Lowering Emissions and Costs Associated with Urban Deliveries Utilising Advanced VRLA Technology

Benefits of pharmacist care in hypertension in Canada
IMPROVING HEALTH AND LOWERING COSTS

2 Canadian Pharmacists Association
Broadstreet301-343 Railway StreetVancouver, C.-B. V6A [email protected]
The following report is based on peer-reviewed research published in the Canadian Pharmacists Journal titled Cost-eff ectiveness of pharmacist care for managing hypertension in Canada and authored by Carlo Marra, PharmD, PhD (lead author); Karissa Johnston, MSc, PhD; Valerie Santschi, PharmD, PhD; and Ross T. Tsuyuki, BSc(Pharm), PharmD, MSc, FCSHP, FACC.
Carlo Marra, B.Sc.(Pharm.), Pharm.D., Ph.D.Carlo is a Professor and Dean in the School of Pharmacy at the University of Otago in Dunedin, New Zealand. He is trained as a health services researcher with a Ph.D. in health outcomes. He is very interested in investigating the value for money proposition for pharmacist care of patients and the clinical outcomes of these services. He has published more than 225 peer-reviewed articles and has presented at a similar number of conferences.
The report was prepared by Broadstreet Health Economics & Outcomes Research.
Karissa Johnston, PhD Karissa is a Principal at Broadstreet HEOR, adjunct professor at Memorial University as well as an epidemiologist with 15 years of experience in the analysis of health data, and seven years of experience with consulting in health economics and outcomes research studies. Karissa completed a Master’s degree in Statistics, and a PhD in Epidemiology at the University of British Columbia. As a consultant, she has conducted and overseen studies employing a wide breadth of methodological approaches, including study design, database analysis, retrospective chart review, discrete choice experiment, pharmacoeconomic and budget impact modelling, and systematic literature review and evidence synthesis. Karissa has published peer-reviewed articles in disease areas including oncology, HIV, renal disease, premature birth, cardiovascular disease, and infection.

3Canadian Pharmacists Association
Introduction
Worldwide impact of hypertension
Worldwide, hypertension is the number one risk factor for disease and premature mortality.1 With around a quarter of the planet’s population estimated to have high blood pressure (about 1.13 billion people),2 it is responsible for about 7.5 million deaths annually3 and is associated with approximately 10% of direct medical costs globally.4 Adding to the gravity of this situation is the fact that treatment and control of hypertension are poor, with over 40% of patients having uncontrolled blood pressure.5 Taken together, these facts point to a considerable gap in hypertension care, a gap that requires new thinking to address this important and far-reaching public health problem.
Benefits of pharmacist intervention
The WHO’s Global Action Plan for the prevention and control of non-communicable diseases 2013–2020 specifies, as one of its nine voluntary targets, a 25% reduction or containment of the prevalence of raised blood pressure. Intervention by pharmacists in hypertension care could make a significant contribution to that goal and can have meaningful results both in terms of benefits to health and cost effectiveness. Clinical trial evidence has clearly demonstrated the advantages of pharmacist intervention, including education, consultation, and/or prescribing, which can lead to a reduction in blood pressure. Beyond that, as hypertension is a major risk factor for cardiovascular disease, kidney failure and death, there is considerable opportunity to improve outcomes by preventing the onset and/or progression of these diseases by reducing the care gap in hypertension control.

4 Canadian Pharmacists Association
Hypertension in Canada
In Canada, around 5.3 million people are living with hypertension.6 Prevalence in 2015 was reported to be 24% in adults and a third of those cases are not adequately controlled.7,8
Prevalence is also expected to increase. Research from the US suggests that by 2030, hypertension prevalence will increase by 7.2% from 2013 numbers.9,10 In Canada, the situation is likely to be, at best, only slightly less severe.8 While we are faring better than most countries with regards to both the prevalence and control of high blood pressure, improving on those numbers would have real benefits both in terms of lives saved and improved, as well as in reduced healthcare costs.
Costs and burden of hypertension
The burden of hypertension on society is enormous both in health and economic terms. Evidence from the Institute for Health Metrics and Evaluation shows that, worldwide, high blood pressure was second only to dietary risks as cause of death in 2010.12 It is responsible for 50% of the overall risk for heart disease and stroke,13 as well as 28% of kidney failure.14 It is also a contributing factor for dementia. Globally, it costs society more than $370 billion (2001 US dollars) per year, with indirect costs relating to premature death and time missed from work estimated to be about 10% of the world’s health expenditures.4 Being able to improve these numbers even slightly would result in countless lives saved and improved and millions—perhaps even billions—of dollars saved.
17 %
21 %
26 %
35 %
2002
2008
2030
Hypertension in Prince Edward Island
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
16 %
19.6 %
24 %
33 %
2002
2008
2005
2030
Hypertension in Canada
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
19 %
23 %
28 %
39 %
2002
2008
2030
Hypertension in Nova Scotia
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
22 %
27 %
33 %
45 %
2002
2008
2030
Hypertension in Newfoundland andLabrador
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
18 %
22 %
26 %
36 %
2002
2008
2030
Hypertension in New Brunswick
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
15 %
19 %
23 %
31 %
2002
2008
2030
Hypertension in Quebec
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
16 %
20 %
24 %
34 %
2002
2008
2030
Hypertension in Ontario
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
17 %
20 %
25 %
34 %
2002
2008
2030
Hypertension in Manitoba
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
17 %
21 %
25 %
35 %
2002
2008
2030
Hypertension in Saskatchewan
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
16 %
19 %
24 %
32 %
2002
2008
2030
Hypertension in Alberta
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
15 %
18 %
22 %
30 %
2002
2008
2030
Hypertension in British Columbia
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
15 %
19 %
23 %
31 %
2002
2008
2030
Hypertension in Yukon
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
14 %
18 %
21 %
29 %
2002
2008
2030
Hypertension in NorthwestTerritories
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
17 %
20 %
25 %
34 %
2002
2008
2030
Hypertension in Nunavut
Age-standardized prevalence of diagnosed hypertension among adults aged 20 years and older
01 200501
200501200501200501
200501200501
200501 200501 200501
200501 200501
200501
200501
2002,11 2008,11 2015,7 2030 projection based on linear extrapolation of observed increases over time.

5Canadian Pharmacists Association
Opportunities for Pharmacist Intervention
How pharmacists can help
For most people, it is far easier to see and speak to a pharmacist than a physician. In fact, on average, people see their pharmacist 5 to 7 times more often than they see their family doctor.15 Pharmacists are highly accessible primary healthcare providers and ideally placed to address the care gap in hypertension management. A number of studies have already demonstrated how effective their intervention can be in this area. To date, pharmacist interventions in hypertension have largely been focused on patient education and counselling, recommendations to physicians about therapy management (including drug related problems, recommendations for changing pharmacotherapy and development of a care plan) and direct medication management with the patient (including monitoring with adjustment or change in medication).
We have studied a number of scenarios for what we term partial scope pharmacist intervention to full scope intervention. In the latter case, pharmacists make use of their full scope of skills for possible interventions, including prescribing. We found that all scenarios resulted in health improvements and cost savings when compared to current practice.
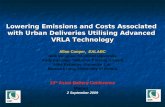
Full scope intervention includes the assessment of and counselling about cardiovascular risk and blood pressure control, reviewing antihypertensive medications, prescribing/titrating of drug therapy, laboratory testing, and follow up visits with the patient. This type of intervention has been shown to result in an average 18.3 mmHg reduction in systolic blood pressure.16
Partial scope intervention includes combinations of patient education, counselling, referrals, diagnostics, and interventions. Notably, in this case, the pharmacist may not be able to prescribe. These types of interventions have been shown to lead to a lowering of both systolic and diastolic blood pressure, with an average systolic blood pressure reduction of 7.6 mmHg.17
Pharmacist Intervention
Reduction in Systolic Blood Pressure
7.6 mmHg
18.3 mmHg
Partial scope
Full scope

6 Canadian Pharmacists Association
Purpose of the analysis
While there is good evidence available for the health benefits of pharmacist intervention in hypertension management, including a recent clinical trial conducted in Canada,16 as well as a combined analysis that looked at 39 trials internationally,17 there has been, until now, a lack of research done on the economic value of this type of intervention, particularly in Canada. The analysis we have commissioned sought to extrapolate the observed benefits in trials of pharmacist intervention in blood pressure control in order to project the potential health impacts and cost effectiveness of pharmacist interventions over a longer time period.
We used a cost-effectiveness model to look at potential differences in long-term cardiovascular and kidney failure outcomes when different levels of blood pressure reduction were achieved through several potential levels of pharmacist intervention. The model takes into account various health outcomes, costs and quality of life. Costs considered include direct medical costs, as well as the costs associated with implementing the pharmacist intervention strategy. In general, we examined whether the intervention would decrease cardiovascular events and kidney failure; the magnitude of differences in survival and quality of life that could be achieved; the effects on direct medical costs and the cost-effectiveness of the intervention.
About the model
The model, which has been peer-reviewed and published in the Canadian Pharmacists Journal (C. Marra, K. Johnston, V. Santschi, R. Tsuyuki. Cost-effectiveness of pharmacist care for managing hypertension in Canada), was developed to compare two general scenarios for the relevant population.a For the first scenario, we consider the costs and health benefits of continuing with usual care, with limited opportunity for pharmacists to intervene in the care path. The second scenario analyzes the costs and health benefits of pharmacist intervention, with the magnitude of the impact dependent on the specific details of the type of intervention considered. The base case for the model examines the costs and health benefits of treating an eligible population over the course of 30 years,b but it is adjustable and allows other timeframes and health factors to be considered.
The model assumes that under usual care blood pressure stays consistent, as there is no increase in intervention. Without increased intervention, no decrease in blood pressure could be expected (in reality, this is a conservative assumption as blood pressure tends to get worse over time). The cost assumptions used for pharmacist intervention were based on six visits in the first year and quarterly thereafter.c In terms of costs of medicines, a
a. The population used in the model was based on the population of the clinical trial conducted by Tsuyuki et al, to reflect the typical population accessing hypertension care in Canada. The average age was 63.5 years and the population was fairly evenly split between men and women. Average systolic blood pressure was 149.5, with 78% of the population already receiving treatment for high blood pressure.
b. The assumed new incidence per year will be 75,000 cases (418,000 x 35% eligible x 50% assumed to access intervention; rounded slightly).9
c. Costs were set at $125 for the first visit and $25 for subsequent visits, which reflects the current fee schedule in Alberta.

7Canadian Pharmacists Association
conservative assumption was made that costs would increase by $30/month as a result of the intervention. This assumption is termed conservative because no difference in medication use was observed, on average, in clinical trials; pharmacists typically helped to optimize the medications that patients were already taking. In practice, the intervention group would likely have a reduction in physician visits for medication management, which would offset the additional pharmacist consultations, but this was not incorporated into the model—again, to be conservative.
Costs for cardiovascular disease and kidney failure were based on a review of published, peer-reviewed literature. ‘Background’ medical costs were set to the Canadian average.18
The trial testing the pharmacist intervention occurred over six months, and the model is based on the assumption that this intervention would continue to be effective in the longer term. The model allows for testing shorter and longer time horizons. It incorporates both conservative and optimistic estimates for a number of costs and benefits, including background medical costs, full and partial pharmacist intervention and a range of potential blood pressure outcomes.
For more detailed information on the different potential scenarios for and benefits from pharmacist intervention, we invite you to visit our website. The model discussed here has been set up as an interactive tool that allows users to explore changes in economic and health impact under different timeframes and health scenarios.
What the analysis demonstrates
The analysis shows a real and significant benefit from pharmacist intervention, both in terms of cost savings and health benefits when compared with usual care. In all analyses, the rates for cardiovascular disease and kidney failure are lowest with the full scope of pharmacist intervention and highest under the usual care regime. The results also highlight the relatively low costs of the program, particularly relative to the costs of treating cardiovascular disease or kidney failure.
Health Benefits
The analysis demonstrates a range of health benefits associated with pharmacist intervention in high blood pressure care. Previous research has shown that systolic blood pressure would be reduced by 18.3 mmHg with full scope pharmacist intervention.16 When this is applied to our analysis, in the base case, over 30 years, it is estimated that for every five people receiving the intervention, one cardiovascular event (defined as stroke, myocardial infarction (MIs), angina and heart failure) would be avoided and four years of life would be saved. When the eligible population receiving the interventiond is considered as a whole over 30 years of full scope intervention, this would result in the following when compared to usual care: 130,000 fewer strokes; 260,000 fewer MIs; 76,000 fewer cases of angina; 70,000 fewer instances of heart failure; and 1,800 fewer instances of kidney failure. It would also result in an additional 953,000 years lived when the health impact is analyzed across the population.
d. 930,000 individuals initiating in year 1, plus 75,000 new individuals per year.

8 Canadian Pharmacists Association
select region: for the NATIONAL report only (in Billions)CANADA
5 years 5 years
43805 CV events - full intervention67446 CV events - partial intervention86505 CV events - usual care
619 Kidney failure - full intervention786 Kidney failure - partial intervention803 Kidney failure - usual care407 Life years saved - full intervention183 Life years saved- partial intervention
36459354382 Costs - full intervention37320695929 Costs - partial intervention35215446042 Costs - usual care
10 years 10 years
208272 CV events - full intervention310631 CV events - partial intervention388254 CV events - usual care
1600 Kidney failure - full intervention2030 Kidney failure - partial intervention2073 Kidney failure - usual care
16159 Life years saved - full intervention7104 Life years saved- partial intervention
83620736584 Costs - full intervention88203889383 Costs - partial intervention85928397235 Costs - usual care
15 years 15 years
385486 CV events - full intervention556586 CV events - partial intervention678375 CV events - usual care
2770 Kidney failure - full intervention3507 Kidney failure - partial intervention3578 Kidney failure - usual care
88298 Life years saved - full intervention37982 Life years saved- partial intervention
135980818604 Costs - full intervention144742859705 Costs - partial intervention142317255130 Costs - usual care
20 years 20 years
567009 CV events - full intervention797271 CV events - partial intervention953225 CV events - usual care
4059 Kidney failure - full intervention5127 Kidney failure - partial intervention5220 Kidney failure - usual care
266658 Life years saved - full intervention111590 Life years saved- partial intervention
191497019262 Costs - full intervention204430771466 Costs - partial intervention201719547207 Costs - usual care
25 years 25 years
739211 CV events - full intervention1021093 CV events - partial intervention1206301 CV events - usual care
5386 Kidney failure - full intervention6777 Kidney failure - partial intervention6884 Kidney failure - usual care
572748 Life years saved - full intervention232618 Life years saved- partial intervention
247592336018 Costs - full intervention264217169291 Costs - partial intervention260946752957 Costs - usual care
30 years 30 years
899326 CV events - full intervention1230075 CV events - partial intervention1444065 CV events - usual care
6671 Kidney failure - full intervention8363 Kidney failure - partial intervention8477 Kidney failure - usual care
953485 Life years saved - full intervention376810 Life years saved- partial intervention
302109253447 Costs - full intervention321853422664 Costs - partial intervention317815726575 Costs - usual care
30 years-15706473128 Economic outcome - full intervention4037696090 Economic outcome - partial intervention
1,44
4,06
51,
230,
075
899,
326
5 years 10 years 15 years 20 years 25 years 30 years0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
Time horizon
Cardiovascular events(stroke, MI, angina, heart failure)
Usual carePartial interventionFull intervention
8,47
78,
363
6,67
1
5 years 10 years 15 years 20 years 25 years 30 years0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
Time horizon
Kidney failure events
Usual carePartial interventionFull intervention
7,104
111,590
376,810
16,159
266,658
953,485
10 years
20 years
30 years
Timehorizon
Growth in saved life-years
Full intervention
Partial intervention
317,
816
321,
853
302,
109
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative cost of hypertension (MILLIONS)
Usual care
Partial intervention
Full intervetion$4,037.7
-$15,706.5
-$20,000
-$15,000
-$10,000
-$5,000
$0
$5,000
$10,000
30 years
Economic outcome of pharmacist intervention (MILLIONS)
Partial intervention Full interventionSavi
ngs
Cost
s
318
322
302
$0
$50
$100
$150
$200
$250
$300
$350
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative medical costs for individuals with hypertension (BILLIONS)
Usual care
Partial intervention
Full intervention$4.0
-$15.7
-$20
-$15
-$10
-$5
$0
$5
$10
30 years
Economic outcome of pharmacist intervention (BILLIONS )
Partial intervention Full intervetion
Savi
ngs
Cost
s
use BILLIONS graphic ONLY for canada AND MILLIONS FOR PROVINCES.
select region: for the NATIONAL report only (in Billions)CANADA
5 years 5 years
43805 CV events - full intervention67446 CV events - partial intervention86505 CV events - usual care
619 Kidney failure - full intervention786 Kidney failure - partial intervention803 Kidney failure - usual care407 Life years saved - full intervention183 Life years saved- partial intervention
36459354382 Costs - full intervention37320695929 Costs - partial intervention35215446042 Costs - usual care
10 years 10 years
208272 CV events - full intervention310631 CV events - partial intervention388254 CV events - usual care
1600 Kidney failure - full intervention2030 Kidney failure - partial intervention2073 Kidney failure - usual care
16159 Life years saved - full intervention7104 Life years saved- partial intervention
83620736584 Costs - full intervention88203889383 Costs - partial intervention85928397235 Costs - usual care
15 years 15 years
385486 CV events - full intervention556586 CV events - partial intervention678375 CV events - usual care
2770 Kidney failure - full intervention3507 Kidney failure - partial intervention3578 Kidney failure - usual care
88298 Life years saved - full intervention37982 Life years saved- partial intervention
135980818604 Costs - full intervention144742859705 Costs - partial intervention142317255130 Costs - usual care
20 years 20 years
567009 CV events - full intervention797271 CV events - partial intervention953225 CV events - usual care
4059 Kidney failure - full intervention5127 Kidney failure - partial intervention5220 Kidney failure - usual care
266658 Life years saved - full intervention111590 Life years saved- partial intervention
191497019262 Costs - full intervention204430771466 Costs - partial intervention201719547207 Costs - usual care
25 years 25 years
739211 CV events - full intervention1021093 CV events - partial intervention1206301 CV events - usual care
5386 Kidney failure - full intervention6777 Kidney failure - partial intervention6884 Kidney failure - usual care
572748 Life years saved - full intervention232618 Life years saved- partial intervention
247592336018 Costs - full intervention264217169291 Costs - partial intervention260946752957 Costs - usual care
30 years 30 years
899326 CV events - full intervention1230075 CV events - partial intervention1444065 CV events - usual care
6671 Kidney failure - full intervention8363 Kidney failure - partial intervention8477 Kidney failure - usual care
953485 Life years saved - full intervention376810 Life years saved- partial intervention
302109253447 Costs - full intervention321853422664 Costs - partial intervention317815726575 Costs - usual care
30 years-15706473128 Economic outcome - full intervention4037696090 Economic outcome - partial intervention
1,44
4,06
51,
230,
075
899,
326
5 years 10 years 15 years 20 years 25 years 30 years0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
Time horizon
Cardiovascular events(stroke, MI, angina, heart failure)
Usual carePartial interventionFull intervention
8,47
78,
363
6,67
1
5 years 10 years 15 years 20 years 25 years 30 years0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
Time horizon
Kidney failure events
Usual carePartial interventionFull intervention
7,104
111,590
376,810
16,159
266,658
953,485
10 years
20 years
30 years
Timehorizon
Growth in saved life-years
Full intervention
Partial intervention
317,
816
321,
853
302,
109
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative cost of hypertension (MILLIONS)
Usual care
Partial intervention
Full intervetion$4,037.7
-$15,706.5
-$20,000
-$15,000
-$10,000
-$5,000
$0
$5,000
$10,000
30 years
Economic outcome of pharmacist intervention (MILLIONS)
Partial intervention Full interventionSavi
ngs
Cost
s
318
322
302
$0
$50
$100
$150
$200
$250
$300
$350
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative medical costs for individuals with hypertension (BILLIONS)
Usual care
Partial intervention
Full intervention$4.0
-$15.7
-$20
-$15
-$10
-$5
$0
$5
$10
30 years
Economic outcome of pharmacist intervention (BILLIONS )
Partial intervention Full intervetion
Savi
ngs
Cost
s
use BILLIONS graphic ONLY for canada AND MILLIONS FOR PROVINCES.
select region: for the NATIONAL report only (in Billions)CANADA
5 years 5 years
43805 CV events - full intervention67446 CV events - partial intervention86505 CV events - usual care
619 Kidney failure - full intervention786 Kidney failure - partial intervention803 Kidney failure - usual care407 Life years saved - full intervention183 Life years saved- partial intervention
36459354382 Costs - full intervention37320695929 Costs - partial intervention35215446042 Costs - usual care
10 years 10 years
208272 CV events - full intervention310631 CV events - partial intervention388254 CV events - usual care
1600 Kidney failure - full intervention2030 Kidney failure - partial intervention2073 Kidney failure - usual care
16159 Life years saved - full intervention7104 Life years saved- partial intervention
83620736584 Costs - full intervention88203889383 Costs - partial intervention85928397235 Costs - usual care
15 years 15 years
385486 CV events - full intervention556586 CV events - partial intervention678375 CV events - usual care
2770 Kidney failure - full intervention3507 Kidney failure - partial intervention3578 Kidney failure - usual care
88298 Life years saved - full intervention37982 Life years saved- partial intervention
135980818604 Costs - full intervention144742859705 Costs - partial intervention142317255130 Costs - usual care
20 years 20 years
567009 CV events - full intervention797271 CV events - partial intervention953225 CV events - usual care
4059 Kidney failure - full intervention5127 Kidney failure - partial intervention5220 Kidney failure - usual care
266658 Life years saved - full intervention111590 Life years saved- partial intervention
191497019262 Costs - full intervention204430771466 Costs - partial intervention201719547207 Costs - usual care
25 years 25 years
739211 CV events - full intervention1021093 CV events - partial intervention1206301 CV events - usual care
5386 Kidney failure - full intervention6777 Kidney failure - partial intervention6884 Kidney failure - usual care
572748 Life years saved - full intervention232618 Life years saved- partial intervention
247592336018 Costs - full intervention264217169291 Costs - partial intervention260946752957 Costs - usual care
30 years 30 years
899326 CV events - full intervention1230075 CV events - partial intervention1444065 CV events - usual care
6671 Kidney failure - full intervention8363 Kidney failure - partial intervention8477 Kidney failure - usual care
953485 Life years saved - full intervention376810 Life years saved- partial intervention
302109253447 Costs - full intervention321853422664 Costs - partial intervention317815726575 Costs - usual care
30 years-15706473128 Economic outcome - full intervention4037696090 Economic outcome - partial intervention
1,44
4,06
51,
230,
075
899,
326
5 years 10 years 15 years 20 years 25 years 30 years0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
Time horizon
Cardiovascular events(stroke, MI, angina, heart failure)
Usual carePartial interventionFull intervention
8,47
78,
363
6,67
1
5 years 10 years 15 years 20 years 25 years 30 years0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
Time horizon
Kidney failure events
Usual carePartial interventionFull intervention
7,104
111,590
376,810
16,159
266,658
953,485
10 years
20 years
30 years
Timehorizon
Growth in saved life-years
Full intervention
Partial intervention
317,
816
321,
853
302,
109
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative cost of hypertension (MILLIONS)
Usual care
Partial intervention
Full intervetion$4,037.7
-$15,706.5
-$20,000
-$15,000
-$10,000
-$5,000
$0
$5,000
$10,000
30 years
Economic outcome of pharmacist intervention (MILLIONS)
Partial intervention Full interventionSavi
ngs
Cost
s
318
322
302
$0
$50
$100
$150
$200
$250
$300
$350
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative medical costs for individuals with hypertension (BILLIONS)
Usual care
Partial intervention
Full intervention$4.0
-$15.7
-$20
-$15
-$10
-$5
$0
$5
$10
30 years
Economic outcome of pharmacist intervention (BILLIONS )
Partial intervention Full intervetion
Savi
ngs
Cost
s
use BILLIONS graphic ONLY for canada AND MILLIONS FOR PROVINCES.

9Canadian Pharmacists Association
select region: for the NATIONAL report only (in Billions)CANADA
5 years 5 years
43805 CV events - full intervention67446 CV events - partial intervention86505 CV events - usual care
619 Kidney failure - full intervention786 Kidney failure - partial intervention803 Kidney failure - usual care407 Life years saved - full intervention183 Life years saved- partial intervention
36459354382 Costs - full intervention37320695929 Costs - partial intervention35215446042 Costs - usual care
10 years 10 years
208272 CV events - full intervention310631 CV events - partial intervention388254 CV events - usual care
1600 Kidney failure - full intervention2030 Kidney failure - partial intervention2073 Kidney failure - usual care
16159 Life years saved - full intervention7104 Life years saved- partial intervention
83620736584 Costs - full intervention88203889383 Costs - partial intervention85928397235 Costs - usual care
15 years 15 years
385486 CV events - full intervention556586 CV events - partial intervention678375 CV events - usual care
2770 Kidney failure - full intervention3507 Kidney failure - partial intervention3578 Kidney failure - usual care
88298 Life years saved - full intervention37982 Life years saved- partial intervention
135980818604 Costs - full intervention144742859705 Costs - partial intervention142317255130 Costs - usual care
20 years 20 years
567009 CV events - full intervention797271 CV events - partial intervention953225 CV events - usual care
4059 Kidney failure - full intervention5127 Kidney failure - partial intervention5220 Kidney failure - usual care
266658 Life years saved - full intervention111590 Life years saved- partial intervention
191497019262 Costs - full intervention204430771466 Costs - partial intervention201719547207 Costs - usual care
25 years 25 years
739211 CV events - full intervention1021093 CV events - partial intervention1206301 CV events - usual care
5386 Kidney failure - full intervention6777 Kidney failure - partial intervention6884 Kidney failure - usual care
572748 Life years saved - full intervention232618 Life years saved- partial intervention
247592336018 Costs - full intervention264217169291 Costs - partial intervention260946752957 Costs - usual care
30 years 30 years
899326 CV events - full intervention1230075 CV events - partial intervention1444065 CV events - usual care
6671 Kidney failure - full intervention8363 Kidney failure - partial intervention8477 Kidney failure - usual care
953485 Life years saved - full intervention376810 Life years saved- partial intervention
302109253447 Costs - full intervention321853422664 Costs - partial intervention317815726575 Costs - usual care
30 years-15706473128 Economic outcome - full intervention4037696090 Economic outcome - partial intervention
1,44
4,06
51,
230,
075
899,
326
5 years 10 years 15 years 20 years 25 years 30 years0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
Time horizon
Cardiovascular events(stroke, MI, angina, heart failure)
Usual carePartial interventionFull intervention
8,47
78,
363
6,67
1
5 years 10 years 15 years 20 years 25 years 30 years0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
Time horizon
Kidney failure events
Usual carePartial interventionFull intervention
7,104
111,590
376,810
16,159
266,658
953,485
10 years
20 years
30 years
Timehorizon
Growth in saved life-years
Full intervention
Partial intervention
317,
816
321,
853
302,
109
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative cost of hypertension (MILLIONS)
Usual care
Partial intervention
Full intervetion$4,037.7
-$15,706.5
-$20,000
-$15,000
-$10,000
-$5,000
$0
$5,000
$10,000
30 years
Economic outcome of pharmacist intervention (MILLIONS)
Partial intervention Full interventionSavi
ngs
Cost
s
318
322
302
$0
$50
$100
$150
$200
$250
$300
$350
5 years 10 years 15 years 20 years 25 years 30 years
Time horizon
Cumulative medical costs for individuals with hypertension (BILLIONS)
Usual care
Partial intervention
Full intervention$4.0
-$15.7
-$20
-$15
-$10
-$5
$0
$5
$10
30 years
Economic outcome of pharmacist intervention (BILLIONS )
Partial intervention Full intervetion
Savi
ngs
Cost
s
use BILLIONS graphic ONLY for canada AND MILLIONS FOR PROVINCES.
Economic Impact
With healthcare dollars scarce and an aging population signaling increasing expenditures on cardiovascular disease and kidney failure, the economic benefits of pharmacist intervention in hypertension management also bear serious consideration. The analysis found that with full intervention for a patient with hypertension, there could be $6,364 (today’s dollars) in cost-savings over 30 years of an individual accessing the intervention. The reduction in healthcare costs related to cardiovascular disease and kidney failure was found to more than offset the increased cost of pharmacist intervention ($7,145 increase in costs for medication and the intervention versus a $15,093 reduction in costs related to cardiovascular disease and kidney failure treatment).
Thus, if the intervention were administered to eligible individualse in Canada (this number is based on the conservative assumption that only half of those eligible would participate),f the projected cost savings over the lifetime of these individuals would be more than 15.7 billion dollars. Further, given current trends in hypertension prevalence rates and healthcare costs, these cost savings are likely to increase. When the time horizon is reduced from 30 years to five years or less, the benefits are dramatically reduced—highlighting the need for patients to continue to access care over time, and for pharmacists to continue to utilize their full scope of practice to provide care.
e. 930,000 individuals initiating in year 1, plus 75,000 new individuals per year. f. National or provincial population w/hypertension x 35% eligible x 50% assumed to access intervention;
rounded slightly.
$ 15.7 BILLIONin savings with full pharmacist intervention compared to usual care over 30 years.

10 Canadian Pharmacists Association
Conclusion
Comprehensive pharmacist care in hypertension, including patient education and prescribing, has the potential to offer both health benefits and cost savings to Canadians and, as such, has important public health implications. The findings show that pharmacist intervention in hypertension management could contribute to filling the hypertension care gap, not simply in a cost-effective manner, but indeed, in a cost-saving manner. It is rare to find a course of action that provides not just lower cost but better care as well. Given both these points, it would seem irresponsible not to give serious consideration to implementing a policy of pharmacist intervention in hypertension care. Indeed, the infrastructure for these services is already present. What needs to happen now is to expand pharmacists’ scope of practice and incentivize pharmacists appropriately to provide this care. With a simple stroke of a pen, health policy could (and should) be changed to improve health outcomes for Canadians.

11Canadian Pharmacists Association
References
1. Ezzati M, Lopez AD, Rodgers A, et al. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360(9343):1347-1360.
2. Collaboration NCDRF. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet. 2017;389(10064):37-55.
3. WHO. Raised blood pressure. 2017; www.who.int/gho/ncd/risk_factors/blood_pressure_prevalence_text/en/. Accessed February 10, 2017.
4. Gaziano TA, Bitton A, Anand S, et al. The global cost of nonoptimal blood pressure. J Hypertens. 2009;27(7):1472-1477.
5. Bakris G, Sarafidis P, Agarwal R, Ruilope L. Review of blood pressure control rates and outcomes. J Am Soc Hypertens. 2014;8(2):127-141.
6. Statistics Canada. High blood pressure, by sex, and by province and territory 2014; www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/health70a-eng.htm. Accessed February 10, 2017.
7. Statistics Canada. Blood pressure of adults, 2012 to 2015; www.statcan.gc.ca/pub/82-625-x/2016001/article/14657-eng.htm. Accessed February 10, 2017.
8. Padwal RS, Bienek A, McAlister FA, et al. Epidemiology of Hypertension in Canada: An Update. Can J Cardiol. 2016;32(5):687-694.
9. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6-e245.
10. Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123(8):933-944.
11. Robitaille C, Dai S, Waters C, et al. Diagnosed hypertension in Canada: incidence, prevalence and associated mortality. CMAJ. 2012;184(1):E49-56.
12. IHME. Global Deaths, 2010; www.healthdata.org/. Accessed February 10, 2017.
13. Lawes CM, Vander Hoorn S, Rodgers A, et al. Global burden of blood-pressure-related disease, 2001. Lancet. 2008;371(9623):1513-1518.
14. Centers for Disease Control and Prevention. End-stage renal disease patients, by selected characteristics: United States, selected years 1980–2010. 2011; www.cdc.gov/nchs/data/hus/2011/051.pdf. Accessed February 10, 2017.
15. Campbell K. DCCT opens new opportunities for pharmacists. California Pharmacist. 1993:26-27.
16. Tsuyuki RT, Houle SK, Charrois TL, et al. Randomized Trial of the Effect of Pharmacist Prescribing on Improving Blood Pressure in the Community: The Alberta Clinical Trial in Optimizing Hypertension (RxACTION). Circulation. 2015;132(2):93-100.
17. Santschi V, Chiolero A, Colosimo AL, et al. Improving blood pressure control through pharmacist interventions: a meta-analysis of randomized controlled trials. Journal of the American Heart Association. 2014;3(2):e000718.
18. Canadian Institute for Health Information. National Health Expenditure Trends, 1975 to 2014; www.cihi.ca/en/nhex_2014_report_en.pdf. Accessed February 10, 2017.

Canadian Pharmacists Association 1785 Alta Vista Drive, Ottawa, ON K1G 3Y6 1-800-917-9489 613-523-0445 [email protected]
www.pharmacists.ca