Immunotherapy with Blinatumomabsbtmo2018.com.br/.../uploads/2018/08/02-08-13H05-PETER-BADER-… ·...
37
Immunotherapy with Blinatumomab What are the possibilities? Peter Bader SBTMO 2018 – ALL Satellite Symposium “Role of MRD and Immunotherapy in Optimizing ALL Treatment Outcomes” Rio de Janeiro, August 2 nd , 2018
Transcript of Immunotherapy with Blinatumomabsbtmo2018.com.br/.../uploads/2018/08/02-08-13H05-PETER-BADER-… ·...

Immunotherapy with BlinatumomabWhat are the possibilities?
Peter Bader
SBTMO 2018 – ALL Satellite Symposium
“Role of MRD and Immunotherapy in Optimizing ALL Treatment Outcomes”
Rio de Janeiro, August 2nd, 2018

2
Objectives
Refractory ALL
Blinatumomab, Product, clinical development
Blinatumomab in Children and Adults
TOWER Study; BLAST Study, AND RIALTO Study
Own data in 18 children
Present data from TOWER (AllHSCT in adults with R/R ALL from Phase 3

3
Poor Outcome for Patients with r/r pB-ALL
Pediatric patients Adult patients
Standard pB-ALL
CR with frontline chemo 98-99% 85-90%
relapse 15-20% 30-50%
Long-term survival after
early relapses
late relapses
25%
50-60%
8%
24%
r/r pB-ALL
Median OS with chemo only - 4.5-8.4 months
5y-median OS with chemo only - 7-10%
Median OS after chemo only - 10 months
Median OS after HSCT 7.4 months 5.8 months
New agents with reduced toxicity are needed to improve outcomes for patients with r/r pB-ALL

4
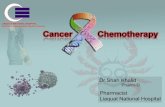
Bispecific T-Cell Engager: Blinatumomab
Nagorsen et al. Leuk & Lymph 2009
Baeuerle P.A. et al. Cancer Res. 2009
Bargou R. et al. Science 2008
Topp M.S. et al. Lancet Oncol. 2015
Activation signals promote CTC proliferation
Klinger M. et al.
Blood 2012
Serial lysis of CD19+ B cells
Hoffmann P. et al.
Int J Cancer 2005

5Nagorsen et al. 2012
Blinatumomab – Mode of Action

6
Blinatumomab – Clinical Develpoment
Nagorsen et al. 2012

© Amgen Inc. All Rights Reserved.
A Phase 3, Randomized, Open Label Study
Investigating the Efficacy of the BiTE Antibody
Blinatumomab Versus Standard of Care
Chemotherapy in Adult Subjects With
Relapsed/Refractory B-precursor Acute
Lymphoblastic Leukemia (ALL)
Study (TOWER) – NCT02013167

8
TOWER Study in Adult r/r pB-ALLS
cre
enin
g/P
re-p
hase
Safe
ty f
ollo
w-u
p
Blinatumomab
cIV infusion
4 weeks on
2 weeks off
2 cycles
SOC
chemotherapy
2 cycles
Consolidation3 cycles
Maintenance 12 months
Ra
nd
om
iza
tio
n

© Amgen Inc. All Rights Reserved.
BLAST: A Confirmatory, Single-Arm, Phase 2
Study of Blinatumomab, a Bispecific T-Cell
Engager (BiTE) Antibody Construct, in
Patients with Minimal Residual Disease B-
Precursor Acute Lymphoblastic Leukemia
(ALL)
Study (BLAST) – NCT01207388

10
BLAST Study in Adult r/r pB-ALL, MRD-basedS
cre
enin
g/P
re-p
hase
Safe
ty fo
llow
-up
Long-t
erm
follo
w-u
pBlinatumomab15 μg/m2 cIV infusion
i.th. prophylaxis
4 weeks on
2 weeks off
Up to 4 cycles
HSCT offered to patiens in CR

© Amgen Inc. All Rights Reserved.
Open-label, multicentre, expanded
access study of blinatumomab* in
paediatric and adolescent patients
with relapsed/refractory B-precursor ALL
Study 320 (RIALTO) – NCT02187354
*Blinatumomab is not licensed for use in paediatric patients in the EU
SC-EU-AMG103-00339-06.17
SC-DE-AMG103-00140

12
RIALTO Study in r/r pB-ALLS
cre
enin
g/P
re-p
hase
Safe
ty fo
llow
-up
Long-t
erm
follo
w-u
pBlinatumomab
cIV infusion
4 weeks on
2 weeks off
Up to 5 cycles
HSCT offered to patiens in CR

13
Key Eligibility Criteria
TOWER Study BLAST Study RIALTO Study
Age ≥18 y ≥ 18 y >28 d and <18 y
CD19+ pB-ALL with≥5% blasts in BM
x x
CD19+ pB-ALL with
<5% blasts in BMMRD ≥10E-4 (- ≥10E-3)
x
Ph negative x x x
2nd or later relapse,
any rlps. after HSCT,
refractory disease
1st relapse w remisson
duration <12 months
x
x
x
x
(x) x
x
x
Adequate liver function x x x
ECOG status ≤2 0 or 1
No prior HSCT x

14
Key Exclusion Criteria
TOWER Study BLAST Study RIALTO Study
Clinical relevant CNS
pathology
x x x
Isolated extramedullary
disease
x x
Chemotherapy within
2 wk,
Radiotherapy within
2-4 wk
x
x
x
x
x
x
Immunotherapy x
Immunosuppression
within 2 weeks
x x
Auto HSCT within 6 wk
Allo HSCT within 12 wk
x
x
x
x
Grade 2-4 aGVHD,
Active cGVHD
x
x
x
x
Abnormal liver or
renal function
x
x
x
x

15
Study Endpoints
TOWER Study BLAST Study RIALTO Study
Primary endpoint:
Efficacy
OS
Primary endpoint:
Efficacy
MRD response after 1 cycle(MRD neg with sensitivity of at least 10E-4 by PCR in reference lab)
Primary endpoint:
Safety
Treatment-emergent/related AEs
Secondary endpoint:
Efficacy
EFS
Remission rate
Safety
Incidence and severity of AEs
Secondary endpoint:
Efficacy (w/wo HSCT)
RFS
OS
Duration of MRD response
Safety
Incidence and severity of AEs
Secondary endpoint:
Efficacy
CR within first 2 cycles
MRD neg. within first 2 cycles
RFS
OS
Rate of allo-HSCT after CR

16
TOWER Study
Blinatumomab vs. Chemo in Adult-ALL
Hagop Kantarjiann et al. NEJM 2017
Prospective 2:1 randomized trial: n=405
Blina: 271 Chemo: 134
Median OS
Blina: 7.7 mo Chemo: 4.0 mo
CR/Cri (12 weeks):
Blina: 36/44% Chemo: 16/25%
6 months EFS:
Blina: 31% Chemo: 12%
Longer remission duration
Blina: 7.3 mo Chemo: 4.6 mo
AES grade 3
Blina: 87% Chemo: 92%
Treatment with blina resulted in longer OS

17
Zugmaier et al.
Blood 2015
n=36
BLAST Study
Blinatumomab in MRD Positive Adult-ALL

18
BLAST Study
Blinatumomab in MRD Positive Adult-ALL
Zugmaier et al.
Blood 2015
28% achieved an OS of 30 mo
Survival may be associated
with MRD response
n=36

19
Results
Evaluable 113
Median age 45 (18-76) yrs
In 2nd/later CR: 36%
MolCR: 78%
Median OS: 36.5 mo
- Mol CR y/n: 38.9 vs 12.5 mo
Median RFS: 18.9 mo
- Mol CR y/n: 23.6 vs 5.7 mo
- 1st / later CR: 24.6 vs 11 mo
BLAST Study (Follow-up)
Blinatumomab in MRD Positive Adult-ALL
Gökbuget et al.
Blood 2018
MRD response resulted in improved OS and RFS

20
RIALTO Study: Patient Demographics and
Baseline Characteristics
Locatelli F, et al. ASCO 2017; Abstract 10530 and poster presentation.
Characteristic All patients (N=40)
Male, n (%) 19 (48)
Median (range) age, years 9 (1–17)
Age group, n (%)
1 month to <2 years
2 to <12 years
12 to <17 years
5 (13)
20 (50)
15 (38)
Prior relapses, n (%)
0 (primary refractory)
1
≥2
5 (13)
11 (28)
24 (60)
Prior allogeneic HSCT, n (%) 21 (53)
Bone marrow blasts (local), n (%)
<50%
≥50%
22 (55)
18 (45)

21
RIALTO Study: Response Within first 2
Cycles
Locatelli F, et al. ASCO 2017; Abstract 10530 and poster presentation.
Median number of cycles started and completed: 2 (range, 1−5)
All patients (N=40)
n/N1* % 95% CI
CR during the first two cycles
<50% blasts
≥50% blasts
t(17;19)
25/40
15/22
10/18
2/2
63
68
56
100
46–77
45–86
31–79
NA
MRD response during the first two cycles†
<50% blasts
≥50% blasts
t(17;19)
19/25
12/15
7/10
2/2
76
80
70
100
55–91
52–96
35–93
NA
HSCT realisation‡
Allogeneic HSCT after CR
Allogeneic HSCT without CR
10/25
3/14
40
21
21–61
5–51

22
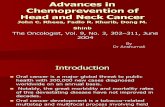
RIALTO Study: Overall Survival
Locatelli F, et al. ASCO 2017; Abstract 10530 and poster presentation.
Censored at time of
allogeneic HSCT N
Median OS,
months
95% CI,
months
Not censored 40 9.8 7.1–NE
Censored 40 8.3 5.4–9.8
181614121086420
0
0
1
0
1
0
1
0
3
1
7
1
12
4
12
4
15
7
16
8
17
9
22
12
30
18
33
25
33
30
37
37
39
39
40
40
0.0
0.2
0.4
0.6
0.8
1.0
Time (months)
Surv
ival pro
babili
ty
Number of subjects at risk:
Median follow-up: 11.8 months
Not censored Censored

Frankfurt Patients (N=18)
N (%) N (%)
Sex
Male
Female
14
4
(78)
(22)
Age
median [range]
13 years
[2 - 20]
Diagnosis
ALL
B-NHL
17
1
(94)
(6)
Number of SCTs before
treatment
0
1
2
7
10
1
(39)
(56)
(6)
Number of relapses before
treatment
1
2
3
4
9
6
2
1
(50)
(33)
(11)
(6)
Number of Blinatumomab
cycles
1
2
11
7
(61)
(39)
Duration of Blinatumomab
cycle
median [range]
28 days
[2-36]

Course after Blinatumomabmedian post treatment observation period: 1.6 years [25 days – 5.5 years]
Response to
BlinatumomabSCT after treatment
Total Yes (%) No (%)
CR (MRD+/-)8 6 (75) 2 (25)
NR10 7 (70) 3 (30)
Total18 13 (72) 5 (28)

Outcome in Patients with SCTs after
Blinatumomabmedian post SCT observation period: 2.5 years [83 days – 5.4 years]
Response to
BlinatumomabOutcome
Total CR (%) Relapse (%) TRM (%)
CR (MRD+/-)6 2 (33) 2 (33) 2 (33)
NR7 3 (43) 3 (43) 1 (14)
Total13 5 (39) 5 (39) 3 (23)

Outcome of patients without SCT (n=5)
Response to
BlinatumomabOutcome
Total CR (%) Lost to
follow-up
(%) Death (%)
CR (MRD+/-)2 2 (100) 0 (0) 0 (0)
NR3 0 (0) 2 (66) 1 (33)
Total5 2 (40) 2 (40) 1 (20)

Outcome of all patients (n=18)median post treatment observation period: 1.6 years [25 days – 5.5 years]
Response to
BlinatumomabOutcome
Total CR (%) Relapse (%) NRM (%) Lost
to FU
(%)
CR 8 4 (50) 2 (25) 2 (25) 0 (0)
NR10 3 (30) 4 (40) 1 (10) 2 (20)
Total18 7 (39) 6 (33) 3 (17) 2 (11)

Overall survival of patients since begin of
treatment with Blinatumomab
Time since begin of treatment (years)
Ove
rall s
urv
iva
l (%
)
0
20
40
60
80
100
2-y-p= 54.6%, 95%-CI: 32.4% - 92.1%
0 1 2 3 4 5 6

Overall survival of patients with CR vs.
patients with NR after treatment with
Blinatumomab
CR includes CR MRD+
Time since end of treatment (years)
Ove
rall s
urv
iva
l (%
)
0
20
40
60
80
100
0 1 2 3 4 5 6
CR: 2-y-p= 71.4%, 95%-CI: 44.7% - 100%
NR: 2-y-p= 45.7%, 95%-CI: 20.3% - 100%

30
Summary Allogeneic SCT remains the gold standard (highest risk, relapsed patients)
Children and adolescents with ALL
CR1: ultra high risk features, persistent MRD
CR2: - late relapses with pers. MRD- early, very early relapse
>CR2: all patients
Level of MRD prior to transplant is a major predictor for outcome
Antibody treatment Remission induction and improvement; reduce toxicity and clear MRD
post transplant
Adult Patients with r/r ALL
High risk for relapse and TRM irrespective of treatment
Patients with persistent remission after Blinatumomab
Efforts are focusing on minimizing the relapse risk by intensifying therapy upfront and by eradicating MRD using the new available immunotherapies e.g. Blinatumomab
Combining all these modalities (new therapies, conventional chemotherapy and HCT) is challenging.

Cooperations
Halvard BönigGerman Red Cross Blood Donor Service Frankfurt/Main, Germany
Winfried S. WelsGeorg-Speyer-Haus, Frankfurt/Main, Germany
PhysiciansMichael MerkerShahrzad BakhtiarEva RettingerAndre WillaschAndrea JarischJan Sörensen
Graft Manipulation,Cell Therapeutics Sabine Huenecke Melanie BremmClaudia CappelVerena PfirrmannSibylle Wehner
Mesenchymal Stroma CellsZyrafete KuçiSelim Kuçi
CIK / T Cell TherapyEva RettingerVerena PfirrmannMichael MerkerLisa-Marie PfeffermannSarah OelsnerVida Meyer Molecular Biology
Andre WillaschChristlinde MauracherGitta NozadFariba SoltaniMiriam StaisHermann Kreyenberg
Pediatric Stem Cell Transplantation & Immunology: Peter Bader / Evelyn Ullrich / Thomas Klingebiel
Clinical Trial OfficeVerena PfirrmannBettina SteinmetzTina Homrighausen
OfficeKirsten Schäfer
NK cells / ExperimentalSara TognarelliJuliane WagnerJochen FrühKatja Thoma
Bio MathematicsEmilia Salzmann-Manrique
Participating Institutions
Düsseldorf, Germany
Roland Meisel
Florian Babor
Friedhelm Schuster
Frankfurt/Main, Germany
Hubert Serve
Gesine Bug
Mainz, Germany
Matthias Theobald
Eva Wagner
Hauptrock Beate
Heidelberg, Germany
Johann Greil

32
Can allogeneic HSCT in ALL be
replaced by antibody therapy?

33
Principal Considerations Treatment of acute leukemia
Multimodal chemotherapy protocols Adults
Children and adolescents
Considerable improvement Leukemia free survival:
90% in children and adolescents with ALL
Indications for SCT CR1 only in high risk patients for ALL
Slow response, hypodiploidy, pers. MRD
CR2 Only high risk patients in children and adolescents with ALL
Early, very early relapses and slow MRD clearance in late relapses
CR3 All patients

34
Stem-Cell Transplantation in Children With Acute Lymphoblastic Leukemia: A Prospective
International Multicenter Trial Comparing Sibling Donors With Matched Unrelated Donors—
The ALL-SCT-BFM-2003 TrialChristina Peters, Martin Schrappe, Arend von Stackelberg, André Schrauder, Peter Bader, Wolfram Ebell,Peter Lang, Karl-Walter Sykora,
Johanna Schrum, Bernhard Kremens, Karoline Ehlert, Michael H. Albert,Roland Meisel, Susanne Matthes-Martin, Tayfun Gungor, Wolfgang
Holter, Brigitte Strahm, Bernd Gruhn,Ansgar Schulz, Wilhelm Woessmann, Ulrike Poetschger, Martin Zimmermann, and Thomas Klingebiel
C. Peters et al.
J Clin Oncol 2015
MSD: 71%
MUD: 69%
MSD: 3%
MUD: 10%MSD: 24%
MUD: 22%
MSD: 79%
MUD: 73%

35
Patient with ALL from 2005-2014n=99 in complete remission at the time of first transplantation
N % N %
Sex
Male
Female
60
39
61
39
Age
< 10 years
> 10 years
35
64
35
65
Remission
CR1
≥ CR2
54
45
55
45
Donor
MSD
MUD
Haploidentical
21
67
11
21
68
11
Phenotype
pB-ALL
T-ALL
bi-pheno ALL
82
12
5
83
12
5
Immunotherapy
(WD of CSA or DLI)
Yes
No
29
70
29
71
Frankfurt Experience
S. Bahktiar, submitted

36
n Events 4-y TRM P
━ 49 7 0.14 ±0.05 .129
━ 50 2 0.04±0.02
Ov
era
ll s
urv
iva
l
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Outcome for ALL2005-2009 versus 2010-2014
months after SCT
TR
M
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
months after SCT
CIR
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
pE
FS
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
n Events 4-y EFS P
━ 49 18 0.63 ±0.07 .365
━ 50 10 0.77±0.06
2010-2014 (n=50) = 87%
2005-2009 (n=49) = 71%
2010-2014 (n=50) = 77%
2005-2009 (n=49) = 63%
n Events 4-y OS P
━ 49 14 0.71 ±0.06 .198
━ 50 6 0.87±0.05
n Events 4-y CIR P
━ 49 11 0.22 ±0.06 .958
━ 50 8 0.19±0.06
S. Bahktiar, submitted

37
CIBMTR Study. Period 2000-2011: Patients n=1458
2y: 50%
Segal et.al: Cancer 2017