Psychopharmacological treatment of neuropsychiatric symptoms
Upload
diego-catonCategory
view
216download
2
Increasing Uptake of Non-Pharmacologic
Approaches to Assess and Manage the Neuropsychiatric
Symptoms of DementiaHelen C. Kales MD
Professor of PsychiatryDirector, Section of Geriatric Psychiatry and
Program for Positive Aging University of MichiganResearch Investigator
VA GRECC, CCMR and SMITREC

Acknowledgements• H. Myra Kim, PhD• Claire Chiang, PhD• Janet Kavanagh, MS• Kara Zivin, PhD • Marcia Valenstein, MD• Francesca Cunningham,
PharmD• Lon S. Schneider, MD• Frederic C. Blow, PhD
• NIMH: R01MH081070
• There are no conflicts to disclose
• Laura Gitlin, PhD• Kostas Lyketsos, MD• NINR: R01NR014200
• Discussion of off-label uses of antipsychotics

Overview• Neuropsychiatric symptoms of
dementia (NPS) symptom description matters
• NPS etiology matters
• Non-pharmacologic management The DICE approach to assessment and
management

The Case of Elizabeth
• 81 year old with dementia
• Daughter called by in-home caregiver about “agitation”

Neuropsychiatric Symptoms of Dementia (NPS)
• Also known as behavioral and psychiatric symptoms of dementia (BPSD)
• Cognitive impairment is the clinical hallmark of dementia, but it is NPS that often dominate both presentation and course
• Present in >90% of patients with dementia at some point in illness course
Sources: Lyketsos et al, Am J Psychiatry, 2000; Sink et al, J Am Geriatrics Soc, 2004; Steffens et al, Am J Alzheimers Dis Other Dementias, 2005

Source: Rabheru (2004)

Miscellaneous but problematic behaviors
• unfriendliness• poor self-care• not paying attention or caring about what
is going on• repetitive verbalizations/questioning• wandering• “inappropriate” behaviors (screaming,
spitting, sexual behaviors)• sleep problems (day-night reversal)

Elizabeth’s “agitation”: further description would
help• Could be: Grumpiness Aggression Resistance Restlessness Anxiety Psychosis

Etiology• Not well understood• Likely heterogeneous
Cognitive loss Preexisting psychiatric illness Environmental factors Comorbid medical conditions Medications Pain Delirium
• Consequence of multiple concurrent factors

Elizabeth’s “agitation”: understanding possible
etiology would help• Could be:
Overstimulating environment Poor caregiver communication Pain Delirium Psychosis

How should we manage Elizabeth?
• Pharmacologic treatment:– In real-world settings,
a patient NPS will often receive an antipsychotic

Real-World Management• There is no FDA-approved
pharmacotherapy for NPS• Therefore, all use is off-label
Antipsychotics Benzodiazepines Mood stabilizers Antidepressants Cholinesterase inhibitors and
Sources: Kales et al, Am J Psychiatry 2007; Maust et al, Under review
% risk difference (CI) NNH(CI)Antidepressant Ref Ref
Haloperidol 9.4 (7.3 - 11.5)** 11 (9 -14)Olanzapine 5.2 (3.4 - 7.0)** 19 (14 - 29)Quetiapine 2.3 (1.3 - 3.4)** 43 (29 -77)Risperidone 4.5 (3.4 - 5.6)** 22 (18 - 29)Valproic acid 3.8 (1.5 - 6.2)** 26 (16 - 67)
Table 3. Adjusted¶ absolute risk differences between study medication users relative to antidepressant users (N=45,669)**p<0.01

The Role ofNon-pharmacologic
Management• Recommended by multiple medical organizations and expert groups as first-line for NPS *except in emergency situations when
behaviors could lead to imminent danger or compromise safety

Non-pharmacologic Management
• These interventions have not yet received widespread uptake
• Study of new nursing home admissions Only 12% received a non-pharmacologic
intervention >70% received >1 psychotropic 15% received >4 psychotropics
Source: Molinari et al, J Gerontol B Psychol Sci Soc Sci, 2010

Why are Non-pharmacologic Management Strategies
Underutilized?• Time• Training• Funding/reimbursement in current care
systems• Lack of guidelines• Symptoms are a moving target

Why are Non-pharmacologic Management Strategies
Underutilized?• ?Perception that they are unproven and/or unlikely to work, especially as compared to medications

Non-pharmacologic Management• What is it?:
Behavioral, environmental and caregiver interventions
• Examples: Caregiver education and support Activity Communication strategies Modifying the environment Acupuncture Aromatherapy Light therapy MassageSource: Gitlin, Kales, Lyketsos et al, JAMA2012

Non-pharmacologic Management
• Inconsistent to no evidence for: Reminiscence Aromatherapy Light Therapy Validation Therapy Simulated Presence Therapy
Source: Gitlin, Kales, Lyketsos et al, JAMA 2012

Non-pharmacologic Management• Brodaty meta-analysis of 23 RCTs with family
caregivers; outcomes related to frequency/severity of NPS and caregiver well-being Significant treatment effect, overall effect size=0.34 Variation among trials in dose, intensity and delivery mode Key features of successful trials=9-12 sessions; tailoring to
patient and caregiver; delivered in the home; multiple components
No adverse effects for any of the trials
• REACH II (generalized approach with targeted behavioral strategy) Problem solving behavioral approach with significant
reductions in frequency of behavioral symptoms• REACH VA (generalized approach with targeted behavioral
strategy) Significant reduction in problem behaviors (p=0.04) and
improvement in caregiver burden (p=0.001) and depression (p=0.009)
Source: Brodaty et al Am J Psychiatry 2012; Belle et al Ann Int Med 2006; Nichols et al Arch Int Med 2011

Non-pharmacologic Management
• Tailored Activity Program (TAP): 8-12 home/telephone sessions by occupational
therapists; caregiver training including customized activity
significant reductions in problem behaviors (p=0.004) including agitation (p=0.14) and decrease in caregiver “hours on duty” (p=0.001)
• COPE Up to 12 home/telephone contacts by health
professionals; assessment for underlying medical issues; caregiver training, significant reduction in problem behaviors (p=0.01) and improvement in caregiver well-being (p=0.002)
Source: Gitlin et al , Am J Geriatr Psychiatry 2008; Gitlin et al, ,JAMA, 2010

Project ACT• N=272 patients• 11 home/telephone sessions over 4-months by
health professionals• Identification of potential triggers of problem
behaviors Communication Environment Patient undiagnosed medical condition
• Caregiver training to modify triggers and reduce caregiver upset
• 3 booster contacts between 16-24 weeks
Source: Gitlin, et al, JAGS, 2010

Project ACT• Medical test results:
Undiagnosed illnesses detected in 34% of subjects
Most prevalent conditions:UTI 14.5%Hyperglycemia 5.9%Anemia 5.1%
Source: Gitlin, et al, JAGS, 2010

Project ACT
Source: Gitlin, et al, JAGS, 2010
Source: Gitlin, et al, JAGS, 2010

Project ACT
Source: Gitlin, et al, JAGS, 2010
• At 16 weeks: Patient improvement in 67.5% of
intervention dyads vs. 45.8% of control dyads (p=0.002)
Reduced caregiver upset (p=0.028) Enhanced confidence in managing
behaviors (p=0.011) Reduction in caregiver upset (p=0.001) Reduction in negative communication
(p=0.17) Improved caregiver well-being (p=0.001) Improvement in ability to keep patient at
home (p=0.001)• Similar outcomes at 24 weeks

Non-pharmacologic Management
• “If these interventions were drugs, it is hard to believe that they would not be on the fast track to approval. The magnitude of benefit and quality of evidence supporting these interventions exceed those of pharmacologic therapies…”
Covinsky , Annals of Internal Medicine 2006

Expert Consensus Panel• Convened in Detroit Michigan, September 7, 2011Faculty:• Mary G. Austrom, PhD Indiana University• Frederic C. Blow, PhD VA Ann Arbor/University of Michigan• Kathleen C. Buckwalter, PhD University of Iowa• Christopher M. Callahan, MD Indiana University• Ryan Carnahan Pharm.D., M.S. University of Iowa • Laura N. Gitlin, PhD Johns Hopkins University • Helen C. Kales, MD VA Ann Arbor/University of Michigan• Dimitris N. Kiosses, PhD Weill Cornell Medical College• Mark E. Kunik, MD VA Houston/Baylor College of Medicine• Constantine G. Lyketsos, MD Johns Hopkins University • Linda O. Nichols, PhD VA Memphis / University of Tennessee • Daniel Weintraub, MD VA Philadelphia/University of Pennsylvania

Panel Results• 1) Create an evidence-informed
approach representing best practice known to date
• 2) Construct an approach that can guide the use of both pharmacologic and non-pharmacologic approaches (roadmap)• Knee-jerk prescribing of meds is not
optimal• Going through the decision-making
steps to derive the treatments tailored to the patient, caregiver, environment is key

Panel Results• 3) We need better and more systematic
ways to differentiate symptoms by phenomena and putative causes.This may improve uptake of behavioral
and environmental modification approaches
This may better direct/target medication use
This will be of critical assistance to future medication trials

Panel Results• 4) Behavioral and environmental
modifications should be tried first-line with three major exceptions:Major depression with or without
suicidal ideationPsychosis causing harm or creating
potential for harmAggression causing risk
Emphasis on SAFETY and ACUITY

Etiology matters!• We don’t know what is prompting
Elizabeth’s symptoms• Knowing the underlying cause will direct
the treatment: Urinary tract infection
Pain
Issues with caregiver
Psychosis
??
??

Panel Results• 5) Definition of the key elements of care
for NPS:
Need accurate characterization and contextualization
Examine underlying causes of NPSDevise treatment planAssess intervention effectiveness
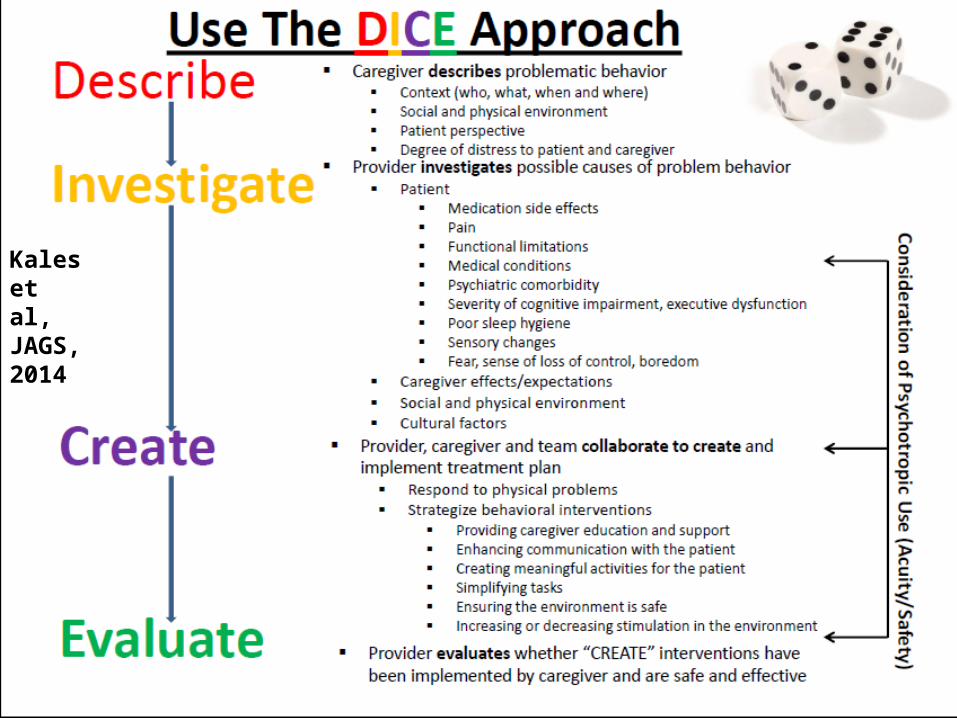
Kales et al, JAGS, 2014

The DICE Approach• Describ
e: Caregiver details the problematic behavior
Linkage of Describe Step with Patient/Caregiver/Environmental Considerations
Patient • What behavior did the patient exhibit (e.g. movie in my head)?
• How did the patient perceive what occurred?• How did the patient feel about it?• Is the patient’s safety at risk?
Caregiver • How much distress did the behavior generate for the caregiver?
• Does the caregiver feel their safety is threatened by the behavior?
• What about the behavior is distressing to the caregiver?• What did the caregiver do during and after the behavior
occurred?
Environment • Who was there when the behavior occurred (e.g. family members, unfamiliar people, etc.)?
• When did the behavior occur (time of day) and what relationship did this have to other events (e.g. occurring while bathing or at dinner)?
• Where did the behavior occur (e.g. home, daycare, restaurant, etc.)?
• What happened before and after the behavior occurred in the environment?

The DICE Approach
• InvestigateExamine possible underlying causes of the problematic behavior
Linkage of Investigate Step with Patient/Caregiver/Environmental Considerations
Patient • Recent changes in medications• Untreated or undertreated pain• Limitations in functional abilities• Medical conditions (e.g. urinary tract infection)• Underlying psychiatric comorbidity• Severity of cognitive impairment, executive impairment• Poor sleep hygiene• Sensory changes (vision, hearing)• Fear, sense of loss of control, boredom
Caregiver • Caregiver’s lack of understanding of dementia (e.g. patient is “doing this to” them “on purpose”)
• Caregiver’s negative communication style (e.g. overly critical or harsh, use of complex questions, too many choices)
• Caregiver’s expectations not aligned with dementia stage (under/over estimation of capability)
• Caregiver’s own stress/depression• Family/Cultural context (e.g. not wanting to involve
“outsiders” or “air dirty laundry”, promise to keep patient at home, etc)
Environment • Over- (e.g. clutter, noise, people) or under- (e.g. lack of visual cues, poor lighting) stimulating environment
• Difficulty navigating or finding way in environment• Lack of predictable routines that are comforting to patient• Lack of pleasurable activities tapping into preserved
capabilities and previous interests

The DICE Approach• Create:
Provider, caregiver and team collaborate to create and implement treatment plan
Linkage of Create Step with Patient/Caregiver/Environmental Considerations
Patient Respond to physical problems• Discontinue medications causing behavioral side effects
if possible• Manage pain• Treat infections, dehydration, constipation, etc.• Optimize regimen for underlying psychiatric conditions• Sleep hygiene measures• Deal with sensory impairments• Prescribe psychotropics if judged necessary
Caregiver Work collaboratively with caregiver/other team members to institute nonpharmacologic interventions including:• Providing caregiver education and support• Enhancing communication with patient• Creating meaningful activities for patient • Simplifying tasks
Environment Work collaboratively with caregiver/other team members to institute nonpharmacologic interventions including:• Ensuring the environment is safe• Simplifying/enhancing the environment

Kales et al, JAGS, 2014

Kales et al, JAGS, 2014
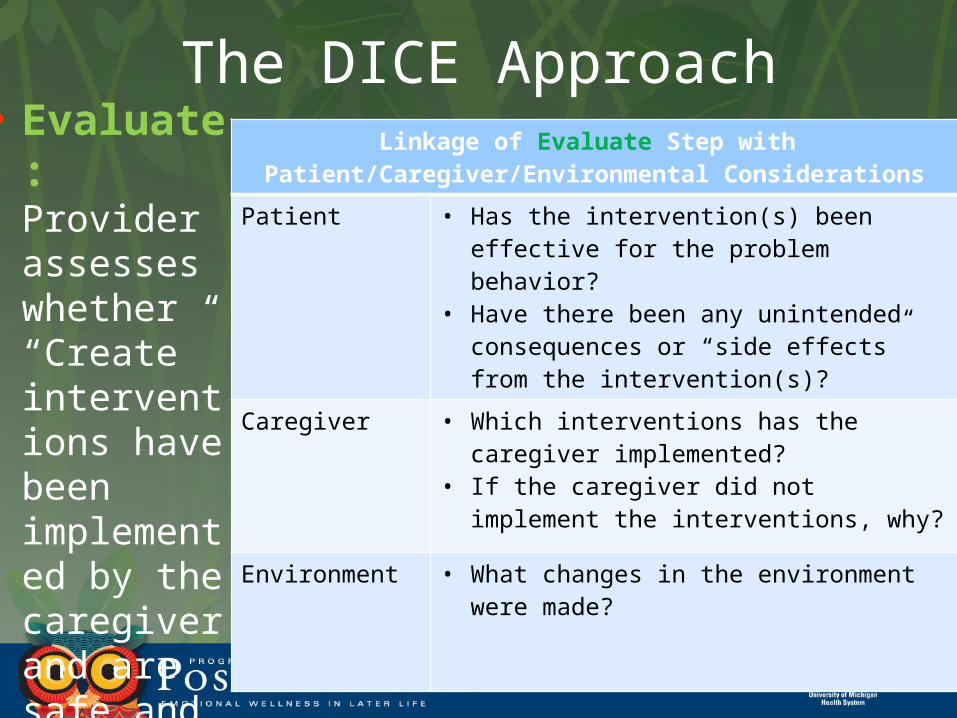
The DICE Approach• Evaluate
: Provider assesses whether “Create” interventions have been implemented by the caregiver and are safe and effective
Linkage of Evaluate Step with Patient/Caregiver/Environmental Considerations
Patient • Has the intervention(s) been effective for the problem behavior?
• Have there been any unintended consequences or “side effects” from the intervention(s)?
Caregiver • Which interventions has the caregiver implemented?
• If the caregiver did not implement the interventions, why?
Environment • What changes in the environment were made?

Using the DICE Approach with Elizabeth• Primary symptom is aggression with a particular
caregiver around ADLs like bathing; patient expresses that baths “hurt”; caregiver is not afraid for her safety but feels that the patient is “doing this on purpose”; there is no psychosis.
• Patient does have an underlying diagnosis of arthritis; she is currently not taking any medications for pain. She is unable to follow multi-step commands due to level of cognitive impairment. Caregiver has a lack of understanding of dementia and tone with patient when frustrated is somewhat harsh and confrontational.
• Consider starting standing pain medication, consider physical therapy. Educate caregiver about the “broken brain” and behavior. Address communication. Enhance bathing environment so that it is soothing and calm.
• Was pain medication effective? How has it impacted aggression around bathing? What of the caregiver/environmental interventions were tried?

The Place for Psychotropics in the DICE Approach
• Three first-line scenarios (major depression; psychosis or aggression with potential for harm)
• Medications as a temporizing measure for harmful behaviors while working up and treating the underlying causes
• Continued use may depend on symptom persistence and non-responsiveness to other treatment strategies
• Psychotropics are unlikely to impact: unfriendliness, poor self-care, memory problems, not paying attention or caring about what is going on, repetitive verbalizations/questioning, wandering

Testing and Implementing DICE
• NINR R01NR014200• Co-PI Gitlin• Co-I Lyketsos• 3.5 year grant to incorporate approach
into a tool using technology
• NIA Submission • Testing of DICE approach in primary care
with team social workers as interventionists

Summary• NPS are ubiquitous but remain often
under- or mistreated with an• Overreliance on medications • Underuse of non-pharmacologic strategies
with a substantial evidence base
• Symptom description and underlying etiology matter
• The DICE approach offers an evidence-informed structured method that is tailored, patient- and caregiver-centered and enables clinicians to conjointly consider pharmacologic, non-pharmacologic and medical treatments