Implementing and Sustaining a Middle and High School Reading and

Soteria Strains
Safe Patient Handling and Mobility Program Implementation Guide
V1.0 edited June 18, 2015
A provincial strategy for healthcare workplace musculoskeletal injury prevention.

Soteria Strains
Implementation and Program Guide
Page 2 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Introduction
Nova Scotia’s health care sector, like publically funded health care elsewhere across Canada, is
challenged to maintain and enhance services and outcomes while at the same time constraining
the pace of increasing costs. Improving the health and safety of Nova Scotia’s health care
workers has the potential to both significantly reduce costs for health care in Nova Scotia while
enhancing patient safety and health outcomes.
The total annual cost of work-related injuries in Nova Scotia’s health care sector is estimated to
be in excess of $100 million. This figure represents both the cost of workers’ compensation and
the uninsured costs associated with work-related injuries, such as additional overtime,
recruitment and retraining, lost knowledge and experience, administrative time, and negative
patient outcomes. While these dollar figures are significant, they tend to obscure the fact that
work-related injuries cause significant pain and suffering for health care workers, forcing some
to leave their chosen profession and leaving others with significantly reduced physical
capabilities.
To improve the health and safety of health care workers in Nova Scotia, it is important to
understand the nature of the injuries these workers experience. A review of the data reveals that
in 2012, almost 80 percent of all time-loss claims reported to the Workers’ Compensation Board
of Nova Scotia (WCB) by health care workers were musculoskeletal injuries and that more than
50% of those claims were linked to some type of patient, resident, or client lift or transfer task.
This includes patient lifting, transferring, and repositioning, which we are calling patient handling
and mobility.
Purpose
The Soteria Strains Safe Patient Handling and Mobility Program guide and implementation
guide were developed by representatives from Nova Scotia’s district health authorities and their
partners. They are intended to provide acute care facilities and organizations in the province
with guidance about implementing and sustaining an evidence-based, effective safe patient
handling and mobility program within their facilities and/or organization.

Soteria Strains
Implementation and Program Guide
Page 3 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
How to Use These Guides
There are two guides: an implementation guide and a program guide.
The implementation guide describes the steps involved in putting the Safe Patient Handling and
Mobility Program in place. Steps are arranged in a recommended, chronological order.
However, steps may occur concurrently or it may be appropriate for an organization to follow the
steps in a different order. Implementation is divided into seven phases outlined in the table
below.
Implementation Guide Overview
Phase Steps
1 Setting the stage for success
2 Conduct a gap analysis; identify priority units; select and train unit-based champions and managers
3 Undertake unit-based assessments; introduce safety huddles
4 Identify, plan for, and implement unit-level controls; plan for and train staff (controls, patient-risk profile, point-of-care mobility status check (PACE))
5 Audit implementation in priority units; identify areas for improvement; document and report; introduce after-action reviews
6 Identify “next”’ priority areas, and implement as per phases 2-5
7 Implement a maintenance and continuous-improvement phase: ensure ongoing monitoring and reporting, a formal review, and identification of improvement opportunities

Soteria Strains
Implementation and Program Guide
Page 4 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
The program guide contains reference material that describes how to implement various
elements of the program and includes numerous tools and templates that may be used and/or
modified by the implementing organization. To improve ease of use, the program guide has
been divided into four sections, each presented as a separate document. The program guide,
its respective sections, and the chapters are outlined in the table below.
Section 1 focuses on organizational processes and activities. Sections 2 and 3 focus on
identifying and mitigating hazards – redesigning the work. Section 4 contains specific
considerations, information, and tools that may be used to supplement the processes described
in sections 2 and 3 when required.
Program Guide Overview
Section # Title Chapter # Title
1 Setting the Stage
1.1 Commitment of Leaders
1.2 Policy
1.3 Program Evaluation and Continuous Improvement
1.4 Communications, Promotion, and Engagement
2 Identifying Hazards and
Assessing Risk
2.1 Identifying Priority Areas
2.2 Unit Assessment
2.3 Patient Risk Profile
2.4 Point-of-Care Mobility Status Check (PACE)
3 Controls
3.1 Selecting Controls
3.2 Equipment Selection
3.3 Equipment Installation and Maintenance
3.4 Safety Huddles
3.5 Key Design and Installation Specifications
3.6 Training
4 Special Considerations
4.1 Emergency Situations
4.2 Bariatric Patients
4.3 Orthopedic Patients
4.4 Cognitive Impairment
4.5 Labour and Delivery
4.6 Patients with Amputations

Soteria Strains
Implementation and Program Guide
Page 5 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Program Scope
The Soteria Strains Safe Patient Handling and Mobility Program is an evidence-based, multi-
factorial program for the prevention of musculoskeletal injuries (MSIs) in acute and tertiary
health care in Nova Scotia. The program includes elements that research indicates are
necessary for an effective patient handling and mobility program. The content was also
influenced by the needs identified by multiple stakeholder groups within organizations in Nova
Scotia that provide and/or support acute and tertiary health care.
The program is one approach to safe patient handling and mobility that is consistent with
evidence-based, best-practice approaches based on the information and research current at the
time the program was developed. Other approaches to safe patient handling and mobility that
include a process to recognize and assess hazards, and control the risks associated with
patient handling and mobility tasks may be equally effective.
While many of the elements of this program may be used to support injury prevention in other
areas of health care, such as continuing care and home care, the focus of this initiative is on
acute and tertiary care. The intent is to share lessons learned and adapt this program to
address the specific patient handling and mobility needs of long-term and home care
residents/clients, workers, and workplaces. Also, MSIs related to other hazards, such as poor
workstation design and material handling, are not addressed in this program guide. Specific
programs to address MSIs related to these hazards will be needed.
Previous efforts to reduce the number of injuries associated with patient handling and mobility
often relied solely on training of staff to use proper body mechanics and manual lifting
techniques. Research has clearly shown that this type of training on its own is not effective in
reducing the frequency or severity of musculoskeletal injuries among health care workers.
Manual patient handling tasks are intrinsically unsafe because they are beyond the capabilities
of the general workforce.
Legislative Requirements
A safe and effective patient handling and mobility program is an inherent element under existing
occupational health and safety legislation. While not specifically mandated in Nova Scotia’s
Occupational Health and Safety Act or its related regulations, the Act’s “General Duty Clause”
(Section 13(1)) requires employers to take “every precaution that is reasonable” to ensure the
health and safety of all persons. More specifically, Nova Scotia’s Occupational Safety General
Regulations, Part 5, Section 26, state that employers must provide equipment and training when
“the lifting or moving of a thing or a person may be a hazard to the health or safety of a person
at the workplace.” It is clear that patient handling and mobility tasks are high risk and
hazardous; as such, employers are required to put in place programs and provide equipment
and training to staff to reduce the risk of injury.

Soteria Strains
Implementation and Program Guide
Page 6 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Acknowledgments
A special thank you is extended to the Soteria Strains Executive Leadership Group, Working
Group, Author/Editor Group, and all the partner organizations.
Thanks is also extended to all employees from all of Nova Scotia’s District Health Authorities
who took the time to complete surveys, attend feedback sessions, share their stories and
provide comments on the program and its importance.
Partner Organizations
AWARE-NS
Health Care Human Resource Sector Council of Nova Scotia
IWK Health Centre
Nova Scotia Department of Health and Wellness
Nova Scotia’s District Health Authorities
Workers’ Compensation Board of Nova Scotia Funding also provided by:
Nova Scotia Department of Labour and Advanced Education
Internal Responsibility System
The internal responsibility system is the underlying philosophy of the occupational health and safety legislation in all Canadian jurisdictions. Its foundation is that everyone in the workplace – both employees and employers – is responsible for their own safety and for the safety of co-workers. Acts and regulations do not always impose or prescribe the specific steps to take for compliance. Instead, they hold employers responsible for determining the steps needed to ensure the health and safety of all employees.
An internal responsibility system does the following:
1. Establishes responsibility-sharing systems 2. Promotes a safety culture 3. Promotes best practices 4. Helps develop self-reliance 5. Ensures compliance
See http://www.ccOH&S.ca/oshanswers/legisl/irs.html for more information.

Soteria Strains
Implementation and Program Guide
Page 7 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Contents Introduction ............................................................................................................................ 2
Purpose .................................................................................................................................. 2
How to Use These Guides ......................................................................................................... 3
Implementation Guide Overview ............................................................................................. 3
Program Guide Overview ....................................................................................................... 4
Program Scope .......................................................................................................................... 5
Legislative Requirements ........................................................................................................... 5
Soteria Strains Safe Patient Handling and Mobility Program Implementation Guide .................. 9
Phase 1 – Setting the Stage......................................................................................................11
Activity 1 – Commitment of Leaders ......................................................................................12
Activity 2 – Create Policy .......................................................................................................13
Activity 3 – Fill Key Program Roles ........................................................................................13
Activity 4 – Raise Awareness & Inspire Desire for Change ....................................................14
Activity 5 – Develop Evaluation Framework ...........................................................................15
Activity 6 – Estimate and Allocate Resources ........................................................................17
Activity 7 – Communicate Progress .......................................................................................18
Phase 2 – Identify Resources and Needs .................................................................................19
Activity 1 – Conduct Gap Analysis .........................................................................................20
Activity 2 – Identify Priority Areas (Units) ...............................................................................20
Activity 3 – Select Priority Unit Peer Champions ....................................................................20
Activity 4 – Conduct Hazard Assessment Training ................................................................22
Activity 5 – Communicate Progress .......................................................................................22
Phase 3 – Undertaking Priority Area Hazard Assessments .......................................................23
Activity 1 – Plan Priority Unit Hazard Assessments ...............................................................23
Activity 2 – Conduct Priority Unit Assessments ......................................................................24
Activity 3 – Communicate Results of Hazard Assessments ...................................................25
Activity 4 - Introduce Safety Huddles .....................................................................................25
Activity 5 – Communicate Progress .......................................................................................26
Phase 4 – Implementing Controls in Priority Areas ...................................................................27
Activity 1 – Identify Hazard Controls for Priority Units ............................................................28
Activity 2 – Approve Hazard Controls for Priority Units ..........................................................29

Soteria Strains
Implementation and Program Guide
Page 8 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 3 – Plan Implementation of Hazard Controls and Training .........................................30
Activity 4 – Implement Hazard Controls .................................................................................32
Activity 5 – Conduct Hazard Controls Training .......................................................................33
Activity 6 – Communicate Progress .......................................................................................36
Phase 5 – Initiate Audit Phase ..................................................................................................37
Activity 1 - Audit implementation Progress .............................................................................37
Activity 2 - Identify Issues and Potential Improvements .........................................................38
Activity 3 – Introduce After Action Reviews ............................................................................38
Activity 4 – Communicate Progress .......................................................................................38
Phase 6 – Continue Roll-Out .....................................................................................................40
Activity 1 - Identify Priority Areas (Units) ................................................................................40
Activity 2 – Identify Priority-Unit Peer Champions ..................................................................40
Activity 3 – Conduct Hazard Assessment Training ................................................................41
Activity 4 – Continue with Phases 3-5 ....................................................................................41
Activity 5 – Communicate Progress .......................................................................................41
Phase 7 – Ensure Ongoing Improvement ..................................................................................42
Activity 1 - Monitor Program Elements ...................................................................................42
Activity 2 – Undertake Formal Program Review .....................................................................43
Activity 3 - Implement Changes Required by Review .............................................................43
Activity 4 – Communicate Progress .......................................................................................44

Soteria Strains
Implementation and Program Guide
Page 9 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Soteria Strains Safe Patient Handling and Mobility Program Implementation Guide
Implementation Phase
Phase Name Phase Activities Notes
1 Setting the
Stage
1. Commitment of leaders
2. Prepare policy
3. Fill key program roles
4. Raise awareness and inspire desire for change
5. Develop evaluation framework
6. Estimate and allocate resources
7. Communicate progress
2 Identifying
Resources and Needs
1. Conduct gap analysis
2. Identify priority areas (units)
3. Identify priority unit peer champions
4. Conduct unit assessment training
5. Communicate progress
3 Priority Unit Assessment
1. Plan unit assessments
2. Conduct priority unit hazard assessments
3. Communicate results of hazard assessments
4. Introduce safety huddles*
5. Communicate progress
* Safety huddles may be introduced as a stand-alone
program element at any time.
4 Implementing
Controls in Priority Areas
1. Identify hazard controls for priority units
2. Approve hazard controls for priority units
3. Plan implementation of hazard controls and training
4. Implement hazard controls
5. Conduct hazard controls training
6. Communicate progress

Soteria Strains
Implementation and Program Guide
Page 10 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
5 Initiate Audit
Phase
1. Assess audit implementation progress
2. Identify issues and potential improvements
3. Introduce After Action Reviews**
4. Communicate progress
**After Action Reviews may be introduced as a
stand-alone element at any time after
safety huddles have been implemented.
6 Continue
Roll-out
1. Identify next priority areas
2. Identify next unit peer champions
3. Conduct unit assessment training
4. Continue with phases 3-5
5. Communicate progress
7 Ensure Ongoing
Improvement
1. Monitor program elements
2. Undertake formal program review
3. Implement changes as required based on review
4. Communicate progress
Implementing a safe patient handling and mobility program is a major initiative requiring system
change, process change, and individual behaviour change at all levels of the organization. A
successful change is characterized by a solution that is effectively designed, developed, and
delivered, and that is embraced, adopted, and used by affected employees. Key factors in
successful and sustained change are:
1. Leaders commitment and support
2. Engagement and communication
3. Effective design, development, and delivery (the "technical" aspects of the change)
4. Systematic framework for ensuring the change is embraced, adopted, and used (the
"people" aspects of the change)
The activities in the implementation phases discussed in this document, in combination with the
program guide and supporting training materials, should provide everything required to satisfy
factors 2, 3 and 4. That leaves factor 1: Leadership Commitment and Support. For an effective
safe patient handling and mobility program to be implemented and sustained, leaders at all
levels, formal and informal, must be committed to the change.

Soteria Strains
Implementation and Program Guide
Page 11 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Phase 1 – Setting the Stage
This section provides guidance on the steps an organization should take in order to maximize
the success of the program in their organization. While all of these steps are important, senior
leadership commitment and participation, and communication and engagement are among the
most important.
Activities Description Lead By
1. Commitment of Leaders
Ensure senior leader commitment and participation.
● Organization’s CEO or equivalent
2. Create Policy Create, sign and communicate a safe patient handling and mobility policy.
● Senior leadership team
3. Fill Key Program Roles
Ensure the following roles are filled and responsibilities defined:
● Senior Leader Champion ● Safe Patient Handling and
Mobility Program Coordinator
● Multi-stakeholder Safe Patient Handling and Mobility Program Coordinating Committee
● Senior leadership team
4. Raise Awareness and Inspire Desire for Change
Communicate to everyone in the organization the new Safe Patient Handling and Mobility Policy and the plan to implement the program.
Messages include: ● Why the safe patient
handling program is important
● The benefits of the program ● The consequences of
maintaining the status quo ● Potential challenges
● Organization’s CEO or equivalent
● Senior Leader team ● Senior Leader Champion ● Safe Patient Handling and
Mobility Program Coordinator ● Multi-stakeholder Safe Patient
Handling and Mobility Program Coordinating Committee
Even though communicating progress is the last activity of each phase, it should be
something that is done on an ongoing basis during each activity, starting as soon as
possible and continuing as each activity is put into action. Regular, frequent checks and
monitoring will allow issues and barriers to be identified. The results of this monitoring
should be reported back to the senior leadership team, perhaps through the Senior
Leader Champion, so that successes can be acknowledged and issues can be
addressed.

Soteria Strains
Implementation and Program Guide
Page 12 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
5. Develop Evaluation Framework
Begin to develop/implement an evaluation framework for the program.
● Senior Leader Champion ● Safe Patient Handling and
Mobility Program Coordinator ● Multi-stakeholder Safe Patient
Handling and Mobility Program Coordinating Committee
● Additional support as required (IT, OH&S, HR, etc.)
6. Estimate and Allocate Resources
Plan for allocation of resources to purchase/install required patient handling and mobility equipment and provide required training to staff.
● Senior Leadership Champion ● Safe Patient Handling and
Mobility Program Coordinator
7. Communicate
Progress Monitor progress and provide updates to stakeholders.
● Senior Leadership Champion ● Program Coordinator with
support of HR and/or Communications staff
Activity 1 – Commitment of Leaders
Commitment and leadership begins at the top with the chief executive officer and senior
managers. By clearly communicating and visibly demonstrating their support for the program,
this group of individuals will create a foundation upon which a successful safe patient handling
and mobility program can build. Without this, the program will almost certainly fail.
The members of the organization’s leadership team can demonstrate their commitment to and
participate in the program by ensuring:
A. They have an understanding of the safe patient handling and mobility program’s
purpose, goals and processes.
B. Measurable objectives are set, included in the program evaluation framework, and used
to guide program implementation and delivery.
C. Appropriate financial, human, and other organizational resources are put in place to
effectively plan, implement, check, review, and revise the Safe Patient Handling and
Mobility Program.
D. Implementation activities 2-4 are completed.
a. A written policy is signed (see “Section 1.2 Policy”) outlining the organization’s
commitment to the Safe Patient Handling and Mobility Program.
b. Roles are defined, responsibilities assigned, accountabilities established, and
authority delegated as needed to implement the program.
c. Raise awareness and inspire desire for change
Refer to Program Guide "Section 1.1 – Leadership Commitment" for more details.

Soteria Strains
Implementation and Program Guide
Page 13 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 2 – Create Policy
A safe patient handling and mobility policy sets a structure to ensure that patient lifts, transfers
and repositioning are performed in a way that minimizes risk of injury to health care workers and
patients. It is an important element in a program with multiple elements and guides
organizational-level decisions and actions as well as frontline health care worker decisions and
actions. While a policy is necessary, it is not sufficient, by itself, to mitigate the risk to health
care workers and patients during patient handling and mobility activities.
A safe patient handling and mobility policy should:
1) State the organization’s commitment to the safe patient handling and mobility program.
2) State the intent of the policy; to protect the health of staff and patients.
3) State that all manual patient handling and mobility tasks are to be avoided wherever
possible.
4) Clarify the roles and responsibilities of health care workers, support workers, and
administrators to help maintain sustainability of the program.
5) Be understood by all health care workers and reviewed on a regular basis.
A policy provides a clear vision of why the program is being implemented, along with its goals
and objectives, and provides a means to hold people accountable for their participation.
Once the policy is finalized and signed off by the organization’s CEO, The senior leadership
team should demonstrate its support for the policy by taking part in a communication process to
inform all staff, at all levels, about the policy, why it is needed, the expected benefits, and the
plan for implementing the program. It is important to include patients and their families when
communicating about the policy so that they understand how the safe patient handling and
mobility program will benefit them and their health care providers.
Refer to section 1.2 – Policy, Appendix 1.2.1 for more details and a sample policy statement
Activity 3 – Fill Key Program Roles
It is essential to define the roles and responsibilities for the safe patient handling and mobility
program and clearly communicate these to the individuals who will be assuming those roles.
The safe patient handling and mobility policy may include one or more statements regarding the
roles and responsibilities various people, positions, or departments have under the program.
However, a more detailed listing of the specific roles and responsibilities for specific individuals
and positions should be developed and approved by the organization’s senior leadership team.

Soteria Strains
Implementation and Program Guide
Page 14 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
At this stage in the implementation of the program, it is important to clearly define the roles and
responsibilities for the:
1) Senior Leadership Champion
2) Safe Patient Handling and Mobility Program Coordinator
3) Multi-Stakeholder Safe Patient Handling and Mobility Program Coordinating Committee
a. Safe patient handling and mobility program coordinating committee
recommended membership:
i. Senior Leadership Champion
ii. Safe Patient Handling and Mobility Program Coordinator
iii. VP of Clinical Services (or equivalent) - if not already the Senior
Leadership Champion
iv. Front line health care workers with multiple professional representation as
required (RN, PT, OT, DI, etc)
v. OHS
vi. Union
vii. Senior Executive Facilities Management/Engineering
services/Maintenance/Operations
viii. Biomedical Engineering
ix. Procurement Officer
x. Finance
xi. Infection Prevention and Control
xii. Patient quality and safety
Roles and responsibilities for these individuals/groups should be specific, well documented, and
clearly communicated to the individual(s) involved and the organization as a whole. Some
possible roles and responsibilities for these individuals/groups are described in section 1.2
Policy, Appendix 1.2.2 - Roles and Responsibilities.
Activity 4 – Raise Awareness & Inspire Desire for Change
Implementing an effective safe patient handling and mobility program is a major change process
for any health care organization, and as such, it requires well-planned, effective communication.
Raising awareness demonstrates commitment to the program and helps ensure its success.
And while good communication will not guarantee the success of a safe patient handling and
mobility program, it is well known that a lack of effective communication can derail a program
before it even starts.
It is helpful to develop, approve and implement a communications plan to ensure that everyone
who should be aware is made aware of the new policy, once created and signed, and also that
key messages related to the program are communicated and understood. Suggested audiences
and messages are referenced in the program guide section 1.4 - Communication, Promotion
and Engagement, Appendix 1.4.1 – Suggested Key Messages by Audience and Phase.

Soteria Strains
Implementation and Program Guide
Page 15 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Communication plays an essential role in meeting numerous goals. Communications should be
two-way and will require multiple stakeholders to be involved. When these goals are achieved
the normal and expected reluctance for change will be transformed. The goals are:
Raise Awareness – Achieving this goal requires answering why this program is
important to the organization and how it will benefit the organization. Note: Much of
this work began with the engagement process used to create this implementation
guide and its companion program guide. Organizations can capitalize on this
groundwork when creating the communications plan by referring back to results from
the perception survey and face-to-face engagement sessions. Find these reports
and more at www.soteriahealth.ca.
Inspire Desire – Achieving this goal requires focusing on the benefits of the program
and the consequences of not initiating change. There will be different messages for
different groups and individuals, who will be impacted in different ways by the
program. While communicating personal benefits is important, this is also a good
time to identify potential challenges, barriers, and the apprehension that workers
might have. The method of communication is important to consider when inspiring
the desire to change. While email and electronic communications may seem more
efficient, they are not as effective as face-to-face conversations. Ideally, these
conversations occur one to one, but may also be done in team meetings. It is to be
expected that even when individuals are inspired and looking forward to change they
may still have some reluctance to accept a new way of doing things.
Grow Knowledge – To achieve this goal, people need to understand what they
need to know about the program. Communications should be focused on answering
questions such as: What is changing? What isn’t changing? How is the new
program the same as how we currently practice? What’s in it for me? How will
patients benefit? Another key message is to ensure awareness of what training will
occur prior to or during the change. People must be sure that they will have the skills
required for the program. Answering questions such as how, when, and why training
will occur will assure people they will be prepared for the change in the way they
practice as the program is implemented.
Refer to Program Guide, “Section 1.4 – Communications, Promotion, and Engagement” to
create and execute a communication, promotion, and engagement plan.
Activity 5 – Develop Evaluation Framework
When implementing a safe patient handling and mobility program, it is important to clearly
define and communicate the goals and objectives of the program. Once this is done, the
organization needs to consider how the program will be monitored and evaluated. A well-
designed evaluation framework will allow the organization to determine if the resources and
effort put into the program were justified and if the program has met its goals and objectives. It
Soteria Strains
Implementation and Program Guide
Page 16 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
will also help to ensure that the safe patient handling and mobility program can continue to
improve over time.
The Multi-stakeholder Safe Patient Handling and Mobility Program Coordinating Committee
(refer to Activity 3) should be tasked with identifying high level goals and objectives for the
program. The Committee should be provided with support and resources to assist with this
work, including:
Training on the Soteria Strains evaluation framework (refer to program guide section 3.6
- Training)
Adequate, dedicated time and reasonable due dates to complete the work
Information on the types of data currently collected, how that data is collected and how
it is used
Access to program guide section 1.3 Evaluation and Continuous Improvement
The Safe Patient Handling and Mobility Program Coordinator should review the indicators in
Soteria Strains Program Guide Section 1.3, Appendix 1.3.2-4, in order to identify if the
organization is currently collecting data related to each indicator and, if so, how. Examples of
how an organization may be collecting data for the indicators required to evaluate the safe
patient handling and mobility program include:
Reports from existing reporting systems, including adverse-incident records,
injury/incident reports
Number of health care providers attending safe patient handling and mobility training
Proportion of total health care providers attending safe patient handling and mobility
training
Hazards and other items discussed at health and safety meetings (meeting minutes)
First aid and incident records for the unit or organization
WCB claims data
Absenteeism records
Health care provider turnover rates
Employee complaints (e.g., workload, equipment and software problems, pain and
discomfort)
Workplace assessments and hazard checklists
Audits to observe working practices and activities
Surveys related to safe patient handling and mobility via self-report questionnaires
Time off for medical visits as a result of patient handling and mobility work strain
Interviews with health care providers involved in patient handling and mobility
Worker morale and satisfaction measures (e.g., suggestion boxes, group meetings,
surveys)
If the organization isn’t currently collecting data related to an indicator, they should investigate
how this data could be collected, for example creating a survey for specific populations. Refer to

Soteria Strains
Implementation and Program Guide
Page 17 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Section 1.3, Appendix 1.3.6, for resources related to developing surveys related to the
implementation of the safe patient handling and mobility program.
The Coordinator should compile the results of this review and develop a plan for evaluating the
program. The plan should specify how data needed for each indicator is or will be collected, and
who will be responsible for collecting this data. This plan should be provided to the Program
Coordinating committee for their review and feedback. Approval for the plan should be obtained
from the appropriate level of management (e.g. senior leader sponsor).
It is important that any systems or processes needed to collect the data for required indicators
be either in place or set up as soon as possible so that the information gathered can be used for
both evaluation and program-improvement purposes. In addition, the Multi-stakeholder Safe
Patient Handling and Mobility Program Coordinating Committee will generate program
evaluation resource materials to support the efforts of individuals/groups, such as managers
and peer champions.
Activity 6 – Estimate and Allocate Resources
Implementing an effective safe patient handling and mobility program requires an investment in
both equipment and people. It is not sufficient simply to tell health care providers to work safely
or use good body mechanics when most patient handling and mobility tasks are high-risk tasks
when performed manually. It is important to plan for and allocate the resources to buy and
install the required equipment and to train staff in methods and techniques that will let them
safely handle and move patients.
Resource issues that need to be considered include:
Initial equipment purchase costs (including required accessories)
Equipment installation costs (including any required retrofitting of spaces – electrical,
structural, etc.)
Ongoing equipment maintenance, testing, and inspection costs
Ongoing costs to replace accessories
Space where health care providers can and be trained to use equipment and can test
equipment
Time and, as required, replacement staff so that health care providers can be trained in
safe patient handling and mobility assessments and methods
Time and, as required, replacement staff to conduct the training sessions
Opportunities for managers and other support staff to receive required training
Funding and communications resources to ensure that all stakeholders are kept
informed about the implementation and ongoing success of the safe patient handling
and mobility program
The Safe Patient Handling and Mobility Program Coordinating Committee selected in Activity 3
will select a number of units to launch the program in. The size and number of units should be
realistic. Refer to Phase 2.2: Identify Priority Units and Section 2.1 of the program guide for

Soteria Strains
Implementation and Program Guide
Page 18 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
more details on selecting units to begin implementation. For planning purposes, it may be
helpful to use the gross-budget-estimation process as shown. This is based on previous
experience in jurisdictions within Nova Scotia and PEI.
This estimate includes cost of equipment and training, but not maintenance of equipment. Also,
there is an assumption that no major structural issues are present within the facility that requires
significant renovation and/or upgrading.
Activity 7 – Communicate Progress
The Senior Leader Champion and, once identified, the Program Coordinator should review the
steps outlined in Activities 1-6 to determine which steps have been completed, those that are in
process, and any that have been missed or were considered complete, but not implemented
fully. They might:
Compare the specific outputs (e.g., the Safe patient Handling and Mobility Policy) to
examples provided in the Soteria Strains Safe Patient Handling and Mobility Program.
Ensure they understand their own responsibilities under the program and that these
have been communicated to others in the organization.
Make certain that the Safe Patient Handling and Mobility Program Coordinating
Committee have been established and understand its purpose and responsibilities.
Ensure staff in various areas of the organization are aware and understand the reasons
why the policy was created and what they can expect as the program is implemented.
Confirm the evaluation framework is created and approved; systems and procedures to
collect required data are identified, planned for, and created; and that individuals
responsible for collecting the data are doing this.
Ensure that the organization has a plan for allocating financial and personnel resources
so the program can be implemented in a timely and efficient manner, and so that it can
meet its goals and objectives.
After the review is completed the Senior Leader Champion and/or Program Coordinator should
inform all stakeholders of results and next steps.
Estimated cost/unit = (# beds) x ($3000 ±15%)

Soteria Strains
Implementation and Program Guide
Page 19 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Phase 2 – Identify Resources and Needs
The goals of phase 2 are to identify which units within an organization are a priority for
implementing the safe patient handling and mobility program, and select and train unit-based
peer champions. Once the champions are trained, they will work with the managers from priority
units to introduce and hold safety huddles.
Activities Brief Description Completed By
1. Conduct Gap Analysis Conduct facility/organization-
level gap analysis
Program Coordinator with assistance from
○ OH&S and/or ○ HR
2. Identify Priority Areas (Units)
Identify priority units for initial implementation
Program Coordinator with assistance from:
○ OH&S and/or ○ HR
and input from the: ○ Safe Patient Handling and Mobility Program Coordinating Committee
3. Select Priority Area (Unit) Peer Champions
Select unit-based peer champions for priority units
(suggested two minimum per unit depending on size and
nature of unit)
Program Coordinator with managers from priority units
4. Conduct Hazard Assessment Training
Train unit-based peer champions and managers for
priority units (unit assessment module)
Program Coordinator with support of OH&S and/or additional staff
5. Communicate Progress Monitor progress and provide
updates to stakeholders Program Coordinator with support from HR and/or Communications staff
Even though communicating progress is the last activity of each phase, it should be
something that is done on an ongoing basis during each activity, starting as soon as
possible and continuing as each activity is put into action. Regular, frequent checks and
monitoring will allow issues and barriers to be identified. The results of this monitoring
should be reported back to the senior leadership team, perhaps through the Senior Leader
Champion, so that successes can be acknowledged and issues can be addressed.

Soteria Strains
Implementation and Program Guide
Page 20 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 1 – Conduct Gap Analysis
Conducting a facility or organizational-level gap analysis is one of the first and most important
steps required to implement a safe patient handling and mobility program. It is very likely that
acute care facilities will have already put into place various controls to reduce the risk of injuries
associated with patient handling and mobility tasks. It may be that health care workers have
been trained on effective patient handling techniques or one or more pieces of equipment have
been purchased and installed. It is possible that lift teams were created but are no longer
together. The organization may even have a safe patient handling and mobility program in
place. Understanding what an organization has and is doing to help prevent injuries related to
patient handling and mobility is vital before moving forward. The gap analysis will help you to
see what is in place, what is working, what isn’t working, and if additional program elements
need to be instituted to help make the program effective. It will help reinforce and invigorate
what is already in place, which can reduce the amount of effort and time required to implement
an evidence-based safe patient handling and mobility program.
Activity 2 – Identify Priority Areas (Units)
When considering how to implement a safe patient handling and mobility program, consider
whether it is possible and reasonable to try to implement it in all areas of the organization at
once. As a first step, create a list of the areas where patient handling and mobility tasks are
performed and then prioritize them for action based on a review of key indicators and
information.
Typically this work will be done by the Multi-stakeholder Safe Patient Handling and Mobility
Program Coordinating Committee, once identified.
Section 2.1 of the program guide provides a step-by-step process that is supported by training
material and may be used to enhance your organization’s current process.
Activity 3 – Select Priority Unit Peer Champions
Once the priority units have been identified, the Program Coordinator should work with the
Managers from these units to select unit based Peer Champions. Each unit should have at least
two peer champions, and larger units should have more to ensure adequate coverage. Each
unit based peer champion will be a resource for safe patient handling and mobility. With the
support of their manager, they will help train others on their unit, reinforce and model safe
handling behaviours, answer questions from co-workers, help co-workers to problem solve
difficult patient handling situations, etc.
A template for completing the gap analysis will be creating during early pilot phases to be
included in section 1 of the Soteria Strains Safe Patient Handling and Mobility Program Guide.

Soteria Strains
Implementation and Program Guide
Page 21 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Follow these steps to select unit based peer champions:
1) The Program Coordinator and manager should meet with all care staff on the priority
unit(s). Ideally this should be a group meeting with all staff present, but individual or
small group meetings will also suffice. The coordinator and manager should:
a. Review the safe patient handling and mobility policy with the staff.
b. Inform the team they have been selected as a priority unit and why.
c. Tell the team about the role of the unit based champion. The manager and
program coordinator will provide material that describes the role and
responsibilities.
d. Provide an opportunity, during this meeting, for the Senior Leader Champion to
communicate the executive leader team’s support and expectations for the
program.
2) To generate a list of candidates the Program coordinator should ask for:
a. The manager to identify a list of candidates.
b. Health care workers to nominate individuals.
c. Request health care workers volunteer.
d. Individuals who are listed who meet the requirements to fill the role of unit peer
champions should be considered.
3) The Program Coordinator and manager should then meet with the selected candidate
champions from each unit, either separately or in a group, to review the responsibilities
of the unit peer champion and the training plan and confirm participation.
4) Peer champion selections should be shared with all unit staff.
The Role/responsibilities of the Unit Based Peer Champion are to:
Provide training to peers on their unit.
Model safe patient handling and mobility behavior.
Act as an ongoing resource for peers, answer questions, and help them problem solve
difficult patient handling and mobility situations.
Participate in continuous improvement efforts that promote, improve, and sustain the
program as well as evaluate training effectiveness.
Act as a resource for unit based peer champions from other units.
Refer to Soteria Strains Safe Patient Handling and Mobility Program Guide Section 1.2 Policy for
more details on program roles and responsibilities.

Soteria Strains
Implementation and Program Guide
Page 22 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 4 – Conduct Hazard Assessment Training
All the peer champions and managers from the priority units will need to be trained so that they
can properly fulfill their responsibilities. A plan needs to be put in place to enable training to be
delivered in a timely manner.
For this phase, each peer champion will require training on:
Unit assessment and control selection
How to conduct safety huddles
Helping with continuous improvement efforts that promote, evaluate, and sustain the
program. Resource material will be provided by the Multi-stakeholder Safe Patient
Handling and Mobility Program Coordinating Committee (generated in Phase 1, Activity
5).
For this phase, each manager will require training on:
Hazard identification, risk assessment, and control selection
Safety huddles
Continuous improvement efforts that promote, evaluate, and sustain the program.
Resource material will be provided by the Multi-stakeholder Safe Patient Handling and
Mobility Program Coordinating Committee (generated in Phase 1, Activity 5).
Activity 5 – Communicate Progress
The Senior Leader Champion and, the Program Coordinator should review the steps outlined in
Activities 1-4 to determine which steps have been completed, those that are in process, and any
that have been missed or were considered complete, but not implemented fully. They might:
Review the process used to collect data for identifying priority units to identify gaps and areas for improvement.
Talk to the managers and staff from across the organization to learn how they feel about the selection process and communication with staff.
Connect with the managers and staff on the priority units to discover how they feel about the selection process and to make sure they understand the role and purpose of peer champions.
Meet with the peer champions to understand how they feel about the selection process and the effectiveness of their training.
Collect training evaluations from the peer champions, review and analyze these to identify possible improvements to content and delivery of the training.
After the review is completed the Senior Leader Champion and/or Program Coordinator should
inform all stakeholders of results and next steps.

Soteria Strains
Implementation and Program Guide
Page 23 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Phase 3 – Undertaking Priority Area Hazard Assessments
During Phase 3 the Program Coordinator will work with managers and, ideally, unit based peer
champions from the top priority units to plan and schedule the completion of unit based risk
assessments. Also, the peer champions will work with their managers to introduce safety
huddles to the health care providers on the unit.
Activities Brief Description Completed By
1. Plan Priority Unit Hazard Assessments
Plan and schedule unit based risk assessments for priority units
Program Coordinator with managers and unit-based champions from priority units
2. Conduct Priority Unit Hazard Assessments
Conduct unit based hazard identification and risk assessments
for priority units
Managers
Unit based champions with support of selected unit staff,
Program Coordinator
and/or OH&S staff
3. Communicate Results of Hazard Assessments
Create prioritized list of hazards to be controlled based on results of unit
based assessments.
Communicate results
Managers
Unit based champions with assistance from selected unit staff, Program Coordinator, and/or OH&S staff
4. Introduce Safety Huddles
Plan and deliver training for safety huddles (Safety Huddle training will
be available as an e-learning module and may be introduced as a stand- alone element at any time during
implementation)
Document work procedures as required.
Unit based champions and managers for priority units
5. Communicate Progress
Monitor progress and provide
updates to stakeholders
Program Coordinator with support from HR and/or Communications staff
Activity 1 – Plan Priority Unit Hazard Assessments
The Program Coordinator should meet with the managers and peer champions to review the
process for conducting the unit assessments. Even though the peer champions and managers

Soteria Strains
Implementation and Program Guide
Page 24 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
should have already been trained on hazard identification and risk assessment, they may need
guidance and assistance to conduct the assessment.
The unit assessments should be conducted as soon as possible, taking into account the needs
of patients on the unit and work schedules. Depending on the size of the unit, the risk
assessment may take anywhere from 3-4 hours, plus time to collect relevant data and review
the results.
Refer to “Section 2.2 – Unit Assessments” in the program guide for more information on
identifying hazards and assessing risk associated with patient handling tasks.
Activity 2 – Conduct Priority Unit Assessments
The unit assessments have three basic components:
1) Gather and review unit specific data
2) Identify patient handling hazards (high risk tasks) on the specific unit
3) Assess the risk for each of the identified hazards
This will allow the manager, unit champion, and participating health care workers to create a
prioritized list of hazards and potential controls for those hazards. It is important at this stage to
understand two things. First, there may be multiple hazards that all have the highest level of risk
associated with them, and it may not be possible to implement controls for all of these hazards.
Second, there may be high risk hazards that need to be controlled, but doing so may take a
great deal of time or be prohibitively costly. In some cases, there may be no known way to
control the hazard. So even though these hazards do need to be addressed, they may require
further study or need to be put into a long-term planning cycle. As a result, lower risk hazards
may become a higher priority at the unit level.
Hazards rated as low-to-medium risk can often be controlled simply and immediately. These
may be dealt with before others are considered or while planning to implement more
complicated controls.
Finally, when prioritizing hazards for controls, it is vital to take into account the issues and
concerns raised by health care workers on the unit. These issues may not always present the
highest risk of injury to staff or patients, however, if no action is taken worker’s level of
engagement may be negatively impacted. This could interfere with future efforts to control
exposure to high risk hazards.
Refer to “Section 2.2 – Unit Assessments” for detailed steps on completing the assessments as
well as a template for documenting results.

Soteria Strains
Implementation and Program Guide
Page 25 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 3 – Communicate Results of Hazard Assessments
Once the Unit Assessment is complete and a list of hazards created and prioritized for control, it
is important to share this information with all of the health care workers on the unit. A variety of
methods should be used to communicate this information and explain why specific hazards
were selected as priorities. This information should be shared during a meeting of all unit staff,
but, alternatively, it could be shared in small group meetings or one-on-one discussions.
Managers and peer champions should resist the urge to communicate this information via email
or by posting a notice on a bulletin board. Emails and notices can be used in conjunction with
meetings, but should not be used as a primary means of communicating this information.
Communications can be developed based on processes and documents generated from
templates in “Section 2.2 –Unit Assessments”. Also, the wrap-up meeting that occurs after the
site visit (see section 2.2) provides an excellent opportunity to communicate early findings to the
participating health care workers.
Activity 4 - Introduce Safety Huddles
Safety huddles help create a culture of performance excellence and continuous learning and
improvement. Often safety issues related to patient handling and mobility are not captured in
incident reports. Without knowing what the issues are, it is impossible to take corrective action.
Safety huddles provide managers and staff a means to share information about the current state
of the unit, discuss safety related concerns, and highlight any new or ongoing issues and how
they can be addressed.
Safety huddles offer health care providers an opportunity to discuss and address safety
concerns they have seen on their units/departments to prevent incidents or near misses in the
future. These huddles with the inter-professional team are held at the same time each day and
typically take as little as 15 minutes to complete. Safety issues raised may include:
New bariatric patients
Significant patient status changes that may result in:
o the need to change how they are handled/moved
o increased risk of falls, etc.
equipment/device issues
environmental concerns
staffing complements
Safety Huddle training will be available as an e-learning module and may be introduced as a
stand-alone element at any time during implementation. After a unit assessment is complete,
safety huddles should be regularly conducted in the unit and any issues not previously identified

Soteria Strains
Implementation and Program Guide
Page 26 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
should be documented. This information may be used to adjust the list of priority hazards or
they may help guide the selection of controls for these hazards.
Guidance on how to run effective safety huddles and how to document issues arising from them
can be found in section 3.4 of the program guide as well as the e-learning module.
Activity 5 – Communicate Progress
The Senior Leader Champion and, the Program Coordinator should review the steps outlined in
Activities 1-4 to determine which steps have been completed, those that are in process, and any
that have been missed or were considered complete, but not implemented fully. They might:
Review the planning process used for the unit assessments to identify if anything was
missed or could be improved. This should be done in conjunction with the unit manager
and peer champions.
Review the assessment process with the unit manager and peer champions to see if
anything was missed or could be improved.
Talk with staff on the unit to find out what they feel about how the assessment was
conducted, whether they understand why and how the assessment was conducted,
whether there was adequate opportunity for staff to express their opinions, if the results
of the assessment were effectively communicated to the staff, and if they were satisfied
with the results.
Meet with the manager and peer champions to learn what they know about safety
huddles and how they are being used on the unit. If there are concerns, discuss how
safety huddles can be improved
After the review is completed the Senior Leader Champion and/or Program Coordinator should
inform all stakeholders of results and next steps.

Soteria Strains
Implementation and Program Guide
Page 27 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Phase 4 – Implementing Controls in Priority Areas
In Phase 4 the Program Coordinator will work with the unit peer champions, managers, and
selected staff to identify the controls needed to reduce the risk associated with each hazard.
These controls should then be approved, or alternative controls selected, and implemented.
When implementing controls, it is important to recognize that control related policies and/or
procedures will need to be created, and staff will need training related to the control (to
understand new policy/procedures, to follow new work method/reporting procedures, to use new
techniques and/or pieces of equipment, etc.) As such, it is essential to create an
implementation plan that helps ensure controls are effective and employees are ready and able
to use them. This plan should be communicated to required stakeholders.
Activities Brief Description Completed By
1. Identify Hazard Controls for Priority Units
Identify hazard controls based on the results of the unit assessments
Managers
Unit champions
Select staff from each unit,
Support from:
Program Coordinator and/or
OH&S and HR as required
2. Approve Hazard Controls for Priority Units
Review and approve controls for implementation
Communicate results
Manager/senior leader with required budgetary/fiscal accountability; with input from the Program Coordinator, the Safe Patient Handling and Mobility Program Coordinating Committee and others (e.g., purchasing, facilities, HR)

Soteria Strains
Implementation and Program Guide
Page 28 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
3. Plan Implementation of Hazard Controls and Training
Plan for implementation of controls including, if necessary, testing and
trialing
Plan for training – Unit based champions (Safe patient handling
Trainer Module)
Plan for training – Managers and Health care Workers (Safe patient handling
Module)
Managers
Unit-based champions
Support from:
selected health care workers from units
Program Coordinator
4. Implement Hazard Controls
Implement identified controls
Monitor implementation process
Create and approve all required control-related policies and procedures
Train unit-based champions to provide
hazard control training
Facilities
Purchasing
Suppliers
Managers
Unit-based champions
Support from:
Program Coordinator
OH&S, and/or HR
5. Conduct Hazard Controls Training
Train health care workers in units where
controls are being implemented
Program Coordinator and/or
Unit-based champions and/or
Equipment suppliers and/or
OH&S staff and/or
HR staff
6. Communicate
Progress
Monitor progress and provide updates
to stakeholders
Program Coordinator
Support from:
OH&S staff and/or
HR and/or
Communications staff
Activity 1 – Identify Hazard Controls for Priority Units
The Program Coordinator should work with the unit manager and peer champions to identify
possible controls for each of the prioritized hazards identified. Ideally, one or more additional
staff members from the unit should assist with this process.
The peer champions should review the basic concepts of hazard control and risk mitigation with
all participants before looking for effective controls. The team working to identify controls should,
at a minimum, understand the hierarchy of controls. Controls can be grouped into four
categories:

Soteria Strains
Implementation and Program Guide
Page 29 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Elimination
Substitution
Engineering
Administrative
Personal Protective Equipment (PPE)
Controls should only be selected from a category if options in a higher category are not
possible. Therefore, when selecting controls, eliminating the hazard should be considered first.
If elimination and substitution is not possible engineering controls (such as equipment or task
redesign) should be considered next. Administrative and PPE controls should only be
considered if engineering solutions are not possible. Note that all engineering controls require
training (an administrative control).
Categories of the hierarchy of controls are described further in “Soteria Strains Safe Patient
Handling and Mobility Program Guide, Section 3.1 - Selecting Controls”.
Refer to “Soteria Strains Safe Patient Handling and Mobility Program Guide, Section 3 -
Planning and Implementing Controls” for more details on identifying, selecting and prioritizing
controls for hazards.
Activity 2 – Approve Hazard Controls for Priority Units
The Program Coordinator should review the list of recommended hazard controls and provide
the Safe Patient Handling and Mobility Program Coordinating Committee and any other
appropriate departmental representatives (OH&S, HR, facilities, etc.) with an opportunity to
comment.
Based on the results of the review process, the Program Coordinator should, if necessary,
modify the list of recommended controls. This list and the specific reasons for changes should
then be discussed with the unit manager and peer champions.
The final list of recommended controls should be presented to the Senior Leader Champion and
then to the facility/organization’s senior leader team for approval.
All health care workers on the unit should be informed of the approved controls. Ideally this
should be done by having the manager and/or peer champions meet with all staff to review the
list of approved controls. They should be prepared to answer questions about why specific
controls were selected and the next steps in the process for implementing controls.

Soteria Strains
Implementation and Program Guide
Page 30 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 3 – Plan Implementation of Hazard Controls and Training
During this activity, the Program Coordinator develops a plan for implementing the approved
controls, working with the unit manager, peer champions and others such as OH&S and/or HR
staff, quality, risk and patient safety, facility engineering and procurement. The plan should be
developed, documented and shared with the unit and support team. The plan will change over
time and changes should be tracked and updated. The most recent version of the plan should
always be available to the team. The plan should include:
A complete list of requirements; this will be largely complete from previous steps and
should be refined at this stage.
Constraints such as budget limits, timelines and scheduling issues that cannot be easily
altered.
A breakdown of activities/steps to complete, described in a logical order (i.e. procure
equipment, install equipment, inspect equipment, train staff).
When refining the requirements list for each control, consider whether more research or
investigation is required. Some examples include:
When equipment is recommended, is it clear exactly what piece of equipment is
needed?
If a work area needs to be modified, is it clear which work area(s) are involved and what
the specific modifications are?
If additional staff training is recommended, is it clear exactly what the goals of the
training are?
Other questions to consider when refining the requirements list are:
Does the control require significant redesign or layout modifications of the unit or
associated work areas?
Will a new policy be required to support the implementation and/or use of the control?
Will a new work procedure be required to support the implementation and/or use of the
control?
Will staff training be required so that the control can be used effectively?
Will required equipment have to be tendered and/or trialed before purchase?
Will the installation or implementation of the control interfere with the delivery of care on
the unit?

Soteria Strains
Implementation and Program Guide
Page 31 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Possible points to consider when listing constraints include:
budget
patient care issues
bed utilization/patient flow
facility age/design/size
timelines
Infection Prevention and Control
number of and schedules of healthcare workers on unit
other projects or initiatives
Some points to consider when defining and sequencing activities:
For equipment, it is important to know exactly what type, make and/or model of
equipment is needed. Refer to Soteria Strains Safe Patient Handling and Mobility
Program Guide Section 3.2 - Equipment Selection for a process to test or trial various
types of equipment.
Frontline health care workers need to be actively involved and engaged when:
o testing or trialing equipment
o modifications to the work space or workstation are identified
o when developing new policies, procedures, and work methods
Include time and resources for effective and meaningful staff consultation and
engagement. Staff engagement, while time consuming, can help avoid problems and
frustrations because workers, as the experts on how their jobs are done, are able to
identify concerns and possible solutions early in the selection, design, or writing phase.
Facility/Engineering should be involved when significant design changes are required.
Also, refer to Soteria Strains Safe Patient Handling and Mobility Program Guide Section
3.5 - Facility Design.
Consider the possible presence of asbestos-containing materials and/or inadequate
structural elements when installing any equipment.

Soteria Strains
Implementation and Program Guide
Page 32 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
It is important to communicate the plan and all changes to frontline health care workers, senior
leadership, and others in the organization. Refer to Soteria Strains Safe Patient Handling and
Mobility Program Guide Section 1.4 - Communications, Promotion, and Engagement for
information about creating a communication plan.
Activity 4 – Implement Hazard Controls
Once a plan for implementing approved control(s) is completed, the next step is to put the plan
into action. The Program Coordinator should monitor the implementation plan to ensure it is
being followed, identify and work to resolve any barriers, and keep the unit managers and peer
champions informed about progress. If barriers do arise, the Program Coordinator should meet
with appropriate staff to resolve and overcome them. If changes to the implementation plan are
required, the Program Coordinator should get approval for these changes and ensure that
everyone is informed about them.
The Program Coordinator should make sure all necessary departments are consulted with and
that the planned staff involvement and engagement takes place. If installing equipment the
Program Coordinator should also verify that the make, model, and type of equipment is correct
before it is installed, and ensure it is being installed where and when it should be. It is also
important that the Program Coordinator work with health care workers from the unit and OH&S
to make certain any new hazards created during implementation or installation are identified and
controlled.
Create and Approve Required Policies and Procedures
When the implementation plan for approved controls is finalized, it will specify what, if any, new
policies and/or procedures will need to be created and approved. As this can be a time
consuming process, work should begin on these as soon as possible. Most organizations will
already have a process for the creation and approval of new policies and procedures and, if so,
this process should be followed. Some additional things to consider:
Who should be on the team that creates the policy and/or procedure? The team should
include members of the Multi-stakeholder Safe Patient Handling and Mobility Steering
Committee plus any other people (as needed) from other areas not already represented.
Will feedback be obtained on the policy or procedure? If so, how, when, and from
whom?
How will the new policy and procedure be communicated? How and when will staff be
trained on the details, requirements, responsibilities, expectations, and accountabilities
related to the new policy and/or procedure?

Soteria Strains
Implementation and Program Guide
Page 33 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Train Unit Peer Champions to Provide Hazard Control Training
Unit peer champions will provide training on safe patient handling and mobility to colleagues on
their units. As controls are being implemented, the champions should complete their training.
In this phase, unit peer champions require training on:
Safe patient handling and mobility principles and selection criteria for assessment
methods including patient risk profiles and the point-of-care mobility status check
(PACE).
After Action Reviews.
How to facilitate training sessions for their peers.
Activity 5 – Conduct Hazard Controls Training
Perform Assessments – Patient Risk Profile
An important element of an effective safe patient handling program is the use of patient risk
profiles, which are used as a baseline for identifying how to safely lift, transfer, and reposition a
patient. These profiles capture key information about the patient at various times during the
patient’s stay on a unit or facility.
See section 2.3 - Patient Risk Profile of the Soteria Strains Safe Patient Handling and Mobility
Program Guide for details on how to complete the patient risk profile.
Points to consider:
Documentation of the patient risk profiles should move with patients as they move
between different units in the facility or are transferred to another facility. Patient risk
profiles should be updated as the patients’ status changes.
Refer to Section 2.3 - Patient Risk Profile of the Soteria Strains Safe Patient Handling
and Mobility Program Guide for details of the assessment.
The patient risk profile can help determine the specific types of lifts, transfers, or
repositioning techniques required. It will also indicate if specialized equipment is required
(e.g., bariatric lift and sling, non-standard beds). Without this information, care staff may
be at an increased risk of injury because the equipment and special instructions needed
for safe lifts or transfers is not available when needed.

Soteria Strains
Implementation and Program Guide
Page 34 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Complete Point-of-Care Mobility Status Check (PACE)
The Point-of-Care Mobility Status Check (PACE) is another vital element of a successful safe
patient handling program; it is related to the patient risk profile, but is used by all health care
workers that need to lift, transfer and/or reposition, a patient.
The PACE Mobility Status Check comprises is divided into four sections that health care
workers need to consider prior to making the decision to engage in any patient handling and
mobility activity. These are:
Physical: the patient’s current physical status (strength, balance, etc.).
Agitation/Aggression: is the patient agitated or displaying aggressive behavior, or does the patient have a history of aggressive behavior.
Communication: is the patient able to respond to simple questions and follow instructions.
Environment: is the environment (work space/area, floor, access, obstructions, etc.) safe for patient handling whether the patient is able to fully assist with the transfer or if equipment is used to perform the handling task
Health care workers will be trained on how to use this tool, which takes staff through a series of
questions that determine if a condition is “Green,” “Yellow,” or “Red”. If any “Red” conditions are
found, then the care provider needs to determine a safe way to lift, transfer, or reposition the
patient.
The PACE should be conducted by all care staff every time they are required to lift, transfer, or
reposition a patient. Results of the PACE will inform health care workers choices regarding the
approach to a patient handling or mobility task. A more conservative approach and/or further
assessment may be required based on changes to the patient’s physical or cognitive status. Or,
the patient’s environment might have changed (e.g., a new piece of medical equipment or
furniture has been brought into the patient’s room) that may create increased risk to the health
care worker or patient.
As noted, if the outcome of the PACE Assessment conflicts with the patient’s current safe lift,
transfer, and repositioning plan, then the health care provider should err on the side of caution,
use the safest method to perform the lift or transfer, and collaborate with their co-workers, unit
peer champions, and manager to revise the lift and transfer plan. The manager should, if
required, arrange for another mobility assessment to be completed.
See Point-of-Care Mobility Status Check (PACE) in the Soteria Strains Safe Patient Handling
and Mobility Program Guide for more information.

Soteria Strains
Implementation and Program Guide
Page 35 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Train Workers on New Controls
Health care workers will need to be trained on any newly implemented control. They might need
to be trained on how to safely and effectively use a new piece of patient handling equipment. It
could be that they also need to be trained on new work methods, assessment protocols, or
reporting procedures. And, of course, they will need to be informed and trained on any new
policies or procedures created.
For equipment related controls, it is often possible to begin training unit staff on how to use
specific pieces of equipment before this equipment is actually installed on the unit. For instance,
if the equipment exists in other units, then these units could be used to train staff prior to the
equipment being installed on their own unit. Or, if space exists, it may be possible to have
equipment installed in a testing /training room so that staff can be trained and provided with
refresher training as needed. Finally, if the organization has multiple facilities some of which are
already using the specific equipment, then it might be possible to provide training to staff in one
or more of these facilities.
No matter the circumstances, because there will always be a training element associated with
new controls, it is vital to plan for how training will be delivered in a timely and efficient manner.
For each element of training required, these questions need to be answered:
What are the goals, objectives, and content of the training?
Who needs to be trained? Only health care workers, Managers, Directors, VPs and
senior leadership? Any others?
When will the training take place and how long will the training session last? How will
affected units cover for employees who are participating in the training?
Where will the training take place? Will all required resources to support the training
(equipment, accessories, mock patients, seating, LCD projector, etc.) be available and is
in the training area/room? Will the training interfere, directly or indirectly, with patient-
care activities, and if so, how will this interference be mitigated?
Does the training area have sufficient space to safely practice patient lifts, transfers,
and/or repositioning tasks and other related activities?
Refer to Section 3.6 - Training of the Soteria Strains Safe Patient Handling and Mobility
Program Guide for more information and training materials
Training programs include a process for monitoring and evaluating, or at least auditing, the
effectiveness of the training. This allows instructors to know if participants have learned and
understood the information presented to them. Competence measures for safe work techniques
and use of assessment tools are included with the training material. Participants in any of the
training sessions should also leave the training confident that they know how to apply the
knowledge and/or skills they have been taught.

Soteria Strains
Implementation and Program Guide
Page 36 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
The program evaluation framework includes on-the-job observations to verify that participants
from each training session are correctly applying what they have learned when they are
delivering care. During these observations the level of support for using the new knowledge or
skills should be identified. Indicators that physical or organizational barriers are preventing staff
from using new skills/knowledge should also be identified.
Activity 6 – Communicate Progress
The Senior Leader Champion and, the Program Coordinator should review the steps outlined in
Activities 1-5 to determine which steps have been completed, those that are in process, and any
that have been missed or were considered complete, but not implemented fully. They might:
Review the process used to identify, prioritize, review, and approve controls to identify if
anything was overlooked or could be improved. This should be done in conjunction with
the unit manager and peer champions. As well, reviewers must ensure that results were
communicated to unit staff and others as appropriate.
Review the process used to plan for the implementation of approved controls to identify
gaps and areas for enhancement. This should be done in conjunction with the unit
manager and peer champions. It is important to ensure that adequate
consultation/engagement opportunities were provided and that the results were
communicated to unit staff and others as appropriate.
Assess how well the plan for implementation of approved controls was followed, if any
issues or barriers were identified, and, if so, how they were overcome. Ensure that the
process used to create and approve required policies and procedures was appropriate
and inclusive.
Verify that all health care workers were provided with training on how to use any
implemented controls. Talk to staff, managers, and peer champions to find out if the
training met their needs and allowed them to safely utilize the control(s). If there are
concerns, then discuss how they can be addressed.
Verify that all health care workers were provided with training on the patient risk profile
and the PACE Assessment tool. Talk to staff, managers, and peer champions to find out
if the training met their needs. Verify that the patient risk profiles and PACE
assessments are being used as intended. If there are concerns, then discuss how these
can be addressed.
After the review is completed the Senior Leader Champion and/or Program Coordinator should
inform all stakeholders of results and next steps.

Soteria Strains
Implementation and Program Guide
Page 37 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Phase 5 – Initiate Audit Phase
Once a decision has been made to implement a particular control, the implementation process
must be monitored to ensure that equipment is being installed correctly (right equipment, in the
right place, with the necessary accessories, etc.) and the design of new work methods or
processes are effective. After Action Reviews (AARs) are a similar process to safety huddles as
they both involve brief team meetings focused on learning and sharing information. However,
safety huddles typically occur at regularly scheduled intervals (e.g., beginning of shift or hand
over) while AARs occur as a result of an action or activity. Refer to Section 3.4 – Safety Huddles
of the Soteria Strains Safe Patient Handling and Mobility Program Guide for more information.
Activities Brief Description Completed By
1. Audit Implementation Progress
Audit progress and success of implementation in priority units
● Program Coordinator with support of unit managers and unit peer champions
2. Identify Issues and Potential Improvements
Identify areas for improvement / additional actions in priority units
● Program Coordinator with support of unit managers and unit peer champions
3. Introduce After Action Reviews
Plan and execute training for After Action Reviews
Document work policy/procedures as required
Note: After Action Reviews may be introduced as a stand-alone element at any time after safety
huddles have been implemented.
● Unit peer champions with support of unit managers
4. Communicate Progress
Document results and report progress to stakeholders
● Program Coordinator with support of HR and/or Communications
Activity 1 - Audit implementation Progress
While continuous improvement activities should be ongoing throughout implementation, this
step is an opportunity to formally review evaluation data and lessons learned. A review of key
performance indicators, previous communications from all phases of implementation, and the
organizational gap analysis should be considered. For an organization, this is an opportunity to
ensure the lessons learned from the current priority areas are applied to improve
implementation/roll-out in other areas. Refer to Section 1.3 - Evaluation and Continuous
Improvement of the Soteria Strains Safe Patient Handling and Mobility Program Guide for more
information.

Soteria Strains
Implementation and Program Guide
Page 38 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 2 - Identify Issues and Potential Improvements
Through the audit process there will be issues such as the use of inadequate or incorrect
equipment, missed training, and incomplete evaluation components. In general terms, the
issues identified will apply directly to a specific unit and how roll-out of the program has
occurred thus far.
Also important during this activity is identifying areas for process improvement. Opportunities to
streamline and improve processes should be identified and prioritized. Process improvements
may be identified that pertain mostly at the unit level; however, they may also apply to
organization-wide processes and/or be applicable to other units and should be captured,
communicated, and executed in a way to be helpful to the organization and other units.
Activity 3 – Introduce After Action Reviews
After Action Reviews are similar to the safety huddles introduced in phase 3; during After Action
Reviews, health care workers immediately assess a situation or event to review what happened,
what should have happened, what accounted for the difference, and what recommendations
could be made for improvement or to prevent a similar event from occurring (or
recommendations to continue/share if the outcome was positive). They may help inform a
formal investigation/root-cause analysis, but should not be considered a replacement for these
processes when an incident dictates the requirement of formal investigation.
An After Action Review is centered around four questions:
1) What was expected to happen?
2) What actually occurred?
3) What went well and why?
4) What can be improved and how?
Teams should be proficient, comfortable, and consistent with executing safety huddles before
introducing training for After Action Reviews. Refer to Section 3.4 – Safety Huddles of the
Soteria Strains Safe Patient Handling and Mobility Program Guide for more information.
Activity 4 – Communicate Progress
The Senior Leader Champion and, the Program Coordinator should review the steps outlined in
Activities 1-3 to determine which steps have been completed, those that are in process, and any
that have been missed or were considered complete, but not implemented fully. They might:
Ensure an audit of the implementation to date has been completed includes a review of
relevant evaluation data, progress reports, and lessons learned

Soteria Strains
Implementation and Program Guide
Page 39 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Verify that units are competent, comfortable, and consistent in their use of safety
huddles prior to introducing After Action Reviews
Identify a priority list of issues to be assigned and/or escalated for planning
Ensure training for After Action Reviews has occurred
After the review is completed the Senior Leader Champion and/or Program Coordinator should
inform all stakeholders of results and next steps.
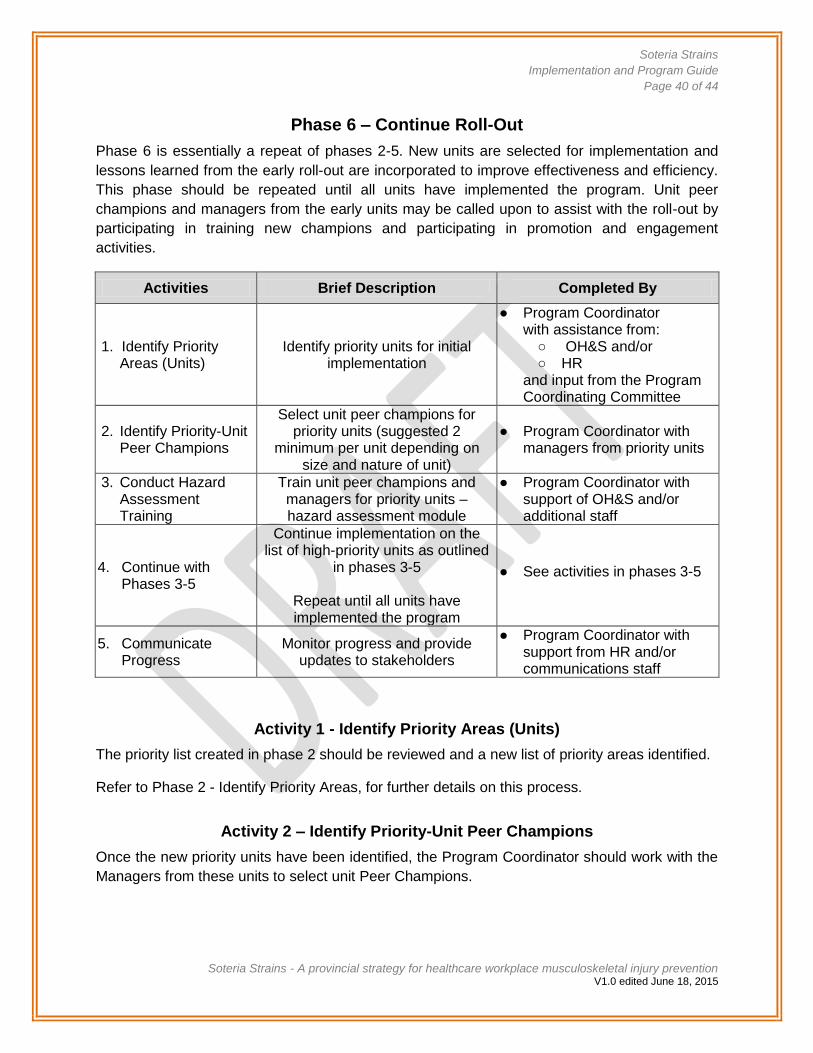
Soteria Strains
Implementation and Program Guide
Page 40 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Phase 6 – Continue Roll-Out
Phase 6 is essentially a repeat of phases 2-5. New units are selected for implementation and
lessons learned from the early roll-out are incorporated to improve effectiveness and efficiency.
This phase should be repeated until all units have implemented the program. Unit peer
champions and managers from the early units may be called upon to assist with the roll-out by
participating in training new champions and participating in promotion and engagement
activities.
Activities Brief Description Completed By
1. Identify Priority Areas (Units)
Identify priority units for initial implementation
● Program Coordinator with assistance from:
○ OH&S and/or ○ HR
and input from the Program Coordinating Committee
2. Identify Priority-Unit Peer Champions
Select unit peer champions for priority units (suggested 2
minimum per unit depending on size and nature of unit)
● Program Coordinator with managers from priority units
3. Conduct Hazard Assessment Training
Train unit peer champions and managers for priority units – hazard assessment module
● Program Coordinator with support of OH&S and/or additional staff
4. Continue with Phases 3-5
Continue implementation on the list of high-priority units as outlined
in phases 3-5
Repeat until all units have implemented the program
● See activities in phases 3-5
5. Communicate Progress
Monitor progress and provide updates to stakeholders
● Program Coordinator with support from HR and/or communications staff
Activity 1 - Identify Priority Areas (Units)
The priority list created in phase 2 should be reviewed and a new list of priority areas identified.
Refer to Phase 2 - Identify Priority Areas, for further details on this process.
Activity 2 – Identify Priority-Unit Peer Champions
Once the new priority units have been identified, the Program Coordinator should work with the
Managers from these units to select unit Peer Champions.

Soteria Strains
Implementation and Program Guide
Page 41 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Activity 3 – Conduct Hazard Assessment Training
The peer champions and managers from the new priority units will need to be trained so that
they can properly fulfill their role and responsibilities. A plan will need to be put in place to allow
this training to be delivered in a timely manner. Managers and peer champions from units that
have already implemented the program may be called upon as resources for training and
communicating lessons learned. For more details on this process, see phase 2.
Activity 4 – Continue with Phases 3-5
The new priority units should continue with implementing the program as outlined in phases 3-5
of this document.
Activity 5 – Communicate Progress
The Senior Leader Champion and the Program Coordinator should review the steps outlined in
Activities 1-4 to determine which steps have been completed, those that are in process, and any
that have been missed or were considered complete, but not implemented fully. Such as:
New priority areas have been identified
Unit champions have been selected from the new priority areas
Training for hazard assessment has been planned and executed
Phases 2-5 continue to be executed
After the review is completed the Senior Leader Champion and/or Program Coordinator should
inform all stakeholders of results and next steps.

Soteria Strains
Implementation and Program Guide
Page 42 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Phase 7 – Ensure Ongoing Improvement
When implementing change, it is often thought a program may not require as much effort once it
is up and running. The opposite is true – especially for leaders. To ensure the program has
long-term impact, it is important to:
Provide support post-implementation.
Understand things that just need more time vs. things that need to be modified vs.
issues of simple resistance.
Understand the importance organizational leader’s play in ensuring change is sustained.
Celebrate overall success and milestones along the way.
Phase 7 is where the extra push to transform and reinforce change is undertaken. As well, this
phase is another stage of continuous improvement. The emphasis is on sustaining the
organization-wide and system-level improvements post-implementation.
Activities Brief Description Completed By
1. Monitor Program Elements
Monitor elements of safe patient handling and mobility program when implemented in one or more units, as per evaluation framework previously established
● Program Coordinator with support of unit managers and unit peer champions
2. Undertake Formal Program Review
Conduct a formal review of the program at least once a year after initial implementation
● Program Coordinator with support of unit managers and unit peer champions
3. Implement Changes as Required by Review
Identify additional organizational and/or system issues that could be improved to reduce the risk associated with patient handling and mobility tasks
● Program Coordinator with support of HR and/or Communications
4. Communicate Progress
Document results, identify improvement opportunities, and report progress to stakeholders
● Unit peer champions with support of unit managers
Activity 1 - Monitor Program Elements
Once the program has been implemented in one or more units the emphasis shifts from
evaluating implementation to evaluating processes. In other words, the questions needing
answers change from “How have we implemented the program?” to “How do we improve the
processes?” Many of the specific evaluation questions will be the same or very similar, some
will be new, and others will no longer be relevant. As more units come online with the program,
the monitoring and reporting should reflect these units.

Soteria Strains
Implementation and Program Guide
Page 43 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
The monitoring and evaluation framework are designed and implemented in phase 1. Refer to
Section 1.3 – Evaluation and Continuous Improvement of the Soteria Strains Safe Patient
Handling and Mobility Program Guide for more details on the differences between evaluating
implementation and process. It is important to remember at this stage many of the questions the
evaluation framework is designed to address cannot yet be answered. It will take time to get to
the point where outcome questions like “What is the effect on injury rates?” will have an answer.
Activity 2 – Undertake Formal Program Review
A formal annual review is necessary to understand how the program is being sustained and
improved over time. Also, it will assist with transparency and accountability to funders and other
stakeholders. Using the evaluation framework and data collected over the course of the year will
be helpful in learning how the program has been accepted in the organization and help with
identifying unresolved issues and areas for improvement. As well, this formal review allows for a
look at issues that may be having a broad impact on the organization such as accountability
frameworks, data management, funding and/or other related processes.
Refer to Section 1.3 – Evaluation and Continuous Improvement of the Soteria Strains Safe
Patient Handling and Mobility Program Guide for details of what to include in the formal audit.
Activity 3 - Implement Changes Required by Review
Unresolved issues and areas for improvement should be prioritized. Assessing the risk related
to these issues is a good way to prioritize and allows for comparison between other
organizational risks such as financial, strategic, patient satisfaction, care quality, reputational,
and legal if a similar process is used for managing these risks.
Risk-exposure scores can be assigned to each issue or area for improvement. This involves
attributing a number to each issue that ranges from 1-5 in two categories, impact and
probability.
The first category, probability, identifies the likelihood that not addressing the issue will put
individuals (or the organization) at risk.
The second category, impact, assesses the potential extent of the harm that will arise from not
addressing an issue.
The scores can be generated through consensus during a group meeting, by averaging results
from surveys/interviews, or a combination of these.
Soteria Strains
Implementation and Program Guide
Page 44 of 44
Soteria Strains - A provincial strategy for healthcare workplace musculoskeletal injury prevention V1.0 edited June 18, 2015
Multiplying the two scores for each category (impact and probability) will provide an exposure
score to use in prioritizing how the issues are addressed.
Probability x Impact = Exposure
For reference:
1 = low
3 = moderate
5 = high
Therefore, a higher-exposure score would be prioritized ahead of a lower-exposure score.
There are likely to be issues with high-exposure scores that are complex in nature and/or cost
prohibitive to address. It is important to begin plans for addressing these issues. While this
planning occurs, issues that have a lower-exposure score but are simpler to resolve should be
addressed.
Activity 4 – Communicate Progress
The Senior Leader Champion and, the Program Coordinator should review the steps outlined in
Activities 1-3 to determine which steps have been completed, those that are in process, and any
that have been missed or were considered complete, but not implemented fully. They might
ensure:
Monitoring and evaluation is being completed as intended
Formal program audit/reviews are scheduled and completed annually
Issues and areas for improvement identified in the audit are addressed
After the review is completed the Senior Leader Champion and/or Program Coordinator should
inform all stakeholders of results and next steps.