Incomitant Squint
41
INCOMITANT SQUINT It is a type of hetrotropia (manifest squint) in which the amount of deviation varies in different directions of gaze.
-
Upload
shreeja-maheshwari -
Category
Documents
-
view
1.263 -
download
3
Transcript of Incomitant Squint
INCOMITANT SQUINTIt is a type of hetrotropia (manifest squint) in which the amount of deviation varies in different directions of gaze.
It includes following conditions:
1. Paralytic squint 2. A and V pattern hetrotropias 3. Restrictive Squint.
PARALYTIC STRABISMUSIt refers to ocular deviation resulting from complete or incomplete paralysis of one or more extraocular muscles.
ETIOLOGYI. Neurogenic lesions 1. Congenital 2. Inflammatory lesions 3.Neoplastic lesions 4. Vascular lesions 5. Traumatic lesions 6. Toxic lesions 7. Demyelinating lesions
II. Myogenic lesions 1.Congenital lesions 2. Inflammatory lesions 3. Traumatic lesions 4. Myopathies lesions III. Neuromuscular junction lesion Myasthenia gravis
CLINICAL FEATURES 1.DIPLOPIAIt may be horizontal, vertical or oblique depending on the muscle paralysed. Diplopia occurs due to formation of image on dissimilar points of the two retina.
2.Confusion. It occurs due to formation of image of two different objects on the corresponding points of retina. 3.Nausea and vertigo 4.Ocular deviation
SIGNS1.Primary Deviation:- It is deviation of the affected eye and is away from the action of paralysed muscle. 2.Secondary deviation:-It is deviation of the normal eye seen under cover, when the patient is made to fix with the squinting eye. IN PARALYTIC SQUINT IT IS GREATER THAN THE PRIMARY DEVIATION
Alternate cover testAllow the pt time to fixate on the target, give them a minute. Then quickly cover the other eye to prevent the pt from regaining fusion.
Exotropia, Constant May be visible with or without alternate cover Secondary deviation is more than primary deviation
3.Restriction of ocular movement:- It occurs in the direction of the action of paralysed muscles. 4.Comensatory head posture It is adopted to avoid diplopia and confusion. 5.False projection or Orientation:- It is due to incresed innervational impulse conveyed to the paralysed muscle.
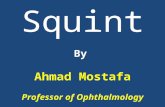
PAHTOLOGICAL SEQUELAE OF AN EXTRAOCULAR MUSCLE PALSYThese occur more in paralysis due to lesions of nerves than the lesions of muscles.These includes: 1.Overaction of the contralateral synergistic muscle. 2.Contracture of the direct antagonist muscle. 3.Secondary Inhibitional palsy of the contralateral antagonist muscle.
Overaction medial rectus Left Right
Primary paresis lateral rectus
Secondary palsy lateral rectus
Contracture medial rectus
PAHTOLOGICAL SEQUELAE OF RIGHT LATERAL RECTUS MUSCLE PALSY
CLINICAL VARIETIES OF OCULAR PALSIES1. ISOLATED MUSCLE PARALYSIS - (Lateral rectus and superior oblique most common) 2.PARALYSIS OF THIRD CRAINIAL NERVE Ptosis Deviation ( down, out and slightly intorted) Ocular movements restricted Pupil is fixed and dilated. Accomodation is completely lost Crossed diplopia
3.DOUBLE ELEVATOR PALSY - It is a congenital condition caused by third nerve nuclear lesion. Characterised by paresis of superior rectus and inferior oblique muscle of involved eye. 4.TOTAL OPHTHALMOPLEGIA Due to combined paralysis of 3rd, 4th & 6th cranial nerves as in orbital apex syndrome and cavernous sinus thrombosis. All extraocular muscles, including LPS & intraocular muscles, viz., sphincter pupillae and ciliary muscles are paralysed.
5. External ophthalmoplegia Due to lesion at the level of motor nuclei sparing the Edinger Westphal nucleus. 6. Intranuclear ophthalmoplegia Due to lesion of Medial longitudinal Bundle. Defective action of MR on the side of lesion Horizontal nystagmus of opposite eye Defective convergence
INVESTIGATIONS1. 2. 3. 4. 5. 6. 7. 8. 9. Every case of squint should be evaluated as previously mentioned. Inspection Ocular movements Pupillary reactions Fundus examination Refraction Direct cover test Alternate cover test Examination of angle of deviation Tests for the grade of binocular vision
ADDITIONAL TESTS1. Diplopia charting
Position and the separation of the two images in different fields in pt. with right lateral rectus palsy.
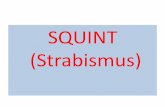
HESS SCREEN TEST
SR
IO
IO
SR
LR
MR
LR
IR
SO
SO
IR
3. Field of binocular fixation where applicable i.e., if pt. has some field of single vision. Using perimeter. 4. Forced duction test (FDT) INVESTIGATIONS TO FIND OUT THE CAUSE OF PARALYSIS ORBITAL USG ORBITAL AND SKULL CT SCANNING NEUROLOGICAL INVESTIGATIONS
DIFFERENCES BETWEEN PARALYTIC & NON-PARALYTIC SQUINTFEATURES PARALYTIC SQUINT NON-PARALYTIC SQUINT
Onset Diplopia Ocular Movements
Usually sudden Usually present Limited in the direction of action of paralysed muscle
Usually slow Usually absent Full
False Projection
Positive
Negative
Head Posture
Changed depending upon the muscle paralysed Present
Normal
Nausea & Vertigo
Absent
Secondary DeviationMore than the primary deviation
Equal to primary deviation Absent
Pathological Sequelae in the Muscles
Present
MANAGEMENT1. Treatment of the cause 2. Conservative measures Wait and watch for 6 months. Vitamin B complex Systemic steroids 3. Treatment of annoying diplopia Use of occluder on the affected eye, with intermittent use of both eyes with changed head posture to avoid suppression amblyopia. 4. Surgical treatment
A AND V PATTERN HETEROPHORIA It is labelled when the amount of deviation in squinting eye varies by more than 100 and 150 ,respectively, between upward and downward gaze. A AND V ESOTROPIA In A esotropia the amount of deviation increases in upward gaze & decreases in downward gaze. The reverse occur in V esotropia. A AND V EXOTROPIA In A exotropia the amount of deviation decreases in upward gaze & increases in downward gaze. The reverse occur in V exotropia. C/F It refers to vertically incomitant stabismus associated with horizontally concomitant strabismus
RESTRICTIVE SQUINTHere, the extraocular muscle is not paralysed but its movement is mechanically restricted. 1. Smaller primary deviation in proportion to limitation of movement 2. FDT positive CAUSES Duanes retraction syndrome Browns superior oblique tendon sheath syndrome Strabismus fixus Dysthyroid ophthalmopathy Incarceration of extraocular muscle in blow out fracture of the orbit.
1. Duanes restriction syndrome It is a congenital motility defect occuring due to fibrous tightening of lateral or medial or both rectus muscle. Limitation of abduction ( Type I ) or adduction (Type II ) or both (Type III ). Retraction of globe and narrowing of palpabral fissure on attempted adduction. Eye in primary position may be orthotropic, esotropic or exotropic 2. Brown superior oblique tendon sheath syndrome - It is a congenital motility defect due to fibrous tightening of superior oblique tendon. Limitation of elevation of the eye in adduction ( positive FDT) 3. Strabismus fixus- Bilateral fixation of eyes in convergent position due to fibrous tightening of the medial recti.
STRABISMU S SURGERY
Strabismus surgery is surgery on the extraocular muscles to correct the misalignment of the eyes. Eye muscle surgeries typically correct strabismus and include the following: Loosening / weakening procedures Recession involves moving the insertion of a muscle posteriorly towards its origin. Myectomy Myotomy Tenectomy Tenotomy
Tightening / strengthening procedures Resection involves detaching one of the eye muscles, removing a portion of the muscle from the distal end of the muscle and reattaching the muscle to the eye. Tucking Advancement is the movement of an eye muscle from its original place of attachment on the eyeball to a more forward position. Transposition / repositioning procedures Adjustable suture surgery is a method of reattaching an extraocular muscle by means of a stitch that can be shortened or lengthened within the first post-operative day, to obtain better ocular alignment. Posterior fixation suture (FADEN OPERATION ) to correct dissociated vertical deviation. Transplantation of muscles in paralytic squint.
Indications: The most common indications for surgical treatment of strabismus include: Development or restoration of normal binocularity: nearnormal alignment is a prerequisite for development of binocular vision and stereopsis. Alignment before two years of age allows the greatest chance for binocularity in children with congenital strabismus. Functional benefits of binocularity include stereopsis, expanded binocular visual fields and prevention of amblyopia. Treatment of diplopia Restoration of normal facial appearance Treatment of abnormal head posture, mainly that related to an abnormality of ocular alignment
Surgical Techniques: the muscles can be reached through a limbal or a fornix-based approach. The four recti insertions merge into the sclera; the average insertion distances from the limbus are: medial rectus 5.5mm inferior rectus 6.5mm lateral rectus 6.9mm superior rectus 7.7mm Type and amount of muscle surgery : It depends upon the type and angle of squint, age of the patient, duration of squint and visual status. o o 1 mm resection of MR will correct about 1 -1.5 (Max. 8mm) o o 1 mm recession of MR will correct about 2 -2.5 (Max. 5.5mm) o o 1 mm resection and recession of LR will correct about 1 -2 (Max. 10 and 8mm)
How much to operate
20
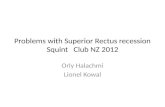
Alternate Cover test with Prism Exotropia, Constant Use prism to quantitate the deviation. Change prism power until movement is neutralized. Use this number to plan surgery
How much to operate?How much to operate Tables: Dosages (surgical) bilat , 2 muscles ie for ET 40PD recess 5.5mm both MR ET XT PD Rec Rst Rec Resect 15 3 3 4 2.5 20 3.5 4 5 3 25 4 5 6 4 30 4.5 6 7 5 35 5 7 7.5 5.5 40 5.5 7.5 8 6 50 6 8 9* 7 60 6.5 8.5 10* 8
Personal experience
STEPS OF RECESSION
STEPS OF RESECTION
RESECTION
Complications and Risks of surgery Infection (1 in 3 years ) Nausea (Tx: Phenergan, etc.) Blood loss Loss of sight? (globe perforation) Scar tissue Diplopia Residual or consecutive strabismus due to overcorrection and undercorrection Oculo-Cardiac Reflex Bradycardia Lost and slipped muscles Anterior segment ischemia: Much of the anterior segment circulation derives from ciliary arteries which are affected by surgery involving the extraocular muscles. This occasionally leads to a peculiar complication called anterior segment ischemia manifesting with a significant anterior chamber reaction, iris atrophy, and various degrees of cataract formation. Conjunctival granulomas and cysts