
INFECTIOUS DISEASES IN CHILDREN - fcm.ucsf.edu Infectious Diseases in Children.pdf · Major...
70
INFECTIOUS DISEASES IN CHILDREN Andi Marmor, MD, MSED Professor of Pediatrics University of California, San Francisco Zuckerberg San Francisco General Hospital Acknowledgement: Hayes Bakken, MD
Transcript of INFECTIOUS DISEASES IN CHILDREN - fcm.ucsf.edu Infectious Diseases in Children.pdf · Major...

INFECTIOUS DISEASESIN CHILDREN
Andi Marmor, MD, MSEDProfessor of PediatricsUniversity of California, San FranciscoZuckerberg San Francisco General Hospital
Acknowledgement: Hayes Bakken, MD

Updates and Current Recommendations
Fever without a source (SBI) Urinary Tract Infections Acute Otitis Media
Influenza
Pertussis Community Acquired PNA
Bronchiolitis
FEVER COUGH
TB Vaccinations
RASHESSCREENING/PREVENTION
Case Presentation: Infant with Fever
Quokka is 2 week old girl with a feverNo symptoms to suggest a source on
exam/historyVS: T 38.5, P 150, R 40’s, o/w WNLExam: well-appearing, no focal findings
to suggest source for fever
The most likely cause of Quokka’s fever is:
A. Viral infectionB. Urinary tract infectionC. Serious bacterial infection
(bacteremia/meningitis)D. HSV infection
THE FEBRILE INFANT

Everything you need to know about SBI in febrile infants - on ONE SLIDE
Schwartz, 2009, Gomez 2010, Greenhow, 2014
2-3%
E.Coli>GBS>S. aureus>enterococcus, S pneumo13-18%
<1%
Greenhow, 2014
E. Coli
E.Coli/GBSS. pneumo

Fever without a source (FWS): Infants <30 days
Appearance and lab criteria do not reliably rule out UTI/SBI in this age group
Urine, blood, CSF, empiric abxrecommended Amp/gentamicin or amp/cefotaximeListeria vanishingly rare…some recommend
treating with cefotaxime aloneDO NOT treat with gentamicin alone

FWS: Infants 30-90 days
UTI still the most common bacterial source, other SBI less likely
Viral source more reliable Named viral syndromes or + rapid viral test
(flu, RSV) SBI unlikelyConsider testing for UTI
Inflammatory markers (CBC/CRP/PCT) helpful in select infantsWell appearing, neg UA AND no viral source
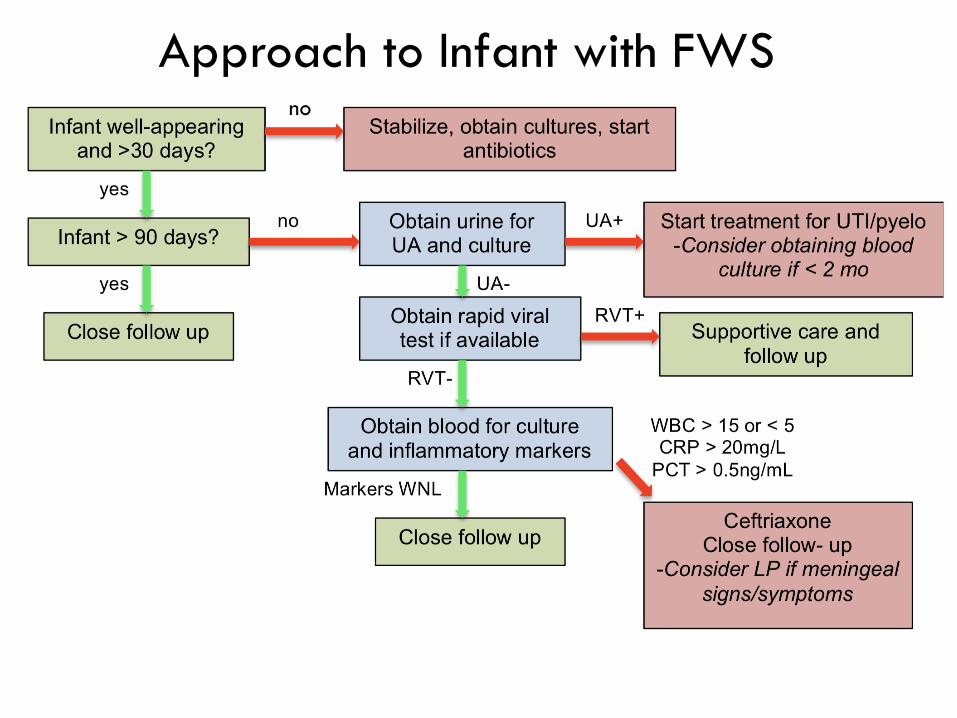
Approach to Infant with FWSno

Case Continued
Since Quokka is less than 30 days, and has no source for her fever, you obtain a UA/urine cx and blood cultures and perform an LP
Her UA is positive for LE and nitritesNow what do you do?

URINARY TRACT INFECTIONS

Risk of UTI in Infants with FWS
0
2
4
6
8
10
12
14
16
18
20
0 1 m 3m 6m 12m 18m
Girls
UncircBoysCircBoys

Who is at risk for UTI/pyelonephritis?
All infants with FWS < 3 mo of ageGirls > 3 mo of ageFWS (>39) and < 24 months
Boys > 3 mo of ageCircumcised: FWS (>39) and < 6 moUncircumcised: FWS (>39) and < 12 mo
Additional Risk Factors:Length of fever (> 2 days)

Diagnostic Dilemmas
Collection of urineBy catheter for: Infants < 3 mo of age (high risk) Ill-appearing/getting antibiotics
Consider bag collection for: Low-risk infant (circ boy> 3 mo, girl/boy>1 year) If UA +, consider cath for culture
Results:+ UA: start empiric treatment, send for cxNeg UA: UTI very unlikely, even in young infantsConsider sending for culture in high risk neonate

Treatment
Empiric treatment based on local E. Coli resistancePO cephalexin safe, tasty, narrow spectrumIV if <2 mo, toxic or not tolerating POTotal course: 7-14 days (for pyelo)
Imaging after UTI U/S in infants <3 mo, older kids if recurrentVoiding Cystourethrogram (VCUG) only if high
grade VUR/obstruction on U/S Roberts 2011;Pediatrics128(3):595–610

Case Continued
Quokka’s 2.5 yo brother Bilby has also had a runny nose and cough for 3-4 days, and Tmax of 38.5
Last night he started pointing at his ear saying “owie”, and mom is concerned that he has an ear infection
What would you do next?

ACUTE OTITIS MEDIA
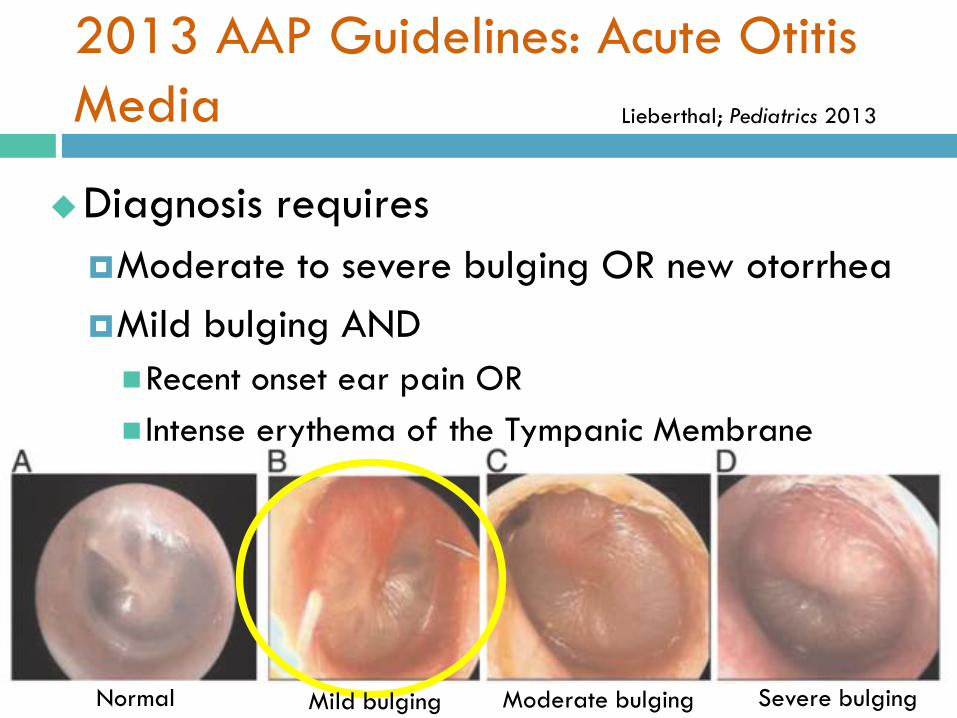
2013 AAP Guidelines: Acute Otitis Media
Diagnosis requiresModerate to severe bulging OR new otorrheaMild bulging AND Recent onset ear pain OR Intense erythema of the Tympanic Membrane
Lieberthal; Pediatrics 2013
Normal Mild bulging Moderate bulging Severe bulging
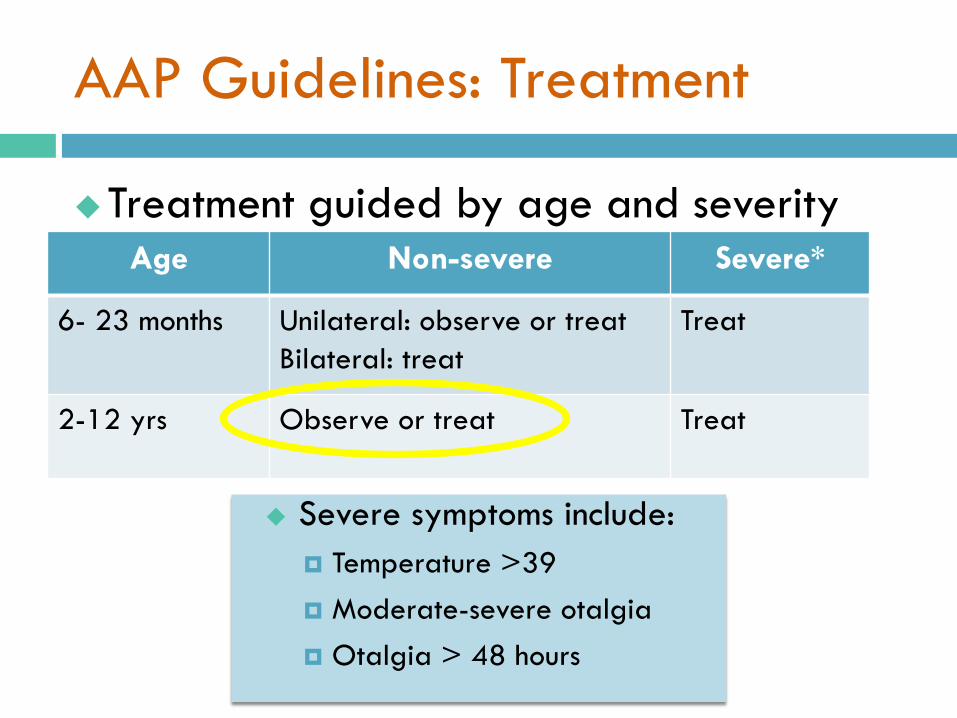
AAP Guidelines: Treatment
Treatment guided by age and severityAge Non-severe Severe*
6- 23 months Unilateral: observe or treatBilateral: treat
Treat
2-12 yrs Observe or treat Treat
Severe symptoms include: Temperature >39 Moderate-severe otalgia Otalgia > 48 hours

AAP Guidelines: Antibiotics
First Line: Amoxicillin (80-90 mg/kg/day)
Amoxicillin-Clavulanate (90m/k/d amox +6.4 m/k/d clav) If Amoxicillin in previous 30 days, + conjunctivitis
Cephalosporins: Cefdinir, cefuroxime, cefpodoximeMay have slightly lower efficacy against S. pneumoniae
Treatment failure = persistent sx for >48-72h Amoxicillin-Clavulanate or IM CeftriaxoneConsider drainage, culture, specialist
Tubes: > 3 infections/6mo OR 4 in last year
Lieberthal; Pediatrics 2013

Case continued
You decide to treat Bilby’s OM supportively, but since he is febrile with cough, you are also concerned about flu
He is well-appearing, with normal vital signs, and no resp distress
He used an inhaler at 6 mo with a viral infection, no other PMH, has not yet received flu shot
Should you test him for influenza?

INFLUENZA

Current season…
CDC, 2019

Who to Test/Treat (RVT= 60% sens/98% spec)
Treat WITHOUT testing: clinical suspicion ANDHospitalized/severe illnessHigh risk for severe disease (<2yrs, chronic disease,
immunosuppressed, chronic ASA therapy)
Test and treat only if + Otherwise healthy AND <48 hrs of illnessHigh risk contacts at home
RegimensOseltamivir (Tamiflu) weight-based dosing BID x 5 d
Our patient?
Case Continued
As you are wrapping up the visit, mom asks if big brother Quoll needs his “TB shot” for first grade
You ask a few clarifying questions:Last PPD when starting kindergarten was
negativeNo travel, no active TB contacts, no chronic
medical conditions

TB SCREENING
Tuberculosis Screening
Universal Screening NOT recommendedScreen those at high risk of disease OR
progressionSymptoms of disease, TB+ close contactHIV disease, immunosuppressedTravel to/immigration from/living with
immigrant from an endemic country, stay in jail/homeless shelter
Quantiferon OK in kids > 2 if BCG

Case Presentation: 3 yo with cough
Bandicoot is a 3 yo who presents with 2 weeks of cough, keeps her awake, and occasional post-tussive vomiting
She has a PMH of bronchiolitis (6 mo) and is up to date for age on vaccinations
VS: T 38.2, P 130, RR 42, O2 sat 95%Her mother wants to know if this could be
“the whooping cough”

PERTUSSIS

Pertussis Epidemiology
Tdap
Acellular pertussis

Pertussis: Clinical Diagnosis
Cough lasting >2 weeks + 1of the following:Apnea* Paroxysms of coughingInspiratory “whoop”Post-tussive vomiting (least specific)
cdc.gov/pertussis
Older children
*May occur without cough
Neonates/young Infants

Pertussis: Treatment
Major benefits:Prevent severe disease* in those at riskPrevent spread to high risk (HR) patient
Empiric treatment (Azithro): high suspicion and/or HR Infants <1 year (< 3mo, preemie at highest risk)Pregnant women near termUnimmunized or underimmunized
Test and treat if +:HR but low clinical suspicionPatient LR but has HR contacts
*Only treatment BEFORE paroxyms may shorten course

Case Continued
Bandicoot’s vaccination status and non-specific sx make pertussis less likely
However, her RR (42) and O2 sat (95%) make you concerned for pneumoniaWell-appearing, in minimal resp distress
aside from tachypneaDecreased breath sounds with crackles over
the LLL

What is the RECOMMENDED next step?
A. Obtain a PA and lateral CXRB. Obtain a blood culture and CBCC. Obtain a sputum cultureD. Start PO amoxicillin and discharge with
close follow upE. Start IV cefuroxime and admit

COMMUNITY ACQUIRED PNEUMONIA

Pediatric CAP: Diagnosis
ClinicalSymptoms of acute illness (ie: fever) + resp
distress (tachypnea*, retractions, hypoxia) ANDFocal lung findings on exam OR on CXR
ImagingChest x-ray NOT recommended routinely in
outpatientsDoes not distinguish between pathogens (viral,
atypical, etc)
Bradley JS, et al. Clin Infect Dis. 2011
*MOST SENSITIVE sign

Pediatric CAP: Laboratory Diagnosis
Routine lab testing NOT recommended Blood cultures:
Clinically worsening or hosp with mod/severe disease Viral testing (flu, RSV)
IF no evidence of bacterial co-infection CBC/CRP
Not recommended Testing for Mycoplasma pneumoniae, S. pneumo
If available, may guide antibiotic selection
Bradley JS, et al. Clin Infect Dis. 2011

Pediatric CAP: Causes
Viral is most common< 2 yrs: S. pneumoniae, C.
Trachomatis2-5 yrs S. pneumoniae, M.
pneumoniae, H influenzae, C. pneumoniae
M. pneumoniae, C. pneumoniae > S. pneumoniae
2 MO TO 5 YRS: OVER 5 YEARS:
Bradley JS, et al. Clin Infect Dis. 2011
Based on age, severity, local resistance
Pediatric CAP: Treatment
Inpatient or Outpatient 1st line treatment:Amoxicillin/ampicillin in infants and young children Macrolide (azithro) in kids > 5
Ill patent or high-level PCN resistance: 3rd generation cephalosporin if suspect S. pneumoVancomycin if suspicion for MRSA+Macrolides if suspicion high for M. pneumoniae
and C. pneumoniae
Bradley JS, et al. Clin Infect Dis. 2011

Case Continued
As you are explaining Bandicoot’s discharge plan to her mother, she asks you to check on baby brother Wallaroo who also has a “cold”
The 9 month old is alert and well-appearingRR of 55, T of 38.5, O2 sat of 91%Moderate retractions, coarse wheezes and
rhonchi throughout on exam
You are concerned about bronchiolitis: what is the next step in diagnosis?
A. RSV testB. Chest XrayC. Response to albuterolD. Response to hypertonic salineE. Nothing, you have already made the
diagnosis
BRONCHIOLITIS
Bronchiolitis
Virally-mediated inflammation, edema, and epithelial necrosis in small airways50-75% caused by RSVrhinovirus > influenza > Human
metapneumovirus > coronavirus
Etiology correlates poorly with severity
A leading cause of admission in kids < 2

Bronchiolitis: Diagnosis
Clinical DiagnosisUpper respiratory prodrome followed by
increased WOB, wheezing, hypoxia, classic lung exam
Radiographs and lab studies are not routinely recommended
Ralston, SL et al Pediatrics. 2014

Treatment: Albuterol trial: if dx uncertain, asthma
suspectedCorticosteroids, racemic epi, HT saline: not
routinely recommendedHT saline: studies mixed, heterogeneity
MonitoringContinuous pulse ox not requiredSupplemental O2 only for persistent < 90%
Ralston, SL et al Pediatrics. 2014Bronchiolitis: Treatment

Apnea: risk fx< 8 weeks corrected agePrevious apnea during illnessNot pathogen specific
Prophylaxis: palivizumab (Synagis)Preterm infants: gestational age <29 wksCHD/CLD: < 12 months old (<24mo if
getting medical therapy)5 monthly doses/season
Ralston, SL et al Pediatrics. 2014Bronchiolitis: Other considerations
VACCINES
“An ounce of prevention is worth a pound of cure.”- Benjamin Franklin

2019 Standard Schedule

Primary Series
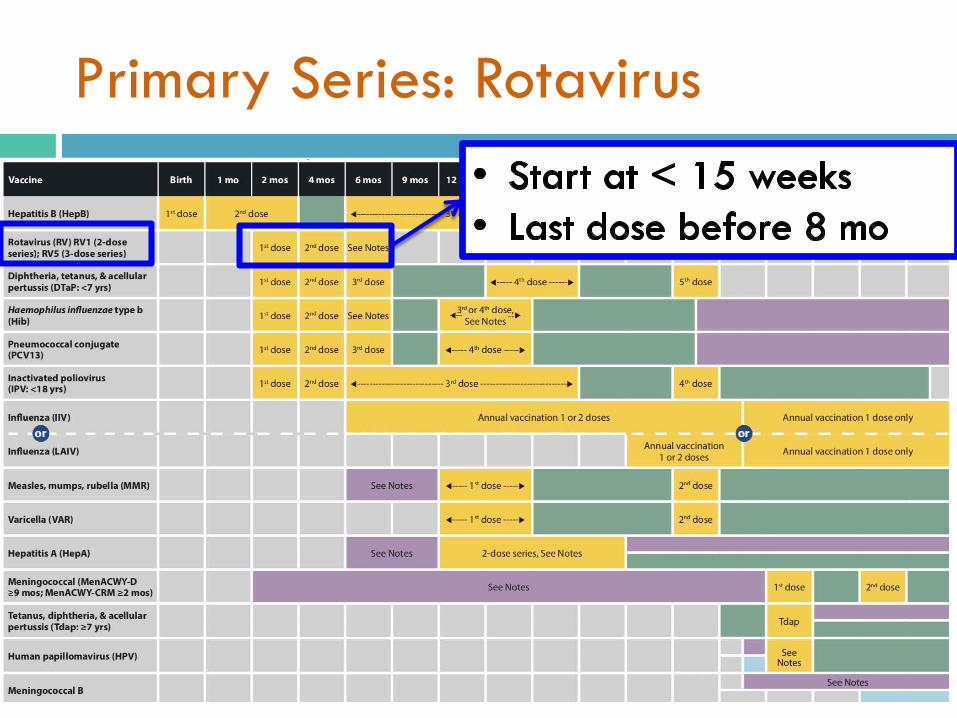
Primary Series: Rotavirus

Primary Series: Hepatitis B

Primary Series: Boosters

Live Attenuated Vaccines
• NEW

Teen Vaccines
• Menactra at 11 and 16yo• TdaP at 11yo: required for 7th grade in CA• HPV (9 valent): 2 doses (if < 15)
• Min age 9; 2nd dose at 6-12 mo
• NEW: Tdap for pregnant teens

Influenza
• NEW
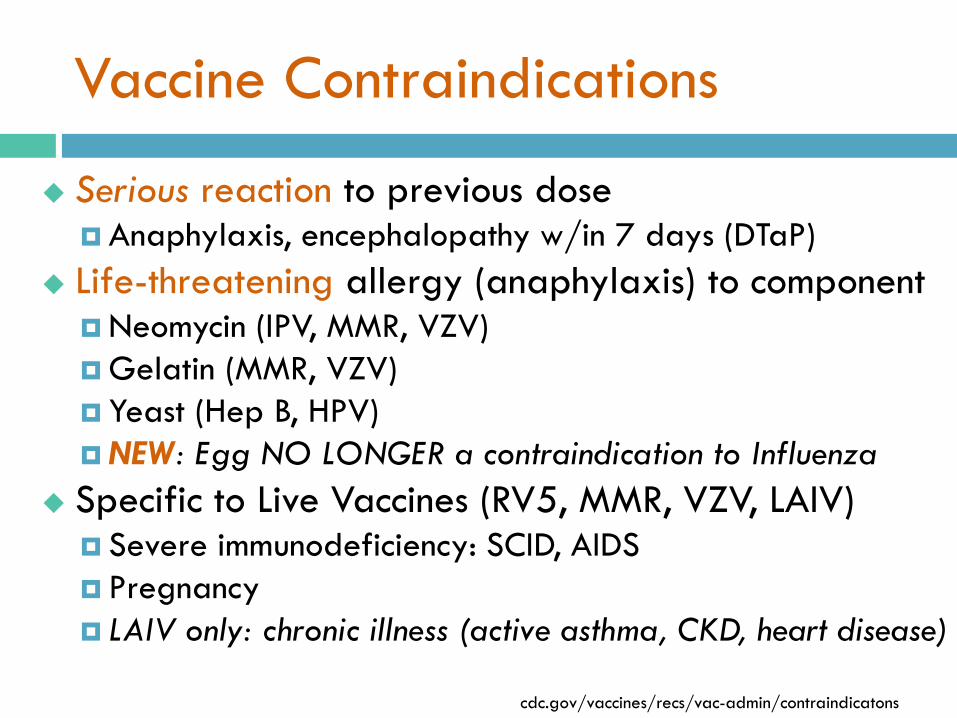
Vaccine Contraindications
Serious reaction to previous doseAnaphylaxis, encephalopathy w/in 7 days (DTaP)
Life-threatening allergy (anaphylaxis) to component Neomycin (IPV, MMR, VZV)Gelatin (MMR, VZV) Yeast (Hep B, HPV)NEW: Egg NO LONGER a contraindication to Influenza
Specific to Live Vaccines (RV5, MMR, VZV, LAIV) Severe immunodeficiency: SCID, AIDS Pregnancy LAIV only: chronic illness (active asthma, CKD, heart disease)
cdc.gov/vaccines/recs/vac-admin/contraindicatons
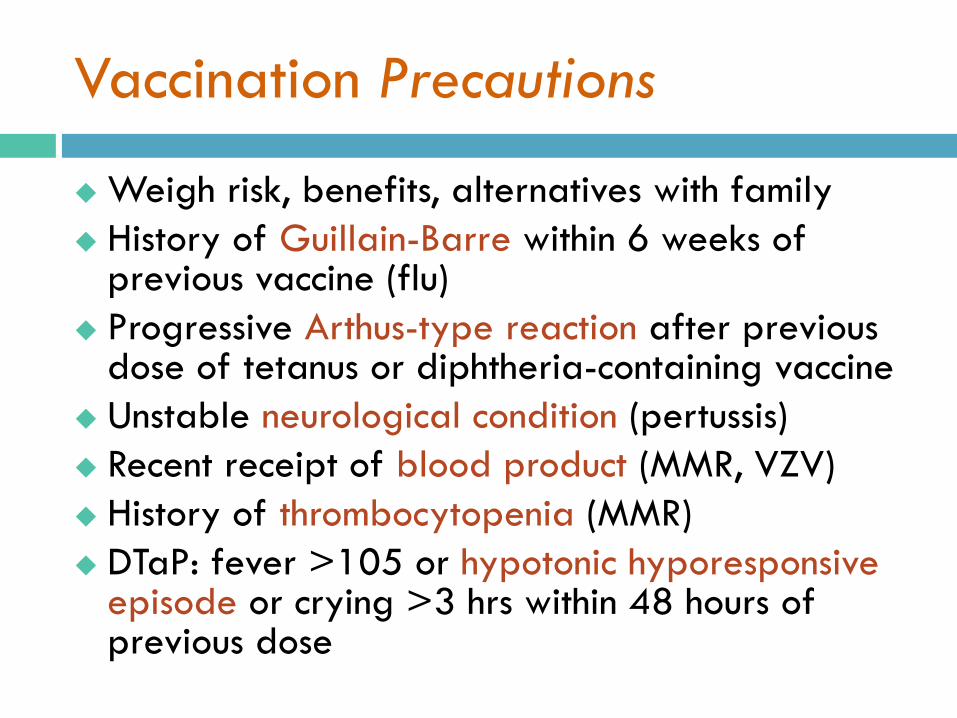
Vaccination Precautions
Weigh risk, benefits, alternatives with family History of Guillain-Barre within 6 weeks of
previous vaccine (flu) Progressive Arthus-type reaction after previous
dose of tetanus or diphtheria-containing vaccine Unstable neurological condition (pertussis) Recent receipt of blood product (MMR, VZV) History of thrombocytopenia (MMR) DTaP: fever >105 or hypotonic hyporesponsive
episode or crying >3 hrs within 48 hours of previous dose

VISUAL DIAGNOSIS
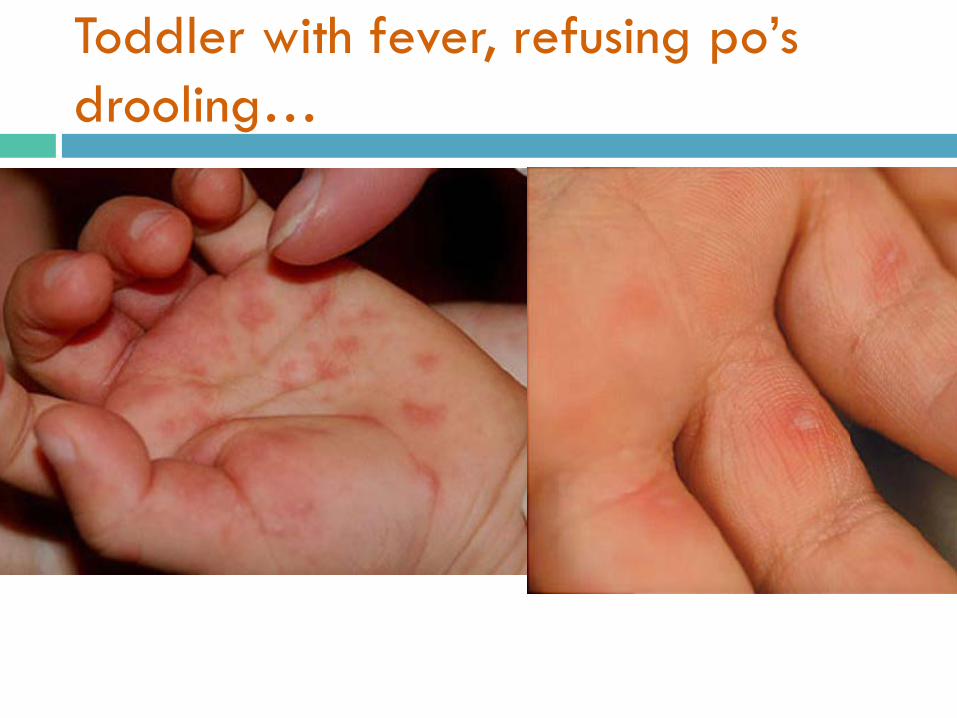
Toddler with fever, refusing po’sdrooling…

Examples of “atypical coxsackie”
Eurosurveillance.orgPediatrics.aapublications.org

5 yo comes back from camp with fever, cough and runny nose, then develops rash proceeding head to toe

PHASE TIME COURSE DESCRIPTION
Prodromal 2-3 days Fever + 3 C’s: cough, coryza (runny nose), conjunctivitis
Exanthem 3-5 days Erythematous macules proceed cranial -> caudal. May become confluent. Koplik spots
Recovery 5+ days Fever subsides and rash fades
Measles

Measles Fast Facts
Droplet/airborne spread, ~90% 2 doses of vaccine = 97% effective Dx by serology (IgM or rise in IgG) or PCR High risk for severe illness = <5yo or >20yo,
pregnant, immunocompromised Severe/fatal complications:
Encephalitis: 1/1000 Resp/neurologic complication: 1-2/1000 Subacute sclerosing panencephalitis (SSPE): rare
No specific treatment (vit A for severe illness)

7 yo with fever, sore throat now with dry, diffuse rash most pronounced on trunk and face

10 mo old with rash on day 7 of amoxicillin for AOM
From: Consultant 360
• Rash started on day 6 of treatment• Started truncally, spread to head and
extremities, including palms and soles• Not itchy, otherwise well

Amoxicillin Drug Eruption
Delayed hypersensitivity (T-cell mediated, Type IV) reaction Morbilliform, often includes palms and soles,
day 5-10 of treatmentNOT a drug allergy, and not associated with
advancement to anaphylaxisAllergy = itchy, urticarial, within hours, may
progress May affect up to 10% of pedi pts treated
with amox or PCN Future use of amox NOT contraindicated

5 yo with temp of 39 for 5 days
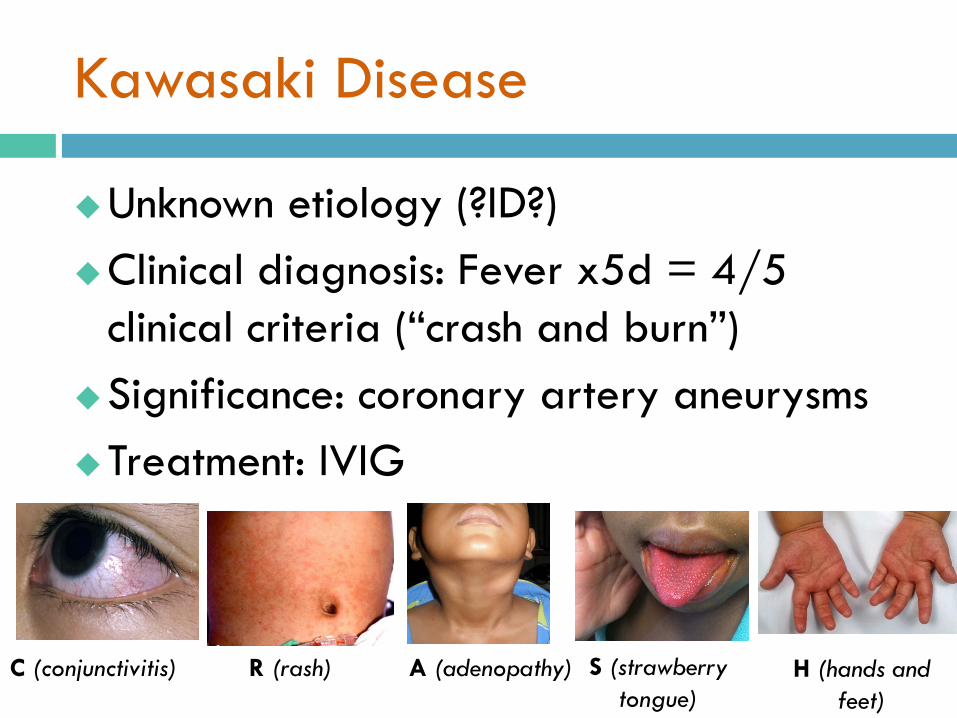
Kawasaki Disease
Unknown etiology (?ID?)Clinical diagnosis: Fever x5d = 4/5
clinical criteria (“crash and burn”)Significance: coronary artery aneurysmsTreatment: IVIG
C (conjunctivitis) R (rash) A (adenopathy) S (strawberry tongue)
H (hands and feet)

Marsupials!
Bandicoot
BilbyQuoll
Quokka
Wallaroo

References
1. Greenhow TL, et al. The changing epidemiology of serious bacterial infections in young infants. Pediatr Infect Dis Journal 2014; 33(6): 595-599
2. Roberts KB and the Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months.” Pediatrics. 2011;128(3): 595–610
3. Lieberthal, A et al. The Diagnosis and Management of Acute Otitis Media. Pediatrics 2012; 131(3): e964-e999
4. Bradley, J. et al. The Management of Community- Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Disease Society of America. Clin Inf Dis. 2011; 53(7): e25-e76
5. Ralston, S. et al. Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis. Pediatrics 2014; 134(5): e1474-e1500
6. AAP Committee on Infectious Diseases. Recommendations for Prevention and Control of Influenza in Children, 2018–2019. Pediatrics. 2018;142(4):e20182367
















