Incision design in implant dentistry based on vascularization of the mucosa

of 6
-
Upload
alexandre-khairallah -
Category
Documents
-
view
224 -
download
0
Transcript of Incision design in implant dentistry based on vascularization of the mucosa
-
8/11/2019 Incision design in implant dentistry based on vascularization of the mucosa
1/6
Incision design in implant dentistrybased on vascularization of the mucosa
Johannes KleinheinzAndreBuchter
Birgit Kruse-LoslerDieter Weingart
Ulrich Joos
Authors affiliations:Johannes Kleinheinz, AndreBuchter, Birgit Kruse-Losler, Ulrich Joos, Department of Cranio-Maxillofacial Surgery, University of Muenster,Muenster, GermanyDieter Weingart, Department of Maxillofacial andPlastic Surgery, Katharinenhospital, Stuttgart,Germany
Correspondence to:Johannes Kleinheinz
Department of Cranio-Maxillofacial SurgeryUniversity of Muenster Waldeyerstr.30 D-48149 MuensterGermanyTel.: 49 251 834 7003Fax: 49 251 834 7184e-mail: [email protected]
Key words: implant dentistry, incision design, supply area, vascularization
Abstract
Objectives: The delivery of an adequate amount of blood to the tissue capillaries for
normal functioning of the organ is the primary purpose of the vascular system. Preserving
the viability of the soft tissue segment depends on the soft tissue incision being properly
designed in order to prevent impairment of the circulation. A knowledge of the course of
the vessels as well as of their supply area are crucial to the decision of the incision. The aim
of this study was to visualize the course of the arteries using different techniques, to
perform macroscopic- and microscopic analyses, and to develop recommendations for
incisions in implant dentistry.
Material and methods: The vascular systems of seven edentulous human cadavers were
flushed out and filled with either red-colored rubber bond or Indian ink and formalin
mixture. After fixation a macroscopic preparation was performed to reveal the course,
distribution and supply area of the major vessels. In the area of the edentulous alveolar
ridge specimens of the mucosa were taken and analyzed microscopically.
Results: The analyses revealed the major features of mucosal vascularization. The main
course of the supplying arteries is from posterior to anterior, main vessels run parallel to the
alveolar ridge in the vestibulum and the crestal area of the edentulous alveolar ridge is
covered by a avascular zone with no anastomoses crossing the alveolar ridge.
Conclusion: The results suggest midline incisions on the alveolar ridge, marginal incisions in
dentated areas, releasing incisions only at the anterior border of the entire incision line,
and avoidance of incisions crossing the alveolar ridge.
Surgical disciplines are always confronted
with the problem of cutting and therefore
damaging healthy soft tissue in order togain access to the area of interest in the
human body. While the access require-
ments have not changed over time, the
incision techniques have changed (e.g. la-
ser (Mausberg et al. 1993; Bryant et al.
1998), electrosurgical knife (Mausberg
et al. 1993; Sinha & Gallagher 2003),
water scalpel (Siegert 2000) and piezosur-
gery (Shelley & Shelley 1986). Irrespective
of the applied technique, the surgical access
must provide for:
(1) optimal visualization of the key area;
(2) problem-free expansion of the soft tissue;
(3) mobilization of the overlying soft tis-sue to cover the surgical field;
(4) no placement over bony defects or
cavities;
(5) sufficient vascularization of soft tissue;
(6) minimum tissue damage;
(7) assured wound healing;
(8) minimum esthetic impairment and
(9) good tissue covering.
Mucosal closure has to protect the bone,
the implant or the augmentation material,Copyrightr Blackwell Munksgaard 2005
Date:Accepted 24 November 2004
To cite this article:
Kleinheinz J, Buchter A, Kruse-Losler B, Weingart D,Joos U. Incision design in implant dentistry based onvascularization of the mucosa.Clin. Oral Impl. Res.16, 2005; 518523doi: 10.1111/j.1600-0501.2005.01158.x
518
-
8/11/2019 Incision design in implant dentistry based on vascularization of the mucosa
2/6
to establish a connection to the local supply
systems as soon as possible, and to avoid
infections or dehiscences.
The consequences of any incision must
always be kept in mind. Unlike embryolo-
gical wound healing, where scarless healing
is possible (Gary & Longaker 2000), any
planned incision or injury of the covering
soft tissue after birth will result in scarring
which differs from regular skin or mucosa
in terms of esthetics, functioning or nutri-
tion and may be a weak point in the future.
Among many factors, vascularization has
proved to be decisive for any kind of tissue
regeneration (Arnold & West 1991; End-
rich & Menger 2000). Growth, maturation
or reconstruction of the body are conceiva-
ble without unimpaired vascularization
(Folkman & Shing 1992). A knowledge of
the course and of the supply area of the
arteries is the basis for selection of theappropriate incision.
The aim of this study was to establish
recommendations for incisions, based on
reliable knowledge of the distribution pat-
terns and course of the vascular system in
the oral mucosa.
Material and methods
Two different techniques were used to
demonstrate the macro- and micro-archi-
tecture of the arterial vascular system in
seven edentulous human cadavers.
A separate description of the venous
system was not undertaken because it
follows the arterial pathways in most parts
of the body.
Vascular corrosion cast
A total of 150 ml of red-colored rubber
bond (MR Givuls Revultex, Heinrich
Wagner, Boblingen, Germany) was injected
into the external carotid arteries on both
sides after flushing out the vascular system
with streptolysin solution at a pressure of
200 mm Hg. The head was then immer-
sion-fixed. This technique allows the de-
monstration and macroscopic evaluation of
vessels ranging from small calibres upto a
diameter of 200mm. After solidification of
the elastic substance, the specimens were
frozen and cut in medio-sagittal direction.
The vascular system of the maxilla and
mandible was transected in the vestibular
and palatal/lingual planes. The course of
the vessels and their relationship to adja-
cent anatomic structures and tissues were
documented in layers.
Indian ink injection
In a second attempt 4 ml of colored Indian
ink and formalin (4%) mixture were in-
jected into the facial, lingual and maxillaryarteries after flushing out the vascular sys-
tem with streptolysin solution passing
through the capillary plexus. The colored
areas of the mucosa were inspected, photo-
graphed and resected in the edentulous area
of the alveolar ridge. After cleaning of
the specimens according to the method of
(Spalteholz 1911) microscopic evaluation
of the microvascularization was carried
out.
Macroscopic evaluation
Following macroscopic preparation, single
arteries were identified and their position
and relationship to adjacent structures and
their course from the exit from the bone up
to the capillary system were described. The
ink-stained areas of the mucosa were as-
sessed with respect to their extent and
borders and were assigned as a supply area
to one of the injected arteries.
Microscopic evaluation
The mucosa of the edentulous alveolar
ridge was evaluated microscopically with
respect to the distribution and orientation
of vessels. Special emphasis was placed on
the crestal area where vestibular and oral
parts of the mucosa are in direct contact.
Results
After preparation, the color-marked main
vessels were identified and their course and
relationship to other tissues and structures
described (Fig. 1). After dissolution of
the surrounding soft tissue the vessels were
demonstrated directly on the underlying
bony surface (Fig. 2). The points of exit
from the foramen and the anastomoses to
other vessels were shown. The results of all
cases are summarized in Fig. 3.
Vascular territories of the maxilla (Fig. 4)
In the posterior part of the maxilla the
vestibular gingiva was supplied by branches
of the infraorbital artery, and the palatal
mucosa by branches of the descending
palatine artery. Anteriorly, in the area of
the premaxilla, the supply was based on the
facial artery regarding the vestibular parts
Fig.1 . Course of main arteries in the maxilla after macroscopic preparation. Vessels filled with rubberbond can
easily be identified.
Fig.2 . After dissolution of soft tissue the relation of vessels and bone is demonstrated.
Kleinheinz et al . Incisions in implant dentistry
519 | Clin. Oral Impl. Res.16, 2005 / 518523
-
8/11/2019 Incision design in implant dentistry based on vascularization of the mucosa
3/6
and partially on the infraorbital artery. In
66% palatal parts were supported by the
descending palatine artery and in 33% by
the anterior superior alveolar artery.
Vascular territories of the mandible (Fig. 5)
The posterior lateral part of the alveolar
ridge was supplied by the facial artery, and
the anterior part by the inferior labial artery
and in 50% additionally by the mental
artery. In 73% of the cases the lingual
mucosa was supported exclusively by the
submental artery and in 27% additionally
by the sublingual artery. Regarding the
lingual supply there were overlappings of
both sides, whereas overlapping was found
in 20% of the cases in the vestibular part
covered by the facial artery.
Crossing area on the edentulous alveolarridge (Fig. 6a, b)
A visible vestibularoral separation line
between the two supply areas at the center
of the edentulous segments was demon-
strated in edentulous spaces, free-end situa-
tions and totally edentulous jaws.
Microscopic evaluation of the alveolarmucosa (Fig. 7a, b)
The demonstrated gingival branches are
arterioles or capillaries, which have the
characteristics not of end-arteries but of
net-arteries with numerous anastomoses.
There is an almost avascular zone in the
crestal area of the edentulous alveolar ridge.
The descriptions can be summarized intothree main vascularization characteristics:
(1) The main course of the supplying
arteries is from posterior to anterior.
(2) These vessels run parallel to the al-
veolar ridge in the vestibulum most
of the time, only gingival branches
stretch to the alveolar ridge.
(3) The crestal area of the edentulous
alveolar ridge is covered by a 12 mm
wide avascular zone with no anasto-
moses crossing the alveolar ridge.
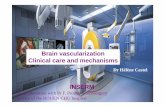
Recommendations for the incision(Fig. 8 ad)
Because of divergent dentitions and, es-
thetic zones, as well as different parts of
the gingiva (marginal, propria, mucosa) it is
necessary to define and distinguish differ-
ent parts of the incision line. The three
decisive areas are:
the crestal part of the edentulous re-
gion,
the bordering papilla in cases of par-
tially dentated jaws, the area of the releasing incision at
the anterior and posterior limit of the
incision.
The midcrestal incision seems to be the
ideal choice for the edentulous area of the
planned implantation. Making the cut in
the area of the avascular zone prevents the
risk of cutting through anastomoses or
cutting out avascular areas of the mucosa.
Fig.3 . Overview after macroscopic preparation of the arteries in the maxilla and mandible. The main courses,
distributions and relations are demonstrated.
Fig.4 . Vascular territories of the maxilla. The colorsshow the supply areas of different arteries: blue
infraorbital artery, red descending palatine artery,
black facial and infraorbital arteries, green
descending palatine and anterior superior alveolar
arteries.
Fig.5 . Vascular territories of the mandible. The
colours show the supply areas of different arteries:
blue facial artery, red submental and sublingual
arteries, black inferior labial and mental arteries.
Fig.6 . After Indian ink injection a vascular separation line is visible in the center of the edentulous alveolar
ridge.
Kleinheinz et al . Incisions in implant dentistry
520 | Clin. Oral Impl. Res.16, 2005 / 518523
-
8/11/2019 Incision design in implant dentistry based on vascularization of the mucosa
4/6
For esthetic reasons, only marginal inci-
sions should be used in the frontal region.
Releasing incisions in the vestibulum
should be avoided because they will cut
obliquely through defined esthetic zones
and not at their borders. Releasing inci-
sions should be carried out, if at all, only at
the anterior border of the incision line to
avoid cutting through the vessels coming
from posterior to anterior. Trapezoid flaps
with anterior and posterior releasing inci-
sions are avoidable in most cases because
the surgical field can be adequately visua-
lized, and mobilization using incising of
the periosteum can be achieved by anterior
incision only.
If it is essential not to touch the marginal
mucosa, an incision in the vestibulum
parallel to the alveolar ridge with tunneling
preparation is recommended.
The papilla will be included in the inci-
sion in the anterior maxilla and recon-
structed using microsurgical techniques
during preparation and wound closure. In
the lateral or posterior segment or in the
event of a single posterior tooth in a free-
end situation the papilla can be left un-
touched by making the releasing incision
in front of the papilla.
Discussion
The different factors to be taken into ac-
count when planning a mucosal incision
include esthetic aspects, plastic-reconstruc-
tion potential and blood-supply require-
ments. In a defect situation, the focus is
on criteria relating to plastic reconstruction
(e.g. preparation and mobilization of local
flaps for coverage or reconstruction pur-
poses). Most flap preparation limitations
are because of inadequacy of the supporting
vascular system.
Esthetic aspects play a decisive role,
especially in the anterior part of the max-
illa. It is essential to make an incision onlyat the border of esthetic zones or areas and
to avoid damaging, displacement or redu-
cing local tissue, because any substitute
tissue is distinctive in its color, consis-
tency, and surface structure.
Among all planning principles, the vas-
cular-nutritive principle seems to be the
most important one. The vascular system
at the margin of a wound represents the
most important nutritional structure for
survival and the basis for reliable wound
healing and therefore must not be damagedunder any circumstances (Arnold & West
1991; Endrich & Menger 2000; Filippi
2001).
Consideration of the vessels involved in
any soft tissue incision should be based on
the extent and boundaries of the areas of
supply of single major vessels. The ana-
tomic principle of the vascular territories
referred to in the literature under the
term angiosomes (Taylor & Palmer 1987;
Houseman et al. 2000). Evaluations of the
vascularization of specific areas of the oral
mucosa have also been carried out (Kin-
dlova & Scheinin 1968; Mormann & Cian-
cio 1977; Piehslinger et al. 1991; Bavitz
et al. 1994; Kerdvongbundit et al. 2003)
but only few studies have referred to total
assessment and a subdivision into angio-
somes (Whetzel & Saunders 1997).
In agreement with the results of other
study groups, the midcrestal incision in the
edentulous area of the alveolar ridge seems
to be indisputably the safest and most
reliable method (Scharf & Tarnow 1993;
Fig.7 . The histologic section of the alveolar mucosa shows a main arterial vessel and the gingival ramification
in thelateral aspectof thealveolarmucosa (a). The avascular zone is in themiddle of the alveolar ridge. There is
only one anastomosis running over the midline (b).
Fig.8 . Recommendations for the incision (a) edentulous areas, (b) edentulous areas: tunneling preparation, (c)
free-end situation and (d) single tooth gap.
Kleinheinz et al . Incisions in implant dentistry
521 | Clin. Oral Impl. Res.16, 2005 / 518523
-
8/11/2019 Incision design in implant dentistry based on vascularization of the mucosa
5/6
Cranin et al. 1998; Heydenrijk et al. 2000).
Incisions, which will repeatedly cross the
alveolar ridge will create small mucosal
areas with uncertain vascularization, lead-
ing to disturbed wound healing, bone re-
sorption and mucosal necrosis.
If the covering soft tissue has to be
extended, e.g., in cases of lateral or vertical
augmentation, this can be achieved with a
periosteal incision and broad undermining
mobilization.
The creation of a trapezoid flap with an
anterior and posterior releasing incision can
be avoided in cases without the necessity of
extended coverage of augmented sites be-
cause sufficient visualization and mobili-
zation can also be achieved using one single
releasing incision. To prevent accidental
cutting into the vessels running from pos-
terior to anterior in the jaws, it seems
appropriate to place the releasing incisionat the anterior border of the midcrestal
incision.
The inclusion of the papilla adjacent to
the edentulous area is controversially de-
bated. Reports of shrinkage and loss of
interproximal bone have led to recommen-
dations for parapapillary incisions (line an-
gle to line angle) (Gomez-Roman 2001;
Velvart 2002). These alternatives, designed
for primary preserving of the papilla, will
not allow unrestricted visualization of the
lateral marginal bone and the adjacenttooth. In the event of augmentation, lateral
mobilization of the gingiva is almost im-
possible.
The marginal incision including the pa-
pilla allows a complete overview of the
entire edentulous alveolar ridge and exact
placement of the implant equidistant from
the neighboring teeth. This incision is
recommended especially for esthetically
problematic areas in the upper incisor re-
gion (Wachtel et al. 2003; Erpenstein et al.
2004). Using microsurgical techniques for
preparation of flaps and reconstruction of
the papilla (Burkhardt & Hurzeler 2000),
shrinkage can be avoided when the under-
lying alveolar bone is not reduced and the
contact point of the prosthodontic treat-
ment is not too far from the alveolar bone
(Tarnow et al. 2003).
From angiologic aspects the papilla is
different from the adjacent edentulous al-
veolar mucosa because the papilla is sup-
plied by vascular anastomoses crossing the
alveolar ridge. This key point allows differ-
ent incisions including or excluding the
papilla. The decision has to be made indivi-
dually, with aspects of esthetics and plastic
reconstruction being taken into account.
Resume
Fournir une quantiteadequate de sang auxcapillaires
pour un fonctionnement normal de lorgane est le
but premier du systeme vasculaire. Preserver la
viabilitedu segment de tissu mou depend de linci-
sion du tissu mou qui doit etre effectuee de maniere
precise pour prevenir la deterioration de la circula-
tion. Une connaissance de geographie des vaisseaux
ainsi que de leurs aires de reserve sont essentiels
pour la decision de lincision. Le but de cette etude a
etede visualiser les arteres en utilisant differentes
techniques afin deffectuer des analyses tant
macro- que microscopiques et pour developper des
recommandations pour les incisions lors de la pose
dimplants dentaires. Les systemes vasculaires de
sept cadavres humains edente
s ont e
te
vide
s etremplis avec soit de lencre de Chine ou unesolution
rouge et du formol. Apres fixation une preparation
macroscopique a ete effectuee pour mettre en evi-
dence le cours, la distribution et laire de reserve des
principaux vaisseaux. Dans la zone du rebord al-
veoaire edentedes specimens des muqueuses ont ete
preleves et analyses microscopiquement. Les ana-
lyses ont mis en evidence les principaux caracteres
de la vascularisation de la muqueuse. Le cours
principal des arteres converge de larriere vers
lavant, les vaisseaux principaux courent parallele-
ment au rebord alveolaire dans le vestibule et laire
crestale des rebords alveolaires edentes et sont cou-
verts parune zone non-vascularisee sans anastomose
traversant le rebord alveolaire. Ces resultats sugger-ent donc des incisions au milieu de la ligne du rebord
alveolaire, des incisions marginales dans les zones
dentees, des incisions dacces seulement dans la
frontiere anterieure de la ligne dincision generale et
labstention dincision traversant la crete alveolaire.
Zusammenfassung
Die Gestaltung der Inzision in der dentalen
Implantologie aufgrund der Vaskularisierung der
Mukosa
Ziele: Das erste Ziel des Gefasssystems ist es, eine
adaquate Menge Blut zu den Kapillaren zu fuhren,
um eine normale Funktion des Organs zu gewahr-
leisten. Der Erhalt der Lebensfahigkeit des Weich-
teilsegments hangt von der Weichgewebsinzision ab,
welche sauber gestaltet sein sollte, um die Zirkula-
tion nicht zu beeintrachtigen. Die Kenntnis des
Verlaufs und der Versorgungsgebiete der Gefasse ist
fur die Wahl der Inzision entscheidend. Das Ziel
dieser Studie war, den Verlauf der Arterien mittels
verschiedener Techniken sichtbar zu machen, um
makroskopische und mikroskopische Analysen
durchfuhren zu konnen und um Empfehlungen fur
Inzisionen in der oralen Implantatchirurgie zu en-
twickeln.
Material und Methoden: Das Gefasssystem von 7
zahnlosen menschlichen Kadavern wurde ausge-
spult und entweder mit rot gefarbter Gummiflus-
sigkeit oder mit indischer Tinte und einer
Formalinmixtur aufgefullt. Nach der Fixierung
wurde eine makroskopische Praparation durchge-
fuhrt, um den Verlauf, die Verteilung und die Ver-
sorgungsgebiete der grossen Gefasse aufzuzeigen. Im
Bereich des zahnlosen Alveolarkammes wurden
Proben der Mukosa entnommen und mikroskopischanalysiert.
Resultate: Die Analysen zeigten die generellen Ei-
genschaften der Vaskularisation von Schleimhauten.
Die Hauptrichtung der versorgenden Gefasse ver-
lauft von posterior nach anterior, die Hauptgefasse
liegen parallel zum Alveolarkamm im Vestibulum
und die Kammregion des zahnlosen Alveolar-
kammes wird durch eine avaskulare Zone ohne
den Alveolarkamm uberkreuzende Anastomosen
bedeckt.
Schlussfolgerung: Aufgrund der Resultate werden
Inzisionen im Bereich der Kammmitte des zahnlo-
sen Alveolarkammes und marginale Inzisionen
im bezahnten Bereich vorgeschlagen. Entlastungssch-
nitte sollten nur an der anterioren Grenze der
gesamten Inzisionslinie gelegt werden. Inzisionen,
welche den Alveolarkamm uberkreuzen, sollten
vermieden werden.
Resumen
Objetivos: El suministro de una cantidad adecuada
de sangre a los capilares tisulares para el funciona-
miento normal de un organo es el proposito primario
del sistema vascular. La preservacion de la viabilidad
del segmento de tejido blando depende en la incision
del tejido blando que debe estar debidamente disen-
ada en orden a prevenir mermas en la circulacion.
Un conocimiento del curso de los vasos al igual que
del areade suministro es crucial para la decisiondela
incision. La intencion de este estudio fue visualizar
el curso de las arterias usando diferentes tecnicas,
para realizar analisis macro- y microscopicos, y
desarrollar recomendaciones para incisiones en
odontologa de implantes.
Material y metodos: Se vaciaron los sistemas vas-
culares de 7 cadaveres humanos edentulos y relle-
nados con pegamento de goma de color rojo o con
una mezcla de tinta india y formalina. Tras la
fijacion se llevoa cabo una preparacion macrosco-
pica para revelar el curso, distribucion y area de
suministro de los vasos principales. En el area de la
cresta alveolar edentula se tomaron especmenes y
se analizaron microscopicamente.
Resultados: Los analisis revelaron las principales
caractersticas de la vascularizacion mucosa. El
curso principal de las arterias de suministro as desde
posterior a anterior, los vasos principales corren
paralelos a la cresta alveolar en el vestbulo y el
area crestal de la cresta alveolar esta cubierta por una
zona avascular sin anastomosis que crucen la cresta
alveolar.
Conclusion: Los resultados sugieren incisiones en la
cresta alveolar, incisiones marginales en areas den-
tadas, incisiones liberadoras solo en el borde anterior
de la lnea completa de incision, y evitar las inci-
siones que crucen la cresta alveolar.
Kleinheinz et al . Incisions in implant dentistry
522 | Clin. Oral Impl. Res.16, 2005 / 518523
-
8/11/2019 Incision design in implant dentistry based on vascularization of the mucosa
6/6
References
Arnold, F. & West, D. (1991) Angiogenesis in
wound healing. Pharmacology and Therapeutics
52: 407422.
Bavitz, J., Harn, S. & Homze, E. (1994) Arterial
supply of the floor of the mouth and lingual
gingiva.Oral Surgery Oral Medicine Oral Pathol-
ogy Oral Radiology and Endodontics 77:
232235.
Bryant, G.L., Davidson, J.M., Ossoff, R.H., Garret,
C.G. & Reinisch, L. (1998) Histologic study oforal mucosa wound healing: a comparison of a
6.0- to 6.8-mm pulsed laser and a carbon dioxide
laser. Laryngoscope 108: 1317.
Burkhardt, R. & Hurzeler, M.B. (2000) Utilization
of the surgical microscope for advanced plastic
periodontal surgery. Practical Periodontics and
Aesthetic Dentistry12: 171180.
Cranin, A.N., Sirakian, A., Russell, D. & Klein, M.
(1998) The role of incision design and location in
the healing processes of alveolar ridges and im-
plant host sites. International Journal of Oral &
Maxillofacial Implants13: 483491.
Endrich, B. & Menger, M.D. (2000) Regeneration
der Mikrozirkulation wahrend der Wundheilung?
Unfallchirurg 103: 10061008.Erpenstein, H., Rasperini, G. & Silvestri, M.
(2004) Lappenoperationen. In: Erpenstein, H. &
Diedrich, P., eds. Atlas der Parodontalchirurgie.
1st edition, 111. Munchen: Elsevier Urban&
Fischer.
Filippi, A. (2001) Wundheilung der mundschleim-
haut. Deutsche Zahnarztliche Zeitschrift 56:
517522.
Folkman, J. & Shing, Y. (1992) Angiogenesis. Jour-
nal of Biological Chemistry267: 1093110934.
Gary, H.G. & Longaker, M.T. (2000) Scarless
Wound Healing. New York: Dekker.
Gomez-Roman, G. (2001) Influence of flap design
on peri-implant interproximal crestal bone loss
around single-tooth implants. International Jour-
nal of Oral & Maxillofacial Implants16: 6167.
Heydenrijk, K., Raghoebar, G.M., Batenburg, R.H.
& Stegenga, B. (2000) A comparison of labial and
crestal incisions for the 1-stage placement of IMZ
implants: a pilot study. Journal of Oral & Max-
illofacial Surgery58: 11191123.
Houseman, N.D., Taylor, G.I. & Pan, W.R. (2000)The angiosomes of the head and neck: anatomic
study and clinical applications. Plastic and Re-
constructive Surgery105: 22872313.
Kerdvongbundit, V., Vongsavan, N., Soo-ampon, S.
& Hasegawa, A. (2003) Microcirculation and
micromorphology of healthy and inflamed gingi-
vae.Odontology91: 1925.
Kindlova, M. & Scheinin, A. (1968) The vascular
supply of the gingiva and the alveolar mucosa
in the rat. II. Spontaneous and experimentally
induced changes of the microcirculation. Acta
Odontologica Scandinavica26: 629640.
Mausberg, R., Visser, H., Aschoff, T., Donath, K. &
Kruger, W. (1993) Histology of laser- and high-
frequencyelectrosurgical incisions in the palateof pigs. Journal of Craniomaxillofacial Surgery
21: 130132.
Mormann, W. & Ciancio, S.G. (1977) Blood supply
of human gingiva following periodontal surgery.
Journal of Periodontology48: 681692.
Piehslinger, E., Choueki, A., Choueki-Guttenbrun-
ner, K. & Lembacher, H. (1991) Arterial supply of
the oral mucosa.Acta Anatomica 142: 374378.
Scharf, D. & Tarnow, D. (1993) The effect of crestal
versus mucobuccal incisions on the rate of im-
plant osseointegration. International Journal of
Oral & Maxillofacial Implants 8: 187190.
Shelley, E.D. & Shelley, W.B. (1986) Piezosurgery:
a conservative approach to encapsulated skin le-
sions. Cutis 38: 123126.
Siegert, R. (2000) Wasserstrahldissektion in der par-
otischirurgie erste klinische resultate. Laryngo-
Rhino-Otologie79: 780784.
Sinha, U.K. & Gallagher, L.A. (2003) Effects of steel
scalpel, ultrasonic scalpel, CO2 laser, and monopolar
and bipolar electrosurgery on wound healing in
guinea pigoralmucosa. Laryngoscope 113: 228236.Spalteholz, W. (1911) Uber Das Durchsichtigma-
chen Von Menschlichen Und Tierischen Prapar-
aten. Leipzig: Hirzel.
Tarnow, D.T., Elian, N., Fletcher, P., Froum, S.,
Magner, A., Cho, S.C., Salama, M., Salama, H. &
Garber, D.A. (2003) Vertical distance from the
crest of bone to the height of the interproximal
papilla between adjacent implants. Journal of
Periodontology74: 17851788.
Taylor, G.I. & Palmer, J.H. (1987) The vascular
territories (angiosomes) of the body: experimental
study and clinical applications. British Journal of
Plastic Surgery40: 113141.
Velvart, P. (2002) Papilla base incision: a new
approach to recession free healing of the interden-tal papilla after endodontic surgery. International
Endodontic Journal 35: 453460.
Wachtel, H., Schenk, G., Bohm, S., Wenig, D.,
Zuhr, O. & Hurzeler, M.B. (2003) Microsurgical
access flap and enamel matrix derivative for the
treatment of periodontal intrabony defects: a con-
trolled clinical study. Journal of Clinical Perio-
dontology30: 496504.
Whetzel, T.P. & Saunders, C.J. (1997) Arterial
anatomy of the oral cavity: an analysis of the
vascular territories. Plastic and Reconstructive
Surgery100: 582587.
Kleinheinz et al . Incisions in implant dentistry
523 | Clin. Oral Impl. Res.16, 2005 / 518523