
A Tool for Criticality Accident Emergency Planning, Training and
Upload
hannah-rodgersCategory
view
218download
1
INFECTIONS IN ACCIDENT INFECTIONS IN ACCIDENT AND EMERGENCYAND EMERGENCY
http://www.tcd.ie/Clinical_Microbiology/Notes on :
Contents of LectureContents of Lecture
Number of Possible Clinical Cases presenting to A/E
Meningitis Animal/Human Bites Tetanus Trauma/Wounds Peritonitis Severe Pneumonia Measles
Each Case FormatEach Case Format
Clinical PresentationDifferential DiagnosesInvestigations-including
biochemistry,haematology,radiology, Microbiology etc
Management

Case OneCase One 15 year old girl presents to A/E by ambulance from G.P
practice, Letter stated she had presented there that day with 1 day
history of headache , feeling generally unwell (No past medical history), G.P had noted non-blanching rash on back of patient, She has administer 4 megaunits of Benzyl Penicillin I/m, called Ambulance
On presentation to A/E, girl was confused /disorientated, photophobic, BP: 80/50 mmHg, Pulse Rate 140 regular, Temperature 35º C (hypothermic) (patient cold), Rash noted on thighs and back– non-blanching

Rash Of Meningococcaemia
Case OneCase One
What to do?Diagnosis
Clinical ExaminationClinical Examination
Of Note:GCS: 12Photophobic, Pupils reacting, Fundoscopy
impossible, nuchal rigidityMild cyanosis
DexamethasoneDexamethasone
Additional studies have shown the benefit of using DEXAMETHASONE 0.15mg/KG 6 hourly2-4 days (give with or before ANTIBIOTIC)
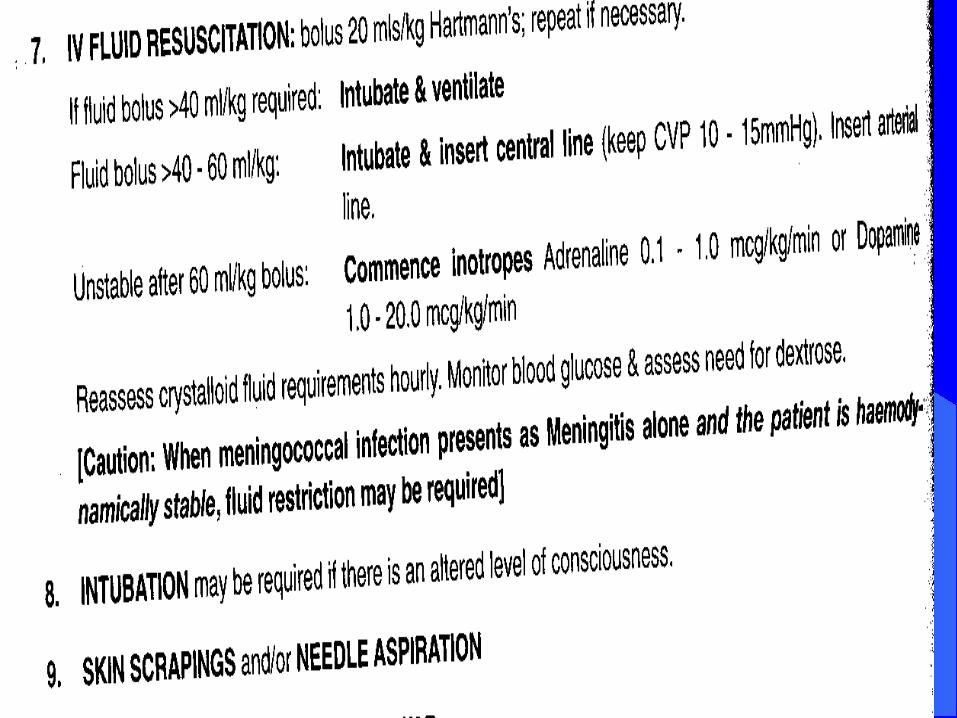
11. FURTHER CONSULTATION: early phone consultation with relevant specialists is desirable, cosider tertiary centre referral
12. COAGULATION13. FURTHER MANAGEMENT14. LP: if meningitis suspected and no
contraindications do when haemodynamically stable( usually day 2-3)
15. NOTIFY public health and initiate CHEMOPROPHYLAXIS if necessary
KEY POINTKEY POINT
The speed with which meningococcal infection is recognised and treated is critical to achieving a successful outcome and clinical suspicion alone mandates treatment
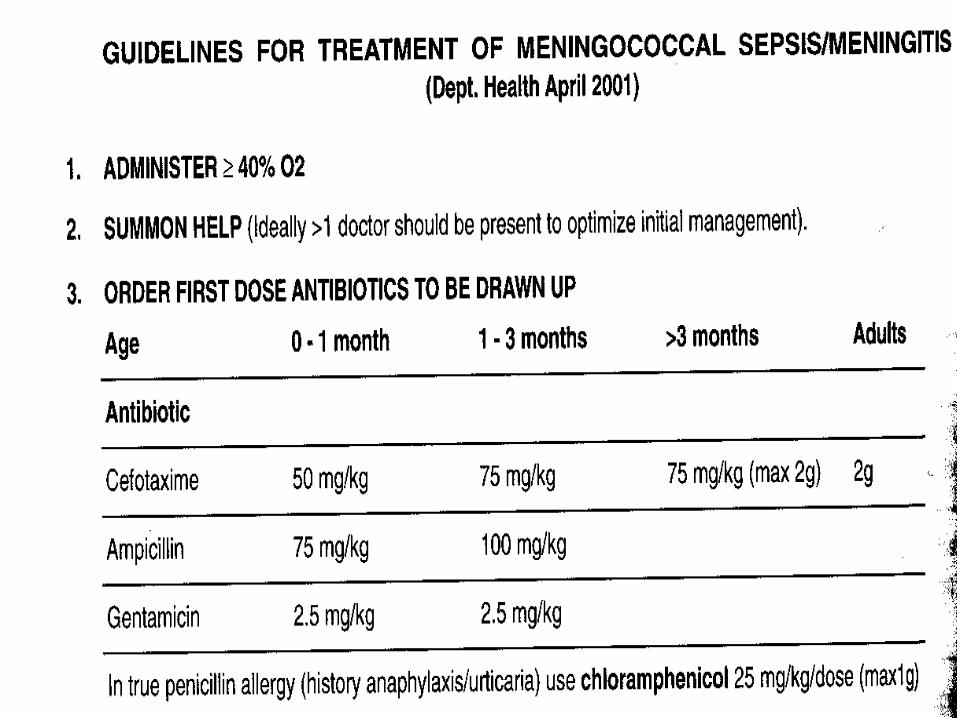
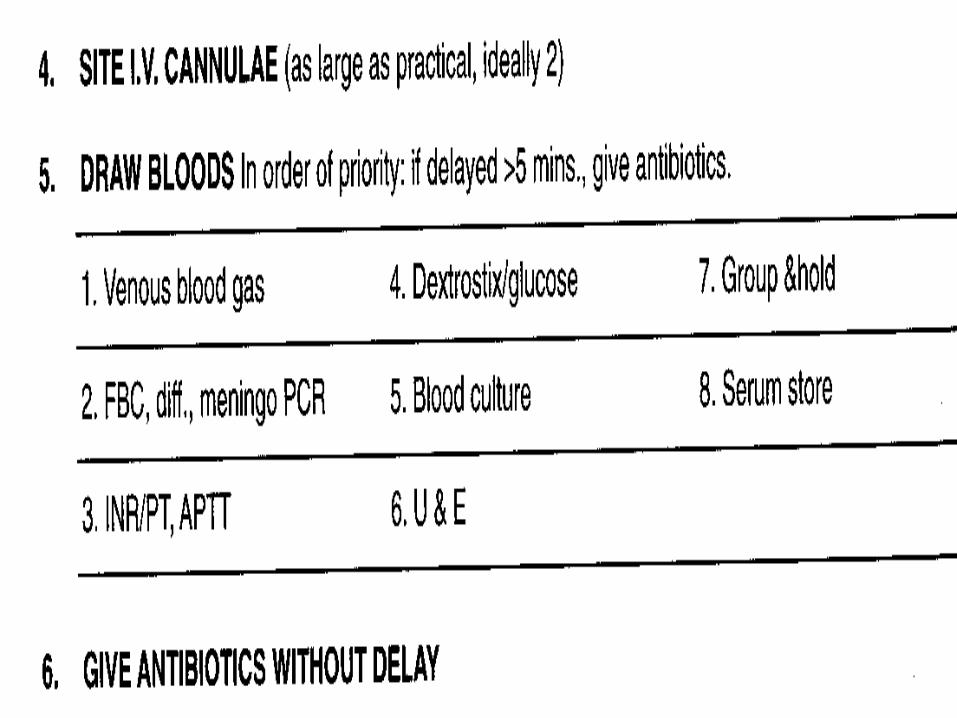
Action-STATAction-STAT Recovery Position, Oxygen given, Assistance requested Large gauge cannulas x 2 for access Blood taken for FBC, U/E, Coag ,Glucose, Group and
Cross match and Blood Cultures, EDTA (FBC) bottle taken for Neisseria meningitidis PCR
Cefotaxime 2 g I/v given ( also give with or before Dexamethasone 0.15mg/KG 6 hourly2-4 days)
Intravenous fluids given 2L Hartmanns STAT Urinary Catheter placed in situ Anaesthetist on call and Microbiologist called
UREGENTLY
ActionAction
Skin Scrapings taken for Gram stain to see Gram negative diplococci consistent with diagnosis
Patient transferred to Intensive Care within 15 minutes
Any additonal specimensAny additonal specimens
Cerebrospinal Fluid –Lumbar puncture depending on Platelets and Coagulation Screen and if hemodynaically stable
Clotted blood sample for OMP for Neisseria meningitidis also
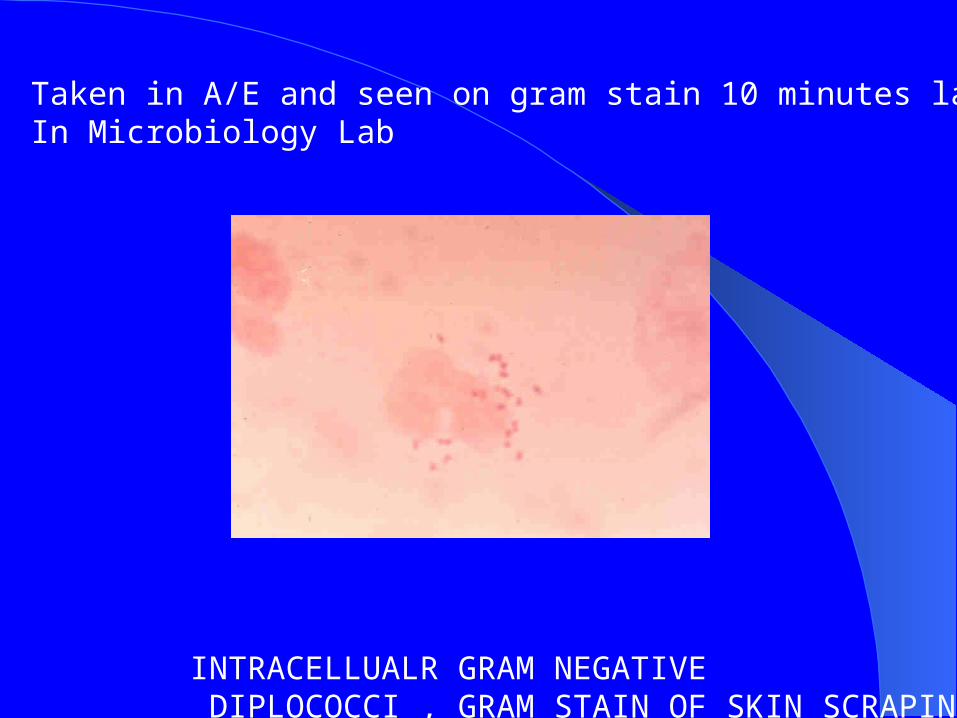
INTRACELLUALR GRAM NEGATIVE DIPLOCOCCI , GRAM STAIN OF SKIN SCRAPINGS
Taken in A/E and seen on gram stain 10 minutes later In Microbiology Lab
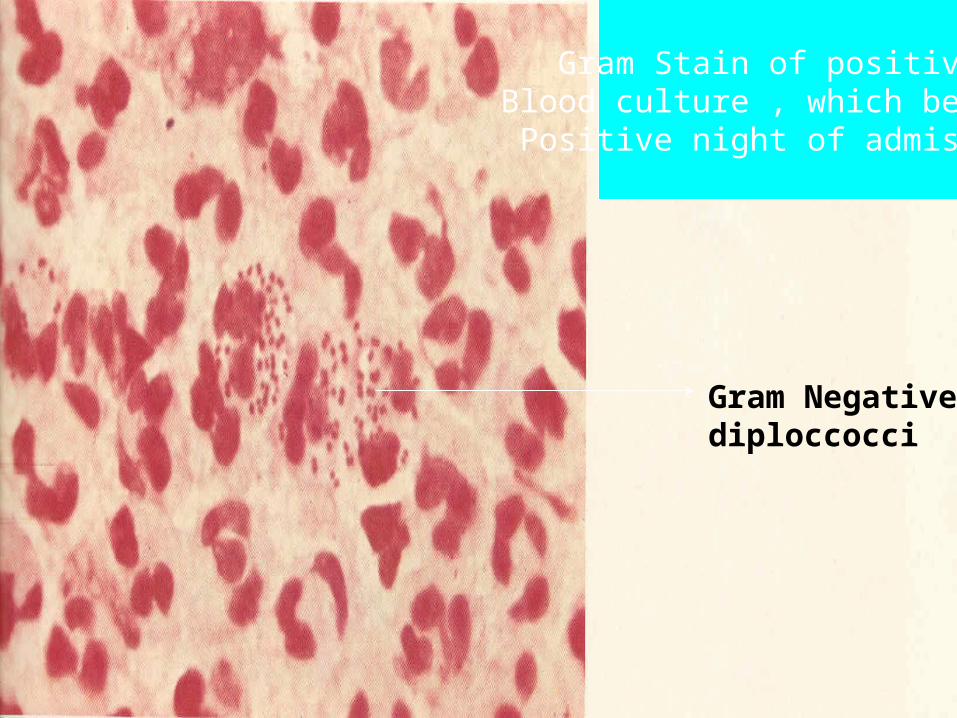
Gram Stain of positive Blood culture , which became
Positive night of admission
Gram Negative diploccocci

DiagnosisDiagnosisMeningococcal SepticaemiaMeningococcal Septicaemia
OutcomeOutcome
Patients survived no loss of limbs or cognitive function but significant areas of skin affected remain painful until replaced by normal skin
Rehabiliation took months
See handout cards
ANIMAL/HUMAN BITESANIMAL/HUMAN BITES
Case 2 HistoryCase 2 History
28 year old gentleman presents 1 hour after (at 4 a.m) with human bite to right hand sustained during a fist fight with his brother outside a nightclub
He complains of a painful 2nd and 3rd metacarpal joint
They have now made -up
On examinationOn examination
There is a 1 x 1 cm rugged abrasion with the indentation of teeth on either side overlying the 1st metacarpal joint on the right hand
All movements of hand appear intact- no evidence of tendon damage
Otherwise there are no injuries to the rest of the body
No significant medical history
No known allergies No history or risk of
HIV/Hepatitis in brother

Action Action
The wound is cleaned ,irrigated with bethadine and debrided (if required)-It is extremely important that this is throughly carried out
X-ray of Right hand is carried out to outrule fracture – no fracture seen
Co-amoxiclav is prescribed for 5 days
Patient is asked to return for follow-up with G.P
Human BiteHuman Bite
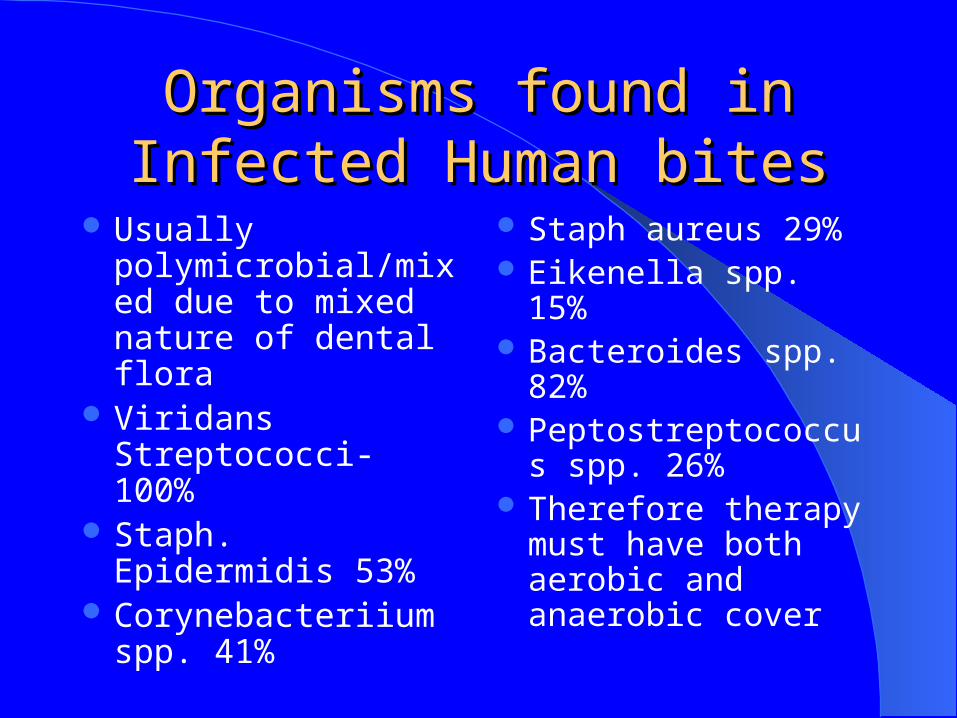
Organisms found in Infected Organisms found in Infected Human bitesHuman bites
Usually polymicrobial/mixed due to mixed nature of dental flora
Viridans Streptococci- 100%
Staph. Epidermidis 53%
Corynebacteriium spp. 41%
Staph aureus 29% Eikenella spp. 15% Bacteroides spp. 82% Peptostreptococcus
spp. 26% Therefore therapy
must have both aerobic and anaerobic cover
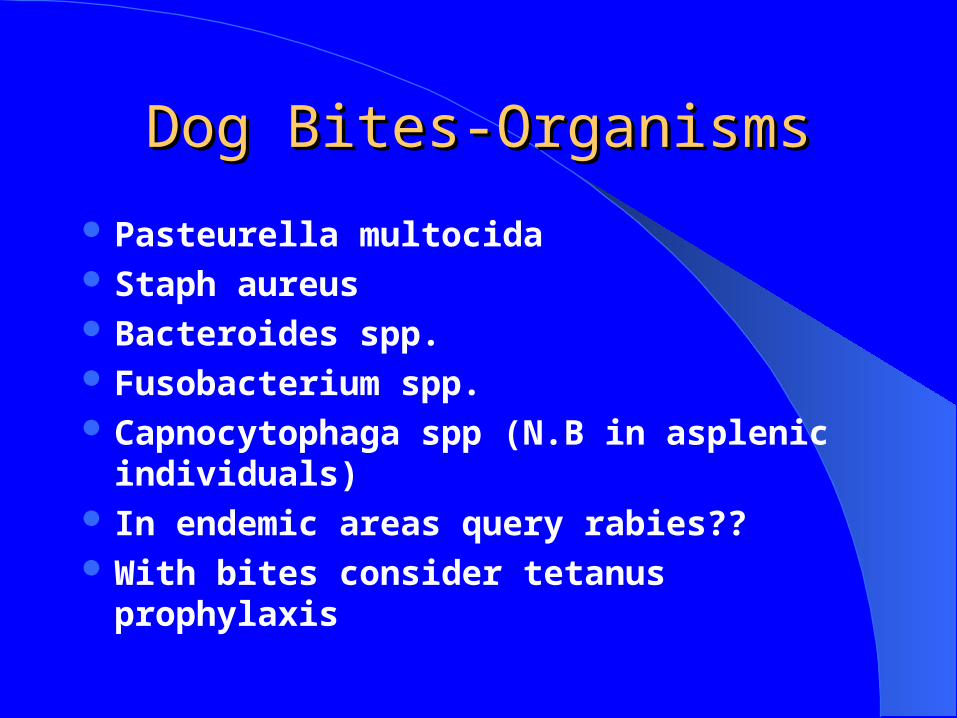
Dog Bites-OrganismsDog Bites-Organisms
Pasteurella multocida Staph aureus Bacteroides spp. Fusobacterium spp. Capnocytophaga spp (N.B in asplenic
individuals) In endemic areas query rabies?? With bites consider tetanus prophylaxis
Case Three Case Three
Case ThreeCase Three
A 72 year old man presents unable to move her jaw, leg muscle spasms and a history of a leg laceration sustained in the garden from a rose bush thorn four days earlier.
Diagnosis?
On ExaminationOn Examination
The man has trismus and a 5x6x2 cm avulsion of the skin on the anterior tibial aspect with black necrotic tissue 2x3x2 cm on the medical aspect of wound.
He had run water over this at the time and bandaged it up himself but did not clean the wound throughly when it happen or seek advice
He never had a course of tetanus vaccination He is allergic to penicillin

Laceration with escharLaceration with eschar
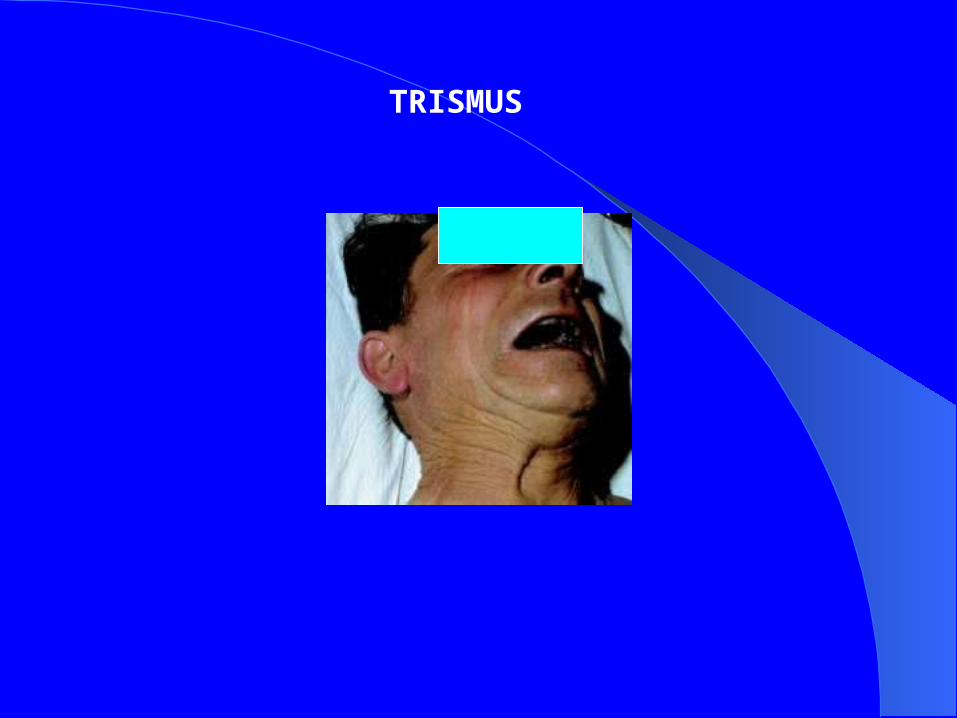
TRISMUS
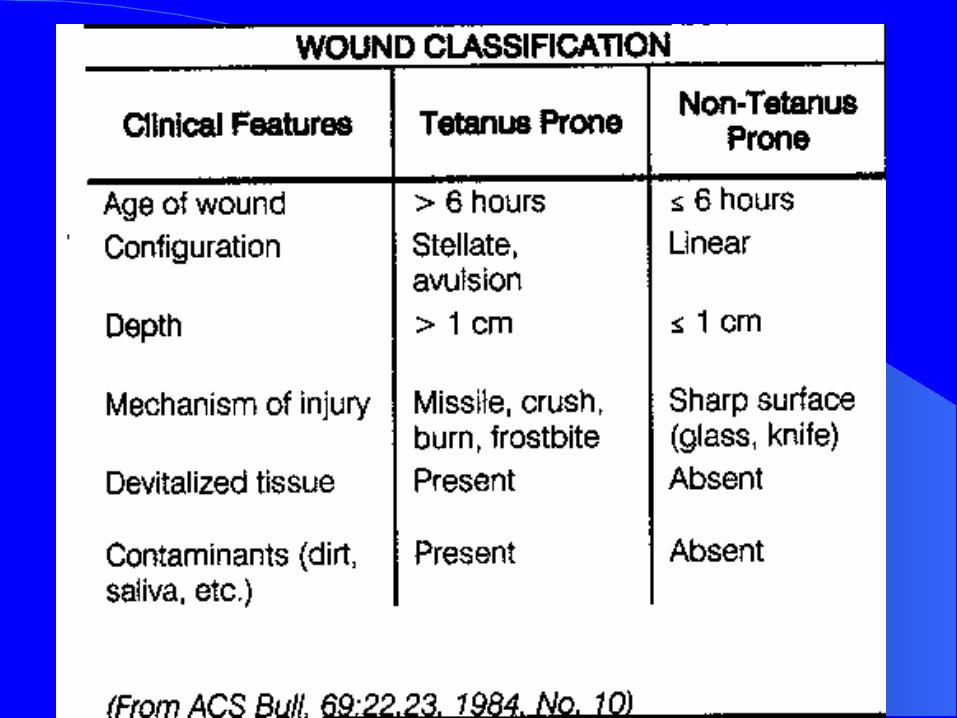

Tetanus ProphylaxisTetanus Prophylaxis
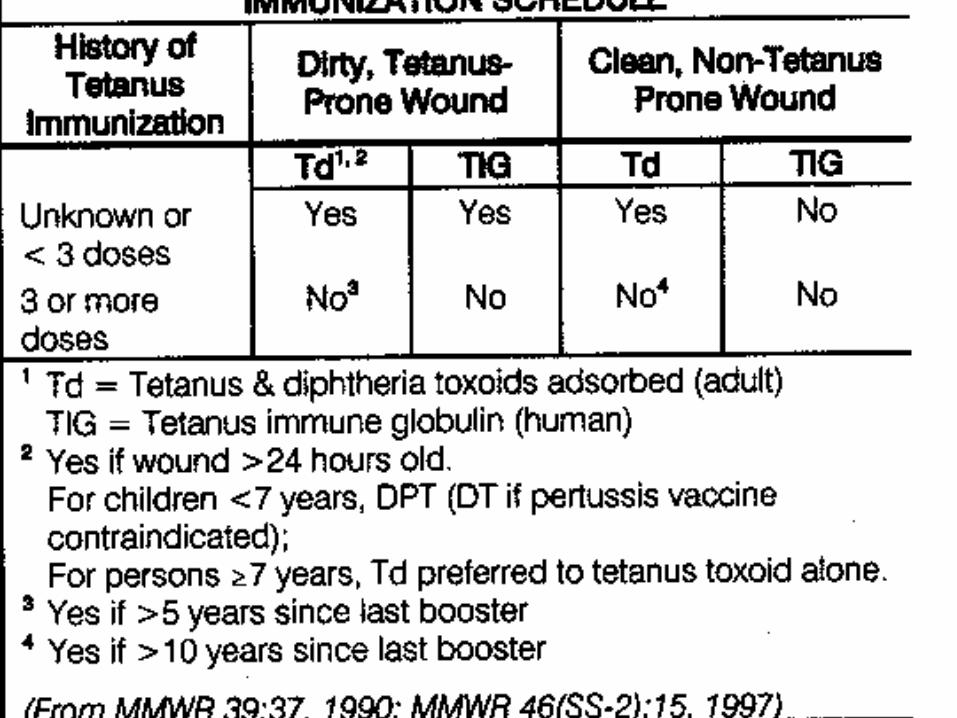

DiagnosisDiagnosis
Tetanus due to Clostridium tetani exotoxin-GABA antagonist- results in blocking of the inhibitory pulses to motor neurones, acts at myoneural junction of skeletal junction and neuronal membranes in the spinal cord
Treatment (not prophylaxis)Treatment (not prophylaxis)
Supportive therapy for muscle spasm- in this case ventilation and sedation required
Human Tetanus ImmunoglobulinTetanus toxoid vaccination (Td)Metronidazole 500 mg 6 hourly I/v for 10
daysCleaning, Irrigation and Debridement of
wound Immediate
OutcomeOutcome
Patient remained ventilated for a number of weeks
Wound required subsequent skin grafting
KEY POINTKEY POINTCLEAN, IRRIGATE, DEBRIDE CLEAN, IRRIGATE, DEBRIDE ALL WOUNDS IMMEDIATELY ALL WOUNDS IMMEDIATELY
AND THROUGHLYAND THROUGHLYVACCINATION AVAILABLE VACCINATION AVAILABLE
Case 4Case 4
Patient presents complaining of Patient presents complaining of
Severe abdominal pain for 6 hoursEpisodes of vomitingHad noted some change in bowel habit over
the past 8 months
Case 4Case 4On Examination: T: 39.5oC Pulse: 95/min Tender in right lower quadrant of abdomen Rebound tenderness Absent bowel sounds Admit!!
Investigations: Blood Cultures FBC, U&E, ESR, CRP,Coag screen, Group and Hold X Ray abdomen(PFA)
Likely DiagnosisLikely Diagnosis
‘Acute Abdomen’
DiiferentialAppendicitisPeritonitis secondary to perforated ulcer,
large bowel neoplasm, diverticulitis, etc.

Likely DiagnosisLikely DiagnosisPFA

Likely DiagnosisLikely DiagnosisPFA
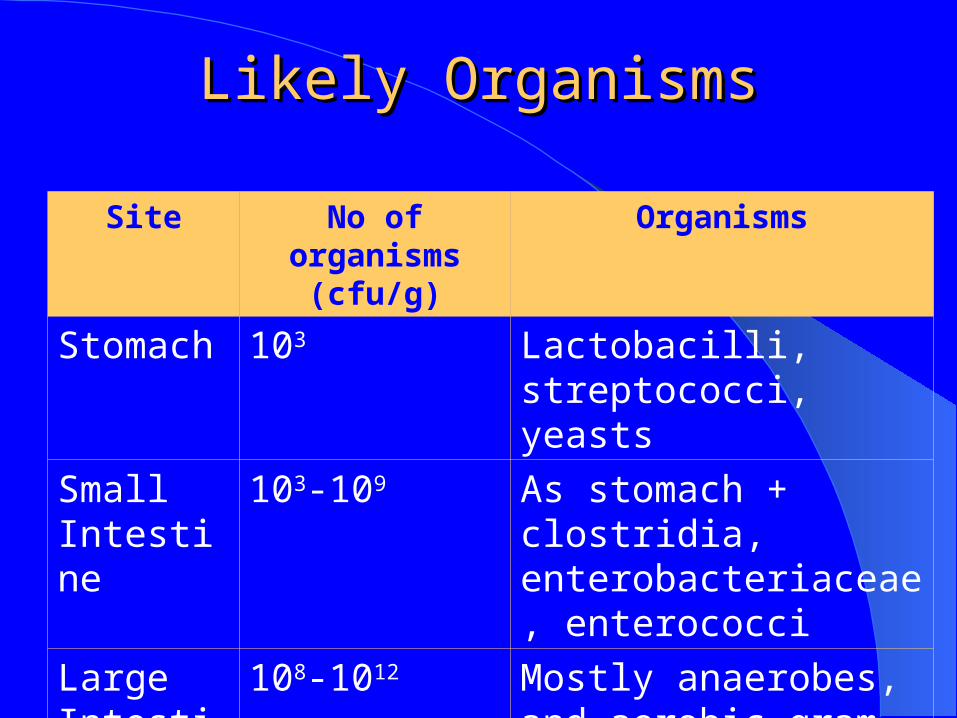
Likely OrganismsLikely Organisms
Site No of organisms (cfu/g)
Organisms
Stomach 103 Lactobacilli, streptococci, yeasts
Small Intestine
103-109 As stomach + clostridia, enterobacteriaceae, enterococci
Large Intestine
108-1012 Mostly anaerobes, and aerobic gram negatives and Enterococci
SurgerySurgery Taken to theatre for laparotomy Discover tumour in descending colon which has
perforated and has an associated abscess and peritonitis
Tumour removed with some difficulty, some pus spilled into peritoneum
section of colon removed and colostomy put in situ Pus sent for Culture and Sensitivity Antibiotics: IV Co-Amoxiclav+ Ciprofloxacin+
Metronidazole
Blood Cultures E. coli:
– S – Gentamicin, cefuroxime, ciprofloxacin– S Ampicillin, cephradine
Bacteroides fragilis– S – metronidazole
Swabs at surgery as above + enterococci spp. S Ampicillin
Admitted to ICU, improves over next few weeks but develops MRSA colonisation
CASE 5CASE 5
Case 5Case 5
Katie, 2 year oldPC: fever 38oC, Cough,HPC: x 4/7O/E: difficult to examine, irritable, noticed
white spots in mouth, some chest signsInv: FBC, U& E, CRP, ESR, CXR, swab
from lesions to microbiology

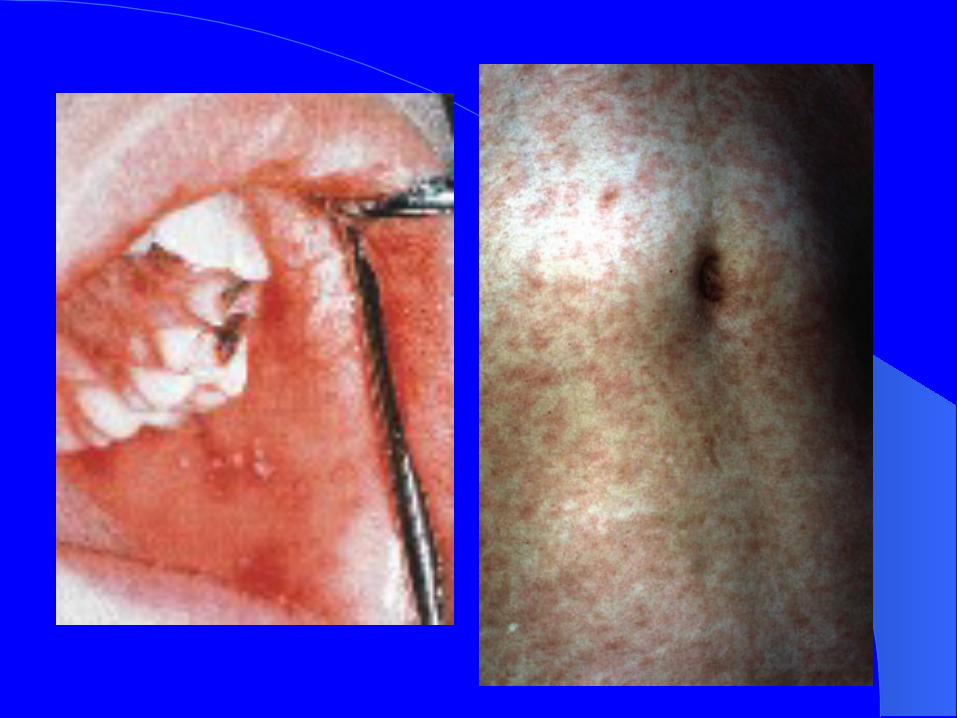
Later in the day, you notice Later in the day, you notice a rash appearing…a rash appearing…
Measles!!Measles!!
No Tx in children, supportive therapy
IsolateNotify to public healthVaccination is preventative
Case 6Case 6
Case 6Case 6
Brian, 63
•PC: ache and discharge from site of old fracture repair
•HPC: RTA 3/12 ago, femur fractured and screws inserted, wound infected with E. coli treated with Co-amoxyclav for 3/52

Case 6Case 6
PMHx: At time of RTA also had -
• subdural haematoma treated with burr hole
• 4 fractured ribs
• lacerated spleen requiring splenectomy
• Developed MRSA pneumonia in ICU

Case 6Case 6
• Social Hx: retired barrister, ex smoker, lost wife in same RTA
• Presently not an any antibiotics, no allergies
• O/E: T 38.5oC, pus from very tender tibial wound, nil else

Case 6Case 6
• Inv:
- FBC, U&E, CRP, ESR,
- X ray femur
- pus sent for culture and sensitivity
Would you admit this patient?
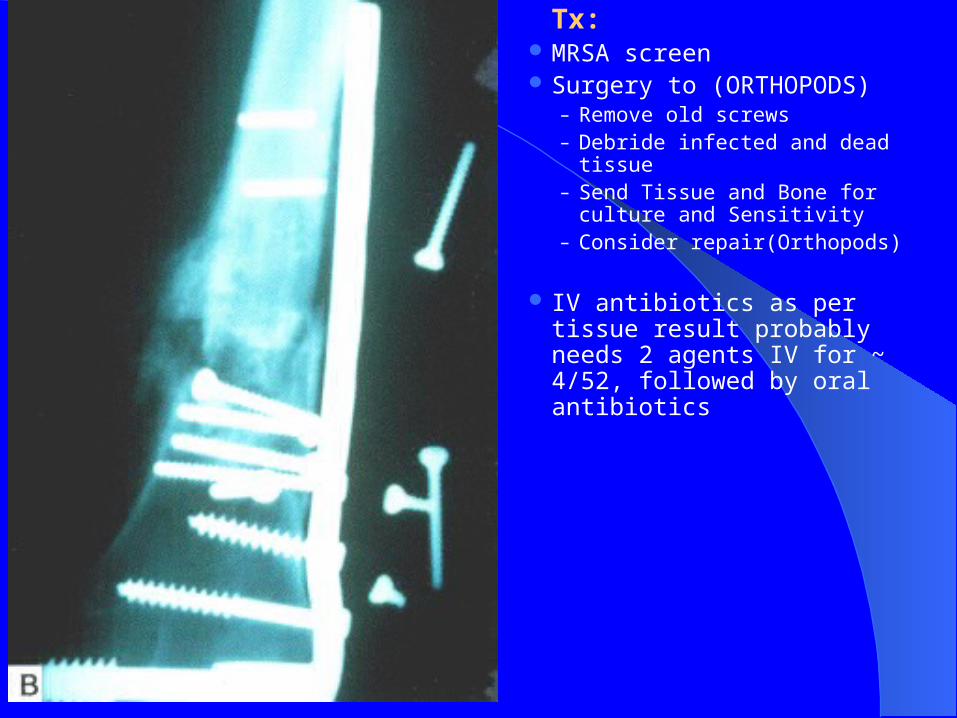
Tx: MRSA screen Surgery to (ORTHOPODS)
– Remove old screws– Debride infected and dead tissue– Send Tissue and Bone for culture
and Sensitivity– Consider repair(Orthopods)
IV antibiotics as per tissue result probably needs 2 agents IV for ~ 4/52, followed by oral antibiotics
Community Acquired Community Acquired PneumoniaPneumonia
Case 7Case 7
Presentation Presentation
72 year old previously fit gent retiredFamily have noted that he was distracted
over the past 4 days and forget his routine G.P appointment for Vit .B 12 injection
He is also catching his breath a lot
On examination-CURBOn examination-CURB
Confusion ( doesn`t know the day of the week or month)
RR 34 breaths per minutesBP 130/70 mmHgUrea has come back from the lab at 13
mmol/ L

Chest X-RAYChest X-RAY
Decision Decision
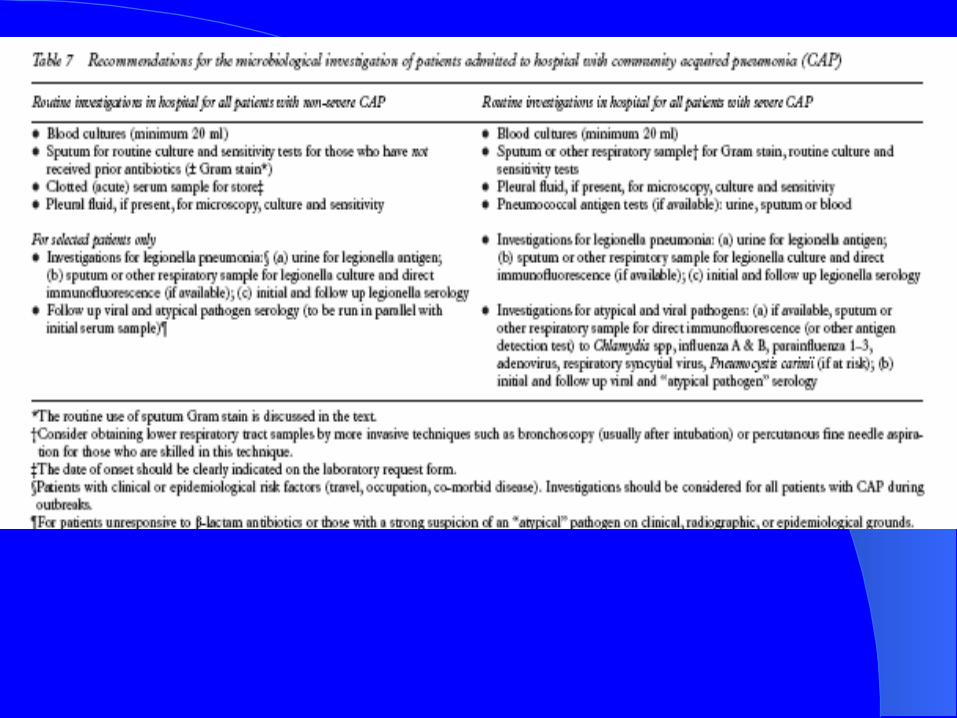
Do you admit this patient?What tests would you send to the
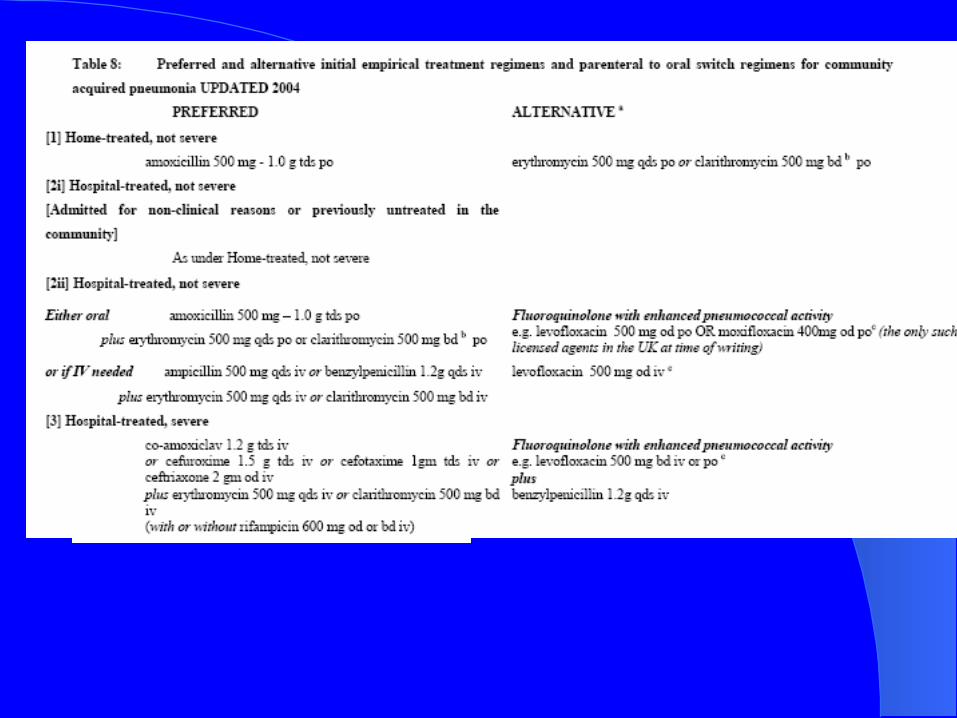
microbiology lab?What therapy do you choose?

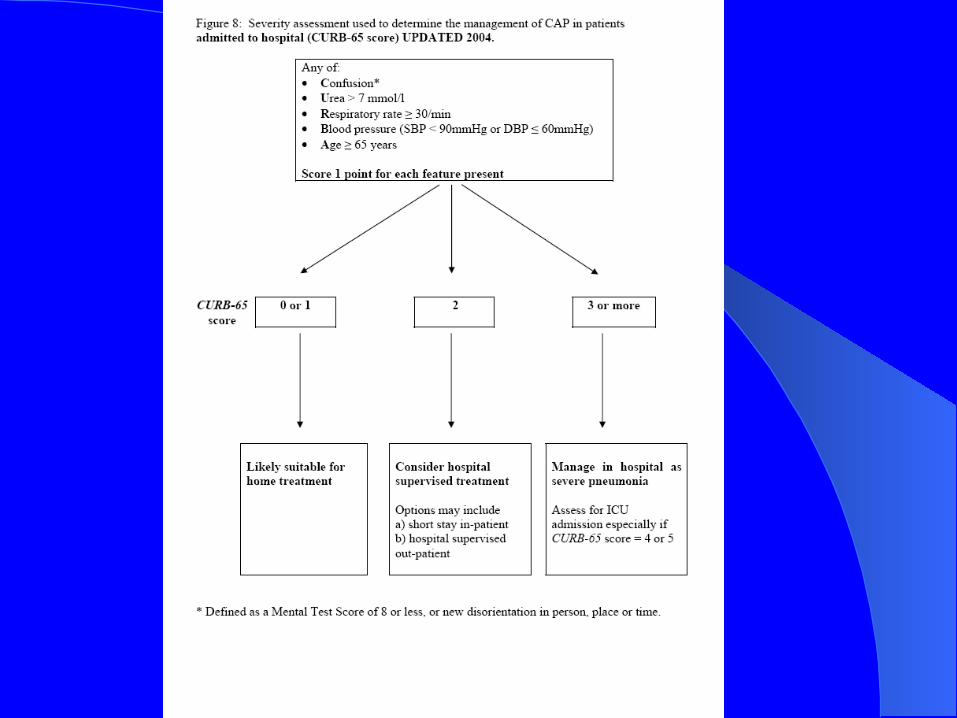
KEY POINT KEY POINT USE CURB-65 TO ACCESS :USE CURB-65 TO ACCESS :DETERMINES WHETHER TO DETERMINES WHETHER TO
ADMIT PATIENT AND ADMIT PATIENT AND THERAPYTHERAPY


















