
in Management of Renal Stones
5
nr. 3 / 2019 • vol 18 Romanian Journal of Urology 29 Clinical studies Initial Experience Using the Minimal Invasive Percutaneous Nephrolitholapaxy Technique in Management of Renal Stones H. Muresanu 1,2 , A. Grelus 1,2 , I. Ioiart 1,2 1 Department of Urology, Arad County Emergency Clinical Hospital, Arad, Romania 2 Faculty of Medicine, “Vasile Goldis” Western University of Arad, Romania Correspondence to: Dr. Grelus Alin, M.D. Arad County Emergency Clinical Hospital, Department of Urology 2-4 Andreny Karoly st, code 310037, Arad, Romania Tel: +40770219973 e-mail: [email protected] Abstract Introduction and Objectives. The aim of this subject is to present the results of the initial experience with the mini- mal invasive percutaneous nephrolitoholapaxy (MIP) technique in the Urology Clinic from SCJU Arad. Materials and Methods. The Urology Clinic from SCJU Arad, reported 15 cases of renal and ureteral lithiasis who un- derwent MIP technique between November 2018 – February 2019. All patients signed the informed consent, blood and urine samples were collected preoperatively, in order to assess the biological status of patients. Stone size (largest diameter) was measured on x-ray, the strategy of intervention was planned by consulting the urographic or comput- ed tomographic images, by case. Interventions were performed under spinal anesthesia and prophylactic antibiotics were administered to all patients preoperatively. An 16 Ch Storz nephroscope was used, lithotripsy being achieved with an 30 W Ho:YAG Auriga QI laser, finally a 14 Ch – balloon nephrostomy was inserted. Results. The mean age of patients was 48 years (range 24 – 72 years), the mean operative time was 47 minutes (range 35 - 59 minutes). Patients had a single stone, either located in the renal pelvis or in the middle and lower calyces. Par- ticular cases: one case of horseshoe kidney, one case of surgical solitary kidney, one case of sepsis with patient under anticoagulant treatment, one case of pregnancy, one case of bilateral staghorn calculi with chronic renal disease and one case of stone located on the lumbar ureter. The mean stone size was 14 mm (range 8 mm - 20 mm), except the case of bilateral staghorn calculi (3.4 – 5 cm diameter, 80 minutes). The clinical and biological status of patients, an- alyzed postoperatively, showed no significant hemorrhage, one cases complicated with acute pyelonephritis, stone free rate was achieved in percent of 87.4%, nephrostomy ablation time between 24-48, mean hospitalization time 4 days, better tolerance and low pain for smaller nephrostomy tubes. Conclusions. MIP technique is a better alternative in the treatment of small and medium size renal stones. The post- operative complications are minimal, and the stone free rate is similar to classic percutaneous nephrolithotomy, also in selected cases and with surgeon’s experience, MIP can exceed the contraindications, in order achieve maximal therapeutic results. Key-words: minimally invasive percutaneous nephrolitholapaxy; nephrolithiasis; percutaneous nephrolithotomy.
Transcript of in Management of Renal Stones

nr. 3 / 2019 • vol 18 Romanian Journal of Urology 29
Clin
ical
stu
diesInitial Experience Using the Minimal Invasive
Percutaneous Nephrolitholapaxy Technique in Management of Renal Stones
H. Muresanu 1,2, A. Grelus1,2, I. Ioiart1,2
1 Department of Urology, Arad County Emergency Clinical Hospital, Arad, Romania2 Faculty of Medicine, “Vasile Goldis” Western University of Arad, Romania
Correspondence to: Dr. Grelus Alin, M.D. Arad County Emergency Clinical Hospital, Department of Urology 2-4 Andreny Karoly st, code 310037, Arad, Romania Tel: +40770219973 e-mail: [email protected]
Abstract
Introduction and Objectives. The aim of this subject is to present the results of the initial experience with the mini-mal invasive percutaneous nephrolitoholapaxy (MIP) technique in the Urology Clinic from SCJU Arad.
Materials and Methods. The Urology Clinic from SCJU Arad, reported 15 cases of renal and ureteral lithiasis who un-derwent MIP technique between November 2018 – February 2019. All patients signed the informed consent, blood and urine samples were collected preoperatively, in order to assess the biological status of patients. Stone size (largest diameter) was measured on x-ray, the strategy of intervention was planned by consulting the urographic or comput-ed tomographic images, by case. Interventions were performed under spinal anesthesia and prophylactic antibiotics were administered to all patients preoperatively. An 16 Ch Storz nephroscope was used, lithotripsy being achieved with an 30 W Ho:YAG Auriga QI laser, finally a 14 Ch – balloon nephrostomy was inserted.
Results. The mean age of patients was 48 years (range 24 – 72 years), the mean operative time was 47 minutes (range 35 - 59 minutes). Patients had a single stone, either located in the renal pelvis or in the middle and lower calyces. Par-ticular cases: one case of horseshoe kidney, one case of surgical solitary kidney, one case of sepsis with patient under anticoagulant treatment, one case of pregnancy, one case of bilateral staghorn calculi with chronic renal disease and one case of stone located on the lumbar ureter. The mean stone size was 14 mm (range 8 mm - 20 mm), except the case of bilateral staghorn calculi (3.4 – 5 cm diameter, 80 minutes). The clinical and biological status of patients, an-alyzed postoperatively, showed no significant hemorrhage, one cases complicated with acute pyelonephritis, stone free rate was achieved in percent of 87.4%, nephrostomy ablation time between 24-48, mean hospitalization time 4 days, better tolerance and low pain for smaller nephrostomy tubes.
Conclusions. MIP technique is a better alternative in the treatment of small and medium size renal stones. The post-operative complications are minimal, and the stone free rate is similar to classic percutaneous nephrolithotomy, also in selected cases and with surgeon’s experience, MIP can exceed the contraindications, in order achieve maximal therapeutic results.
Key-words: minimally invasive percutaneous nephrolitholapaxy; nephrolithiasis; percutaneous nephrolithotomy.

Romanian Journal of Urology nr. 3 / 2019 • vol 1830
Clin
ical
stu
dies Introduction and Objectives
Nephrolithiasis is characterized as a chronic and morbid disease, with high incidence during world-wide population, which involves bio-umoral and lo-co-regional factors, who favors development and pro-gression of lithogenesis [1]. Considering the urgency and high morbidity state of this disease, various min-imal invasive treatment methods have developed over the years. In the early 1980’s, percutaneous nephroli-thotomy replaced open surgery in the majority of re-nal stone treatments [2]. However, this minimal invasive technique, can end up with various procedure - related accidents and complications like hemorrhage, effrac-tions, which can increase the patients morbidity and can prolong the hospital stay [3]. To reduce the disadvan-tages of conventional percutaneous nephrolithotomy, an MIP technique was developed in 2005 by Prof. MD Udo Nagele, which implies an ergonomic redesigning of smaller instruments and usage of pressure manage-ment for stone extraction with the “whirlpool effect”, avoiding peak pressures above 30 cmH2O, to prevent renal reflux and fluid overload [4]. This technique offers the following advantages: a single step dilatation, auto-matic pressure manage-ment, stone extraction through “whirlpool ef-fect”, optional closure of the access tract using a gelatin thrombin matrix. Also this technique has spread it’s indications regarding stone size, to 6-12 mm stones located in the inferior calyces, cannot be enhanced by flexible URSR, being also available for renal pel-vic stones larger than 24 mm. Other indications in-clude: diverticular stones, anatomical variations and persistence of stones after ESWL [5].
Materials and MethodsThis is a retrospective
study which analyzed 15 cases of renal lithiasis in the Urology Clinic from SCJU Arad, who under-
went percutaneous nephrolithotomy – MIP technique between November 2018 – February 2019. All patients signed the informed consent, blood and urine samples were collected preoperatively, in order to assess the biological status of patients. Erythro cyte suspension was prepared for all pa tients before surgery. Stone size (largest diameter) was measured on x-rays or by summing the measurements of multiple stones, the strategy of intervention was planned by consulting the urographic or computed tomographic images, by case. Interventions were performed under spinal anesthesia and prophylactic antibiotics were administered to all patients preoperatively. After puncturing the calyces, urine samples were collected for culture, in case of purulent stasis, the intervention was temporized, and a nepthrostomy was inserted for drainage. An 16 Ch Storz nephroscope was used, lithotripsy was achieved with an 30 W Ho:YAG Auriga QI laser, finally a 14 Ch – balloon nephrostomy was inserted. Complete blood count and blood serum creatinine of patients were an-alyzed first postoperative day.
Figure1. Position of the 16 Fr Nephroscope
with laser lithotripsie

nr. 3 / 2019 • vol 18 Romanian Journal of Urology 31
Clin
ical
stu
dies
Results The mean age of patients was 48 years (range 24
– 72 years), the mean operative time was 47 minutes (range 35 - 59 minutes). Patients had a single stone, either located in the renal pelvis or in the middle and lower calyces. Particular cases: one case of horseshoe kidney, one case of surgical solitary kidney, one case of sepsis with patient under anticoagulant treatment, one case of pregnancy and one case of bilateral staghorn calculi with chronic renal disease and one case of stone located on the lumbar ureter. The mean stone size was 14 mm (range 8 mm - 20 mm), except 1 case of bilater-al staghorn calculi (3.4 – 5 cm diameter, 80 minutes). The clinical and biological status of patients analyzed postoperatively, showed no significant hemorrhage, one complicated case with acute pielonephritis, stone free rate was achieved in percent of 87.4%, nephrosto-my ablation time between 24-48, mean hospitalization time 4 days, better tolerance and low pain for smaller nephrostomy tubes.
DiscussionsPlanning of intervention is the key factor for ther-
apeutic success and high stone free rate [6]. Stone size (largest diameter) was measured on x-rays or by sum-ming the measurements of multiple stones, the strat-egy of intervention was performed by consulting the
urographic or computer tomographic images, by case. Access to pelvic and lower calyceal stones is made by puncturing the lower calyces, followed by a simple dila-tation without complications (effractions, hemorrhage)
[7]. MIP may provide non traumatic and effective stone treatment with low complications due to: smaller in-struments, a single step dilatation, automatic pressure management, stone extraction through “whirlpool ef-fect”, possibility for insertion of smaller nephrostomy tubes or even closure of the access tract using a gelatin thrombin matrix [4]. In our case the clinical and biologi-cal status of patients analyzed postoperatively, showed no significant blood loss that needed transfusion, only one case complicated with acute pyelonephritis, which will be discussed at particular cases, nephrostomy ab-lation time was between 24-48, mean hospitalization time 4 days, patients had better tolerance and low pain for smaller nephrostomy tubes, we used 14 Ch balloon nephrostomy tubes.
Indications for MIP include the following: to 6-12 mm stones located in the inferior calyces, that cannot be enhanced by flexible URSR, renal pelvic stones larg-er than 24 mm, calculus persistence following ESWL [8]. In our cases, patients had a single stone, either located in the renal pelvis or in the middle and lower calyces, and one case of bilateral staghorn calculi and one case of stone located on the lumbar ureter. The mean stone size was 14 mm (range 8 mm - 20 mm), except the case of bilateral staghorn calculi (3.4 – 5 cm diameter).
When referring to op-eration time Prof. MD Udo Nagele states that mean operation time has dropped when compared to miniaturized PCNL (mini PCNL), because of the “whirl pool” effect of extracting the stone frag-ments, also hospitalization time has been reduced and patients’ satisfaction has risen significantly [9]. In our case the mean operative time was 47 minutes (range 35 - 59 minutes), except the case of bilateral staghorn calculi (3.4 – 5 cm diameter, 80 minutes).
MIP proves to be supe-rior to Flexible URSR and
Figure 2. Position of the 14 Ch Baloon Nephrostomy

Romanian Journal of Urology nr. 3 / 2019 • vol 1832
Clin
ical
stu
dies ESWL in terms of stone free rate [10]. In our case Stone
free rate was achieved in percent of 87.4%, nephrosto-my ablation time between 24-48, mean hospitalization time 4 days, better tolerance and low pain for smaller nephrostomy tubes.
Contra indications for MIP include: coagulation dis-orders, pregnancy, urinary tract infections, and extreme obesity [10]. Although considering the contraindications we have encountered particular cases such as: one case of sepsis with patient under anticoagulant treatment, one case of pregnancy, also other particular cases: one case of horseshoe kidney, one case of surgical soli-tary kidney one case of bilateral staghorn calculi with chronic renal disease and one case of stone located on the lumbar ureter, which will be discussed individually.
A case of 72 year old female patient with multiple comorbidities of fibrillation, cardiac insufficiency, dia-betes type II, on anticoagulant treatment with Sintrom 4 mg 1/day, transferred from Internal Medicine to our department for urosepsis from an obstructive left renal pelvic stone (2 cm diameter), needed emergency urine derivation, a 12 Ch nephrostomy tube was inserted in the middle calyces, urine samples were collected for culture , and antibiotics were administered after cul-ture results. In the third day, because of the comorbid-ities and anesthetic risk ASA 3 in local anesthesia we decide to extract the stone through MIP, after Laser Lithotripsie, 14 Ch nephrostomy tube was inserted. Although the patient was on anticoagulant treatment, we had minimal bleeding, no need for transfusion after surgery, stone free rate 95% (a small fragment migrat-ed in the inferior calyces). Nephrostomy ablation time 72 h, hospitalization stay - 7 days. After a week the pa-tient was re-admitted with acute pyelonephritys, the fragment from the left inferior calyces migrated on the ureter, double j stent was inserted, the fragment was extracted by URSR.
A case of 27 years old female patient with pregnan-cy (7 months), got intermitted for urosepsis from an obstructive right pelvic stone (1.7 mm diameter), a 12 Ch nephrostomy tube was inserted, urine was collect-ed for culture, antibiotics were administered. After one week, in local anesthesia we performed MIP, through the nephrostomy pathway, with complete stone re-moval, 14 Ch nephrostomy tube was inserted. Again no need for transfusion after surgery, urine culture was sterile, nephrostomy ablation time 48 h, hospitalization time 10 days.
A case of 32 years old male patient with surgical sol-itary left kidney, who had right laparoscopic nephrec-
tomy in our center for right congenital hydronephrosis grade 5 with unfunctional kidney, got intermitted for grade 3 congenital hydronephrosis on the left side, and secondary pelvic stone (1,3 mm diameter). Endopielo-tomy was performed, and complete stone extraction by MIP with laser lithotripsie. 14 Ch nephrostomy tube was inserted. No need for transfusion after surgery, urine culture was sterile, nephrostomy ablation time 48 h, hospitalization time 4 days. Risk of hemorrhage and renal insufficiency on solitary kidney were minimalized.
A case of 62 year old male patient, with chronic re-nal disease stage 3 (creatinine 12 mg/dl), with bilateral staghorn calculi and acute pyelonephritis. After a right 12 Ch nephrostomy tube and a left double J stent was inserted, antibiotherapy and three episodes of dialysis, creatinine levels decreased at 4 mg/dl, we performed bilateral MIP for complete staghorn calculi, with mul-tiple pathways, three on the right side and one on the left side. After four episodes of surgery, the patient was transfused 2 times, due to his secondary anemia, the stone free rate was 80% on the left kidney, and 93% on the right kidney, bilateral double J stent was inserted.
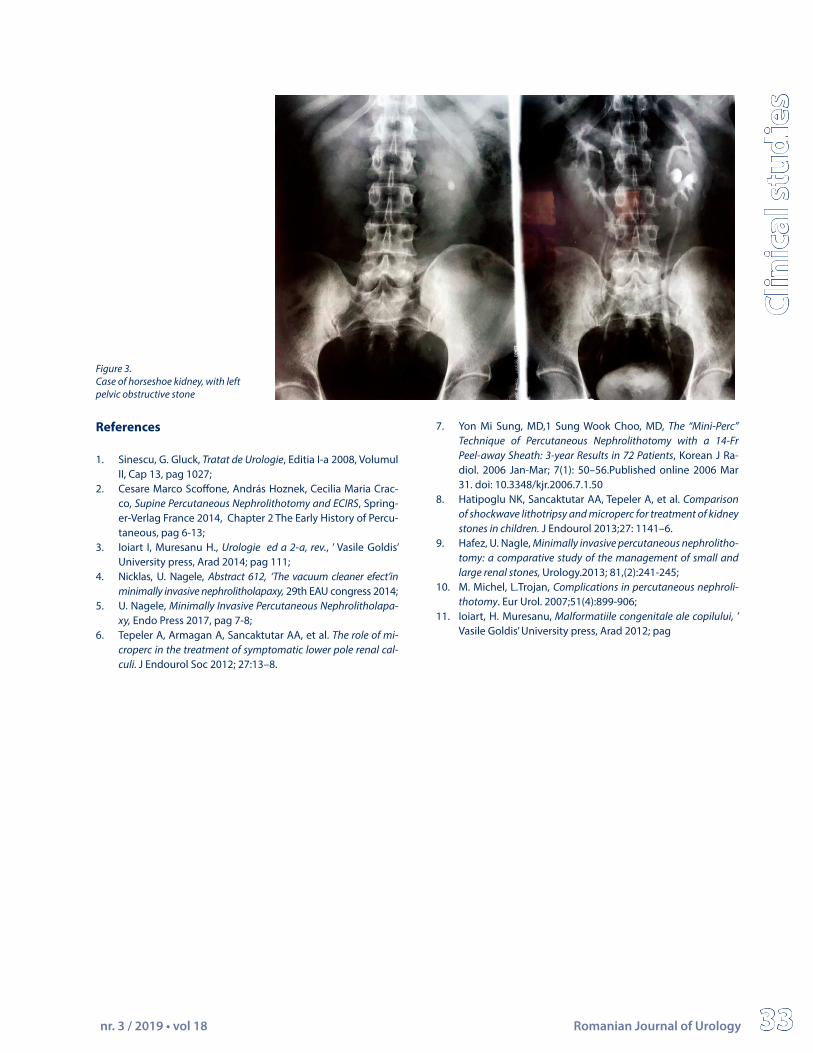
A case of 42 years old male with particular anatom-ic position of horseshoe kidney, got intermitted in our clinic for left hydronephrosis from an obstructive pelvic stone (20 mm diameter). Radiological particularity of horseshoe kidney refers to abnormal approach of the two renal masses at the inferior pole, and abnormal ori-entation of the calyces, from the usual posterior plan
[11]. Although, MIP was performed through the left pos-terior middle calyces, with complete removal of stone fragments. No transfusion was needed after surgery, urine culture was sterile, Nephrostomy ablation time 48 h, hospitalization time 4 days.
Conclusions“MIP” technique of percutaneous nephrolithoto-
my is a better alternative in the treatment of small and medium size renal stones. The postoperative complica-tions are minimal, and the stone free rate is similar to classic percutaneous nephrolithotomy, also in selected cases and with surgeon’s experience, MIP can exceed the contraindications, in order achieve maximal ther-apeutic results.
nr. 3 / 2019 • vol 18 Romanian Journal of Urology 33
Clin
ical
stu
dies
References
1. Sinescu, G. Gluck, Tratat de Urologie, Editia I-a 2008, Volumul II, Cap 13, pag 1027;
2. Cesare Marco Scoffone, András Hoznek, Cecilia Maria Crac-co, Supine Percutaneous Nephrolithotomy and ECIRS, Spring-er-Verlag France 2014, Chapter 2 The Early History of Percu-taneous, pag 6-13;
3. Ioiart I, Muresanu H., Urologie ed a 2-a, rev., ’ Vasile Goldis’ University press, Arad 2014; pag 111;
4. Nicklas, U. Nagele, Abstract 612, ‘The vacuum cleaner efect’in minimally invasive nephrolitholapaxy, 29th EAU congress 2014;
5. U. Nagele, Minimally Invasive Percutaneous Nephrolitholapa-xy, Endo Press 2017, pag 7-8;
6. Tepeler A, Armagan A, Sancaktutar AA, et al. The role of mi-croperc in the treatment of symptomatic lower pole renal cal-culi. J Endourol Soc 2012; 27:13–8.
7. Yon Mi Sung, MD,1 Sung Wook Choo, MD, The “Mini-Perc” Technique of Percutaneous Nephrolithotomy with a 14-Fr Peel-away Sheath: 3-year Results in 72 Patients, Korean J Ra-diol. 2006 Jan-Mar; 7(1): 50–56.Published online 2006 Mar 31. doi: 10.3348/kjr.2006.7.1.50
8. Hatipoglu NK, Sancaktutar AA, Tepeler A, et al. Comparison of shockwave lithotripsy and microperc for treatment of kidney stones in children. J Endourol 2013;27: 1141–6.
9. Hafez, U. Nagle, Minimally invasive percutaneous nephrolitho-tomy: a comparative study of the management of small and large renal stones, Urology.2013; 81,(2):241-245;
10. M. Michel, L.Trojan, Complications in percutaneous nephroli-thotomy. Eur Urol. 2007;51(4):899-906;
11. Ioiart, H. Muresanu, Malformatiile congenitale ale copilului, ’ Vasile Goldis’ University press, Arad 2012; pag
Figure 3. Case of horseshoe kidney, with left pelvic obstructive stone


















