Infections in Accident and emergency Philip G. Murphy Consultant in Medical Microbiology, AMNCH...
43
Infections in Accident and Infections in Accident and emergency emergency Philip G. Murphy Consultant in Medical Microbiology, AMNCH Clinical Professor, TCD Tel. ext. 3919 [email protected]
-
Upload
sara-melton -
Category
Documents
-
view
213 -
download
0
Transcript of Infections in Accident and emergency Philip G. Murphy Consultant in Medical Microbiology, AMNCH...

Infections in Accident and emergencyInfections in Accident and emergency
Philip G. Murphy
Consultant in Medical Microbiology, AMNCH
Clinical Professor, TCD
Tel. ext. 3919

Lecture objectives
• Integrate Microbiology knowledge to A&E Doctor• Consider factors unique to A & E dept Vs GP• Emergency infections• Trauma infection eg tetanus• Systematic approach to A & E infection• Ix and Dx clinical Vs empirical• Others: tourist fever, bites, sharps, infection control• Is an antibiotic indicated ?
Unique factors in A&E
• Concerned patient/parent ?? Need admission
• Interface of community and hospital
• Gatekeeper of all inpatient admission
• Under-resourced in IRL
• Over usage Vs GP.
• GP 2nd opinion
• Triage

Emergency Infections• Meningitis (Pen access)
• Bacteraemia / septicaemia
• Endocarditis
• Osteomyelitis
• Otherwise minor infection in
Immunsuppressed eg varicella
septicaemia
Fresh splinter haemorrhageMeningococcal petechiaepurpura & DIC (bleeding NG)

MeningitisMeningitis
• Bacterial: N. Men ABC, pneumococcus, Hib, E coli, List.• Viral: Enterovirus group, Herpes• Hx: prodrome, contact • Dx: Meningism, fever, rash• Ix: CT. CSF and blood C&S, PCR• Rx: Ceftriaxone, pen• Px: ?who, rifampicin 600mg bd 2 days• Public Health

What is Shock?
• A physiologic state characterised by– Decrease in tissue perfusion – Inadequate oxygen delivery
• Delivery isn’t keeping up with demand
• May be bacterial: LPS, toxin
Gram negative – E. coli
Gram Positive - Staphylococcus aureus

What is SIRS?What is SIRS?
The systemic inflammatory response syndrome is systemic level of acute inflammation, that may or may not be due to infection, and is generally manifested as a combination of vital sign abnormalities including fever or hypothermia, tachycardia, and tachypnoea.

Risk Factors for SIRS/SepsisRisk Factors for SIRS/Sepsis• Extremes of age• Indwelling lines/catheters• Immunocompromised states• Malnutrition• Alcoholism• Malignancy • Diabetes• Cirrhosis• Male sex• Genetic predisposition?

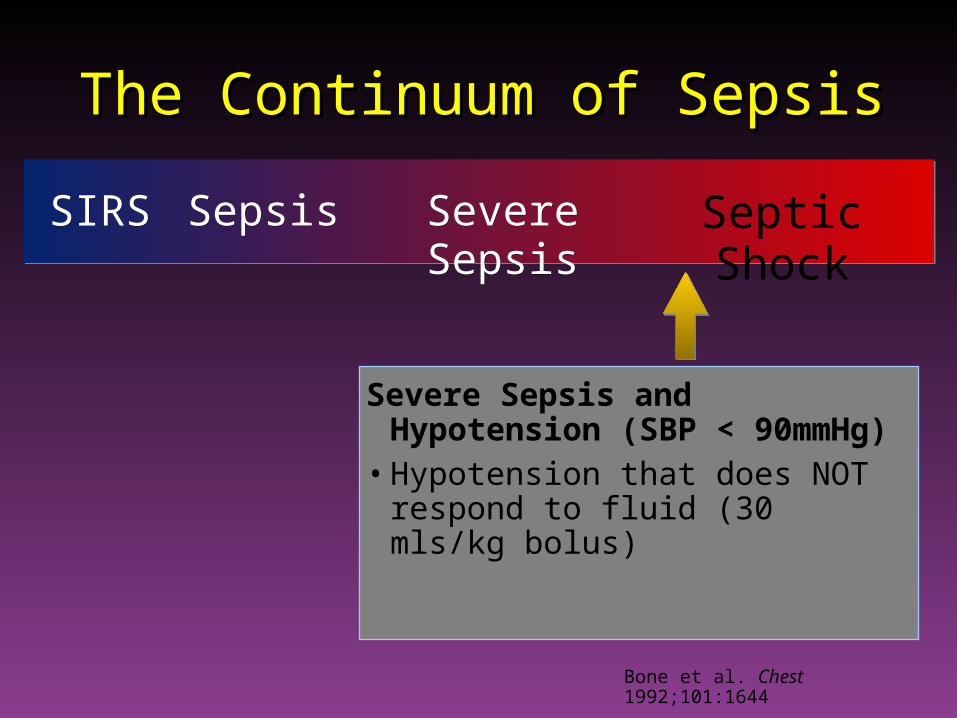
The Continuum of SepsisThe Continuum of Sepsis
Bone et al. Chest 1992;101:1644
SepsisSepsisSIRS Severe SepsisSevere Sepsis
Systemic Inflammatory Response Syndrome SIRS criteria-must have 2 or more of the following:
• Temp < 36 ° C or > 38 ° C• HR > 90
• RR > 20 or PCO2 < 4.3
• WBC < 4 or > 12 or immature bands > 10%
Septic ShockSeptic Shock

The Continuum of SepsisThe Continuum of Sepsis
SepsisSIRSSIRS Severe SepsisSevere Sepsis Septic ShockSeptic Shock
Sepsis = • Suspected or confirmed
infection• 2 or more SIRS criteria
Bone et al. Chest 1992;101:1644; Balk, RA

The Continuum of SepsisThe Continuum of Sepsis
SepsisSepsisSIRSSIRS Severe Sepsis Septic ShockSeptic Shock
Sepsis plus Organ Dysfunction• Elevated Creatinine• Elevated INR. Hyperbili • Altered Mental Status• Elevated Lactate >4• Hypotension that responds to fluid
Bone et al. Chest 1992;101:1644
The Continuum of SepsisThe Continuum of Sepsis
SepsisSepsisSIRSSIRS Severe SepsisSevere Sepsis Septic Shock
Severe Sepsis and Hypotension (SBP < 90mmHg)
• Hypotension that does NOT respond to fluid (30 mls/kg bolus)
Bone et al. Chest 1992;101:1644

Septic ShockSeptic Shock
• Combination– Distributive– Cardiogenic– Hypovolaemic
• Most common form of Shock
• On a continuum from SIRS to Septic Shock

Why so Important?Why so Important?Mortality of Severe Sepsis
0
50,000
100,000
150,000
200,000
250,000D
ea
ths
/Ye
ar
AIDS*Severe
Sepsis‡AMI†Breast
Cancer§
†National Center for Health Statistics, 2001. §American Cancer Society, 2001.
*American Heart Association. 2000. ‡Angus DC et al. Crit Care Med. 2001 .
Shock: antibiotic Mx
• Bactericidal not bacteriostatic
• Rapid kill without LPS release eg gentamicin
• Broad cover and de-escalate later in recovery
• Beta lactam + aminoglycoside
• +/- ano2 (metronidazole)
• +/- glycopeptide (vancomycin)
• System review focus

Why so important?•Overall mortality from SIRS/sepsis is approx. 20%. •Mortality is roughly linearly related to the number of organ failures, with each additional organ failure raising the mortality rate by 15%. •Hypothermia is one of the worst prognostic signs. Patients presenting with SIRS and hypothermia have an overall mortality of ~80%.

Organism susceptibilityConcurrent therapyDrug rep pressurePatient pressurePoliciesProphylaxisDrug familiarity:Dosage / costToxicity / kineticsBioavailability
Best guess susceptibilityPatient immune stateNature of infectionPatient physiologyAllergy historyBreast feedingPregnancyAge ComplianceSocial/work issues
Factors influencing prescribing Choice

Trauma infectionTrauma infection
• Wound management
• Compound or closed
• Dirty e.g., Tetanus
• cSSI e.g.,Cellulitis
CellulitisCellulitis
• 90% Haemolytic Streptococci• 10% Staphylococci
• Culture if skin broken• Rx Penicillin + Flucloxacillin• Increase dose until erythema controlled• Monitor CRP• 2nd line Clindamycin• Beware necrotising fasciitis


Tetanus preventionTetanus preventionClostridium tetanus toxin = neuromuscular toxin S+S: muscle spasm near wound, later generalised, lockjawRx: Ig, vaccine, antibiotic
• Type of woundClean (Low Risk) Tetanus Prone (High Risk)• Clean incised wound Any wound or burn > 6 hours old • Superficial graze Any wound with one or more of
the following:• Scald
Contact with soil, manure, compost
Puncture type woundInfected woundCompound fractureWound containing foreign bodiesLarge amount of devitalised
tissueAnimal or human bite

Risk assessment of wounds for use of tetanus immunoglobulin (TIG)
Age Immunisation status Clean wound Tetanus prone wound
<4 y <3 doses or unknown DTaP/IPV+/-Hib TIG, DTaP/IPV +/- Hib3 or more doses Nil Nil Consider TIG
>4 to 9y <3 doses or unknown DTaP/IPV TIG plus DTaP/IPV3 doses only, >5 years since last dose DTaP/IPV DTaP/IPVConsider TIG3 or more doses, <5 years since last tetanus toxoid Nil Nil Consider TIG4 or more doses, >5 years since last dose Nil DTaP/IPV, consider TIG
>10 y <3 doses or unknown Td TIG plus Td/IPV3 or more doses >10 years since last dose Td Td, consider TIG3 or more doses, <10 years since last dose Nil Consider TIG
www.immunisation.ie
? AntibioticUse a system approach
• URT
• LRT 70% of antibiotic prescriptions
• SST
• GUT- STD
• CVS Shock emergency
• CNS meningitis emergency
• GIT diarrhoea
• Common viral: HS, VZ
• Others: tropical parasites, Toxoplasmosis etc
• Post-op hospital & minor ops.

Primary care
• 80% of all antibiotics
• 80% respiratory tract indications
• >50% still probably unnecessary
• Cough probably the commonest acute single reason for consulting (130 per 1000 patients per year)

LRTI
Apical TB
Multi-lobar Pneumococcal
Diffuse alveolar Influenzae
Bronchial pneumococcal
Etiologic determinants for pneumonia
Host characteristics Age State of health Immunocompetence
Environmental exposure Geographic location Community acquired vs nosocomial Closed population settings (daycare centers, military camps, nursing homes) Unusual exposures (eg, animals)
Pathogen characteristics Virulence Inoculum size

Community Acquired Community Acquired PneumoniaPneumonia
• Epidemiology:– Incidence 3/1000– Mortality 2-30%
• <1% for those not requiring hospitalisation
– fewest cases in 18-24 yr group– probably highest incidence in <5 and >65 yrs– mortality disproportionately high in >65 yrs
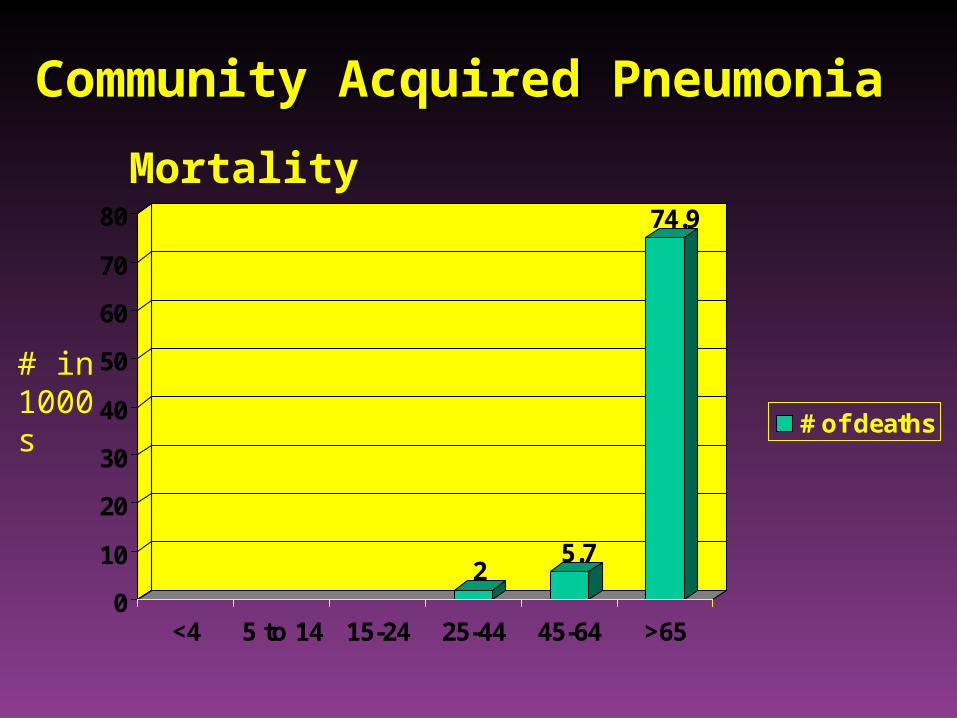
Community Acquired PneumoniaCommunity Acquired Pneumonia
25.7
74.9
0
10
20
30
40
50
60
70
80
<4 5 to 14 15-24 25-44 45-64 >65
# of deaths# in 1000s
Mortality

• Risk Factors for pneumonia– age– alcoholism– smoking– asthma– immunosuppression– institutionalisation– COPD– PVD– dementia
Community Acquired Pneumonia
ID Clinics 1998;12:723. Am J Med 1994;96:313

• Laboratory Tests:• CXR
• FBC with differential
• U+E
• glucose
• LFTs
• Sputum culture
• Blood culture
• oxygen saturation
• Urinary antigen: pneumococcus or Legionella
Community Acquired Pneumonia

Diagnostic Evaluation• CXR
– usually needed to establish diagnosis
– prognostic indicator
– rule out other disorders
– may help in etiological diagnosis
• Only 3% of outpatients and 28% of ED patients with suggestive signs and symptoms actually have pneumonia
Community Acquired Pneumonia
J Chr Dis 1984;37:215-25

CURB-65: Confusion (8 or less on AMT)Urea > 7Resp Rate > 30BP (< 90/60)Age > 65 Score: 0-1 low risk (non severe - discharge)
2 increased risk (consider admission)3 high risk (severe – admit)
Also useful: Sats <92% or PaO2 <8 kPa
Bilateral diseaseAge >50Co-morbidity
BTS CAP guidelines: Thorax 2004

CURB-65 Mortality
0 0.7%
1 3.2%
2 13%
3 17%
4 41.5%
5 57%

Microbial aetiology
• Haemophilus influenzae (3-10%)• Streptococcus pneumoniae (20-60%)• Moraxella catarrhalis
• Mycoplasma pneumoniae (1-6%)• Chlamydia pneumoniae (4-6%)• Chlamydia psittaci• Legionella pneumoniae (2-8%)• Coxiella burnetti• Viral (2-13%)• 40-60% No cause identified • 2-5% 2 or more causes identified
Conventional
Atypical

Pneumococci Vs time since last antibiotic(n =919 children)
0
10
20
30
40
50
602-
7 w
eeks
15-A
ug
16-2
3
24-3
1
32-3
9
40-4
7
48-5
2
sensitiveresistant
Hospital CAP Hospital CAP Antibiotic strategy
• 1st line: Augmentin +/- macrolide (clarithromycin)
Moxifloxacin if pen allergic
• 2nd line: 3rd gen ceph +/- quinolone
eg., ceftriaxone +/- ciprofloxacin

Tourist FeverTourist Fever
• Think global - act local
• Avian influenzae (H5N1)
• SARS
• Haemorrhagic fevers (Lassa, Ebola)
• Legionella
• Typhoid
• Others

Avian flu Avian flu Acute onset of fever ( ≥ 38°C) with S & S of an acute respiratory infection. AND At least one of the following exposures < 7 days prior to onset of symptoms: Contact with poultry or wild birdsReside in or have visited an area of a country where influenza A/H5N1 is currently suspected or
confirmed as reported in the HPSC web-sitehttp://www.ndsc.ie/hpsc/A-Z/Respiratory/AvianInfluenza/AffectedCountries/Having been in close contact with sick or dead domestic poultry and/or wild birds in an affected
area;or having been in a home or farm where sick or dead domestic poultry have been reported in the
previous six weeks in an affected area;
Human Contact: Having been in close contact (<1 metre) with a person reported as a probable or confirmed case of influenza A/H5N1;
Laboratory Contact: Having worked in a laboratory where there is potential exposure to influenza A/H5N1.
http://www.ndsc.ie/hpsc/A-Z/Respiratory/AvianInfluenza/Guidance/File,2199,en.pdf
Inform Public Health infection control and Occupation Health. Health care workers caring for cases of suspected A (H5N1) should be considered for prophylaxis
with oseltamivir (Tamiflu).

Avian influenza arrives in Paris

+ case definition
Infection Control/ Isolation and Reporting• Strict hand hygiene. • Patient to be put into a side room in the ED
immediately.• Staff to wear respirator mask – minimum standard
FFP2, gown/plastic apron, gloves.• Patient to wear surgical mask.• Inform and consult with Infection Control prior to
moving or transferring patient (e.g. X ray).

Blood borne virus exposure(eg needle stick)
• Risk assessment of wound & injury
• Wound toilet
• Hep B – vaccine if non immune
+/- HBIg if source positive
• Hep C - Monitor blood, LFT’s
• HIV – assess for PEP

Animal bites
• Dogs 80%
• Cats 10%
• Humans 5%
• Others 5%
• Basic wound Mx do not close (2o closure)
• Antibiotics if deep Rx Augmentin
• Rabies Rx Vaccine x 5 (+ Ig if high risk)

Infection Control
• Irish A&E departments inadequate– isolation, toilet and washing facilities
• Attempt to isolate and cohort:
diarrhoea,TB., Norovirus

Lecture self assessmentGive examples for each
• How does A&E differ from 10 and 2o care
• Emergency infections
• Management of infected trauma
• Other examples