in Internal Medicineassume that specific indications predicate similar therapeutic4 actions...
123
;4, Approvr Ic-ro D is~d l, o iliho;td in Internal Medicine PoProduced by FYrr r VOL IV N() 9 September 1971 NATIONAL TECHN!CAL INFORMATION SERVICE 1itinofl.d, Va 722,3 C--[s ii, )
Transcript of in Internal Medicineassume that specific indications predicate similar therapeutic4 actions...

;4,
Approvr Ic-roD is~d l, o iliho;td
in Internal MedicinePoProduced by
FYrr r
VOL IV N() 9 September 1971 NATIONAL TECHN!CALINFORMATION SERVICE1itinofl.d, Va 722,3
C--[s ii, )

Security Classification . 1DOCUMET CONTROL DATAR- & D.
rSecuwtly classificationm of title, body of abafroct and indiexinj annotation must be entered when the *retail report is classified;I. ORIGINATING ACTIVITY (Cooperate* WAe) as. REPORT S'ECURITY CLASSIFICATIONIDepartment of Medicine 2. GROUP
3. REPORT TITLE
NEPHK)LOGY SYMPOSIUM
VOL IV NO 9, SEPTM BER 1971. PRESENT CONCEPTS IN IMTEAL ETDIcin;* (See -tem fii)O. ESCRIPTIVE NOTES (2T'pe of feuh and inchiage datea)
Symposium (medical) September 1971S - AU THOR(S) fFilet now. Middle Sh eitif seaChojnacl(1, Ricbard E. (destEAitor). Contributors: Rubini IE, Cnojnaciti RE,Conger JD, Steinmuller SR, Schwartz AB, Cong, r MR, Shinaberg JH.
.REPORT DATE VA. TOTAL NO. OF PAGES 21. NO. OF REFS
"September 1971 n7 (pp 705-821) 92
€ONTRACT OR GRANT NO i. ORIGINATOR'S REPORT NU&MEMRS)
6. PROJECT NO.
C. ob. OTH4eR REPORT NOM (Ati o•oberpieiet moe be aeeial&dale Ie~tm )
10. OSSTR*ISTION STATEMENT
The distribution of this document is unlimited.
III. SUPPLEMENTARY NOTES 12. SPONSORI~iG NiLTlA*V-4C-YIMIT-
There are 12 symposia per year and these LETTEWAN GENERAL HOSIWLcompose one volume. BEach symposium is on I Presidio o° San Frcncisco, Calif 94129
irespK alty in the field of interna'W"ASJkSTRA C
"%The papers in this issue of Present Concepts offer insight into both broad andspecialized areas of Nephrology. In several presentations, comprehensive reviews,not elsewhere available, are presented. A mixture of theoretical and practical ideashas been embodied in the majority of articles so that understanding vould precedefuture decision in any of these areas.
)The first article is another approach to the problem of fluid and electrolytebalance correction of pathologic deviations. Cookbook types of therapy are szecifi-cally not included since they have little value to the individual patient. Sufficientemphasis is made on basic concepts so as to enable rational decision. The physicisn'spresentation of his experience in caring for acute renal failure patients off thecoast of Vietnam is both rewarding and disillusioning since post-trauratic renalfailure is associated with excessive mortality. The excellent report on the natho-genesis of- glomerular disease is a timely fact-laden dissertation with i= ediate valaefor understanding the immunologic events occurring in patients vith glomerulonephritislupus nephritis, and Goodpasture's syndrome. An article on malignant hyperuension pro.vides objective evidence vhich solidifies the need for treatment to normotensive levei4even if glomerulax- filtration rate falls, albeit transiently. The discussion of pyelo. Jnephritis presents new facets of diagnosis which should be beneficial to every cliui- -cian. The last article is a paper on drug abuse and is published as a needed Aid indiagnosis and treatment of this extensive contemporary problem. Immediate applicationis obvious and pitfalls are properly described.
Four full-page, black and white, cartoons appropriate to the subject are include.
D 003&4 ,8 1 JAN 04. MCf 6CIAIFID
4"w 1 7 409 4114 pe A'a 409--1.- UN---M -S-- - -

777'~ -- , 77-- T
-- Security classification'KXV. LINK A LINK I LINK CS* tOLE WT POLE WT ROLE WT
-, NEHROIOGY
NEPHRTIC SMliROLXE
'LECTROLYTES, vater-electrolyte balance
"PARMUERAL mT IAPY
R~IAL FAIUJR acute
BZI)2M,0OGY, glomerulonepbritic
HYPEEIRTESION, m-lwignant phase
."URMZAIY TRACT IN•FEC'1ON ,
M=NFCKiG, urinary tract
DURG ABSE, acute intoxication
r I
I J
- -4
UNClASSIFIESecurity a..usificatOR

PRESENT CONCEPI'S IN ITERNAL MEDICINE
(UEST EDITOR FOR SEFIEMBER 1971S
MAJ Richard E.Chojnacki, MCChicef. Gcn'ral Medicine Service and Nephroloqy Section
f ASSISTANT FDITOR
bLittic Applewhitc. MS.
EDITORIAL BOARD
C('OL John J. l)cllcr, Ir., MIC Chief, Department of Medicinei.TC Neil W. Cuip. MC Assistrnt Chief, Department of
Medicine and Chief,
Hematology(: Go. (;corge B. Hamilton, MC Chief, GastroenterologyCOl. Iugh S. Wi]--V, MC Chief. DermatologyCOL. (;abricl (rcgoratos. MC Chief, CardiologyCOL. Joseph I.. McGerity. MC Chief, AllergyILI(C James L.. Stewart. Jr., MC Chief, PediatricsIT1l: D)arrcll S. Buchanan. MC Chief, NeurologyMAJ Richard 1" Chojnacki, MC Chief, General Medicine"i.TC I-divard E. Ma'.. MC Chief, Pulmonary and Infcctious
Diseases
I.'''ERMAN GENERAL HOSPITALPrcsidio of San Francisco, California 94129
I.iiRMNGNEA OSIA
g a

PRESENT C:ON(:I*PT'S IN INT'IRNAI. MFiI( :INIEV( Ii.t1MtE IV Septcember 1971 Nurnb'r 9
iii
NIPIIROLOGYS YMPOSIUM i
C!
((INTI Ni S
'r'rd ........................... ...
A R 11C]I-"S
IPRIN(IPL I-S 01 PARENTERAL THERAPY .................... 707Milton h'. Rubinm. M.D. and Richard E. Chojnacki. M.D.
ACUTF RINAL FAILURRF ............................. .739.('I)R John D. Conger. MC. USN
RI'(I-N'I AI)VAN(ES IN TIlE IMMUNOLOGY OF GLOMERULONEPHRITIS.. 759MAJ Stepheni R. Steinnin lei. MC
"I1II!" MAI I(;NANT PIIASIF OF i0YI"IRTENSION ...................... 785
AIll:in I. S.hwar,,. MI).
URINARY TRAC T INI-ICTION .......................... SIl('19 Miclla R. R.Cncr. MC
MANA(;I'MhNT 01: AC(LITII INTOXICATION WITHi BARBITURATEIS.III'ROIN AND I.SI) ........ ........................ ,13
LT Jame% HI. Shinaberger. MC USAR
Department of Medicine
-z I.E7TER MA N GENERA L HOSPITAL
' I -• ,• . . '"'''' ti" ; ;'','; • ' • ,,•;"

41,
FOR THCOMING S YMPOISIA. ..
NEUROLOGY
MEDICAL WRITING
GASTROENTEROLOGY
A
Irrersu Coencepts. Vol IV Nip 9. September 1971
o b

I. R FWIt'OR 1)
The sevcral papers found in this issue of Present Qrnepls offer insight intobx)th broad and specialized areas of Nephrology. In several prcscmations,comprehensive reviews, not elsewhere available, are presented. A mixtureof theoretical and practical ideas has been embodied in the majority ofarticles so that understanding would precede future decision in any ofthese areas. It is hoped zhat this volume will make a useful addition to theInternist's bookshelf.
Thc first article, by Rubini and Chojnacki, is yet another approach to theproblem of fluid and electrolyte balance correction of pathologic devia-tions. Cookbook types of therapy are specifically not included since theyhave litt!e value to the individual patient. Sufficient emprasis is made onbasic concepts so as to enable considered, rational decision. Doctor JohnCongcr's presentation of his experience in caring for acute renal failurepatients off the coast of Vietnam is both rewarding and disillusioning sincepost-ir.anmatic renal failure is associated with excessive mortality. As inprevitots reports, patient chcmistrics c.Atcn improved with dialytic treatmentwhile infectious complications precluJcd :,urvival. Doctor Stcinmullcr'soc'c'llcnt report on the pathogcncs.6 of gloiaerular disease is a timely fact-laden dk.w-rtation with immediate value for understanding the immunologic
vcnt.s occurt ing in patients with glomerulonephritis, lupus nephritis, and(;Goodp.'sturc's syndrome. Dcctor Schwartz' article on malignant hypcrten-siot, provides objective evidence which solidifies the need for treatment tonormotcnsive levels even if glomerular filtration rate falls, albeit transiently.Doctor Michael Conger's discussion of pyelonephritis presents new facets ofdiagnosis which should be of benefit to every clinician. Finally, DoctorShiraberger's paper on drug abuse is proudly published as a nc :ded aid indiagnosis and treatment of this extensive contemporary problem. Immediateapplication is obvious and pitfalls are properly described.
MAJ RICHARD E. CHOJNACKI, MC(;ucst Fditor
rPcxc'ni (o'nt vp t. Iit' I I' No '. Septcmbher 19 71
-t3

FORGET THE HISTORY AND PHYSICAL,A
Present Concepts. Vol iv No 9. September 19 7)
706

* ~Pt !NCPI.EY 01- PAREiNTRAI. THERAPY"
Milli)- F R-ub'in. MDAI) and Rlichard E. Chojnacki, M).D
lbe phys~iolosia madhansms of 3ncml 'vater arld electr*-? yte turnover ia-n~v. e intaim., absorption, body distribution..and -'ltimtsly, excretion, With parenteral theuYW, itysio-logic oontrvilsi of intake m3 utboorptlon a" bypessad, andbminostatio regulation In 3Argely 4opullent cc renal excretion.astrogsnico decision umat fall betiman tho lij~ts of renal
capacity of oamvatlon to minimise depiletion, and *nhanedexcretion to dissipate~ sarfolt. With smil renal functions,there is substantial 2sevay in adequate parenterul tberepy,,but it behooves the physician to be ever vary of overdispezilmnoson renal adjustmnts to correct therapeutic: errors. Errorsof omission are onlyr partially compnsable by oonssriatoryus-Niinsa of the kidney, because there is an Inexrabla, lose
of water and solutes that eventually mast lead to depletion;error* of ooasio a %n be rectifid only to a degree byappropriate renal1 ezaretion. TOmoral 1imits to moba ooe-sation are also inherent, and coincident, demans for conser-vation of one substmnos and excretion or another my be cam-petitive, so that oam correctve action is 0only at the expenseof another. Theres aTe ma~y examples of apparently discordantvenal response. Thus, in order t~i conserve potasslA, an-&acidurine my be excreted despite alkslosis. Uner certain air-oim~stances, the body sacrfifoes tonicity to inaintain voluse,e *g. the salt-f ree urine despite hypernatreimia, of dahydrationyor the sodim diuresis despite byponatremis. of chroic waterintoxication. In otherst tonicity is protected at the cqwnseof volme, e.g. salt retaining atates with Impaired waterdiuresis, despite edeme-
This discussion of certain piaotioss of pamute~ral fluidmanagement is mome appropxiate in principle rather than inspecific example. Therapy of a single patien~t requires cog-nitive decision based on a variety of Indidu~alisedI data end
I romI ,1 Ifintuunt (it MedIC11. W ld-ho~trtu Vcemns Admini~tration llo~pitaI and Lrtrivcrity of Cilfuorn,.u.141 n Angcks I I tt (1uhn~ncki ~rpare c'1 ihis irticic w-t~h Dr Rubini durfing thu' ycar 6'-%j awiot~sd
v tilt VA .ttlsnrth liotu t:ou rntt~fifl toi Lttfitn in 'n 1 970( im~il liutitL~vui rf Meic inc. 11nivcr~uty oi iuiforn,. I. o- Angck-%
I'reew~i (Ctimcp~s. 1'(; IF No 9. Y'opienihrr 1971

h .f l d',r .p I A/I, I II,~ ti. ill III, It/j'r 1611.,111 1111d (1 'punz A I
ciraoumtances rather than any prede fined formals, or routine.3uch recipes for parenteral therapy by necessity minimizeinteractions betwueen ooncurrent homeostatie disruptions, andassume that specific indications predicate similar therapeutic4actions consistently. In adlc!tion,, a baseline of "normsl 3 isinferred, as if all acute and chronic physiologic alterationswere a distortion of the steady state of the he<hy person.Howver,, chronic disease may define a nov baseline of homo-stasis, and parenteral treatmnt of the sick patient oftenmust -be directed to re-establish that steady salte. The
impsiionofa preeonosived state ofnormality deduced from
asteacute disordewr prompting active therapy. An attemthas benmade to focus oodeainof this chapter to themore seeeand extreme derangements of water and electrolytemetabolism as well as steady-state requirements because it isin these clinical settings that sound and effective parenteralmanagement is most critical.
GEINE:RAL PRINCIPLES
Parenteral requirements may be arbitrarily divided intotrecomponents: jgtnag therapy, de-lot therapy, and
replacement therapy. Appropriate parenteral therapy requiresconsideration of each of these three aspects ooncurrent,.7 topromote or maintain fluid and electrolyte hoaeostasis.
Maintenance themapy is the provision of basal requirementsof fluid,. electrolytes, anid, eventually, calories, traceminerals and vitamins, et cetera. Hamostasis demands sufficientfluid for the excretion of wastes, the stabilization of bodytemperature by water loss through the skin, and the repletionof respiratory losses. This quantity is often termed theob.Ui~tor water requirement, i.e.* the maintenance requiremntfor fluid in its minimum rather than optima sen"e.
Basal electrolyte requirements are minimal as efficientrenal compensatory mechani sas are evoked with moderate deficits,aid the rate of fa~rther depletion is minimins ed. Losses in thefeces and in sweat are normaflly a minor fracetion of total ox-oration. They also are dir-ini shed with depletion, but withless efficiency than urinary losses. With abstinence of intake,the bowel and skin losses become major detexuinants of deficits.
rr i I (111 1'. 1 11' IV V. .S'pienibcr 197)

Pint, qIh'% , I I r,..i,'ral Iht'rn pl Itv ll Ru in d ho itt, u At "
Basal requirements of water, sodium and potassium may be de-rived from TABLES I and II. The obligatory water loss is thedifference between minimum losses and the water of oxidation.Obligatory electrolyte losses are the miniamm losses in fecesand urine, plus the several alq/day lost from. the skin surfaceas will be subbequent.ly discussed. Such vdnm asm Pe asalte of oontiun depletion and henoe they are theoretic
rather than finite.
Homeostatic requirements for water and electrolytescannot be inferred fro wmaxia oonoentration of these sub-stanoss in urine. Thus, the familiar concentration testperformed under paraphysiologioal stress such as water dep-rivation cLnnot be oontinued indefinitely. While man canconcentrate his urine to approximately 1400 mOs/L, the maximumintake concentration of total solute is approximately 600 mOs/L.)%zimum intake is compared to rximu excretory capacityexpressing both values as concentrations. Figure 1. Intakeconcentration is based on mxium infusion concentration thatpermits a steady state; output concentration is the approx-imate ceiling concentration of these solutes in urine obtainedunder a variety of circumstanoes.
MAXIMUM INTAKE CONCENTRATION Dl VS
800 , MAXIMUM URINE CAPACITY 1F
800-
mM/L400-i
Na CI K UreaFigure 1.
i'r,•in (,Cm cp•. I I"V No Y. Srpr.rn•ehr 19 71

710j
IAIILII
DITERMINANTS OF WATER BALANCE
USUAL RANGE. FXTRIrMI-millli~ters
IntakeFoods. liquids* 1000-1500 20.00atOxidation of tood or tissue 500>- 800 2.000
OutputUrine 400-1200 10.000*
1 5.000§Lunre% 500. coo 2.000Skin i'ueatl 300- 500 15.000 III ecsc. SG- 100 1 0.0001Stomach AXspirate 6.000Iligh bowe-l Or 8.000I ass bowel I i~tuba 5.000
Waiicr turnoer .i. pc~tcnt body water 1'24 hours
Infant 15-35%
including pre-forrned 11,0Sa-, water diizrcsis - diabetes insipidusa- osmtotic diuresis - inassis glycosuria or sustained mannitol diuresisJ4,11i1i3tircJ min performing heavy physical effort in dry Iropical environmlentScholera
IlABLE 11CONSERVATION OF SODIUM AND POTASSIUM
MINMUM TIMI RE',)UIRE-D0(ONCI NTRATION TO ACHIEVE
OR WMOU'NTMAY %IIN I N1UM LOSSEIS CIRCUMISTANCE.S
11i ro (I nill (it 1-2 d.i'. atntainance + iniinralocorticoidsI Cie, 4 , nil qWdav )l %%eek abistaminanc + mniaralocorticoid,VtIiim1.'1 1 60111l q/l Immediate concentration increases with pro-
longed aspirationllowcl! 120 1-11 l/I immediate conccntration increases% with pro-
longed aspirationý, l I fiill fill scverail week- acclimatization and profuse scating
l'oia'.slumlUrine 34 nil (/32-4 weecks- K deficiencyI ezve 2-4 rnl-q/da) 2.4 weeks. K deficiencyStomat~ih 2-4 mlq/L day% :oncentration falls ,.ith protracted
lossesBowel 2-4 mi-qIL davs severe potassium deficiency or pro-
longed asp!rationS wc.it 2-3 ml q: L seve-ral sve-ks K deficiency
assuming.wa~mmal act.d secretiontall bowel a~iae r entiall) isoitonic hci with progressive los~ses thLrc is inceasing exchange of
Na for k. arid Na."or,"ostion aspirate apocethtfpls'a. Lower valuc,, may be obtainedif water is ussd for flus'ung or if ingested watetus losit t.ore itis absorbed
V alue- below plasma1 conventration may occur with maxiumal water diumies i-ut net loi,% ,s g; -atcr.
P'resen-t C'.nccpts. I ol IV N,) 9. September 19 71

Rgficit tberapy is replaoeast of losses that haveoamu-nd beforle the Ofl~et of therapy; these are finite losses,I , aM can be estimated from direct a~ssays, laboratory findings,history and physical examination. Deficit requirements in-volve both quantitative and qualitative considerations. Thus,the sawe quantity of sodium my be a~inistered to correctadeficit of body sodium content in a patient with Izypovoleialand a normal or high plasms sodium ooncentration as is requiredto replaois a deficit in body sodium in a patient with bypo-natremia, ard edema. In the former instanoe, sodium should begiven in sufficient water to expaad the extraciellular fluid.,and benoe normal salIn might be a logical prescrirtion. Inthe latter, relative or absolute waater excess is *%.dent, sothat if salt in deemed neoeseary, hypertonic salins should beidminist~rsd an a 3 or 5 percent sodium chloride (Y&al) solution.
Since gastrointestinal losses are most ocmonly the causeof deficit, knWledgs of the volume lost wAn its probableoomposition is critical to estivate repletion requirements.Typical losses are depicted in ?&BIA in, more extensive.3.pletions can be estimted from the maxims 'volumes in TABLZI as electrolyte losses are generally proportionate. As notedin TABIZ III, oompeaxtive indices provide a simple estimate ofthe percent of sodium replacement which should be given assodixm bicarbonate or its equivalent by subtracting 100.
AC'ID BASE INDEX OF GASTROINTE-STINAL FLUID DEFICITS
Aspia~e(Na) 100Derivation Index: (CI) x -F -x 100
Stomach 50-90*
Saline 80
Plasma 100 Arbitrary
Iligh intcstmet 120-140
Low inlesline 150-200
Value,~ frontl 50-120 ca u-tiaIk he Lon'~idctcd wuited for repletion with normail %3linc (Indc\ 80)PaI.ntwatiw -wr('::n i% highly aIklirnc except ini the czc -3f fi;tiilae when it i% gzcnflt) admin ked
Preven I (omccr is. VnidI V No 9. Sep 1cm her 1 971

-If.' : -
Pi'rim, Itpe ,. Iezrcnzacral JIhrvaj Rulni and (ChmnactA
Replacemsnt therapy is the repletion of continuing ab-normal losses. These may involve losses through the kidney,gastrointestinal tract, skin or lungs. Again, not only mustthe voluse of fluid lost be replaced, but the composition ofthe replacement solution should be "tailored' insofar asPossible to the composition of the fluid lost. Replacementtherapy is always a supplement to maintenance therapy, andmay be a ccmplement to deficit therapy. As a generality,tosses of fluid derived proxinal to the duodemm are acid andtend to •emk the extracellular fluid alkaline (alkalosis);losses from progressively more distal sites are alkaline tend-ing to leave the extracellular fluid more acid (acidosis).The site of derivation rather than the site of renoval char-acterize the pH and bicarbonate content of gastrointestinalaspirates.
7lle ('nc•pt •, /er," !da/an c
The steady state of homeostasis is often referred to as"Ozero external balance" whereby intake and output of a sub-stance are equal. Zero balance also implies normal bodycontent as it is assumed that if an excess or deficit werepresent, and intake continued, output would adjust to om-pensate. It is obvious that this concept is an oversiup-lification, but it is clinically useful and convenient todescribe body homostatic mechanias and derangements in termsof positive, negative, or zero balances.
Physiologic balanoe must be defined not only in terms ofexternal balance or whole body content of fluid and variouselectrolytes, but the internal compartnentalization of thesecontents, i.e. cellular and extracellular distribution. Wheneither the external or the internal balances are deranged,there is a tendency to return both balances to zero coinci-dently, as the content of cells are in equilibrium with thecontent of extracellular fluids. The fact that a load ofisotonic saline is excreted, despite unchanged extracellularconcentration, unequivocally points to a volume stimulatedregulation of balance.
Diverse contemporary homeostatic mechanisms are alwaysintegrated. Distortions of both external and internal zerobalance are not only quantitative but also involve the contentof one substance relative to another, i.e. concentration of a
-' rc'scn i (',,n, ,'l' I,,4I II \., Q •,.~'rcm b r I 0)-

I'm, til;/(- ,,/ Iarciti,'ra; I.-crap; Hu'thlim av:d C'h.,!tclu'l
solute in extracellular water or the relationship of intra-cellular potassium to sodium. Appropriate renal ccopensationto achieve sero balance is often a complex process. Considerthe renal adjustment to the prosaic act of infusion of a literof isotonic salt solution, i.e. 1000 al of water, 150 uEq ofNa+, and 150 mEq of Cl. The kidney mnut not only excrete theload of water and solute in toto,, but wast be concerned withthe temporal relationship of the exmrtlon of one solute asrelated to another, as well as their ft. •ntration in theloading fluid. In the case of isotonie sodium chloride in
which the chlorede is in substantial excess of its concen-tration in the extraoellular volume, urinary chloride outputincreases prior to the increase in urin flow; water is thenexcreted in excess of the extra solute and finally sodium andto a lesser degree, chloride is excreted in excess of extrawater.
Despite the wide range of qualitative and quantitativerenal adaptation it is easily possible to exceed renal com-pensation and a chronic overload may develop. Excretoryadjustments are often interrelated, the most obvious exmuplebeing the accumulation of water when the amount of salt givenconcomitantly exceeds renal excretory capacity.
WArf R
The first order of concern in parenteral requirementsand therapy is water. Normal water balance may be defined asthe physiologic state wherein intake is approximately equalto output when neither intake nor output is manipulated.Because intake is usually intermittent and output continuous,an arbitrary period of reference of 24 hours is usually assumed,Water balance is never static, and continuously fluctuates inreflection of activity and metabolic stato. Thus, if oneassums that 3ero balance is reached at a specific time, i.e.at meal timi-s, a normal man subsequently either ingests awater excess stimulating regulatory mechanims to reducepositive water balance or undergoes water privation stimulatingthirst and renal conservation of water.
As a dynamic Loncept, water balance cannot be arbitrarilydefined relative to body weight, intake or excretion withoutreference to the coincident balance of sodium and chloride.
A ', 1(,,' ',:, r:." I,,'11 \,, o..n Scpiem hbcr 1971

"/I4
I',mu ip, P , 'art nit ral N:-rajui ui," ,.. ( 7Vpna, Iz
The temporal as well as quantitative aspects of derangementsof water balanoe are critical to the physiologic and pathologicresponses so induced. khile the main regulatory mecharnis ofwater balance is renal, overwhelming excess or deficits ofwater my ultimately cause a renal response which is inappro-priate or converse, e.g. antidiuresis of cevere water intox-ication or the reduced solute output (and isotonic oliguria)that occurs with massive salt excess. Thirst also regulateswater balance, albeit at a primeval level. In the activitypattern and conscious behavior of moderm rnn, imbibition ischiefly by habit or custom rather than from thirst.
Water balance is intimately related to thermal balance.In order to maintain thermoneutrality, heat loss over anyperiod must equal the total heat produced. A healthy, activemale in a comfortable environmental temperature will loseapproximately 1000 calories per di'y by evaporation of waterfrca the skin and lungs. Additional losses include 2000calories by radiation and conduction from the skin and 100calories by increase in temperature of inspired air andexcretion. Hear dissipation favors convection and radiationroutes in the nresence of lov ambient temperatures, whileevaporation is of prime importanca when ambient temperaturesare equal to or greater than body temperature. In thissituation heat cannot be radiated and heat loss is primarilyby evaporation of water from lungs and skin. Each milliliterof 6tter vaporized requires a dissipation of 0.58 calories.Loss of heat from the body is dependent on the amount of waterevaporated, not on the amount of sweat produced.
Even in the absence of sensible sweating, water require-zents are directly proportionate to the caloric expenditure.An adult metabolizing 30 calg/24 hr utilizes approximately100 ml H20/100 cal or 2.0 liters. This ration of fluidrequired per calories expended is relatively constant in mostmaimalian species, while caloric requirements per kilogramof body weight evolves progressively through infancy and child-hood and varies substantially among different species. Asmetabolic rate is proportionate to surface area, rather thanbody weight, water turnover can be similarly expressed in allspecies at about 1100 cc/i 2 of body surface/24 hr. Increasedcaloric requirements, as in protracted fever or thyrotcxioosis,impose an additional but proportionate water requirement sincebasal metabolic rate increases 13 percent for each degree ise
in body temperature.
.. T, <'- - -A ; -

• - m m m I I ! ,
/7t•,,Iru q', I I' r '!/,nIf r,.i /h r.q',i /•l'll anSI ( hun'l,'a&,
The obligatory volume of urine is determined by theamount of solutes that must be excreted and is relativelyindependent or water ingestion or abstinence, e.g. if dailysolute load is 300 mO0m, and maximum urinary osmolality ia1200 zO=/kg, 400 ml urinary water is required to excretethis load. With greater solute loads, maximum urine osmolalconcentration falls, and the obligatory volume of urineincreases more nearly geometrically than linearly. Massiveglycosuria may impose a solute load of several o soles perday. Skin losses of water may increase 10-20 fold withphynical exertion in a hot dry enviroment; fecal losses mayincrease 3-4 fold with diarrbea., and much more with choleraicstates. In such abnormal cir•matances, water balance tendsto lag negatively, and zero balance is approached, but seldomreached by greatly augmnted intake under the provocation ofthirst alone.
Generally, the urine is more concentrated than plasma,indicating that a mild degree of dehydration is the normalsteady state. Even under ordinary zircumstances, man drinksepisodically in excess, and swings internittently into posi-tive balance. He then excretes free water to correct anexcessive water load. It is the aim of parenteral therapyto maintain a slight positive balance of water so as to allowa modest facultative urinary excretion, i.e. that volume ofurine in excess of obligatory excretion. Facultative wateris not identical to free water excreted, although free wateris always facultative. Urine is therefore generally lessconcentrated than it could be and still maintain soluteexcretion. This is probably normal in a physiologic senseas a number of movilian species from rats to man maintainan intake of water in modest excess of obligatory losses.
The intake of water is in four forms: (1) that waterdrunk in response to thirst stimuli or habit to meet thecultural patterns, (2) that water which is pre-formed infoods and taken primarily in satiation of hunger, (3) thatwater which is derived from the oxidation of tissue constit-ueuts, and (4) that water which is infuased or otherwiseintroduced into the body by prescription. The character ofthe diet relates to water available for excretion by the typeof food eaten (pre-formed water) dnd the nutrient compositionthereof (water of oxidation). Bread contains 20 percentpre-formed water, meats scme 75 percent, and vegetables andfruit from 70-95 percent. The water obtained from oxidation
v' , ,. ., -I

fi "1 a i vlAca uhn1,Own,1.-- ,
depends predominantly on the amount of hydrogen of the moleculeconcerned (protein 0.41 cc/gm, carbohydrate 0.55 cc/gm, fat1.07 cc/gm). Approximately 12 ml of water are derived fromeach 100 calories metabolized (protein 10.5, carbohydrate 13.8,fat 11.5 ml/l00 cal).
In addition to the quantitative aspects of water balance,there is also a temporal aspect. An increasingly negativebalance of water, produced at a modest rate, may lead to welltolerated contraction of body water although a rapid loss ofsimilar magnitude caused by sweating may cause collapse.Chronic water excess may be totally asynptomtic and manifestedonly by reduction in serum osolal conc'ntration or it may pro-duce a crescendo of symptoms from mental confusion to eventualcoma. A load of water may induce water intoxication if givenso rapidly that renal compensatory mechani-us lag substantiallyin excretion. Acute water intoxication evokes a strikingsyndrome complex marked by restlessness, acute weakness,diarrrhea, salivation, itcbing and vomiting, tremor, musclewitches, and convulsions. Forced acute water poisoning hasbeen awarded a reputation as a medieval or oriental torturealthough it is potentially lethal, the discomfort is shortlived and coma rapidly supervenes. The acute syndrome isprimarily seen when large water loads are introduced intothe gastrointestinal tract and probably reflects rapid lossof sodium and chloride into the intestinal tract, as well asthe hemodilution and hypo-osmlality caused by water absorption.Positive water balances produced more slowly by ingestion ofsimilar volumes are seen in psychiatric illness with ocmpulsivewater drinking and yet with much less adverse symptoms eventhough a positive balance of 20 percent of body water may benoted. The centrml nervous symptomology of water excess isin many ways similar to that of water deprivation, and aterTrems, both may be associated with oliguria. Epilepticsubjects are particularly prone to seizures with overhydration,and it is reputed that Napoleon "encouraged" ingestion of weteras a means of separa+ting potential epileptics from his draftedrecruits.
There i3 also a poorly understood phenomenon of resistanceto water intoxication that cannot be completely related toaugmented renal excretion. It is demonstrable by giving ratsprogressive increuents of water on successive days and findingan increased tolerance to acute water intoxication that ismanifested before diu.-esis and even after nephrectomy. Gluco-corticoids have similar effects, at least in the rat, of
*'i . 1 , i ,iI \ "•:, • .. .. r '

P'inclni ,I Parenlerl 7J7wran v- Ruhin! and (Tajunacki
inducing resistanoe to oa produced by massive wter loading.In this species, and possibly in man, adrenalectomy increasessusoeptibility to acute water intoxication. The situation
ae s akin in man to the clinical tolerance to hyponatreaiawhich clearly depends on the rate of development as well asthe degree.
ISOTONICITY AND OSMOLALITY
Sucoessful parenteral therapy requires not on4 restorationand waintenance of vo?.une but alo a noral solute oonosntrationin that volume. Solutions which are at the cono2entration ofplasma and extrecellular fluids are 3iso-omolal" or "isotonic"although the latter toma is oftan used inoorrectly.
Isotonicity of a solutiou is defined as that concentrationat whiah suspended red cells are unchanged in volum Tonicityis independent of omolality, e.g. the addition of urea oralcohol to an infusion does not alter tonicity becaume thesesubstanoes freely per mate red cells and yet such additionobviously altere omolality. Tonicity is defined relative toa mabrane of reference, while omolality is a colligativeproperty of a solution whether or not a mmbrane is present.Isotonic solutions are not necessarily of the sm oolalconcentration as the fluid within tbe cell and oategorixationof isotonicity depends to a degree ow the species of Lan tcells utilised. Thus, rabbit erytt±cyten define isotonicityat 1.1 percent sodium chloride, vhile 0.9 percent sodi~mchloride is isotonic for htan red cells. The clinical useof isotonic saline ixplins a w•tchbug with the omolal oon-centration of the extraeollular fluid. This is only partiallytrue, however, as the effective omolal onucentration of thefluid bathing cells is soae 5-10 percent lower than that ofisotonic saline, and my vary ± 5 percent froa patient topatient.
Plama is the conduit between the protoplasm and fluidleaving or entering the body. As plama is isotonic bydefinition, only fluid containing a suitable concentrationof solute can traverse the plain. It is this coincidentsolute m-oement that controls the flow of water across bio-logic membranes and is inflrenood by simple diffusion,hydrostatic pressure, cellular metabolic activity and trans-membrane ionic fluxes.
Prrsern I (',u cps. I',,l I V .\ o 9. Scplember 19 71

718
hrimu iphls qj Parentcral lhcrapr - Rubim and (holnat cA
The complexity of (tranmembrame) wter and salt movementsis exemplified by the changes which occur in the volume andcomposition of fluids introduced in the peritoneal cavity.Isotonic glucose solution increases in volume prior to absorp-tion because of the transperitoneal movement of sodium andchloride which temporarily raise omolality above that ofplama. Isotonic saline by contrast is readily absorbed, andonly by the addition of 3.5 to 4 percent gluoose say the ab-sorptive forces be balanced. The dependence of water movementon the character of solute dissolved may be further illustratedin several simple physical-chemical experiments: (1) isotonicsaline will lose fluid across a oellop-ane membrane to isotonicglucose because oellophane as compared to the red cell membraneis more permeable to salt than glucose, and (2) when isotonicsolutions of mgnesium sulfate and sodium chloride are similarlyseparated, the sulfate side expands at the expense of the chlo-ride side, reflecting the different rates of solute diffusion,i.e. chloride diffuses faster than sulfate.
I'ROCIANIRi. OF PARENTERAL THERAPY
The first requirent for parenteral management is asafe and ready access to the circulation. IndWelling venouscatheter techniques have greatly simplified procedure, butcare must be constantly applied to avoid introduction of in-fection by use of bactericidal ointmnt at the site of skinpuncture. Cortinuous infusion ninluises the risk of clottingwhile peripheral venous catheters sLould not be used for morethan a week (preferably 3-4 days) without chanrin the siteof infusion. Solutions of glucose above 14 perosnt are poorlytolerated in peripheral veins, but introduction of a catheterinto large deep veins such as the Jugular, the iliac, or eventhe vona cava, permits the rapid dilution of more hypertonicsolutions which otherwise tend to injure the venous Intm..The addition of glucooorticoids to oore_•ial hypertonicinfusion solutions, presirbly to mininmie infl•amtory reac-tion, is probably unnoessary but sems harmless. Beparin in=all amounts also may be added to hypertonic infusions.
Is a genaral principle, single component solutions arepreferable to polyionic solutions if several solutes must begiven simultaneoualy. The addition of potassium chloride orsodium bicarbonate in specific and carefully considered
t rescit Concpt•. V'ol I * \ o 9. September 19 71

7/v
I'rinciph"v uifl'arc,:wrul 77ifcnzpt' - Rubmin and (hwjnarki
mounts to isotonic @0li1 is proframble to IstauWAI'd mixturesprepackaged for marketing convenience rather the physiologicwrit. All additives should be labeled on the infusi 5a bottle
-- orders should define rate of adanie'.-rtion, thie cbaracterof pazenteal, fbzids, and volme pi'escr'kbed. Bottles shtouldbip comaeoutively zoabsi'ed to slydaiu. jonfusion aid to readilypendt bedside recognition of the speed of aduinistretieL.noe maring staff should be alerted to ir~ooopired changes inor= -now, thirst,, a=1ety,. headacbs, and others, as probableIM~waftiom to slow but not opltoly stop the bifusion andto uoti4y Ye zes onsdbl pbysician. h use of indvllingmitial winous aelbaters to determine pressure at frequentIntervals is hS~pfu1 wbon the volvin required is =~certainor smal oýesaio is liuited,, especially in elderly ordabalitated aibjects. Fortuntely there in a vide flexibilityof physiologic adaptation to oversolow2 application of perenk-level thasamW so tkat a trial and obeervation routira Is
laboratory stuies needed for ratioel, psazentezal maw&mat InaolW. the buistocrit, and the sodium, pot&asim andWdoaibeste content of plans. Plams, or blood pH determinedaeither slactraitrically or indirectly fran pCO2 and bicar-bautt. in especially helpful. Omolait~y of plases my be
Inaluanble,, eseclally for reoco~itiorn of odza1ating oswtiematerial other then sodius, suzch " as itol or uree. Thewelatiemabip to sodim concentration, and serves to delineat.states of amion excesses occurring in urewia or lactic acidouis.UUrim stodes of primn utility include a avasure of concentra-ties (omolaI&ty is preferred to specific gravity) and pg.Unless there is obvious excessive loss of body fluid, plasmdetentizitiorns ane zoT essential then zund= detoronationsof urnLmzy electrolytes.
In chronic disorders of body fluid and electrolyte balance,.came intAlis is kmown., the detenzuirtion of sodium, potassium&an chloride content of spot smaples of urine is increasinglyvalble, but 24, hour collections Qrs m~perior. The cognizanceof .ttemvl, electrolyte losses froms all liquid excretions and
as~d~m from ti. ki body is essential, and continuous ooq~letedaily collections should be obtaintud. The pbysician mist corn-.eider the delay in obtaining the collection and the ti re-4quired flor laboratory stadiies in the interpretation. of thePatimit' s status of the Amomet 4
Present, Concepts. Vol IV No 9. September 1971

721)
Prinu :ph' tf Parenteral Therapy Rubut and Chojnacki
Parenteral therapy should be carefully re-evaluated atleast daily, an approach facilitated by P .ccurate tabulationand charting of pertinent data. Too often, decision is madepredominantly from laboratory data. The wary clinician,however, should never regard the laborattory as more than anadjunct to informtion gained directly by clinical observationof the patient becaube even with reliable data and reasonablededuction, the patient will sometines show clinical deterio-ration before or despite biochemical inprovement.
Parenteral Therapy of :ypo-Osmolal States
The symptcas of hypo-osmolality are non-specific andinclude weakness, lethargy and coma. Intraoellular hydrationis increased except possibly in certain chronic disease statesassociated with proportionate intraoellular potassium losses"~the sick cýell syndrome. Clinical dependence on such signsas skin turgor or fingerprint clarity may be inadequate,especially in the elderly. As red blood cells w•ell, heuato-crit may be elevated. Cerebral spinal pressure may be mcd-erately Increased but papilledem is unusual. The electro-encephalogram may show non specific slowing. Thirst occursdespite h-po-omolality in response to acute changes in volume,toxicity, or possibly potassium deficiency. Urinary sodiumis usually not helpful diagnostically as it may be reduced(seconiary to reduction of filtered load?) or increased,
In most instances, mater deprivation alone Ls optimumtherapy. This is zors easily prescribed than expedited asthe hospital environmnt i permeated with the idea thatforcing fluids is an attribute next to cleanliness. Crackedice and liquid nutrients are proferred indiscriminatly bywell meaning aides., visitors, and other patients who seem toequate thirst with neglect. More rapid correction of planaoiolality requires the administration of hypertonic saltsolutions. This option depends on definite acute clinicalindications because pulmonary edema, oongestive heart failureand hypertension may ensue, especially if whole body sodiumis already increas4d. With treatnt, the rise in sermusodium will be predicated on the redistribution of water,and not simply the dilution of sodim in a static extracellularfluid volum. Therefore, whcle body water must be used tocalculate the amount required to achieve the desired changein concentration. In most instances, such calculation in-dicates a need for very large quantities of hypertonic saline
i'r, wi • ( 'n p)i I , I I , S,. ptcbnhcr 19-1
3

S~~ri ~Ic>. u q h'\c,1 i l(trtraJ Ilftrru/r R,,htu an.d ( 7tt'ptw Am
to rais conoentration to norwal, much to the consternation ofthe physician. A trial of 25-50 peroent corrmection is usuallysufficient to demonstrate whether clinical improvemnt willoccur. Administration 3hould be slow, preferably over a 12hour period followed by a 12 hour period of observation. Asa rough guide, 6 ma of water becomes isotonic for every mill-mole of sodium chloride given in excess of noriml saline.Sodium excretion in the urine may remain unr-hanged until thebody des.lcit is reploed or may increase under the stizilusof expanded volume or the persistence o. an altered "osostat".
The removal of water in exoess of malt may 'e accomplibedby inducing an osmotic diuresis, usually with mnuitol. Theconcentration of urinary sodium during vigorous diuresis withthis agent is approximately 30-40 mZq/L, mo that three-fourthsof urine volume is in excess of the oamolar ratio of plan&.Urine flow, however, is proportionate to the filtered load ofmannitol so that a substantial plaama mannitol concentrationis necessary. Increasing plasma omo.ality in this mannermay reduce cerebral edema by establishing an omotic gradient.Rebound phenomena are mininized as the excess vater drawn fromc3lls is carried into the urine. Because plams, volume expandsinitially with large mannitol loads, the procedure ie notentirely without rAsk of pulmonary edea. Barry, however,reccueuls the use of mnnitol, it least in a trial dose of20 grams, in most patients even in the presence of mild tomoderate heart failure, /1/ Urea may be similarly employedbut rapid infusion of concentrated solutions of urea may pro-voke nausea, vomiting and somnolence. Urea slowly enterscells and, as urea is excreted into the urine and extraoell-ular fluid concentration falls its subsequent diffusion backinto the plasma may lag behind that of water and central ner-vous system syMptoms may be aggravated.
Concentrated glucose infusior, my also be effective, butthe high blood sugar levels needed to induce a brisk osmoticdiuresis are not well tolerated and require massive loads.Finally, the induction of maweting is more of a theoreticpossibility than a practical measure for application in sickpatients.
Pri-sr ,i't (',onceptisf l*,1 I I % . .S(ptcnzb.-- /971
- - ~ - ,~.~-t,--,xr --

P:incipk'm q] Parent'ral A7urapv -kubtin and CholizacA':
I'mrcntiew ThicralpN' o ilypero-inolal StajtnŽ
Clinicadl recognition of hypero~aolal states Is based onintuition aid knowledge of precipita'.ing factors. Symptomsthat are suspect include somnolence,. lethargy,, or coma (arather similii' picture to the symptoms of hyponatremic statesa).Restlessness, anxiety and even manic activity any be premonitorymanifestations, headache or visual difficulties may be prominent.Precipitating factors include diabetes and water deprivation.
The skinfolds are lax and norm%! skin elasticity is lost,sweating stops. Subeutaneous tissue is plastic and thin., themucous membranes are dry and sali-sa is scanty. Vaginal mucosais also dry,. a finding that may be useful diagnostically infemale patient.,s breathing through their mouths. The patientmy have a staring appearance and the voice may be hoarse.There is a general apathy and delayed response to interrogation.Thirst my be a complaint upon direct questioning,, but becausethe patient is often severely ill and stuporous, its presenceis often not spontaneously ascertained. Recuabent hypotenuionmay be prominent, or postural hypotenulton and faintness my bethe chief reflection of hypovolemia. Cold extremities., threadypulse, collapsed veins may also be present, ocular tension maybe dimainished on palpation.
Confirmation is obtained by the demonstration of elevatedplaina sodium or osslality. Asotesia raises plasma oamolal~itybut effective oinolal concentration is normal. Increased cir-culating lipid or protein any artefactually raise serum sodiuemdue to displacement of plasma water. A. true byperoinolal stateWa be due to substantial hyperglycemia, e g. greater than
500 mg/).00 cc (18D mg/l00 cc = 10 z~as/L), w~hile lower bloodlevels have less importance except for the aggravation ofwater and salt by lossess by osmotic diuresis. With hypergly-cemia, plasm sodium is not a reliable indicator of hyperos-molality since it accounts for loes than its usual. half oftotal plama solute. Excessive sweating, hypertonic or dryaalt a&Rinis3ration are occasional causes of hyperoinolality,but most cases are due to water deprivation or to an excessiveobligatory loss of watar secondary to solute overload.
1'rc~t ni: (i' rpI%. I ofI iV A o9. Sep fern bcr 19 71
- - -- 2A
Principlev of Parenteral Therapy -Rubin and OCwjnacki
The classic example of hyperomolal hypovoleidL is an olderpatient with nephroseler-osis who is unable to cono ntrate hisurine normally. Admitted to the hospital and unable to eat byhimself, he is started on a tube feeding mixture. Too often, Ithe emphasis is on total calories, protein, vitamins and elec-trolytes so that wter needs are neglected. The inability tooonserve wter is further compounded by thI fixed loss of water
acocapa:Ving inoreabed urea nitrogen excretion. With hypovo-leaia, salt retaining stimuli are added. On the fourth orfifth hospital day, the patient has lapsed into coi and asrmsodium is found to be 165 uW/L. A myocardial infarct orcerebral vascular aecident that was suspected as the oause ofdeterioration my hab actmLlly been induced by dehydration,thus fbu-her ocplicating recognition of the original oause Iof difficulty.
yperommolality is often (buit not neoesarily) coincident iwith hypovolemia and the sympt~atology of increased ccnoen-tration merge with that of decreased volu. Hypovoleia, dueto loss of whole blood volume is disoussd subsequently in thesubection on acute volue deficits. The comonest clinicaloause of bypovolemia and ultimately hyperomolality is dehy-dration, a clinical term applied in a broader snse than simple
desiccation.
The recognition of dehydration is facilitated by charac-terisation of urinary output. With dehydration, urine ischaracteristically reduced in volume; it is highly concentratedbut low in sodium content as the body attempts to conservevolums at the expense of tonicity. The•e findings do notneoesmarily prove dehydration, as patients with acute glamr-ulonsphritis may produce a mall volum of highly ooncentratedurine with little sodius. Similarly, acute reduction in renalbloodflow my serve to pr-luoe oliguria with sodium retentionand increased osmolar concentration. Conversely,, the findingof a copious urine volu with increased sodium concentrationdoes not rule out dehydration as renal functiou my be inad-equate or an omotic diuresis my be present.
The relationship of solute load to water requirementdepends on conuentrating ability, the rate of solute excretion(that is, the degree of omotic diuresis) and to a lesser degree,the predominant solute excreted. Prefeeding protein increasesconcentrating ability, protracted overb•dration diAminisbes it.With reasonably normal filtration rates and usual solute intake,the specific gravity at. urine flow greater than 1.5 co/min
Prescnt Con, epts. Vol IV No 9. September 19 71
NI

724
Prtnciplek of Parenteral Therapy - Rubini and Cho;nacki
should be less than 1.010. The finding of consistently ioo-tonic or slightly hyperto=ic urine with outputs of over2000 oc/24 hr should suggest that an ossotic diuresis ispre sent.
In general, the mainstay of parenteral treatmnt of hyper-osmolar states with hypovolemia is 5 peroent glucose in w.ter,although 0.45 percent saline my be used to replete volumawhen water is needed in excess of salt. Isotonic intravenousglucose solutions may be infused at a rate of 1-2 cc/min with-out producing glycosuria (0.5 g glucose/kg/In). This isapproximately one-half the equivalent rate tolerated by dogs.The limiting restriction to the rate of infusion of 5 percentglucose is the blood glucose concentration and thus dependson antecedent diet and nutritional status as well as the factorswhich influence the action of insulin.
For practical purposes, infusions of 5 percent glucosebehave as if only water were infused. There is an appreciablelag to diuresis following glucose infusion that is not pro-portional to the rate of infusion, and hence is not explicableby rate of fall of plaia oinolality or the rate of expansionof body water. This phenomenon most probably represents thelag time for the disappearance of all circulating antidiuretichormone. Peak diuresis, on the other hand, is directly relatedto load and loading rate. Diuresis persists after cessationof infusion for a one to two-hour period, independent of theamount of positive water balance accried at the end of infusion,although the amount of urine produced over this period isclearly load-related.
In normal individuals, a diuresis of over 35 cc/min maybe achieved for brief periods, but it is difficult to sustainwater diuresis above 20 cc/min for protracte4 periods even withconstant water intake. If continuous dater intake substantiallyexceeds the rate of output, urine flow my abruptly fall assymptoms of water toxicity appear. Because there is an apparentfloor to solute concentration in urino of about 80 zOs/L,continuously high urine flows are necessarily solute depleting(especially of sodium and chloride). Hyponatremic and hypo-chloremic states as well as most chronic debilitating diseasesimpair the ability to excrete a water load and diuresis may beabsent, reduced in quantity, or delayed. Pain, fear and manydrun atimulate antidiuretic hormone (ADH) release and my in-hibit the production of free water and excretion of a positive
P'rcesent C',ncpts. Vol / V. S.p tcmber 19 71

725
Irintc'phl' "J I'zarentcrul 1herapv - RithiI anild (7ojnacki
water load. Thus. gluoose infusions are an unreliable thera-peutio mans of inducing a sustained diurests, e.g. after drugingestion, when a high rato of urine flow is desired; an omoticdiuresis with as non-absorbable solute such as mamnitol ispreferable.
Parenteral T-herapy of Acidotic States and the Therapeutic Induction of Alkalosis
Severely acidotic clin:.cal states are frequently comli-oated by coincident azotemla, hypercapnia and hypoxia so thatthe etiology of specific syqpto is difficult to deteruirewith certainty. The most coemon cause of severe acute acidosisis the retentive ecccwmlation of organic acids, especiallylactic acid or keto-acids duo to overproduction or ancxia.loss chronic and usually less sevwre satabolic acidosis ismost oomsonly caused by protracted loss of alkaline intestinalsecretions. Arter:i-tl blood pH values below 7.25 are associatedwith mental disturb3icas and possibly oam; jactitatione,papilledem and arrytbaias may occur. Cardiac output isincreased and peripheral blood flow and beat loss is accentu-ated. Severe acidosis is paieticularly deleterious in thepresence of a borderline cardiac ocpensation as the greatlyincasaed cardiac deAand and the diversion of blood frce vitalorgans may initiate a vicious cycle of acidosis failureanoxia more acidosis, and so on. Death is inLient with ablood pH that is slightly below 7.00.
The aia of therapy is to decrease the causative factorsof acidosis, e.g. anoxia, carbon dioxide retention or insulinlack. In addition, sodin bicarbonate or lactate solutionsare generally uusd. Rapid 3hifts from n wre acidouic toovert alkalouis should be avoided because of the risk of in-ducing arrbytbadis. Hypoolowia with oovulsions may alsooccur wvth o rc.-rettioa tr r~i &o.i of +tabo'alkalonis5 eopecially in children.
The "bicarbonate deficit' is unrliable in assesaing thedegree of acidosis since other buffers, notably hemoglobin,tissue proteins and possibly the skeleton are involved incispenamtion of what can be considered a proton load. To
estiwmte the bicarbonate needed, a general rule of thumb isto subtract the observ•d bicarbonste from an ideal normal of
Presentt Conc,'pis. V1alI V No 9. September 1971

726
7 Prun ihje ,,. Iti'of ,:ci ral 77iraptv Ruhji and (o7iujaki
approximately 27 .)VL and to multiply this differency by 14percent of body weight, i.e. a value suamwhere between extra-cellular volume and whole body water. Usually, only half ofthe deficit is given in the first 24 hours. In situations ofextreme acidosis, e.g. methyl alcohol poisoning, it may bedesirable to give extremely large amounts of bicarbonate rapidlyuntil urine pH becomes alkaline. Calculation of bicarbonatedistribution under these circmstances my reveal a substantialdiscrepancy between the amount administered and that amountretained in the chloride space or excreted in the urine whichconfirms the existence of umeasured cellular buffers.
Intravenous solutions employed to increase plasma pHcontain bicarbonate, lactate or acetate. In theory, all aresimilar because acetate and lactate are rapidly metabolizedto bicarbonate. Bicarbonate, or its equivalent, may be givenas ooiercially prepared balanced isotonic solutions, usuallycontaining about 30-45 n)s/L of base excess as one-sixth molaror one molar lactate, or the desired amount of bicarbonatemy be added to other.fluid requirements. More concentratedsolutions of bicarbonate, e.g. five percent, are occasionallyemployed but lactate containing solutions have generally beenaccorded the greatest popularity, perhaps due more to famil-iarity than on a scientific basis. Even though it is producedby fermentation, a process more expensive than chemical, lac-tate is used preferentially to bicarbonate in the manufactureof balanced solutions that are stored, because bicarbonatesolutions tend to decompose with the formation of insolublecarbonates. Available solutions of lactate contain tuh- racemicform of tha substance although the metabolim of d-lactate issubstantially slower than that of 1-lactate. /2/ Lactate andpyruvate concentrations in the plasma my rise tempoaarily innormal individuals receiviug lactate ion. Acetate solutionsare more stable and potentially cheaper to produce cemicallybut have had limited use except for peritoneal dialvsis.Plasma lactate and pyruvate do not increase with acetate,and plasma clearance of acetate is rapid. in certain circu*-stances such as in diabetic acidosis or in =-weic petientsundergcing chronic lialysis, there appears to be a slowing ofthe wtabolism of acetate ion; hence, limiting its utility.
k special case of acute acidosis is primary lactic aci-dosih in which the defeclt seems to be the irreversible con-7ersion of pyruvate to lactate which accumulates in extra-cellular volume producing a severe, progressive, and often
I'riwn• h n, '. i 9,1 I" .V,, 9. Sepirinb hr 19 7]
72:7
l1i-iicile% *'j 1'arctitem(. l7terap,i Ruidw and O7u'/acki
lethal retention acidosis. Alkali tberapy with bicarbonatehas been notoriously unsuccessful in promting salvage sug-gesting that reduced plasma pH is the misdirected focus oftherapy.
Parentcral Therapy) of Alkalosis
Clinioal states of alkalosis are less commn than acidotic.states and the infusion of acid to correct severe alkalouis isseldom required as an emrgency mamure. Although respiratoryalkalosis is freqnent, especially in patients with &=.ety oxcentral nervous system, injury or disease, the syMtoms arerelatively minor and nay be smjliorated by rebreatbig ('r 002administration. The respiratory alkalosis of salicylate in-
* tozication or liver disease is also due to central nervouss~imulation, but these saltes are complicated by ooinc;.dentor potential metabolic acidosis ind my fare poorl.7 with 002ztherapy. Metabolic alkalosis is most inaonly seen afterprotracted vomiting, nasogastric waction and diuretic abuse.It nay also follow successful therapy of acute pulmonary in-sufficiency with respiratory acidosis, I.e. patients who havesuffered prolonged renal losses of abloride whos& alkalosiswill persist until the chloride deficit is reploted. In mostinstances, repletion of chloride ion as sodium chlorids isadequate therepy because renal excretion of sodium bicarbonatecontinues -untU chloride deficit is abrogated. Coincidentpo'assium deficiency may intensify the metabolic alkalosis(vide infra). When chloride must be givon without sodium orpotassium, ammniumn chloride may be used, except in patientswith liver disease who are prone to hepatic oom. Hydrochloric&acid Wa be adainstered as a one percent solution,. or thehydrochloride of arginine or lysine may be given.
P.arenterai Pntavsuum Thierapy
Potassium deficiency is most often due to exaggeratedrenal loss, e.g. with chronic thiazide adminlatration orsecondary hyperalcksteronism. Substantial loav by the wayof the intestinal tract is less frequent, e.g~. laxativeingestion for many months. Because pottassium is effectivelyconserved by the normal kidrey, albeit scehat le"s efficiently
Prcscnz Czncep is. Vol I V No 9. Septem ber 19 71

7-'S
Prn'pho Parewnia ,I Iiicripi' Rithimand C hoinarki
-than is nodium., clinical deficiency cLausd by extzwirenal lossrequresweeks to develop. Equilibrilu is achieved with
potassium int~msu as low as 10-15 ngq/day. Most natiirel foods
Hypok..lemia is often., but not invariably., found inpotassium defi4ciency states. Sodium balance intiimtely affect,6wnrm pottassium and with severe malt depletion, serum potassilummay be increased while body potassium is reduced. Although anoversimplified tautology, the pbysician should re call vhenpotassium leaves the cell,. sodium and hydrogen. replaces it,and when potassium lossen are repaired and potassium enterscells, this ion flux is reversed providing for 3K = 2N&+ lB'-.The association of acidosis and release of cellular potaosiuminto the blood, sand of hypokalenia with alkalosis is theni~derfftood. Similarly, the renal taublar exchange of potassiumor hydrogen ion for sodium cha~racterives urine pH - when therenal tubular cell is actively conserving potassium, urine isacid; mhen the renal tubultr cell is wa~ting potassiumn, itexcretev less acid and urine is alkalin Thuso the paradoxicalaciduria of metabolic alkilosia associated with potassiumdeficiency -ccurs on2ly with extrareval causes of the potassium
deficit. Since Aidrini1s :bility to ooncentrate the urineoccurs early with potassium deficiency., the ftiadig of an
depletion should suggest an alternative diagno&4 .s. Urinepotassium concentration bel~ow 10 mI~q/L supports an impressionof potassium deficit., and monitoring of urine concentration
sium deficient patients waill not excl-vte infused potassiumbeyond minimal levels provided sodiumt reabsorption is notexcessive.
The uptake of glucose and production of glycogen by theliver my further reduce serum potsissiux end glucose infulsionsm-y precipitate hypokalemic pa-ralysis in subjects alreadypotassium depleted. For thia reason, glucose infus ions shouldbe withheld 'until petassium, deficit is substantially repletedand parents ral potassium should be added to saline rather thanglucose if severe hypokalemia Ia evident.
When potassium depletion, with or without 1iypokalez:.a,4is associated with arrbythmias, muscle paralysis or ile'uL-,
'rcsrn t (tmcc-pts. V!I V V9. Septem br1 13

IlrinciCph'v ,J Purente'ral llicrapy - Riebint and Othjnackl
partial rapid repletion of the potassium deficit is desirable.As the amount of potassium which has actually been lost isI clinically difficult to estimte short of whole body countingor by isotope dilution, therapy for the patient with normlrenal function is primarily directed to give a modest excessof potassiua and to depend on renal excretion to adjust forovertreatment. In the presence of oliguria or renal failure,pasenteral or even oral replaoent thorapy mist be approachedwith caution. The potential irreversibility of the renallesion of potassium deficiency suggests that even modest de-pletion is undesir'b1e. Uen clinical circumstance indicatesthe likelihood of continued potassium loss, especially withsymptows possibly caused by potassium deficziency, the pre-ventive treatment of potassium depletion is justified. Ifpotassium cannot be given orally, parenteral administrationis advisable.
The practical approach to parenteral therapy requires aready willingress to include potassium in parenteral. regimenswith special attention to correction of coincident deficienziesof sodium and chloride. Once urine flow is assured, and inthe absence of accelsrated tissus catabolism, potassiva canbe given in solutions of 20-/40 Aq/L at a rate not exceeding20 u~q/hour.
Kunin et al /3/ and Clementsen /4/ indicate that potassiumWay be infused at 40-60 mzq/hr provided that glucose is g ien
simIltaneously. The presence of severe potassium depletionmay limit the rate at which potassium salts may be infusedsafely. Animls deficient in potaselux aie readily made hyper-kalemic at rates of intake of potassium tolerated with impunityby Anmals previously fed a potassiuR excess. TABIE IV.Becai-se hyperkalewia may rapidly develop, alectrocardiographicmonitoring is advisable with parenteral potaasimt iufusions.
The most oomon clinical cause of hypokaleuia is upperintestinal aspiration. The splinting of the upper gastro-intestinal tract by continuous gastric suction is a cmonprocedure of surgical managewent. That hypochloremic alkalosisand hypokaleaia nay occur is broadly acoapted on most surgicalservices. The mechanism of such alkalosis, ofteu incorrectlyascribed to the rwoval of potassium in the gastric aspirate,is a result of the progressive depletion of chloride, as chlo-ride concentration in gastric aspirate is generally in excessof sodium. Becuase of mild dehydration, hypovoleola andsurgical stress, there is a coincident stimulus for sodium
I'r•'¶,:'t (',,iicpl�t~. V v'i (1. Srptcmhcr 1971

IIrw , qli". of I'jreiacraI lwrcrei~i kul',,i aund (lripiacbg
TA~RU IV
DIETARY IhEPEUT ON POTASSIUM TOLERANCEMortalitty Figures on Four Groups of Eight Rats'
ORAL STRESS PARENTrERAL STRESS(100 grnl4hr)
K Itae 21S 511 10 Intake 0.1 mEq 0.5 mEq 0.1 mEq
l ow 0 2 9 9 Low 2 8 .. ý
Normal 01 0 3S Normal I 2 8
I igh 1 5Hg
Rah tcpr-Ied pota%%ium arc rcLt~tnt to potaisurn strevs rats depleted of potaw'umarc senmitized.Oral -trc~s wajs induced hythe addition to dnniking water of increasinfly concentrated solutionts ofK(1 for four days..Wt 2-10prcn solutions. gavage, feeding was employed bccaure some ratsttufuscd to drink; the volume adminitered was the avenage imbibed by the one-percent poup.
Parenitcral stress wast given :ntr-aperitonca!Iy in 2 cc volume; sodium chloride %%2s added to themore dilute solutions of potassium to make 211 solutions cquimnohe. Nephrectomny increased over-allmortalitv but failcd to alter the relattve protection of antecedent prefeedingr or the sensitivity of ante-cedent depletion. indicaiting that the effect is most hikcl) operative at a cellular level. Mechanism ofdeath;%s unknown hbut probably due to acute cadiac arrhythmia.
retention. Bypokalemia. also reflects the renal adjistmsntas more potassium is excreted in exchange for sodiuma in thepresence of alkalosis. The degree Of~ alii is usuallymoderate and its importance is more to stiztulate recognitionby the physician of the abnormal physiologic State than toconstitute a serious stress to postoperative recovery. Iffluid andi caloric requirements are met., potassium need notbe added for ei-yerl.l days.
Potassimr cencentration in gastric fluid is generallybelow 20 m-Ma/L anri falls With continuous gastric aspiration.Removal of severa2. liters by gastric suction withdraWs fromthe body less that, 100 nEq of potassium., andI deficits of this
magitdeare tolerated with Iiapnity by the individual notpreviously depleted. Howeveri, the Superimposition of glucio-corticoid stress undier these circtmutanoes my provoke a dropin sertm potassium and the dyeVo0PMt Of mild metabolic
1'rescni (,ipti -pti. VtiI V Vei 9. Sepicnzbe- 19 71

PrI::im,,'I ,,J I'r Run i ,at f Ili( rapv i ,ubitu ::d (T:t4 l ta: At
alkalosis with minimal change in overall body bhlance.Similarly, the elevated serum potassium in nephrectomizedadrenalectomized dogs allowed to develop an Addisonian crisisis substantially corrected by glucocorticoid administrationindicating that the gradient of potassium across the cellmembranz is critical to its plasm concentration, independentof whole body content of potassium. With protracted gastricaspiration, parenteral administration of potassium is advis-able, especially in patients who have been chronically illand are likely depleted of potassium before surgery. Theproblem may become further compounded by the need to admin-ister glucose feedings which promote glycogen production, asserum potassium may decrease further and cardiac arrhythmiasmay result, especPlly if the patient is digitalized.
The repletion of potassium losses under these circum-stances is dependent not only on the administration of ad-equate amounts of potassium, but also on the concomitantadministration of chloride ion. The use of such pota3siumsupplements as gluconate, citrate or phosphate may fail tocorrect alkalosis and hypokalemia unless adequate amomuts ofsodium chloride are also given. As the primary mechanism ofalkalosis is chloride deficiency, the use of ammonium chlorideor lysine monohydrochloride might be considered and, in mostinstances, the serum potassium will rise.
The amount of potassium that can be conveniently andsafely given parenterally is limited and full repletion ofbody stores must usually await reinstitution of oral feedings.Ideally, the potassium requirement should always be given bymouth and preferably with normal foods. The institution ofa reasonably normal diet with offer at least 60-80 mEq/day.When larger amounts are required, potassium supplements areuseftal, but enteric coated tablets containing potassium chlo-ride should be avoided, as small bovel ulceration and stenosishave been reported.
The ratio of nitrogen to potassium in protoplam is con-sistent from calculations ba&ed on losses during starvation,retention during repletion of protein deficiency and fromdirect carcass and muscle analysis. Hovever, nitrogen canbe retained (protoplas formed?) in absence of potassium.Figure 2.
S/'rc•' ft C ,,;++''i l.,;I \ , (+ .Scpicp r bcr 1971

Pr,,~ iu~c ~'IIdr,,hral ~ur:~~ - kl~n, ad (7~'iwcA
-20 DEPETIO
G1m RPETO
__________ TESTOSTERONE _
4 e :2 Is 20 24 29 36 40 44 48
I ic 2 (;rihit iI~u~tration of testostcrone-induced positive nitrogen balance occurring in the prcwnn-c,[f puitaw~uum depiction.
ACUTE: VOLUME DEFICITS
The fundamntal defect in shock is a reduced perfusion oftissues to a. degree insufficient to sustain jstabolic function.This may be due te E de~cline in blood pressu~re or increase inthe peripheral resistance to blood flow as well as to inadequac~yin blood volume. The stupor, coldness and pallor of the skin,weakness of the peripheral pulse, and oliguzia represeent theeffects of decreased blood flow to specific organs. In additionto the initial iscebuic derangsimnts of prinary function, aseries of secondary deleterious metabolic effects involving theliver, brain, kidneys and endocrine glands exaggerate exid per-petuate the shock state. Accomipanying these secondary changesis acidosis, reflecting the altered oxidative metabolim oftissue. From the point of view of parenteral therapy, thecritical repletion is that of volum, as the fundiamental treat-ment is improveusnt of oxygenation of tissues., rather thin thetemporary correction of pH.
I'rcwcn! ( 'nci.I ' I I" 'J.!pirmcnihr 19 71

Prum, ipl,% j, 'arc,', rat 17,rap - Ruhtm i.,d (h ',na'k
The central blood volume is about 50 percent of wholebody blood volume and it is equally divided between thethoracic contents and the splanchnic bed. Approximately 75percent of the blood is normally contained in the venoussystem and an additional 12 percent is in the capillary beds.Because veins and capillaries constitute a low pressuresystem, small changes in pressure may cause striking changesin volume. The converse holds true in the arterial bed wherevolume elasticity is minor and large changes in pressure mayoccar independently of arterial volume.
In defense of the plasma volume, extravascular albuminis released from the liver and lymphatics in an attempt tomaintain oncotic pressure and thus draw fluid from the extra-cellular space into the plasma. As the extracellular spaceis some five times the plasma volume, it may be consideredan unlimited volume reservoir provided sufficient protein isavailable to maintain the necessary oncotic gradient. Theplasa protein reserve is modest and probably no more than25 percent of total bcdy albumin exists ext-'vascularly. Theresponse to acute hypovolemia is therefore limited, and afterthe plasma protein reserve is mobilized, further correctionof hypovolemia depends upon transfusior -f aJlkmnn or plasmaor the introduction of an oncotic equivalent.
A number of plasma expanders have been utilized. Theseinclude materials prepared from natural biologic products andartifically synthesized macromolecules. In general, nonehave proven ideal, and such complications as retention in thereticuloendothelial rystem, allergic reactions, antigenicity,disturbed clotting, capillary fragility, thrombosis, aggrega-tion and clumping of erythrocytes, and impaired flow throughsmall vssels resulting from increased viscocity have beennoted. Artificial expanders such as poLyvInyl-pyrrolldone,gelatin, and hydrozyethyl starch have been gradually sup-planted by a dextran. Biologic products such as lyophilizedplasma and modified human globin have proven less satisfactorythan concentrated human albumin.
In burn cases, decreased plasm volume occurs secondaryto trapping of plasma outside the normal vascular volume, aswell as those losses due to weeping and evaporation. Asimilar transcapillary exudation occurs with certain bacter-emias. With intestinal obstruction, largs quantities ofplasma and its ultrafiltrate may be rapidly conpartmentali.adas an unphysiolcogic "third space' in the bowel lumen. With
I'rc•'ctf (',,n l%'I. I,,ill , /1 .Scptcrmbcr III1

/t.IIJ'rii h tii ,j hIrt itir u Ilchrapr- Riuhim wid (7tuuji tAi
barbituate poisoning or endotoxemiO infections, rassivesplanchnic dilitation may trap a substantial portion of theblood volum. In these instances, the par~,nteral therapyrequired is substantial and often of massive proportic-n. Evenin these coplicated examples of hypovoleuja, recognition ofthe exact cause of shock is often less imdiedtely vital thanits alleviation, but ultlmately is critical to successful-nagewent.
As plamsM volume reflects the extracellular volume ofwhich it is an intimate part, decrease in extracellular volumefor any cause increases sensitivity to shock; and salltipreloading is protective. Figure 3.
NORMAL DEHYDRATED TF.-ATED
ECF ECF-~ I
ICF ICF , ICF
IIBODY WATER 55% 40% 50%
OUTSIDE 1:3 1:2 l:13•INSIDE
] EXTRACELLULAR FLUIDPyTPACELLILA! FLD
I 3 Relativc dIsLrinuion N-Id cora.par•aentahmzaZion of body water in -nrmalc) and in dchydrautonuilh and withoul partial saline replaccment.
PIRFNITI'RAL TiftRAP) I\ RELATIONSHIP TO SURGERY
The management of a patient through surgery is a test ofthe physician's understanding of fluid and electrolyte problems.Coincident with the direct trauma to tissue may be probleus of
I're.,ewt C'occpts. r'd! lI A v, 9. Septe "er 1971
ME
-75
rlimt th1 % of Ian ri ,itral Ihcrap - Rutmt a; d (CtIoJpid( At
anesthesia, immobilization, .starvation, protein depletion,dehydration, sweating, renal and cardiac insufficiency.Relative hormonal deficienci.s or imbalances involving thepituitary, thyroid, and adrenal glands may develop. Inad-equate replacement of acute deficits because of vomiting,diarrhea, upper or lower intxtinal aspiration, and others,may complicate the issue.
The imobilized postoperative patient depends uponmedical action to maintain body homeostasis. Saperimposedis a hazily demarcated syndrome generally terms "the injuryreaction". Despite extensive study two decades ago, surpria-ingly little is known about the mechanism of this catabolicstress. It is composed of a series of physiologic responsesthat append surgery and influence fluid and electrolyte man-agement. These responses include an increased urinaryexcretion of nitrogen, the loss of body weight consistentwith the mobilization of fat stores, an increase in bodytemperature, pulse rate, and oxygen consumption despite aieduction of respiratory quotient, and diminution in urinevolume with increased urine concentration. Sodium retention,potassium loss into the urine, hyperglycemia, and increasedurea production due to enhanced catabolism of protein char-acterize these states. Cellular loss of potassium with hyper-kalemia and fat mobilization with hypertriglyceridemia mayalso occur. With diminution of urine output, there is aninability to excrete salt-containing parenteral fluids despitean increased solute load of urea due to prerenal azotemia.
An increased secretion of adrenal corticosteroids couldexplain many of these findings, but the injury reaction mayoccur in the adrenalectomized patient receiving constant dosesof gluco- and mineralocorticoids and is minimized in the verysick and in the very old. This surgical response is maximalin the robust young, healthy patient underoing elective surgery.The fact that these physiologic changes are the normal andusual accompaniment of uneventful surgery should be recognizedby the physician. Attempts at their modification by largedoses of androgens, high protein feedings, and other measures,have been largely temporary in effect. A recent trend hasbeen preoperative anticipatory treatment with loading of water,potassium and protein for repletion of unrecognized deficits. /5/
The duration, as well as the magnitude of the responseto surgery depends to a large degree upon the overall healthof the patient and the extent and type of surgical procedure
Pri ,,n ( n ',• r, II \ Q . .Septe ber 191-I
47'

performed. Especially prominent responses occur with invasionof the pleural or peritoneal cavities or with trauma to theskeleton. When surgical complications are superimposed, thepattern of metabolic rebponse to surgery is further altered,and recovery is deferred as starvation and immobilization 8reprolonged.
Postoperative parenteral therapy depends on the degree ofderangement ard the time anticipated before oral feedings canbe restumed. if recovery is rapid, and postoperative courseuneventful, the potentiality of electrolyte depletion my beneglected and a vates, intake of approximately 1000 cc in excessof urine volume given daily. Preferably, this should be as a10 or 15 percent glucose solution to minimize protein catabolism.If oral intake must be postponed until the fourth day or longer,modest amounts of sodium may be added to match urinary excretion,remembering that salt retention is the usual acute response tosurgery and a natruresis may be prominent during the laterrecovery phase.
As potassium deficits over 100 mEq may approach pathologicsignificance, potassium balance should also be considered.Homeostatic requirements of potassium during prolonged parenteraltherapy are readily met by the inclusion of potassium parenteralregimen in concentrations of 5-10 mEq/L plus additional potassiumto make up known external losses. The amount required must beassessed individually with a concerted effort to give potassiumslowly and to implement oral intake as soon as poscible.
There may be some advantage of giving phosphate in chronicparenteral therapy because phosphate is the main intracellularanion, and presumably behaves in parallel with tissue potassiummovements. There is also some evidence for a phosphate deple-tion syndrome in man characterized by anorexia, weakness,skeletal pain and malaise which can develop with protractedlow phosphate intakes, especially if phosphate-binding gelsare ingested. /6/
Whether magnesium should also be administered is uncertain,although prolonged parenteral therapy of magnesium-free fluidswill undoubtedly result in mild mangesium depletion. However,there is inadequate clinical correlation of symptomatologywith serum levels and quantification of body magnesium stores.The adult human body contains about 25 grams of magnesiumequally divided between bone and soft tissue. The metabolism
• .I'rccnIC'i¢ f s, ,, I't I ,,/I | \, :. .S'¢picimher v -J

Arm,; ipw.s of hrcnu'ral Therapy'- Rubini and Chojnacki
and excretion of magnesium varies with a wide variety ofpathologic and physiologic a~lterations and is only partiallyrelated to intake. Average excretion in the urine is100-=0 ag/day on an intake of approximately twice thisamount. A -ininium requirement for magnesium in man has notbeen define-d, and production of experimental magnesium do-
maisienc bwinthedsrawocuing aansu frmthe ocndietions wiee-reoute oonrt pt~aftero aany wes obclinical Fan deficinyidi-
inseyi ishoteer is cleritcly diaognosie citeari-al, esereclevel-: balelo 1.n0 lambjshol alrThe plnca yndician ton the osibiler
prseo hyof magnsiu defic utiensscy.iastric wice co~ntainswpichxin levia1.0 by/ aivng magnesium deficinot bay occurgainm patienes witspcle trmos..tritchciong oiare withebyptssothomlr. bn onelulsionbis smyfalsc.urit pRolonged develsenof
magesim i th sea ccu ina umber of condictions with-magnoesit should be sufficient to maintai dagnesienc balance,ficut toaderfionts mayl bhe preseded torelt antncedent defia-
syptase. possbydft magnesium deficiency, &r uc condtaionsdppcx~tly1. xq athagesu deiinymaynesiurin atent wth roongZ avo ridch auctionar dwitatioypando
theseal bowetinlie pborofuse swraeatWing, orolexterna drainagencof paalinteblepnrai fluid, hhrpteincuso or lo intestinalyosecretioshol The intestienal taclosseintare mgessentbalane.ibuolargto launsmyb aneedtheir replaeteanteiscubstntdeic-lisotnicy oifm chlorgeide is donsidertdiascations owmtaoicthlsisku orapossis due to iantestinal lossces has endisiossed
A tesifiple sc hereaofrepeteac lsset of intstna secretions.2ihse shwnigh TABlud profuse swacid-bas orexternal daritraryofeasuret bfaidity oanreai akluiit reaive tor plow intsed o
seretai oneps. The intsia trac lo.e arecbe 1971,ýll
iwoa opas n hi -paeeti usatal

I7PrI,,ctph'e of IVarc' 'rul ileraplv R ubhmi und C7hojficak
the chloride content. Note that normal saline falls withinthe range of the aoid-base index of gastric aspirate and,
repleted with saline. Pancreatic secretion is highly alkaline,
especially in the case of pancreatic fistulae, while aspiratesof the upper bowel are less alkaline due to acid stomach fluidadmixture. Despite extensive praootional literature extollingthe advantage of solutions whose composition aims to mimicspecific intestinal losses, most patients with normal kidnyfunction are able to adjust urinary excretion to compensatefor moderate alkalosis or acidosis if only saline is givenfor replacement. However, in the case where several litersof f.uid, arc, being drained or aspirated, it behoovou thephysician to institute careful collections of all exteriorizedsecretions, to measure their volume, and to analyze thes atleast for sodium chlorlde and potassium. In practice hisgeneral principle to follow is - implement Judicious re-placement of known losses and then give scvemhat more thanis lost so as to replete previously unrecognized deficits.
1. Barry KG, Brooks MH, Hano JE: The prevention of acuterenal failure. In Renal Failare. PhiladelphiaJ. Lippincott Compan', 10 7, pp 259-Z71.
2. Watten RH, GutMan RA, Fresh 3J: Comparison of acetate,lactate and bicarbonate in treatitag the acidosis ofcholera. Iancet 2: 512-514, 1969.
3. Kunin AS, Surawicz B, Sims EAH: Decrease in oear potassiumconcentrations and appearance of cardiac arrhythnias duringinfusion of potasaium with glucose in potassium-depletedpatients. N ew J Meda 266:228-233; 1962.
4. Clementsen HJ: Potassium therapy. A break with tradition.lancet 2:175-177, 1962ý
5. Abbott WE, Krieger H, Holden WD, Bradshaw J, Iesey 3:Effect of intravenously administered fat on body weight,and nitrogen balance in surgical patients. YAtabolisma6:681-702, 195t.
6. Lotz M, Zi-an E, Bartter FC: Evie.ence for a phosphorusdepletir-n syndrcve in man. New _3 d 278:4D9-45, 1968.
'j"c (',i , Cet f pt'. "iIl /1' I ,V, 9.cplemher 1971
I )ia.igni,,. *•arta.rgCrn.n ( ornplhc:riions and Prognosar in .War /.one Setling
.CI)R John 1). (:onger, MC, USNI'
Acute tubular necrosis and other nephropathies havecontributed to mortality and morbidity in war-related injuriesand diseases since accurate medical recording began. DuringWorld War II, 40 percent of severely wounded casualties hadsome degree of acute tubular ischemia at postmortem examina-tion. /1/ In the fib-st year of the Korean War, morphologicallydetectable tubular necrosis was seen in 18 percent of theautopsies carried out after battlefield deaths.* Mortalityrates among patients with acute renal failure accompanyingwar-related injury and disease, determined primarily by theseverity of the underlying condition and associated compli-cations, have varied from 10 to 90 percent. /1-4/
The management of acute renal failure is challengingand involves meticulous attention to the details of fluidand electrolyte therapy. Development of effective methodsof dialysis has provided an additional modality in the treat-ment of acute renal failure. Its adjunctive value is beingevaluated in the combat setting of Vietnam.
The purposs of this report is to present the author'sexperiences in the treatment of acute renal failure as itoccurred in the battle zone enviroznent of the I Corps regionof Vietnam while he was aboard the US Navy Hospital ShipsSANTUARY and REPOSE from January through October 1970. Thediagnostic criteria, etiologic factors, modalities of manage-ment, clinical complications and results of the managementare presented and discussed. Guidelines for improved methodsof treatment are suggested based upon the results of the study.
*In part. aI articic ipparcd in US' Aoatv Med 57:1971
÷Ncphrohlgm,. NaialI Ihopilal Oakland. Oakland. Cahifornij 94627
*Shrciner (I Per, Mhal c"pcrcnk-c. Korean War. 1951
I'rceeUtl C',n epis. I I N o' 9. September 19 71

"t Ii t I, R, Itu lugtl in m IWar ltai. . ý , i
In January 1970 a program for the treatment of patientswith acute renal failure was instituted aboard the USS RFeose.When that ship left Vietnam waters in MArch, a similar facilitywas established on the USS Sanctuary. The dialysis unit con-tained two beds, bed scales, a Travenol® 100-Liter Win Coilartificial kidney and material for peritonoal dialysis. Thetechnical staff included two nurses and four corpsmen trainedin the operation of both hemo- and peritoneal dialysis.
Patients were evaluated on admission by the author.Surgical consultations were obtained as indicated. Baselineweights were determined, followed by daily, pre- and postdialysis weights. The following laboratory studies wereobtained on a daily besis: complete blood count, blood ureanitrogen (BUN), serum electrolytes, calcium and phosphorus;coagulation studies - prothrombin time, partial thrombo-plastin time, fibrinogen and platelet count; blood gasstudies -arterial pH, pO2 and pOO2. Routine urinalysis -,sperformed on available admission urine as well as electrolyteconcentrations and evaluation of the sediment for formed ele-ments. Urinary myoglobin and hemoglobin levels were alsodetermined. Cultures were taken of all wounds, drain sites,sputum, blood and urine on admission, every three days there-after, and at other times as clinically indicated. Bloodcultures were also obtained after each dialysis. Retrogradepyelography was performed when historioal factors or physicalfindings suggested possible obstructive uropathy.
N.,ute ofI RenaI h,,lur
Tventy-four patients were referred for care during thenine month period described. TABLE I categorizes the 24patients by sex and national origin. The nean age was 25years. All but. five of ths patients wore active duty Americanmilitary personnel. The referring facilities inc~luded themajor military and civilian hospitals in the I Corps area ofVietnam. TABLE IM. The mean time from injury or onset ofillness to transfer to the dialysis unit was 4.5 days, rangingfrom 2 to 9 days. In 19 of the patients renal failure followedtrauma; nontraumatic conditions were etiologically related in
I'r,.et/ (',t,' clit. VW,I .1 , Na 9. September 1 9 71
- - i~-~ - - - -

Ac'u Renal I " r" in IW'ar l/him ( "ng'r
I'ABI I- I
PATIENT DISTRIBUTION
TOTAL 24
SEX Male 23Female I
MEAN AGE 25
AGE (2-47 years)
ORIGIN MILITARY 22American IsVietnamese 3Korean I
CIVILIAN 2
1ABLI: 11
RIEFIRRAL DATA
F4A0ILi rY PATIENTS
SANCTUARY 685th Evac 4NSA 3Ist Mcd. 6REPOSE 2Hue Prov. 295th Evac I
five cases. With the exception of two Cases with extensivebmrns, the trauzatic injuries were ibe result of a widepenetrating-comabat-missile spectrum. TABIZ III. In thenontrauma group, one instance of each of the following con-ditions was encountered: falclpartm uluria, reticulucell saroma with hyperurioemia, methanol ingestion, acuteglomrulonsphuitis and prolonged diarrhea with dehydrationand shook.
TABLE Ir records the total number of exposures topotential etiologic antecedents of acute renal failure that
Present Conteps. Vol iV No 9. September 19 71
e - - -, - - "

were vxp~erienced. Although nearly all Patients had received
blood, no transfusion r-eactions were documented. Hypotensionof variable severity either at the time of injury or duringsubsequent surgery, i-iffuse sepsis, and brief courses oftherapy with nephrotoxidc antibiotics were common. No casesof obstructive uropathy were discovered.
TAB[ E. Mi
1:RFRQ11- NC Y OF O RGAN TRA UM A
Exlrerit~e\16Stsl* ltý,uc. lirtj( Krt. 9Niulliple Jflipu~zttion 5 JSir.yc .imputlllon% 2
B'.we 12I SIK
Liver 4soleen 4
Vm:.sla~rKidnceý 3('NS 4Burn,.
i'ABLE IV
RENAL FAILURE ANTECEDENTS
Irrantcrimomi 17
Scp'.pr. I io
10k.,neijn% (in. strcptomvcln.
(.i.C litc aIter failurepe1. tirtu'in
Twenty-one of the referrals suiffered an olig-iric fc'M Ofkidney failure. There were three patients - all with bilateralamouta.aions of the 'Lower extremities - who presented Withrising BUN and seruim Dpotassium levels despite urine voluinerover one liter zer day. For those with oliguria, the mean tineof onset was three days postl, injury or illness, with a rangeof 0-5 d:L s. The avera~s duration of oligguria was 8.5 day'swith a range of 2 to 15 days. Diuresis failed to occur in anyof ithe patients wh17 expired. TABTZ V.

743
4ciair I-reuaI auhi~re in i1'ar Ionic C :gi
Non-olguric3 patientsMean onset post injury 3 days (5-0 days)Duration (survivors) 8.5 days ( 15-2 days)Diuresis (expired) 0 patientsSurvival time of thws
expired I I days (3 1-1 days)
Mean admission laboratory values and rangas are shown inTABIE VI. The low bematocritis occurring in the majority ofthe patien~ts were the result of blood loss due to tramm anda variety of coagtilopathies. Elevated heniatocrits: were presentonly in ths two buirn patients. Elevated white blood countsreflected the septic or stress-hypoxic astates in which mostreferrals arrived. TIM BUI' s were not excessively elevatedbecause of the relatively short periods of shutdown prior totr.ansfer. Hyponatrenia. was eow~on in both the trauma andnontralmia groups except for those with burns who were hyper-natrm~ic. Due to frequent nasogastric auction and intestinaldiversion procedures, hypchlomrie-hypokalemic alkalosis wasnearly as comon initially aa hyperkaleuia with acidosis.Severe acidosis was observed in patients with combined massivetram and aignificant hypoxemia from pulmonary coimplications.in can be seen in TABIE VI, bleeding and clotting abnormlsitieswere frequent. The two mejor typea of disturbance were a dif-fuse intravascular coagulation most ofte+n associated withsepticemia., and the factor-deficiency syndr associa'tedwith atiltiple transfusions of stored blood. 'The single patientwith falaipariz mAlaria developed an isolated throubocytopeniarelated to the disease and quinine tberapy. Blood gas deter-mirations reflect the high~ inc~idence of pulmonary problems.The usual. physiologic defect was a ventilation-perfusion im-hs~lanos with hyooxa. and bypocarbia. The underlying pathologyin nearly every case was either severe lung contusion, necro-tizing pneumoniti3, or thb so-called Nwet lung syndrome". /5/Urinary electrolytes and sediment analysis were valuable inassessing the cause of renal dysfunction and in separiatingthose with pre-renal azotemia from those with intra-renal.pathology. Seventeen of the 20 patients with oliguria had
Present Cmicepis. Vol /V No 9. September 1971
- ~ -. - A-4

7.14
wh~, R• in I wlirt in I|'at /,w t,,n~ger
IAIIII VI
AI)MI''%I( N I A,()RAIIORY VAI IIFS
I MI AN RAN(;I
I lcmatocri(111) 31 50-19
White blood cells(cu rmm) 14.000 2.300-24,300
Blood urea nitrogen(mgIIO0ml) 73 150-30
Sodium(mEqiL) 130 151-110
P',tassium(mEq/L) 4.8 7.4-3.2
Chloride(.al'qIL) 89 105-68
Iwo3(mI'q/L) 19 36-6
Plaltelel cotomn(cu rmim) 120.000 32.000-278,000
lrotlhrohmin IItite(.co 17 24-13
Partial thromboplastin time(sce) 43 55-35
Fibrinogen(mga I OOmI) 150 300-50
pH 7.30 7.50-6.91
PO0(mmHg) 83 117-40
PCO,(mmllg) 32 43-24
URINE
5Sod an m
(m )q/L} 38 70-12
0 20 mhq/L 17 patients)( 20 mFnqlL 5 patients)
(Pigmented granular costs: 20 patients)
Presc-n; ('(,nc cp.tVo I'o V /V 9. Septenyber 197;

I, " IwiRnal l.'alur" in War on '- (Conger
urinary sodium concentrations grea-ter than 20 mEq/L. Detectionof typical p~gmnted casts of acute tubular necrosis on micro-scopic examination of sediment proved to be the best indicatorof frank renal shutdown. These casts were found on urineexamination in 20 of the 23 patients. Osmolality studies wereof less help because a number of patients had received osmoticdiuretics prior to admission.
MANAGEMENT
Attempts to induce a diuresis were made in nearly everypatient, either at the referring facility or shortly afteradmission to the dialysis unit. TABLE VII. On one occasiondiuresis occurred following the use of saline and albumin ina paraplegic patient with unrecognized peritonitis and a per-forated gastric ulcer. Using ethacrynic acid, a temporaryincrease in urine output occurred in two others, but was notsustained despite continued use of the drug. Response todiuretics did not appsar to be dose related. Where transientdinresis followed ethacrynic acid therapy, only 25 mg of thedrug was given, intravenously. Subsequent trials with higherdoses in these patients, and up to 150 mg of etbacrynic acidand 160 mg of furosemide in others, were not successful.
TABLF Vl1
ATTEMPTS AT DIURESIS INDUCTION
NO. TIMIS TEMPORARILYA(;i N I USED aUCCESSFUL SU"CFSSI UL UNSUCCESSFUL
I'liua cxp,,ndcr I .. 7
Hhacryric acid 9 ... 2 7
Mannitol 7 ... ... 7
Furemide 4 ... ... 4
The severity of the complications of renal failurepresented by the patient, determined the initial modalitiesof therapy. Those presenting with pulmonary edema, hyper-kalemia or serious neuro2ogic :xnifestations of uremia
l'recent (,ncepI. VWi I V N,, 9. September 19 71

I (!(i Rt I a llr 11 Ii :I / 9i ( , ,.i1i'( i
underwent hemodialysis following immediate placement of4ainton-Scribner shunts in an available extremity. A programof fluid, potassium and pro-ein restriction, coupled withhigh parenteral carbohydrate koccasionally sodium bicar-bonate and insulin intake, was initiated in the less criticalcases. Kayexalate was used to control ser-um potassium.Sa.nting and dialysis -were undertaken in these patients Lhen(a) the serum potassium could no longer be maintained below6.0 mEq/L, (b) the BUN reached a level of 110 to 120 mg/i00 ml,(c) there was evidence of progressive wound sepsis and delayedhealing: or kd) the overall clinical cordition precluded thecontinued use of the initial conservative program. Periods ofhemodialysis varied from four to eight hours, were most oftencarried out ev., _- other day, but frequently daily and occa-sionally every third day. Regional heparinization, althoughused initially, was replaced by a system in which the LeeWhite clotting time was kept in the range of 12 to 15 minuteswith small, intenmit÷vent doses of heparin, and blood flowrates were maintained continuously at. 250 to 300 cc/min.Dialysis was carrieQ out with whole blood, packed RBC or nocoil priming depending upon the volume and hematologic statusof the patient.
Pezitoneal dialysis was used in thcse patients withoutmarked catabolixm who had intact peritoneal membranes. Theaverage duration of this method of treat, nt was 48 to 72 hours.
In addition to managenent of the renal failure, intensivetherapy -was undertaken to alleviate underlying and associatedsurgical and medical problems. Primarily this involved anti-biotics with debridement-drainaee orccedures for septic com-plications, hyperalimentation pro1reins to promote wound heal-ing, ventilatory therapy for progressive pulmonary insuf-ficiency, and treatment of coagulopathies.
Increments of blood urea nitro=-en were calculated dailyfor all patients. -1;_U3 T iii. .Tlthough there was some over-lap, it is evident that the catabolic states of tissue damageand pyrexia increased the rate of rise- of the BUN. In septi-cemia patients with lar•e areas of soft tissue injury, dailyincreases o'f BT7UN were consistently over 45 mg/l00 ml. Seven-teen cf the 23 patients reQuired dialvsis. The remaindereither did not need dialysis or expired before the manifestclinical indication for it. There were 49 hemodialysis runs
Pr, , ,S ,r

747'
*.h :twc Renal I"ahur m War Zone - C,,ger
1 %III I viii
I)AII Y IN( Ri-MI \IS IN 131.001) URI-A NITRO(;EN(Ia,y li(XJI Id)
%if AN RAN(,I°
STrau mna 28 (62-I10) •
!•Non-traunia 1 2 (31- 4) e
I'ebriie 25 (62-11I)
Afebrde 16 (30- 4) •
carried out on 12 patients with an average of four dialysisruns per patient. Peritoneal dialysis was used six tims onfive patients. TABLE oX..p-a
TABLE IX
MODALIT!IES OF MANAGEMENT
NO. OF PATIENTS NO. OF DIALYSES _
SDialysK 17 Hemodialysis 49lieniolialysn, 12 No. pe: pt. (average) 4Peritoncel dijlNs,s 5 Peritoneal Dialysis
( onwcrvative (No tihlysi'q 7
?re- and -st-dialysis laboratory values are shown inTABIS X. In ge,.'ral it can be seen that dialysis was effectivein improving metabolic parameters. BUN and electrolyte cor-rections were intentionally made by -mall increments in orderto avoid neurologic, neuromuscular and cardiac complications.The mean decrement of BUN was 52 mg/lOO ml per dialysis.There was considerable variability, hMwever, as can be seenfrom the table. Ultrafiltration was varied according to thehydration status of the patients, which accounts for the widerange of values. On one occasion urea was added to the bathto retard the rate of urea removal, rein:ting in a 15 mg/lOO mlincrease. The situation occurred in a patient who developedseizures following an initial dialysis during which the BUNfell from 200 to 86 mg/l00 ml. A second dialysis was requiredwithin 2-4 hours because of recurrent hyperkalemia. Urea wasadded to the bath to prevent the likelihood of further neuro-logic manifestations of dysequilibrium. /6/ 3
Ir,' nt ('t c,,,p i. 1.' 11' \,, Se .cptcmhcr 1971
U: 7

748
.l,.hn Rital I aihlrc" ti War Zirn- (-ioliger
I AlIl P- X
I AW)HVA IOIRY VAI II. S
-'RI IIAI Y-I%110%1i DIAl Y;I%
%fran Riangc Wall Range
Blood urea nitrogen(ng/1 00mil) l19 208.0- 15.0 77 140.0- 15.0
Sodiu'n(inEq :L) 133 141.0-110.0 138 149.0-128.0
Potassium(mEq /L) 5.7 9.5- 3.1 4.0 6.7- 2.7
Chloridc(nEq L) 88 106.0- 64.0 95 106.0- 75.0
1lC'O.•
(i-lq 1 ) 22 36.0- 6.0 19 24.0- 14.0(Calclull -5
(,ig I/l (IW 1l 6.2 10.0- 4.1 %.0 9.6- 7.0
Blhod eij nitrogen
(figp I(l W 1) /dialysis -52.0 .114 to +15
Weight(kg) /dialysis -2.0 -4.2 to +0.7
COMPLICATIONS OF DIALYSISThere were five instances in which clinical complications
were related to dialysis. Two were neurologic ,ith one patienthaving recurrent seizures, the other progressive lethargy andsomnolence. Both were transient and probably resulted from toovigorous dialysis. Fever occurred twice. Once it was thoughtto be a reaction to blood used in coil priming. On the otheroccasion, a fever spike with parasitemla developed in thepaticnt with falciparum malaria. This occurred after he hadbecome afebrile and had had negative Malaria, =ears for threedays. It was conjectured that the plesiteaxia va related tothe rate of quinine removal with dialysis. Gastrointestinalhemorrhage from unrecognized duodem•l ulcers began at thetermination of a dialysis run in one patient. His coagulationparameters were normal at the time bleeding was first noted,but a Lee-fnite clotting time of 20 xim~tes had been obtainedearlier in the run, following a dose of heparin.
i'rc•citt ('P,,u pis. I',,/ IV No 9. Septembcr 1971
Ua -- ~-.~- *-

74v
Acute Renal iiiilurv in W~ar Zone - CongerIITfif mrnjor ',llnlcaJ complicationa for all patiLonts from
the time of initial managpment at the referring facility untildisposition are shown in TABLE XI. The most frequent problemswere related to sepsis and occurred exclusively .'.n the traumagroup. Positive blood cultures were obtained in 12 patientswith documented 3epticemia. A single instance of Pseudomonasmeningitis was associated with Pseudomonas septicemia.
TABLE XI
CLINICAL COMPLICATIONS
Sepsis 51 Gastrointestinal hemorrhage 5Wound infection 16 Encephalopathies; 5Septicemia 12 Wet Lung Syndrome 5Pneumonia 7 Acidosis 3Peritonitis 6 Arrhythmiias IAhscesses 6 Hemopneumothorax IUrinary infections 3 Atelectasis IMeningitisI
TABLES III and XIII provide additional data on infectiouscomplications. (-ther relat-ively common problems were gastro-intestinal and wound hemorrhage, encephalopathies due tometabolic abnormalities, and the "wet lung syndrome". Severemetabolic acidosis with a large anion gap developed in threepatients. The onset was acute in each instance and at a timewhen ureIa and acid-base balance appeared to be well controlledwith dialysis. Twice an .w-ilerlying factor of sudden extremehypoxia was noted, but the onset appeared to be spontaneousin the third instance. Although pyruvate-lactate levels werenot measured, it was assumed that lactic acid was the majorcontributor in the absence of other causes for the acidosis.The lack of renal tubular capacity to respond to the acid loadadded to the severity of the complication. Improvement, wasachieved in one instance with sodium bicarbonate and allevia-tion of the hypoxia. In the oth-er two cases, only partialand intermittent cc~rrection was possible despite similar treat-ment plup dialysis. Digitalis toxieity manifes'Zed by parox-ysmal atrial taciiycardiat with variable atrio-vent-ricular block
1'rc'"nI 'iiu fs 11'i I V;V 9. Seplernber / 971
...... ...... .......

7.50
It itic Ritalu, I air,' mt Ii'r Ame; (o : i
INI IH IlOLIS (COMPLICATIONS
TIMI; OF ONSET
Sill' NO. OF PATI[ENTSPrcwcnt on Admi;iion Unit Acquird
Wound inlcciions 13 3? |•Pneumoniatnl. 5 23
Scplicemia 7 5Peritonitis 5 1Abscesses 4 1Urinary infectionw 2 lMeningitis 1 0
occurred on one occasion associated with hypokalemia. Alarge hemopneumothorax following thormcentesis and massivepostoperative atelectasis of one lung following laparotomyoccurred in one patient.
Infectious complications were analyzed to determinewhether these were present on admission or acquired there-after, in order to (a) evaluate the unit's contribution toinfectious complications and (b) to determine the associationbetween sepsis and the occurrence of renal failure. Infec-tions were considered nosocomial with respect to the dialysisunit if they were either not present on admission, or ifalteration in the dominant pathogen cultured from a septicsite on admission was demonstrated. The majority of woundinfections and most instances of pneumonia and peritonitiswere present at the time of admission. Although septicemia,focal abscess formation and urinary, tract infections weremore often present when the patient was received in transfer,the difference was not significant. The single case of men-ingitis had developed before the time of admission. Althoughno causal relationship between sepsis and acute renal failurecan be derived from these data, there exists a strong associ-ation between the two entities. TABLE XIII.
TABLE XIII gives a breakdown of bacteria cultured fromvarious sites on admission and thereafter. Organisms wereconsidered dialysis-unit acquired if a new dominant organism
I'resen; Concepts. Vol IV .'o 9. September 19 71
•.,'• 1
• z

*It'th IRenadl IliIhirt ti IIm r /Wa ur • -'Gnigcr
TABLE Xl11
INF•CTIOUS COMPLICATIONSCULTURE DATA
ORGANISMS*Staph. aur. Pro#. Prot. • E. conl PL A K-E M-H Alaec. Cand(coag. +) (Indoie -) (Indole .)
I. Admission
Thial I 5 7 12 27 I' 4 ... .
Wounds I 4 6 8 14 11 2 ... .
Spuitini ... I I 3 4 3 2 ... .
Ilhood .. ... ... I 6 3....[Irnc.....2 ... ... ...
S i. f id .. .... ... ... I. ... .... ...
II. Unit Acquired
"rotai I 2 2 3 4 6 4 1 1
wVou ind ... I 1 1 2 ... I ... ...
Sputu 1 I ... I I I 3 2 I ...111oi~ , .I..w . 3 ... ... ...
It fl len ... ... .. ... I .Sp. h..... •. .• . ..
Supli,. ;,ii. tSluphyhwtt'uC UUm U%
I'. 4'101 I.: u iherichia coli11%. A "'wist4 hdguonu% 'acruginomK-I% m Kk1.i-.idia.EnterobuctcrM-11 'Air',.ltcrelleaA. factc. w AkculigenO 1aWcall1('ml n (-andida
appeared, or if the site Was originally sterile or shovednormal flora. Polymi•robial inf-etion of all Mites exceptthe blood and urine Was the rile; howeverp on three occasionseven blood multures were ui3nutAmoug6ly positive for twoorganisms. The data show that all oultures-vhethr prjitive
I'rer,,il ('t1trep/s. VIo IV No 9. September 1971

I, UIR !' uhal I ailu rn t ltr,m ( ",i, r
at admission or after hospitalization in the unit- 6Tew outgram-negative orgarnisms in all but four instances. Again,regardless of origin, Pseudomonas aeruginosa, KlebsiellaEnterobacter and E. coli were the most common bacteria.Proteus was tne next most frequent isolate in both groups.Alcalienes faecalis and Mima-Herellea were never culturedas the predominant or sole organism and were of questionablesignificance. 'Staphylococcus aureus was the principal bac-terium in one instance of pneumonia and was grown from a -biliary drain on another occasion. The sole case of Candidasepticemia occurred in a patient with a polyethylene centralvenous pressure catheter - the tip of which was also foundpositive for the organism on culture.
RI S' L.FS
Of the 24 patients referred to the dialysis unit, sevensur-ived, 15 expired while in the unit, and two others diedsubsequently in PAXGM facilities following their initialdialysis therapy aboard the SANCTUARY. Of the seven survivors,six i-egained normal renal function as determined by BUN, serumcreatinine, creatinine clearance, urine concentrating anddiluting ability, and urinalysis studies. The seventh patient
vith acute glomerulorephritis attained partial return of renalfunction with a creatinine clearance of 30 cc/min at the timeof discharge, cne month post dialysis.
'When the survival figures are analyzed on the basis ofmodalitj of therapy and type of antecedent illness, the resultsshown in TABLES XIV and XV are obtained. Of seven patientswho did not receive dialysis therapy, four died. Three of theexpired patients did not require dialysis at the time of deathand one patient expired before its institution. Of the 17dialyzed patients, four survived and 13 died -11 while inthe dialysis unit and two following transfer. Four of thefive pitients in the nontrauma group survived. In the traumagroup there were three survivors out of 19 patients.
AI
I'rc~nr (*m cp 1' I l I V o 9. Se'pie'nber 19 71

At uw Renal !.'ailr re IVar Xtur - (0niger
TABLI. XIV
St'RVIVAL - MODALITY 01: THERAPY
NO. OF P.A.T1ENTS
Conservative therapySurvived 3Expired 4
Dialysis therapy 17Sur'Aved 4Expired I1Transferred, subsequently
expired 2
TABLE XV
SURVIVAL - ANTECEDENT ILLNESS
Trauma 19 Non-trauma 5Survived 3 Survived 4Expired 14 Expired ITransferred, subse-
quently expired 2
P'revett (Coicepts. "1l IV No 9. September 1971
......... ;
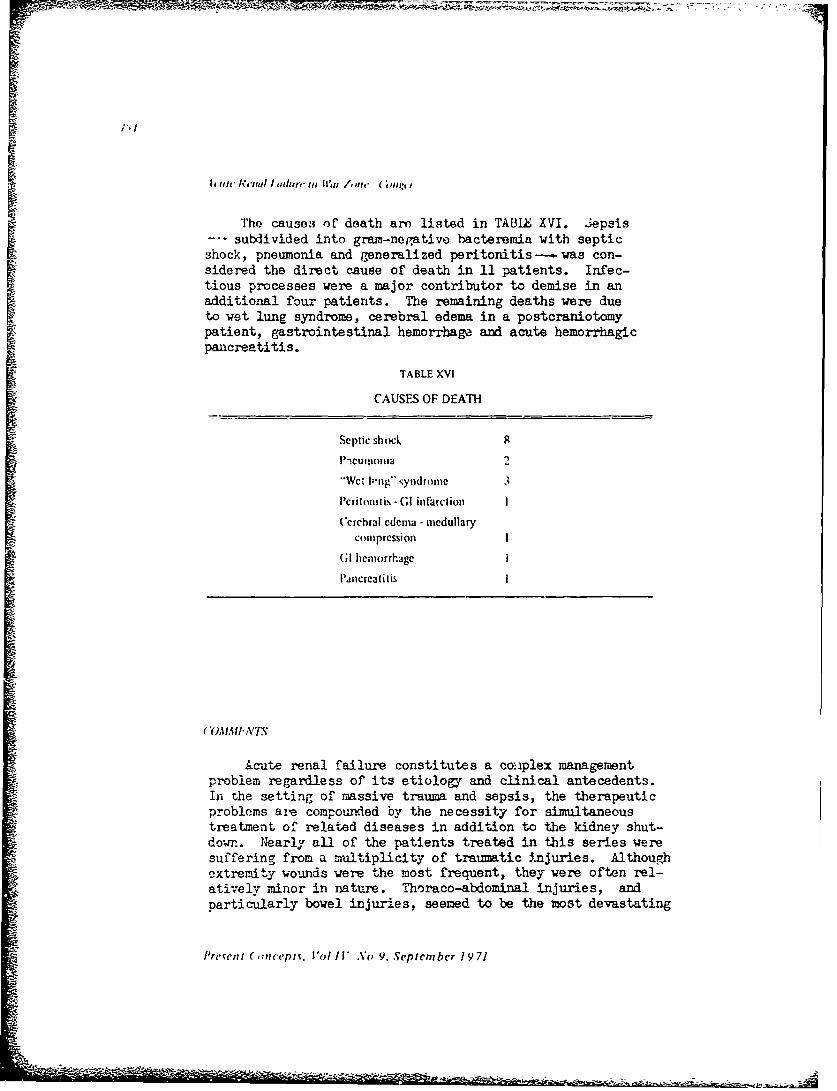
";°I
It it It 'I / atn/r" iii II'm /,)In" " tlrII I
The causes of death arm listed in TAMIZ XVI. Jepsis--- subdivided into gram-negative bacteremia with septicshock, pneumonia and generalized peritonitis-- was con-sidered the direct cause of death in 11 patients. Infec-tious processes were a major contributor to demise in anaadditional four patients. The remaining deaths were dueto wet lung syndrome, cerebral edema in a postcraniotomypatient, gastrointestinal hemorrhage and acute hemorrhagicpancreatitis.
TABLE XVI
CAUSES OF DEATH
Septic shocL 8
"1Wet I-rig'" 'vydrome 3
IPcritonitis - (;I infarclion I
Cerchrai edema - medullary
compression I
(GI hemorrhage i
I'ancrcatitis I
(OMA1" A'T.W
Acute renal failure constitutes a couplex managementproblem regardless of its etiology and clinical antecedents.In the setting of massive trauma and sepsis, the therapeuticproblems are compounded by the necessity for simultaneoustreatment of related diseases in addition to the kidney shut-down. Nearly all of the patients treated in this series weresuffering from a multiplicity of traumatic injuries. Althoughextremity wounds were the most frequent, they were often rel-atively minor in nature. Thoraco-abdominal injuries, andparticularly bowel injuries, seemed to be the most devastating
i'rcrwnt (mnc'piv. 'ol /I* No 9. September 19 71
- r

7-5
Acutie Rena.l I-thlure in War Zon• -Cukz'cr
in terms of patient mortality; They were frequently associatedwith sepsis and poor womnd healing, and necessitated prolongedparenteral feeding.
The etiologj of acute renal failure in the trauma groupDappears to involve a combination of clinical factors. Twothirds of the group had documented hypotension before the on-set of renal failure. Nearly all caees received blood trans-fusions, but without known reactions. Sepsis was an earlycomplication in these patients; however, except in those withseptic shock, it was difficult to determine the exact onsetof sepsis and its temporal relationship to the kidney shut-down. There were no instances of overt myoglobinuaria orhemoglobinuria; urinary tests for these substances wereeither negative or not significant. Contrariwise, the causalfactors in the nontrauma group were more readily explicableand intimately related to the basic disease process as anaccepted complication.
Oliguria was a manifestation of renal failure in nearly
all patients; but three had urine volumes exceeding a literper day while there was progressive rise in the BUN and serumpotassium. All cases of "high-output" renal failure /7/occurred in individuals with bilateral amputations of thelower extremities in highly catabolic states. The urine wascharacterized by low overall solute excretion and a relativelyhigh rate of free water clearance. The urine volume couldbe further increased with diuretic agents, but there waslittle effect on solute excretion.
In general, the data from the present experience wouldindicate that attempts at diuresis with either plasmh expandersor diuretics are of little value when there is good clirncaland laboratory evidence that oliguriia is due to acute tubularinju.y. Often the immediate, critical problem at the t` ,-,fadmission was overhydration, resulting from unsuccessful fluidtrials to "flush the kidney".
T•he treatment of acute renal failure, as an isolatedaspect of the total disease process, was successfu3 in thatnone of the patients expired as a direct result of a renalmetabolic comp-icatJon. This is not to say, however, thatfurther improvement J.n dialysis techniques and metabolic man-agement could not prov-ide further benefit in treating thebasic disease and its complications. Though controlled stud.ie~s
I're'win/ (sn•p•'i . 1"d ' V No 9. Sept•',n • hr I • :i

A tc Jtie AN'nt, I' 1 ',a r" ;yi War /.•,tc" (Yng -r
are lackin-, it would appear that patients tend to feel betLerand recover more often with early and frequent dialysis designedto restore approximate biochemical normalcy. The survival datafail to indicate that early dialysis significantly altered theultimate outcome, but the time from onset of renal failure todeath was possibly somewhat longer in those expiring.
A disappointing observation was that vigorous ultrafiltra-tion with several kilograms of fluid removal was not beneficialin reversing the "wet lung" process once it was established.Interstitial and alveolar edema fluid seemed to remain fixedregardless of weight loss or the addition of mannitor or albu-min to the patient's vascular volume.
Technical difficulties encountered were mainly those ofhypotension both in the early and late phases of dialysis, thefinding of adeque.te shunt sites in those with multiple extrem-ity injuries, and occasional clotting of the coil or venoustubing when attempting to keep the degree of anticoagulationat a minimum. None of these constituted an insurmountableproblem and both standard and innovative measures could beapplied to alleviate them. Whether regional heparirizalionshould have been used more frequently in the trauma patientsis uncertain. Bleeding waa not an overall significant problem;however, in one patient with multiple unsuspected duodenalulcers, who bled massively following dialysis, hemorrhage wasthe direct cause of death.
The major clinical problem and primary prognostic indi-cator was the presence of sepsis. It was extremely difficultto ýeverse the process, and once septicemia, severe pneumoni-tis, peritonitis or progressive wou4d infection developed, thereseemed to be little of therapeutic benefit available. No doubtthe frequency of virulent gram-negative organisms was a sig-nificant factor. The disc sensitivity and tube-dilution studiesperformed on initial cultures suggested that the Pseudomonas,Kiebsiella-Enterobacter, r. coli and Proteus becteria shotldhave responded to the appropriate antibiotics - includingkanamaycin, gentawycin, chloramphenicol, ampicillin and ceph-alothin -even when appropriate adjustments in dosage bothfor dialysis and decreased renal function were made. /8,9/An _dditional possibility may be that more vigorous and earlysurgical debridement, drainage and amputation should be carriedout, in view of the overall disappointing results in casespresenting infectious complications.
Prc'i',z. ( c,,• cy1 •. I ,i I IV 9. .•S i•,i cr 1 -V 1

t verail survival of Lhis group of patients was 20 percentwith all but one of the deaths occurring in the trauma group.It is evident from this experience that the prognosis forpatients with acute renal failure depends upon the severityof the underlying trauma or illness and its complications.Though the metabolic consequences of kidney shutdown could becontrolled, the mortality rate was not appreciably less thanthat noted with pre-dialysis methods of management. Tmprovedsurvival rates will have to await improved management of thebasic injuries and prevention of septic complications.
References
S. Smith iY, Jr, Post RS, Teschan PE, et a!: Post-traumaticrenal insufficiency in military casualties. (I..Manaement, us^ of artificial kidney, prognosis. SurgicalResearch Team. Army Medical Service Graduate School,4aRhington, D.C. February 1955.
2. Tsschan PE, Post RS, Smith LH Jr, et al: Post-traumaticrenal insufficiency in military casualties. I. linicalcharactr.ristics. Amer J Med 18:172-186, 1955
3. Proceedin:us of Study Group on Acute Renal lFailure. U3Army Surgical Research Unit, Brooke Army Medical Center,Fort Sam Houston, Texas. Symposium, Cctober 14-16, 1957
4. Ahelton A, Donadlo JV Jr: Post-traumatic acute renalfailure in Vietnam. A comparison with the Korean warexperience. John Hopkins 1ed J 124:95-105, 1969
5. Ashbaugh DG, Petty TL, Bigslow DB, et al: Continuouspositive-pressure b-eathing in adult respiratory distresssyndrome. J Thorac Cardiov Surg 57:31-41, 1969
6. Peterson CP, Swanson AG: Acu+e eacephalopathy occurringduring hemodialysis. Arch Intern Med 113:877-880, 196/4
7. Snreiner GE: In Renal Disease. Black DAK (ed).Philadelphia: FA Davis Company, 1967, p 310
8. XKunin GM: A guide to the use of antibiotics in patientswith renal disease. A table of recommended uoses andfactors governi.ng serum levwls. Ann Intern Med67:151-158, 1967
9. Gingell JS, Chisholm CD, Calnan JS, et al: The dose,distribution and excretion of gentamycin with special-eference to renal failure. J Infect Dis 119:396-401, 1969
're.•cnli ('mt, optv. Vol I I' No 9. Srptcmbcr 19 71

758
MM 'QWTH THESE POTENTDIURETICS, I JUST DOAN'T
~~ __ GET NO RESPECT ICý
Present Conlcepts. VolI1V No 9. September 19 71

RF(.:INT AI)VANCES IN THlE IMMUNOLOGY OF GLON'ERULONEPHRI HlS
MAJ Stcphcn R. Stcinniuller. MC
In 1827 with his description of a heterogenous group ofpatients having "albuminous urine" and renal insufficiency,Richard Bright established chronic renal disease as an entityand provided an eponym for a large group of disorders affectingthe kidneys. By 1836, Bright had collected some 100 caseswhich he presented in tabular form in the Guy's Hospital Reportscf that year. The common denominator of these findings wasalbuminuria associated with gross morphologic changes in thekidneys at postmortem. It is probable that the majority ofthese patients were suffering from chronic glomerular diseases.
Little progress was made in the delineation and under-standing of these diseases until the systematic work by Volhardand iahr in 1914 in which inflammatory processes of the glo-merulus were separated from conditions which were thought tobe either primarily vascular or degenerative in origin. Sincethen classification and understanding of glomerulonephritishas remained primarily descriptive either from a clinical ora pathological standpoint. A laclk of information concerningeither etiology or pathogenetic mechanism has made otherapproaches impossible. The outstanding contributions ofauthors such as Addis, Ellis, Jennings and Earle, Longcape,and others were concerned with the clinical ard pathologicalcorrelations of a group of diseases whose origns remained amystery. Ir. the 1950s and 1960s with the development ofcorticosteroids and antimetabolites as potential therapy, thelack of fundamental knowledge of these illnesses became morecritical.
Appreciating the deficiencies of the clinical approach,a number of workers began in the 1930s to develop experimentalmodels of human glomerulonephritis in laboratory animals.Many of the inherent limitations of human study could thus bebypassed, allowing great latitude in the manipulation ofexperimental material. Thus, beginning in earnest in 1933with the work of M. Masugi utilizing poorly understood immune
i',• ,a; t ,n w : ti. I U.I II \,, V ..'cp htc cr 19-1

mechanisms to produce clinical and pathological disease statesindistinrTuishable from human glomerulonephritis, a new concept
of the pathophysiology of glomerular injury has evolved. Al-though many details remain unclarified and etiologic factorsart still largely unknown, the progress to date has been suf-ficient to create a new basis for the classification andpossible treatment of glomerulonephritis.
I-XPEIIMENTAL MODELS
Great effort has been expended in the development andunderstanding of models of immunologic glomerular injury. Ithas become evident from such study that two mechanisms areoperative in experimental and human disease states thefirst mediated by an antibody assault formed and directedspecifically against constituents of the glomerular basementmembrane (GBM), and the second caused by circulating solubleimmune complexes (i.e. antigen-antibody complexes unrelatedto glomerular tissue) passively lodging within the glomerulusleading to injury of this innocent bystander. Application ofthese concepts of pathophysiology to human disease is impos-sible without familiarity with the animal models from whichthey have been developed.
Ncphmtmc'Ncpull,i ll"Ihc Maiszgi. Stc hlzy and Katy ulodels
tRcreir (" (. I R A el :1 led Pro, 214:191-205. 1969)
Working in 1933, Masagi was able to show the developmentof glomerulonephritis in rats injected with serum from ducksor rabbits immunized against rat kidney antigens. The char-acter and severity of the resulting disease was related to thestrength and dosage of heterologous serum used and both acuteand chronic nephritis were produced. Figure 1. In this modellarge doses of heterologous serum led to early heavy protein-uria, and subsequent development of the nephrotic syndrome,renal failure, and death weeks or months after. Smaller dosescaused lesser degrees of proteinuria with the gradual develop-ment of a chronic glomerulonephritis. In both instances,renal morphology in the initial phase consisted of swellingand proliferation of endothelial cells, basement membranethickening, and occasional fibrin thrombi. later there was
Ic,• l(,,onc/'li%. 1',,/ I' N ;,V, c, pt'l teuihrr 1 971

*(, I
h/m/'n,it ,lo~, ,.0 ,;h litcru oIt m•hritis . Sh-hinmulher
I 1g. I.Ma.sigi modcl. Kidney from rat is injectcd into rabbit to develop antikidney antibody. This is directedinoly against the rat kidney bascmcnt membrane. injection or rat with antikidney antiserum from therabbit prrdumcs nephroloxic ncphritis which is based on an immunological a-sult directed aainst theglomcrular hawnwnel membrane. The renal disease may be either acute nephrotic syndrome or chronicnephritis. depending on dose or potency of the antikidney antibodis given. (Good. Fig. 7.) Reproducedwith Iwrtrnission.
progressive thickening of glomerular basement membranes withendothelial and epithelial proliferation, lobule tion of tufts,the formation of adhesions and fibrous scars with gradualobliteration of the glomerulus.
In the Kay model (Figure 2) nephrotoxic serum was producedin the duck by injection of rabbit kidney antigens. In thiscast injection of the serum into rabbits was followed by a 6-8day period without proteinuria or morphologic change afterwhich heavy proteinuria and glomerulonephritis developed.
Analysis by several groups has established the salientfeatures of these models. The toxic effect of the hetero-logous serum lies in the presence of antibodies directed'against basement membrane antigens. Moderate donse lead toinmediate fixation of antibody on basement membrane sites ofthe target gloesruli. This is followed by a sequenoe of com-plement fixation and activation, chemotactic attraction ofpolymorphonuclear leukocytes by a C36 7 oomplex and perhapsliberation of lysozomal enzymes. Depletion of animls ofeither polymorphonuolear leukocytes or complement averts both
I'rsvi',I ('C,,tcep v, VWl I/V No 9,, Scptem her / V 71

h tllll,,[ii ,, .l ' i 'I ¢I,[',,m rtd, e, j 'un rl .\ .c nl jjllcli[tr
the early morphological changes and the immediate proteinuria.In the Kay model the fact that duck gamma globulin fixes rabbiltcomplement poorly explains the lack of immediate toxicitydespite antibody fixation. When larger doses of antibodv areadministered, leading to saturation of most of the antigenicsites, proteinuria develops even in complement and polymorpho-nuclear leukocyte depleted animals. The reason for this isunkno-im.
Dixon's group have &!so shown that following this initialperiod of injury there occurs an autologous phase with thedevelopment of host antibodies directed against the heterologousantibody fixed within the glomeruli. Fixation of these newlyformed antibodies to GBM-bound heterologous antibody resultsin sustained nephritis and explains the delayed appearance ofdisease in the Kay -odel. Elimination of this host responseby x-radiation jr neonatal induction of tolerance to foreigngamma globulin prevents this autologous phase, permittinggradual healing of the initial phase glomerular lesions.
-i•
:XCK A-4.16J13e 14
fl", .• N5 ApTS'.p
Ka'. viudei ,Anti~xod'a. : nal,, iahhil glomcrular membranes is formed :m th,: duck Small doc..age" (,I(1ý. ' .|in:ribhil kidncý %.crum ,nlck led into rabbit Rabbit complemcn, is. poorl\ f,\cd h\ duck arntfb,,d(!
! h rah~tfor|• nt~od, agm,. duk gmmaglobulin tonic of which i, fix,:d to it, glnmeruhar memblrane -"N d]illctn', Imm l J t hi O lck, led immunological arsault may cn~ue %,hete for one reaton or another foreign.,rnlg, n iv..iitla icd to ho,,| glorrirular membrane -.;hen antibod.% apwan~t that ant.zgcni b(orno•.aala~
. • ~~,(--,,d I I" I P Reptrductd ".th Memitqon
I'r •,• (',t;, l,1. Il l" ,,9. Septern er 19 71

Iinnuu,,/,•,'i' ,fi (h, 'tncrulru(')p/rili. - Se•'i,,nuiIlhr
Although the intensive study of the Masagi and Kay modelshas permitted significant insights into the mechanisms ofrenal injury caused by anti-GEM antibodies, it was not untilSteblay's demonstration of the induction c f autologous anti-Galdisease in sheep in 1962 that applicability of these models toforms of human glomerulonephritis became established. TheSteblay model (Figure 3) consisted of the injection of hetero-logous glomerular basement membranes isolated from otherspecies, combined with Freund's complete adjuvant, into sheep.Animals thus treated invariably developed a fulminant glomer-ulonephritis terminating in death within ieeks to montho. Thepathology in these cases was remarkably similar to human rapidlyprogressive glomerulonephritie, showing prominent epithelialcell proliferation with fibro epithelial crescents formationand glomerular obliteration. The disease was transferable tohealthy animals by either cross-circulation or the injectionof serum from nephrectomized diseased animals. In the lattercase Dixon's group has shown a sharp rise in the level of cir-culating autologous anti-GBM antibodies once their site ofremoval (the kidney) is eliminated. These investigators haverecently denonstrated similar rises 4- antibody titers in thesera of certain nephrectomized patients awaiting transplantation.
WD.IY x. I , -
SI.CEP ~80 AP4?ODS0J
NF4'hlJv 1I11,,[J¢I. Ii•otl.d h,,,.rmcnt flllcnlrdn•.c% froinm prillait (or hum1nlan N (•~V ,me,. ii 'cted int the %}i'cp.I .hc, p . m. ,kci antihokdy ap.,in, IIIhC, for•.in ITIClIehlanrc. , hich c'oiwra.:tl v. tlb antlgen, fit. the "heep', own,gJornerular irembranc. Thus. a direcled Imnunohlogcal assault occuri apanst the shecp'ý gllmerular membrane,
"ai aiujt, intib~d, rormed In the %heep. The die=w r•'ndrnrd li a !.13 rrnrcieih'e nephrb I;to. FI-i. R)Htcprodc• cd with permtOion,

764
Immunology of Glomendonephritis - Steinpnuller
The demonstration that the immunization of sheep to hetero-logous glomerular basement membrane antigen causes the formation ofantibodies having cross-reactivity to autologous antigens ledseveral workers to investigate the possibility of immunizinganimals to homologous and autologous glomerular antigens.These efforts were surprisingly successful in a number ofhosts, which led to the production of true autoimmune anti-GBMnephritis.
Analysis of the histopathology of all these models ofnephrotoxic nephritis by immunoflourescent techniques revealsintense staining for IgG and BIC in a linear, ribbon-likepattern along the glomerular basement membranes (Figure 4).By extensive investigation the specificity of the histochemicaltechniques used and tho pathogenic significance of the lineardeposition of immiunoglobulins have been well-established.This pattern may now be considered the hallmark of directimmunologic assault on the glomerulus.
°.
' t
Fig. 4. Flut.;cscent photomnicrograph of a diseased glomerulus stained with flurescene-labeled anti-globulin to IgG. Note the ribbon-like pattern corresponding to the deposition of immunoglobuhnin the Masugi, Kay. and Steblay models.
Present Concepts, Vol I"I' No 9. Septembcr 1971
L.

SI'' , ,i r,, I G'e ,,q(;:cPtonene loneIIhratt Simtiaanulr
Iitiiiu ' ('on11111 I)r111t, ii,, "fh ti ine D Tih ''.. I lev'.ui- an:ud o I hei u1 dot ,ik
Scium Si" Model tlic luute anid chroni)
The injection of foreign proteins into animals or man hasbeen repeatedly shown to result in the typical syndrome ofseunm sickness, manifested by fever, arthralgia, arteritisand glomerulonephritis. The pathogenesis of the syndrome hasbeen clearly delineated by several investigators. Figure 5.The injected antigen elicits an antibody response after avariable period, usually within 14 days. As increasitg amountsof antibody are produced, complexing of antibody with antigenoccurs within the circulation. Complexes formed early in thecourse under states of antigen excess tend to be soluble sincethe amounts of antibody available are too small to form macro-molecular precipitating aggregates. These circulating solublecomplexes are biologically active in fixing and activating thecomplement system and other mediators of increased vascularpermeability. These changes appear necessary for the subse-quont deposition of the complexes within glomerular capillaryloops and vessel walls. Finally, complement activation in situ
IOUO .10
~ 0,3 so
""- 1 EI- ,
2n 0
\: .._* 60--"-- ,~'ll *2., l
200i':.
0.1 . ,
2 4 S 10 12 14 16 16 20
Days iler inlectlons of IMSA
i ic 5 Cla sic picture of 'scrum sacknes as rccalcd hy immunochemical analyses of Dixon and c(orkcrs.Note that the .rtentis and glomcrulonephritit begin Ahilc soluble antigen-antibody :omplc.es arc preteniin the circulation just prior to the ontct of immune elmainaton. BSA-bovmc scrum albumin. (Good, I ig. I..as taken from Diton I J Arch Pcrh o0 20. 1958. rig 2 i Reproduced sith permission
Pre.zent Concepts. 'o! I* No 9. September 1971
... .e ....

/hllwltmoht.t v J 7 f Plittruh mepll hrilt% Mcmhnlnm chr
by deposited immune aggregates initiates the injurious inflam-matory response (vide infra). Thus, the appearance of glomer-ular and arterial lesions closely parallels the developmentof the antibody response and the subsequent disappearance ofcirculating antigen, as complexes are deposited within bloodvessels or are cleared by the reticulo-endothelial system.Free antibody first becomes detectable in the circulation atthe time of disappearance of antigen, reaching a peak levelthree days later. Small amounts of antibody are subsequentlyproduced and the serum level falls as normal immunoglobulincatabolism takes place. The resulting glomerulonephritis isshort-lived, corresponding to the period during and shortlyafter antigen removal. Pathologically there is a marked pro-liferation of endothelial cells with encroachment on capillarylumina and diff'ase swelling of the glomerulus. Polymorpho-nuclear leukocyte accumulation is seen at the sites of tissueinjury. By immunoflourescent techniques (Figure 6) antigen,antibody, and BIC globulin (C3 - the third component ofcomplement) are seen deposited in a granular, lumpy-bumpyfashion along the basement membrane. Early in the course,electron microscopy reveals occasional deposits along theendothelial side of the basement membrane while later studyshows large electron dense "humps" along the epithelialsurface. These are believed to represent large macromolecularaggregates of antigen amtibody complexes. Proteinuria is aprominent result of the tissue injury but rapidly clears withmorphologic healing following disappearance of circulatingcomplexes. Proof of the central role of these protein aggre-gates in the pathogenesis of the disease is given by theprompt development of identical lesions in animals injectedwith soluble immune complexes created in vitro.
With more complete understanding of acute serum sicknessin the 1950s, efforts to produce chronic disease states byprolonging the phase of antigen excess were initiated. Dixonand co-workers and later Germuth and associates were able toproduce chronic glomerulonephritis in rabbits through repeatedinjections of foreign antigen over periods of weeks to months.In such experiments, animals could be divided into three groupsdepending upon the degree of their antibody response. Animalsdeveloping extremely high titers of anLtbody were able to main-tain states of antibody excess within the circulation despiteincreasing doses of antigen. Under these circumstances pre-cipitating insoluble complexes were formed and were rapidlycleared by the reticulo-endothelial system. Glomerulonephritis,
Prc•cnt Concepts Vo; I/V o 9. September '9 -1

* ' I
767
Immunology of Glomerulonephritis - Steimnullcr
Fig. 6. Fluorescent phctomicrograph from animal with acute serum sickness. Note the lump)y-bumpy pattern of flurescnce from IgG + BI C which is characteristic of acute serum sickness-typeglomerulonephntis.
occurring after the initial exposure to antigen, quicklycleared and chronic disease did not develop. Anaphylaxiswas a common sequel of antigen injection. A second group ofanimals failed to produce any antibody and did not show renalinjury. Animals producing average or low levels of antibody,however, developed progressive glomeralonephritis. In thisgroup states of antigen excess could be obtained repeatedlywith antigen injection and soluble immune complexes werepresent for prolonged periods. The renal disease was mani-fested by hematuria, prolL-nuria, azotemia and frequentlydeath. The nephrotic syndrome was a common feature. Theearliest morphologic change was pronounced diffuse thickeningof basement membranes, followed by proliferation of endo-thelial and epithelial cells, lobula'.Aon and scarring ofcapillary tufts, with subsequent obliteration by collagenosistissue. By immunofluorescent techniques bntigen, antibody,and BIC were deposited together in the same granular, lumpyfashion as in acute serum sickness. 'xtent of deposition wasrelated only to the degree of basemeat membrane change, andin no case could either antigen or antibody be demonstratedalone, without the other. By electron microscopy dense sub-epithelial deposits were noted within the basement membranewith sheets of epithelial cell cytoplasm over them. The sizeand distribution of these dense "humps" corresponded cleselyto the deposits seen by immunofluorescenc,.
Present Concepts. Vol IV N.o 9. Sptcpmler 1971
-* .-

Inu7," unn, rJ (hm.nd, phIsJ-hrI1l.. S- l nuller
To determine reversibility of disease once established,Dixon's group followed a number of rabbits with mild to severeproteinuria and morphologic change at biopsy for a variableperiod after cessation of antigen injections. In those animalswith the most pronounoed histologic change and heaviest pro-teinuria, scarring and destruction proceeded relentlessly torenal failure. When only mild proteinuria was present inassociation with early morphologic change, proteinuria de-creased or disappeared after cessation of antigen injection.At sacrifice or death little morphologic improvement could beseen even in animals with clinical evidence of healing. Immuno-fluorescent staining for antigen and BlC was progressively lessintense, however, and breaking up of the subepithelial densedeposits could be seen by electron microscopy. Thus, thesestudies demonstrated a "point of no return" beyond which heal-ing could not occur, and showed that histologic healing whenit. occurred lagged far be'.Jind clinical and immuno-histochemicalchanges.
r'hc Hlcman Model
In 1959 Heyman and co-workers reported the results of aseries of experiments involving the production of the nephroticsyndrome in rats by the intraperitoneal injection of rat kidneyextracts and Freund's adjuvants. The severity of the diseaseappeared to be related to the dose injected. When extracts ofliver, muscle and lung were used with adjuvant disease wasseldom produced. Additionally, Freund's adjuvant alone or ratkidney suspension alone were ineffective. The disease, oncestarted, continued despite cessation cf the injections; andat autopsy moderate to severe membranous glomerulonephritiswith focal interstitial plasma cell and lymphocyte infiltrationwere seen.
Although this model was initially thought to be analagousto the Steblay model, subsequent investigadion revealed thatIgG and BjC were deposited in the glomeruli of affected animmlsin a granular, lumpy-bumpy fashion in contrast to the linearpattern cf anti-GBM nephritis. Figure 7. Electron dense sub-erithelial deposits like those of chronic serum sickness, werenuted corresponding presumably to agg -gates of antigen-antibodycomplexes. Figure 8. The final isolation of the specific renaltubular antigen involved allowed the characterization of thepathophysiology of ties model. Injection of complete Freund's
I'rcvc,,i ( ,nt ,'/,'s. � ' i .\ n V S' pici'.l'cr ." -

- - t -, _ •-r.- 2. .--
769
flh?,?l'102" of Glom'nenhIphritia •Steninudler
adjuvant combined with a purified high density lipoproteinobtained from the brush borders of proximal tubular cells wasshown to lead to production of auto antibodies which thenreacted with both the injected antigen and the minute quan-tities of autologous renal tubular antigen. As in the serumsickness models, complexes vere deposited with complement inthe glomeruli of the affected animals, leading to proteinuriaand nephritis. The disease was self-perpetuating because ofthe normally occurring continuous liberation of renal tubularantigen into the animal's circulation. The elimination ofthe normal state of tolerance to this autologous circulatingantigen by immunization thus produced a progressive glomerulo-nephritis through passive accumulation of antigen-antibody-aggregates vithin the glomerulus. The applicability of thismodel to human and animal autoiLmmune states is obvious.
,4 2q %
,." ,.)
01 ILtR MODiLSPer, z~tcnt 1)mpho•};i~ I1¢ ,:,, n z in�,vir- t rfection in mice
Ilq 7 I-lu.-cent photomicrocraph oi the kidney in the Hieyman modcl The granular pattern ofl, auin !( depo ition ,korrespai. t -, subep;z'.eht . ni znurc complex deoiits.
I ,c. S ri.:h, Poition of giomuiar *uit. I ritec ! diInuwc irregulatity in the sub jith* imal aspcct of the.gltruLar bq,::cn e inc brant' wkit;; m.n' dcn.c dL'-',owit, prcen;. Intervening projection, of the laminaden' r, a s.en. uh., h art notcd a; tin,- . to ý=ror:n' tihe dcpo,;I, (nr-rro on the lefti. In one focus (arrowor ti. • riht lear arca. atr noted in the baement mcn -rz,,C T l: . sn. Fir.. 5.) Reproduced with pcermis-sior. from pubhhc:. W\.B. saundcr ( o.. and ..ul":. 1'hotogra.n rcdi.ced from fiurc wh:-h shouedrna.cifi:a:kon'\ "1OO '
3ertain mouse strains injected shortly after birth withlymphocytic choriomeningitis virus (Lai) carry the virusthroughout l3 fe making low levels of anti-LU4 antibody. Dif-ferent strains vai:f in the amount of virus present, and in
SFrcsc,: (., cct;.. l I'.,11 \ S: ' c • ' "i't" • 19-
77o
hnintttmilwh,gr e, (,,ineflTh~inl('phrius - Si'nnulnlt'r
the time and extent of their antibody response. Mice havingleast amounts of virus and antibody do not develop nephritiswhile those with the highest levels show the early developmentof chronic disease. Within the glomeruli, antibody, complementand virus particles can be shown deposited together in theclassic granular, lumpy-bumpy pattern. Gamea globulin elutedfrom these kidneys readily binds LC2 virus, and circulatingIgG-virus complexes can be detected in the serum of diseasedanimals. These findings would seem to establish the processas an immune complex mediatsd naphritis.
Auto iminune di~ica of \c% Ze..bnd niicc
Gertain strains of New Zealand mice have been found todevelop an auto immune illness comparable to human systemiclupus erythematosus. The disease appears earlier and is moresevere in females, and is characterized by hemolytic anemia,glomerulonephritis and antinucleic acid antibodies. Thenephritis appears in large measure related to deposition ofDNA complexes and anti-DNA antibodies. The importance oflatent infection with murine leukemia virus in contributingto the development of disease is currently being investigated.The finding of virus like particles within cells from patientswith SLE make this model attractive for further understandingof its human counterpart.
Addilionj' Aspect.is of Imnmunolhnidl Iiit, r%
Role ofanlibod) chtrat iciilcs. complcx mi,.. complement. the coagultion proce• and mediators ofincreascd %ai, ular p crf lht•
Deposition of immune complexes with resulting diseaseappears to occur only in special circumstances. Complex sol-ubility is important and relates to antibody characteristicsand circumstances of formation. In the case of precipitatingantibodies, complex solubility occurs only when formationtakes plece with antigen in slight excess, leaving antigenicsites unsaturated. In certain circumstances, however, nonprecipitating antibodies are formed, making the relative con-centrations of antigen and antibody unimportant. In this casesize also appears less important. Under most conditions com-plexes of less than 19S in weight do not localize in bloodvessels and glomeruli; however, in the case of non-precipitating
Prc.,wnt (t',,u cpti. I ,I1 .\ I ' .Ao cptcmbleCr I 1j -1
-1 ---i-i -'il I my ---,,-,.. . .. . .
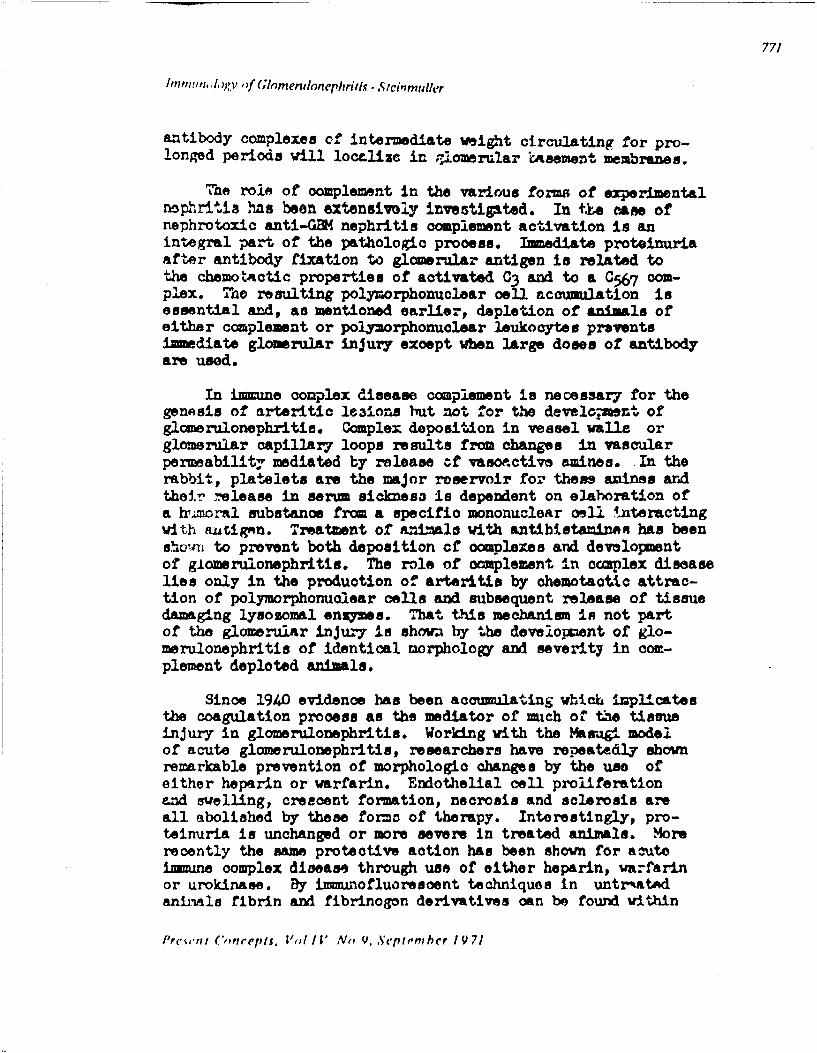
771
In1un, ;,ogv ,f ( G;imerulonephrit.s - Sicinmuller
antibody complexes of intermediate weight circdating for pro-longed periods will locelize in ,,Iomerular rasement membranes.
""ne role of complement in the various forms of experimentalnophritis has been extensivoly investigated. In t.•e case ofnephrotoxic anti-GBM nephritis complement activation is anintegral part of the pathologic process. I.mediate proteinuriaafter antibody fixation to glomerular antigen is related tothe chemotsactic properties of activated C3 and to a C56 7 cm-plex. The resulting polymorphonuclear cell accumulation isessential and, as mentioned earlier, depletion of animals ofeither complement or polymorphonuolear leukocytes preventsimmediate glomerular injury except when large doses of antibodyare used.
In immune complex disease complement is necessary for thegenesis of arteritic le31ons but not for the develo-iment ofglomerulonephritie. Complex deposition in vessel walls orglomerular capillary loops results from changes in vascularpermeability mediated by release of vasoe.ctive amines. In therabbit, platelets are the major reservoir for these anines andtheir .elease in serum sickness is dependent on elaboration ofa rmoral substance from a specific mononuclear omll 4-teractingwith .utigmn. Treatment of anials with antibistaminoR has beenshiv-1 to prevent both deposition cf complexes and developmentof g±omerulonephritis. The role of complement in ocaplex diseaselies only in the production of arteritis by ohemotaotic attrac-tion of polymorphonuclear cells and subsequent release of tissuedamaging lysozomal enzymes. Ihat t-his mechanism in not partof the glomerular injury is shown by the develouxzent of glo-merulonephritis of identical morphology and severity in com-plement deploted animals.
Since 1940 evidence has been accumulating whiAc implicatesthe coagulation process as the mediator of much of the tissueinjury in glomerulonephritis. Working with the Margil modelof acute glomerulonephritis, researchers have repeatedly shownremarkable prevention of morphologic changes by the use ofeither heparin or warfarin. Endothelial cell proliferationand swelling, crescent formation, necrosis and sclerosis areall abolished by these forma of therapy. Interestingly, pro-teinuria is unchanged or more severe in treated animals. Morerecently the same protective action has been shown for acuteimmune complex disease through use of either heparin, warfarinor urokinase. By imiunofluorescent techniques in untr'atedaninAls fibrin and fibrinogon derivatives can be found within
Preswt '.,ncepts. V,,/ IV N, V.,Septemnher 19 71

772
Imnfunolo, ofl Gomenibmnephrtis - Steinmuller
endothelial and mesangial cells as wall as within the urinaryspace. More severe cases deironstrate creacent formation.The distribution of this matcrial differa from That of IgGwhich is deposited only along baes•snt rembranes. Treatmentabolishes only the staining for fibrinogen derivatives andnot igG. Similar staining and morphologic changes can becaused by nonimume mechanisms, i.e. induced intravascularcoagulation. In all caser studied with electron microscopy,fully polymerized fibrin can occasionally be demonstratedeither within the capillary space or in endothelial cells.More commonly, various forms of incompletely polymerizedfibrin (fibrinoid) are seen along the basement membranes andwithin mesangial and endothelial cells. The toxicity of thesesubstances is presumed to be related to both inefficient break-down by phagocytizing cells and interference with the vascularsupply. As mentioned before, the more severe casee show suchmaterial within the urinary space in association with fulminantcrescent formation. The fact that several different forms ofanticoagulation are successful in aborting these pathologicchanges suggests that their protective action is mediatedthrough inhibitions of the coagulation system not by someother mechanism, e.g. anticomplementary eff6ct or antiinflam-matory effect. All this information speaks for the coagulationprocess as the primary cause of the proliferative and sclerosinglesions of most forms of glomerulonephritis. Although protein-uria is not prevented by anticoagulant treatment in Masaginephritis it is eliminated in induced intravascular coagulationnephritis and in Iine complex disease in mice. These obser-vations suggest possible differences in the causes of protein-uria between anti-GSK disease and immune complex '-isease.
Unfortunately the proximate events leading to coagulationwithin nephritic glomeruli are unknown. Ag-Ab complexes havebeen shown to accelerate the coagulation process in vitro,probably through an effect on platelets. Yet actual initiationof the coagulation process has yet to be demonstrated for eitherimmune complexes or for tissue bound antibody. More investi-gation is needed in this important area.
APPLICATIONS OF EXPERIMENTAL NEPHRITIS TO HUMAN DISEASE
Techniques developed in the understanding of experimentalmodels have proven extremely valuable in the study of human
Presen i C,,ccpis. Voi IV No 9. Septem hi r 19 71

P Mr- -
773
Immunology of Glomerulonephritis - Steinmuller
glxserulonephrLitis. The iimunofluoresoent examination ofrenal biopsy specimens and the use of methods for the elutionof antibody have allowed identification of most forms of glo-merulonephritis as either anti-GB4 disease or imune complexdisease. Although the basic causes of the alterations inJirmmity remain unknown, certain aspects of human glomerularinjury are now clear.
Anti-GBM Diseasc
Goodpasture's synrome and rapidly progressive glomerulo-nephritis (RPGN), two uncommon forms of nephritis, haverepeatedly been shown to be associated with deposition ofantigloerular basement membrane antibodies in a linear fashionwith complement. The finding of fibrin and fibrin degradationproducts within the glomerular capillarlee and cells is pre-sumed to be the cause of the marked cellular proliferationleading to a rapidly fatal clinical course. Figure 9. Thatantibodies eluted from diseased kidneys produce fulminantMasagi type nephritis when injected into primates establishestheir pathogeniciy. When patients with these diseases arenephrectomizwd prior to transplantation these antibodies risein titer in the circulation. Subsequent placement of healthyrenal tissue in these patients with high antibody titers hasbeen shown to result in the disappearance of circulating anti-body concomitant with the development of disease in the trans-planted kidney. At biopsy or postmortem IgG is again seendeposited in linear fashion along the basement membranesassociated with the expecTed histology. In view of thesefacts it has now becone accepted practice to wait for thegradual disappearance of circulating antibody over periodsof months before considering transplantation.
Some differences in the specificity of auto antibodiesfrom these two diseases have been described. Thus IgG fromkidneys of patients with Goodpasture's syndrome appear tohave greater reactivity with other renal and non-renal antigensas well as with glomrular antigens from other species. Incontrast, antibody from RPGN kidneys shows little reactivitywith renal tubular antigens and alveolar basement membraneantigens, and is far more species specific. These findingshelp explain the differences in pulmonary involvement despiteidentical renal histology and course.
Present Concepts. Vol IV No 9. September 1971
i7i•| i i l t i • .- ~- -- ,-".~- -. -. - ,~ _ _ _ _ _ _ _ _ _ _ _ _ _
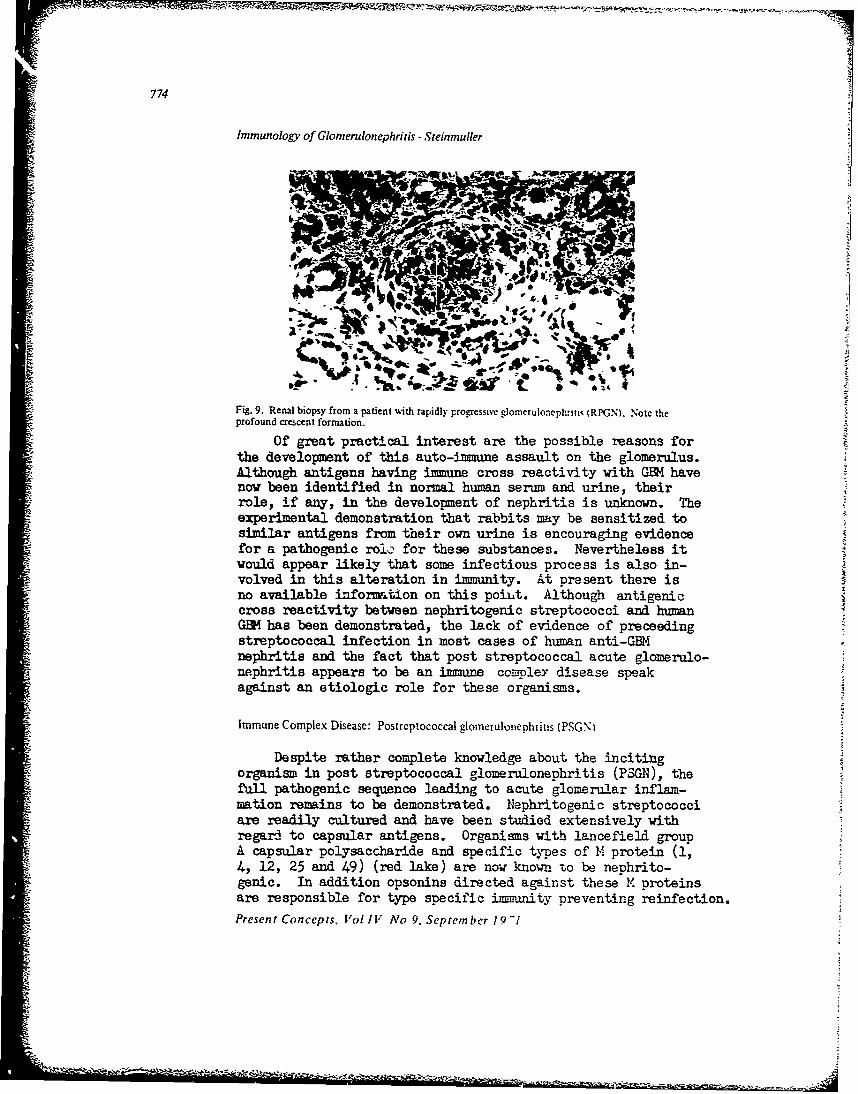
774
Immunology of Glomerulonephritis -Steinmuller
Fig. 9. Renal biopsy from a patient with rapidly progressive glomerulonephrmi (RPGN). Notc the
profound crescent formation.
Of great practical interest are the possible reasons forthe development of this auto-immune assault on the glomerulus.Although antigens having immune cross reactivity with GEM havenow been identified in normal human serum and urine, theirrole, if any, in the development of nephritis is unknown. Theexperimental demonstration that rabbits may be sensitized tosimilar antigens from their own urine is encouraging evidencefor a pathogenic roic' for these substances. Nevertheless itwould appear likely that some infectious process is also in-volved in this alteration in immunity. At present there isno available information on this poibt. Although antigeniccross reactivity between nephritogenic streptococci and humanGEM has been demonstrated, the lack of evidence of preceedingstreptococcal infection in most cases of human anti-GEMnephritis and the fact that post streptococcal acute glomerulo-nephritis appears to be an immune compley disease speakagainst an etiologic role for these organisms.
Immune Complex Disease: Postreptococcal glomeruloneph i itis (PSGN i
Despite rather complete knowledge about the incitingorganism in post streptococcal glomerulonephritis (PSGN), thefull pathogenic sequence leading to acute glomerular inflam-mation remains to be demonstrated. Nephritogenic streptococciare readily cultured and have been studied extensively withregard to capsular antigens. Organisms with lancefield groupA capsular polysac-charide and specific types of M protein (1,4, 12, 25 and 49) (red lake) are now known To be nephrito-genic. In addition opsonins directed against these M proteinsare responsible for type specific immunity preventing reinfection.Present Concepts. Vol IV No 9. September 1 9
42 ~ - ~ ~ -'

77.5
lm tl,~O ,rf (;l/u,,cr*,lb ,.iphri;i,•. - t.Jm~t~
The sequenco of inffection, followed by a latent period
and nephritis associated with rising titers of antibodies tovarious streptococcal antigens and a fall in serum complement,strongly suggests an immnoiogic basis for the illness. Effortsto document this impression have met with varied success.Lange et. al. in 1966 reported that all cases show the presenoeof IgG and BIC in a granular distribution along the glomerularbasement membrane. The majority of investigators have foundthese proteins in most but not all cases, again in a granular,lumpy distribution. By electron •icroescopy dense deposits arefound along the subepithol.al surf1ace of the basement membranein all cases which by feriItin conjugated antibody techniquesare composed of IgG plus BIC presumably linked to an unknownantigen. Additionally, donse deposits have been reported inthe subendothelial area, betueon endothelial cells and withinthe capillary lumen. These deposits appear to contain IgGand B)C while fibrinogen derivatives are also suggested.
Efforts to complete this pathogenetic puzzle by demon-strating streptococcal antigen within glomeruli have untilrecently been rather unsuccessful. Michael et. al. were ableto show such proteins in only two of ten patients, while Segaland co-workers reported finding streptococcal antigen in Sixof ten cases. Recently, Tresar and associates have shown byvery elegant study such antigen in all oases of this disease.
The antigen is a lipoprotein of 120,000 molecular weight con-tained in the plasma membrane of nephritogenic streptoooccibut not in other bacteria. Within the first few days of onsetof disease antigen is distributed in the glomerulus in thesame fashion as IgG and Rj C. later, plasma membrane specific'antibody appears in the circilation and presumably saturatesall free-bind~ing sites on the deposited antigen which there-after cannot be staine~d Wy immunofluorw,'joent techniques. Thisfact might explain earlier Cailures to demonstrate the antigen inlate biopsies. If this wortk can be reproduced by other invest-igators the initial Jmpieasion of Schiock in 1908 that PSONrepresents serum sickness will be largely confirmed. Never-theless, the reasons why some people develop the disease Whileothers infected with nephritogenic streptocooci do not, rm•insto be elucidated. Extrapolating from experimental models, onewould expect that affeoted individuals would be good antibodyproducers against this lipoprotein antigen, while those witAsubclinical or no diseaso would have low or absent titers ofantibody.
Pre.-11t (',1Irept.l. I I I' N .o 1 /. % ,pr ,I, b 'r ,' •V i/

776
Immunology of Glonicruiloephritis - Steinmuller
Another line of investigation which may yield additionalunderstanding of FSGN as well as some other forms of glomerulo-nephritis is the study of cryoglobulins. these interestingmacro-molecules have been found in a high percentage of patientswith PSGN when specifically looked for with sensitiw techniques.Most contain IgG plus BIC while IgM is also occasionally a partof the complex. These proteins can be shown to be biologicallyactive in fixing complement and in causing glomerulonephritiswhen injected into animals. Nevertheless, the role in humandisease at present remains unclear.
Membranous Glomerulonephritis
This common cause of the nephrotic syndrome in adulthoodis characterized by the isolated finding of progressive, dif-fuse thickening of all glomerular basement membranes. Figure 10.The course is prolonged and variable with ultimate remissionor death in uremia being equally common. At present there arefew clues to the etiology. Immiunofluorescent study repeatedlydemonstrates granular deposition of IgG plus BIC along thethickened membranes, corresponding to electron dense subepi-thelial deposits (as in the Heyman model, Figure 8). Thattha disease is immune complex mediated is reasonably certain;however, the antigen involved, the reasons for the lack ofcellular proliferation despite ongoing complex deposition, andthe mechanism of remission are unknown. Since experimentallyit is the clotting system which appears to initiate cellularprolIferation, it may be that some characteristic of the com-ple•.es is different from that in other forms of iruune complexdisease or that the slow deposition and low levels of complexesare inadequate to trigger this mechanism. The protractedcourse over several years would suggest that the antigen in-volved is an endogenous, autologous one circulating in lowconcentration to which normal tolerance has been lost rs inthe Heyuan model. However, remission under UIhem circumstancesis hard to understand. The recent 'Indin- of low levels ofcirculating cryoglobulins in most cases of membranous nephro-pathy may prove to be of great importance,.
Present) C,,neepis. Vol I V No 9. Seprt-m her 19 71

777
Immunology of Glomnerulonephritis - Steinmulleu
Fig. 10. Membranolb glomeruloni.phritis shoming severe thickening of all basement membranes.
Systemic Lupus Erythematosus Nephritis (SLE)
SIE represents one of the most intensively studied of theimmune mediated diseases of humans. The repeated demonstrationof antibodies to DNA, nucleoprotein, and other nuclear andcytoplasmic antigens in symptomatic patients has led to thecoaviction that these antibodies play a causative role in theperipheral manifestations of the disease. The recognition ofrenal disease as a major cause of morbidity and ultimate deathin these patients has led to the widespread application ofpercutaneous renal biopsy for diagnostic and experimentalevaluation of all stages of the illness. The growing body of-evidence supports the conclusion that lupus nephritis is animune complex disease expressing itself in at least threemorphologic patterns with gener11y differing clinical severityand prognosis. The reasons for these differences are completelyunknown but are probably related to differences in antibody,antigen, the quantity of circulating imnune complexes, or inthe presence and quantity of cryoglobulins.
The experimental obseivations implicating immune mechanismsin the development of lupus nephritis are many. Extensivestudy has shown anti-DNA antibodies to be specific for activelupus erythematosus. They are identified in the sera of mostpatients with active nephritis in varying titer generallycorresponding to the severity of clinical manifestations.,
Present Concepts. Vol I X No' 9. Sep onmb er 19 71

-r tm¶,,h "r oJ G ,,me.r.t ,mt- n'it, St . n' dlChr
That these antibodies are pathogenic has been suggested bytheir elution from affected renal tissue it, much higher titerthan in the corresponding serum. Furthermore, DNA antigencan be demonstrated in sera and glomeruli after antibodyelution. Besides anti-DNA antibody and D•A antigen, anti-bodies against nucleoprotein and phosphate buffer-extractiblenuclear antigens have also been found within affected glo-meruli. Other antigen antibody systems may play an even moreimportant role in the production of renal lesions. Forinstance, all patients having anti-risosomal antibodies appearto manifest clinical renal disease. In addition, mixed cryo-globulins composed of IgG, IgM and perhaps other constituentsare commonly seen in low titer in the sera of lupus patientsand in some cases have been demonstrated as deposits withinglomerular lesions. Finally, during periods of active renaldisease, serum complement levels fall as in serum sicknessand PSGN, suggesting the presence of biologically activecirculating immune complexes.
By immuno-histochemical techniques and electron micros-copy, complex deposition appears to have three distinctpatterns corresponding to the different light microscopicmorphologies. Cases with pure membranous changes have depo-sition of IgG, BIC in a finely granular pattern along thebasement membranes. The only distinguishing feature from"idiopathic" membranous nephropathy lies in the slightlygreater prominence of the mesangium in lupus. As expected,electron microscopy demonstrates subepithelial electron densedeposits corresponding to immune complex aggregates. Further-more, the course and prognosis of this lesion generally paral-lels that of its ideopathic counterpart. In contrast to thispattern are the diffuse proliferative lesions usually leadingto progressive deterioration and renal death. In these casesfibrinoid necrosis, wire loops, endothelial and mesangialcell swelling and proliferation are prominent features.Neutrophil infiltration and nuclear fragmentation appear in
the more severely affected areas. Imrniofluorescent studiesshow localization of IgG and BIC in coarse lumps along thebaseme 7t membrane and in mesangial cells. Fibrinogen deriv-atives can be seen in the same pattern. By electron micros-copy large dense deposits are located subendothelially, oftenpartially or completely phagocytized by endothelial andmesangial cells. Figure 1i. Other deposits can be foundwithin the capillary lumens either free or within polymorpho-nuclear cells. Occasional deposits are also seen lying within
I'r~ tt ( lC',,i cpit• 1 ul II \, 9•. 'N'j,!c":"cr 1 -1

779
imnmnunology of Ghotnendonephritis - .%'te,;nfuller
Fig. 11. Electron micrograph of a glomerular capiliar) loop from a patient with diffuse lupus nepti:sis.
EN = endothelial cell nucleus. CL = capillary lumen. EP = epithehal cell with foot processes lying onbasement membrane. Note the dense deposit marked by asterisk as well as the deposits shown by arrowscovered by endothelial cell cytoplasm.
the basement membrane or on the subepithelial side. Thisdistribution of immiunoglobulins, complement, and fibrin hasbeen described occasionally in severe cases of PSGN as wellas in idiopathic membranoproliferative glomerulonephritis.The mechanism behind this mesangial and subendothelial depo-sition in contrast to the membranous pattern is not understoodbut may relate to the compition, size, or quantity of thesemacro-molecules in the circulation. Experimental evidence inanimals and the presence of fibrin and fibrinogen derivativesin human lesions implicate the coagulation system as causingat least part of the observed tissue injury. It can easilybe imagined that subendothelial deposits in contact with thecirculation would be more biologically active than subepi-thelial ones. Nevertheless, proof of the pathogenicity ofthese deposits thus far is incomplete, and the exact detailslinking these immune complexes to the subsequent nephritisare unknown.
The third pattern of SIE renal involvement is focal andlocal proliferation with occasional necrosis of glomerulartufts. This form is usually associated with good prognosisand rapid response to corticosteroids. Occasionally, progres-sion to more generalized proliferative disease is seen,however. Imminofluorescent studies indicate mild diffusedeposition of IgG and BIC along basement membranes with heavierdeposition within lesions and mesangial areas. To answerwhether or not the differences between this pattern and the
Present Conceptj . I'ol " .\', 9. Scptn.,, 1 9 i1
S

7so!
diffuse proliferative type are qualitative or merely quanti-
tative will require much additional study.
I.,p•id Ncplirosis (Nil discase, minimal ch;i,)ge discsc)
This lesion is present in most casej of childhood nephroticsyndrome and is seen in about 25 percent of adults presentingwith nephrosis. The histology by light microscopy consists ofeither no change from normal or occasional focal, local tf•Lick-ening of basement membranes. In long standing recurrent cases,focal areas of scarring, irregular mild basement membranethickening, increase in mesangial cells and matrix and obso-lescent glomeruli are found. Immunofluorescent studies lookingfor deposition of IgG, IgM, and BlC have been uniformly unsuc-cessful. Under electron microscopy there is fusion of epithe-lial cell foot processes, believed to represent a nonspecificnormal reaction to increased protein passage across the base-ment membrane barrier. Occasional small subendothelial densedeposits have been reported but apparently bear no relation-ship to areas of basement membrane thickening. More commonare areas of platelet aggregation and occasional fibrin thrombiwithin capillary lumina. These findings may explain thegradual scarring and glomerular obliteration seen in longstanding cases.
Although it was formerly believed that lipoid nephrosismerely represented an early stage of idiopathic membranousnephropathy, it is now clear that these are two distinctdiseases unrelated to each other. No convincing cases ofprogression from the one to the other have ever been presented,the distinctly different ultrastructural morphologies clearlyexplain why.
The repeated failure to demonstrate immunoglobulin depo-sition has suggested to some workers a possible metabolic orbiochemical cause unrelated to immune mechanisms. Neverthe-less, the high incidence of atopy and eosinophilia in manycases, as well as the sensitivity of the lesion to cortico-steroid therapy, has convinced many investigators that sig-nificant immune events were being somehow missed by routineprocedures. Consequently, the recent report by Gerber andParonetto may represent a significant breakthrough in theunderstanding of this disease. By preparing antibody in goatsthrough the use of rare IgE myeloma protein, they have beenable to deMon~trate linear deposition of IgS in a coma like
I'r•',('7 ('picr,'pl,. /"f1 1V ,' Vv 'i. Sr r'fr'ml,'rr / Q 71

781 17r
fashion along basement membranes in all cases of lipoid nephro-sis studied. Unfortunately, other glomerular diseases studiedalso showed this reaction, suggesting that it may be a non-specific finding. Although much further work will be zeoessaryto clarify the pathogenic role, if any, played by this immuno-globulin deposition, at least one line of investigation isnow available.
Memb:.aioproliferative Glomerulonephritis
This group is a mixed bag of morphologic lesions andclinical expressions. Under this heading will be includedtrach entities as diffuse proliferative glomerulonephrit"associated with nephrotic syndrome, chronic hypocompleme.emicnephritis of childhood, lobular glomerulonephritis, necrotizingglomerulonephritis, some patients with acute post streptococcalglomerulonephritis pursuing a rapidly progressive course, aswell as cases having similar histology brat no antecedent strep-tococcal exposure. An immule basis for these diseases seemslikely, but few cases have been well-studied from that pointof view. Most cases have normal complement levels except fortiuse patients with hypocomplementemic nephritis in whichselective degradation of C3 by an unidentified serum factoroccurs. Electron microscony shows subendothelial and mesangialdeposits similar to the p-iliferative form of lupus nephritis.Iimmunofluorescent staining of' IgG and BlC in a lumpy patternis c-mmonly, but not consistently, seen. Prognosis is generallypoor except when a streptococcal etiology is present. Sincesome of these cases may present with rapid clinical deterio-ration associated with epithelial proliferation and crescentformation indistinguishable from RPGN, the examination of thesebiopsies with electron microscopy and ixmmnofluorescbnce ismandatory. Again the findings of fibrinoid necrosis andfibrin thrombi suggest an intimate role for the coagulationprocess especially in the more severe cases. It is likelythat the renal involvement of Henoch-Schoenlein purpura,hypersensitivity angiitis, and Wegener's granulomatosis issimilar in mechanism to these membrano-proliferative diseases.
Immuh net ('otnplc\ Ncph ritis w-th Kno~ ii Antlic.,
Under this heading may be included the nephrotic -. ndromeof penicillamine therapy, persisting Australia antigeneiaia,secondary syphilis, anl at least one case of carcinoma. In
I'rcwenz (',,nc ,).I d Il"V ,o 9. Sepictmher 19 -1
-

C
tlnnhnflogivV of (Iomendonephritiv - Steinnzull'r
addition the acute glomerulonephritis of falciparum malariais most likely related to immune complex deposition. In thecases of disease related to Australian antigen and quartanmalaria, antigen has been definitely shown to be depositedwithin affected glomeruli along with IgG and BIC. When IgGwas eluted from a patient with membranous glomerulonephritisand carcinoma of the lung, antibody specific for tumor antigenswas found. Unfortunately, efforts were not made to identifytumor antigen within the glomerular immune deposits. Thusfar, efforts to demonstrate penicillamine in immune depositshas been unsuccessful, probably for reasons -f technique. Incases of secondary syphilis with nephrosis no efforts havebeen made to 'emonstrate the causative antigen, although lumpydeposits of IgG have been identified by electron mic'oscopyand immunofluorescence. No doubt the presencs of treponemaantigen will be demonstrable in these deposits when properlystudied.
Suggested R eadine
Bacani F-', Valeasque. F, Kanter A, et al: Rapidly progressive(non streptococcal) glomerulonephritis. Ann Intern Med69:463-485, 1968
Baldwin DS, Lowenstein J, Rothfield NF, et al: Clinical courseof the proliferative and membranous forms of lupus nephritis.Ann Intern Med 73:929-942, 1970
Barratt TM, Soothill JF: Controlled trial of cyclophosphamidein steroir-sensitive relapsir.g nephrotic syndrome of child-hood. lancet 2:479-482, 1970
Benoit FL, Rulon DB, Theil GB, et &l: Goodpasture's syndrome.A clinicopathologic entity. Amer J Med 37:424-444, 1964
Cameron JS, Glasgow EF, Ogg CS, et al: Membranoproliferativeglomxerulonephritis and persistent hyponomplementemia.Brit Med J 4:7-14 '.3 (ct), 1970)
Carpenter CB: Immunologic aspects of renal disease.Ann Rev Med 21:1-16, 1970
Christian CL: Immnune complex disease. New n J Med280:878-884, 1969
Comerford FB, Cohen AS: The nephropathy of' systemic lupuserythematosus. Medicine 46:425-473, 19(.7
Prt',ent ('onccpist I'll 1 Ao 9. Scl,tcinher I()-/
-%

[.m~,,/gr J (;/,me'nthnephrattr .At,'ntulher
Dixon FJ: The pathogenesis of glomerulonephritis.Amer J Med 44:493-498, 1968
Gerber MA, Paronetto F: IgE in glomeruli of patients withnephrotic syndrome. Lancet 1:1097-1099 (My 28), 1971
Good RA, Finstad J, Cain WA, et al: Models of immunologicdiseases and disorders. Fed Proc 28:191-205, 1969
Peptinstall RH: Pathology of the Kidney. Boston: Little,Brown and Company, 1966, pp 235-396
Herdmann RC, Edson JR, Pickering RJ, et al: Anticoagulantsin renal disease in children. Amer J Dis Child 119:27-35, 1970
Kincaid-Smith P, laver MC, Fairley KF: Dipyridamole andanticoagulants in renal disease due to glomerular andvascular lesions. Med J Australia 1:145-151 (24 Jan), 1970
Koffler D, Kunkel HG: Mechanisms of renal injury in systemiclupus erythematosus. Amer J Y-d 45:165-168, 1968
Lange K, Tresar G, Sagel I, et al: Routine iimunohistologyin renal diseases. Ann Intern Med 64:25-40, 1966
lewis EJ, Covallo T, Harrington JT, et al: An imunopathologicstudy of rapidly progressive glomerulonephritis in the adult.Human Pathology 2:185-208, 1971
McCluskey RT: Evidence for immunologic mechanisms in severalforms of human glomerular diseases. Bull NY Acad Med46:769-788, 1970
Michael AF, Drumond KN, Good RA, et al: Acute poststreptococcal glomerulonephritis: Immune deposit disease.J Clin Invest 43:237-248, 1966
Rosen S: Membranous glomerulonephritis. Current status.Human Pathology 2: 209-231, 1971
Schreiner GE: The nephrotic syndrome. In Diseases of theKidney. Strauss MB, Welt LG (eds). Boston: Little, Brownand Company, 1965, p 335
Schur PH, Austen KF: Complement in human disease.Ann Rev Meal 19:1-24, 1968
Schur PH, Sandson J: Imunologic factors and clinicalactivity in systemic lupus erythematosus. New Eng J Med278:533-538, 1968
Segal BC, Andres GA, Hsu KC, et al: Studies on thepathogenesis of acute and progressive glomerulonephritisin man by immunofluorescein and immunoferritin techniques.Fed Proc 24:100-108, 1965
Strauss MB: Immunosuppressive treatment of proliferativeglomerulonephritis. New Eng J Med 285:632-633, 1971
Tresar G, Sewar M, Ty A, et al: Partial characterization ofantiger c streptococcal plasma membrane components in acuteglomerulonephritis. J Clin Invest 49:762-768, 1970
Present (Concepts. V'ol1" .Vo 9. September 19-1
•L'• ,•,•, -• • ';, .2• *t;.'•• >, . . . . . . . . . ..

- •
".S4
Vassalli P, McWluskey RT: The coagulation process andglomerJalar disease. Amer J Med 39:179-183, 1965
White IRM, Glasgow EF, Mills RJ: Clinicopathological studyof nephrotic syndrome in childhood. lancet 1:1353-1359, 1970
I'r e'n: (',u• pis. I'(1! I I' No Q. Se'pirn: her i Q-I

"1 HIE MALIGNANT PHASE OF HYPERTENSION
Relationship of the Kidney with Pathogenesis. Prognosis, and Therapy
Allan B. Schwartz, M.D.*
Malignant hypertension is a deva&tating entity. It is nota distinct disease itself but should be considered a syndromerepresenting '. specific phase of hypertension having variousetiologic p'issibilities. The etiologies vary f.cm primaryessential hypertension with nephroangiosclerosis .I nephritis,lupus nephritis, et cetera. 'The one common feat,_re that the longlist of etiologic considerations have is renal involvement. Bydefinition, the malignant phase of hypertension must have an ab-normality in some parameter of renal evaluation or the diagnosisis tenous. S3chottstaedt and 3okolou /1/ in their 1953 review ofclinical parameters associated with the malignant phase of hyper-tension found high percentages of cerebral and cardiac involvementbut found 100 percent renal involvement in their study of lO cases.'They wrote, "The kidney is the organ most seriously involved inmaligi ant hypertension". Renal involvement is recognized by pro-teinuria on urinalysis and abnormal renal functional parameterssuch as azotemia or elevated serum creatinine. These crude param-eters call attention to the obv )us loss of renal Conction threat-ening to result in uremia and e ath should the malignant phase ofhypertension go unchecked. The malignant phase of hypertensionis a vascular disease for certain. Histologically, fibrinoidnecrosis of arterioles throughout the body has been recognizedas the classic lesion.
As to the pathophysiology of the malignant pha~a of hyper-tensicn, no cilear explanation is yet available. It appearsthat some primary alteration occurs in arteriolar structuralintegrity, reducing luminal area and the effective perfusionvolume of the arteriole, i.e. reducing the available vascularspace. And, as stated by Poiseuille's law (resistance toviscous flow varies inversely with the fourth power of theradius), this reduction in vascular radius dramatically in-creases peripheral vascular resistance. Cardiac systolicejection force attempts to compensate for this increased vas-cular resistance by producing a more forceful ejection and a
"*,\,tnt Nfeor ot Mcdit,nc. D;•mon of Ncphrolog) and Vascular D:eew . Department of%lcti nc. flahncr anin Mcd'cmi College and to,,pital, Philadelphia. Pcnn.] h-anla
I'r %cnii (C'n e'piv. Vl"l /i" Ni' Q. Sel'tem her 1971

S...•,, ,l• _, o .... . . ..n ~/z ,J II cr I. ': S n ~
progressive increase in systolic pressure becomes apparent.At these excessive preisures, further alterations of stretch-ing and constrictior of arterioles results and a viciouscycle is set in motion. As a result, there is a progressiveincrease in both diastolic and systolic pressure.
Further vascular alterations occur as plasma appearslocally in zones of dilatation in the wals of terminalarterioles at an early stage in the process. Local overstretching or tearing of medial muscle fibers occurs whichmay simultaneously destroy the muscle and turn the vesselinto a semi-permeable sembrano. This allows various colloidmaterials to escape into the tissue while the destroyed vas-cular tissue itself becomes saturated with concentrated plasmaproteins giving the appearance of fibrin, i.e. fibrinoidnecrocis. /2/
Recently, evidence has arisen that points to a hemato-logic coagulation abnormality associated with the vascularchanges of malignant hypertension. An increase in permea-bility of =all blood vessels has been thought to set inmotion the fibrin deposition in the wall and in the lusen ofvessels. These fibrin deposits then induce fragmentation ofred blood cells, which leads to microangiopathic hemolyticanemia which then results in further deposition of fibrinuntil finally the vessel is occluded and the peripheral bas-cular resistance is maximum. /3/
Another area of research has to do with a deposition oflipid-like material in subendothelial areas of glomerularcapillaries. These lipid deposits have been demonstrated byelectron microscopic examination of glomerular capillariesfrom renal biopsies of patients having the malignant phaseof hypertension. /4/
The humoral and neurogenic aspects of the malignantphase of hypertension are still open to question. Peart /5/suggested that aldosterone excess was a defense mechanismbrought c.ut to counteract the angiotensin induced sodium loss.Oversecretion of aldosterone in malignant hypertension wasbelieved by Cope and Pearson /6/ to be a consequence of renaldamage. lAragh, Sealey, and Somers /7/ in 1966, found astrong correlation between secondary hyperaldosteronism ofmalignant hypertension a-d increased levels of plasma renin.These data strongly suggested a renal course of stimulation
I'rccn r ,ncCptr. 1 ,1 I/I Ph''; •r ') "/

Malignant Phase ouilypertension - Schwarzr
for the hyperaldosteronisa observed in the more advanced stagsof the malignant phase of hypertension. Certainly, some of thehigbest plain renin actLvity values that have been reoordedhave been in maligmnt hipertansion.
Intravenous injection of angiotensin has been implicatedin causing fibrinoid necrosis in the rat as has a partly puri-fied renin preparation. /8,9/ This ability to produce necroticvascular lesions is also shared by various pressor amines suchas tyramine, 7sthoAine, and norepinephrine. /10-12/
Amine hypertension has been recognized clinically. Foodssuch as cheeses and fermented material such as beer containtyromine which has been shown to elevate blood pressure byieleasing norepinephrine. /13/ In the presence of m~onomineoxidase inhibition, the usual degradation of norepinephrine isretarded and exoessive tyramine ingestion may provoke severeor even malignant hypertension. Certainly, pheochrmocytomahas been a reoognived cause of malignant hypertension.
The relationship between the sympathetic nervouts system,catecholamines, and renal humoral mechanisms have been wellestablished. Wathem et al /14/ in 1958, demonstrated therelationship between catecholamines and the renin-angiotensinsystem by infusing norepinephrine in anesthetized dogs andevoking an acuto release of renin. Michelakis and Horton /15/in 1970, confirmed this relationship in man by infusing nor-epinephrine in humn volunteers a.nd evoked an increase inperipheral plasma renin activity. It is possible that thisinterrelationship between the sympathetic nervous system andthe renin-angiotensin system could be intimately involved asthe "trigger mechanism" of the malignant phase of hypertension.
It is also possible that an existing renal parenchymaldisease could in itself intrinsically initiate an abnormalhumoral vasopressor substance which alone could be the •triggermechanism" of the malignant phase of hypertension. There isalready evidence for a renal humoral vasopressor substanceexisting as a major factor responsible for the blc.d pressureelevation and vascular damage of the malignant phase of hyper-tension. /16/ This vasopressor effect of the kidney has beenpresented in the setting of both primary essential hypertensionand chronic renal parenchymal disease, i.e. chronic glomerulo-nephritis.
Prcc,'rnt (onrccpt. i 'lIV No V'. St p,:c I;,cr I -l

44
111l41lviaw Ph1low°,, llvTa-rhvinwn, .t itvirl/i
I am certain it is obvious to the reader that I am fos-tering the concept that there is a peripheral vascular alter-ation that initiates the malignant phase of hypertension.The question that arises is, "What triggers the vascularalteration?". It is interesting to hypothesize that thitt"trigger mechanism" might involve a renal-sympathetic nervoussystem catecholamine chanism which once set in notion willdevelop into a vicious cycle resulting in arteriolar fibrinoidnecrosis.
The clinical syndrome of the malignant phase of hyperten-sion is a reflection of the diffuse vascular alterations,specifically fibrinoid necrosis and the resultant compromisedperfusion of vital organs - brain, heart, kidneys and eyes.
That the above process is reversible is a thesis gainingsupport each year. The blood pressure must be reduced toallow vascular changes to heal. The resistance vessels mayreturn to their normal caliber, perfusion will improve, andthe syndrome w-4i abate.
PROGNOSIS OF MALIGNANT HYPERTENSION
The prognosis of malignant hypertension is definitelyimproved today over 20 years ago and even -0 yearsa . Theapparent reasons for this improvement are twofold:(l) theavotilability of relatively safe, potent antihypertensiveagents which have been developed for clinical use during theperio&, and (2) an increasing knowledge and understanding ofthe use of the antihypertensive agents in the presence ofrenal ikaufficiency associated with the mlignant phase ofhypertension.
Before the advent of such early therapy as sympathecte-ny,malignant hypertension was consistently a fatal disease in amaximum of four or five years and 80 percent fatal in the firstyear. /17-19/ In 1938, Page /'20/ reported on beneficialresul's of anterior nerve root section. He wns the first toshow an improvement in the course of malignant hypertensionin that there was some evidence of improvement of cardiacpareneters, eye grounds, and renal function. The patientstill eventually succumbad to the disease, however.
Prcevni (tn',, cpts. i ,I I V .%'(, 0, Seprcnzbher IQ1-1
- -- - -

The advent of ganglionic blocking agents and adrenergicblocking agents brought about an improvement in the survivalstatistics. Enoephalopathic a"d cardiac causes of deathassociated with malignant hypertension declined. However,the peroentage of renal causes of death increased demon-strating a failure to arrest the arteriolar fibrinoid necrosiswithin the kidney.
In 1956, McCormack et al /21/ showed definite evidenceof healing of acute destructive lesions of malignant nephro-angiosclerosis in patients treated with potent antihypertensiveagents including hexmmethonium, pentolinium, chlorosondamine,mecamylamine, reserpine, and hydralazine. Although an autopsystudy, there had been soae transient clinical remissionseffected in these patients with malignant nephroangiosclerosisby intensive treatent with the agents noted above. Renalfailure was the primary cause of death of 14 out of 19 treatedpatients. There was a definite "cessation of Activity and aregression in both arteriolar necrosis and thrombonecrosis".This was associated with disappearance of most of the foci offibrin accumulation and of the evidence of acute vascular damage.
McCormack et al /21/ noted in their review that in somecases treatment was not wholly effective and minimal activelesions of malignant nephroangiosclerosis persisted and wereapparently progressive, although certainly not nearly asrapidl,- as fn the untreated patient. Their words were notheeded and, for the next few yeara, hypertensiologi~ts fearedtreatment of malignant hypertension associated with renalinsufficiency.
The relationship of renal insufficiency and survivalrate of patients with malignant hypertension has been inter-esting to follow through the evolution of successful anti-.iypertensive therapy.
In 1959, Harington et al /22/ reported that malignanthypertension associated with a blood urea nitrogen of greaterthan 60 mg/lO0 cc before therapy correlated with only a 10pe.rcent survival by two years. Those patients with a bloodurea nitrogen less than 60 mg/100 cc had a 55 percent survival' - two years.
Proven, ('onccp rS. I ,,I I o Q, . fl' r I S(
~?

In 1961, Dollery /23/ expressed the opinion that pro-gressive renal failurs could not be halted by antihypertensivetherapy. With respect to the blood urea level, he reportedonly a 15 percent one year survival if malignant hypertensionwas accompanied by & blood urea level of over 60 mg/100 cc(blood urea nitrogen greeter than 30 m/lOO cc). The one yearsurvival for patients having malignant hypertension and ablood urea level less than 60 mg/100 cc was 73 pelcent.
In a report by Mohler and Freis /24/ in 1960, a corre-lation of five-year survival was made with normal or nearlynorml levels of nonprotein nitrogen before treatment.
Sokolow and Perloff /25/ reported a five-year survivalof 5 of 11 patients who had creatinins clearanos values greaterthan 45 cc/min before therapy with ganglionic blocking agents.Of 15 patients with poor renal function before treatment, nonesurvived even three years.
Kirkenda•. /26/ wrote that successful lowering of bloodpressure improved signs of necrotizing arteriolitis thatallowed histologic improvement. To produce the same improve-ment of histology in the kidney "one must reduce the bloodpressure and blood flow to the kidneys so that glomerularfiltration rate and renal excretory function are reversiblydecreased." Thus ona is on the horns of a dilemma! /26/Ki• cendall in 1961, as were many others, was faced with thefact that the closer to normotension the patient came, theworse the renal function became dur..ng the early phase oftreatment of the malignant hypertension. The key to the abovequotation is that aggressive reduction of blood ?ressure mightinitially lower renal function, but this initial decline is afunctional one that is "reversible".
Through the 1960's, physicians were still unable to cope Iwith malignant hypertension coexisting with significant renal
-* insufficiency, Therapy was often withheld or ineffectivelyadministered at the first hint of blood urea nitrogen rise.As recently as 1966, Langford and Bonas /27/ advocated thatwhen a rise in blood urea nitrogen occurs, it is usually bestto hold the pressure at the level that has been obtained oreven to let the blood pressure go slightly higher rat)-'r thanimmediately pressing on to further blood pressure reduction.They did, however, recognize the need to continue antihyper-tensive therapy in treating malignant hypertension despite the
lon (" cc• z . ". NII . "( rtPcmbr'r I. -I
-+-**-*

R-
791
rise in blood urea nitrogen to permii; healing of the nocrotizingarteriolitia. They also agreed that At may be necessary toutilize dialysis while hypotensive, therapy was being given inthe face of worsening renal functi :).
Schroeder /28/ claimd that if improvement in renal func-tion does not occur early, the treatuent can be consideredonly life extending and he predicted a steadtly progressivemortality. He did, however, recognize the value of effectivelowering of blood pressure of malignant hypertension with mildto moderate renal insufficiency and noted that in his experi-ence, one-quarter of such treated patients survive five years.
Woods and Blythe /29/ appear to have the most encouragingexperience in the literature dealing with survival of patientshaving malignant phase of hypertension complicated by severerenal insufficiency. These authors of aggreasive therapytreated 20 patients with malignant hypertension and a bloodurea nitrogen of 50 mg/100 cc or Uigher and noted a 55 percentone-year survival, and a 35 percent two-year survival and a25 percent longer term survival.
In 1969, it was again reported that aggressive treatmentof accelerated hypertension in patients with azotemia resultedin slight worsening of renal function during the first twoweeks. However, by three months of effective treatment, renalfunction had improved to levels batter than pretreatmentvalues. /30/
The conclusion is that reduction of blood pressure tonormal levels in patients with malignant phase of hypertensioncomplicated by renal insufficiency does not necessarily resultin irreversible deterioration of renal function and my actuallyimprove renal function in a large proportion of patients.
At Hahnemann it is obvious to our staff that the only wayto attack malignant hyperteniioi:, associated with primarynephroangioscleroais is to lowe:- promptly and aggressivelythe blood pressure to normotensLve levels. However, primaryrenal parenchymal disease, such as chronic glomerulonephritisand lupus nephritis, may be associated with a secondary formof malignant hypertension wl ,.h presents entirely different
Pre c n Co (0,,cc'pr. i',I " .V \ o 9. Se!c t, h• t r I 7 1I

ii7112
Abilq.ninatt Ph1ow+ I, l|lt' wrlvi',%tpit S. it stiv.irlz
considerations. The physician is now faced with the necessityof considering two separate prognostic %spects in one patient,i.e. "What is the prognosis of the primary renal parenchymaldisease and what is the prognosis of the secondary and co-existing malignant hypertension?". Renal insufficiency mightbe a definite feature of either. The clear distinction mustbe made early between malignant hypertension due to primarynephroangiosclerosis versus malignant hypertension due toprimary renal parenchymal disease. Often, the only means bywhich the distinction can be made is the kidney biopsy. Oncethe diagnosis of primary nephroangiosclerosis is established,the treatment program for the malignant phase of hypertensionwith renal insufficiency is clear cut - normotonsionbe acauired and tAintained.
Normotension provides the only setting in which thenecrotizing arteriolar changes within the kidney will heal.Normotension =ast be maintained even if renal insufficiencyappears to worsen in the early phase of tieatment. Thisfurther loss of glomerular filtration rate manifesting a risein serum creatinine and blood urea nitrogen is a functional,reversible loss.
The sudden decrease in perfusion pressure resulting fromthe antihypertensive prescription will result in a decreasedglomerular filtration rate. A transient worsening of azotemiaand even uremia may occur during the early vascular healingphase. A need for supportive peritoneal dialysis or hamo-dialysis therapy may become apparent in some cases. Certainly,if the diagnosis is made early and treatment initiated early,this need will be transient. Once the fibrinoid vaecularchanges have healed and renal arterioles are again patent, theglomerular perfusion will improve and glomerular filtrationrate will gradually increase. Such an example is representedin the following case presentation.
CASE REPORT
The patient is a 32-year-old black female who presentedwith a one-week history of rapidly progressing dizziness,severe suboccipital headache, and nausea. On the day of ad-mission, she had several episodes of vomiting. There was no
P'reven t Concept.s. [ol / I* No 9. Scpeti nor 1 Q71

I Aihignat IPha , oJ Ilylc'rtenstm - SchIwarti
past history of renal disease, hypertension, cardiovasculardisease, or diabetes. The family history was negative forhypertension.
The physical examination demonstrated the blood pressureto be 230/156 = Hg in the right arm and 228/152 rm Hg in theleft aim. Pulse rat-, was 96 beats/mia and regular. Oraltemperature was 98.6 F. Funduscopic exination revealedsevere arteriolar aasm, soft cottonwool em2d&Tes, flame shapehemorrhages, and - Apilledema bilaterally. 'he heart examina-tion demnr-traec.8 the point of naximal impules in the sixthintercc.--'s,. sa,'cve li the a+terior adllary line. A prominentleft ven-ricular heave was noted. An atrial gallop was present.A grade IlI/VI early systolic ejection munmur was noted at thesecond right intercostal space. The lng fields were clear.Abdomelnai examination showed no palpable liver, spleen, orkidneys. "here was no costovertebral angle tenderness andthere was no abdominal bruit. Femoral pulses wore strongbilaterally. All periphern! pulses were found t1, be normal.There was a trace of pretibial and pedal edema bilaterally.The neurologic evaluation showed the patient to be moderatelylethargic, but she was well-oriented for time, place, andperson. There was no nuchal rigidity and no localizing neuro-logic abnormality.
Laboratory evaluation demonstrated the blood urea nitrogento be 109 mg/100 cc, serum creatinine 11.5 mg/100 cc, serumsodium 137 mEq/L, serum potassium 3.8 mEq/L, serum chloride98 mEq/L, and serum iarbon dioxide combining power 20.9 mwiEq/L.Urinalysis demonstratced 8-10 red blood cells/HPF and 10-15white blood cells/HPF, and a one plus reaction to protein.Tests for urine, sugar, and acetone were negative. Urinespecific gravity was 1.005. Complete blood count showed ahematocrit of 29 percent, hemoblobin of 9.6 gm/l00 cc, whiteblood count of 5,150 with 65 percent segmented forms, 5 percentbands, and 30 percent lymphocytes. The peripheral plasma reninactivity was 5000 ng/l00 cc (Method of Boucher). The initialtherapy consisted of aipha-methyldopa 500 mg intravenously andfurosimide 80 mg intravenously. The alpha-methyldopa wasrepeated in a dose of 500 mg intravenously every six hoursfor four doses. At that time, the patient was started on oraltherapy consisting of alpha-methyldopa 500 mg every six hoursin combination with hydralazine 50 mg every six hours andfurosimide 80 mg every 12 hours. Within 12 hours after thepatient's admission, the blood pressure was reduced to 120/80
Hg and within 24 hours the oral medication described abovewas maintaining a blood presmsre of 100/70 mg Hg in the supineposition.I'rec nt (onlc pt.. ", 1 I" .\'d ','i" lcr 1 1 '

794
S•l~~tltlihtlivitn Mawlt (if Ih'pertemnwJ - Schwazrtz
Three days later the blood urea nitrogen had increased to150 mg/100 cc and the serum creatinine had risen to 16.2 mg/0OO cc.A renal arteriogram demonstrated patent main renal arteriesbilaterally. There was moderate arcuate and interlobulararterial narrowing within the renal cortex. The transit timeof the radiopaque material was delayed and there was absenceof nephrogram effect. On the fifth hospital day the bloodurea nitrogen was noted to have increaued to 193 mg/lO0 ccand the serum creatinine was 15.3 mg/100 cc. The patient haddeveloped further evidence of uremia and peritoneal dialysiswas instituted for the ensuing 48-hour period. Open renalbiopsy was then performed. The renal biopsy demonstratedevidence of fibrinoid necrosis of +,he afferent arteriolesand interlobular arterioles. Figure 1. There was alsotypical onion-skin effect in arterioles diffusely throughoutthe kidney. Figure 2. The interstitium was moderately in-volved with round call inflamatory reaction, edema, and amild degree of fibrosis. The glomeruli were nonspecificallythickened and minimally proliferative. Figure 3. Only a fewof the glomeruli were entirely hyalinized. Two 24 -hour urinesfor vanillylmandelic acid excretion, were 6 mg/24 hours and7 mg/24 hours. Riepeated urinary cultures demonstrated nosignificant growth.
The clinical course was marked by normotensive responseto the medications (furosimide, hydralazine, and alpha-methyldope). The patient showed continuous impro-ement in overallwell-being. Over the next three weeks, there was a stabili-zation of the blood urea nitrogen at 14 ;/lG'100 cc and theserum creatinine at 11.3 mg/lO0 cc.
An orthostatic response to the i.dications was noted asthe blood pressure was consistently ltwer in the standingposture than it was in the supine posture. The average bloodpressure in the standing posture was U5/8O mm Hg and theaverage blood pressure in the supine postura was 170/100 mm Hgduring the patient's hospitalization. For this reason, thepatient's bed was tilted 30 degrees upright at the head. Thepatient was discharged3 and followed at frequent intervals asan outpatient. Medications were continued and occasionaladjustments were made to maintain normotensive blood pressurelevels. Associated with the marked orthostatic response noted,three episodes of dizziness occurred during the next few months.However, there was no syncope. Again the supine blood pressurewas consistently higher than the normotensive-to-slightly-hypotensi.e standing blood pressure. The patient's bed at home
t'ri. nt (Cincepiv. I', l 1' A(P 9 Sepicetm wr I 9 1
- -- ~-~.-.-?

795
Alalignantz Phase of JIliperimision - Srhwrtzr:
I. *PF 9
-k-
- SNS
V.g~
Wj X.~
40L~~a,
4(' ~.~
; 'for- hcnu' Hc':q durngz:acutt -haw -IM 1. -060; xrr,,u aindi,~aze fibrinoid nmcrogisofwtcriolc. 2-. 3rrow bindlcatc% n'or-,'m.ific Zhckcn~nc and prill-ratil-, of glowmerulus.I ilo. t 2. fiow rif Obihra:,cn finicr~loular. 2rz% b% -onion rn efice;:i&. g ME )Fig 3.1lowernrlit. Mild nen-pcafit, thickc.-unc and rrolifcrra;v- ofclorncrulut iIl&F. X180).
Prceten; C('auct-s. 1I li I V NVo '.Sep m-n he- 1 -'1

was placed in the 30 degree head-up tilt position to avoidthe mild blood pressure elevations while she slept.
During the outpazient follow-up period, the patient wastrr.ined to record her own blood pressures at home. She keptan extremely accurate record which corresponded we'" with thein-office readings.
The funduscopic picture cleared over the initial threemonths of outpatient follow-up and her residual funduscopicchanges consisted of mild arteriolir narrowing with ao evidenceof hemorrhages or exudata)s.
The paz.ent returned to work after three months and main-tained full employment following that date.
The blct- urea nitrogen and serum creatinine progressivelydecreased over the next few months, wnd within two montihs thecreatinine clearance increased to 30 mtilin.
After having maintained a steady improvement while normo-tensive for seven months, the natient was readmitted to thehospital for elective evaluation of her renal status. Therepeated kidney biopsy showed definite evidence of afferentand interlobular artericlar patency. Figure 4. There was noevidence of the typical onion-skin effect and fibrinoid necro-sie which bad been noted in the initial biopsy. Many glarulidid show s9me evidence of shrinking and there was an increaseof Bowman's space. Figure 5. However, the gion.rular capi-llaries were no longer thickened and the degree of prolifera-tion was less than had been noted iu the initial biopay. Thecreatinin. cleas-ance was 30 mi/min and the serum croatininewas 3.6 mg/l00 cc.
Repeated evaluation of the peripheral plasma reninactivity demonstrated v•iues below 1000 ng/l0Q cc in contrastto the initial value of 5000 ng/l00 cc during the initialhospitalization.
The patient was then seen at monthly intervals. &emaintained a normotensive blood pressure in the upright postureand a minimum degree of hypertension was recorded only occa-sionally in the supine posture. The medication was continuedrigidly by the patient. Thirteen months after initial treat-ment tbe patient's blood urea nitrogen was 42 mg/100 cc and
i'r, tant 'C,,nc-pis. V',, I " .\' Q. c F' n o pte I• rr'"

791,
M.4Itzigizwnt JPiuw vi 1 £ ~ie4'!ZI4[0 A.
a ti pi 1'
V-1
jj~ ~qf~/~~ '4A-
t ~ ~4;%AP 2 0 4%
F:F ,Ioj Rena,*~ 4"1.,--: ýcvcn rnonilh% o! r:;~~' , 3;,1 t-;o I~~T 12C
Fh: 5 hr,- Renal biopt¶ after .717.01 tnc 1h , -;1*,~ .'.-* 1- ioop- arc more
ri'r(w,1 (vqccp:ý i 1 A\ ~
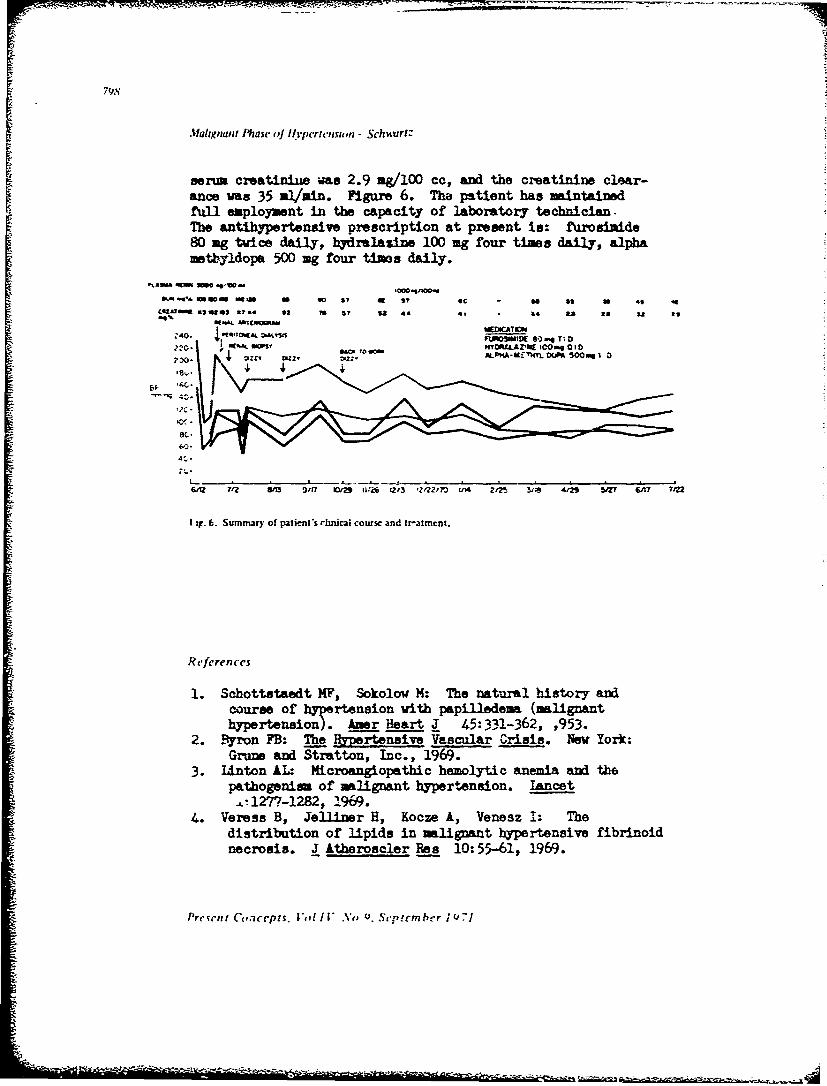
79S
Afahigi.ni Phasc ,J Ilyperiensiorz - SchiturlZ
Ber=i creatinit was 2.9 ag/lO0 cc, and the creatinine clear-ance was 35 al/amin. Figure 6. Tha patient has maintainedfull employment in the capacity of laboratory technician.The antibypertensive prescription at present is: furosinide80 ag twice daily, hydralazine 100 ag four times daily, alphamathyldopa 500 mg four timos daily.
S . . . .g i
1~.4 aS Seot ted Ma, Uooo 14: Th natra bis -o
92~ 70ae by4SI U ST 5 44 41 34 ts &5 11 I
h r i . re4 EDICAT•340. .WA ow~n : . •rtFeVSIUa E Crs mg T 1 r22-1 -1- A- HYcttiAcanEm1i0 ad th1
path TOrn•Oft AL-Kn hTHYL DA5 e00 e 1 0
GM 7 7-2 am g i ns 1 1-9 l6b. 1215 2' 0 In' zI2l 3i9 412 5a2 GA? ?122
1 ig. 6. Summaury of paiien*S rInliCal course and Ir-atmcnt.
References
1. Schottstaedt H,, Sokolow M: The natural history, acourse of hypertension with papilledena (malignanthypertension). Amer Heart 3[ 45:3431-362, ,953.
2. £Byr-on FB: The Pa resv Vascular Crisis. Now York:Grune and Aton, Inc., 1969.
3. lrnton AL.. Microang'opatbic hemolytic anemia and thepathogonim of mlignant hypertension. tancet
.L!277-1282, 1.969.4. Veress B, Jelliner H, Kooze A, Venesz 1: The
distribution of -lipids in malignant hypertensive fibrinoidnecrosis. J Athoroscere Res 10: 55-61, 1969.
Present: Conicepts. Voi I/[.t' Nou. Sep rem her ;QU71

5. Peart WS: Possible relationship between salt and theangiotensin system in essential hyper-Lension. (In bookunknown) by KD Bock and PT. Cottier (eds). Berlin:Springer-Verlag, 1960.
6. Cope CL, Pearson J: Aldosterone secretion in severerenal hypertension. ;lin Sci 25:331-341, 1963.
7. Iaragh 3H, Sealey JE, Sommers SE: Patterns of adrenalsecretion and urinarj excretion of aldosterone and plasmarenin activity in normal and hypertensive subjects.'irc -as 18:158-174, 1966.
P. Byron FB; Angiotensin and renal vascular damage, BritJ Ep Pa__th 45:7-12, 1964.
9. Asscher AW, Anson SG: A vascular permeability factorof renal origin. bature 198:1097-1099, 1963.
10. Duff GL, Hamilton 3D, Magner D: Experimental productionof arteriolonecroeis and madionecrcsis of arteries bymeans of tyramine injection. Proc Soc Exp Biol Med41:295- 1939.
11. Herbertson BM, Kellaway JD: Arterial necroeis in therat produced by methoxamine. J Path Bact 80:87-92, 1960.
12. Giese J: Acute hypertensive vascular disease. II Studieson vascular reaction patterns and permeability changesby means of vital microscopy and colloidal tracertechnique. Acta Path Microbiol Scand 62:497-515, 1964.
13. Cmroe :,H Jr: The mechanism of action of some drugs vnthe sympathetic nervous system. Physiol Physicians1:5-8, 1963.
14. Wathen RL, Kinsebury WS, Stouder DA, et al: Effectsof infusion of catecholanii-es and angiotensin II onrenin release in anesthetized dogs. Amer J Physiol209:1012-1024, 1965.
15. Michelakis AM, Horton R: The reJ3tionship betweenplasma renin and aldosterone in normal man. Circ Res26 and 27 (suppl):185-194, 1970.
16. Onesti G, Schwartz A, Swartz 3, Famirez 0, Brest AN:Vascular factors in renal hype rtensioD. (Abstract)Circulation 37 and 38 (suppl):150: 1968.
17. BJork S, Sannerstedt R, Angervali G, et al: Treatmentand profession in malignant hypertension. Clinicalfollow-up study of 93 patients on modern iedical treat-ment. Acta Med Scand 166:175-187, 1960.
18. Keith NM, Wagener HP, Barker NW: Some different typesof essential hypertension: Their course and prognosis.Amer J Med Sci 197:332-343, 1939.
Pr w tŽ n, - . - , -;as

VIIj m " USi
19. Kincaid-Smith P, McMichael J, Murphy EA: The clinicalcourse and pathology of hypertension with papilledqua(malignant hypertension). q=_z' J Ied (New Series)27:117-153, 1958.
20. Page IH: Medical aspects of surgical treatment ofhypertension. JAMA 110:1161-1165, 1938.
21. McCnrnack IJ, Beland JE, Schneckloth RE, et al:Effect of anidhypertensive treatment on the evaluationof the renal lesions in malignant nephrosclerosis.Amer J Path 34:1011-1021, 1958.
22. Harington M, Kincaid-Smith P, McMichael J: Resmts cftreat•int in malignant hypertension. A seven yearexperience in 94 cases. Brit Med J (No. 5158)2:969-980, 1959.
23. Dollery CT: Malignant hypertension. In Treatment ofHypertension. Pickering GW, Cranston WIj, Pears MA(eds). Springfield, pp 175. Thomas, 1961, p 47(No. 343,h Amer lectures in Living Chemistry, BonnerstoneDivision)
24. Mohler ER, Jr, Freis ED: Five-year survivai of patientswith malignant hypertension treat6d with an~ihypertensiveagents. Amer Heart J 60:329-335, 1960.
25. Sokolow M. Perloff b: Five-year survival of consecutivepatients with malignant hypertension treated with anti-hypertensive atents. Amer J Cardiol 6:858-863, 1960.
26. Kirkendall WM: The management of hypertension patientswith renal insufficiency. Hypertension recent advances.
.The 2nd Hahnemann ym sium on Hypertension Disease.Brest AN, Moyer JH (eds). Philadelphia: tea andFebiger, 1961.
27. Iangford HG, Bonas JR: Treatzent of the uremic hyper-tensive patient. Mod Treatm 3:62-67, 1966.
28. Schroeder HA: Azotemic malignant hypcrtension. (letterto the Editor) New Eg Mad 277:291, 1967.
29. Woods, JW, Blytho WB: Management of malignant hyper-tension complicated by renal insufficiency: T-iuthere.perience. Trans t' 3iat Asso 79:108-114, 1967.
33. Mroczek WJ, Davidov M, Gavrilovich L, et al: Thevalue of aggressive therapy in the hypertensive patientwith azotension. Circ!Llation '0:893-904, 1969.
i'rev'rnt p',,n•f C s. :'I I ,No Scltcnzhcr JI -1

*~~ý - ** -"
So7 I
URINARY I'PACI INFECI iON
Its Diagnosis and Significance
CP' Michael R. Conger, MC*
The role of urinary tract infection in the evolution ofsignificant renal disease is a subject of fervent current in-vestigation. The significance of asymptomatic bacteriuria ishotly Jebated. This paper viil attempt to clarify why thereis a cisparity of thought on this subject and bring the presentlyknown facts together so that the reacer will be able to appraisecritically future references to the topic.
Iagnosis of urin.m.r, tract infection
There is no problem ciagnosing urinary tract infection inthe patient with fever, flank pain, ..ysuria, ana pyuria. Theproblem lies in determining the significance of symptoms witha normal urinary sediment or bacteriuria in the absence ofsymptoms. TABLE I outlines a few common reasons for the mis-diagnosis of urinary tract infections.
A frequently confusing problem is the fintoing of pyuria ina "routine" urina.ysis. Although this fin,:ing shoulz alert cneStq a •:iagnosis of infection, yuria can occur in the absence ofbacteriuria. TABLE II outlines the nonbacterial causes )f pyuriswhich -'ust also be consicered when it is ciscovered. When urinecultures are sterile in such instances (or have an insignificantbacterial growth), genitourinary tract tuberculosis should beconsidered and excluded by obtaining at least three morningurines for Ziehl-Neelson staining =nd cultures.
"Prcwnt addxcs., Dcpartmcnt of Surgcr). •enua'i Arm) Hoqital. For: RrBag. Nortlh Carolina
Prescni Ci',,ccpui V,,Ii .V,, NI. Sptzcmhcr 19)71

S0i2
=.1
TAHLI I
REASONS FOR MISDIAGNOSIS OF URINARY TRACT INFECTION
-'PYURIA 05 WBCjIjpF SPUN URINE) -I
occurs only in 50 percent of women with a3ymptomaticbacteriuria
occurs in the absence of bacteriuria
-"WBC CASTS"
may come from prostate
-•POSTERIOR URETHRAL INFECTION
may occur in patients without ba,:teriuria
"-DYSURIAmay not mean bladder infection even with 1000- 10,000
organisms per milliliter
-.BACTERIURIA
exists asymptomatically
TABLE 11
NON-BACTERIAL CAUSES OF PYURIA
GLOMERULONEPHRITi;
LUPUS NEPHRITIS
RENAL TUBULAR CELLS MISDIAGNOSEDAS WIIITE BLOOD CELLS
BLADDER TUMORS
URETHRITIS (Tnchomonaq
Present Concepts. Vol IV No 9. September 1971
8U3
Urinary Tract Infection. Conger
Although glomerulonephritis or lupus nephritis cause pyuria,they should be apparent from other clinical manifestations.Renal tubule cells resemble white blood cells but can be diffcrrentiated from them by the use of peroxidase stain (Sedi-stainMRJ).Bladder tumors should be considered as a cause of pyuria when thepatient is past forty or has a history of exposure to anilene dyesor heavy cigarette smoking. Urethritis without infection of theurine can often be con"irmed by comparing a two-part urine collec-tion. Trichomoniasis as a cause of pyuria can be determined byexamination of the sediment and recognition of the organism. Itis therefore apparent that symptomatology and urinalysis may aid
in diagnosing urinary tract infection, but the urine culture isstill required to confirm it.
Urine is normally sterile. It had been theorized thatshowers of bacteria occurring normally could cause a low titer ofbacteria to appear in the urine via glomerular filtration. Stameyand Pfau /1/, hcroever, gave intravenous bacterial injections todogs without resultant bacteriuria. Thus there is strong evidence
that bacteremia does not induce bacteriuria in nonobstructedindividuals. Despite the known sterility of urine, it has been
shown that only two percent of women with sterile urine, as provenby suprapubic needle aspiration, have a sterile midstream collec-tion. Figure 1. We are therefore obligated to develop someground rules for deciding the significance of a positive culture.If the female perineum is meticulously scrubbed and a total voidedspecimen contains more than 105 organisms per milliliter, there isan 80 percent chance that the patient has a urinary tract infec-tion. Two such positive specimens gives a 91 percent chance thatthe patient is infected, and three such cultures gives a 95 per-
cent chance. /2/ Realistically, however, waiting for two or three
consecutive procedures to approach a respectable range of errorrepresents a serious time delay as well as additional expense.Also, this statistical presentation does not tell one how manypeople with less than 1O5 bacteria have significant infection andmany physicians have misinterpreted these figures to mean thatno one with less than 105 organisms per milliliter has a signifi-cant infection. Stamey and Pfau /1/ list three alternatives tothe total voiding cultures which can avoid these problems:(1) suprapubic needle aspiration of the bladder, (2) midstreamurine specimen collected on lithotomy table after nurse cleansthe perineum, and (3) catheterization of the bladder.
I'reenI Con'epti, Vol IV No 9, Sep tem ber 1971

p.o
I rltlrlrl" Ireit I 1"1ic, i1sut ( "e~rlgcr
26/54 culturescontailned 6rom-negafive bacill;
S40 38 ,9
i-.
30
0 2201.2 >" 4.
C2 16.7
L
I0 -- :7.4 -
0 i- 100 100- 1000- I0,000- >100)0001000 I0,000 100,000
Bacteria per ml.I ig I. Midstream bacterial counts in 54 femalcs with sterile suprapubic bladder aspirations. /1l/iReproduced by permision of the authors and The Williams and Wilkins Co.. publixhers.1
Needle aspiration of the bladder is safe, offers a 99 per-cent confidence level for obtaining sterile urine, and is pain-less, but may be emotionally distressing to the patient. Stameyand Pfau ./l suggest that collecting a midstream specimen from,a patient on a cystoscopy table after a trained nurse hasthoroughly cleansed her perineum is nearly as efficient (95percent confidence level). Figure 2. This is not practical forzost physicians, however. Although catheterization is an accurateway of diagnosing urinary tract infections, there is the risk ofcausing an infection. The risk is reasonably small in outpatientswithout a urinary tract abnormality, but in any hospitalizedpatient the incidence of infection is high -- as high as 20 per-cent on a medical ward according to one report. /3/ If a patient
Present Concepts. Vol IV A'o 9. September 1971

1lrinarr Irut I /til. i tvi,,i ( ;,nrr
needs catheterization because ofi obstruction it shoul I not be
av)i:ed, but to uZe a catheter for diagnosis may lenJ1 to a
mtrbi :ity o0' its D)wn.
50
40 - 39.04-C 3
4-oO.30
0
0204-C
a2i0.9.1 2.6
5. 4.0
2.
0 1- 100- 200- 300- 400-500- 600- "700- 800-100 200 300 400 500 600 700 600 900
Bacteria per ml1.
I ,g. Midstream cultures voided from cystoscopy table in 15! females with %terile suprapuhbic bladdetaspiratton% 1'I1; (Rcproduced by permixson of the authors and The Williams and Wilki tl Co. puhhbshers
For normal use, a midstream specimr.en after the patient
cleanses the perineum woulc seem to be the best method if the
-atient is reliable. Results should probably be confirmed by
secona specimen. If patient displays poor hygiene or is unableto follow instructions, a midstream collection following a perinealscrub by a nurse woula be advisable. A suprapubic needle aspira-tion wouli be a reasonable alternative and should be considered incases where the diagnosis is questionable by other means.
Prc;cni (.,,ncepts. I'ol 11" No 9. September 1971
A I

806
Urinary Tract Infection - Ornger
In determining the significance of a colony count, despitethe care (or lack of it) vith which the specimen is collected,one should be cognizant of the type of organisms cultured be-cause lactobacilli, streptococci (except enterococci), andstaphylococci (other than in diabetic patients) are usuallycontaminants. Such organisms when present in large numbersgenerally signif.y a poorly collected specimen and call foranother carefully obtained specimen. Some pitfalls must alsobe avoided which might falsely lower a significant urinarybecterial count, such as antibiotic therapy, hydration, frequencyof voiding, fastidious organisms, and contamination of the speci-men by soap.
Significance of Urinary Tract Infections
The incidence of bacteriuria in various population group3 iswell-established. It varies from four percent in males seen inthe medical outpatient department to almost 100 percent in patientswith indwelling catheters for over 96 hours. /9/
The rarity of bacteriuria in young males has been documentedby Kunin's work /5/ in which he reported only two positive culturesin 7,731 boys and young men, 1,116 of whom were between the ages Df15 and 29 years.
To enable one to estimate prognosis and judge the effect oftherapy, urinary tract infection has been conveniently divided intofour categories /6/: (1) uncomplicated acute urinary tract infec-tions, (2) complicated acute urinary tract infections, (3) asyrrpto-matic bacteriuria of unknown duration, and (4) chronic bacteriuria.
Acute urinary tract infection may often be self-limited butshould be treated because in a few instances it is followed bychronic bacteriuria. With repeat episodes of infection a thoroughevaluation should be undertaken and all young men should have acomplete urologic evaluation at the time of their first episode.Complicated urinary tract infections are acute episodes and astructural abnormality is present. The infection dill not usuallybe cured until the anatomic defect is corrected.
Present Concepts. Vol I V No 9. Septcm ber 19 71

Urinary Traci Inkcuon - Ginger
Asymptomati c bacteriuria is usually a problem of femalesanti a careful history will often reveal previously undescribedsymptomns of urinary tract infection. A number of these patientswill alscz go on to develop subsequently symptomatic infections.Chronik bacteriuria means persistent bacteriuria with repeatedsymptomatic intervals interspersed with asymptomatic intervals.Many of these patients have an associated obstructive uropathy.These infections are often resistant to treatment for a numberof reasons including resistant bacteria, obstruction, renalcalculi (which are a constant reservoir of infection), emergenceof antibiotic-resistant mutants, and an environment unfavorableto antibiotic action in the renal parenchyma. The possibilitythat local and humoral mechanisms in the kidney are not favorableto eradication of the infection may als account for the failureof adequate treatment.
The Danger of Chronic Infection
It is an inherent quality of physicians which makes themwant to treat and eradicate any pathologic condition. Thepresence of asymptomatic or chronic bacteriuria is a primeexample of such a situation, but workers in this area are havingdifficulty jeciding whether or not the mere presence of bacteriain urine is (cangerouz.
There is no indication that chronic bacteriuria ooes anypermanent damage to the u~rethra or to the bladder, however, agreat deal of controversy revolves around whether or not chronicbacteriuria leads to chronic pyelonephritis. The controversy ismade almost unresolvable by a complete lack of agreement on adefinition of pyelonephritis as reflected in the comment byPetersdorf and Turck /6/:
Nephrologists tend to equate pyelonephritisa disease characterized predominantly by tubulardysfunctlion that eventuates in uremia; urologiststhink of pyelonephritis in terms of obstructiveuropathy and vesicoureteral reflux as forerunnersof infection; pediatricians think of pyelonephritisas a disease associated with congenital abnormalitiesthat lead to repeated infections, failure to thrive,
nand renal insufficiency; anq pathologists are stillstruggling witn the problem of how to define the
P'resecnt Con, ('p . i',1 It' No 9. Scpicinber 1971

fIlrmalr"rr Ira l~t I ie ,,new (';,Pjgg€'r
,Jisease morphologically and to establish a rela-
tionship between a specific histologic pictureand a variety of pathogenic stimuli, includingeialgesic ingestions, irradiation, potassiumdepletion, hypertension, and infection.
It _s known that a large percentage of pregnant womenwith untreated bacteriuria will develop acute pyelonephritis.Savage et al /7/ reported that 26 percent of those untreatedversus zero percent of the treated women in a double blindstudy developed acute pyelonephritis before the terminationof the pregnancy. Therefore, a strong recommendation fortreatment of bacteriuria in pregnancy is made especially toprevent acute pyelonephritis. An association with prematurity,perinatal death, and toxemia has been suggested, but this demanosfurther stuay. /7,8;
Studies /9-11, have shown that approximately 50 percent ofpatients with recurrent bacteriuria have culturable bacteriaobtainable from the ureter. Renal pelvic bacteriuria has beentaken by many to mean that this is consistent with chronicpyelonephr. tis, but this has never been proven. Stamey and Pfau /1'prefers to call this "pyelitis".
There is a defect in tne concentrating ability of thekidney in chronic pyelonephritis. TABLE III. A similar defecthas been demonstrated in cases of renal bacteriuria and, moreimportantly, this defect existed only on the bacteriuric sidein patients who did not have renal bacteriuria bilaterally.This concentrating aefect improves following eradication of thebacteriuria. '12, Some people consider this evidence for chronicpyelonephritis, however, thi's is merely '"guilt by association".According to Stamey ana Pfau 11, no one has proven that bacteriain the renal pelvis lead to chronic destruction of renal tissue.Both chronic pyelonephritis and pelvic bacteriuria could cause adefect in concentrating ability.
Hemagglutination studies demonstrated higher titers of anti-bodies to bacteria in cases of acute pye~onephritis than they doin cystitis. Tne persistence of antibody titers is also observedin patients with chronic pyelonephritis from whom bacteria carx.r.tbe cultured. /7,13Y Guttman et al /14/ sl.owed that ir 57 patientswith sterile urine and chronic pyelonephritis, 11 had bacterial
Preseni %onccpts. Vol I V N., 9. September 1971

I IIIIaii I" Iu I /fle it,. m f,11yr'
vnrlanits in tieir urine. These variants which are i-'fi~uittU) ulture ,ioul - explain the existence of titers In patientswithout culturable bacteria but whether or not this is relatedto chr')nic pyelonephritis is yet to be proven.
TABLE Ill
CONCENTRATING ABIUfY IN MiLLIOSMCLES*
Right Kioncy Left Kidne,
BLADDERBACTERIURIA 936.1 918
infe-ted Kidney Non4nfectedi ~K~dney .
RENALBACTERIURMA 675 875
Initial AfterIrradication
AFITERIRRADICATION
OF INFECTION 73 !?62
"Adapted irom Ronald. et al: Ann Intern 3mcd 70:723-733, 1969
Stamey an: Pfau /1 believe that the only way to determinethe existence of pyelonephritis is by intravenous urograms thatshow :iestruction of the renal cortex. A recent intravenouspyelograph stuoy in two parts, /15,16/ done in Wales showed noevinence of chronic progressive pyelonephritis in 93 women with"chronic bacteriuria, 50 percent of whom were over the age of 45years. Aoki et al /17/ showed by immunofluorescence the presencein the kidney of bacterial antigen in six of seven patients with"a bacterial" pyelonephritis. Again there is no proof that thisleads to chronic pyelonephritis. A point against its leading tochronic pyelonephritis was mace by Sanford and Barnett /18/ whenthey showed that the existence of antigen following acute pyelo-nephritis in rats oid not leao to progressive scarring and lossof tissue.
Even though bacteriuria is ten times more common in fer.alesthan in males, this sexual predominance is not seen in chronicpyelonephritis. This woulo point away from bacteriuria as a
Presciit Concepts. Vol i F No 9. Septenzber 1971

Srnnarr Tract infec'tin - Conger
cause of chronic pyelonephritis. /I/
Freedman /19! in an autopsy review, found 64 cases ofchronic, nonobstructive pyelonephritis. Only 15 of these casesoied with uremia, and of these 15 only one had a history ofurinary tract infections during life, and only two had positivecultures prior to the onset of uremia.* Fourteen of the 15,however, had a history of other disease predisposing to renaldisease.
COMMIJNT
The majority of the current evidence points toward thefact that bacteriuria has little to do with the development ofchronic renal disease, however, future work shoula always beconsidered with an open mina.
*1ltt% might ,uggc-t that "ahactcnal'" pyclonephnlt. i.e. an immunologic phenomenon. is an Important
factoTr JJI)
References
I. Stamey TA, Pfau A: Urinary infections: A selective reviewand some observations. Calif Med 113:16-35, 1970
2. Kass EH: Asymptomatic infections of the urinary tract.Trans Amer Ass Physicians 69:56-63, 1956
3. Turck M, Gotte B, Petersdorf RG: IlTe urethral catheter andurinary tract infection. J Urol 88:834-837, 1962
4. Kass EH: The role of asymvpt----ic bacteriuria in thepathogenesis of pyelonephritis. Biology of Pyelonephritis,Quinn EL, Kass EH (eds). Boston: Little, Brown and Company,1960, pp 399-412
5. Kunin Cy, Zacha E, Paguin AJ: Urinary tract infection inschool chilcren. I. Prevalence of bacteriuria and associatedurologic findings. New Eng J Med 266:1287-1296, 19)62
6. Petersdorf RG, Turck M: Some current concepts of urinarytract infections. Disease-a-Month December 1970
Prcsent Concepts. Vol IV No 9. September 19 71
' ,I --. " D .- 4
.- | , - ' I - -r - •' '-~ -

O man- Ii, I hilt, ii-it t i,,vr
7. Savage EW. Haji SN, Kass EH, et al: Demographic anoprognostic characteristics of bacteriuria in pregnancy.Medicine 46:385-4o7, 1967
8. Wilson MG, Hewitt WL, Monzon OT: Effect of bacteriuriaon the fetus. New Eng J Med 274:1115-1118, 1966
9. Turck M, Anderson KN, Petersuorf RG: Relapse and re..n-fection in chronic bacteriuria. New Eng J Med 275:70-77,1966
10. Turck M, Ronald AR, Petersdorf RG: Relapse ana reinfec-tion in chronic bacteriuria. II. The correlation betweensite of infection and pattern of recurrence in chronicbacteriuria. New EngJ Med 278:422-427, 1968
11. Stamey TA, Govan DE, Palmer JM: The localization andtreatment of urinary tract infections: The role of bacter-icidal urine levels as opposed to serum levels. Medicine44:1-36, 1965
12. Ronald AR, Cutler RE, Turck M: Effect of bacteriuria onrenal concentrating mechanisms. Ann Intern Med 70:723-733,1969
13. Carter MJ, Ehrenkranz J, Burns J, et al: Serologic responseto heterologous eschericzhia sero groups in women withpyelonrphritis. New Eng J Med 279:1407-1412, 1968
14. Guttman LT, Turck M, Petersdorf RG, et al: Significance ofbacterial variants in urine of patients with chronic pyelo-nephritis. J Clin Invest44:1945-Yf52. i5kc
15. Sussman M, Asscher AW, Waters WE, et al: Asyn.ptomatic.significant bacteriuria in the nonpregnant woman. I. De-scription of population. Brit Med J 1:799-803, 196.
16. Asscher M4W, Sussnan M, Waters WE, et al: Asymptomati:"significant bacteriuria in the nonprtwuant wom.n.iI. Response tu trxatnient anc follow up. Brit Med J
17. Aoki S, imamrura S, Aok. M. et al: "Abacterial" andbacterial oye]oneohrAitis. New Eng J !.ied 281:1375-13F2-1961
18. Sanford JFP, Barnett JA: Imm.unologic studies in urinarytract in..ctions. Prognnostuz and jiagnostic. JAMA1 ýe: 57-5c2, lt)c5
l9. Freed,.an LR: Chroni- pyeineph-ritis at autopsy. AnnIntern Med 66:697-7i0, .9:7
Present; ('Cnrpis. Vol I V .%'(, 9. S, p.rm her I fY71
% -~- -
b,!:
Iýriw
__ 00 ý Wil
t oot2510oo oe0 G0 00 C- 0
0Do0 003 /13Do ~ 00 0 0 1
0 0030
000300C,,r Z4) 0 0 C'AID~ 00 00 000
0~ 00 003000000
022A ()oo 0 0 0 3
000cI00 300 1, 0
"-".-'IfOe~ IALSI~TRANIN i ~ AS0IEoo.
0 0 3Prcic'q,1 L 6 i' 0 aV No 9 C 0 0~b 7
UP c 000 00
0 0 ;) 0 j

MANA(;FMEN'! 01: ACU I".- INT(OXICATI,)N WrITiH BRBITURATI'S,IHIERO(IN AND L.SD)
I.T(: Janics 11. Shinabergcr, MC USAR
BARBITURATE INTOXICATION
Barbiturates remain the drug molt often reported as thecause of poisoning in adults in tha United States. A fairlyrecent estimate suggests there are more than 15,000 hospitai-ntions and 1,000 deaths annually from such intoxications.
Because of the current drug culture evolving in the countryand particularly in our own commity, this is probably agross underestimation. In addition to the former classicalcase of acute massive ingestion for suicidal reasons, a nowclass of overdose problem is being seen in greater numbers.These are the chronic barbiturate abusers who regularly take15 to 20 "reds" or "yellows" per day and who are seen as acute"overdose problems when they abruptly increase their intake to30 or 40 capsules in a given day, either through despondencyor actual error in judgment in calculating the dose requiredto produce the desired effect. Presumably because of toleranceor enzyme induction, thesn intoxications tend to take a mildercourse, but their treatmint is complicated by the possibilityof the potentially lethal barbiturate withdrawal syndrome ifthe background of chronic abuse is unrecognized. The signsand symptoms are given in TABLE I.
T;catment
Necessary treatment for mild intoxications as in recentingestion or low dosage may be only induction of emesis (ifthe patient is alert) or lavage and observation if the patientis only mildly depressed. Enesis may be induced by injectionsof apomorphine, 0.07 m/kg of body weight. Emesis is moreeffective if the stomach contains liquid. Nalorphine shouldbe immediately accessible in the event that apomorphine produces
*(b•zf. Iictno t,,i I.I*: 'nit. %%ad.-wozth 'cWtcramn Adininvtaration |loipltal. I o% Ang- cCalifotnta
lPrcst. (',,, c•'i. I'ol I I \ 9. .S',ep) l ber 1Q1-

s14
SManalzc'mc'n: ,:ImDrg Alpine ab rg'
es -7.
> >
a0 -
7" •g - -<-0". ,, -••8 I : -
~ I
E n
72 9
"s E
<<
Vn i 2 oo eicne (-

V hll -fll, /I/, /hi t.-1 I 'lttt;" |/ 1t,:r hl l y I~
respiratory depression. If lavage is done, it will be mosteffective if 2-3 liters of saline containing a slurry of atleast 1 gm/kg activated charcoal (powder, not tablets) isused. The charcoal quantitatively absorbs the drug and pre-vents "s absorption by the gaatrointestinal tract. Followinglavage )-90 ml of castor oil is instilled into the stomach.The lipid soluble drug is selectively dissolved into the nonabsorbable oil which remover the remainder of the drug fromthe bowel. In the presence of even minimal depression, oilinstillation should not be done unless a cuffed nasotrachealtube is in place and inflated.
Any patient who will tolerate an endotracheal tuberequires it. The cuff should be deflated 15 minutes every2 hours, and tracheobronchial suctioning with aseptic tech-nique should be faithfully performed as frequently as neces-sary. With any degree of hypoventilation and certainly ifthe pO2 is 70 mm Hg or less, mechanical assistance should beprovided. A head down position and frequent turning helpprevent atelectesis. With prolonged coma, aspiration orbacterial pneumonitis is comon and tests for this should befrequent. Gram-negative infections are common. A simpleoxygen saturation test has recently been described which willdetect aspiration pnezmonia before clinical or radiologicalfindings are present. Maintenance of adequate airway andventilation is the single most important aspect of sedativeoverdose management.
tlypotension
Barbiturates and most other sedatives produce vaso-dilation and relative hypovolemia. Surprisingly large amountsof plasma expanders may be required to produce a normal centralvenous pressure (CVP), tissue perfusien and glomerular filtra-tion. Vasopressors, preferably with inotropic action shouldbe used rarely and only when it is certain that effectivecirculating plasma volume is normal. If renal perfusion isadequate blood pressures somewhat lower than those ususelyconsidered normal are acceptable in the comatose, totallyrelaxed patient.
I'rcent (',,n cpts. 'ol I" .V,, '. Scpieinbcr 19 7i

Maniap'm,'nt it] h rug Abuu," .Shinaherle'
I ly polhcriulna
I Rewarming to prevent ventricular fibrillation is indicatedif body temperature falls to 32 C.
Forced Diuresis
With the exception of phenobarbital, the barbiturateshave pK values higher than physiological pH and are not ex-creted in the active form in significant amounts in the urine.The excretion of phenobarbital (pK 7.2) can be significantlyincreased by forced alkaline diuresis provided the urinary pHis maintained above this level. The excretion of short-actingbarbiturates can be increased about 20 percent by forced os-motic diuresis. The increased clearance is related to theincreased urine flow. Since flow rates above I00 ml/hr arerequired, careful attention to replacement of electrolytes isnecessary. An additional 40 ml/hr should be given for insen-sible loss (less if on respirator, more if fever is present).
Dialysis
Peritoneal dialysis is relatively inefficient for removalof barbiturates, but is occasionally necessary in children.Hemodialysis should be considered when the following factorsare present: (1) the patient is elderly, (2) there are com-plicating diseases (3) failure to improve with conservativemanagement, and (4M blood levels are 3.0 mg/lO0 cc short-actingor 7 mg/•l00 cc long-acting. Hemodialysis is somewhat lesseffective for short-acting barbiturates and dialysis withlipid dialysate may be considered. If dialysis is elected,careful attention to all of the general supportive measuresmust be maintained throughout the procedure.
Psychiatric Assistance
The most important time for the psychiatric evaluationand therapy is imediately after awakening.
Present Concepts. Vol IV No 9. September 1971

--
(71RONlCBRAR111l7 RA 72EA/A BUE
TIlE BARBITURATE ABSTINtENCE SYNDROMI
Chronic barbiturate abuse has become extremely widespreadand a special note regarding the barbiturate abstinence s-drome is included because of its medical importance. Barbi-I: turic acid was synthesized in 1863 and barbital was intro-duced into medical practice in 1903. Chronic intoxicationand convulsions upon withdrawal were described in Germany asearly as 1905. Subsequent reports of barbiturate dependencywent unheeded until the studies of Isbell and co-workers in1950 who did controlled experiments in man which demonstratedconclusively that the abuse of barbiturates can induce physicaldependency. The intoxication syndrome resembles alcoholicintoxication and is characterized by lethargy or somnolence,wide-based staggering gait, nystagmus on lateral gaze, slurredspeech, impaired judgment, and emotional lability. Theabstinence syndrome is far more serious than the abstinencesyndrome of opiate addiction. Not only are convulsions andtemporary psychosis liable to develop, but death may occur.Minor abstinence manifestations inciludýe apprehension, muscularweakmess, tremulousness, postural fainting due to posturalhypotension, gastrointestinal disturbances and musculartwitching. Major manifestations include one or all of thefollowing: generalized tonic-clonic convulsions, psychoticdelirium, fever, and death. Up to 100 mg of pentobarbitalper day can be takea safely without developing major absti-nence manifestatior". Above that level, the percentage ofincidence of major withdrawal abstinence syndrome variesdirectly with increasing daily dose. Convulsions may devclopas early as 16 hours, but usually occur on the second or thirdday of withdrawal. The development of temperature above 101 Fduring withdrawal is an indication for vigorous treatment.Diphenylhydantoin has never been demonstrated to offer pro-tection from barbiturate withdrawal seizures. Abrupt with-drawal from meprobamate, glutethimide, methyprylon, ethinamate,ethchlorvinyl, chlordiazpoxide, and diazepam has been reportedto result in grand mal seizures, psychotic behavior, or both.
i'rcewni (0',l cpi . I'e,, I " .V, . Scpicrt •hcr 1 () '

+• •l~Alllii•+gltmcll v! I)riig :3 Jflixe SI•ihlrnh'rg',r
Recently Smith and Wesson2 have proposed a safe methodfor barbiturate withdrawal. Basically, the daily dose ofbarbiturate, which is practically always secobarbital orpentobarbital, Ls estimated by history from the abuser. Thisis usually from 500 to 3000 milligrams. Each 100 mg of shortacting barbiturate is equated to 32 mg of phenobarbital andthis is given as total daily dose divided into four doseswhich are somewhat higher in the evening than in the mornings.After two days of stabilization and close observation, thetotal daily dose is decreased by 30 mg per day. If symptomsdevelop during withdrawal an injection of 200 mg of pheno-barbital is given immediately and the decrease in dosage isdiscontinued until withdrawal symptoms have subsided.
kab, il 11. Alschu! S. Kornetsky C. et al- Chronic barbiturate intoxication. Ar cpcrimcntal study.Arch NcurolPs'c¢hiat 64: 1-28. 1950
2 Smtth DE. Wesson DR Phcnobarbstol technique for treatment of barbiturate dependency.Arch Gen Psvchiat 24:56-60. 1971
HEROIN OVERDOSE
Severe overdose may be almost instantly fatal and is notamenable to treatment. Overdose produces pinpoint pupils,depressed blood pressure and respiration, coma, shock, andpulmonary edema. Diagnosis usually easy from "tracks" orevidence of "skin popping". The signs and symptoms are listedin TABLE I.
Treat me nt
Immediate injection of nalorphine 2-10 mg (if no veinsare usable, inject into sublingual venous plexus). Repeatas often as necessary to prevent recurrence of apnea or hypo-tension. Response is judged by dilation of pupils. Hypotensionmay require plasma expanders and pressors. These patientsshould be observed for at least eight hours because pulmonary
Pre,'t Conn'epts. V,4 11' No 9. Sepie'mber 1971

* ------- --
ihtnagwitcni - J I)r ol A1 Alpme - .•,'h'rixr
edema may appear later and be fatal. Treatment consists ofdiuretics, oxygen, tourniquets, and occasionally digitalis.The precise etiology of the pulmonary edema is unknown.Theories include: (1) overdose of the common adulterantquinine, (2) particulate thrombo-embolism, (3) hypoxia,and (4) anaphylactic reaction with lung as target organ.Addicts are also susceptible to staphylococcal pneumorna andendocarditis. It should be remembered that the nalorphineused in treatment may produce an abrupt withdrawal syndromewhich may require treatment.
LYSERGIC ACIi) DIETHYLAMIDE (LSD)
Making a diagnosis on basis of history of 1SD ingestionis risky since much of what is sold as LSD is actually phen-cyclidine (sernylan). strychnine, amphetamines and atropine.TABLE I includes typical signs and symptoms. LM and otherhallucinogens induce a hypersuggestible state that can beexploited by reassurance. Hyperactivity can be controlledby "talking the patient down". Urge the patient to keep hiseyes open since this usually decreases the panic and hallu-cinations. Although the phenothiazines are useful whensedation is necessary, their use can be hazardous when ananticholinergic drug has been mixed with the I3D as severehypotension can be produced. TABKE I. Excessive drynessof the mouth and absence of sweating are clues to possibleadulteration with anticholinergics. If an "anticholinergiccrisis" is produced by treatment with phenothiazines, 2-4 mgphysostigmine given Intramuscularly and repeated as often asnecessary may reverse the crisis. It may be safer to useparenteral LibriumQ or Valium®) and to rely heavily on reas-surance.
I'r'•vCni ( .,nc epi. ',,/I I 1 , '. Scp!cni ,'r j i 71

DxONORS
Present ('wmccpls. Vol It" No 9. September 1971

ACKNOWIEDGEMENTS
The splendid dedicatc. efforts of Mrs. Marian Anderson, secretary to the Chief,(General Medicine, Mrs Lottie Applewhitc, medical editor, and Mr. Ion Stockton,illustrator, deserve sp r;ial recognition and thanks. This edition would not havebeen possible without their assistance and determination to produce a qualitypublication. REC