for populationscreening or as an isolated diagnostic tool is not recom-mended. False-positive results can create unwarrantedanxiety and lead to excessive invasive testing. It should benoted that nearly one third of patients who have a posi-tive serologic panel do not have IBD. Serologic panelsare most useful in children who have indeterminate coli-tis to differentiate CD from UC (Table 2). (34) Higherserologic antibody titers and a greater number of positivemarkers are associated with a more aggressive diseasecourse. (35)(36) Notably, anti-Saccharomyces cerevisiae-positive CD patients are more likely to have perianal diseaseand ileal stricturing disease requiring resection. (37)
Imaging studies play an important role in the diag-nosis of IBD. With CD, a barium upper gastrointestinalradiographic series may demonstrate stenosis, abnormalseparation of bowel loops, and fistula formation. Com-puted tomography scan can assess for intestinal wallthickening and is important in the assessment of urgentcomplications of IBD, such as abscess formation andfistulizing or stricturing disease. Magnetic resonance im-aging (MRI) is beginning to play a larger role in childrenwho have IBD because there is no radiation exposure.MRI has greater than 90% sensitivity and specificity fordetecting CD of the small intestine and has the potentialto distinguish colonic CD from UC because mucosaland full-thickness bowel wall inflammation enhance dif-ferently. (38)(39)
Endoscopy, including esophagogastroduodenoscopyand colonoscopy with biopsy sampling, is the gold stan-dard for diagnosing IBD. Inflammation of the uppergastrointestinal tract can be seen in both UC and CD,although the presence of noncaseating granulomas inthe stomach (versus nonspecific gastritis) is diagnosticof CD.
Endoscopic features of UC include the characteristiccontinuous inflammation beginning in the rectum andextending a variable distance proximally into the largeintestine. A sharp demarcation may exist between normaland diseased colon. The mucosal surface may be ery-thematous and granular, and there can be a loss of thenormal vascular pattern with remarkable friability in areasof endoscope contact (Fig. 2). There may be small ero-sions, patches of exudates, and pseudopolyps. “Patchy”
Figure 1. Evaluation of a patient suspected of having inflam-matory bowel disease (IBD). ESR!erythrocyte sedimentationrate, UGI!upper gastrointestinal, VCE!video capsuleendoscopy
gastrointestinal inflammatory bowel disease
18 Pediatrics in Review Vol.32 No.1 January 2011
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from
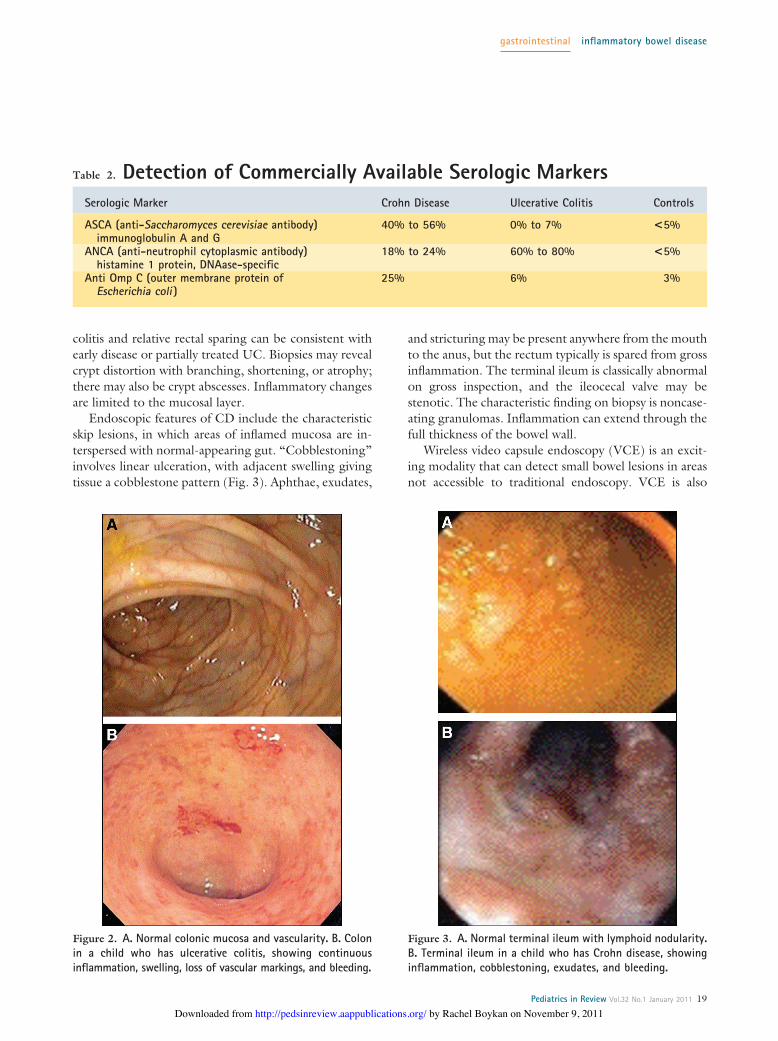
colitis and relative rectal sparing can be consistent withearly disease or partially treated UC. Biopsies may revealcrypt distortion with branching, shortening, or atrophy;there may also be crypt abscesses. Inflammatory changesare limited to the mucosal layer.
Endoscopic features of CD include the characteristicskip lesions, in which areas of inflamed mucosa are in-terspersed with normal-appearing gut. “Cobblestoning”involves linear ulceration, with adjacent swelling givingtissue a cobblestone pattern (Fig. 3). Aphthae, exudates,
and stricturing may be present anywhere from the mouthto the anus, but the rectum typically is spared from grossinflammation. The terminal ileum is classically abnormalon gross inspection, and the ileocecal valve may bestenotic. The characteristic finding on biopsy is noncase-ating granulomas. Inflammation can extend through thefull thickness of the bowel wall.
Wireless video capsule endoscopy (VCE) is an excit-ing modality that can detect small bowel lesions in areasnot accessible to traditional endoscopy. VCE is also
Table 2. Detection of Commercially Available Serologic MarkersSerologic Marker Crohn Disease Ulcerative Colitis Controls
ASCA (anti-Saccharomyces cerevisiae antibody)immunoglobulin A and G
40% to 56% 0% to 7% <5%
ANCA (anti-neutrophil cytoplasmic antibody)histamine 1 protein, DNAase-specific
18% to 24% 60% to 80% <5%
Anti Omp C (outer membrane protein ofEscherichia coli )
25% 6% 3%
Figure 2. A. Normal colonic mucosa and vascularity. B. Colonin a child who has ulcerative colitis, showing continuousinflammation, swelling, loss of vascular markings, and bleeding.
Figure 3. A. Normal terminal ileum with lymphoid nodularity.B. Terminal ileum in a child who has Crohn disease, showinginflammation, cobblestoning, exudates, and bleeding.
gastrointestinal inflammatory bowel disease
Pediatrics in Review Vol.32 No.1 January 2011 19
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from
helpful in identifying disease recurrence, evaluating anas-tomotic sites, and detecting luminal complications suchas malignancy. The drawbacks of VCE are difficulty withcapsule ingestion in young children and risk of capsuleretention.
TreatmentMedical Management
Immense progress has been made in the medical man-agement of pediatric IBD over the past decade. Theprimary goals of therapy are induction and maintenanceof remission, prevention of disease complications (suchas fistula, stricture, abscess, and cancer), control of post-operative disease recurrence, maintenance of normalgrowth and development, and maximization of qualityof life.
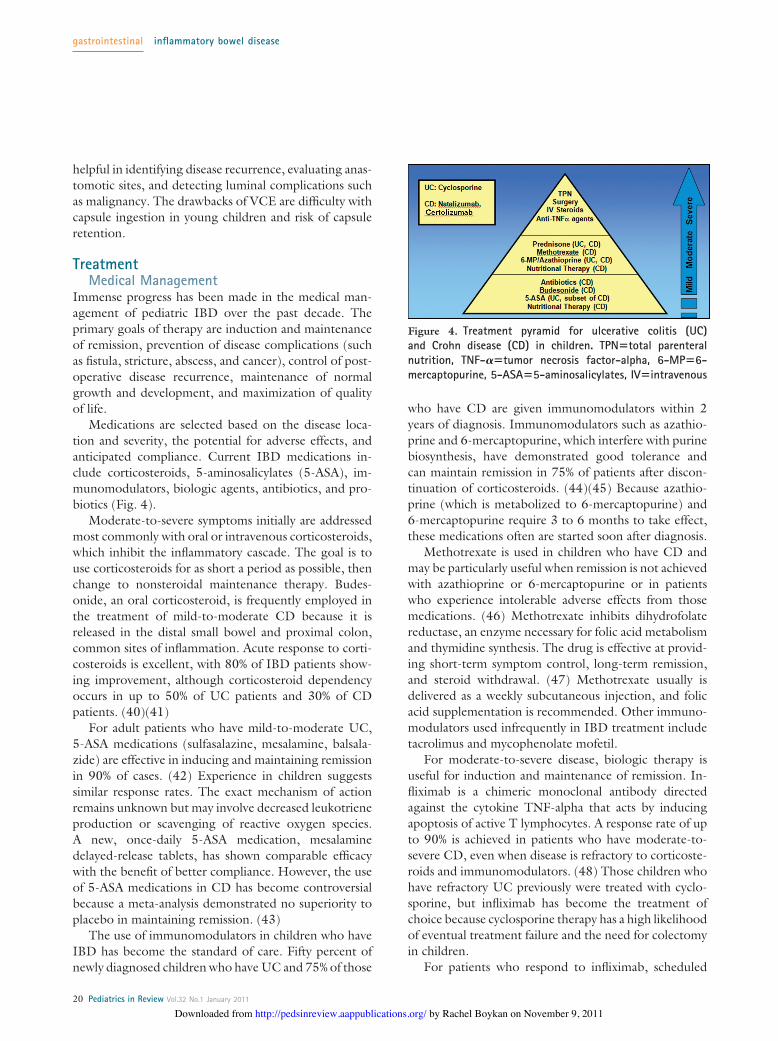
Medications are selected based on the disease loca-tion and severity, the potential for adverse effects, andanticipated compliance. Current IBD medications in-clude corticosteroids, 5-aminosalicylates (5-ASA), im-munomodulators, biologic agents, antibiotics, and pro-biotics (Fig. 4).
Moderate-to-severe symptoms initially are addressedmost commonly with oral or intravenous corticosteroids,which inhibit the inflammatory cascade. The goal is touse corticosteroids for as short a period as possible, thenchange to nonsteroidal maintenance therapy. Budes-onide, an oral corticosteroid, is frequently employed inthe treatment of mild-to-moderate CD because it isreleased in the distal small bowel and proximal colon,common sites of inflammation. Acute response to corti-costeroids is excellent, with 80% of IBD patients show-ing improvement, although corticosteroid dependencyoccurs in up to 50% of UC patients and 30% of CDpatients. (40)(41)
For adult patients who have mild-to-moderate UC,5-ASA medications (sulfasalazine, mesalamine, balsala-zide) are effective in inducing and maintaining remissionin 90% of cases. (42) Experience in children suggestssimilar response rates. The exact mechanism of actionremains unknown but may involve decreased leukotrieneproduction or scavenging of reactive oxygen species.A new, once-daily 5-ASA medication, mesalaminedelayed-release tablets, has shown comparable efficacywith the benefit of better compliance. However, the useof 5-ASA medications in CD has become controversialbecause a meta-analysis demonstrated no superiority toplacebo in maintaining remission. (43)
The use of immunomodulators in children who haveIBD has become the standard of care. Fifty percent ofnewly diagnosed children who have UC and 75% of those
who have CD are given immunomodulators within 2years of diagnosis. Immunomodulators such as azathio-prine and 6-mercaptopurine, which interfere with purinebiosynthesis, have demonstrated good tolerance andcan maintain remission in 75% of patients after discon-tinuation of corticosteroids. (44)(45) Because azathio-prine (which is metabolized to 6-mercaptopurine) and6-mercaptopurine require 3 to 6 months to take effect,these medications often are started soon after diagnosis.
Methotrexate is used in children who have CD andmay be particularly useful when remission is not achievedwith azathioprine or 6-mercaptopurine or in patientswho experience intolerable adverse effects from thosemedications. (46) Methotrexate inhibits dihydrofolatereductase, an enzyme necessary for folic acid metabolismand thymidine synthesis. The drug is effective at provid-ing short-term symptom control, long-term remission,and steroid withdrawal. (47) Methotrexate usually isdelivered as a weekly subcutaneous injection, and folicacid supplementation is recommended. Other immuno-modulators used infrequently in IBD treatment includetacrolimus and mycophenolate mofetil.
For moderate-to-severe disease, biologic therapy isuseful for induction and maintenance of remission. In-fliximab is a chimeric monoclonal antibody directedagainst the cytokine TNF-alpha that acts by inducingapoptosis of active T lymphocytes. A response rate of upto 90% is achieved in patients who have moderate-to-severe CD, even when disease is refractory to corticoste-roids and immunomodulators. (48) Those children whohave refractory UC previously were treated with cyclo-sporine, but infliximab has become the treatment ofchoice because cyclosporine therapy has a high likelihoodof eventual treatment failure and the need for colectomyin children.
For patients who respond to infliximab, scheduled
Figure 4. Treatment pyramid for ulcerative colitis (UC)and Crohn disease (CD) in children. TPN!total parenteralnutrition, TNF-"!tumor necrosis factor-alpha, 6-MP!6-mercaptopurine, 5-ASA!5-aminosalicylates, IV!intravenous
gastrointestinal inflammatory bowel disease
20 Pediatrics in Review Vol.32 No.1 January 2011
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

maintenance infusions are continued every 6 to 12 weeks.Gut mucosal healing has been demonstrated followinginfliximab therapy. Infliximab also plays an importantrole in treating fistulizing CD, which typically is moreresistant to conventional therapies, and extraintestinalmanifestations of IBD. PG, vasculitis, uveitis, EN, andarthritis have responded to this therapy.
Infliximab is the only immunomodulator approvedby the United States Food and Drug Administration forchildren who have CD. However, two other anti-TNFagents, adalimumab and certolizumab, appear effica-cious. Response rates are similar to infliximab, but be-cause these antibodies are more fully humanized, allergicreactions may be less common. Adalimumab has shownefficacy in children who are intolerant or become unre-sponsive to infliximab. (49)
Natalizumab (anti-alpha 4 integrin) inhibits the ad-hesion, migration, and activation of monocytes, macro-phages, and lymphocytes in a variety of tissues and hasdemonstrated clinical efficacy in treating children whohave CD. (50) Three cases of progressive multifocalleukoencephalopathy associated with the human JC viruswere described following trials in adults, which has cre-ated concern about its routine use.
Nutritional therapy may be a primary or adjunctivetreatment in CD. Exclusive enteral nutrition from ele-mental or polymeric formulas has been associated withshort-term remission in up to 80% of children, equal tothe response rate from corticosteroids. (51) The mecha-nism involves adequate suppression of bowel inflamma-tion and the induction of mucosalhealing. (51) Improved growth anddevelopment, without the adverseeffects of corticosteroids, makes en-teral nutrition an excellent choicefor first-line therapy in childrenwho have active CD. However,after induction, long-term medica-tions, such as immunomodulators,are necessary to maintain remis-sion. Supplements such as iron, fo-lic acid, calcium, and vitamin D arerequired in certain situations.
Antibiotics have specific indica-tions in IBD treatment. Metronida-zole is used to treat perirectal fistu-las, although recurrence rates arehigh and toxicity (eg, paresthesias)often limit long-term use. (52) Cip-rofloxacin is also useful in fistulatreatment. Both antibiotics are pre-
scribed for treatment of pouchitis following colectomyor ileoanal pouch procedures in UC patients. (53) Rifaxi-min, a nonabsorbed oral antibiotic, has shown benefit insymptom reduction of abdominal pain and diarrhea inchildren who have IBD. (54)
Probiotics have not been shown reproducibly to alterthe natural history of CD, but for children who havenewly diagnosed UC, probiotics are beneficial for main-taining remission when added to standard treatmentregimens. (55) Probiotics are also helpful in the preven-tion and treatment of pouchitis. (56)(57) Safety in IBDpatients is well established.
Significant adverse effects exist for all of the previouslydescribed medications (Table 3). A favorable risk-benefitratio is the goal when considering any therapy. Infliximabis contraindicated in patients who have active tuberculo-sis, opportunistic infection, history of demyelinating dis-ease, malignancy, congestive heart failure, or concurrentserious infection. Immunity to varicella should be as-certained before use of anti-TNF therapy. Recently, anaggressive malignancy, hepatosplenic T-cell lymphoma,has been described in young patients (mostly male) whowere treated with a combination of infliximab and eitherazathioprine or 6-mercaptopurine. (58)
Surgical ManagementDespite improvements in medical strategies, surgerymaintains an important therapeutic role. Indications forsurgery include uncontrolled gastrointestinal bleeding,bowel perforation, obstruction, intractable disease de-
Table 3. Adverse Effects of Medications CommonlyUsed to Treat Inflammatory Bowel Disease
Medication Class Important Adverse Effects
Corticosteroids Cushingoid facies, growth suppression, osteopenia,hypertension, hyperglycemia, acne, cataracts,hypothalamic-pituitary-adrenal axis suppression
5-Aminosalicylates Hypersensitivity reaction, disease exacerbation,headache, diarrhea, rash, pneumonitis, interstitialnephritis
6-Mercaptopurine,azathioprine
Bone marrow suppression, pancreatitis, hepatitis, rash,vasculitis; increased risk of lymphoma
Methotrexate Hepatitis, liver fibrosis, rash, folic acid deficiency,nausea, vomiting, hair loss
Anti-tumor necrosisfactor
Resurgence of tuberculosis, histoplasmosis, varicella,malignancies (including lymphoma), fatallymphoproliferative syndromes, anaphylaxis, serumsickness syndrome, lupuslike syndrome, increased riskof serious infections
Anti-integrin Progressive multifocal leukomalacia
gastrointestinal inflammatory bowel disease
Pediatrics in Review Vol.32 No.1 January 2011 21
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

spite standard therapy, and dysplasia. At times, surgicalresection is used to treat growth failure, especially if itallows the discontinuation of corticosteroids.
The surgical procedure of choice in UC is resection ofthe entire colon with ileal pouch-anal anastomosis. Thiscurative procedure can be performed either as a primaryoperation or in a staged approach, depending on thecondition of the patient. Long-term results are excellent,and continence can be achieved in 89% of patients after2 years with creation of a J-pouch reservoir. (59) Themajor complication occurring after ileoanal pull-throughis inflammation of the pouch (pouchitis), which occurs in10% to 40% of children. (60)(61)
In CD, segmental bowel resection is the most com-mon surgery and typically involves removing the diseasedterminal ileum and adjacent inflamed colon. Short seg-ments of bowel that are narrowed from fibrosis can betreated with stricturoplasty. Perirectal disease also maynecessitate surgery.
Adjunctive TherapiesOral nutrition supplements and either nasogastric orgastrostomy feedings may be critically important in ad-dressing chronic undernutrition in children who haveIBD. The administration of adequate calories with theaddition of these supplements can help to reverse growthfailure.
Complementary and alternative medicine approachesare used by up to 40% of patients who have IBD. Toprevent medication interactions and limit undue adverseeffects, these therapies are not routinely recommendedwithout physician consultation.
The need for family education and reassurance cannotbe overemphasized. Adolescents who have IBD mayhave a particularly difficult time because of issues relatedto growth failure, body image (eg, cushingoid featuresand acne from corticosteroids), and social invalidismfrom abdominal pain and diarrhea. Pubertal delay mayalso cause significant anxiety. Recent trials with growthhormone and IGF-1 have shown some promise in im-proving growth.
In general, patient and family counseling and peersupport groups are very helpful.
Prognosis and Disease ComplicationsDisease symptoms recur in up to one third of patients at1 year and more than one half at 2 years after initiationof therapy. Factors that predispose to a relapse of CDinclude the number of previous strictures and the pres-ence of FC or FL in the stool. (62)(63)(64) In UC, asignificant number of patients remain corticosteroid-
dependent after 1 year, and 5% may require colectomy.(40)
Toxic megacolon, although rare in children, occurs inapproximately 5% of adults who have severe UC and maybe triggered by hypokalemia or opiate use. Colonic per-foration may occur and colectomy may become neces-sary. (65) Patients who have severe colitis (more than fivebloody stools per day, fever, hypoalbuminemia, anemia)require hospitalization, bowel rest with parenteral nutri-tion support, intravenous corticosteroids, and very care-ful monitoring. Anecdotal experience supports the use ofinfliximab in reducing colectomy rates among patientswho have severe colitis.
The risk of colorectal cancer depends on the extentand duration of the disease. (66) The cumulative inci-dence of colorectal cancer in patients who have pancolitisis 5% to 10% after 20 years and 12% to 20% after 30 yearsof disease. Screening is recommended beginning 8 yearsafter diagnosis.
Patients who experience early-onset CD have a lowerfinal adult height compared with predicted mid-parentalheight, with an average height reduction of 2.4 cm.Population studies have not shown a difference in finaladult height in pediatric patients who have UC. (67)Osteopenia and osteoporosis can occur because of vita-min D deficiency, corticosteroid use, and high concen-trations of circulating inflammatory cytokines, whichinhibit IGF-1. Abnormally low bone mineral density isfound in nearly 50% of patients who have IBD. Maintain-ing disease remission, avoiding corticosteroids, exercis-ing, and ensuring adequate calcium and vitamin D in-take are imperative to optimize bone development andmineralization in the growing child, particularly duringpuberty. Dual-energy radiograph absorptiometry scansshould be performed in children who experience growthfailure and prolonged steroid use. (25)(68)(69)
Issues for the General PediatricianChildren and adolescents who have IBD should avoidthe use of nonsteroidal anti-inflammatory drugs (includ-ing ibuprofen) because their routine use can trigger adisease flare, enteropathy, or gastritis. Cautious use ofacetaminophen is suggested for treatment of minor painand fever. The casual use of antibiotics should be limitedin children who have IBD to prevent the risk of C difficilecolitis, which has been associated with increased morbid-ity. Children taking immunosuppressive medications andbiologic therapy should be restricted from live vaccineadministration. With administration of inactivated vac-cines, seroconversion is not always obtained if immuno-suppressive therapy is being used concomitantly. Mea-
gastrointestinal inflammatory bowel disease
22 Pediatrics in Review Vol.32 No.1 January 2011
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

surement of growth velocity, evaluation of pubertalSexual Maturity Rating staging, and annual-to-biannualeye examinations are recommended, even for asymptom-atic children who have IBD.
References1. Cuffari C. Inflammatory bowel disease in children: a pediatri-cian’s perspective. Minerva Pediatr. 2006;58:139–1572. Kugathasan S, Judd RH, Hoffmann RG, et al. Epidemiologicand clinical characteristics of children with newly diagnosed inflam-matory bowel disease in Wisconsin: a statewide population-basedstudy. J Pediatr. 2003;143:525–5313. Benchimol EI, Guttmann A, Griffiths AM, et al. Increasingincidence of paediatric inflammatory bowel disease in Ontario,Canada: evidence from health administrative data. Gut. 2009;58:1490–14974. Sawczenko A, Sandhu BK. Presenting features of inflammatorybowel disease in Great Britain and Ireland. Arch Dis Child. 2003;88:995–10005. Weinstein TA, Levine M, Pettei MJ, Gold DM, Kessler BH,Levine JJ. Age and family history at presentation of pediatricinflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2003;37:609–6136. Halfvarson J, Bodin L, Tysk C, Lindberg E, Jarnerot G. Inflam-matory bowel disease in a Swedish twin cohort: a long-termfollow-up of concordance and clinical characteristics. Gastroenter-ology. 2003;124:1767–17737. Cho JH. Inflammatory bowel disease: genetic and epidemio-logic considerations. World J Gastroenterol. 2008;14:338–3478. Lashner BA, Shaheen NJ, Hanauer SB, Kirschner BS. Passivesmoking is associated with an increased risk of developing inflam-matory bowel disease in children. Am J Gastroenterol. 1993;88:356–3599. Walters TD, Silverberg MS. Genetics of inflammatory boweldisease: current status and future directions. Can J Gastroenterol.2006;20:633–63910. Russell RK, Drummond HE, Nimmo ER, et al. Analysis of theinfluence of OCTN1/2 variants within the IBD5 locus on diseasesusceptibility and growth indices in early onset inflammatory boweldisease. Gut. 2006;55:1114–112311. Elson CO. Genes, microbes, and T cells–new therapeutictargets in Crohn’s disease. N Engl J Med. 2002;346:614–616
12. Bouma G, Strober W. The immunological and genetic basis ofinflammatory bowel disease. Nat Rev Immunol. 2003;3:521–53313. Saxon A, Shanahan F, Landers C, Ganz T, Targan S. A distinctsubset of antineutrophil cytoplasmic antibodies is associated withinflammatory bowel disease. J Allergy Clin Immunol. 1990;86:202–21014. Ehrhardt RO, Ludviksson BR, Gray B, Neurath M, Strober W.Induction and prevention of colonic inflammation in IL-2-deficientmice. J Immunol. 1997;158:566–57315. Fiocchi C. Inflammatory bowel disease: etiology and patho-genesis. Gastroenterology. 1998;115:182–20516. Sanderson JD, Moss MT, Tizard ML, Hermon-Taylor J. My-cobacterium paratuberculosis DNA in Crohn’s disease tissue. Gut.1992;33:890–89617. Wakefield AJ, Pittilo RM, Sim R, et al. Evidence of persistentmeasles virus infection in Crohn’s disease. J Med Virol. 1993;39:345–35318. Farrell RJ, LaMont JT. Microbial factors in inflammatorybowel disease. Gastroenterol Clin North Am. 2002;31:41–6219. Grand RJ, Homer DR. Approaches to inflammatory boweldisease in childhood and adolescence. Pediatr Clin North Am.1975;22:835–85020. Motil KJ, Grand RJ. Ulcerative colitis and Crohn disease inchildren. Pediatr Rev. 1987;9:109–12021. Werlin SL, Grand RJ. Severe colitis in children and adolescents:diagnosis, course, and treatment. Gastroenterology. 1977;73:828–83222. Griffiths AM. Specificities of inflammatory bowel disease inchildhood. Best Pract Res Clin Gastroenterol. 2004;18:509–52323. Palder SB, Shandling B, Bilik R, Griffiths AM, Sherman P.Perianal complications of pediatric Crohn’s disease. J Pediatr Surg.1991;26:513–51524. Kanof ME, Lake AM, Bayless TM. Decreased height velocity inchildren and adolescents before the diagnosis of Crohn’s disease.Gastroenterology. 1988;95:1523–152725. Hyams JS, Wyzga N, Kreutzer DL, Justinich CJ, GronowiczGA. Alterations in bone metabolism in children with inflammatorybowel disease: an in vitro study. J Pediatr Gastroenterol Nutr.1997;24:289–29526. Hyams JS. Extraintestinal manifestations of inflammatorybowel disease in children. J Pediatr Gastroenterol Nutr. 1994;19:7–2127. Passo MH, Fitzgerald JF, Brandt KD. Arthritis associated withinflammatory bowel disease in children. Relationship of joint dis-ease to activity and severity of bowel lesion. Dig Dis Sci. 1986;31:492–49728. Hyams JMJ, Treem W. Characterization of hepatic abnormal-ities in children with inflammatory bowel disease. Inflamm BowelDis. 1995;1:2729. Roberts EA. Primary sclerosing cholangitis in children. J Gas-troenterol Hepatol. 1999;14:588–59330. Kirschner BS, Sutton MM. Somatomedin-C levels in growth-impaired children and adolescents with chronic inflammatory boweldisease. Gastroenterology. 1986;91:830–83631. Mack DR, Langton C, Markowitz J, et al. Laboratory valuesfor children with newly diagnosed inflammatory bowel disease.Pediatrics. 2007;119:1113–111932. Fagerberg UL, Loof L, Lindholm J, Hansson LO, Finkel Y.Fecal calprotectin: a quantitative marker of colonic inflammation inchildren with inflammatory bowel disease. J Pediatr GastroenterolNutr. 2007;45:414–420
Summary• Recent major advances have been made in the
diagnosis and treatment of pediatric IBD, andunderstanding of its pathophysiology continues toevolve.
• The long-term outcome for children who have IBDcontinues to improve with better appreciation ofgenotype-phenotype correlations, earlier diagnosis,and more effective treatments.
• Although the incidence of pediatric IBD appears tobe rising, the future for affected children andadolescents appears promising.
gastrointestinal inflammatory bowel disease
Pediatrics in Review Vol.32 No.1 January 2011 23
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

33. Joishy M, Davies I, Ahmed M, et al. Fecal calprotectin andlactoferrin as noninvasive markers of pediatric inflammatory boweldisease. J Pediatr Gastroenterol Nutr. 2009;48:48–5434. Sabery N, Bass D. Use of serologic markers as a screening toolin inflammatory bowel disease compared with elevated erythrocytesedimentation rate and anemia. Pediatrics. 2007;119:e193–e19935. Dubinsky MC, Johanson JF, Seidman EG, Ofman JJ. Sus-pected inflammatory bowel disease–the clinical and economic im-pact of competing diagnostic strategies. Am J Gastroenterol. 2002;97:2333–234236. Dubinsky MC, Ofman JJ, Urman M, Targan SR, Seidman EG.Clinical utility of serodiagnostic testing in suspected pediatric in-flammatory bowel disease. Am J Gastroenterol. 2001;96:758–76537. Zholudev A, Zurakowski D, Young W, Leichtner A, BousvarosA. Serologic testing with ANCA, ASCA, and anti-OmpC in chil-dren and young adults with Crohn’s disease and ulcerative colitis:diagnostic value and correlation with disease phenotype. Am JGastroenterol. 2004;99:2235–224138. Darbari A, Sena L, Argani P, Oliva-Hemker JM, Thompson R,Cuffari C. Gadolinium-enhanced magnetic resonance imaging: auseful radiological tool in diagnosing pediatric IBD. Inflamm BowelDis. 2004;10:67–7239. Paolantonio P, Ferrari R, Vecchietti F, Cucchiara S, Laghi A.Current status of MR imaging in the evaluation of IBD in apediatric population of patients. Eur J Radiol. 2009;69:418–42440. Hyams J, Markowitz J, Lerer T, et al. The natural history ofcorticosteroid therapy for ulcerative colitis in children. Clin Gastro-enterol Hepatol. 2006;4:1118–112341. Markowitz J, Hyams J, Mack D, et al. Corticosteroid therapyin the age of infliximab: acute and 1-year outcomes in newlydiagnosed children with Crohn’s disease. Clin Gastroenterol Hepa-tol. 2006;4:1124–112942. Hanauer SB. Review article: the long-term management ofulcerative colitis. Aliment Pharmacol Ther. 2004;20(suppl 4):97–10143. Camma C, Giunta M, Rosselli M, Cottone M. Mesalamine inthe maintenance treatment of Crohn’s disease: a meta-analysisadjusted for confounding variables. Gastroenterology. 1997;113:1465–147344. Verhave M, Winter HS, Grand RJ. Azathioprine in the treat-ment of children with inflammatory bowel disease. J Pediatr. 1990;117:809–81445. Ramakrishna J, Langhans N, Calenda K, Grand RJ, VerhaveM. Combined use of cyclosporine and azathioprine or6-mercaptopurine in pediatric inflammatory bowel disease. J Pedi-atr Gastroenterol Nutr. 1996;22:296–30246. Weiss B, Lerner A, Shapiro R, et al. Methotrexate treatment inpediatric Crohn disease patients intolerant or resistant to purineanalogues. J Pediatr Gastroenterol Nutr. 2009;48:526–53047. Uhlen S, Belbouab R, Narebski K, et al. Efficacy of methotrex-ate in pediatric Crohn’s disease: a French multicenter study. In-flamm Bowel Dis. 2006;12:1053–105748. Hyams J, Crandall W, Kugathasan S, et al. Induction andmaintenance infliximab therapy for the treatment of moderate-to-severe Crohn’s disease in children. Gastroenterology. 2007;132:863–87349. Rosh JR, Lerer T, Markowitz J, et al. Retrospective evaluationof the safety and effect of adalimumab therapy (RESEAT) in pedi-atric Crohn’s disease. Am J Gastroenterol. 2009;104:3042–304950. Hyams JS, Wilson DC, Thomas A, et al. Natalizumab therapy
for moderate to severe Crohn disease in adolescents. J PediatrGastroenterol Nutr. 2007;44:185–19151. Griffiths AM, Ohlsson A, Sherman PM, Sutherland LR. Meta-analysis of enteral nutrition as a primary treatment of active Crohn’sdisease. Gastroenterology. 1995;108:1056–106752. Brandt LJ, Bernstein LH, Boley SJ, Frank MS. Metronidazoletherapy for perineal Crohn’s disease: a follow-up study. Gastroen-terology. 1982;83:383–38753. Sandborn WJ, Pardi DS. Clinical management of pouchitis.Gastroenterology. 2004;127:1809–181454. Muniyappa P, Gulati R, Mohr F, Hupertz V. Use and safety ofrifaximin in children with inflammatory bowel disease. J PediatrGastroenterol Nutr. 2009;49:400–40455. Miele E, Pascarella F, Giannetti E, Quaglietta L, BaldassanoRN, Staiano A. Effect of a probiotic preparation (VSL#3) oninduction and maintenance of remission in children with ulcerativecolitis. Am J Gastroenterol. 2009;104:437–44356. Gionchetti P, Amadini C, Rizzello F, Venturi A, Poggioli G,Campieri M. Diagnosis and treatment of pouchitis. Best Pract ResClin Gastroenterol. 2003;17:75–8757. Gionchetti P, Morselli C, Rizzello F, et al. Management ofpouch dysfunction or pouchitis with an ileoanal pouch. Best PractRes Clin Gastroenterol. 2004;18:993–100658. Thayu M, Markowitz JE, Mamula P, Russo PA, Muinos WI,Baldassano RN. Hepatosplenic T-cell lymphoma in an adolescentpatient after immunomodulator and biologic therapy for Crohndisease. J Pediatr Gastroenterol Nutr. 2005;40:220–22259. Koivusalo A, Pakarinen MP, Rintala RJ. Surgical complicationsin relation to functional outcomes after ileoanal anastomosis inpediatric patients with ulcerative colitis. J Pediatr Surg. 2007;42:290–29560. Stavlo PL, Libsch KD, Rodeberg DA, Moir CR. Pediatric ilealpouch-anal anastomosis: functional outcomes and quality of life.J Pediatr Surg. 2003;38:935–93961. Tilney HS, Constantinides V, Ioannides AS, Tekkis PP, DarziAW, Haddad MJ. Pouch-anal anastomosis vs straight ileoanal anas-tomosis in pediatric patients: a meta-analysis. J Pediatr Surg. 2006;41:1799–180862. Greenstein AJ, Zhang LP, Miller AT, et al. Relationship of thenumber of Crohn’s strictures and strictureplasties to postoperativerecurrence. J Am Coll Surg. 2009;208:1065–107063. McLeod RS, Wolff BG, Steinhart AH, et al. Risk and signifi-cance of endoscopic/radiological evidence of recurrent Crohn’sdisease. Gastroenterology. 1997;113:1823–182764. Lamb CA, Mohiuddin MK, Gicquel J, et al. Faecal calprotectinor lactoferrin can identify postoperative recurrence in Crohn’sdisease. Br J Surg. 2009;96:663–67465. Sheth SG, LaMont JT. Toxic megacolon. Lancet. 1998;351:509–51366. Brostrom O, Lofberg R, Nordenvall B, Ost A, Hellers G. Therisk of colorectal cancer in ulcerative colitis. An epidemiologicstudy. Scand J Gastroenterol. 1987;22:1193–119967. Sawczenko A, Ballinger AB, Savage MO, Sanderson IR. Clin-ical features affecting final adult height in patients with pediatric-onset Crohn’s disease. Pediatrics. 2006;118:124–12968. Harpavat M, Keljo DJ. Perspectives on osteoporosis in pediat-ric inflammatory bowel disease. Curr Gastroenterol Rep. 2003;5:225–23269. Sylvester FA. IBD and skeletal health: children are not smalladults! Inflamm Bowel Dis. 2005;11:1020–1023
gastrointestinal inflammatory bowel disease
24 Pediatrics in Review Vol.32 No.1 January 2011
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from
PIR QuizQuiz also available online at http://pedsinreview.aappublications.org.
6. Which of the following symptoms or signs is seen in children who have Crohn disease, but not in childrenwho have ulcerative colitis?
A. Anemia.B. Arthritis.C. Loose stools.D. Perianal fistula.E. Weight loss.
7. Which of the following infections can mimic the intestinal inflammation of Crohn disease?
A. Epstein-Barr virus.B. Herpes simplex virus-1.C. Measles virus.D. Rotavirus.E. Tuberculosis.
8. Which of the following tests is the “gold standard” for diagnosis of IBD?
A. Abdominal computed tomography scan.B. Endoscopy and colonoscopy with biopsy.C. Fecal lactoferrin.D. Serologic panel.E. Wireless capsule endoscopy.
9. A 15-year-old boy received the diagnosis of Crohn disease of the colon 6 months ago. He has had activedisease despite 5 months of 6-mercaptopurine therapy and two courses of corticosteroid therapy. Of thefollowing, which medication is most likely to induce remission?
A. Azathioprine.B. Infliximab.C. Mesalamine.D. Metronidazole.E. Rifaximin.
10. An adolescent girl who has ulcerative colitis has been successfully maintained on 6-mercaptopurine for2 years and presents today for a health supervision visit. She asks which immunizations she can have inthe future. Which of the following vaccines is contraindicated?
A. Human papillomavirus vaccine.B. Influenza vaccine.C. Measles, mumps, and rubella vaccine.D. Pneumococcal vaccine.E. Tetanus toxoid.
gastrointestinal inflammatory bowel disease
Pediatrics in Review Vol.32 No.1 January 2011 25
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.32-1-142011;32;14Pediatrics in Review
Sarah R. Glick and Ryan S. CarvalhoInflammatory Bowel Disease
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/32/1/14including high resolution figures, can be found at:
References
http://pedsinreview.aappublications.org/content/32/1/14#BIBLat: This article cites 69 articles, 9 of which you can access for free
Subspecialty Collections
stinal_disordershttp://pedsinreview.aappublications.org/cgi/collection/gastrointeGastrointestinal Disorders_disordershttp://pedsinreview.aappublications.org/cgi/collection/nutritionalNutrition and Nutritional Disordersfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from