In The Right Words: Addressing Language and Culture in ... · language access, including examples...
54
IN THE RIGHT WORDS: Addressing Language and Culture in Providing Health Care ISSUE BRIEF NO . 18 AUGUST 2003 BASED ON A GRANTMAKERS IN HEALTH ISSUE DIALOGUE SAN FRANCISCO , CA
Transcript of In The Right Words: Addressing Language and Culture in ... · language access, including examples...

IN THE RIGHTWORDS:
Addressing Language andCulture in ProvidingHealth Care
I S S U E B R I E F N O . 1 8
A U G U S T 2 0 0 3
B A S E D O N A
G R A N T M A K E R S
I N H E A L T H
I S S U E D I A L O G U E
S A N F R A N C I S C O , C A

I S S U E B R I E F N O . 1 8
A U G U S T 2 0 0 3
B A S E D O N A
G R A N T M A K E R S
I N H E A L T H
I S S U E D I A L O G U E
S A N F R A N C I S C O , C A© 2003 Grantmakers In Health. All materials in thisreport are protected by U.S. copyright law. Permissionfrom Grantmakers In Health is required to redistributethis information, either in print or electronically.
This publication is available on-line at www.gih.org.
IN THE RIGHTWORDS:
Addressing Language andCulture in ProvidingHealth Care


G R A N T M A K E R S I N H E A L T H iii
advancing research; and roles forfoundations in supporting improvedlanguage access, including examples ofcurrent activities.
The Issue Dialogue focused mainly onactivities and programs that ensurelinguistic access to health care for allpatients. Although language and cultureare clearly inseparable, a full exploration of the field of cultural competence andinitiatives that promote its application tothe health care setting are beyond the scopeof this Issue Brief. The day’s discussion did,however, raise provocative issues of culturethat are reflected throughout this report.
Special thanks are due to those who partici-pated in the Issue Dialogue, but especiallyto presenters and discussants: Ignatius Bau,J.D., program officer at The CaliforniaEndowment; Maria-Paz Beltran Avery,Ph.D., senior project director at theEducation Development Center; AliceChen, M.D., M.P.H., Soros PhysicianAdvocacy Fellow at the Asian and PacificIslander American Health Forum; PamelaDickson, M.B.A., senior program officer at The Robert Wood Johnson Foundation;Maren Grainger-Monsen, M.D., directorof the bioethics in film program atStanford University’s Center forBiomedical Ethics; Carola Green, programcoordinator at Vista Community Clinic;Timothy Henderson, M.A., vice presidentfor programs at Quantum Foundation,Inc.; Terry Hernandez, program officer atMid-Iowa Health Foundation; VivianHuang, M.H.S., senior policy analyst atthe California Primary Care Association;
As part of its continuing mission to servetrustees, executives, and staff of healthfoundations and corporate givingprograms, Grantmakers In Health (GIH)convened a group of experts fromphilanthropy, research, health care practice,and policy on April 4, 2003, to discuss theroles of language and culture in providingeffective health care. During this IssueDialogue, In the Right Words: AddressingLanguage and Culture in Providing HealthCare, health grantmakers and experts frompolicy and practice participated in an openexchange of ideas and perspectives onlanguage access and heard from fellowgrantmakers who are funding innovativeprograms in this area. Together theyexplored ways to effectively supportcomprehensive language services, includingthe use of interpreters and translation ofwritten materials.
This Issue Brief synthesizes key points fromthe day’s discussion with a backgroundpaper previously prepared for IssueDialogue participants. It focuses on thechallenges and opportunities involved withensuring language access for the growingnumber of people who require it. Sectionsinclude: recent immigration trends anddemographic changes; the effect oflanguage barriers on health outcomes andhealth care processes; laws and policiesregarding the provision of language servicesto patients, including an overview of publicfinancing mechanisms; strategies forimproving language access, includingenhancing access in delivery settings,promoting advocacy and policy change,improving interpreter training, and
Foreword
G R A N T M A K E R S I N H E A L T H iii

Lindsay Josephs, program specialist atEndowment for Health; Kelvin Quan,J.D., M.P.H., chief financial officer andgeneral counsel at the Alameda Alliance forHealth; and Mara Youdelman, J.D.,LL.M., staff attorney at the NationalHealth Law Program.
Rea Pañares, M.H.S., program associate atGIH, planned the program and wrote thisreport with editorial assistance from Anne
Schwartz, Ph.D., vice president of GIH,and Angela Saunders, communicationsmanager at GIH. Judy Frabrotta ofFrabotta Company also contributed to thisreport. Lauren LeRoy, Ph.D., president andCEO of GIH, moderated the IssueDialogue and provided editorial assistance.
This program was made possible by grantsfrom The California Endowment and TheRobert Wood Johnson Foundation.
iv I N T H E R I G H T W O R D S

Grantmakers In Health (GIH) is anonprofit, educational organizationdedicated to helping foundations andcorporate giving programs improve thenation’s health. Its mission is to fostercommunication and collaboration amonggrantmakers and others and to helpstrengthen the grantmaking community’sknowledge, skills, and effectiveness. GIH is known today as the professional homefor health grantmakers and a resource forgrantmakers and others seeking expertiseand information on the field of health philanthropy.
GIH generates and disseminatesinformation about health issues andgrantmaking strategies that work in healthby offering issue-focused forums,workshops, and large annual meetings;publications; continuing education andtraining; technical assistance; consultationon programmatic and operational issues;and by conducting studies of health philan-thropy. Additionally, the organizationbrokers professional relationships andconnects health grantmakers with eachother, as well as with others whose workhas important implications for health. It also develops targeted programs andactivities and provides customized serviceson request to individual funders. Coreprograms include:
• Resource Center on HealthPhilanthropy. The Resource Centermonitors the activities of healthgrantmakers and synthesizes lessonslearned from their work. At its heart arestaff with backgrounds in philanthropyand health whose expertise can helpgrantmakers get the information theyneed and an electronic database thatassists them in this effort.
• The Support Center for HealthFoundations. Established in 1997 torespond to the needs of the growingnumber of foundations formed fromconversions of nonprofit hospitals andhealth plans, the Support Center nowprovides hands-on training, strategicguidance, and customized programs onfoundation operations to organizations at any stage of development.
• Building Bridges with Policymakers.GIH helps grantmakers understand theimportance of policy to their work andthe roles they can play in informing andshaping public policy. It also works toenhance policymakers’ understanding of health philanthropy and identifiesopportunities for collaboration betweenphilanthropy and government.
GIH is a 501(c)(3) organization, receivingcore and program support from more than200 foundations and corporate givingprograms each year.
About
G R A N T M A K E R S I N H E A L T H v

vi I N T H E R I G H T W O R D S
GIH is committed to promoting diversity andcultural competency in its programming,personnel and employment practices, and gov-ernance. It views diversity as a fundamentalelement of social justice and integral to itsmission of helping grantmakers improve thenation’s health. Diverse voices and viewpointsdeepen our understanding of differences inhealth outcomes and health care delivery, andstrengthen our ability to fashion just solutions.
GIH uses the term, diversity, broadly toencompass both differences in the attributesof individuals (such as race, ethnicity, age,gender, sexual orientation, physical ability,religion, and socioeconomic status) and oforganizations (foundations and givingprograms of differing sizes, missions,geographic locations, and approaches tograntmaking).
Diversity Statement

Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Changing Demographics, Changing Needs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Health Consequences of Language Barriers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
More Than Words: The Role of Culture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Laws and Policies for Ensuring Language Access . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Strategies for Improving Language Access in the Health Care Setting . . . . . . . . . . . . . . . . . . .16
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .39
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .41
G R A N T M A K E R S I N H E A L T H vii
Table of Contents


G R A N T M A K E R S I N H E A L T H 1
IntroductionMutual understanding between providersand patients is essential for achievingsatisfactory health care outcomes.Physicians must be able to obtain anaccurate reading of the patient’s symptomsand medical history, and patients must beable to grasp the nature of their conditionand the recommended course of treatment.Often, life-altering decisions regardingtreatment alternatives must be based solelyon information about risks and benefitscommunicated in the span of a brief officevisit. Even for those who are fluent inEnglish and acculturated to the Americanmedical system, the complexity of informa-tion coupled with the emotion and anxietyof illness creates substantial opportunitiesfor miscommunication. Under even thebest of conditions, patients may havequestions and concerns they find difficultto put into words, or misconceptions thatlead to tragic consequences. For thegrowing millions of people living in thiscountry with limited English proficiency,and for the providers who care for them,linguistic and cultural barriers canrepresent additional and enormousobstacles to good medical care.
The growth in immigrant populations andthe corresponding rise in language diversityin the U.S. have raised concerns about theability of the nation’s health care system tocare for all patients appropriately. Whilethe use of professional interpreters in othersettings such as international diplomacyand law is standard, professional medicalinterpreters are still a luxury in most healthcare settings (Chen 2003). Providers andcommunities are struggling with how toaddress the needs of populations with
diverse languages and distinct culturalperceptions of health. Public policy and private efforts from nonprofitorganizations, health care systems, andfoundations have made some progress inconfronting these problems and providingresources for action, but more remains tobe done. Foundations can play animportant role in helping ensure that allpatients have access to linguistically andculturally appropriate health care services.
ChangingDemographics,Changing Needs The U.S. experienced 13 percentpopulation growth between 1990 and2000. During this period, the nationbecame more racially and ethnicallydiverse, with declines in the non-Hispanicwhite population and increases in theHispanic, non-Hispanic black, and Asianand Pacific Islander populations (Andruliset al. 2003). In large part, growing diversitywas fueled by the rise in the nation’sforeign-born population, which increased44 percent during this time period to 28.4million people. In 2000, the foreign-bornpopulation comprised 10 percent of thetotal population, its highest proportionsince 1930 (U.S. Census Bureau 2002c).
Growth in the foreign-born population hasled to the increase in the nation’s languagediversity. Over 300 different languages arespoken in the U.S., and nearly 47 millionpeople (almost 18 percent of the nation’spopulation) speak a language other thanEnglish at home (Figure 1). Spanish is, byfar, the most common foreign languagespoken in the U.S. Spanish-speakers alone
“Imagine pulling in a
member of the custodial
staff to help you deal with
the nuances of an
international business deal.
You can’t.”
ALICE CHEN,
ASIAN AND PACIFIC
ISLANDER AMERICAN
HEALTH FORUM

2 I N T H E R I G H T W O R D S
Figure 1. Languages Spoken at Home in the United States
Language Number Percentage*
Language other than English 46,951,595 17.9
Spanish or Spanish Creole 28,101,052 10.7
Chinese 2,022,143 0.8
French (including Patois and Cajun) 1,643,838 0.6
German 1,383,442 0.5
Tagalog 1,224,241 0.5
Vietnamese 1,009,627 0.4
Italian 1,008,370 0.4
Korean 894,063 0.3
Russian 706,242 0.3
Polish 667,414 0.3
Arabic 614,582 0.2
Portuguese or Portuguese Creole 564,630 0.2
Japanese 477,997 0.2
French Creole 453,368 0.2
Other Indic languages 439,289 0.2
African languages 418,505 0.2
Other Asian languages 398,434 0.2
Greek 365,436 0.1
Other Indo-European languages 327,946 0.1
Hindi 317,057 0.1
Other Pacific Island languages 313,841 0.1
Persian 312,085 0.1
Other Slavic languages 301,079 0.1
Urdu 262,900 0.1
Other West Germanic languages 251,135 0.1
Gujarathi 235,988 0.1
Serbo-Croatian 233,865 0.1
Other Native North American languages 203,466 0.1
Armenian 202,708 0.1
Hebrew 195,374 0.1
Mon-Khmer, Cambodian 181,889 0.1
Yiddish 178,945 0.1
Navajo 178,014 0.1
Miao, Hmong 168,063 0.1
Scandinavian languages 162,252 0.1
Laotian 149,303 0.1
Other and unspecified languages 144,575 0.1
Thai 120,464 0.0
Hungarian 117,973 0.0* All percentages are approximate.
Source: U.S. Census Bureau 2003b.

G R A N T M A K E R S I N H E A L T H 3
increased by 43 percent between 1990 and2000, now comprising almost 11 percentof the total population. Over 21 millionindividuals self-report their ability to speakEnglish as less than “very well” (U.S.Census Bureau 2003a). These individualsare often referred to as limited Englishproficient (LEP), defined in the context ofthe health care setting as “a person who isunable to speak, read, write, or understandthe English language at a level that permitshim/her to interact effectively with healthand social service agencies and providers”(Office of Civil Rights 2002).
Foreign-born residents and associated LEPpopulations are concentrated in certainparts of the country (Figure 2). In fivestates, the foreign-born population rateexceeds the national average of 10 percent:California (26 percent), New York (20
percent), Florida (18 percent), New Jersey(15 percent), and Texas (12 percent).Moreover, half of the foreign-bornpopulation is concentrated in fivemetropolitan areas: Los Angeles, New York,San Francisco, Miami, and Chicago (U.S.Census Bureau 2002c). In California, 40percent of its population speaks a languageother than English at home, and in someareas the percentage is even greater; forexample, in the Santa Ana/Anaheim area,67 percent speak a language other thanEnglish at home. Miami/Hialeah leads thenation’s largest cities with the highestpercentage of its population that speaks a language other than English at home at 82 percent; and 37 percent ofMiami/Hialeah’s city population reportsnot speaking English well or at all(Andrulis et al. 2003).
Figure 2. Percentage of Population with Limited English Proficiency, 2000
Percent of State LEP Population■ 10% and above (9 states)■ 5% – 9.9% (11 states)■ 2.5% – 4.9% (15 states)� Less than 2.5% (16 states)Source: Chen 2003.

4 I N T H E R I G H T W O R D S
The composition of the nation’s foreign-born population is also changing. Since1970, the number of immigrants fromEurope has steadily declined, whereaspopulations from Latin American and Asia have both increased (Figure 4) (U.S.Census Bureau 2002c). Latin Americancountries constituted half of the foreign-born population, with countries such asMexico, Cuba, El Salvador, and theDominican Republic leading the way. Infact, Mexico alone accounted for over halfof the foreign-born population from thisregion and more than one-quarter of thetotal immigrant population (U.S. CensusBureau 2002a). Immigration from Asiannations comprised 26 percent of theforeign-born population and wasdistributed relatively evenly among the five largest contributors: China, thePhilippines, India, Vietnam, and Korea(U.S. Census Bureau 2002b).
While the highest foreign-born populationrates are concentrated in California, Texas,and northeastern metropolitan areas, thegreatest rates of growth occurred in theSouth and Midwest, with many cities experiencing triple-digit increases between1990 and 2000 (Figure 3). During thisperiod, Augusta, Georgia experienced thelargest growth, with a 766 percent increasein its foreign-born population. The threelargest cities in North Carolina (Raleigh,Greensboro, and Charlotte) had increasesin their Hispanic population well over 450 percent. Grand Rapids, Michigan andDes Moines, Iowa also saw high rates offoreign-born growth at 167 percent and151 percent, respectively (Andrulis et al.2003). These changes present significantchallenges for health and other socialprograms as policymakers andcommunities struggle with how to servethis influx of newcomers.
Figure 3. Growth in Limited English Proficiency, 1990-2000 (Percentage)
Source: Chen 2003.
Percent Growth of State LEP Population■ Greater than 100% (15 states)■ 50% – 99% (14 states)■ 0% – 49% (18 states)� Decline in LEP Population (4 states)

G R A N T M A K E R S I N H E A L T H 5
Broadly categorizing immigrants accordingto the continent or even the country oftheir birth does not tell the whole story oflinguistic and cultural diversity. Significantvariations exist within categories withrespect to primary language, religiousbeliefs, and cultural practices. Although theprimary language of most Latin Americancountries is Spanish, each Asian countryhas a different national language andmultiple dialects. In the Philippines, forexample, over 70 different dialects arespoken, even though the national languageis Tagalog. Furthermore, individualcountries or subgroups within countriesmay have specific health beliefs andpractices that are not broadly shared.Traditional Mexican culture, for example,includes the “hot-cold” theory of disease,where illnesses, food, and medicines areclassified as hot or cold. Prevention ortreatment is then based on restoring thehot-cold balance, where “hot” diseases aretreated with “cold” foods and vice versa.This practice is not common in other Latin American countries (Families USAFoundation 1995).
HealthConsequences ofLanguage BarriersA consistent body of research points to the extent of language barriers in healthcare settings and its implications for health.Moreover, the personal stories of those whohave encountered these barriers illustratethe reality of the system. The following sections describe the ramifications of poorlinguistic access, including: decreasedaccess to health services, compromisedpatient comprehension, low patientsatisfaction, reduced quality of care, and an increase in health care costs.
AccessLanguage barriers have been shown toimpede access at several entry points, fromhaving health insurance to receiving basicand preventive care to accessing specialtyservices. In a study of the effect of Englishlanguage proficiency on enrollment ofMedicaid-eligible children in publicly
Other areas
Asia
Latin America
Europe
2000199019801970
10
9
19
9
19
33
26
7
4451
26
8
1523
39
62
Figure 4. Foreign-Born Population by Region of Birth: 1970 to 2000 (Percentage)
Source: U.S. Census Bureau 2002c.

6 I N T H E R I G H T W O R D S
comparing LEP versus English-speakingAsian and Hispanic patients foundsignificantly worse reports of care on multiple domains, including timeliness of care, provider communication, staffhelpfulness, and plan service (Weech-Maldonado et al. 2001). Oftentimes,satisfaction with care at a particularinstitution determines whether a patient will return for subsequent care at the sameinstitution, if given a choice (Chen 2003).
Quality of CareLanguage barriers diminish quality of careand can lead to serious complications andadverse clinical outcomes. One studyfound that patients with a language barrierwere more likely to have self-reportedoutpatient drug complications. They werealso more likely to have a number of othermedical problems, such hospitalizationsand lower medication compliance. When aprescribing physician is unable tocommunicate effectively with his/herpatient, serious side effects may occur if anaccurate history is not taken (Ghandi et al.2000).
Costs to the Health CareSystemLanguage barriers can escalate costs to the health care system by increasinginefficiencies and unnecessary testing.When treating LEP patients, providersoften order additional tests and othercostly, and sometimes invasive, proceduresfor fear of missing a diagnosis when a goodhistory would have sufficed. The practice isso common it has come to be characterizedas “veterinary medicine.” In the absence of verbal communication, test results,visual assessment of symptoms, and hand
funded health insurance programs, mostfamilies with eligible children reported notknowing eligibility guidelines and difficultytranslating enrollment forms as reasons fornot enrolling in the program (Feinberg etal. 2002). In a nationwide telephone studyof insured adults, Spanish-speaking Latinoswere significantly less likely than non-Latino whites to have had a physician visit,flu shot, or mammogram in the precedingyear. To isolate the role of language, non-Latino whites were then compared toEnglish-speaking Latinos. No difference in utilization was found, which points tolanguage as the driving force for thisdisparity in access to preventive services(Fiscella et al. 2002).
Patient ComprehensionOnce LEP patients get into the system,language barriers may compromisecomprehension of diagnosis, treatmentinstructions, and plans for follow-up care(Crane 1997). At the same time, languageconcordance —when the physician andpatient speak the same language —hasbeen associated with better patient self-reported physical functioning,psychological well-being, and healthperceptions, as well as lower pain (Perez-Stable et al. 1997).
Patient SatisfactionPatients are more satisfied when they haveaccess to a trained and qualified interpreter.In one study, 32 percent of those whoneeded an interpreter, but did not get one,said they would not return to the hospitalif they became insured, while only 9percent of those who did receive aninterpreter said they would not return(Andrulis et al. 2002). Another study

G R A N T M A K E R S I N H E A L T H 7
A Closer Look at Language Barriers
A Vietnamese-speaking patient is unable to schedule a follow-up appointment for anabnormal mammogram because the receptionist speaks only English. As a result,treatment and necessary procedures are delayed.
A Chinese-speaking woman visits her primary care physician complaining of a mass in herwrist. Luckily, this physician is able to speak the patient’s language and communicateeffectively. She is referred for a biopsy and returns to the same physician several weekslater for a follow-up appointment. The patient tells her physician that the surgery was performed, but she did not know what the surgeon found. She also mentions that shewas prescribed medications, but has stopped taking them because she felt fine. Herphysician examines the bottles and discovers the medications are for tuberculosis. Thepatient was not aware of this diagnosis. More alarming, she was not aware the diseasecould be spread easily to others and that effective treatment includes taking hermedications for one year.
A Mien-speaking man with chronic hepatitis is referred to a gastroenterologist for a biopsyof his liver. Through a Mien interpreter, he reported back to the referring physician thathe was yelled at by a staff member for not bringing his own interpreter. After multiplefrustrating encounters, he asked to be referred to another doctor, a bold act for someonewhose culture does not normally allow for questioning of a physician’s authority.
A patient presenting with shortness of breath that was attributed to hyperventilation afteran earthquake was later found to have diabetic ketoacidosis, a severe complication ofdiabetes requiring aggressive treatment to avoid coma or death. Language problemsprevented a discussion of the patient’s history.
A call from the mother and sister of a Spanish-speaking man reported that he was “intoxicado.” Paramedics and the hospital personnel incorrectly interpreted this asintoxicated or drunk and, therefore, left him alone, offering no treatment. It turned outthe man was actually having a stroke, and this mistake resulted in him being paralyzed.After settling out of court, the health care institution was required to pay $71 million.
A Spanish-speaking patient presenting chest pain, unrelated to coronary artery disease, isscheduled for multiple unnecessary diagnostic procedures, due to the inability of themedical team to get a good history.

8 I N T H E R I G H T W O R D S
More Than Words:The Role of Culture Language access is only part of the answerin effectively addressing the health careneeds of the LEP population. Culture playsa critical role in an individual’s approach tohealth and healthy living. Cultures vary inperceptions of illness and their causes;beliefs with respect to health, healing, andwellness; adoption of health behaviors; andattitudes toward the health care system(National Center for Cultural Competence1999). Consider the example of an elderly,first-generation Laotian man who wasprescribed four teaspoons a day of an oralantibiotic. Although the gentleman wasable to get his prescription filled, when apublic health nurse visited his home, sherealized he was not taking his prescribedmedicine because he had no idea what ateaspoon was; he had only used chopsticksand large soup spoons (Families USAFoundation 1995). Hmong cultureprovides another illustrative example. In the Hmong language, there is no wordfor cancer or even a concept of it. In tryingto explain radiation, inexperiencedinterpreters or family members usedlanguage translated as “we’re going to putfire in you,” which obviously deterspatients from agreeing to treatment (Morse 2002).
There are numerous examples of howculture plays a role in the health careencounter. In many cultures, patients arereluctant to raise issues they deem asinsignificant with their providers. Forexample, a persistent cough in the early
motions must form the basis of a diagnosis(Chen 2003). These add up to unnecessarycosts to the health care system. A study in aChicago pediatric emergency departmentdocumented the cost of language barriers.After controlling for severity of illness, vital signs, tests, and insurance status, theinvestigators found that visits that had alanguage barrier were on the average $38more expensive and required more time,on the average 20 minutes more, thanthose without language barriers (Hamperset al. 1999).
Taken together, this body of research andcases show that speaking a language otherthan English puts a patient at risk foradverse health outcomes and reducedquality of care. The landmark Institute of Medicine (IOM) report, UnequalTreatment, suggested that factors within the health care system may exert differenteffects on patients, resulting in negativeconsequences for those with limitedEnglish proficiency. It further stated that“language mismatches are a fertile soil forracial and ethnic disparities in care” (IOM2002). Many of these findings suggest astrong need for improving oral and writtencommunication about the importance ofpreventive physician visits and medicationinstructions. Additionally, enhancedpatient-provider communication may leadto more effective diagnosis, reducing theneed for unnecessary testing and moreaggressive treatment. Lastly, improvedcommunication about publicly fundedprograms may improve access to care foreligible patients, as well as provide newfunding streams for hospitals and healthsystems treating these patients.

G R A N T M A K E R S I N H E A L T H 9
hours of the morning is typically anindication of asthma in a child. Someparents may not mention this problem if not specifically asked about it by theprovider because they may deem it asunimportant, particularly if the problemhas persisted for some time. A survey ofthree schools in one Californiacommunity—one with predominantlywhite students, another withpredominantly Hispanic students, and a third with predominantly Vietnamesestudents—found high levels of asthma inthe Hispanic and Vietnamese children,even though many children wereundiagnosed. Providers in the communitycommented that these indicators wererarely brought up during office visits (Kieu 2003).
Political nuances can also creep into theinterpretation process. Some immigrantscome to the U.S. from countries or regionsexperiencing political unrest. Many timeslanguage is directly related to politicalaffinities. In Farsi, for example, there aredialects used by particular regional orreligious groups that may be offensive to others.
Laws and Policiesfor EnsuringLanguage AccessThere is a legal and policy framework thatsupports access to language services. Thissection describes federal laws and policies,recommended federal guidelines, andpublic financing for language accessservices. While some states have specific
laws related to language access, a discussionof these is beyond the scope of this IssueBrief.
Federal Civil Rights PolicyThe legal basis for a patient’s right tolanguage access has existed for some time.Title VI of the Civil Rights Act of 1964states,
No person in the United States shall,on the ground of race, color, or national origin, be excluded fromparticipation in, be denied the benefitsof, or be subjected to discriminationunder any program or activityreceiving federal financial assistance.
The courts have interpreted national originto include individuals with limited Englishproficiency. Recipients of federal funding,such as Medicare and Medicaid providers,may be held liable for discrimination ifthey fail to provide access to languageservices.
In August 2000, President Clintonreiterated this policy by issuing ExecutiveOrder (EO) 13166, Improving Access toServices for Persons with Limited EnglishProficiency, which applied to all federalagencies, not just those focused on health.The EO required each federal agency to develop and implement guidance,specifically tailored toward its grantees, forimproving access to programs and servicesfor individuals with LEP. It also required allfederal agencies to meet the same standardsas their grantees by developing policies for ensuring linguistic access within theirown agencies (U.S. Department of Justice 2000).
“The cultural attitude
of the patient is very
important and must be
factored into any diagnosis
and treatment
recommendations.”
QUYNH KIEU,
THE HEALTHCARE
FOUNDATION FOR
ORANGE COUNTY

1 0 I N T H E R I G H T W O R D S
and effective communication betweenthe provider and LEP applicant/clientabout the types of services and/orbenefits available and about theapplicant’s or client’s circumstances(Office of Civil Rights 2002).
Although HHS recipients haveconsiderable flexibility in fulfilling thisobligation, OCR’s policy guidanceidentified four elements common toeffective language assistance programs(Office of Civil Rights 2002):
• Assessment: Providers should assess thelanguage needs of the population to beserved by determining the languages andnumber of LEP persons in the servicearea, identifying and recording languageneeds of each client/patient served,recognizing possible points of contactwhere language services are needed, andidentifying and obtaining resourcesneeded to provide timely languageassistance.
• Development of Comprehensive WrittenPolicy: Providers should develop andimplement LEP policies and proceduresthat include: furnishing notice to LEPpersons in their language of the right tofree language assistance; offeringcompetent oral language assistance,particularly avoiding the use of thepatient’s friends, family members, orchildren; and translating writtenmaterials.
• Training of Staff: Providers should traintheir staff to ensure that staff understandand implement LEP policies andprocedures. Training is essential tobridging the gap between policies andactual practices.
As the lead federal agency funding mosthealth and social services programs, theU.S. Department of Health and HumanServices (HHS) issued its guidanceimmediately after the EO, applying theselong-standing provisions of Title VI to thehealth care setting. The guidance was draft-ed by the HHS Office of Civil Rights(OCR), the agency responsible forenforcing federal civil rights laws in thehealth care context, including Title VI. The OCR guidance did not impose anynew requirements, but did reaffirm theexpectation that health care entitiesreceiving federal funds were required tooffer meaningful access to linguisticservices, including interpreters. Entitiesthat are responsible for complying with the guidance include: hospitals, nursinghomes, home health agencies, andmanaged care organizations; universitiesand other entities with health or socialservice research programs; state, county,and local health agencies; and physiciansand other providers receiving federalassistance from HHS. The guidanceexplained the legal requirements of TitleVI, provided a roadmap to compliance,identified best practices, and explained the process for handling complaints and enforcing the law (Office of CivilRights 2002).
The LEP policy guidance explained theobligations of federal grantees for ensuringlinguistic access and outlined several broadstrategies for accomplishing this. It states:
The key to providing meaningfulaccess to benefits and services for LEPpersons is to ensure that the languageassistance provided results in accurate

G R A N T M A K E R S I N H E A L T H 1 1
• Vigilant Monitoring: Providers shouldensure that LEP persons canmeaningfully access their services. At leastannually, providers should assess: thecurrent LEP makeup of its service area,the current communication needs of LEP persons, whether existing assistancemeets LEP needs, whether staff isknowledgeable about policies andprocedures and how to implement them,and whether sources of and arrangementsfor assistance are still current and viable.
Enlisting family, friends, and other patientsas interpreters is strongly discouraged bythe OCR guidance. Using children asinterpreters, in particular, is discouragedbecause of potentially damaging psycholog-ical effects when translating sensitivephysical or sexual matters for their elders(Downing and Roat 2002). Materials fromthe National Health Law Program(NHeLP) provide an example of such asituation: A provider performing anultrasound on a pregnant LEP patientinstructed the patient’s seven-year-olddaughter to tell her mother that the babywas stillborn. Only when the daughterbecame upset and refused to translate was aprofessional interpreter called (NHeLP1998). This practice is allowable by theOCR’s policy guidance only when apatient insists on using the trustedindividual, even after being informed oftheir right to an interpreter free of charge.In any other case, the OCR guidance has made it clear that the practice of“requiring, suggesting, or encouraging” apatient to bring his or her friends, minorchildren, or family members to serve asinterpreters infringes on the patient’s civilrights and is unacceptable (Office of CivilRights 2002).
Legislation has been introduced inCalifornia that would prohibit childrenfrom being used as interpreters. This bill(AB 292) would prohibit a state or localgovernmental agency, or a public or privateagency, organization, entity, or programthat receives state funding, from using anychild, or permitting any child to be used, as an interpreter. It would further requirethat they have in place, and available forinspection, an established procedure forproviding competent interpretation servicesthat does not involve the use of children(Huang 2003).
Some communities are enlisting bilingualyouth for limited interpreter roles, apractice that has both benefits andramifications. Often referred to as heritagespeakers—people who were either born inthe U.S. to an immigrant family or whoimmigrated themselves at an early age andspeak English—are seen as an untappedresource in many immigrant communities.Since there are a variety of circumstances inwhich interpretation is needed, they canplay valuable roles as patient greetersand/or navigators (Beltran Avery 2003).Such roles also help these speakers to retainrudimentary language skills and offer themthe opportunity to develop these skillsfurther. This can be a valuable asset,particularly for some of the rarer languages.Yet, caution must be exercised so that theirservices are not extended beyond theseduties to the clinical encounter. Merelybeing bilingual does not qualify someoneas an interpreter and, therefore, it isessential that providers know “where todraw the line, so that they don’t pull thesepeople into the encounter” (Chen 2003).
“Oftentimes family members
build their own agenda for
the patient. The health
encounter eventually
becomes a conversation
between the provider and
the person that speaks
English, while the patient
gets sidelined and left out.”
MAREN GRAINGER-
MONSEN, STANFORD
UNIVERSITY’S CENTER
FOR BIOMEDICAL ETHICS

1 2 I N T H E R I G H T W O R D S
Public Financing MechanismsAlthough federal laws and policies requirerecipients of federal funds to providelanguage services, there is no well-established funding mechanism. Majorsources of federal funding includecategorical grants and matching fundsunder Medicaid and the State Children’sHealth Insurance Program (SCHIP). The recently enacted Community HealthCenters Reauthorization Act includesauthorization for linguistic access grants to community health centers to provide translation, interpretation, and other suchservices, but funding has not yet beendetermined (The Access Project andNational Health Law Program 2003). TheOffice of Minority Health developed theBilingual/Bicultural Service DemonstrationProgram in 1993 to test models of cultural-ly and linguistically competent services andhelp LEP patients navigate managed caresystems. This grant program provides funding for a three-year period and iscurrently funding 20 sites nationwide.OMH anticipates issuing a new request for proposals for another round of grants in 2003.
Currently, the Centers for Medicare andMedicaid Services (CMS) provides theprimary source of federal funding to helpstates and health care providers pay forlanguage services. Through theMedicaid/SCHIP program, language
CLAS StandardsTo help providers and advocates respond tothe needs of the LEP population, the HHSOffice of Minority Health (OMH) issuednational standards for ensuring culturallyand linguistically appropriate services(CLAS) in health care (Figure 5).1 Thesestandards are organized by themes:culturally competent care (Standards 1-3),language access services (Standards 4-7),and organizational supports for culturalcompetence (Standards 8-14). Includingcultural competence with linguistic accessstrengthens the notion that interpretationand translation require knowledge ofculture (California Primary CareAssociation 2002). The standardsconcerning language access reiterate theobligations of federal fund recipientsoutlined in Title VI of the Civil Rights Act (and enforced by the Office of CivilRights). Other standards include practicesrecommended by OMH for adoption byfederal, state, and national accreditingagencies and suggested activities for healthcare organizations. The standards areintended for use by policymakers,providers, patients, advocates, purchasers of health care, accreditation andcredentialing agencies, and other healthcare organizations (IQ Solutions, Inc.2001).
1 Development of the CLAS standards was a multistep process to create a consistent framework from an existing patchwork of independently
developed definitions, practices, and requirements. The first stage of the project involved a review and analysis of existing cultural and
linguistic competence standards and measures, the development of draft standards, and revisions based on a review by a national advisory
committee. The second stage focused on obtaining and incorporating input from organizations, agencies, and individuals that have a vital
stake in the establishment of CLAS standards. The final standards reflect input from a broad range of stakeholders, including hospitals,
community-based clinics, managed care organizations, home health agencies, providers, policymakers, and professional organizations
(IQ Solutions, Inc. 2001).

G R A N T M A K E R S I N H E A L T H 1 3
Figure 5. National Standards for Culturally and Linguistically Appropriate Services in
Health Care
Standard 1: Health care organizations should ensure that patients/consumersreceive from all staff members effective, understandable, and respectfulcare that is provided in a manner compatible with their cultural healthbeliefs and practices and preferred language.
Standard 2: Health care organizations should implement strategies to recruit, retain,and promote at all levels of the organization a diverse staff andleadership that are representative of the demographic characteristics ofthe service area.
Standard 3: Health care organizations should ensure that staff at all levels and acrossall disciplines receive ongoing education and training in culturally andlinguistically appropriate service delivery.
Standard 4: Health care organizations must offer and provide language assistanceservices, including bilingual staff and interpreter services, at no cost toeach patient/consumer with limited English proficiency at all points ofcontact, in a timely manner during all hours of operation.
Standard 5: Health care organizations must provide to patients/consumers in theirpreferred language both verbal offers and written notices informingthem of their right to receive language assistance services.
Standard 6: Health care organizations must assure the competence of languageassistance provided to limited English proficient patients/consumers byinterpreters and bilingual staff. Family and friends should not be used toprovide interpretation services (except on the request of thepatient/consumer).
Standard 7: Health care organizations must make available easily understoodpatient-related materials and post signage in the languages of thecommonly encountered groups and/or groups represented in theservice area.
Standard 8: Health care organizations should develop, implement, and promote awritten strategic plan that outlines clear goals, policies, operational plans,and management accountability/oversight mechanisms to provideculturally and linguistically appropriate services.
Standard 9: Health care organizations should conduct initial and ongoingorganizational self-assessments of CLAS-related activities and areencouraged to integrate cultural and linguistic competence-related mea-sures into their internal audits, performance improvement programs,patient satisfaction assessments, and outcomes-based evaluations.
Standard 10: Health care organizations should ensure that data on the individualpatient’s/consumer’s race, ethnicity, and spoken and written languageare collected in health records, integrated into the organization’smanagement information systems, and periodically updated.
(Continues on next page)

1 4 I N T H E R I G H T W O R D S
federal funding vary, from lack ofawareness of its existence to tight state budgets (The Access Project and NationalHealth Law Program 2003). It is importantto note that while these services are coveredunder Medicaid, the Medicare program, asource of coverage for a growing number of elderly LEP individuals, does not offerseparate reimbursement for language accessservices (Katz 2003).
The nine states that have adopted theMedicaid/ SCHIP option currently use one of three models for paying for languageservices (Figure 6). Some states requireproviders to hire interpreters and then paythe providers for the costs. Other states payinterpreters directly. In New Hampshire,interpreters are required to enroll asMedicaid providers through a specialprocess. These interpreters can bill the statedirectly for their services. Finally, some
services are an optional service. In 2000,CMS reminded states that they couldobtain federal matching funds for languageservices provided to Medicaid and SCHIPenrollees. According to a letter to statehealth officials,
Federal matching funds are availablefor States’ expenditures related to the provision of oral and writtentranslation administrative activities andservices provided for SCHIP orMedicaid recipients. Federal financialparticipation is available in Stateexpenditures for such activities orservices whether provided by staffinterpreters, contract interpreters, orthrough a telephone service.
Currently, only nine states directlyreimburse for language services. Thereasons states do not take advantage of
Standard 11: Health care organizations should maintain a current demographic,cultural, and epidemiological profile of the community, as well as aneeds assessment to accurately plan for and implement services thatrespond to the cultural and linguistic characteristics of their service area.
Standard 12: Health care organizations should develop participatory, collaborativepartnerships with communities and utilize a variety of formats andinformal mechanisms to facilitate community and patient/consumerinvolvement in designing and implementing CLAS-related activities.
Standard 13: Health care organizations should ensure that conflict and grievanceresolution processes are culturally and linguistically sensitive and capableof identifying, preventing, and resolving cross-cultural conflicts orcomplaints by patients/consumers.
Standard 14: Health care organizations are encouraged to regularly make available tothe public information about their progress and successful innovations inimplementing the CLAS standards and to provide public notice in theircommunities about the availability of this information.
Source: Office of Minority Health 2000.
National Standards for Culturally and Linguistically Appropriate Services in Health Care
(Continued from previous page)
G R A N T M A K E R S I N H E A L T H 1 5
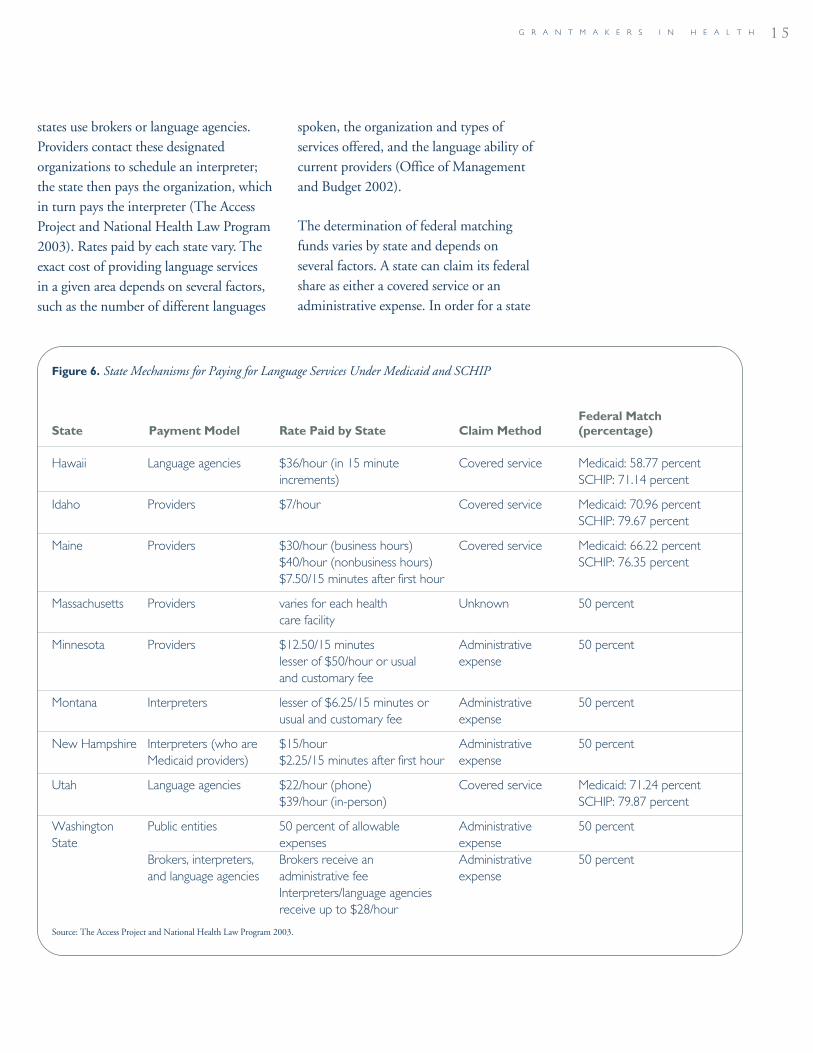
states use brokers or language agencies.Providers contact these designatedorganizations to schedule an interpreter;the state then pays the organization, whichin turn pays the interpreter (The AccessProject and National Health Law Program2003). Rates paid by each state vary. Theexact cost of providing language services in a given area depends on several factors,such as the number of different languages
spoken, the organization and types ofservices offered, and the language ability ofcurrent providers (Office of Managementand Budget 2002).
The determination of federal matchingfunds varies by state and depends onseveral factors. A state can claim its federalshare as either a covered service or anadministrative expense. In order for a state
Figure 6. State Mechanisms for Paying for Language Services Under Medicaid and SCHIP
Federal Match State Payment Model Rate Paid by State Claim Method (percentage)
Hawaii Language agencies $36/hour (in 15 minute Covered service Medicaid: 58.77 percentincrements) SCHIP: 71.14 percent
Idaho Providers $7/hour Covered service Medicaid: 70.96 percentSCHIP: 79.67 percent
Maine Providers $30/hour (business hours) Covered service Medicaid: 66.22 percent$40/hour (nonbusiness hours) SCHIP: 76.35 percent$7.50/15 minutes after first hour
Massachusetts Providers varies for each health Unknown 50 percentcare facility
Minnesota Providers $12.50/15 minutes Administrative 50 percentlesser of $50/hour or usual expenseand customary fee
Montana Interpreters lesser of $6.25/15 minutes or Administrative 50 percentusual and customary fee expense
New Hampshire Interpreters (who are $15/hour Administrative 50 percentMedicaid providers) $2.25/15 minutes after first hour expense
Utah Language agencies $22/hour (phone) Covered service Medicaid: 71.24 percent$39/hour (in-person) SCHIP: 79.87 percent
Washington Public entities 50 percent of allowable Administrative 50 percentState expenses expense
Brokers, interpreters, Brokers receive an Administrative 50 percentand language agencies administrative fee expense
Interpreters/language agencies receive up to $28/hour
Source: The Access Project and National Health Law Program 2003.

1 6 I N T H E R I G H T W O R D S
language barriers in the health care setting,opportunities for improvement, and waysin which grantmakers have supported thesevarious strategies and programs. Currentpractices include:
• relying on the language skills of providersand patients;
• in-person, third-party interpretation,both ad-hoc and professional;
• remote, third-party interpretation usingtechnology; and
• the translation of written materials.
Improving Language Proficiency of ProvidersThe lack of diversity in the health careworkforce often emerges as the broad issuerelevant to language access. While there is aneed to increase the availability of trainedmedical interpreters, there is the dual need to increase the representation ofbilingual/bicultural providers. There areseveral advantages to having a providerwho can speak the same language as thepatient. Bilingual/bicultural providers areideal because insight into the patient’sculture and the ability to speak to thepatient directly help create a connectionbetween provider and patient. When thepatient and provider are from the same culture, mutual understanding of culturalbeliefs and health care practices enablesome providers to pick up on subtlecultural nuances that can influence healthbehaviors and attitudes.
Health care organizations must be able to ensure the accuracy of self-declaredlanguage proficiency of bilingual providers(Green 2003). While both native and
to claim language services as a coveredservice, it must submit a request to CMSto have it added to its Medicaid state plan.States can also choose to claim languageservices as an administrative cost, whichmay offer a lower matching rate,2 butrequire no prior approval (The AccessProject and National Health Law Program 2003).
Strategies forImproving LanguageAccess in theHealth Care SettingThere are several broad approaches toimproving access to language services,including strengthening service delivery,promoting advocacy and policy change,and advancing research. Specific practicesrelated to these approaches are discussed inthis section, along with ways in whichfoundations are supporting and furtheringthese activities.
Improving Access in DeliverySettingsHealth care organizations and providershave used various methods of servicedelivery to reduce linguistic and culturalbarriers between patients and providerswho do not speak the same language.Different practices are appropriate indifferent settings and communities.Oftentimes a combination of severalmethods is most effective at ensuring equal access to linguistic services for allpopulations. The following sectiondescribes current practices for addressing
2 While the match for covered services ranges from 50 to 84 percent, all states receive a standard 50 percent federal match for both Medicaid
and SCHIP for administrative expenses.

G R A N T M A K E R S I N H E A L T H 1 7
nonnative speakers may be familiar withthe language in social settings and/or anacademic context, they may lack theterminology specific to the medicalencounter, particularly if their medicaltraining was in English. While severalhealth plans now publish the language oftheir providers in their provider directories,there is no standardization as to theaccuracy of those self-declarations.Providers may list the languages they speakor those spoken by anyone employed intheir office, oftentimes without furtherquestioning. In efforts to enhance itsservices and accountability, the AlamedaAlliance for Health completed a detailedsurvey of its provider network. The six-page survey not only asked for self-declaredlanguage(s) for each person employed inthe office, but also, “Where did you learnthe language? Are you a native speaker?Did you learn it in high school? Did you learn it in college? Did you entermedical/professional school speaking thatlanguage?” Although the survey cost thehealth plan considerable time and money,it achieved a fairly high response rate(Quan 2003).
Practical limitations prevent use ofbilingual/bicultural providers from beingthe sole strategy for any one health care setting. Developing the language skills ofothers in the health care organization isalso important, as language needs extendbeyond the examination room. Duringtheir visits and when navigating the health care system, patients interact withadministrative and other staff, includingreceptionists, orderlies, lab technicians, and pharmacists. Ensuring that the entirehealth care organization is linguistically
accessible can be a costly and complex taskin large settings with multiple languageneeds (Downing and Roat 2002).
Foundations have played an important rolein supporting the bilingual training of bothproviders and staff. Grantmakers are alsohelping educational institutions enhancethe linguistic ability of current students.For example:
• The Assisi Foundation of Memphis, Inc.funded the Christ Community MedicalClinic, Inc. to help the clinic fundparticipation in Spanish languagetraining for clinic employees.
• The Blue Cross Blue Shield ofMassachusetts Foundation has sponsoreda number of activities to train bothproviders and their staff to be bothlinguistically and culturally competentthrough its Pathways to CulturallyCompetent Health Care initiative. Itfunded the Lowell Community HealthCenter, Inc. for a comprehensive traininginitiative to serve its Brazilian and Africanimmigrant communities throughinterpreting and cultural competence forphysicians and staff. It also establishedthe Latino Consult Service to build thebilingual skills of staff at Beth IsraelDeaconess Medical Center by teamingthem with bilingual and biculturalproviders. It also funded the HealthAccess Collaborative of SoutheasternMassachusetts, Inc. to support thedevelopment and delivery of advancedcultural competence and interpretertraining for professional and clinical staffand basic medical interpreter training foradministrative and reception staff at theNew Bedford and Fall River hospitals,

1 8 I N T H E R I G H T W O R D S
International Health Care WorkersAssistance Center for the Los Angeles andSouthern California area. The first year ofthe three-year grant included planning, andthe center officially opened in 2002. Thepurpose of the center is to help physicians,nurses, radiology technicians, respiratorytechnicians, and others trained in thehealth field from other countries obtainappropriate licenses and credentials to workin the U.S. health care system. It will alsooffer orientation and job placementservices. By helping these workerstransition to the U.S. health care system,the center will help meet the demand for highly trained professionals incommunities that desperately need theirskills, as well as their linguistic and culturalcompetency. Additionally, the projectaddresses the need for racial and ethnicdiversity in the health care workforce.
Similarly, The HealthCare Foundation for Orange County was able to inititatefunding in the area of interpretation byaddressing the broader issue of the ethnicdiversity of the workforce. The foundationfunded a project to train, as interpreters,foreign-educated physicians who wereunable to practice medicine in the U.S.because of their limited English languagecompetency. The ultimate goal of theprogram is to enable these physicians togain the skills necessary to become licensedhealth professionals.
Improving Language Proficiency of PatientsAnother approach for improving languageaccess is promoting English proficiencyamong patients so they can effectively navigate the health care system andcommunicate with providers. Some organizations, like Arlington, Virginia-
neighborhood health centers, andcommunity-based organizations that make up this collaborative.
• The Helene Fuld Health Trust in NewYork supported a grant to Lee College to provide nursing faculty and studentslanguage instruction in medical Spanishto improve their ability to perform healthassessments for Spanish-speakingpatients.
The advantages of having providers whospeak their patients’ languages have raisedquestions about how to take advantage ofthe skills of immigrant health professionals.A group of Latino health care advocates inGeorgia, for example, is pushing for thestate to adopt a new licensing process forhealth care providers that would helpalleviate the shortage of bilingualphysicians and nurses. Under current statelaw, it can take foreign-trained nurses up to three years and foreign-trained doctorsup to seven years to receive their licenses.Groups are asking Georgia’s ProfessionalLicensing Boards Division to review a planthat would give foreign-trained medicalprofessionals a limited license and requirethem to work alongside licensed doctorsand nurses while they learn English, undergo credential reviews, and completefollow-up classes or tests required forformal licenses. Providers would be able to provide needed services to Spanish-speaking patients in their language, while they become proficient in English(Dodd 2002).
In response to the growing number ofimmigrants, consisting of both those whoneed health care and professionals in searchof meaningful job opportunities, TheCalifornia Endowment has funded a $1.4 million project to create an

G R A N T M A K E R S I N H E A L T H 1 9
based ProEnglish, actively promote the useof English and oppose multilingualism.California’s Little Hoover Commission, an independent state oversight agency,issued a report in 2002 on the rights and responsibilities of immigrants inCalifornia—a group that currentlycomprises one-quarter of that state’spopulation. The commission called forincreased efficiency of public services, aswell as a California Residency Program thatwould give immigrants preferential accessto public benefits, including health care, if they agreed to certain responsibilities.Among those responsibilities are the abilityto speak English or the enrollment inEnglish-language training. In presentingthe general concept behind the program,the commission suggested that immigrantswho commit to the residency programwould be given priority over otherimmigrants to receive benefits, such asMedi-Cal, the California Medicaidprogram. Those who choose not to makethis commitment would receive lowerpriority to access public sector services(Little Hoover Commission 2002).
Although promoting self-sufficiency andimproving the effectiveness of publicprograms are noteworthy goals, assumingthat all LEP populations can become fluentis probably unrealistic, particularly when itcomes to health. First, immediate healthneeds make it impossible to wait forlinguistic competence and culturalassimilation. While most immigrants arrivein good health, many refugees—especiallythose fleeing from violent situations and/orpersecution in their homeland—may arrive with complicated medical andpsychological health problems (NationalCouncil on Interpreting in Health Care
2001). Secondly, English as a SecondLanguage (ESL) courses may not besufficient preparation for navigating thehealth care system. These classes generallyemphasize practical communication forsurvival and employment, rather thandeveloping higher-level language skillsneeded to understand explanations ofdisease, bodily processes, and treatmentalternatives (Downing and Roat 2002).Moreover, for most working adults,learning a new language is time-consumingand may take a backseat to supporting andcaring for their families. Many immigrantsalso fear that ESL classes and other venuesthat cater to immigrant populations are toooften frequented by Immigration andNaturalization Service officers. Latinoimmigrants tell of being recruited intoEnglish-language classes by local communi-ty colleges, while simultaneously beingtargeted by law enforcement officers whowait for them to drive to work or class(Little Hoover Commission 2002). Finally,the use of a priority system may causefurther divide among immigrantcommunities, as some groups may find iteasier to assimilate, such as those that comefrom countries with high exposure toAmerican culture. Immigrants that comefrom less developed nations and/or thosefleeing from persecution may be less likelyto succeed in the program, yet be the mostvulnerable and in need of public assistance.
There are positive steps that can be taken to improve language skills andunderstanding of American customs andinstitutions. The Colorado Trust hasemployed a two-pronged approach by initiating its grantmaking on both positiveacculturation and language access to healthcare services. In response to a needs

2 0 I N T H E R I G H T W O R D S
skills and provide ongoing professionaldevelopment for interpreters. Marketinginterpreter bank services and educating the community about the need for high-quality, professional interpreters areongoing challenges (Downs-Karkos 2003).
Expanding Access to Third-PartyInterpretationThird-party interpretation, both in-personand through the use of advancedtechnology, is gaining increased attentionand scrutiny and is being adopted in manyforms. Interpretation services have beenshown to effectively reduce languagebarriers and improve access to care for LEPpatients. Implementation of an interpreterprogram in a large health maintenanceorganization was highly associated with anincrease in the number of physician officevisits, receipt of preventive care, and theamount of prescriptions filled for LEPpatients. This trend was not seen in thecohort of health plan members that did notuse the interpreter services, suggesting theeffect was due to the implementation ofthese services (Jacobs and Goldin 2002).
Ad-hoc InterpretersAd-hoc interpreters are individuals whoseprimary job function in the health caresetting is something other thaninterpretation and includes the patient’sfamily members, friends, clinic staff, oreven fellow patients. These individuals arebilingual, but not formally trained asinterpreters. The danger in using familymembers as interpreters was explained in a previous section of this report and,therefore, will not be described here as astrategy, although this was perhaps themost common method in use at one time.Instead, this section focuses primarily on
assessment focusing on immigrants andrefugees in Colorado, the foundationlaunched the Supporting Immigrant andRefugee Families Initiative in the fall of2000. This five-year, $7.5 million effort has two program components. The firstcomponent addresses mental health and acculturation by strengtheningcommunity-based organizationsthroughout the state that provide directmental health and acculturation services to newcomers. Such services includecounseling, ESL classes, support groups,and parenting classes.
The Colorado Trust’s second componentaims to increase language access services inthe health care setting. The foundationconvened interested stakeholders, such asinterpreters, health care providers, theregional HHS Office of Civil Rights, andimmigrant and refugee organizations fromthe Denver area; the group emerged as theCoalition for Language Access. With thehelp of a facilitator, the coalition identifiedthe critical issues in providing high-qualitylanguage interpretation. One priority wasthe need to train health care providers onhow to effectively work with medicalinterpreters. A curriculum was created inresponse, and presentations were made tointerested providers. Another needidentified as critical was the creation of a high-quality interpreter bank in theDenver area. Through an RFP process, the foundation selected a local organizationto create and manage the interpreter bank.One year into implementation, theinterpreter bank has successfully recruited a cadre of interpreters, provided health care interpretation training, focused oninterpretation ethics, and continues toexplore ways to constantly assess language

G R A N T M A K E R S I N H E A L T H 2 1
other ad-hoc interpreters, includingbilingual clinical or nonclinical staffmembers.
In most instances, the quality of the healthcare encounter is compromised with ad-hoc interpreters whose job functions mayrange from a bilingual physician or nurseto a janitor, receptionist, or an orderly. The interpreter may have only slightlybetter English skills than the patient, lackknowledge of appropriate health-relatedtranslations, or be likely to minimize theprovider’s diagnosis and instructions toalleviate emotional distress. It can alsohinder the organizational effectiveness ofthe health care setting if employees arebeing pulled away from their normal duties to interpret.
A recent study found that mistakescommitted by ad-hoc interpreters weresignificantly more likely to have potentialclinical consequences than those made byhospital interpreters. At Boston MedicalCenter’s outpatient pediatric clinic,researchers found that medical visits ofSpanish-speaking patients had an averageof 31 errors in medical interpretation andthat more than 50 percent of thesemistakes had the potential to adverselyaffect the patient’s health. The mostcommon mistakes included omitting information, substituting words orexpressing personal opinions, and addinginformation (Flores et al. 2003).
For organizations with rare and minimallanguage needs, ad-hoc interpretation can serve as an effective solution whenemployees are adequately trained and givensupport. For example, some organizationshave implemented “Interpreter for a Day”policies where bilingual employees are
relieved of their primary job functions to interpret for that day and are thenrewarded through pay differentials. It isimportant to note, however, that thesesolutions must be augmented byappropriate access to and requirements for formal interpreter training (Downingand Roat 2002).
Recognizing the need to increase thenumber of bilingual personnel in localphysicians’ offices, The Health Foundationof Greater Cincinnati developed a mini-RFP to increase the number of bilingualpersonnel in local primary care offices. The greater Cincinnati area has seen arapid influx of non-English speaking populations, specifically Hispanic and West African immigrants. Some localorganizations that work closely withundocumented immigrants estimate thatthere may be close to 30,000 Hispanicimmigrants in the area. As a result, severalsafety net primary care providers within the foundation’s service area have reporteda dramatic increase in the number ofHispanic and West African patients seekingmedical and dental care. Unfortunately,these sites are minimally staffed andoftentimes have no bilingual personnel. Inmost instances, providers have resorted tousing nonclinical bilingual staff to assistwith translation and interpretation, pullingthese individuals away from their primaryjob functions. In rare cases, area providershave prearranged for an interpreter toaccompany the patient, but the hourly ratefor interpreters has been cost-prohibitivefor those providers with smaller practices.
To address this need, the foundationannounced the availability of $200,000 forgrants to assist primary care providers tothe poor in hiring bilingual employees

2 2 I N T H E R I G H T W O R D S
recommends that “professionalinterpretation services should be thestandard where language discordance posesa barrier to care” (IOM 2002). Health careorganizations have employed a variety ofstrategies, including hiring interpreters,contracting for their services on a per diembasis, contracting with a language agency,and/or using volunteer agencies that helpplace volunteer bilinguals (Downing andRoat 2002). There are trade-offs for eachstrategy, and often a combination ofstrategies works best (Figure 7).
Foundations have supported a variety ofactivities and promising practices thatprovide qualified third-party interpretersfor LEP populations:
• The Consumer Health Foundation inWashington, DC supported La Clinicadel Pueblo to improve and increase accessto quality and specialized medical care for the Latino community throughinterpreter services. The project trainedpatient care coordinators, as well ascommunity medical interpreters for on- and off-site interpretation.
• The United Hospital Fund in New Yorkfunded the Queens Hospital Center totrain linguistically and culturally diversevolunteers to serve as advocates forpatients being treated in one of thecenter’s facilities that specializes in cancer,women’s health, and diabetes. The fundalso supported the Greater New YorkHospital Foundation and the New YorkTask Force on Immigrant Health to workjointly on a project to develop a businessplan and a related research agenda thatwould create centralized medicalinterpretation services for New York City
for direct service jobs. Individual grants of $50,000 were awarded for a one-yearperiod to assist provider organizations with the following:
• the recruitment and training costs forbilingual personnel who would beresponsible for providing direct services(allowable costs included advertising,certification or licensure fees, and/orremedial training for clinical supportpositions); or
• support for salary and benefits for up to six months that is matched by theorganization for another 12 months. The expectation would be to retain theemployee, based upon a satisfactoryperformance review and compliance withthe organization’s personnel guidelines.
Eligible applicants included public orprivate nonprofit organizations that offerdirect medical and/or dental services tolow-income, uninsured, or underinsuredpatients. Providers also had to show thattheir non-English speaking populationcomprised at least five percent of the totalactive patients served or document that thepractice site was located in an area with ahigh concentration of non-Englishspeaking residents. After distributing thegrants under these specifications, thefoundation found that grantees wanted touse a portion of the funding for a spin-offtraining program for medical interpreters.Recognizing the need for appropriate training, a three-day class at local hospitalswas designed (Warren 2003).
Dedicated or Professional InterpretersProfessional interpreters are thoseindividuals whose sole function in thehealth care setting is to interpret. The IOM
“The primary tool that
providers use to diagnose a
patient is language.
Interpretation is a
diagnostic tool.”
MARIA-PAZ BELTRAN
AVERY,
EDUCATION
DEVELOPMENT CENTER

G R A N T M A K E R S I N H E A L T H 2 3
hospitals. The project would also developrelated cultural competency programs formedical staff.
• Several foundations in California, such as the Alliance Healthcare Foundation,The California Endowment, and TheCalifornia Wellness Foundation, arefunding Pacific Asian Language Services(PALS) for Health, a nonprofit,community-based organization offering
free verbal interpreting services to healthcare providers serving limited Englishspeaking Asian and Pacific Islanderclients. PALS also works in trainingproviders on the benefits of usinginterpreters and how to effectively use interpreters.
• Mount Zion Health Fund in SanFrancisco, California has made a numberof grants to reduce LEP barriers to care
Figure 7. Strategies for Using Professional Interpreters
Strategy Description Advantages Disadvantages
Staff • employed part-time or full-time • interpreter is familiar with • productivity of interpreters Interpreter by health care organization provider and patient population depends on language needs of
• usually recruited in most common • interpreter has most likely received patient populationlanguage(s) of patient population formal training and has high • rarely cost-effective to employ
incentives for continuing education interpreters in all language • contributes to operational combinations
effectiveness for an organization because providers do not have to use ad-hoc interpreters
Contract • interpreters are not employed • interpreter has most likely • requires an entity at the health Interpreter by health care organization, but received formal training and has care organization to coordinate
available per diem or on-call high incentives for continuing screening, contracting, dispatching, • can be scheduled in advance or education and payment of interpreters
contacted on short notice when • can be more cost-effective than • hourly rate can be more costly needed staff model when demand is low than staff model (although
organization may save costs on benefits, etc.)
Language • health care organization • takes responsibility for recruiting, • may be prone to hiring unqualified Agency contracts with language agency screening, training, and paying interpreters in times of high
that recruits, contracts, and interpreters demanddispatches interpreters on • agencies concentrate solely on • health care organizations have no demand interpreting and are more likely direct oversight for quality and
• agencies can be for-profit to build relationships with performance of interpretercompanies, community bilingual residents in the interpreter pools, nonprofits, or communitycommunity-based organizations • may have access to a wider
variety of languages
Volunteer • resembles contract interpreters, • cheap way to provide language • few are trained or held Organization but are not compensated for services and promote accountable to minimum
work volunteerism in the community standards
Source: Downing and Roat 2002.

2 4 I N T H E R I G H T W O R D S
and providers wear headsets during theencounter; their conversation istransmitted to a nearby receiver and thendigitally over a fiber-optic line to a centralswitching station in the remote interpreterroom. The interpreter, also wearing aheadset, listens to what is being said by oneparty and then transmits the interpretationto the other. The patient and provider hearonly their language; since the interpretationis simultaneous, it resembles a languageconcordant encounter. With thistechnology, only the patient and providerare present in the room, thereby avoidingthe tendency for them to relate to the in-person interpreter rather than to eachother (Gany 2003; Youdelman and Perkins 2002).
With subsequent funding from the New York City Health and HospitalsCorporation, CIH implemented a pilotproject to test RSMI at GouverneurDiagnostic and Treatment Center in 1999.The hospital is a public facility located in a New York City neighborhood with apredominantly Chinese and Hispanicimmigrant population. Over 50 percent of its patients are LEP. Implementation ofRSMI continues to operate with trainedinterpreters who have been screened forbilingual aptitude and have undergonerigorous training in simultaneous interpret-ing. The interpreters are monitored forquality by a language coach and engage incontinuing education exercises to enhancetheir knowledge base. The initial success of the program has led to expansion of the technology to Bellevue Hospital.Available languages include Spanish,Mandarin, Cantonese, Fuzhao, andBengali (Gany 2003).
for recent Russian and Bosnianimmigrants. One and two-year grantshave funded the International Institute’sNewcomers Health Program to providepatient interpretation and one-to-onecounseling at the Refugee Clinic of SanFrancisco General Hospital.
Remote, Third-Party InterpretationHealth care organizations are turning to avariety of technological innovations toreduce language barriers in the health caresetting. The use of telephone language lineshas been increasing rapidly, while a fewinstitutions have been experimenting withalternative methods, such as video linksand other remote systems. Providers oftenprefer these methods to in-personinterpretation because they do not have to wait for an interpreter to be physicallypresent. With remote systems, however, theinterpreter is not privy to facial expressionsand/or nonverbal cues.
In 1995, New York University’s Center forImmigrant Health (CIH) received aplanning grant from the United HospitalFund to examine projects nationwide thataddress delivery systems for interpreterservices. The objective was to uncovermodels that could effectively be replicatedin the New York area, where diverselanguage needs and geographicallyscattered hospitals presented logisticalchallenges. Their research uncovered a pilot project that was applying translationtechnology used by the United Nations to the health care setting. Remotesimultaneous medical interpreting (RSMI)uses highly trained simultaneous medicalinterpreters who sit in a remote location asthey interpret for doctors and patientsthrough wireless headsets. Both patients

G R A N T M A K E R S I N H E A L T H 2 5
Changing Provider Attitudes
Lack of funding is often identified as the primary obstacle to the use of professionalmedical interpretation. As one health plan found, however, the real issue may be providerattitudes and habits. The Alameda Alliance for Health (the Alliance)—a nonprofit healthplan with 90,000 members, of which 45 percent are LEP—not only pays for the full costof professional medical interpreter services (face-to-face and telephonic), but alsocompensates its physicians and providers who take advantage of these services. Despitethis rich array of benefits, the Alliance found that interpreter services were severely underutilized (Quan 2003). In this case, finances were not the only reason providers were not embracing these services.
There are several nonfinancial reasons why providers do not use interpreter services,even when readily available. First, many physicians may believe that their own languageskills are adequate, despite evidence to the contrary. Others think that patients can bediagnosed and treated without direct communication if hand signals and clinical tests canbe used. Still, many believe that the use of family and friends for interpretation is adequateand that it is more culturally appropriate and less distant than third-party interpretation.Finally, a good portion continue to believe that English is the official language of the U.S.,and patients should be expected to know or learn it (Quan 2003).
Negative experiences and logistical challenges can also dampen providers’ willingness touse these services. Some providers are not used to working with interpreters, and learningthis skill is yet another burden to an already busy workday. The logistics are significant andmay include: arranging for an interpreter, waiting for an interpreter, lacking equipment inexam rooms, an insufficient supply of qualified interpreters, and not being able to find orevaluate qualified interpreters.
There are several approaches for getting providers on board. Hablamos Juntos, a nationalprogram of The Robert Wood Johnson Foundation, is conducting focus groups withphysicians to learn how they view language barriers and third-party interpretation. This information will help determine the best method for presenting this issue to otherphysicians (Partida 2003). The Alliance continues to educate its providers on the benefitsand availability of professional interpreters. A rigorous awareness campaign targetingphysicians more than quadrupled its utilization of interpreters in one year (Quan 2003).
More can be done to create opportunities for educating and training providers, from the early stages of medical school to advanced practice. Starting early by engaging medicalstudents in these issues could shape who they become as physicians (Hernandez 2003).Once in practice, providers should have access to continuing medical education thatfocuses on issues related to language and culture. Modules, where providers andinterpreters are taught to work together, would demonstrate the benefits of working with a qualified medical interpreter. For some providers, one positive experience with an interpreter is enough to make them demand these services in subsequent patientencounters.

2 6 I N T H E R I G H T W O R D S
nightmares in translation. In one smallRhode Island community, one can findtremendous diversity in the Latinopopulation, consisting of Dominicans,Puerto Ricans, Colombians, and Mexicans,all with a slightly different twist on theSpanish language. Some groups are morefamiliar with common colloquialisms,while others use academic Spanish. TheVista Community Clinic in San Diego,California addresses this issue by using themajority usage for a specific term and in its absence, defaulting to proper Spanish(Green 2003). Secondly, in a variety oflanguages and dialects, an equivalent worddoes not exist in the non-English language,particularly for medical procedures andbody parts. In response, Kaiser Permanentehas been trying to gather a group ofmedical interpreters to create a commonlexicon of terms (Quan 2003). Lastly,translation involves finding a balancebetween ensuring an appropriate readinglevel and not assuming a patient isuneducated. Translated materials can oftenbecome so simplistic that it becomesoffensive to the reader (Green 2003).
The HHS Office of Civil Rights policyguidance set forth the following guidelinesfor ensuring access to written materials anddocuments for LEP patients served byrecipients of federal funding:
• translation of all written materials foreach LEP language group that equals thelesser of 10 percent or 3,000;
• translation of at least vital documents foreach LEP language group that equals thelesser of 5 percent or 1,000; and
• translated notice of right to competentoral interpretation of written documentsfor LEP populations below the abovethresholds (Office of Civil Rights 2002).
Translation of Written MaterialsWritten materials serve multiple purposesin health care settings, including relayinghealth education and preventionguidelines, surveying a patient’s medicalhistory, stating dietary restrictions, givingpre- and post-operative instructions,approving advanced directives, and otherimportant tasks. The translation of certaindocuments, when done thoughtfully, canbe a valuable means of relaying importanthealth messages to LEP individuals andtheir families. It is important to recognize,however, that translation from English toanother language is more complex thansimply changing one text into another.Particularly with health and medicalinformation, appropriate translationinvolves cultural considerations andunderstanding the situation in light ofone’s cultural background and beliefs(Anderson 2002).
For example, an American Academy ofPediatrics project to translate the index for child development into Vietnameseillustrates how language cannot beseparated from culture. In describingindications of child development, parentswere instructed to observe how manyblocks a child is able to stack. It is possibleto translate this statement literally. InVietnam, however, children do not playwith blocks; consequently, many childrenwould fail that measure. An equally validmeasure of fine motor skills and a moreculturally appropriate observation wouldbe the child’s ability to handle chopsticks(Kieu 2003).
There are numerous challenges anddifficulties when trying to translateculturally appropriate materials. First, thediversity of one language alone can create
“It’s a very ambiguous line
at times and a very thin line
that you have to walk when
you’re making a translation
that is appropriate
culturally and linguistically
to your entire population.”
CAROLA GREEN,
VISTA COMMUNITY
CLINIC

G R A N T M A K E R S I N H E A L T H 2 7
Even populations above these thresholdswill sometimes need oral interpretation ofwritten documents because of low literacylevels in their primary language. Forexample, the Canby Family Practice Clinicin California, a rural community healthcenter, has a large Spanish-speakingpopulation above the 10 percent threshold,but many patients are illiterate. The clinic’sstaff has been careful to translate vitalhealth forms, such as advanced directives,informed consent forms, financialmaterials, and discharge information, in aprivate and confidential manner. Typicalmedical history forms ask extremelysensitive questions, including onesregarding reproductive and sexual health.When translated in busy waiting rooms,with the presence of other patients, theLEP individual may not be comfortableanswering certain questions. To address thisproblem, the clinic created a translationroom, where patients who need assistancecompleting forms can go and meet with atrained, bilingual interpreter (CaliforniaPrimary Care Association 2002).
The Alameda Alliance for Health spendsapproximately $300,000 a year to translateall its marketing materials, grievancematerials, legal documents, and providerdirectory into all of its threshold languages.The health plan makes a point of creatinghigh-quality original documents thatcontain both English and the targetlanguage, so that if there are familymembers who speak English, they can read through the materials with oneanother (Quan 2003).
A number of foundations have funded thetranslation of health documents. Severalfoundations, for example, have supportedthe translation of a variety of importantpatient education materials:
• Missouri Foundation for Healthsupported the expansion of a gestationaldiabetes education program to Bosnianand Hispanic women through thetranslation of patient handbooks andmaterials to their respective languages.
• The HealthCare Foundation for OrangeCounty supported a Vietnamese versionof the popular Guide for New Parents,produced and distributed by PreventChild Abuse–Orange County.
• Hogg Foundation for Mental Healthsupported the translation into Spanishand printing of the Texas Department ofMental Health and Mental Retardation’spublications: Taking Care of Your MentalHealth and What is Mental Retardation?
• The Annie E. Casey Foundation fundedthe National Health Law Program toproduce a consumer guide to help low-income persons understand and chooseamong managed care plans. Supportincluded translation into Spanish andChinese.
Many screening tools used by providers,particularly those for mental illnesses,appear as questionnaires and self-administered surveys. Accurate andculturally appropriate translation of thesedocuments is essential to proper and timelydiagnosis. The following foundations haveworked to provide these important tools:
• William T. Grant Foundation funded theUniversity of Puerto Rico to create acarefully crafted Spanish version of theChild and Adolescent Psychiatric

2 8 I N T H E R I G H T W O R D S
Foundations can facilitate thiscollaboration among communities byproviding supplementary funding to theirgrantees for wider dissemination of relevantmaterials (Pulley 2003).
Improving TrainingBilingual skills do not automatically makean individual an effective interpreter.Quality interpretation includes sufficientproficiency in both languages, includingmastery of the medical terminology in both languages (Chen 2003). Additionally,trained interpreters have criticallyimportant memory skills, the ability tonegotiate a three-way conversation, andbasic knowledge of cultural attributes thatcan influence health.
Because interpretation in the health caresetting is a specialized skill and requires for-malized training, uniform standards forboth training and practice are prerequisitesfor high-quality translation. There arecurrently no minimum requirements fortraining programs, and many communitieslack access to medically specific interpretertraining programs.3 This lack of trainingnot only compromises the quality of thehealth care encounter, but it may alsotarnish the reputation of qualified, properlytrained interpreters when errors are madein translation. Standards for interpretertraining and practice may help reduce theincidence of ad-hoc and second-rateinterpretation and ultimately reduce costlymedical errors and complications.Development of these standards may leadto certification requirements that supportthe recognition of health care interpretingas a respected profession and an integralpart of the health care team.
Assessment tool, an interiew-based surveythat allows a trained interviewer to makedevelopmental and cultural judgmentsabout psychiatric symptoms.
• Hogg Foundation for Mental Healthawarded the University of Texas HealthScience Center in Houston funding forthe Spanish translation and field testingof various questionnaires concerned withanxiety and related disorders. Thepurpose of the surveys is to aid in thediagnosis and treatment of such disordersamong Hispanic adult populations. Thefoundation also supported the translationof brief, standardized, self-reportedprocedures to identify and monitormental health problems among a varietyof ethnic populations in the Houstonarea. The measures were used to identifynew refugees with potential disorders andto monitor their symptoms until mentalfunctioning is restored. Refugees in theprogram speak Arabic, Serbo-Croatian,Spanish, and Vietnamese.
When translating written materials,communities can work together to identifyand disseminate existing resources, ratherthan continuously re-creating the wheel.One valuable resource may be health-related materials in foreign countries, if they are applicable to the targetcommunity. Similarly, materials developedfor one project may have a life beyond theiroriginal audience. For example, the Pasodel Norte Health Foundation developed a poster of the food pyramid that wastranslated into Spanish and illustrated withfoods specific to the Mexican or Latinodiet. After seeing the poster at a meeting,another foundation was able to pass italong to some of its grantees and clinics.
“When you are talking
about a medical encounter
with an LEP patient, there
are actually four languages
present—English, the
medical language in English,
the second language, and the
medical language in the
second language . . . very
few people have that whole
repertoire at their disposal.”
ALICE CHEN,
ASIAN AND PACIFIC
ISLANDER AMERICAN
HEALTH FORUM
3 Court and conference interpretation are the focus of the majority of training/certification programs.

G R A N T M A K E R S I N H E A L T H 2 9
Currently, medical interpreter trainingprograms are being offered by hospitals,community-based organizations, languageagencies, and a few institutions of highereducation. These programs have noconsistent standards for training orcertification and vary widely in structureand quality. Training programs run thegamut and seem to fall into one of thefollowing categories:
• eight hours of instruction withouttesting;
• a language proficiency test followed byless than one day of instruction;
• two days of instruction, occasionallyaccompanied by a practicum;
• 40 hours or more of instruction with a practicum and a final exam (with orwithout a preceding language proficiency test);
• a combination of medical and courtinterpreter training;
• one semester at the community collegelevel with a practicum;
• more than one semester at the collegelevel; and
• advanced degrees in interpreting.
The National Council on Interpreting inHealth Care (NCIHC) emphasizes theimportance of establishing minimumcriteria for a standardized medicalinterpreting training program. There issome consensus that training programsshould consist of a minimum of 40 hoursof instruction and include the followingtopic areas: medical terminology,interpreting skills, code of ethics or ethicalissues, role play, and cultural awareness.Training should culminate in an oral final
test and, ideally, a practicum whereinterpreters can actually practice what they learned (NCIHC 2002).
Several challenges crop up when trying to develop standards and certification for interpreters. With the diversity inlanguages, creating proficiency tests for alllanguages is a daunting task, particularlyfor some of the rarer languages. Research isneeded to determine what the average levelof proficiency is for speakers of a certainlanguage (Green 2003). On a cautionarynote, the use of common protocols andframeworks may adversely affect speakersof languages who come from disruptededucational systems and/or rely on oral,rather than written, communication. Rigidstandards might reduce or eliminate thepool of qualified people available to serveas interpreters (Beltran Avery 2003).
Some organizations, like the MassachusettsMedical Interpreters Association and theCalifornia Healthcare InterpretersAssociation (CHIA) have issued standardsof practice for their states (Figure 8). CHIAembarked on the development of suchstandards with funding from TheCalifornia Endowment. CHIA’s Standardsand Certification Committee reviewed andanalyzed existing practice standards andcombed both academic and health careinterpreter training literature. After acollaborative process of public review andfeedback from numerous stakeholders,CHIA released California Standards forHealthcare Interpreters: Ethical Principles,Protocols, and Guidance on Roles andIntervention in the fall of 2002. Thisdocument, also known as Standards ofPractice, is meant to serve as a reference forall health care interpreters and those who

3 0 I N T H E R I G H T W O R D S
The Endowment for Health worked withthe New Hampshire Minority HealthCoalition to develop a pilot project toimplement the following: the ongoingtraining of qualified medical interpreters,the development of a program to brokerinterpreter services, the development of atraining program to educate healthprofessionals on cultural competency anduse of a medical interpreter, and educationand outreach to health care consumerswith limited English proficiency aboutmedical interpretation. This grant will alsohelp create a formal medical interpretationadvisory committee that will overseeactivities related to intepreter services.
Promoting Advocacy and Policy ChangeDespite evidence linking language barriersand disparities, there is not universalagreement on the role interpreter servicesshould play. An example of this skeptismcan be found in the words of Dr. YankCoble, president of the American Medical
work with them. It should serve as the basisfor the development of interpreter trainingcurricula; job descriptions, performanceevaluations, and organizational policies andprocedures; and tests for California stateaccreditation, certification, or licensure.Ultimately, the goal of the Standards ofPractice is to contribute to the acceptance of health care interpreting as a recognizedprofession, subsequently leading tosustainable financing mechanisms andsatisfactory reimbursement policies (CHIA 2002).
The California Endowment has investedover $15 million to ensure equal access forLEP consumers. One of its various strategiesfocuses on improving the training andprofessionalization of medical interpreters.In addition to funding CHIA for thecreation of the Standards of Practice, it hassupported the development of interpretertraining curricula for community collegesand community-based organizations and a compendium of interpreter trainingprograms in California, which includes an analysis of trends in the state.
Figure 8. CHIA’s Standards of Practice
CHIA’s Standards of Practice consists of three main sections that guide interpretersthrough the complex task of health care interpreting. The sections include:
Section 1: This section consists of six ethical principles that guide the actions Ethical Principles of health care interpreters. Each principle has an underlying value
description followed by a set of performance measures that demonstrate how the interpreter’s action follows the principle.
Section 2: This section describes procedures standardizing how interpreters Protocols work with patients and providers in the health care encounter
before, during, and after their interaction or session.
Section 3: This section describes four roles interpreters can play in the health Complex Roles care encounter and highlights strategies for setting appropriate
boundaries.
Source: CHIA 2002.

G R A N T M A K E R S I N H E A L T H 3 1
Association, who has stated, “without abody of scientific evidence to establish itsworth, or government money to pay for it,medical interpreting is an unfunded andunaffordable frill” (Kaiser FamilyFoundation 2003). In stark contrast, theIOM recommends that “greater resourcesshould be made available by payors toprovide coverage for interpretation servicesfor limited-English proficient patients andtheir families” (IOM 2002). To promoteacceptance of interpretation in health care, foundations are working to createawareness among providers and the generalpublic about its necessity in deliveringhigh-quality care and the importance ofdeveloping sustainable financingmechanisms.
Convening Stakeholders to Advance PolicyIn 2002, The California Endowmentdeveloped the Medical Leadership Councilfor Language Access, a collaborative of 25 local medical societies, physicianspecialty associations, ethnic physicianorganizations, health systems, and healthplans working to create solutions that willimprove the provision of interpreter andtranslation services to LEP patients.4
The California Endowment convenes the council biannually to discuss howorganized medicine and health careproviders can support increased languageaccess in California. Topics thus far haveincluded models for providing languageassistance services (including the use of
technology) and the policy issues involvedwith public financing for these services.Council member organizations also engage in education and informationdissemination among their organizations’membership, through discussions atmember meetings, writing membernewsletter articles, soliciting membersurveys, and promoting continuingmedical education and trainingopportunities. Council members are paid a stipend for their participation and involvement.
In response to rising numbers of non-English speaking county residents, TheHorizon Foundation in Howard County,Maryland, convened a multidisciplinaryteam of health and human serviceproviders to explore the issue of languagebarriers to health services. Thesediscussions led directly to a joint initiativeof local community-based organizationsand the foundation to address languageand cultural barriers to health and wellnessin their community. The project willinclude: a major outreach to the county’sethnic communities; focus groups andsurveys to clarify language and cultural barriers to health; the coordination of thelocal nonprofit community to generateexpertise; and the investigation of bestpractices in translating health material,creating new lines of communication forhealth issues, and expanding overall accessto care for those with the greatest needs.
4 Council members include: American Academy of Pediatrics, District IX; California Association of Public Hospitals and Health Systems;
American College of Obstetricians and Gynecologists, District IX; American College of Physicians-American Society of Internal Medicine,
California Chapter; California Medical Association; Fresno-Madera Medical Society; Los Angeles County Medical Association; San
Francisco Medical Society; St. Joseph Health System; Sutter Health; Scripps Health (invited guest); Catholic Healthcare West; California
Academy of Family Physicians; Association of American Indian Physicians; California Association of Health Plans; Asian and Pacific
Islander American Health Forum; California Healthcare Association; California Latino Medical Association; California Primary Care
Association; Golden State Medical Association; San Diego County Medical Society; Sierra-Sacramento Valley Medical Association;
Santa Clara County Medical Association; Wellpoint Health System; and Kaiser Permanente (invited guest).

3 2 I N T H E R I G H T W O R D S
• conducting legal and policy research, • fostering the development of coalitions
that include providers and advocates, • developing a network among the
coalitions in various states, and • developing an action kit to assist coalition
participants in changing state policies forfunding interpreter services.
Each coalition will work to educate opinionleaders and policymakers on the importanceof providing interpreter services and explorethe feasibility of implementing the federalreimbursement option in their state. Localfoundations in each of the first three pilotsites have been invaluable components ofthe coalitions, providing funding as well asidentifying key stakeholders, conveningmeetings and conference calls, and workingwith immigrant rights coalition andcommunity groups.
The first in a series of local meetings took place in October 2002, with supportfrom the Mid-Iowa Health Foundation.Representatives from the foundation, TheAccess Project, and NHeLP met with inter-ested stakeholders, including the Bureau ofRefugee Services, Iowa Department ofPublic Health, Mercy Medical Center,Central Iowa Health System, State PublicPolicy Group, and Broadlawns MedicalCenter. The foundation played a key rolein organizing the meeting and enlistingcommunity members.
In New Hampshire, with the help of theEndowment for Health, over 100 individu-als attended a November 2002 meeting toexplore expanding interpreter services,since the state already takes advantage offederal matching funds. Organizers of themeeting included the New HampshireMinority Health Coalition, Southern New
In spring 2002, the Blue Cross and BlueShield of Minnesota Foundationcommissioned a statewide survey on theuse of interpreters in Minnesota. The foun-dation surveyed health and human serviceorganizations located in 44 Minnesotacounties and received a 90 percentparticipation rate. In November 2002, itconvened an invitational forum to sharethe findings of the survey and generateaction to promote the use of interpreters inMinnesota’s health care system. Thefoundation worked with the Lao AssistanceCenter of Minnesota, and the forum wasattended by 75 policymakers, collegeeducators, and health care representatives.Both the survey and the forum uncoveredthat interpreters were widely used inMinnesota (78 percent of respondents useinterpreters on staff, on a contract basis, orvia a language agency) and considered“extremely effective” in meeting thecultural and linguistic needs of LEPpatients. Organizations highlighted severalchallenges for expanding the use of interpreters, including unstable or inadequate funding, a shortage of qualifiedinterpreters, and being able to effectivelyand efficiently respond to smaller pocketsof LEP populations. The foundation is cur-rently aligning its existing grantmakingactivities to respond to these challenges.
With funding from The CommonwealthFund, The Robert Wood JohnsonFoundation, and local foundations, TheAccess Project and the National HealthLaw Program (NHeLP) are collaboratingon a project to help communities advocatefor the adoption (or enhancement) ofMedicaid/SCHIP funding for interpreterservices in their states. The projectincludes:

G R A N T M A K E R S I N H E A L T H 3 3
Hampshire Area Health Education Center,and the New Hampshire HospitalAssociation. The Endowment for Healthbegan its coalition building prior toworking with The Access Project andNHeLP, but efforts have since strengthenedas a result of this newer collaboration. Thecoalition is currently identifying its keygoals and planning its strategic direction.
Upcoming meetings are being planned forPalm Beach, Florida, with the help of theQuantum Foundation. In a recent needsassessment, the foundation identifiedlanguage access as a priority for its servicepopulation. Many of the individualsinterviewed for the survey expressedfrustration with the lack of bilingual health care services in many area hospitals(The Access Project 2002). While specificactivities are still being planned, the work will focus on implementingMedicaid/SCHIP funding for language services in Florida.
Raising Awareness and AdvancingKnowledgeThe California Endowment has recentlyembarked on a public engagementcampaign in partnership with California’sethnic media. The project will support thedevelopment, placement, and tracking ofan integrated advertising and editorial campaign targeting LEP groups. Specificcampaign activities include:
• informing consumers about the issue oflanguage access through 200 print, radio,television, and on-line ethnic mediaoutlets that target 12 linguistic groups;
• administering pre- and post-surveysmonitoring the level of awareness of theseissues among the top 12 linguisticgroups; and
• forming linkages to ongoing advocacyand systems change efforts.
There is a delicate balance to be struck inefforts to stimulate demand forinterpretation services by informingpatients of their rights, since the availabilityof these services is still so limited, especiallyin the area of rare or indigenous languages.
The Commonwealth Fund also fundedNHeLP, along with the Summit HealthInstitute for Research and Education, Inc.,to examine the legality of collecting data onrace, ethnicity, and primary language—anactivity most health plans and providersview as illegal. The report firmly stated thatcollecting such information was indeedlegal. It further noted that no federalstatute required the collection andreporting of primary language data. Thereport called upon the federal governmentto support access to quality care for LEPpopulations by promoting the collection ofprimary language in the health care setting.
Advancing ResearchThe IOM recommends that “futureresearch should identify best practiceswhere the availability of interpretationservices is limited” (IOM 2002).Foundations can play an important role inhelping communities determine whichstrategies are most effective in addressingthe language needs of their populations.While the evidence documenting the needfor language services is substantial,information about which solutions havebeen most successful and cost-effective isneeded. For this reason, several foundationsare working to increase this knowledgethrough supporting research, evaluations of current practices, and demonstrationprograms.

3 4 I N T H E R I G H T W O R D S
• grow capacity for medical interpreters inregions with new and fast-growing Latinopopulations;
• develop technologies that will enablecost-effective and accurate interpretationin the health care setting;
• create and distribute resources to build onwhat is known about medicalinterpretation;
• link relevant experts nationwide in orderto unify the field and explore the sciencebase for medical interpreting;
Demonstration Programs to DiscoverInnovative ModelsThe Robert Wood Johnson Foundation has launched Hablamos Juntos: ImprovingPatient-Provider Communication forLatinos, a $10 million dollar nationalprogram to help improve access to qualityhealth care for Latinos with limited Englishproficiency. The goal of the program is toexplore cost-effective ways for providers touse interpretation and translation indelivering services. Specific activities are to:
The Power of Film
Viewing the real-life experiences of families and the intersection of their cultures with theculture of medicine can be a powerful means for conveying the importance of services toovercome language and cultural barriers. Funded by The California Endowment, TheCommonwealth Fund, the Greenwall Foundation, and the Arthur Vining DavisFoundation, the medical education project and documentary films Worlds Apart providean intimate view of patients and physicians struggling across science and religion, language,culture, generation gaps, and family customs to come to grips with life and deathdecisions.
For participants at the Issue Dialogue, the films illustrated the inherent complexity of medical conditions and their consequences for patients and their families. In the case ofJustine, a four-year-old Laotian girl with a hole in her heart, the family was forced to weighthe need for open-heart surgery against their belief that a surgical scar would damage hernext reincarnation. In another example, Mohammad, an elderly man from Afghanistan,refused chemotherapy following surgery for stomach cancer. The chemotherapytreatment recommended by his physician was by continuous infusion, which would haveprohibited Mohammad from attending Muslim prayer services, because of therequirement to be completely clean before each prayer. His physician was unaware of thereason for his refusal until his daughter accompanied him on a visit to inquire about herfather’s deteriorating condition—six months later. By then, it was too late.
Another point that emerged from the films is the effect of medical decisions on familydynamics and structure. Justine’s mother was not the sole decisionmaker for the child, and,in fact, her grandmother had a strong role in the decision to refuse surgery. When hermother finally consented to the surgery, she was ostracized from the family for goingagainst their cultural beliefs. In Mohammad’s case, his more-assimilated daughter wasblamed for hastening her father’s death by using the word cancer to explain his illness.
(Continues on next page)

G R A N T M A K E R S I N H E A L T H 3 5
• advance an understanding of the businessimplications of medical interpreterservices in health care;
• expand the ability of plans and providersto track care by race and ethnicity; and
• explore how technology can assist inimproving language access.
Three screening criteria were used to selectproposals from interested organizations.Applicant organizations were required to:serve a catchment area home to “a new and
fast-growing” Latino population; serve themajority of Latinos in a given community;and have access to a range of delivery sites,including the emergency room, theinpatient care setting, outpatient andprimary care sites, and the pharmacysetting or the settings where other ancillaryservices are provided. In its first year offunding, the program awarded 10 sitesnationwide with planning grants of$150,000 each. Grantees have conductedneeds assessments and are taking inventory
Other family members wanted to protect him and described his diagnosis as “theproblem” or “the dark spot on the x-ray.” In both cases, the generation gap betweenolder, less-acculturated family members and younger, more-assimilated ones resulted inpainful and disruptive familial relationships.
The issues involved with medical decisions are emotionally and intellectually challengingand speak to extraordinary communication challenges in health care encounters. Whenexplaining treatment recommendations, physicians must remember to respect, as well asfully explore, the patient or family’s reluctance to choose certain procedures. Often opendialogue with the patient could uncover alternative treatments that would result infavorable clinical results while remaining sensitive to the patient’s beliefs. Alternatively,communication could be further enhanced if materials were available to educate patientsabout the right kinds of questions to ask a physician, for example, to ask whether thereare any other alternatives to the particular type of treatment being proposed. Interpreterscan be of enormous help in these situations. Well-rounded interpreter training programsaddress issues related to cultural mediation or brokering, as well as other sensitive,multilevel considerations. Interpreters learn to consider factors such as the patient’s levelof education, the extent of familial involvement, and the role of religion.
The Worlds Apart films offer tremendous opportunity for discussion about addressing thehealth care needs of a pluralistic society. A study guide will accompany the films and beused to teach medical students and health care professionals about cross-culturalcommunication and cultural sensitivity. Foundations could use the materials to engageboard members and as inspiration for exploring solutions to the problem of linguistic andcultural barriers to care.
The Worlds Apart films and a companion facilitator’s guide will be available for distribution in the fall of 2003. Please contact Maren Grainger-Monsen, M.D., producer and director, [email protected] or Raina Glazener, project coordinator, at [email protected] or650.725.9564 for details.
(Continued from previous page)

3 6 I N T H E R I G H T W O R D S
of best practices, policy analyses, bringingtogether experts in the field to forgeconsensus or meet specific objectives, or a combination of such activities.
Evaluation of Interpretation ModelsThere is little research comparing differentmethods of technological interpretationwith one another and with in-personinterpretation. Recognizing this need formore research and evaluation on effectivemodels, The Commonwealth Fund andThe California Endowment are jointlyfunding an evaluation of Center forImmigrant Health’s remote simultaneousmedical interpretation project. Arandomized controlled study will comparethe cost of using the service at full capacityto the cost of more common interpreterservices, such as in-person interpretationand telephonic interpretation. The studywill also examine associated healthoutcomes and patient satisfaction (Gany 2003).
Initial studies have seen some markedsuccess with RSMI, including a high levelof physician and patient satisfaction withthis technology. Physicians have reportedan improved ability to communicate withpatients and a corresponding improvementin their ability to diagnose illnesses,including those that rely heavily onpatient-physician communication, such asdepression. RSMI has increased accuracyand the exchange of information, withoutextending the time the physician spentwith the patient; therefore physicianefficiency was enhanced. RSMI alsoappears to be cost-effective, as comparedwith both in-person interpreting andtelephonic interpreting.
of their existing resources. Next stepsinclude developing their implementationplans and associated programrequirements.
The Commonwealth Fund is working toimprove communication and quality ofcare through its Patient Communicationand Quality of Care for UnderservedPopulations initiative. Announced in March 2003, the initiative is designed to identify causes and consequences ofpoor communication in medical settingsand to evaluate methods to addresscommunication barriers for underservedpatients, including minorities, those withlimited English proficiency, and patientswith low health literacy. As many as fivegrants of up to $125,000 each for twoyears will be awarded under this initiative.The grants will focus on communicationand improved quality of care forunderserved patients, with projects that include:
• finding the root causes ofcommunication problems at both the individual and systems levels;
• identifying the consequences of poorcommunication in areas such as patientcompliance, health outcomes, access,health service utilization, and medicalerrors;
• developing or evaluating the bestmethods for addressing communicationproblems; and
• supporting or analyzing policies toimprove health communication for theunderserved.
Project activities may include research togenerate new knowledge, work to developsolutions to currently known problems,evaluations of interventions, identification

A Business Model for ProvidingLanguage Services
Particularly in today’s economic environment, businesses make tough choices in balancingtheir social agenda with their business interests. There are four different motivating factorsthat can shape how an organization interprets its corporate responsibility. Some factorsmay be more compelling than others, such as compliance with legal requirements, buteach has its own unique considerations. These factors can be illustrated in a matrix for calculating the return on corporate responsibility (Figure 9). In applying this model to theprovision of language services, Kelvin Quan, J.D., M.P.H., CFO and general counsel atAlameda Alliance for Health, demonstrated how health care organizations and providerscould examine this issue in light of their own business practices.
Figure 9. The Virtue Matrix: Calculating the Return on Corporate Responsibility
FRONTIER
CIVIL FOUNDATIONSource: Martin 2002.
The bottom portion of the matrix comprises the civil foundation of corporate behavior.These practices promote socially responsible behavior and business interests, but do notextend beyond meeting society’s baseline expectations. In the compliance quadrant,health care organizations and providers must adhere to certain federal and state laws that
STRATEGICProfit making; Results in positive reaction from owners/constituencies
SOCIAL JUSTICEMay be contrary to owners’ interests
COMPLIANCERequired by laws, regulations
or contracts
CHOICEDictated by norms and
customs of industry/society
G R A N T M A K E R S I N H E A L T H 3 7
The Robert Wood Johnson Foundation hasconducted focus groups with its HablamosJuntos grantees to test a device known as aphraselater—a small, handheld devicedeveloped in the military that ispreprogrammed with phrases. The providerspeaks into the device, which can identifythe phrase closest to it and say it in the
language to the patient. The testing is still in the early phases, and although it is probably inadequate for complexencounters, it may have utility in certainparts of the health care setting (Dickson2003).
(Continues on next page)
3 8 I N T H E R I G H T W O R D S
promote language access. Compliance with legal requirements as the sole motivatingfactor, however, is a reactive rather than proactive approach to addressing languagebarriers. When organizations think only in terms of compliance, there is the risk ofcreating a “race to the bottom” mentality that stifles creativity and innovation and resistsfurther expansion. From the choice quadrant, an entity may choose to undertake a newinitiative that is spurred by industry norms, such as offering health care benefits to employ-ees’ dependents. By not meeting industry norms, the entity suffers competitively by itsomission. Unfortunately, language services are not the industry standard in the currenthealth care market, as reflected in the relatively few health care organizations andproviders that offer them.
The top portion of the matrix represents the broader frontier. It encompasses practicescompanies engage in because they consider them the right things to do. In the socialjustice quadrant, these initiatives benefit society, but they may have negativeconsequences for the organization or no apparent value to business interests. Whilelanguage services may promote quality of care and ultimately contribute to the eliminationof health disparities, organizations may not see them as producing greater efficiency orcost savings. Such conclusions often provide justification for not initiating language services.Some organizations may be motivated by social justice considerations and respond to thevalue placed on certain services by the community. These organizations are in theminority when it comes to language access. Where practices may not appear to be in theorganization’s interests but are motivated by social values, as can be the case for languageservices, organizational leadership is essential to their successful and sustained implementa-tion.
In the most ideal circumstances, a business case can be made for practices that are alsoconsistent with corporate social responsibility, by either improving the bottom line orhelping to capture a greater market share. When considering language services in thestrategic quadrant, some organizations believe that these services will reduce unnecessarytesting and may reduce medical errors that can result in misdiagnosis, suboptimal care, and lawsuits. Linguistic services may also promote patient satisfaction and the willingnessto return to facilities that provide interpreters, resulting in a favorable public image andincreased corporate value. This motivating factor has the greatest potential for growth and creativity as organizations develop new ways to attract consumers and offer the best services.
Philanthropy can play a role in promoting language access in each of these four quadrants.They can support and inform the development and implementation of sound laws andregulations; promote the concept of social justice; and work to make language services anindustry standard. Foundations can also support efforts to document the business case forproviding language services, including studies to determine the cost-benefit of linguisticservices and to strengthen the evidence base showing that language access can have apositive return on investment.
(Continued from previous page)

G R A N T M A K E R S I N H E A L T H 3 9
ConclusionThe growth of populations with limitedEnglish proficiency and the creation ofrelated legal requirements and guidelineshave increased consciousness of the issue of language access. As providers andcommunities struggle to care for these populations, the field is ripe withopportunities for foundations to getinvolved and contribute to the growingbody of knowledge around these issues.Philanthropy can take a significantleadership role in these efforts bypartnering with local community groups,educating policymakers and health careorganizations, and reaching out toimmigrant and minority populations. As this report points out, there are a varietyof activities that foundations could chooseto pursue, including:
• promoting awareness among providersabout the importance of language servicesand their obligation to provide them, aswell as equipping them with resources,such as medical education andexperiential learning opportunities, toenable them to better serve their patients;
• facilitating agreements among healthplans to create an industry standard forcovering the costs of professionalinterpretation;
• developing and broadly disseminatinghigh-quality health education materials in multiple languages;
• tapping into resources outside of theU.S., such as materials already translatedin other countries, to strengthen the workdone here;
• increasing public awareness of theavailability of interpreter services andempowering patients with informationon what types of questions to ask in thehealth care encounter;
• building the field of professional medicalinterpretation through enhancededucational opportunities, standardsdevelopment, and recognition ofinterpreters as integral to the health care team;
• developing an agenda for long-termsustainable funding and for greaterutilization of existing funding, such as federal matching grants for stateMedicaid programs;
• building the business case andencouraging the development of newfinancing mechanisms that could lead to the establishment of standardreimbursement policies;
• creating awareness within communitiesabout the issue of language access andworking with community members,policymakers, and government officials to support policies that guarantee equalaccess to linguistic services;
• supporting financial incentives thatencourage the use of interpreters, both at the policy level and at the institutionallevel;
• helping communities explore systemschange and policy development to ensurethe sustainability of initial investments,including seed money provided forinterpreter training and certification;
• supporting research to identify andevaluate the most effective modes ofdelivering language services in specificcommunities, including technologicaladvancements;

4 0 I N T H E R I G H T W O R D S
By filling this needed leadership role,foundations can help shape the languageaccess agenda to ensure that all patientshave equal access to quality health care and thus take important steps towardeliminating racial and ethnic disparities in health.
• using grants as a mechanism foradvancing the field by puttingstipulations into awards that granteesmust incorporate cultural competenceinto their projects; and
• working with nontraditional partners,such as anthropologists and arts councils,to better understand how culturalpractices influence health.

G R A N T M A K E R S I N H E A L T H 4 1
ReferencesThe Access Project, and National HealthLaw Program, Language Services Action Kit:Interpreter Services in Health Care Settingsfor People with Limited English Proficiency(Boston, MA: June 2003).
The Access Project, Health Care Access Issue in Palm Beach County (Boston, MA:February 2002).
Anderson, Charles, LinguisticallyAppropriate Access and Services: AnEvaluation and Review for HealthcareOrganizations (Santa Rosa, CA: NationalCouncil on Interpreting in Health Care:June 2002).
Andrulis, Dennis, Lisa Duchon, andHailey Reid, Dynamics of Race, Culture,and Key Indicators of Health In the Nation’s100 Largest Cities and Their Suburbs(Brooklyn, NY: State University of NewYork Downstate Medical Center, February2003).
Andrulis, Dennis, Nanette Goodman, and Carol Pryor, What a Difference anInterpreter Can Make: Health CareExperiences of Uninsured with LimitedEnglish Proficiency (Boston, MA: TheAccess Project, April 2002).
Beltran Avery, Maria-Paz, EducationDevelopment Center, remarks atGrantmakers In Health Issue Dialogue,In the Right Words: Addressing Languageand Culture in Providing Health Care, April 4, 2003.
California Healthcare InterpretersAssociation, California Standards forHealthcare Interpreters: Ethical Principles,Protocols, and Guidance on Roles andIntervention (Los Angeles, CA: 2002).
California Primary Care Association,Providing Health Care to Limited EnglishProficient Patients: A Manual of PromisingPractices (Sacramento, CA: February 5,2002).
Chen, Alice, Asian and Pacific IslanderAmerican Health Forum, remarks atGrantmakers In Health Issue Dialogue,In the Right Words: Addressing Languageand Culture in Providing Health Care, April 4, 2003.
Civil Rights Act of 1964, 42 U.S.C. §2000d (1964).
Crane, J.A., “Patient Comprehension of Doctor-Patient Communication onDischarge from the Emergency RoomDepartment,” Journal of EmergencyMedicine 15(1):1-7, 1997.
Dickson, Pamela, The Robert WoodJohnson Foundation, remarks atGrantmakers In Health Issue Dialogue, In the Right Words: Addressing Languageand Culture in Providing Health Care, April 4, 2003.
Dodd, Aileen, “Foreign Doctors, NursesStart Over, Activists Want to StreamlineLicensing” Atlanta Journal-Constitution,November 5, 2002, p. B-1.

4 2 I N T H E R I G H T W O R D S
Grainger-Monsen, Maren M., StanfordUniversity, Center for Biomedical Ethics,remarks at Grantmakers In Health IssueDialogue, In the Right Words: AddressingLanguage and Culture in Providing HealthCare, April 4, 2003.
Green, Carola, Vista Community Clinic,remarks at Grantmakers In Health IssueDialogue, In the Right Words: AddressingLanguage and Culture in Providing HealthCare, April 4, 2003.
Hampers, Louis C., Susie Cha, David J.Gutglass, et al., “Language Barriers andResource Utilization in a PediatricEmergency Department,” Pediatrics103(6):1253-1256, 1999.
Hernandez, Terry M., Mid-Iowa HealthFoundation, remarks at Grantmakers InHealth Issue Dialogue, In the Right Words:Addressing Language and Culture inProviding Health Care, April 4, 2003.
Huang, Vivian, California Primary CareAssociation, remarks at Grantmakers InHealth Issue Dialogue, In the Right Words:Addressing Language and Culture inProviding Health Care, April 4, 2003.
Institute of Medicine, Unequal Treatment:Confronting Racial and Ethnic Disparities(Washington, DC: National AcademyPress, 2002).
IQ Solutions, Inc., National Standards forCulturally and Linguistically AppropriateServices in Health Care Final Report, reportto the Office of Minority Health, U.S.Department of Health and HumanServices under Contract No. 282-99-0039(Rockville, MD: March 2001).
Downing, Bruce, and Cynthia Roat,Models for the Provision of Language Accessin the Health Care Setting (Santa Rosa, CA:National Council on Interpreting inHealth Care, March 2002).
Downs-Karkos, Susan, The ColoradoTrust, personal communication toGrantmakers In Health, March 4, 2003.
Families USA Foundation, “CulturalCompetence in Health Care,” States ofHealth 5(4):1-3, May 1995.
Feinberg, Emily, Katherine Swartz, AlanM. Zaslavsky, et al., “Language Proficiencyand the Enrollment of Medicaid-EligibleChildren in Publicly Funded HealthInsurance Programs,” Maternal and ChildHealth Journal 6(1):5-18, March 2002.
Fiscella, Kevin, Peter Franks, Mark P.Doescher, and Barry G. Saver, “Disparitiesin Health Care By Race, Ethnicity, andLanguage Among the Uninsured,” Medical Care 40:52-59, 2002.
Flores, George, Barton Laws, SandraMayo, et al., “Errors in MedicalInterpretation and Their Potential ClinicalConsequences in Pediatric Encounters,”Pediatrics 111(1):6-14, January 2003.
Gany, Francesca, Center for ImmigrantHealth, personal communication toGrantmakers In Health, March 11, 2003.
Ghandi, Tejal K., Helen R. Burstin, E.Francis Cook, et al., “Drug Complicationsin Outpatients,” Journal of General InternalMedicine 15:149-154, 2000.

G R A N T M A K E R S I N H E A L T H 4 3
Jacobs, Elizabeth, and Gayle Goldin, A Volunteers in Health Care Guide toOvercoming Language Barriers (Pawtucket,RI: Volunteers in Health Care, 2002).
Kaiser Family Foundation, “Wall StreetJournal Examines Issues SurroundingMedical Interpretation,” Kaiser DailyHealth Policy Report, January 9, 2003.
Katz, Michael, Centers for Medicare and Medicaid Services, personalcommunication to Grantmakers In Health, March 21, 2003.
Kieu, Quynh, The HealthCare Foundation for Orange County, remarks at Grantmakers In Health Issue Dialogue, In the Right Words: Addressing Languageand Culture in Providing Health Care, April 4, 2003.
Little Hoover Commission, We The People:Helping Newcomers Become Californians(Sacramento, CA: June 2002).
Martin, Roger, “The Virtue Matrix:Calculating the Return on CorporateResponsibility,” Harvard Business Reviewpp. 69-75, March 2002.
Morse, Ann, “Language Access: GivingImmigrants a Hand on Navigating theHealth Care System,” State Health Notes23(381), October 7, 2002.
National Center for Cultural Competence,“Rationale for Cultural Competence inPrimary Health Care,” Policy Brief 1(Washington, DC: Winter 1999).
National Council on Interpreting inHealth Care, The Role of the Health CareInterpreter: An Evolving Dialogue (SantaRosa, CA: April 2001).
National Council on Interpreting inHealth Care, Models for the Provision of Health Care Interpreter Training (SantaRosa, CA: February 2002).
National Health Law Program, EnsuringLinguistic Access in Health Care Settings:Legal Rights and Responsibilities(Washington, DC: January 1998).
Office of Civil Rights, U.S. Department of Health and Human Services, “PolicyGuidance on the Prohibition AgainstNational Origin Discrimination as ItAffects Persons with Limited EnglishProficiency,” Federal Register 67(22):4968-4982, February 1, 2002.
Office of Management and Budget, Reportto Congress: Assessment of the Total Benefitsand Costs of Implementing Executive OrderNo. 13166: Improving Access to Services forPersons with Limited English Proficiency(Washington, DC: March 14, 2002).
Office of Minority Health, U.S.Department of Health and HumanServices, “National Standards on Culturallyand Linguistically Appropriate Services(CLAS) in Health Care,” Federal Register65(247):80865-80879, December 22,2000.
Partida, Yolanda, Hablamos JuntosNational Program Office, remarks atGrantmakers In Health Issue Dialogue, In the Right Words: Addressing Languageand Culture in Providing Health Care, April 4, 2003.

4 4 I N T H E R I G H T W O R D S
U.S. Census Bureau, Coming to America: A Profile of the Nation’s Foreign-Born (2000 Update) (Washington, DC: February 2002c).
U.S. Department of Justice, “ExecutiveOrder 13166—Improving Access toServices for Persons with Limited English Proficiency,” Federal Register65(159):50121-50122, August 16, 2000.
Warren, Judith, The Health Foundation of Greater Cincinnati, personalcommunication to Grantmakers In Health, February 10, 2003.
Weech-Maldonado, Robert, Leo S.Morales, Karen Spritzer, et al., “Racial andEthnic Differences In Parents’ Assessmentsof Pediatric Care in Medicaid ManagedCare,” Health Services Research 36(3):575-594, 2001.
Youdelman, Mara, and Jane Perkins,Providing Language Interpretation Servicesin the Health Care Setting: Examples Fromthe Field (Washington, DC: NationalHealth Law Program, May 2002).
Perez-Stable, Eliseo, Anna Napoles-Springer, and J.M. Miramontes, “TheEffects of Ethnicity and Language onMedical Outcomes of Patients withHypertension or Diabetes,” Medical Care 35(12):1212-1219, 1997.
Pulley, Barbara, QueensCare, remarks atGrantmakers In Health Issue Dialogue, In the Right Words: Addressing Languageand Culture in Providing Health Care, April 4, 2003.
Quan, Kelvin, Alameda Alliance forHealth, remarks at Grantmakers In HealthIssue Dialogue, In the Right Words:Addressing Language and Culture inProviding Health Care, April 4, 2003.
U.S. Census Bureau, “Census 2000Summary File 3, Matrices P19, P20,PCT13, and PCT14,”<http://factfinder.census.gov>, February 25, 2003a.
U.S. Census Bureau, “Census 2000Summary File 3, Matrix PCT 10,”<http://factfinder.census.gov>, February 25, 2003b.
U.S. Census Bureau, Coming From theAmericas: A Profile of the Nation’s Foreign-Born Population From Latin America (2000 Update) (Washington, DC: January 2002a).
U.S. Census Bureau, A Profile of theNation’s Foreign-Born Population From Asia (2000 Update) (Washington, DC:February 2002b).

1100 connecticut avenue, nwsuite 1200washington, dc 20036tel: 202.452.8331 fax: 202.452.8340www.gih.org