New technologies, new toxicities: New radiotherapy modalities

Immunotherapy Related Toxicities and their Management:
What the Oncology Pharmacist Needs to Know
Advanced Clinical Practice for Cancer Pharmacists Course
Michael Powell Pharmacist Advanced, Cancer & Blood Disorders
Gold Coast University Hospital

Aim
• To provide an overview of the main immunotherapy side effects • Anti CTLA-4 monoclonal antibodies
• Anti PD-1/PD-L1 monoclonal antibodies
• To outline how these toxicities are best managed according to current evidence and practice

Wolchok et al, ASCO 2013 Abst#9012

Anti CTLA-4 Monoclonal Antibodies: Ipilimumab

Alatrash et al, Expert Opin Drug Saf 2013; 12(5): 631-45

Alatrash et al, Expert Opin Drug Saf 2013; 12(5): 631-45

Immune Mediated Toxicities (imAEs): Ipilimumab
• Dermatological
• Gastrointestinal
• Hepatotoxicity
• Endocrinopathies
• Neurological toxicity
• Ocular toxicity
• Pancreatitis
• Pancytopaenia
• Renal toxicity

Immune Mediated Toxicities (imAEs): Ipilimumab
•Dermatological
•Gastrointestinal
•Hepatotoxicity
• Endocrinopathies • Neurological toxicity
• Ocular toxicity
• Pancreatitis
• Pancytopaenia
• Renal toxicity

Immune Mediated Toxicities (imAEs): Ipilimumab
• Unique set of side effects not previously seen commonly in oncological practice
• As cancer immunotherapies become more widely used, early recognition of imAEs and initiation of treatment are critical to reduce the risk of sequelae
• Ensure alternate causes for toxicity have been considered and eliminated if identified: • E.g. hepatotoxicity, neurological toxicity – may be MAb drug related, but
consider alternative drugs, disease progression, infection
• From trials: 60% patients will experience an imAE with around 20% of these developing a severe or life threatening toxicity
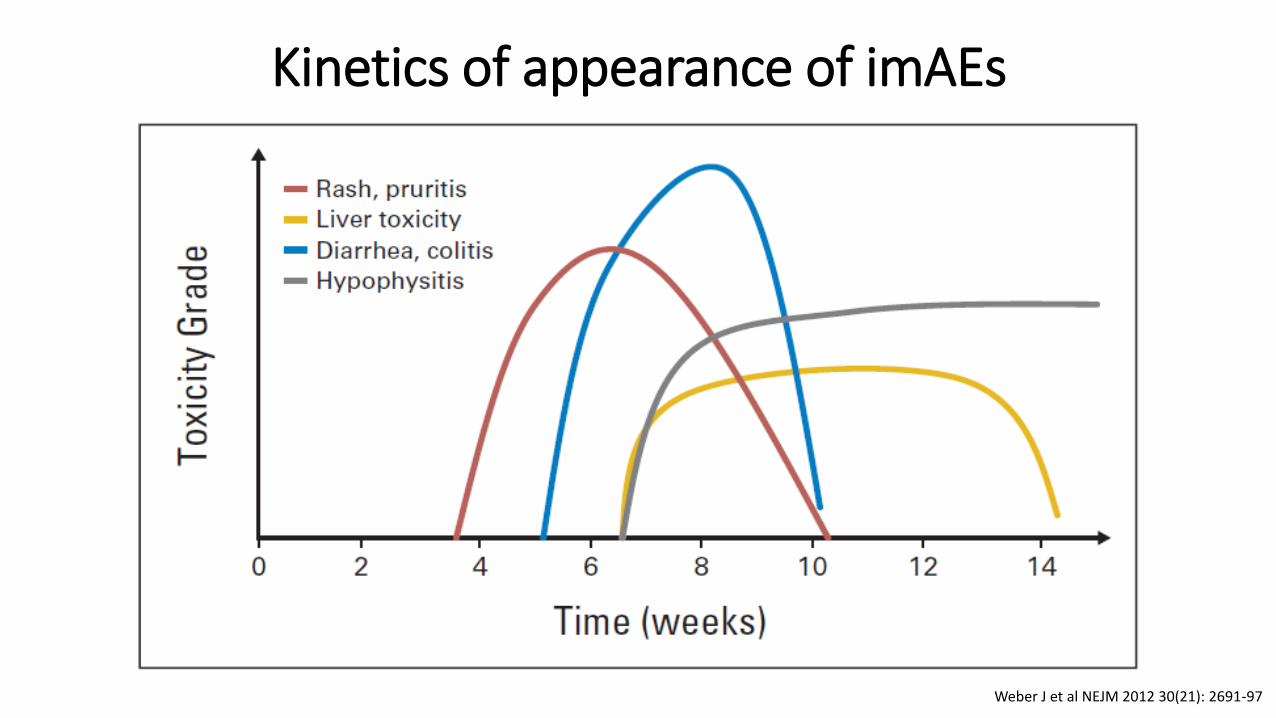
Kinetics of appearance of imAEs
Weber J et al NEJM 2012 30(21): 2691-97

Dermatological imAEs
• Typically presents as maculopapular rash • Often with intense generalised pruritis
• Can occur 2-3 weeks after initiation of Ipilimumab
• Trials report 47-68% incidence rates (4% severe)
• Why considered immune-related? • Biopsies of skin lesions showed T-cell infiltrates associated with apoptotic
melanocytes
• Anti-melanocyte activity: incidence of skin depigmentation, alopecia


Management Recommendations
Follow-Up (a) Symptoms controlled
(b) Ongoing mild symptoms 1-2 wks
(a) Continue Ipilimumab therapy
(b) Administer systemic corticosteroid therapy and continue Ipilimumab
Management
Symptomatic treatment
Administer symptomatic treatment e.g. antiH2’s, topical corticosteroids
Monitor patient
Continue Ipilimumab therapy
Determine Severity Mild or Moderate Grade 1 or 2: localised, papules/pustules <10-30% body surface

Management Recommendations
Follow-Up (a) Symptoms controlled
(b) Ongoing moderate to severe symptoms
(a) Resume Ipilimumab at next scheduled dose if symptoms improve to G0-1 or baseline
(b) Continue to omit Ipilimumab until resolves then as above
Management
Omit scheduled Ipilimumab dose
Consider oral corticosteroid therapy
Determine Severity
Severe Grade 3: rash, pruritis

Management Recommendations
Follow-Up Symptoms controlled
Consider initiating corticosteroid tapering based on clinical judgement
Management
Permanently discontinue Ipilimumab Administer high dose IV corticosteroid therapy
Determine Severity Very severe Grade 4: rash, pruritis

Dermatological imAEs: Specific Drug Guidelines
• Mild to moderate skin rash • Topical thick moisturisers, oatmeal baths (scalp lesions – low dose steroid containing
shampoo or topical coal tar) • Oral antihistamines e.g. Loratidine/cetirizine • Topical corticosteroids e.g. betamethasone 0.1% cream • Sun avoidance and use of broad spectrum sunscreens, cool compresses for itching • If ongoing symptoms: oral corticosteroids as below
• Severe rash • Oral corticosteroids: Prednisolone 1mg/kg daily • Once symptoms resolved to Grade 0 or 1 or to baseline, ensure tapering of dose over
> 4 weeks to prevent rebound toxicity
• Very severe (grade 4) rash • High dose IV corticosteroids: Methylprednisolone 1-2mg/kg/day • Once symptoms resolved to Grade 0 or 1 or to baseline, ensure tapering of dose over
> 4 weeks to prevent rebound toxicity

Dermatological imAEs
• Rarely: Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis with several reports of deaths • Bullous lesions • Mucosal lesions • Systemic signs
• Permanently discontinue Ipilumumab

Gastrointestinal toxicities • CTLA-4 blockade results in dysregulation of GI mucosal immunity
• Histopathology shows focal active colitis with crypt destruction, loss of goblet cells and neutrophilic/lymphocytic infiltrates in the crypt epithelium

GI Toxicities
• Enterocolitis is a frequent immune-related toxicity
• Involves the descending colon > sigmoid colon, ascending colon or rectum
• Symptoms include: • Diarrhoea • Colitis • Abdominal pain • Blood/mucus in stools • Ileus • Systemic symptoms: fever, fatigue,
weigh loss • Rarely: bowel perforation (<1%)
GI Toxicities
• GI imAEs occur in approx. a third of patients(1) • 10% > Grade 3
• Pooled safety data showed 3/1498 patient died from GI toxicity
• Another review of 511 patients showed 1% incidence of bowel perforation, and 5% hospitalised with severe enterocolitis(2)
• Median time to onset is at 5-6 weeks, peaking at 8 weeks from start of treatment
• Resolution in 90% of cases, median time from onset to resolution of 4 weeks
(1) Ibrahim et al J Clin Onc 2011; 29: Abst 8583 (2) Tarhini Scientifica 2013; 1-19

Colitis Management Guidelines
Robert C, ESMO 2014

Immunosuppressive therapy: Grade 3-4 Colitis
• First line: Methylprednisolone IV 1-2mg/kg/day until symptom resolution or reduce to maximum grade 1, then taper over at least 1 month
• Second line (if no response to steroids within 5 days, no contraindications such as sepsis, perforation): Infliximab IV 5mg/kg single dose (?continue 2 weekly similar to IBD treatment) + continue steroids
• Alternative second line (e.g. hepatitis): Mycophenolate Mofetil 500mg-1000mg po bd

Hepatotoxicity
• Less common (3-9%)
• Hepatic failure leading to death rare (<1%) but have occurred
• Inflammatory hepatitis similar to autoimmune disease • Usually asymptomatic elevation of ALT/AST and bilirubin (some patients have
fever and malaise)
• Time to onset ranges from 3-9 weeks from start of treatment
• Mild to moderate hepatotoxicity (AST/ALT >5-8 x ULN and/or TB >3-5 x ULN) • Omit scheduled dose, monitor until resolution and evaluate patient for
alternative causes (e.g. meds, disease progression, infection) • Resume Ipilimumab once AST/ALT <5 x ULN and TB <3 x ULN

Hepatotoxicity
• Severe (AST/ALT >8 x ULN and/or TB >5 x ULN) • Permanently discontinue Ipilimumab, administer high dose IV corticosteroids,
monitor until resolution and evaluate patient for alternative causes (e.g. meds, disease progression, infection)
• Consider steroid taper over at least 1 month based on clinical judgement if LFTs reduce
• Corticosteroid-refractory • Defined as no response to steroids OR LFT elevations during steroid taper that do not
respond to re-escalation • Consider alternative immunosuppressant e.g. mycophenolate 500mg-1000mg po bd,
tacrolimus 0.1-0.15mg/kg/d (avoid infliximab) • Antithymocyte globulin used successfully (case report)
• Consider antimicrobial prophylaxis in patient receiving immunosuppression for > 4 weeks

Endocrine Toxicity
• Immune infiltration of thyroid and/or pituitary glands: • Leads to acute inflammation of thyroid (thyroiditis) or pituitary gland (hypophysitis)
• Resulting in: • Adrenal insufficiency – severe dehydration, hypotension, shock
• Hypothyroidism
• Hypogonadism
• Incidence about 10%, severe in 2-4% and occurs at 7-10 weeks after start
• Symptoms can be non-specific and include: headache, fatigue, visual field defects, electrolyte disturbances, behavioural changes
• Need to consider that prolonged systemic corticosteroids used for other imAEs can contribute to adrenal insufficiency and hypogonadism

Endocrine Toxicity: Management
• Diagnosis involves checking serum TSH, free T4, ACTH, morning cortisol (in addition to imaging assessment) • Consider Synacthen test, LH/FSH, testosterone, prolactin
• If endocrinopathy not suggestive of adrenal crisis: • Refer early to endocrinologist • Withhold scheduled Ipilimumab dose • Consider short-term high dose corticosteroids (e.g. Dexamethasone 4mg po 6
hourly or equivalent) with tapering over >1mo once symptoms resolve • HRT where relevant according to bloods: T4, hydrocortisone, sex hormones
• Resume Ipilimumab at next scheduled dose assuming symptoms/labs improved
Endocrine Toxicity: Management
• If adrenal crisis (severe dehydration, hypotension, shock): • Refer early to endocrinologist
• Immediately initiate IV corticosteroids with mineralocorticoid activity (e.g. methylprednisolone, hydrocortisone)
• Once stabilises, HRT where relevant according to bloods: T4, hydrocortisone, sex hormones
• Withhold Ipilimumab until complete resolution or stable on HRT then can resume • If unable to reduce steroids to Prednisolone 7.5mg or equivalent per day should
permanently discontinue Ipilimumab(1)
(1) Tarhini Scientifica 2013; 1-19

Other Toxicities
• Neurological toxicity • Motor/sensory neuropathy, muscle weakness (MG-like symptoms): manage
according to severity with steroids, withholding/discontinuing Ipilimumab
• Some cases of fatal Guillain-Barre syndrome reported
• Ocular toxicity • Scleritis/uveitis: consider topical corticosteroids
• Pancreatitis – lipase elevation
• Pancytopaenia
• Renal toxicity - glomerulonephritis
PD-1/PD-L1 Checkpoint Inhibitors
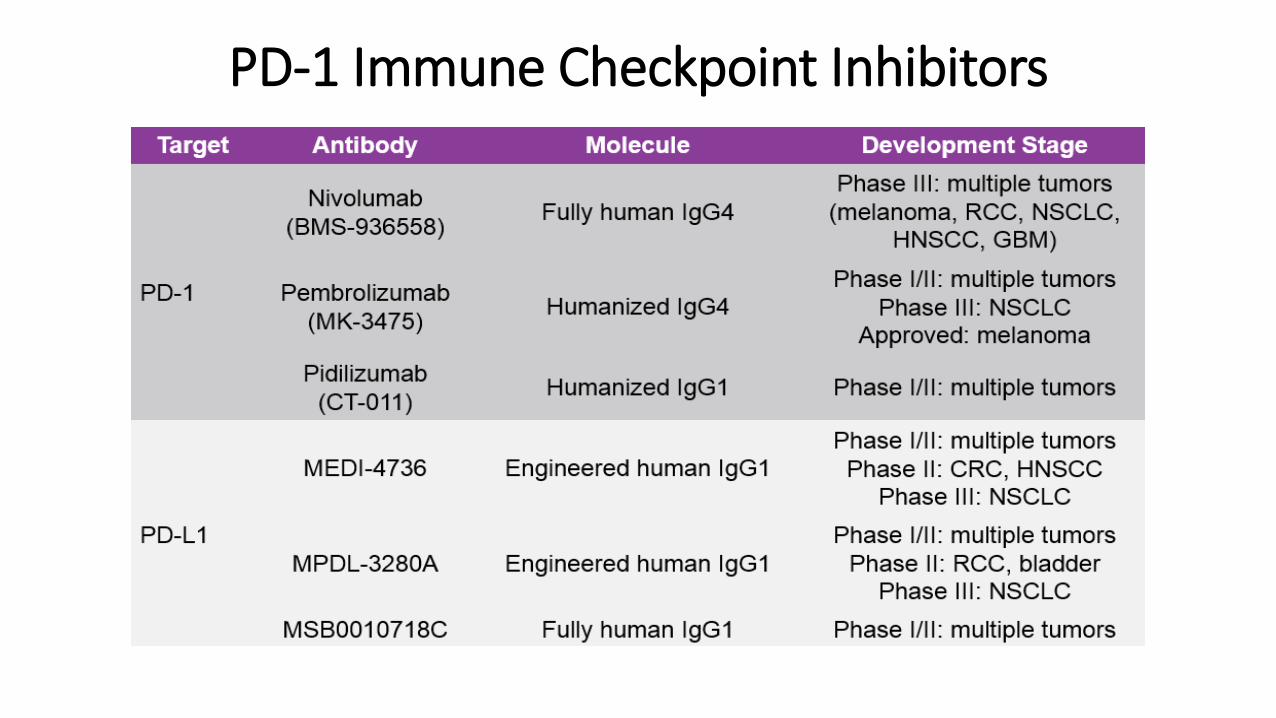
PD-1 Immune Checkpoint Inhibitors
PD-1 Immune Checkpoint Inhibitors
• Less clinical data on toxicities related to PD-1 checkpoint inhibitors, compared with Ipilimumab
• So far, it seems different adverse effect profiles of PD-1 vs CTLA-4 inhibitors
• Overall, lower incidence of imAEs with PD-1 inhibitors compared with Ipilimumab (although not devoid of them)
• Most frequent toxicities reported are mild fatigue, rash, pruritis, diarrhoea and colitis

Nivolumab
Topalian et al J Clin Onc 2014; 32: 1020-30

Nivolumab
Topalian et al J Clin Onc 2014; 32: 1020-30

Nivolumab
Topalian et al J Clin Onc 2014; 32: 1020-30

Pembrolizumab
Hamid et al NEJM 2013;369:134-44
PD-1 vs CTLA-4 Toxicities
• Looks like less imAEs: • In Topalian study: incidence of colitis, hepatitis, hypophysitis, thyroiditis and
uveitis = 1%
• Some concerns about pneumonitis • Can range from mild (asymptomatic, radiographic findings only) to severe or
rarely life-threatening
• Three cases of fatal pneumonitis reported in early phase nivolumab studies
• Likely class effect – reported for both nivolumab and pembrolizumab

Nivolumab Investigator Brochure V13_21JUL14[1]

Combination Immune Checkpoint Therapy
Wolchok et al NEJM 2013; 369: 122-33

Phase 1 Study: Schedule
Wolchok et al, ASCO 2013 Abst#9012

Clinical Activity: Concurrent Regimen
Wolchok et al, ASCO 2013 Abst#9012

Treatment-Related AEs (>10% pts)
Wolchok et al, ASCO 2013 Abst#9012

For pharmacists……..
• Start brushing up on your endocrinology and gastro knowledge!
• Like with oral TKIs, remember non-cytotoxic doesn’t = non-toxic
• As a member of the MDT, challenge yourself to contribute to the management of these patients • E.g. don’t let the doctors reduce those steroids too quickly (minimum 4
weeks)
• Be aware of the pre-emptive monitoring required • LFTs, TFTs prior to each cycle
• If able, discuss with patients about side effects esp GI, skin
• Use the BMS patient education stuff…….