Infiltrating fibromatosis the breastInfiltrating fibromatosis ofthe breast WLADIMIRV BOGOMOLETZ,...
5
J Clin Pathol 1981 ;34:30-34 Infiltrating fibromatosis of the breast WLADIMIR V BOGOMOLETZ, EDOUARD BOULENGER, AND ARLETTE SIMATOS From the Departments ofPathology, Cytology, and Surgery, Institut Jean Godinot, Reims, France SUMMARY A case of fibromatosis of the breast in a 65-year-old woman is described. The difficulties in the histological and cytological differential diagnosis of fibromatosis in such an uncommon site are emphasised. Among the benign mesenchymal lesions of the breast masquerading as clinical carcinoma, fibro- blastic and fibrous proliferations such as fibromatosis are fairly rare. Their inflammatory, reactive, or truly neoplastic nature is often difficult to determine histologically, and the cytological features of fine- needle aspiration from these lesions may also be misleading. We report the case of a 65-year-old woman with an unusual fibroblastic proliferative lesion of the right breast of three years' duration and with the features of an infiltrative fibromatosis. We empha- sise the problems of differential diagnosis, histo- genesis, and cytological aspects of fibromatosis of the breast. Case report A 65-year-old postmenopausal woman, para 8, was admitted to our institution in July 1979 for investigation of a mass in the right breast. The patient stated that she had first noticed this mass about three years previously after a minor trauma to the right breast when she was hit on the chest by the fall of concrete material from a ceiling. At the time of injury the patient had not noticed skin bruising of the right breast. Before the present hospital ad- mission the mass had been increasing in size and had become somewhat tender with a slight 'milky' dis- charge from the right nipple. On physical examination both breasts were pendulous, and a firm and movable 4 x 4 cm painless mass was palpable in the lower inner quadrant of the right breast. Although the area of the skin overlying this mass was slightly depressed, there was no skin fixation or nipple retraction. The left contralateral breast appeared normal. Axillary lymph nodes were not felt. The liver was not enlarged. There was no history of previous surgery. Accepted for publication 7 May 1980 30 Mammography confirmed the presence in the right breast of a suspicious opacity (Fig. 1). Other routine radiological and laboratory investigations showed no significant abnormality. Fig. 1 Mammography ofright breast showing an opacity with an 'infiltrating' border. Percutaneous fine-needle aspiration of the mass was performed and yielded scanty cellular material. Cyto- logical examination revealed a few enlarged fibro- blasts without atypia, scattered in an haemorrhagic background. Four clusters of epithelial cells were also identified, two of which consisted of fairly normal cuboidal or columnar cells of probable duct origin. In the other two aggregates, the cells were haphazardly arranged, overlapped, and showed anisocytosis, anisonucleosis, and hyperchromasia (Fig. 2). On account of these markedly atypical cells and notwithstanding the scantiness ot the cellular material available, a positive report of malignancy on February 28, 2020 by guest. Protected by copyright. http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.34.1.30 on 1 January 1981. Downloaded from
Transcript of Infiltrating fibromatosis the breastInfiltrating fibromatosis ofthe breast WLADIMIRV BOGOMOLETZ,...

JClin Pathol 1981 ;34:30-34
Infiltrating fibromatosis of the breastWLADIMIR V BOGOMOLETZ, EDOUARD BOULENGER, AND ARLETTE SIMATOS
From the Departments ofPathology, Cytology, and Surgery, InstitutJean Godinot, Reims, France
SUMMARY A case of fibromatosis of the breast in a 65-year-old woman is described. The difficultiesin the histological and cytological differential diagnosis of fibromatosis in such an uncommon siteare emphasised.
Among the benign mesenchymal lesions of thebreast masquerading as clinical carcinoma, fibro-blastic and fibrous proliferations such as fibromatosisare fairly rare. Their inflammatory, reactive, or trulyneoplastic nature is often difficult to determinehistologically, and the cytological features of fine-needle aspiration from these lesions may also bemisleading.We report the case of a 65-year-old woman with
an unusual fibroblastic proliferative lesion of theright breast of three years' duration and with thefeatures of an infiltrative fibromatosis. We empha-sise the problems of differential diagnosis, histo-genesis, and cytological aspects of fibromatosis ofthe breast.
Case report
A 65-year-old postmenopausal woman, para 8,was admitted to our institution in July 1979 forinvestigation of a mass in the right breast. Thepatient stated that she had first noticed this massabout three years previously after a minor trauma tothe right breast when she was hit on the chest by thefall of concrete material from a ceiling. At the time ofinjury the patient had not noticed skin bruising ofthe right breast. Before the present hospital ad-mission the mass had been increasing in size and hadbecome somewhat tender with a slight 'milky' dis-charge from the right nipple.On physical examination both breasts were
pendulous, and a firm and movable 4 x 4 cm painlessmass was palpable in the lower inner quadrant of theright breast. Although the area of the skin overlyingthis mass was slightly depressed, there was no skinfixation or nipple retraction. The left contralateralbreast appeared normal. Axillary lymph nodes werenot felt. The liver was not enlarged. There was nohistory of previous surgery.
Accepted for publication 7 May 198030
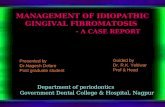
Mammography confirmed the presence in the rightbreast of a suspicious opacity (Fig. 1). Other routineradiological and laboratory investigations showedno significant abnormality.
Fig. 1 Mammography ofright breast showing an opacitywith an 'infiltrating' border.
Percutaneous fine-needle aspiration of the mass wasperformed and yielded scanty cellular material. Cyto-logical examination revealed a few enlarged fibro-blasts without atypia, scattered in an haemorrhagicbackground. Four clusters of epithelial cells werealso identified, two of which consisted of fairlynormal cuboidal or columnar cells of probable ductorigin. In the other two aggregates, the cells werehaphazardly arranged, overlapped, and showedanisocytosis, anisonucleosis, and hyperchromasia(Fig. 2). On account of these markedly atypical cellsand notwithstanding the scantiness ot the cellularmaterial available, a positive report of malignancy
on February 28, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.1.30 on 1 January 1981. Dow
nloaded from

31Infiltratingfibromatosis ofthe breast
(b)
Fig. 2 (acI(I( /)l) C} tolo()gaicl si i .I ectfsp epai-ed/oo /ie-ncedlcaspiration oa/reast. Two different aggregates of markedlyacty-pical ce/slls interpretedas.'ali nant'. (Papanicolaou A 700).
(a)
was issued.
In view of the cytological report, the abnormalmammographic image, and the overall clinicalimpression, a right mastectomy with clearance ofaxillary nodes was performed, but no excisionalbiopsy specimen was submitted for frozen section.
Pathology
The surgical specimen was a right breast withattached axillary fat contents. The lower innerquadrant contained a firm, irregular, and infiltratingmass (3 x 2 cm) situated close to the deepest marginof excision. The remainder of the breast tissue was
markedly fatty. A total of 16 lymph nodes were
dissected from the axillary contents.Histologically this lesion consisted of interlacing
bundles of proliferating fibroblasts with some
attempt at forming a 'storiform' pattern (Fig. 3a).The lesion had a definite infiltrating border, fibro-blasts spreading into the surrounding fat (Fig. 3b).The degree of cellularity was variable. The fibro-blasts were well-differentiated and uniform in size,although some were enlarged but not displayingnuclear atypia (Fig. 4). Mitoses were few in themultiple sections examined. Scattered lymphocytic
aggregates, some congested capillaries, and patchyfat necrosis were also present around the peripheryof the lesion; multinucleated histiocytic giant cellswere not noted. Ductal and lobular structures ap-peared entrapped within the fibroblastic prolifera-tion with resulting features of pressure atrophy,which included bizarre nuclei in the epithelial cells(Fig. 5). A few of the ducts situated at the peripheryshowed some degree of epithelial hyperplasia butthere was no evidence of intraduct or invasivecarcinoma. The central portions contained muchhyalinised collagen with interspersed obliteratedducts showing marked periductal elastosis; foci ofnecrobiosis and calcification were also noted.Surgical excision of the lesion appeared complete,and the 16 lymph nodes examined were free ofmetastatic deposit.Based on the histological findings, a diagnosis of
fibroblastic proliferation consistent with. infiltrativefibromatosis was made.
Discussion
Our case of fibromatosis of the breast raises severalproblems, particularly from the point of view ofdifferential diagnosis and histogenesis.
on February 28, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.1.30 on 1 January 1981. Dow
nloaded from

Ilogomoletz, Boulenger, and Simatos
x44
4%*
nw'
i/44
A'....
",.'."%
i 1,
i.....W.
opV
-sw
I
eosin x
;:;:..:-X.I.... .!....W
W.,Fig. 4 Fibromatosis ofbreast.
Representative high-power field showing
proliferating and well-differentiated
fibroblasts. Note one mitosis in the centre.
HandEx 400.
Fibromatosis may be defined as an infiltrating showing no cytological features of unequivocal
fibroblastic proliferation, which is locally aggressive neoplasia.' 2 Some authors have added that there
but non-metastasising, the fibroblasts concerned should be no features of inflammatory response.3"
32
6-A
v.4,
on February 28, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.1.30 on 1 January 1981. Dow
nloaded from

Infiltratingfibromatosis ofthe breast 33
(a) (b)Fig. 5 Fibromatosis ofbreast. (a and b) Two aspects of 'entrapped' small ducts with lining epithelium showingatypical hyperplasia. Note hyperchromatic and irregular nuclei. H andE x 400.
This complementary criterion may be questionableon the grounds that a fibromatosis could elicit aninflammatory response from the infiltrated breasttissue if the latter is particularly prone to react tolocal aggression, for example, fat. It should also benoted that nodular fasciitis, which is characterised byboth fibroblastic proliferation and inflammatoryresponse, has been classified with the fibromatoses.2
Fibromatosis must be distinguished from simplehyperplasia of reparative connective tissue whichstops spontaneously. However, scar tissue of varyingaetiology may continue to proliferate and induce afibroblastic infiltrating pseudotumour. Thus theborderline between a post-inflammatory reparativeprocess and a true fibromatosis becomes blurred,one merging with the other. In this situation, histo-logical features of inflammation, such as inflam-matory cells, prominent capillaries, and even fatnecrosis, may still be present.
Fibromatosis must be further differentiated fromfibrosarcoma, although this was not a problem inour case.
In a gland such as the breast, which containsadipose tissue, the difficulty is to distinguish fatnecrosis with persisting fibroblastic activity fromtrue fibromatosis. Ordinary fat necrosis of the breasttends to undergo peripheral fibrosis, and eventuallythe entire area is replaced by dense fibrous tissuealthough cystic cavities may still be identified.5 It isunusual for simple fat necrosis of the breast to showpersistent fibroblastic activity over many monthsleading to gross enlargement of the lesion.
Recently, Rosen et al.6 reported one case offibromatosis of the breast and were able to compile15 cases of this type from the literature. In terms ofdifferential diagnosis, these authors mentioned only
the distinction of fibromatosis from fibrosarcoma.Two further cases of fibromatosis of the breast havebeen reported by Ali et al.7Our case also exemplifies the difficulty of the
cytological interpretation of fine-needle aspirationfrom fibromatosis of the breast. As a result of fibro-blastic proliferation, mammary ducts becomeconstricted with pressure phenomena on their epi-thelial lining. In addition to fibroblasts, the aspiratemay contain some of these modified epithelial cellswhich show anisocytosis with nuclear pleomorphismand hyperchromasia. The overall cytological patternmimics carcinoma. In this situation, the scantinessof these atypical cells and the presence of well-differentiated fibroblasts are cautionary signposts.As with other fibromatoses, local recurrences can
be expected when fibromatosis of the breast isincompletely excised, as shown by Zayid andDihmis.8 Wide local excision should therefore be thepreferred treatment for fibromatosis of the breast;mastectomy does not appear to be justified in viewof the non-metastasising nature of the lesion. How-ever, even when a biopsy specimen is submitted forfrozen section and fibromatosis is correctly diag-nosed, the surgeon may be faced with technicaldifficulties, such as involvement of the pectoralismajor muscle,9 10 and mastectomy may then haveto be considered.
We thank Mrs A Christoph for technical assistanceand Miss MJ Bianchi for secretarial help.
References
1 Enzinger FM, Lattes R, Torloni H. Soft Tissue Tumours.WHO International Histological Classification ofTumours No. 3. Geneva: WHO, 1976,
on February 28, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.1.30 on 1 January 1981. Dow
nloaded from

34 Bogomoletz, Boulenger, and Simatos
2 Stout AP, Lattes R. Tuimors of the Sofi Tissises. ArmedForces Institute of Pathology. Atlas of Tumor Patho-logy 2nd Ser. Fasc. 1. Washington: AFI P, 1967.
Ashley DJB. Evans' Histological Appearances of Tiuiuouirs.3rd ed. Edinburgh: Churchill Livingstone, 1978.
Mackenzie DH. The fibromatoses: a clinicopathologicalconcept. Br MedJ 1972;4:277-8 1.
Haagensen CD. Diseases of the Breast. 2nd ed. Philadel-phia: Saunders, 1971: 202-11.
6 Rosen Y, Papasozomenos SC, Gardner B. Fibromatosis ofthe breast. Cancer 1978 ;41:1409-13.
' Ali M, Fayemi AO, Braun EV, Remy R. Fibromatosis ofthe breast. A mazer J Suirg Pathol 1979;3:501-6.
Zayid 1, Dihmis C. Familial multicentric fibroniatosis-desmoids. Cancer 1969;24:786-95.
Haggit RC, Booth JL. Bilateral fibromatosis of the breastin Gardner's syndrome. Cancer 1970;25:161-6.
Kalisher L, Long JA, Peyster RG. Extra-abdominal des-moid of the axillary tail mimicking breast carcinoma.Am J Roentgenol 1976; 126:903-6.
Requests for reprints to: Dr WV Bogomoletz, Depart-ment of Pathology, Institut Jean Godinot, BP 171,51056 Reims Cedex, France.
on February 28, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.34.1.30 on 1 January 1981. Dow
nloaded from