Immunomodulatory Effects of Tyrosine Kinase Inhibitors
12
INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html 17 1 Abstract— Tyrosine kinase inhibitors (TKIs) have dramatically improved the outcome of chronic myeloid leukemia (CML). Even though TKI therapy does not necessarily eliminate all leukemic cells, a small proportion of CML patients is able to discontinue the treatment successfully and be considered cured. Besides inhibiting the actual target BCR-ABL1 kinase in leukemic cells, TKIs inhibit several off-target kinases in normal healthy cells, such as lymphocytes. To date, little is known about the long-term in vivo effects of TKI treatment on the function of the immune system. However, constantly growing evidence suggests that some TKIs have a dual-mode of action; the direct cytotoxic effects induced by oncokinase inhibition are accompanied by the activation of immune system 2 , which is potentially relevant for the long-term control of CML. In this review, we have summarized the reported immunomodulatory effects of the three TKIs, which currently are accepted for first-line use in CML (imatinib, dasatinib and nilotinib). Understanding the mechanisms of TKI-induced functional cure and the role of immune system in this process will hopefully not only benefit CML patients, but also patients with other malignant diseases in the future. Index Terms— Chronic myeloid leukemia, dasatinib, imatinib, immunomodulation, nilotinib, tyrosine kinase inhibitors. I. INTRODUCTION he treatment of CML has significantly improved during the past 10-20 years after the tyrosine kinase inhibitors (TKIs) entered the clinics.[1] Even though the TKI therapy has Received April 25., 2013 and accepted after minor revision May 15, 2013. This work was supported in part by the Finnish special governmental subsidy for health sciences, research and training, and grants from the Finnish Cancer Societies, the Emil Aaltonen Foundation, the Academy of Finland, the Biomedicum Helsinki Foundation, the Finnish Medical Foundation, the Blood Disease Foundation, the Finnish Association of Hematology, the Sigrid Jusé lius Foundation and the KA Johansson Foundation. A, Kreutzman was with Hematology Research Unit Helsinki, Helsinki University Central Hospital, Finland. She is now with the Department of Immunology, Princes University Hospital, Madrid, Spain (e-mail: [email protected]). K. Porkka is with the Hematology Research Unit Helsinki, Department of Medicine, Helsinki University Central Hospital, P.B. 700, 00029 HUCH, Finland. (e-mail: [email protected]). S. Mustjoki is with the Hematology Research Unit Helsinki, Department of Medicine, Helsinki University Central Hospital, P.B. 700, 00029 HUCH, Finland. (e-mail: [email protected]). 2 Figure changed the course of the disease, these drugs do not eradicate all tumor cells as it has been shown in vitro that leukemic stem cells are resistant to TKI therapy.[2-4] This means that the majority of patients will relapse if the treatment is stopped,[5-7] but recent results suggest that in some patients therapy discontinuation is feasible although residual leukemic cells exist.[8-10] It would be important to understand the mechanisms of cure and ways to achieve it in a larger proportion of patients in order to avoid life-long treatment with expensive TKI drugs. One curative approach could be the modulation of the immune system with the single agents or the combination regimes including TKIs in order to better target the malignant cells. This idea is supported by several arguments. First, the chronic nature of the disease and the slow progression rate in most cases is a favorable setting for immunotherapy. Furthermore, in most patients TKI therapy induces a state of minimal residual disease, which is often needed for successful immunotherapy.[11] Second, the malignant CML cells carry a well-defined and specific tumor antigen and the peptides derived from the fusion zone of the p210 bcr-abl protein are able to produce an immune response.[12-20] In accordance with this, leukemia antigen-specific T-cells such as anti-PR1 (the HLA-A2-restricted 9-mer peptide from proteinase 3), and anti-WT1 (Wilms tumor 1 protein) T-cells are shown to be present in CML patients, although they may be anergic.[21, 22] However, it is believed that the immune system is not permanently compromised, as CML patients can successfully be treated with immunomodulatory agents such as IFN-.[21, 23-28] It is also thought that the high efficiency of allogeneic stem cell transplantation is another evidence of the immune system controlling CML.[29, 30] Furthermore, donor lymphocyte infusions in the case of relapse have been reported to induce complete remissions.[31-34] In addition, as already mentioned above, a small proportion of CML patients are able to discontinue the TKI treatment successfully [8] although the disease is clearly measurable with the sensitive BCR-ABL1 RQ-PCR technique.[9] This proves that the immune system plays a role in the disease control of CML and can eliminate malignant cells II. LYMPHOCYTE ANERGY IN CML In the majority of cancer patients, the immune system is dysfunctional and unable to produce an efficient immune response against the malignant cells.[35] Indeed, immune cell Immunomodulatory Effects of Tyrosine Kinase Inhibitors A. Kreutzman, K. Porkka, and S. Mustjoki T
Transcript of Immunomodulatory Effects of Tyrosine Kinase Inhibitors

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
17
1
Abstract— Tyrosine kinase inhibitors (TKIs) have dramatically
improved the outcome of chronic myeloid leukemia (CML). Even
though TKI therapy does not necessarily eliminate all leukemic
cells, a small proportion of CML patients is able to discontinue the
treatment successfully and be considered cured. Besides inhibiting
the actual target BCR-ABL1 kinase in leukemic cells, TKIs inhibit
several off-target kinases in normal healthy cells, such as
lymphocytes. To date, little is known about the long-term in vivo
effects of TKI treatment on the function of the immune system.
However, constantly growing evidence suggests that some TKIs
have a dual-mode of action; the direct cytotoxic effects induced by
oncokinase inhibition are accompanied by the activation of
immune system2, which is potentially relevant for the long-term
control of CML.
In this review, we have summarized the reported
immunomodulatory effects of the three TKIs, which currently are
accepted for first-line use in CML (imatinib, dasatinib and
nilotinib). Understanding the mechanisms of TKI-induced
functional cure and the role of immune system in this process will
hopefully not only benefit CML patients, but also patients with
other malignant diseases in the future.
Index Terms— Chronic myeloid leukemia, dasatinib, imatinib,
immunomodulation, nilotinib, tyrosine kinase inhibitors.
I. INTRODUCTION
he treatment of CML has significantly improved during the
past 10-20 years after the tyrosine kinase inhibitors (TKIs)
entered the clinics.[1] Even though the TKI therapy has
Received April 25., 2013 and accepted after minor revision May 15, 2013.
This work was supported in part by the Finnish special governmental subsidy
for health sciences, research and training, and grants from the Finnish Cancer
Societies, the Emil Aaltonen Foundation, the Academy of Finland, the Biomedicum Helsinki Foundation, the Finnish Medical Foundation, the Blood
Disease Foundation, the Finnish Association of Hematology, the Sigrid
Jusélius Foundation and the KA Johansson Foundation. A, Kreutzman was with Hematology Research Unit Helsinki, Helsinki
University Central Hospital, Finland. She is now with the Department of
Immunology, Princes University Hospital, Madrid, Spain (e-mail: [email protected]).
K. Porkka is with the Hematology Research Unit Helsinki, Department of
Medicine, Helsinki University Central Hospital, P.B. 700, 00029 HUCH, Finland. (e-mail: [email protected]).
S. Mustjoki is with the Hematology Research Unit Helsinki, Department of
Medicine, Helsinki University Central Hospital, P.B. 700, 00029 HUCH, Finland. (e-mail: [email protected]).
2 Figure
changed the course of the disease, these drugs do not eradicate
all tumor cells as it has been shown in vitro that leukemic stem
cells are resistant to TKI therapy.[2-4] This means that the
majority of patients will relapse if the treatment is stopped,[5-7]
but recent results suggest that in some patients therapy
discontinuation is feasible although residual leukemic cells
exist.[8-10] It would be important to understand the
mechanisms of cure and ways to achieve it in a larger
proportion of patients in order to avoid life-long treatment with
expensive TKI drugs.
One curative approach could be the modulation of the
immune system with the single agents or the combination
regimes including TKIs in order to better target the malignant
cells. This idea is supported by several arguments. First, the
chronic nature of the disease and the slow progression rate in
most cases is a favorable setting for immunotherapy.
Furthermore, in most patients TKI therapy induces a state of
minimal residual disease, which is often needed for successful
immunotherapy.[11] Second, the malignant CML cells carry a
well-defined and specific tumor antigen and the peptides
derived from the fusion zone of the p210bcr-abl protein are able to
produce an immune response.[12-20] In accordance with this,
leukemia antigen-specific T-cells such as anti-PR1 (the
HLA-A2-restricted 9-mer peptide from proteinase 3), and
anti-WT1 (Wilms tumor 1 protein) T-cells are shown to be
present in CML patients, although they may be anergic.[21, 22]
However, it is believed that the immune system is not
permanently compromised, as CML patients can successfully
be treated with immunomodulatory agents such as IFN-.[21,
23-28] It is also thought that the high efficiency of allogeneic
stem cell transplantation is another evidence of the immune
system controlling CML.[29, 30] Furthermore, donor
lymphocyte infusions in the case of relapse have been reported
to induce complete remissions.[31-34] In addition, as already
mentioned above, a small proportion of CML patients are able
to discontinue the TKI treatment successfully [8] although the
disease is clearly measurable with the sensitive BCR-ABL1
RQ-PCR technique.[9] This proves that the immune system
plays a role in the disease control of CML and can eliminate
malignant cells
II. LYMPHOCYTE ANERGY IN CML
In the majority of cancer patients, the immune system is
dysfunctional and unable to produce an efficient immune
response against the malignant cells.[35] Indeed, immune cell
Immunomodulatory Effects of Tyrosine Kinase
Inhibitors
A. Kreutzman, K. Porkka, and S. Mustjoki
T

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
18
anergy has been described in several types of cancers and it is
thought to be one of the main hinderances in successful
immunotherapy.[36, 37] Similarly in CML, the observed
leukemia-specific T-cells have shown to be functionally
exhausted [38] or anergic.[39] One contributing factor is the
activation of programmed death receptor 1 (PD-1)
signaling.[38] PD-1 is a member of the immunoglobulin
superfamily, which expression can be induced on T- and
B-cells and activated monocytes.[40] PD-1 mediates inhibitory
signals through the binding of its ligand PD-L1 and PD-L2. In
chronic virus infections, the PD-1 signaling has been identified
as an important mechanism for antigen-specific T-cell
dysfunction.[41, 42] Similarly, many tumor cells highly
express PD-L1 and in this manner suppress tumor
immunity.[43, 44] Mumbrecht et al. have demonstrated that
also in CML, the CD8+ T-cells derived from patients express
higher levels of PD-1 than healthy CD8+ T-cells, and in the
mouse model the PD-L1 blockade on tumor cells leads to
prolonged survival.[38] Similarly recent paper by
Christiansson et al. described that cytotoxic CD8+ T-cells in
CML patients express high levels of PD-1. Furthermore, the
PD-L1 expression on myeloid tumor cells was higher in
patients than in healthy controls, and interestingly, patients
with high Sokal risk score had increased levels of PD-L1
expressing CD34+ stem cells.[45] In addition to the
PD-1/PD-L1 pathway, also other anergy mechanisms (such as
regulatory T-cells, myeloid derived suppressor cells) may
operate in CML patients.[45]
III. TYROSINE KINASE INHIBITORS
CML is caused by an oncogenic translocation forming the
characteristic Philadelphia chromosome (Ph) in the
hematopoietic stem cells. The resulting fusion gene produces
BCR-ABL1 protein with constant tyrosine kinase activity,
which in turn leads to uncontrolled cell proliferation and
reduced apoptosis.[46] After the discovery of BCR-ABL1, the
development of targeted therapies has emerged rapidly and the
first trials with a selective inhibition against the BCR-ABL1
tyrosine kinase began the revolution in the treatment of
CML.[47-50]
The first-generation TKI imatinib quickly replaced the
previous standard therapies for CML as it became soon evident
that imatinib treatment resulted in superior treatment
responses.[47-49, 51] However, long-term follow-up has
shown that a proportion of imatinib-treated patients do not
respond well to the treatment and eventually progress to
advanced phases of CML.[52] In addition, some patients are
unable to continue imatinib treatment because of
intolerance.[53] Since the emerging cases of resistance and
intolerance, several pharmaceutical companies have developed
second-generation TKIs such as dasatinib, nilotinib and
bosutinib. In addition to inhibiting BCR-ABL1 more
effectively, they are more flexible in binding to different
BCR-ABL1 conformations [54-57] and they are able to inhibit
several imatinib-resistant mutations.[57-61] Therefore, in
many countries these drugs have been approved for the
treatment of imatinib-resistant CML patients.[62-64] Moreover,
in the first-line setting, both dasatinib and nilotinib are shown to
result in deeper therapy responses in a shorter time than
imatinib treatment.[65, 66]
The key challenges today in treating CML are the evolving
mutations against TKIs. For example, several dasatinib
(T315I/A, F317L/V/I/C, and V299L)[67, 68], nilotinib (T315I,
E255K/V, Y253H, F359V/C/I)[68] and bosutinib-resistant
mutations (T315I and V299L) have been observed.[69] Of
these, the most important is the T315I mutation, which is
resistant to all first- and second-generation drugs. For these
patients, there are several third-generation TKIs in phase I/II
trials. These new candidate molecules are potential inhibitors of
the T315I mutation and include compounds such as XL228,
PHA-739358, AT9283, and DCC-2036.[70] However, the most
promising at the moment is ponatinib (AP24534), which is
highly active against the T315I mutation and has already
entered in clinical trials.[71]
IV. IMMUNOMODULATORY EFFECTS OF TYROSINE KINASE
INHIBITORS
The first TKI that entered to the clinics was imatinib, which
is therefore also the most studied. Numerous groups have
shown that imatinib has inhibitory effects on several kinases
including ABL, ARG, BCR-ABL1, c-KIT, platelet derived
growth factor receptor (PDGFR), DDR1 and NQO2.[72]
Whereas nilotinib has significantly similar inhibition profile as
imatinib, dasatinib inhibits a broader range of kinases including
the SRC family (FGR, FYN, SRC, YES, BLK, HCK, LCK,
LYN), TEC family (BMX, BTK, ITK, TEC, TXK), and SYK
families (SYK and ZAP-70)(Table 1).[55, 73-76] Of these,
several are known to be important in the function of the
immune system. For example LCK, FYN, and ITK are essential
in T-cell signaling, whereas LYN, SYK, and BTK are involved
in B-cell signaling.[77] Further, the GCK-activated signaling
pathways participate in the modulation of cell adhesion, cell
migration and immune cell responses.[78] PTK6 (BRK) has
been described to mediate signaling pathways that are involved
in the regulation of cell cycle and migration.[79] A unique
feature of bosutinib is that it does not inhibit c-KIT or PDGFR,
and it targets the STE family of kinases and in particular the
STE20 subfamily.[80] These kinases are known regulators of
apoptosis, cell cycle, migration, lymphocyte polarization and
adhesion, and B-cell class switch.[81] Also CAMK2G, a
Ca2+
/calmodulin-dependent protein kinase shown to be
involved in regulating signaling networks controlling the
proliferation of myeloid leukemia cells,[82] is inhibited by
bosutinib but not by dasatinib.[80] The third-generation TKI
ponatinib is a potential inhibitor of a discrete subset of protein
tyrosine kinases including members of the class III/IV
subfamily of tyrosine kinases (RTK), FLT3, c-KIT, fibroblast
growth factor receptor 1 (FGFR1) and PDGFR.[83, 84]
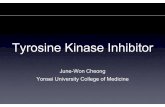
In the following paragraphs, the immunomodulatory
effects of different TKIs will be presented in detail by the
immune cell type (figure 1).

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
19
A. T-cells
T-cells have several well-characterized functions in tumor
immunology. They circulate through tissues and scan major
histocompatibility complex (MHC)-peptide complexes
presented on antigen-presenting cells (APCs), which can
specifically activate T-cells through the T cell receptor (TCR).
In addition, T-cells are capable of sensing a variety of signals,
such as potential danger signals associated with cancer.
Activated T-cells are then able to recognize antigens directly on
the tumor cell surfaces (reviewed by Restifo et al).[85]
Tumor-infiltrating lymphocytes (TILs) are a well-known
example of the antitumor activity of T-cells and the presence of
TILs have been correlated with clinical outcome.[86] Several
vaccine studies have also indicated the usefulness of cytotoxic
T-cell (CTL) responses, especially in treating minimal residual
disease.[87] In CML, the importance of T cell-mediated
immune responses was observed already in the 1980 s when
CML patients were transplanted with T cell-depleted grafts to
avoid graft-versus-host disease (GVHD). Even though the
depletion of T-cells successfully reduced the mortality from
GVHD, it also significantly increased the risk of relapse.[88]
Further proof of the beneficial role of antileukemic T-cells was
obtained when transplanted patients were given donor
lymphocyte infusions, which alone induced complete
remissions in patients who had relapsed.[31-34]
To date, several in vitro studies have shown that imatinib,
nilotinib, and dasatinib have inhibitory effects on T-cells.
Imatinib was reported to impair T-cell function first time in
2004 when Dietz et al. showed that the presence of imatinib
inhibited T-cell proliferation when cells were stimulated with
dendritic cells (DCs) or phytohaemagglutinin (PHA). Washout
of imatinib restored the proliferative capacity of T-cells. These
results were confirmed in a mouse in vivo-model.[89] The
following reports supported these first findings as they showed
that imatinib inhibits the proliferation of activated T-cells, and
reduce antigen-triggered expansion of CD8+ T-cells in
response to cytomegalovirus (CMV) and Epstein-Barr virus
(EBV) peptides.[90] Further, imatinib was shown to inhibit
PHA-induced proliferation of normal peripheral blood
mononuclear cells (PBMCs) in vitro.[91] The effects of
imatinib on the expression of T-cell activation markers (CD25
and CD69) have been controversial; both suppressive and
neutral effects have been reported [89-91].
The cytokine production of CD4+ and CD8+ T-cells has
also been reported to be reduced by imatinib treatment.[92] For
example the activation of whole blood with Staphylococcus
enterotoxin B resulted in lower production of Th1-type of
cytokines such as IL-1, IFN- and TNF- in imatinib treated
patients.[93] Similar inhibitory effects of imatinib on the
production of IL-2 and IFN- by T-cells have also been
reported in other studies.[90, 91]
The suppressive effects of imatinib therapy on leukemia
specific T-cells (such as the inhibition of IFN- and granzyme
B (GrB) release) have also shown to affect the lysis of CML
progenitor cells.[94] Further, imatinib seemed to inhibit the
antigen-specific IFN- secretion of both CD4+ and CD8+ T
effector cells. The same study showed that the cytolytic
functions of CD8+ CTLs were not altered.[92] Ex vivo studies
using autologous blood samples as stimulators to detect
antileukemic T-cell responses have shown that CML patients in
remission on imatinib were able to respond to stimulation by
cytokine secretion.[95]
The effects of imatinib treatment on antiviral immune
responses in vivo was studied by Mumprecht et al. Primary
CTL responses were not impaired in imatinib-treated mice, but
the secondary expansion of specific memory CTLs was
reduced both in vitro and in vivo, which resulted in impaired
protection against reinfection.[96] Imatinib treatment in vivo
selectively inhibited the expansion of antigen-experienced
memory CTLs without affecting primary T- or B-cell
responses.[96] The in vivo effect of imatinib has also been
studied by analyzing the response of CD8+ T-cells to Listeria
moncytogenes.[97] In vitro, imatinib had no effect on
antigen-specific expansion, cell division, cell cycle progression
or IFN- expression of naïve or memory T-cells. However,
imatinib induced apoptosis in these specific cells. Again, the
primary response was not altered whereas imatinib treatment
resulted in diminished memory response, suggesting that
imatinib treatment affects the ability of the CD8 memory pool
TABLE 1
TARGETS OF IMATINIB, NILOTINIB, AND DASATINIB
Modified from Hantschel et al., 2008.[55]
Imatinib Nilotinib Dasatinib
ABL ABL ABL HCK TXK EPHA3 LIMK2 SLK
ARG ARG ARG LCK DDR1 EPHA4 MYT1 STK36
BCR-ABL1 BCR-ABL1 BCR-ABL1 FGR DDR2 EPHA5 NLK SYK
c-KIT c-KIT c-KIT BLK ACK FAK PTK6/BRK TAO3
PDGFR PDGFR PDGFR FRK ACTR2B GAK QIK TESK2
DDR1 DDR1 SRC CSK ACVR2 GCK QSK TYK2
NQO2 NQO2 YES BTK BRAF HH498 RAF1 ZAK
FYN
LYN
TEC
BMX
EGFR
EPHA2
ILK
LIMK1
RET
RIPK2
Fig. 1. Immunomodulatory effects of imatinib and dasatinib on lymphocytes.
CML
Treg
Dasatinib
Mobilization of cytotoxic lymphocytes and expansion of LGLs, sensitized for
Th-1 type immune responses
NK-cells
LGL
Imatinib
Downregulation of
Tregs
Expansion of NK-cells and enhanced
cytotoxicity
NK-cells Restored NK-function
Treg Downregulation of Tregs
NK-cells
Treg T-cells
T-cells
T-cells
B-cells
B-cells
LGL
?
Anti-
leukemic activity
through antibody
production
? Inhibition
Expansion of differentiated memory
T-cells, decreased
expression of PD-1
Anergic T-cells (eg. expression of PD-1)
B-cells ? Quantitative and functional defects
Significant
increase in the percentage of
Tregs
Fig. 1. Immunomodulatory effects of imatinib and dasatinib on lymphocytes in CML patients.

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
20
to respond to antigen and has the potential to increase
susceptibility to infection.[97]
Similarly to imatinib, dasatinib blocks the function of
normal human T-cells in vitro at clinically relevant
concentrations. Several studies have reported that dasatinib,
when constantly present, inhibits the proliferation of both
CD4+ and CD8+ T-cells.[39, 98-101] Dasatinib has also shown
to inhibit the activation of T-cells[39, 98-100] and
antigen-specific proliferation of murine CD4+ and CD8+
transgenic T-cells in vitro and in vivo. The induction of
T-cell-mediated cytotoxicity following immunization with a
non-replicating recombinant virus was also inhibited.[102]
Furthermore, the presence of dasatinib hindered T-cell cytokine
production and degranulation in both CD4+ and CD8
+ T-cells in
a dose-dependent manner.[39, 98-100] It has been suggested
that CD4+ T-cells are more sensitive to the inhibitory effects of
dasatinib than CD8+ T-cells, and that naïve T-cells are more
sensitive than memory T-cell subsets.[99] In addition, the
inhibition of the proliferation of CD8+ T-cells has been
associated with lower secretion of IFN- and GrB.[101] Several
studies have also shown that dasatinib inhibits TCR-mediated
signal transduction.[100] The impaired TCR signaling led to
decreased proliferation and function of CD8+ T-cells.[101]
This seemed to be mediated through the SRC-family kinase
LCK, a candidate kinase for suppressed T-cell function.[98]
Furthermore, signal transduction and proliferative responses
via IL-2 remained unaffected, suggesting that the inhibitory
effect of dasatinib is specific for TCR mediated signaling.[100]
Dasatinib has also been reported to arrest CD8+ T-cells in the
G0/G1 phase of cell cycle. These effects were mediated by the
downregulation of the TCR phosphorylation and the NF-B
signaling transduction cascade.[101] Despite of these
inhibitory effects, dasatinib does not seem to induce apoptosis
in T-cells.[100, 101]
To date, only a few studies have reported
immunomodulatory effects of nilotinib. However, the available
data is similar to those of imatinib and dasatinib. It has been
shown that nilotinib inhibits the proliferation of CD8+ T-cells
in vitro at therapeutically relevant concentrations.[103] The
inhibition of CD8+ T-cells specific for leukemia or viral
antigens was associated with a reduced expansion of antigen
peptide specific CD8+ T-cells and with a decreased release of
IFN- and GrB. In addition, the inhibitory effect caused by
nilotinib was reported to be two times stronger than by imatinib.
These effects were mediated through the inhibition of the
phosphorylation of ZAP-70, LCK and ERK 1/2 and the NF-B
signaling transduction pathway.[103]
As a conclusion, it seems that when assessed in vitro, all the
studied TKIs possess more or less inhibitory effect on various
T-cell functions by blocking different kinases. However, it
needs to be taken into account that in these studies TKIs are
usually present throughout the experiment, which is not true in
the in vivo setting. For example, the maximum plasma
concentration for dasatinib is achieved already within one hour
after the drug intake and the half-life of only 3-5 hours,[104,
105] which obviously can affect the in vivo effects of the TKI.
B. Dendritic cells
Dendritic cells (DCs) are specialized APCs found in all
tissues. DCs ingest samples from the environment and present
the collected information to T- and B-cells in the adaptive
immune system. By presenting antigens, the DCs are capable of
initiating an immune response. Compared with other APCs
such as macrophages, DCs are very effective and can elicit very
low number of T-cells to respond. Once the DCs have captured
the antigen in the peripheral tissues the cells migrate into lymph
nodes where they present the antigen to lymphocytes.[106]
Distinct deficiencies have been reported to occur in CML
derived DCs (CML-DCs), such as reduced migration,
endocytosis, phagocytosis, antigen processing, DC maturation
and cytokine production as reviewed by Eisendle et al.[107]
Imatinib has been shown to restore the beneficial DC-related
immune functions in CML.[108] In addition, Sato et al. showed
that adding imatinib to DCs derived from CML patients
resulted in better allogeneic antigen presentation by mixed
leukocyte culture compared with the control cells without
imatinib.[109] Furthermore, imatinib enhanced antitumor
immune responses to DC-based immunization against an
imatinib-resistant BCR-ABL negative lymphoma.[110] In vitro
treatment of APCs with imatinib has also shown to enhance the
activation of naive antigen-specific T-cells and restore the
responsiveness of tolerant T-cells from tumor-bearing hosts.
Furthermore, in vivo treatment with imatinib not only prevented
the induction of tolerance of tumor-specific CD4+ T-cells
preserving their responsiveness to a subsequent immunization,
but also resulted in enhanced vaccine efficacy.[111] Although
imatinib seems to have beneficial effects on the function of
DCs, there are no reports of the effects of second generation
TKIs.
C. B-cells
B-cells are responsible for antibody production and errors in
B-cell development can give rise to immunodeficiency,
leukemia and lymphomas, and autoimmune diseases.[112] To
date, very few studies have explored the effects of the different
TKIs on B-cells. In the context of CML, B-cells have been
proposed to have beneficial anti-leukemic activity in patients
treated with imatinib as the treatment induces CD5+ B-cells
and IgM natural antibodies with anti-leukemic reactivity.[113]
However, in imatinib-treated patients the phenotype of plasma
cells was reported to be abnormal and it correlated with the
reduced gamma-globulin levels.[114] Imatinib treatment has
also been reported to decrease Ig levels and cause
hypogammaglobulinemia.[115-117] In addition to CML,
similar observations have also been reported in gastrointestinal
stromal tumor (GIST) patients who have been treated with
imatinib.[117]
D. NK-cells
NK-cells are a crucial part of the innate immunity and they
have a well-defined ability to recognize stressed cells (for
example transformed or infected cells) and destroy them.
Further, NK-cells can also provide help to the adaptive immune

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
21
system for example by producing IFN-.[118] Besides
cytotoxic T-cells, also NK-cells may have a role in the immune
control of cancer.
A recent report by Chen et al. concluded that CML is
associated with quantitative and functional defects within the
NK-cell compartment.[119] Several groups have reported
effects of the different TKIs on NK-cells and the results have
been controversial. Some studies have reported that imatinib
has no direct influence on NK-cell reactivity in vitro.[120] In
contrast, an earlier study by Cebo et al. showed that imatinib
treatment inhibits the NKG2D activating pathway and that the
modulation of NKG2D by imatinib interferes with NK-cell
recognition and cytolysis.[121] Accordingly, Chen et al.
reported that imatinib treatment cause a limited in vitro
expansion of NK-cells from CML patients and a reduced
degranulation response to K562 target cells.[119]
Similarly dasatinib has been shown to reduce NK-cell
cytotoxicity and cytokine production both using human cells
and an in vivo mouse model.[39, 102, 120] In contrast to these
studies, one publication reported that NK-cells in
dasatinib-treated patients have increased capability to kill K562
cells.[122] This finding is supported by reports showing that
NK-cell cytotoxicity is improved in dasatinib-treated CML
patients who have achieved a good therapy response.[122, 123]
Analysis of NK-cell signaling has revealed that dasatinib
inhibits proximal signaling events leading to decreased
phosphorylation of PI3K and ERK that are crucial for NK-cell
reactivity. Imatinib and nilotinib showed no relevant effect on
NK-cell PI3K or ERK activity.[120]
There are only a few papers reporting the effects of nilotinib
on NK-cells. In one publication by Salih et al., nilotinib did not
alter the cytotoxicity of NK-cells, but at high levels it impaired
the cytokine production in vitro.[120] This could be explained
by the finding that nilotinib increased the cell death within the
CD56bright
CD16neg
NK-cell subset, which is known to secrete
cytokines.[120] In contrast, Hayashi et al reported that nilotinib
decreased NK-cell cytotoxicity.[122]
In summary, the effects of TKIs on NK-cell function are
still controversial and additional research is needed. As with
T-cells, it should be kept in mind that the in vivo
pharmacokinetics of the TKIs differs from in vitro situation. In
addition, also the in vitro results have shown that the inhibitory
effects of TKIs on the NK cell function are reversible, as the
washing of the dasatinib-treated NK-cells restored their
cytotoxicity.[39, 120, 124]
E. Immunosuppressive cells
Tumors possess several mechanisms how they can disrupt
the anti-tumor immunity. This can be done for example by high
jacking the parts of the immune system such as by recruiting
myeloid-derived suppressor cells (MDSC) or regulatory T-cells
(Tregs) to provide protection against the immune attack.
Normally these cells contribute to peripheral tolerance, but in
cancer patients they have been shown to enhance tumor
survival and growth as reviewed by Whiteside [125] and
Lindau et al.[126]
MDCS are a group of immature CD11b+CD14-CD33+
cells (including precursors of macrophages, granulocytes, DCs
and myeloid cells) that are produced in response to various
tumor-derived cytokines. These inhibitory myeloid cells are
able to suppress both CD4+ and CD8+ T-cell mediated
immunity.[85] Interestingly, Christiansson et al. reported that
untreated CML patients have higher MDSC levels compared to
healthy individuals.[45]
In addition to MDSCs, the presence of Tregs has shown to
be correlated with poor prognosis in a number of cancers and
therefore several studies are now exploring the possibility to
eliminate Tregs to improve therapy responses.[127] However,
the elimination of Tregs can lead to autoimmune side effects in
addition to improved anti-tumor immunity.[128, 129] Imatinib
is known to inhibit the proliferation of Tregs and their
production of IL-10, TGF-1 and GrB in a dose-dependent
manner. In addition, the expression of CD69, GITR, FoxP3,
and CTLA-4 of activated Tregs was inhibited by imatinib.[110,
130] In contrast, another study showed that when used at
concentrations achieved in clinical use, imatinib did not impair
the production of IL-10 and TGF- by Tregs.[110] Analysis of
Treg TCR-induced signaling cascade indicated that imatinib
inhibited phosphorylation of ZAP70 and LAT.[110] Imatinib
treatment of mice decreased the frequency of Tregs and
impaired their immunosuppressive function in vivo.[110]
Dasatinib has been shown to profoundly prevent the
proliferation of Tregs in a dose-dependent manner, and to
decrease the production of corresponding cytokines. Treatment
of Tregs with dasatinib also inhibited the suppressive capacity
of Tregs. The mechanisms of this inhibition included the arrest
of cells in the G0/G1 phase of cell cycle, down-regulation of the
transcription factor FoxP3, glucocorticoid-induced tumor
necrosis factor receptor and CTLA-4 as well as inhibition of
signaling events through SRC and NF-B.[131] Similarly
nilotinib has been shown to inhibit and impair the function of
Tregs in a dose-dependent manner.[132]
In summary, TKIs also affect the immune regulatory cells
such as Tregs and this may lead to beneficial effects by
reversion of the suppressive mechanisms.
V. CLINICAL OBSERVATIONS
As described above, TKIs seem to possess mostly
immunosuppressive effects in vitro. Therefore, it has been of
interest to see whether similar effects are observed in vivo in
patients, as such strong inhibition of the immune system would
most likely lead to serious infections and other adverse-effects.
However, to date no increased rate of infections, secondary
malignancies or autoimmune disorders in TKI-treated patients
have been observed in large clinical studies.[66] A few cases of
panniculitis has been reported in imatinib-resistant CML
patients who were later treated with dasatinib.[133] Moreover,
Duman et al. reviewed eight cases of CML patients who had
developed secondary tumors after they had been treated with
imatinib.[134-136] Further, a few case reports suggesting that
in some circumstances dasatinib treatment may be associated
with abnormal viral infections. For example, parvovirus B19,
herpes virus 6 and reactivation of CMV infections have been

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
22
described in dasatinib-treated patients.[137] Our group has also
observed that in a selected group of patients experiencing large
granular lymphocyte (LGL) lymphocytosis during dasatinib
treatment, 40% had CMV reactivation.[138] Also, a high
number of CMV-specific T-cells were detected in these
patients.[39, 138] In contrast, in a recent report including only
first-line dasatinib-treated CML patients no increased incidence
of CMV reactivation was observed.[139]
Hayashi et al. recently reported that imatinib, nilotinib and
dasatinib-treated patients have similar numbers of CD8+ and
CD4+ T-cells during the treatment.[122] In contrast, Rohon et
al. reported that dasatinib-treated patients have a lower
proportion of T-cells in the blood,[140] and consequently an
increased number of NK-cells.[122, 140] The percentage of
immunosuppressive regulatory T-cells (CD4+CD25high
FoxP3+)
has been reported to be significantly higher in untreated CML
patients compared to healthy controls.[141] We and others have
reported that the number of Tregs in the blood is decreased
during dasatinib treatment.[138, 142] However, in other TKI
treated patients the number of Tregs has been found to be
similar as in healthy volunteers.[122, 141]
Mumprecht et al. reported that in imatinib-treated patients,
the PD-1 expression in CD8+ T-cells is increased up to 60%
whereas it is less than 10% in healthy controls.[38]
Interestingly, in dasatinib-treated patients CD8+ T-cells are
shown to express less than 20% of PD-1.[39] This finding
indicates that unlike imatinib, dasatinib may decrease PD-1
expression close to the levels of healthy controls, which could
be of importance as the lack of PD-1 signaling pathway is
associated with an improved survival and might restore the
function of CML-specific CTLs as shown in a CML mouse
model.[38]
The role of immunoregulatory genes has also been studied
in association with the response to TKI therapy. Especially
killer-immunoglobulin-like receptors (KIRs) are of special
interest as they are able to regulate both the function of
NK-cells and CD8+ T-cells. The presence of a stimulatory
KIR2DS1 gene was found to be a negative prognostic factor
and a lower proportion of KIR2DS1+ patients achieved
complete cytogenetic remission (CCgR) during imatinib
therapy.[143] Similar association with the rate of CCgR was
not found among dasatinib treated patients,[144] but the
absence of the inhibitory KIR2DL5A, 2DL5B, and 2DL5all
genes were associated with improved molecular response.[143,
145, 146]
In summary, despite the highly immunoinhibitory effects of
TKIs in vitro, these drugs do not seem to cause increased risks
of infections. In contrast, especially dasatinib, as described in
more detail below, seems to modify the immune system to a
more cytotoxic direction and decrease the number of
suppressive Tregs, which might have a positive impact on the
therapy outcome.
A. Dasatinib-induced lymphocytosis
In 2007, we noticed that imatinib treatment is associated
with the increased number of lymphocytes in the bone marrow,
and this correlated with the better therapy response.[147] The
lymphocyte infiltration was a mixed population including
B-cells and their precursors, T-cells and NK-cells. A few years
later, our group observed that dasatinib-treated patients had an
increased number of LGLs in the blood, which was also
associated with an improved therapy response.[138] This
observation was later confirmed by several other groups.[123,
139, 148, 149] The dasatinib-associated lymphocytosis is
characterized by an increased absolute blood lymphocyte count
(> 3.6 x 109/L) and it typically occurs 3-4 months after the
initiation of dasatinib treatment. It has been reported that nearly
30% of dasatinib-treated patients develop lymphocytosis.[148,
150] Importantly, there is an increasing evidence indicating that
lymphocytosis is associated with excellent therapy
responses.[123, 138, 148, 150] Such an expansion of T-LGLs
(CD3+CD8+CD56neg
) has also been described after autologous
and allogeneic bone marrow transplantation, and also in these
patient groups it has been associated with better treatment
responses.[151-155]
The role of cytomegalovirus (CMV) infection in the
development of LGL lymphocytosis has also been considered.
In our original reports we observed that 40% of the patients
who developed LGL lymphocytosis during dasatinib therapy
had also modest CMV reactivation and some patients even
suffered from symptomatic CMV reactivation such as from
CMV colitis.[39, 138] Further, all patients who had LGL
expansion during dasatinib therapy were cytomegalovirus
(CMV) seropositive[142] and most patients also had an
elevated number of CMV-specific CD8+ T-cells.[39] However,
in these studies most patients were treated with dasatinib
second-line and in other publications studying first-line CML
patients, no CMV reactivations have been observed.[139] The
understanding of the causative role of CMV in the development
of LGL lymphocytosis needs further studies, but it could be that
previous CMV infection increases the pool of specific
lymphocytes which are more prone to expand and mobilize
during dasatinib therapy.[156]
The exact mechanism causing LGL lymphocytosis during
dasatinib-therapy is still unknown. However, our group
recently demonstrated that dasatinib is able to induce a rapid
and dose-dependent mobilization of non-leukemic
lymphocytes and monocytes in blood peaking 1-2 h after the
oral intake of the drug. Importantly, the blood counts closely
mirrored drug plasma concentration. The mobilization was
coupled with a more effective transmigration of leukocytes
through an endothelial cell layer. Similar effects on blood cell
dynamics and function were not observed with any other TKI
(imatinib, nilotinib and bosutinib).[156] Furthermore, NK-cell
cytotoxicity was shown to be improved 1 hour after the intake
of dasatinib.[156] The wide kinase inhibition profile of
dasatinib seems to affect signaling pathways in leukocytes or
surrounding tissues causing rapid leukocyte increase in blood,
but the exact kinase involved in this process is still unknown.
This rapid mobilization is thought to account partially for the
observed LGL lymphocytosis during dasatinib treatment, but
additional mechanisms such as the decreased amount of Tregs,
genetic factors and primary lymphocyte pool may play a role.

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
23
VI. IMMUNOMODULATORY EFFECTS OF TKIS IN OTHER
CANCERS
The most famous success story of using TKIs in other
cancers than CML is the treatment of gastrointestinal stromal
tumors (GIST) with imatinib. GIST is a common type of
soft-tissue sarcoma mainly caused by a mutation in the KIT
gene, which results in the activation of the receptor in the
absence of its ligand and finally to uncontrolled cell growth and
tumor formation.[157] The discovery of the molecular
background of the disease led to successful clinical trials with
imatinib, which is also able to inhibit KIT. The
second-generation TKIs dasatinib and nilotinib are also able to
induce beneficial therapeutic responses in GIST patients.[158,
159] Interestingly, recent reports indicate that the superior
therapy responses seen in imatinib-treated GIST patients might
not only be due to the effective inhibition of the KIT
oncoprotein but also due to the immunomodulatory effects.
Balachandran et al. reported that imatinib potentiates antitumor
T-cell responses in a mouse model of GIST. Within the tumors,
imatinib was shown to increase the number of activated CD8+
T-cells, but to decrease the frequency of Tregs, consequently
significantly increasing the CD8+ T-cell to Treg ratio.
Interestingly, imatinib-treatment significantly decreased the
intratumoral IDO-expression. IDO is a protein, which promotes
the development, stabilization and activation of Tregs while
suppressing effector T-cells. These results were confirmed in
patient samples; imatinib-sensitive tumors contained a higher
frequency of CD8+ T-cells, but lower frequency of Tregs when
compared to imatinib-resistant tumors.[160]
Another disease associated with an activating mutation in
the KIT oncoprotein is systemic mastocytosis (SM). Already in
2006, Shah et al. demonstrated a significant inhibitory activity
of dasatinib against both wild-type and mutated c-KIT.
Dasatinib was shown to selectively kill primary neoplastic bone
marrow mast cells from patients with SM.[161] Interestingly,
in a recent paper by Yang et al., the in vivo antitumor effects of
dasatinib on the c-KIT mutant mastocytoma tumor was
demonstrated to be dependent on T cell-mediated immunity.
They showed that dasatinib treatment significantly decreased
the levels of Tregs while improving the antigen-specific T-cell
responses against tumors. The combination of dasatinib and
agonistic anti-OX40 (a potent co-stimulatory signal to T-cells)
antibody resulted in better therapeutic efficacy compared with
either drug alone, which was associated with increased number
of tumor antigen-specific T-cells in the tumor
microenvironment. Moreover, the combination of dasatinib and
anti-OX40 inhibited the function of Tregs and resulted in a
significant up-regulation of the IFN--induced chemokines
CXCL9, 10, and 11, which attracts CTL to the tumor
microenvironment.[162]
These two examples (GIST and SM) in addition to effects
observed in CML patients suggest that TKI treatment may have
beneficial immunomodulatory effects in vivo which need to be
studied in more detail in order to be able to utilize them in
future treatment regimens.
VII. FUTURE PROSPECTS
The current experience with TKIs in CML suggests that
only a small proportion of patients can achieve a state of
complete molecular remission (CMR) where therapy
discontinuation can be considered.[163] The CMR rates with
the 2nd
generation inhibitors dasatinib and nilotinib are better
and it could be that these drugs are also more effective against
the leukemic stem cells.[164] However, it seems that the total
eradication of leukemic cells is not needed in order to be able to
discontinue the treatment successfully and therefore better
ways to boost the immune system may increase the rate of
successful discontinuations.
There are already data showing that the combination of
immunomodulatory agents such as IFN- with the imatinib
treatment may increase the rate of superior molecular
responses.[165, 166] In addition, IFN- monotherapy after
imatinib treatment increases the rate of successful therapy
discontinuations.[166, 167] Ongoing clinical trials have
combined IFN- with 2nd
generation TKIs and their effects
remains to be seen. Further, the combination of imatinib with
anti-CML vaccines (mostly against p210bcr-abl) seems to
improve therapy responses.[168]
In the future it would be of interest to combine TKI
treatment with different types of immunomodulatory agents
such as with immune checkpoint inhibitors (for example PD1,
PD-L1, CTLA-4 and OX40 antibodies), which have now
entered in the first clinical trials.[169, 170] They could have
synergistic beneficial effects with TKIs, although also the risk
of side effects may increase. However, such combination
regimens may not only turn out to be useful in CML, but also in
other cancers, as was already shown in mastocytoma mouse
model.[162]
ACKNOWLEDGMENT
Personnel at the Hematology Research Unit Helsinki are
acknowledged for their expert technical assistance.
REFERENCES
[[1] M. Bjorkholm, L. Ohm, S. Eloranta, A. Derolf, M. Hultcrantz, J. Sjoberg, T. Andersson, M. Hoglund, J. Richter, O. Landgren et al
"Success story of targeted therapy in chronic myeloid leukemia: a population-based study of patients diagnosed in Sweden from 1973
to 2008," J Clin Oncol 29(18):2514-2520, 2011.
[2] S. M. Graham, H. G. Jorgensen, E. Allan, C. Pearson, M. J. Alcorn, L. Richmond, T. L. Holyoake "Primitive, quiescent,
Philadelphia-positive stem cells from patients with chronic myeloid
leukemia are insensitive to STI571 in vitro," Blood 99(1):319-325, 2002.
[3] M. Copland, A. Hamilton, L. J. Elrick, J. W. Baird, E. K. Allan, N.
Jordanides, M. Barow, J. C. Mountford, T. L. Holyoake "Dasatinib (BMS-354825) targets an earlier progenitor population than
imatinib in primary CML but does not eliminate the quiescent
fraction," Blood 107(11):4532-4539, 2006. [4] I. Sloma, X. Jiang, A. C. Eaves, C. J. Eaves "Insights into the stem
cells of chronic myeloid leukemia," Leukemia 24(11):1823-1833,
2010. [5] J. Cortes, S. O'Brien, H. Kantarjian "Discontinuation of imatinib
therapy after achieving a molecular response," Blood
104(7):2204-2205, 2004.

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
24
[6] P. Rousselot, F. Huguet, D. Rea, L. Legros, J. M. Cayuela, O. Maarek, O. Blanchet, G. Marit, E. Gluckman, J. Reiffers et al
"Imatinib mesylate discontinuation in patients with chronic
myelogenous leukemia in complete molecular remission for more than 2 years," Blood 109(1):58-60, 2007.
[7] S. Merante, E. Orlandi, P. Bernasconi, S. Calatroni, M. Boni, M.
Lazzarino "Outcome of four patients with chronic myeloid leukemia after imatinib mesylate discontinuation," Haematologica
90(7):979-981, 2005.
[8] F. X. Mahon, D. Rea, J. Guilhot, F. Guilhot, F. Huguet, F. Nicolini, L. Legros, A. Charbonnier, A. Guerci, B. Varet et al
"Discontinuation of imatinib in patients with chronic myeloid
leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre Stop Imatinib (STIM)
trial," Lancet Oncol 11(11):1029-1035, 2010.
[9] P. Koskenvesa, A. Kreutzman, P. Rohon, M. Pihlman, E. Vakkila, A. Räsänen, M. Vapaatalo, K. Remes, T. Lundan, H. Hjorth-Hansen
et al "Imatinib and pegylated IFN-a2b discontinuation in first-line
chronic myeloid leukemia patients following a major molecular response," Submitted.
[10] D. M. Ross, S. Branford, J. F. Seymour, A. P. Schwarer, C. Arthur,
P. A. Bartley, C. Slader, C. Field, P. Dang, R. J. Filshie et al "Patients with chronic myeloid leukemia who maintain a complete
molecular response after stopping imatinib treatment have evidence
of persistent leukemia by DNA PCR," Leukemia 24(10):1719-1724, 2010.
[11] O. Bruserud, E. Ersvaer, A. Olsnes, B. T. Gjertsen "Anticancer
immunotherapy in combination with proapoptotic therapy," Current cancer drug targets 8(8):666-675, 2008.
[12] M. Bocchia, P. A. Wentworth, S. Southwood, J. Sidney, K.
McGraw, D. A. Scheinberg, A. Sette "Specific binding of leukemia oncogene fusion protein peptides to HLA class I molecules," Blood
85(10):2680-2684, 1995.
[13] M. Bocchia, T. Korontsvit, Q. Xu, S. Mackinnon, S. Y. Yang, A. Sette, D. A. Scheinberg "Specific human cellular immunity to
bcr-abl oncogene-derived peptides," Blood 87(9):3587-3592, 1996.
[14] G. J. Bosch, A. M. Joosten, J. H. Kessler, C. J. Melief, O. C. Leeksma "Recognition of BCR-ABL positive leukemic blasts by
human CD4+ T cells elicited by primary in vitro immunization with
a BCR-ABL breakpoint peptide," Blood 88(9):3522-3527, 1996. [15] G. J. ten Bosch, A. C. Toornvliet, T. Friede, C. J. Melief, O. C.
Leeksma "Recognition of peptides corresponding to the joining
region of p210BCR-ABL protein by human T cells," Leukemia 9(8):1344-1348, 1995.
[16] G. Pawelec, H. Max, T. Halder, O. Bruserud, A. Merl, P. da Silva, H.
Kalbacher "BCR/ABL leukemia oncogene fusion peptides selectively bind to certain HLA-DR alleles and can be recognized
by T cells found at low frequency in the repertoire of normal donors," Blood 88(6):2118-2124, 1996.
[17] Y. Osman, M. Takahashi, Z. Zheng, T. Koike, K. Toba, A. Liu, T.
Furukawa, S. Aoki, Y. Aizawa "Generation of bcr-abl specific cytotoxic T-lymphocytes by using dendritic cells pulsed with
bcr-abl (b3a2) peptide: its applicability for donor leukocyte
transfusions in marrow grafted CML patients," Leukemia 13(2):166-174, 1999.
[18] P. Yotnda, H. Firat, F. Garcia-Pons, Z. Garcia, G. Gourru, J. P.
Vernant, F. A. Lemonnier, V. Leblond, P. Langlade-Demoyen "Cytotoxic T cell response against the chimeric p210 BCR-ABL
protein in patients with chronic myelogenous leukemia," J Clin
Invest 101(10):2290-2296, 1998. [19] R. E. Clark, I. A. Dodi, S. C. Hill, J. R. Lill, G. Aubert, A. R.
Macintyre, J. Rojas, A. Bourdon, P. L. Bonner, L. Wang et al
"Direct evidence that leukemic cells present HLA-associated immunogenic peptides derived from the BCR-ABL b3a2 fusion
protein," Blood 98(10):2887-2893, 2001.
[20] W. M. Wagner, Q. Ouyang, G. Pawelec "The abl/bcr gene product as a novel leukemia-specific antigen: peptides spanning the fusion
region of abl/bcr can be recognized by both CD4+ and CD8+ T
lymphocytes," Cancer Immunol Immunother 52(2):89-96, 2003. [21] J. J. Molldrem, P. P. Lee, C. Wang, K. Felio, H. M. Kantarjian, R. E.
Champlin, M. M. Davis "Evidence that specific T lymphocytes may
participate in the elimination of chronic myelogenous leukemia," Nat Med 6(9):1018-1023, 2000.
[22] K. Rezvani, M. Grube, J. M. Brenchley, G. Sconocchia, H. Fujiwara,
D. A. Price, E. Gostick, K. Yamada, J. Melenhorst, R. Childs et al "Functional leukemia-associated antigen-specific memory CD8+ T
cells exist in healthy individuals and in patients with chronic
myelogenous leukemia before and after stem cell transplantation," Blood 102(8):2892-2900, 2003.
[23] F. Bonifazi, A. de Vivo, G. Rosti, F. Guilhot, J. Guilhot, E.
Trabacchi, R. Hehlmann, A. Hochhaus, P. C. Shepherd, J. L. Steegmann et al "Chronic myeloid leukemia and interferon-alpha: a
study of complete cytogenetic responders," Blood
98(10):3074-3081, 2001. [24] H. M. Kantarjian, S. O'Brien, J. E. Cortes, J. Shan, F. J. Giles, M. B.
Rios, S. H. Faderl, W. G. Wierda, A. Ferrajoli, S. Verstovsek et al
"Complete cytogenetic and molecular responses to interferon-alpha-based therapy for chronic myelogenous leukemia
are associated with excellent long-term prognosis," Cancer
97(4):1033-1041, 2003. [25] F. X. Mahon, X. Delbrel, P. Cony-Makhoul, C. Faberes, J. M.
Boiron, C. Barthe, C. Bilhou-Nabera, A. Pigneux, G. Marit, J.
Reiffers "Follow-up of complete cytogenetic remission in patients with chronic myeloid leukemia after cessation of interferon alfa," J
Clin Oncol 20(1):214-220, 2002.
[26] D. Chakrabarti, B. Hultgren, T. A. Stewart "IFN-alpha induces autoimmune T cells through the induction of intracellular adhesion
molecule-1 and B7.2," J Immunol 157(2):522-528, 1996.
[27] A. Burchert, S. Wolfl, M. Schmidt, C. Brendel, B. Denecke, D. Cai, L. Odyvanova, T. Lahaye, M. C. Muller, T. Berg et al
"Interferon-alpha, but not the ABL-kinase inhibitor imatinib
(STI571), induces expression of myeloblastin and a specific T-cell response in chronic myeloid leukemia," Blood 101(1):259-264,
2003.
[28] L. Gabriele, P. Borghi, C. Rozera, P. Sestili, M. Andreotti, A. Guarini, E. Montefusco, R. Foa, F. Belardelli "IFN-alpha promotes
the rapid differentiation of monocytes from patients with chronic
myeloid leukemia into activated dendritic cells tuned to undergo full maturation after LPS treatment," Blood 103(3):980-987, 2004.
[29] R. H. Collins, Jr., O. Shpilberg, W. R. Drobyski, D. L. Porter, S.
Giralt, R. Champlin, S. A. Goodman, S. N. Wolff, W. Hu, C. Verfaillie et al "Donor leukocyte infusions in 140 patients with
relapsed malignancy after allogeneic bone marrow transplantation,"
J Clin Oncol 15(2):433-444, 1997. [30] W. J. Norde, I. M. Overes, F. Maas, H. Fredrix, J. C. Vos, M. G.
Kester, R. van der Voort, I. Jedema, J. H. Falkenburg, A. V.
Schattenberg et al "Myeloid leukemic progenitor cells can be specifically targeted by minor histocompatibility antigen
LRH-1-reactive cytotoxic T cells," Blood 113(10):2312-2323, 2009.
[31] H. J. Kolb, J. Mittermuller, C. Clemm, E. Holler, G. Ledderose, G.
Brehm, M. Heim, W. Wilmanns "Donor leukocyte transfusions for treatment of recurrent chronic myelogenous leukemia in marrow
transplant patients," Blood 76(12):2462-2465, 1990.
[32] W. R. Drobyski, C. A. Keever, M. S. Roth, S. Koethe, G. Hanson, P. McFadden, J. L. Gottschall, R. C. Ash, P. van Tuinen, M. M.
Horowitz et al "Salvage immunotherapy using donor leukocyte
infusions as treatment for relapsed chronic myelogenous leukemia after allogeneic bone marrow transplantation: efficacy and toxicity
of a defined T-cell dose," Blood 82(8):2310-2318, 1993.
[33] D. L. Porter, M. S. Roth, C. McGarigle, J. L. Ferrara, J. H. Antin "Induction of graft-versus-host disease as immunotherapy for
relapsed chronic myeloid leukemia," The New England journal of
medicine 330(2):100-106, 1994. [34] A. J. Barrett, B. N. Savani "Does chemotherapy modify the immune
surveillance of hematological malignancies?," Leukemia
23(1):53-58, 2009. [35] T. F. Gajewski, Y. Meng, C. Blank, I. Brown, A. Kacha, J. Kline, H.
Harlin "Immune resistance orchestrated by the tumor
microenvironment," Immunological reviews 213:131-145, 2006. [36] P. S. Kim, R. Ahmed "Features of responding T cells in cancer and
chronic infection," Current opinion in immunology 22(2):223-230,
2010.

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
25
[37] J. T. Kurnick, P. P. Pandolfi, G. Pawelec "Current Challenges in Immunology," International Trends in Immunity 1(1):5-9, 2013.
[38] S. Mumprecht, C. Schurch, J. Schwaller, M. Solenthaler, A. F.
Ochsenbein "Programmed death 1 signaling on chronic myeloid leukemia-specific T cells results in T-cell exhaustion and disease
progression," Blood 114(8):1528-1536, 2009.
[39] A. Kreutzman, K. Ladell, C. Koechel, E. Gostick, M. Ekblom, L. Stenke, T. Melo, H. Einsele, K. Porkka, D. A. Price et al "Expansion
of highly differentiated CD8+ T-cells or NK-cells in patients treated
with dasatinib is associated with cytomegalovirus reactivation," Leukemia 25(10):1587-1597, 2011.
[40] R. J. Greenwald, G. J. Freeman, A. H. Sharpe "The B7 family
revisited," Annual review of immunology 23:515-548, 2005. [41] C. L. Day, D. E. Kaufmann, P. Kiepiela, J. A. Brown, E. S. Moodley,
S. Reddy, E. W. Mackey, J. D. Miller, A. J. Leslie, C. DePierres et
al "PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression," Nature
443(7109):350-354, 2006.
[42] S. Urbani, B. Amadei, D. Tola, M. Massari, S. Schivazappa, G. Missale, C. Ferrari "PD-1 expression in acute hepatitis C virus
(HCV) infection is associated with HCV-specific CD8 exhaustion,"
J Virol 80(22):11398-11403, 2006. [43] P. Greaves, J. G. Gribben "The role of B7 family molecules in
hematologic malignancy," Blood 121(5):734-744, 2013.
[44] B. Seliger, F. M. Marincola, S. Ferrone, H. Abken "The complex role of B7 molecules in tumor immunology," Trends in molecular
medicine 14(12):550-559, 2008.
[45] L. Christiansson, S. Soderlund, E. Svensson, S. Mustjoki, M. Bengtsson, B. Simonsson, U. Olsson-Stromberg, A. S. Loskog
"Increased level of myeloid-derived suppressor cells, programmed
death receptor ligand 1/programmed death receptor 1, and soluble CD25 in Sokal high risk chronic myeloid leukemia," PLoS One
8(1):e55818, 2013.
[46] R. Hehlmann, A. Hochhaus, M. Baccarani "Chronic myeloid leukaemia," Lancet 370(9584):342-350, 2007.
[47] A. Hochhaus, B. Druker, C. Sawyers, F. Guilhot, C. A. Schiffer, J.
Cortes, D. W. Niederwieser, C. Gambacorti-Passerini, R. M. Stone, J. Goldman et al "Favorable long-term follow-up results over 6
years for response, survival, and safety with imatinib mesylate
therapy in chronic-phase chronic myeloid leukemia after failure of interferon-alpha treatment," Blood 111(3):1039-1043, 2008.
[48] T. P. Hughes, J. Kaeda, S. Branford, Z. Rudzki, A. Hochhaus, M. L.
Hensley, I. Gathmann, A. E. Bolton, I. C. van Hoomissen, J. M. Goldman et al "Frequency of major molecular responses to imatinib
or interferon alfa plus cytarabine in newly diagnosed chronic
myeloid leukemia," The New England journal of medicine 349(15):1423-1432, 2003.
[49] S. G. O'Brien, F. Guilhot, R. A. Larson, I. Gathmann, M. Baccarani, F. Cervantes, J. J. Cornelissen, T. Fischer, A. Hochhaus, T. Hughes
et al "Imatinib compared with interferon and low-dose cytarabine
for newly diagnosed chronic-phase chronic myeloid leukemia," The New England journal of medicine 348(11):994-1004, 2003.
[50] F. P. Santos, H. Kantarjian, A. Quintas-Cardama, J. Cortes
"Evolution of therapies for chronic myelogenous leukemia," Cancer J 17(6):465-476, 2011.
[51] E. A. Hahn, G. A. Glendenning, M. V. Sorensen, S. A. Hudgens, B.
J. Druker, F. Guilhot, R. A. Larson, S. G. O'Brien, D. G. Dobrez, M. L. Hensley et al "Quality of life in patients with newly diagnosed
chronic phase chronic myeloid leukemia on imatinib versus
interferon alfa plus low-dose cytarabine: results from the IRIS Study," J Clin Oncol 21(11):2138-2146, 2003.
[52] A. Hochhaus, S. G. O'Brien, F. Guilhot, B. J. Druker, S. Branford, L.
Foroni, J. M. Goldman, M. C. Muller, J. P. Radich, M. Rudoltz et al "Six-year follow-up of patients receiving imatinib for the first-line
treatment of chronic myeloid leukemia," Leukemia
23(6):1054-1061, 2009. [53] J. Pinilla-Ibarz, J. Cortes, M. J. Mauro "Intolerance to tyrosine
kinase inhibitors in chronic myeloid leukemia: Definitions and
clinical implications," Cancer 117(4):688-697, 2011. [54] N. P. Shah, C. Tran, F. Y. Lee, P. Chen, D. Norris, C. L. Sawyers
"Overriding imatinib resistance with a novel ABL kinase inhibitor,"
Science (New York, NY 305(5682):399-401, 2004.
[55] O. Hantschel, U. Rix, G. Superti-Furga "Target spectrum of the BCR-ABL inhibitors imatinib, nilotinib and dasatinib," Leukemia &
lymphoma 49(4):615-619, 2008.
[56] T. Ernst, A. Hochhaus "Chronic myeloid leukemia: clinical impact of BCR-ABL1 mutations and other lesions associated with disease
progression," Seminars in oncology 39(1):58-66, 2012.
[57] A. Hochhaus, P. La Rosee, M. C. Muller, T. Ernst, N. C. Cross "Impact of BCR-ABL mutations on patients with chronic myeloid
leukemia," Cell Cycle 10(2):250-260, 2011.
[58] E. Weisberg, P. W. Manley, W. Breitenstein, J. Bruggen, S. W. Cowan-Jacob, A. Ray, B. Huntly, D. Fabbro, G. Fendrich, E.
Hall-Meyers et al "Characterization of AMN107, a selective
inhibitor of native and mutant Bcr-Abl," Cancer Cell 7(2):129-141, 2005.
[59] M. Golemovic, S. Verstovsek, F. Giles, J. Cortes, T. Manshouri, P.
W. Manley, J. Mestan, M. Dugan, L. Alland, J. D. Griffin et al "AMN107, a novel aminopyrimidine inhibitor of Bcr-Abl, has in
vitro activity against imatinib-resistant chronic myeloid leukemia,"
Clin Cancer Res 11(13):4941-4947, 2005. [60] A. Ray, S. W. Cowan-Jacob, P. W. Manley, J. Mestan, J. D. Griffin
"Identification of BCR-ABL point mutations conferring resistance
to the Abl kinase inhibitor AMN107 (nilotinib) by a random mutagenesis study," Blood 109(11):5011-5015, 2007.
[61] H. J. Khoury, J. E. Cortes, H. M. Kantarjian, C.
Gambacorti-Passerini, M. Baccarani, D. W. Kim, A. Zaritskey, A. Countouriotis, N. Besson, E. Leip et al "Bosutinib is active in
chronic phase chronic myeloid leukemia after imatinib and
dasatinib and/or nilotinib therapy failure," Blood 119(15):3403-3412, 2012.
[62] A. Hochhaus, M. Baccarani, M. Deininger, J. F. Apperley, J. H.
Lipton, S. L. Goldberg, S. Corm, N. P. Shah, F. Cervantes, R. T. Silver et al "Dasatinib induces durable cytogenetic responses in
patients with chronic myelogenous leukemia in chronic phase with
resistance or intolerance to imatinib," Leukemia 22(6):1200-1206, 2008.
[63] J. Cortes, P. Rousselot, D. W. Kim, E. Ritchie, N. Hamerschlak, S.
Coutre, A. Hochhaus, F. Guilhot, G. Saglio, J. Apperley et al "Dasatinib induces complete hematologic and cytogenetic
responses in patients with imatinib-resistant or -intolerant chronic
myeloid leukemia in blast crisis," Blood 109(8):3207-3213, 2007. [64] H. Kantarjian, R. Pasquini, N. Hamerschlak, P. Rousselot, J.
Holowiecki, S. Jootar, T. Robak, N. Khoroshko, T. Masszi, A.
Skotnicki et al "Dasatinib or high-dose imatinib for chronic-phase chronic myeloid leukemia after failure of first-line imatinib: a
randomized phase 2 trial," Blood 109(12):5143-5150, 2007.
[65] G. Saglio, D. W. Kim, S. Issaragrisil, P. le Coutre, G. Etienne, C. Lobo, R. Pasquini, R. E. Clark, A. Hochhaus, T. P. Hughes et al
"Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia," The New England journal of medicine
362(24):2251-2259, 2010.
[66] H. Kantarjian, N. P. Shah, A. Hochhaus, J. Cortes, S. Shah, M. Ayala, B. Moiraghi, Z. Shen, J. Mayer, R. Pasquini et al "Dasatinib
versus imatinib in newly diagnosed chronic-phase chronic myeloid
leukemia," The New England journal of medicine 362(24):2260-2270, 2010.
[67] Y. Deguchi, S. Kimura, E. Ashihara, T. Niwa, K. Hodohara, Y.
Fujiyama, T. Maekawa "Comparison of imatinib, dasatinib, nilotinib and INNO-406 in imatinib-resistant cell lines," Leukemia
research, 2008.
[68] S. Soverini, A. Hochhaus, F. E. Nicolini, F. Gruber, T. Lange, G. Saglio, F. Pane, M. C. Muller, T. Ernst, G. Rosti et al "BCR-ABL
kinase domain mutation analysis in chronic myeloid leukemia
patients treated with tyrosine kinase inhibitors: recommendations from an expert panel on behalf of European LeukemiaNet," Blood
118(5):1208-1215, 2011.
[69] J. E. Cortes, H. M. Kantarjian, T. H. Brummendorf, D. W. Kim, A. G. Turkina, Z. X. Shen, R. Pasquini, H. J. Khoury, S. Arkin, A.
Volkert et al "Safety and efficacy of bosutinib (SKI-606) in chronic
phase Philadelphia chromosome-positive chronic myeloid leukemia patients with resistance or intolerance to imatinib," Blood
118(17):4567-4576, 2011.

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
26
[70] M. Agrawal, R. J. Garg, J. Cortes, A. Quintas-Cardama "Tyrosine kinase inhibitors: the first decade," Current hematologic
malignancy reports 5(2):70-80, 2010.
[71] J. E. Cortes, D.-W. Kim, J. Pinilla-Ibarz, P. D. L. Coutre, R. Paquette, C. Chuah, F. E. Nicolini, J. F. Apperley, H. J. Khoury, M.
Talpaz et al: A Pivotal Phase 2 Trial of Ponatinib in Patients with
Chronic Myeloid Leukemia (CML) and Philadelphia Chromosome-Positive Acute Lymphoblastic Leukemia (Ph+ALL)
Resistant or Intolerant to Dasatinib or Nilotinib, or with the T315I
BCR-ABL Mutation: 12-Month Follow-up of the PACE Trial. In: Blood 2012: Abstract 163. 2012.
[72] M. Deininger, E. Buchdunger, B. J. Druker "The development of
imatinib as a therapeutic agent for chronic myeloid leukemia," Blood 105(7):2640-2653, 2005.
[73] U. Rix, O. Hantschel, G. Durnberger, L. L. Remsing Rix, M.
Planyavsky, N. V. Fernbach, I. Kaupe, K. L. Bennett, P. Valent, J. Colinge et al "Chemical proteomic profiles of the BCR-ABL
inhibitors imatinib, nilotinib, and dasatinib reveal novel kinase and
nonkinase targets," Blood 110(12):4055-4063, 2007. [74] O. Hantschel, U. Rix, U. Schmidt, T. Burckstummer, M. Kneidinger,
G. Schutze, J. Colinge, K. L. Bennett, W. Ellmeier, P. Valent et al
"The Btk tyrosine kinase is a major target of the Bcr-Abl inhibitor dasatinib," Proceedings of the National Academy of Sciences of the
United States of America 104(33):13283-13288, 2007.
[75] M. Bantscheff, D. Eberhard, Y. Abraham, S. Bastuck, M. Boesche, S. Hobson, T. Mathieson, J. Perrin, M. Raida, C. Rau et al
"Quantitative chemical proteomics reveals mechanisms of action of
clinical ABL kinase inhibitors," Nature biotechnology 25(9):1035-1044, 2007.
[76] K. C. Lee, I. Ouwehand, A. L. Giannini, N. S. Thomas, N. J. Dibb,
M. J. Bijlmakers "Lck is a key target of imatinib and dasatinib in T-cell activation," Leukemia 24(4):896-900, 2010.
[77] J. M. Bradshaw "The Src, Syk, and Tec family kinases: distinct
types of molecular switches," Cellular signalling 22(8):1175-1184, 2010.
[78] S. M. Feller "Crk family adaptors-signalling complex formation and
biological roles," Oncogene 20(44):6348-6371, 2001. [79] J. H. Ostrander, A. R. Daniel, C. A. Lange "Brk/PTK6 signaling in
normal and cancer cell models," Current opinion in pharmacology
10(6):662-669, 2010. [80] L. L. Remsing Rix, U. Rix, J. Colinge, O. Hantschel, K. L. Bennett,
T. Stranzl, A. Muller, C. Baumgartner, P. Valent, M. Augustin et al
"Global target profile of the kinase inhibitor bosutinib in primary chronic myeloid leukemia cells," Leukemia 23(3):477-485, 2009.
[81] P. Ling, T. J. Lu, C. J. Yuan, M. D. Lai "Biosignaling of mammalian
Ste20-related kinases," Cellular signalling 20(7):1237-1247, 2008. [82] J. Si, S. J. Collins "Activated Ca2+/calmodulin-dependent protein
kinase IIgamma is a critical regulator of myeloid leukemia cell proliferation," Cancer Res 68(10):3733-3742, 2008.
[83] T. O'Hare, W. C. Shakespeare, X. Zhu, C. A. Eide, V. M. Rivera, F.
Wang, L. T. Adrian, T. Zhou, W. S. Huang, Q. Xu et al "AP24534, a pan-BCR-ABL inhibitor for chronic myeloid leukemia, potently
inhibits the T315I mutant and overcomes mutation-based
resistance," Cancer Cell 16(5):401-412, 2009. [84] J. M. Gozgit, M. J. Wong, S. Wardwell, J. W. Tyner, M. M. Loriaux,
Q. K. Mohemmad, N. I. Narasimhan, W. C. Shakespeare, F. Wang,
B. J. Druker et al "Potent activity of ponatinib (AP24534) in models of FLT3-driven acute myeloid leukemia and other hematologic
malignancies," Molecular cancer therapeutics 10(6):1028-1035,
2011. [85] N. P. Restifo, M. E. Dudley, S. A. Rosenberg "Adoptive
immunotherapy for cancer: harnessing the T cell response," Nature
reviews Immunology 12(4):269-281, 2012. [86] T. Sasada, S. Suekane "Variation of tumor-infiltrating lymphocytes
in human cancers: controversy on clinical significance,"
Immunotherapy 3(10):1235-1251, 2011. [87] K. Rezvani "Posttransplantation vaccination: concepts today and on
the horizon," Hematology / the Education Program of the American
Society of Hematology American Society of Hematology Education Program 2011:299-304, 2011.
[88] J. M. Goldman, R. P. Gale, M. M. Horowitz, J. C. Biggs, R. E.
Champlin, E. Gluckman, R. G. Hoffmann, S. J. Jacobsen, A. M.
Marmont, P. B. McGlave et al "Bone marrow transplantation for chronic myelogenous leukemia in chronic phase. Increased risk for
relapse associated with T-cell depletion," Annals of internal
medicine 108(6):806-814, 1988. [89] A. B. Dietz, L. Souan, G. J. Knutson, P. A. Bulur, M. R. Litzow, S.
Vuk-Pavlovic "Imatinib mesylate inhibits T-cell proliferation in
vitro and delayed-type hypersensitivity in vivo," Blood 104(4):1094-1099, 2004.
[90] R. Seggewiss, K. Lore, E. Greiner, M. K. Magnusson, D. A. Price,
D. C. Douek, C. E. Dunbar, A. Wiestner "Imatinib inhibits T-cell receptor-mediated T-cell proliferation and activation in a
dose-dependent manner," Blood 105(6):2473-2479, 2005.
[91] K. Cwynarski, R. Laylor, E. Macchiarulo, J. Goldman, G. Lombardi, J. V. Melo, F. Dazzi "Imatinib inhibits the activation and
proliferation of normal T lymphocytes in vitro," Leukemia
18(8):1332-1339, 2004. [92] C. Leder, S. Ortler, R. Seggewiss, H. Einsele, H. Wiendl
"Modulation of T-effector function by imatinib at the level of
cytokine secretion," Experimental hematology 35(8):1266-1271, 2007.
[93] H. Gao, B. N. Lee, M. Talpaz, N. J. Donato, J. E. Cortes, H. M.
Kantarjian, J. M. Reuben "Imatinib mesylate suppresses cytokine synthesis by activated CD4 T cells of patients with chronic
myelogenous leukemia," Leukemia 19(11):1905-1911, 2005.
[94] J. Chen, A. Schmitt, B. Chen, M. Rojewski, M. Ringhoffer, S. von Harsdorf, J. Greiner, P. Guillaume, H. Dohner, D. Bunjes et al
"Imatinib impairs CD8+ T lymphocytes specifically directed
against the leukemia-associated antigen RHAMM/CD168 in vitro," Cancer Immunol Immunother 56(6):849-861, 2007.
[95] C. I. Chen, H. T. Maecker, P. P. Lee "Development and dynamics of
robust T-cell responses to CML under imatinib treatment," Blood 111(11):5342-5349, 2008.
[96] S. Mumprecht, M. Matter, V. Pavelic, A. F. Ochsenbein "Imatinib
mesylate selectively impairs expansion of memory cytotoxic T cells without affecting the control of primary viral infections," Blood
108(10):3406-3413, 2006.
[97] P. Sinai, R. E. Berg, J. M. Haynie, M. J. Egorin, R. L. Ilaria, Jr., J. Forman "Imatinib mesylate inhibits antigen-specific memory CD8
T cell responses in vivo," J Immunol 178(4):2028-2037, 2007.
[98] S. Blake, T. P. Hughes, G. Mayrhofer, A. B. Lyons "The Src/ABL kinase inhibitor dasatinib (BMS-354825) inhibits function of
normal human T-lymphocytes in vitro," Clinical immunology
(Orlando, Fla 127(3):330-339, 2008. [99] R. Weichsel, C. Dix, L. Wooldridge, M. Clement, A. Fenton-May,
A. K. Sewell, J. Zezula, E. Greiner, E. Gostick, D. A. Price et al
"Profound inhibition of antigen-specific T-cell effector functions by dasatinib," Clin Cancer Res 14(8):2484-2491, 2008.
[100] A. E. Schade, G. L. Schieven, R. Townsend, A. M. Jankowska, V. Susulic, R. Zhang, H. Szpurka, J. P. Maciejewski "Dasatinib, a
small-molecule protein tyrosine kinase inhibitor, inhibits T-cell
activation and proliferation," Blood 111(3):1366-1377, 2008. [101] F. Fei, Y. Yu, A. Schmitt, M. T. Rojewski, B. Chen, J. Greiner, M.
Gotz, P. Guillaume, H. Dohner, D. Bunjes et al "Dasatinib exerts an
immunosuppressive effect on CD8+ T cells specific for viral and leukemia antigens," Experimental hematology 36(10):1297-1308,
2008.
[102] C. K. Fraser, S. J. Blake, K. R. Diener, A. B. Lyons, M. P. Brown, T. P. Hughes, J. D. Hayball "Dasatinib inhibits recombinant viral
antigen-specific murine CD4+ and CD8+ T-cell responses and
NK-cell cytolytic activity in vitro and in vivo," Experimental hematology 37(2):256-265, 2009.
[103] J. Chen, A. Schmitt, B. Chen, M. Rojewski, V. Rubeler, F. Fei, Y.
Yu, X. Yu, M. Ringhoffer, S. von Harsdorf et al "Nilotinib hampers the proliferation and function of CD8+ T lymphocytes through
inhibition of T cell receptor signalling," Journal of cellular and
molecular medicine 12(5B):2107-2118, 2008. [104] N. P. van Erp, H. Gelderblom, H. J. Guchelaar "Clinical
pharmacokinetics of tyrosine kinase inhibitors," Cancer treatment
reviews 35(8):692-706, 2009. [105] B. J. Druker, M. Talpaz, D. J. Resta, B. Peng, E. Buchdunger, J. M.
Ford, N. B. Lydon, H. Kantarjian, R. Capdeville, S. Ohno-Jones et
al "Efficacy and safety of a specific inhibitor of the BCR-ABL

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
27
tyrosine kinase in chronic myeloid leukemia," The New England journal of medicine 344(14):1031-1037, 2001.
[106] K. Palucka, J. Banchereau "Cancer immunotherapy via dendritic
cells," Nature reviews Cancer 12(4):265-277, 2012. [107] K. Eisendle, D. Wolf, G. Gastl, B. Kircher-Eibl "Dendritic cells
from patients with chronic myeloid leukemia: functional and
phenotypic features," Leukemia & lymphoma 46(5):663-670, 2005. [108] M. Mohty, E. Jourdan, N. B. Mami, N. Vey, G. Damaj, D. Blaise, D.
Isnardon, D. Olive, B. Gaugler "Imatinib and plasmacytoid
dendritic cell function in patients with chronic myeloid leukemia," Blood 103(12):4666-4668, 2004.
[109] N. Sato, M. Narita, M. Takahashi, K. Yagisawa, A. Liu, T. Abe, K.
Nikkuni, T. Furukawa, K. Toba, Y. Aizawa "The effects of STI571 on antigen presentation of dendritic cells generated from patients
with chronic myelogenous leukemia," Hematological oncology
21(2):67-75, 2003. [110] N. Larmonier, N. Janikashvili, C. J. LaCasse, C. B. Larmonier, J.
Cantrell, E. Situ, T. Lundeen, B. Bonnotte, E. Katsanis "Imatinib
mesylate inhibits CD4+ CD25+ regulatory T cell activity and enhances active immunotherapy against BCR-ABL- tumors," J
Immunol 181(10):6955-6963, 2008.
[111] H. Wang, F. Cheng, A. Cuenca, P. Horna, Z. Zheng, K. Bhalla, E. M. Sotomayor "Imatinib mesylate (STI-571) enhances
antigen-presenting cell function and overcomes tumor-induced
CD4+ T-cell tolerance," Blood 105(3):1135-1143, 2005. [112] T. W. LeBien, T. F. Tedder "B lymphocytes: how they develop and
function," Blood 112(5):1570-1580, 2008.
[113] S. Catellani, I. Pierri, M. Gobbi, A. Poggi, M. R. Zocchi "Imatinib treatment induces CD5+ B lymphocytes and IgM natural antibodies
with anti-leukemic reactivity in patients with chronic myelogenous
leukemia," PLoS One 6(4):e18925, 2011. [114] G. Carulli, E. Cannizzo, V. Ottaviano, G. Cervetti, G. Buda, S.
Galimberti, C. Barate, A. Marini, M. Petrini "Abnormal phenotype
of bone marrow plasma cells in patients with chronic myeloid leukemia undergoing therapy with Imatinib," Leukemia research
34(10):1336-1339, 2010.
[115] J. L. Steegmann, G. Moreno, C. Alaez, S. Osorio, A. Granda, R. de la Camara, E. Arranz, F. G. Reino, F. R. Salvanes, J. M.
Fernandez-Ranada et al "Chronic myeloid leukemia patients
resistant to or intolerant of interferon alpha and subsequently treated with imatinib show reduced immunoglobulin levels and
hypogammaglobulinemia," Haematologica 88(7):762-768, 2003.
[116] G. Cervetti, G. Carulli, S. Galimberti, A. Azzara, E. Cannizzo, G. Buda, E. Orciuolo, M. Petrini "Reduction of immunoglobulin levels
during imatinib therapy of chronic myeloid leukemia," Leukemia
research 32(1):191-192, 2008. [117] R. Santachiara, R. Maffei, S. Martinelli, A. Arcari, F. Piacentini, E.
Trabacchi, P. Alfieri, A. Ferrari, G. Leonardi, G. Luppi et al "Development of hypogammaglobulinemia in patients treated with
imatinib for chronic myeloid leukemia or gastrointestinal stromal
tumor," Haematologica 93(8):1252-1255, 2008. [118] E. Vivier, S. Ugolini, D. Blaise, C. Chabannon, L. Brossay
"Targeting natural killer cells and natural killer T cells in cancer,"
Nature reviews Immunology 12(4):239-252, 2012. [119] C. I. Chen, S. Koschmieder, L. Kerstiens, M. Schemionek, B.
Altvater, S. Pscherer, J. Gerss, H. T. Maecker, W. E. Berdel, H.
Juergens et al "NK cells are dysfunctional in human chronic myelogenous leukemia before and on imatinib treatment and in
BCR-ABL-positive mice," Leukemia, 2011.
[120] J. Salih, J. Hilpert, T. Placke, F. Grunebach, A. Steinle, H. R. Salih, M. Krusch "The BCR/ABL-inhibitors imatinib, nilotinib and
dasatinib differentially affect NK cell reactivity," International
journal of cancer 127(9):2119-2128, 2010. [121] C. Cebo, S. Da Rocha, S. Wittnebel, A. G. Turhan, J. Abdelali, S.
Caillat-Zucman, J. H. Bourhis, S. Chouaib, A. Caignard "The
decreased susceptibility of Bcr/Abl targets to NK cell-mediated lysis in response to imatinib mesylate involves modulation of
NKG2D ligands, GM1 expression, and synapse formation," J
Immunol 176(2):864-872, 2006. [122] Y. Hayashi, H. Nakamae, T. Katayama, T. Nakane, H. Koh, M.
Nakamae, A. Hirose, K. Hagihara, Y. Terada, Y. Nakao et al
"Different immunoprofiles in patients with chronic myeloid
leukemia treated with imatinib, nilotinib or dasatinib," Leukemia & lymphoma 53(6):1084-1089, 2012.
[123] D. H. Kim, S. Kamel-Reid, H. Chang, R. Sutherland, C. W. Jung, H.
J. Kim, J. J. Lee, J. H. Lipton "Natural killer or natural killer/T cell lineage large granular lymphocytosis associated with dasatinib
therapy for Philadelphia chromosome positive leukemia,"
Haematologica 94(1):135-139, 2009. [124] S. J. Blake, A. Bruce Lyons, C. K. Fraser, J. D. Hayball, T. P.
Hughes "Dasatinib suppresses in vitro natural killer cell
cytotoxicity," Blood 111(8):4415-4416, 2008. [125] T. L. Whiteside "The tumor microenvironment and its role in
promoting tumor growth," Oncogene 27(45):5904-5912, 2008.
[126] D. Lindau, P. Gielen, M. Kroesen, P. Wesseling, G. J. Adema "The immunosuppressive tumour network: myeloid-derived suppressor
cells, regulatory T cells and natural killer T cells," Immunology
138(2):105-115, 2013. [127] K. Oleinika, R. J. Nibbs, G. J. Graham, A. R. Fraser "Suppression,
subversion and escape: the role of regulatory T cells in cancer
progression," Clinical and experimental immunology 171(1):36-45, 2013.
[128] I. Poschke, D. Mougiakakos, R. Kiessling "Camouflage and
sabotage: tumor escape from the immune system," Cancer Immunol Immunother 60(8):1161-1171, 2011.
[129] H. Nishikawa, S. Sakaguchi "Regulatory T cells in tumor
immunity," International journal of cancer 127(4):759-767, 2010. [130] J. Chen, A. Schmitt, K. Giannopoulos, B. Chen, M. Rojewski, H.
Dohner, D. Bunjes, M. Schmitt "Imatinib impairs the proliferation
and function of CD4+CD25+ regulatory T cells in a dose-dependent manner," International journal of oncology 31(5):1133-1139,
2007.
[131] F. Fei, Y. Yu, A. Schmitt, M. T. Rojewski, B. Chen, M. Gotz, H. Dohner, D. Bunjes, M. Schmitt "Dasatinib inhibits the proliferation
and function of CD4+CD25+ regulatory T cells," British journal of
haematology 144(2):195-205, 2009. [132] F. Fei, Y. Yu, A. Schmitt, M. T. Rojewski, B. Chen, J. Greiner, M.
Gotz, D. Bunjes, M. Schmitt "Effects of nilotinib on regulatory T
cells: the dose matters," Molecular cancer 9:22, 2010. [133] S. Assouline, P. Laneuville, C. Gambacorti-Passerini "Panniculitis
during dasatinib therapy for imatinib-resistant chronic myelogenous
leukemia," The New England journal of medicine 354(24):2623-2624, 2006.
[134] B. B. Duman, S. Paydas, U. Disel, A. Besen, E. Gurkan "Secondary
malignancy after imatinib therapy: eight cases and review of the literature," Leukemia & lymphoma 53(9):1706-1708, 2012.
[135] D. Verma, H. Kantarjian, S. S. Strom, M. B. Rios, E. Jabbour, A.
Quintas-Cardama, S. Verstovsek, F. Ravandi, S. O'Brien, J. Cortes "Malignancies occurring during therapy with tyrosine kinase
inhibitors (TKIs) for chronic myeloid leukemia (CML) and other hematologic malignancies," Blood 118(16):4353-4358, 2011.
[136] P. R. Pilot, K. Sablinska, S. Owen, A. Hatfield "Epidemiological
analysis of second primary malignancies in more than 9500 patients treated with imatinib," Leukemia 20(1):148; author reply 149,
2006.
[137] R. Garcia-Munoz, A. Galar, C. Moreno, P. Rodriguez-Otero, E. Panizo-Morgado, M. Ponz-Sarvise, M. Fernandez-Alonso, M.
Rubio, J. Merino, B. Cuesta et al "Parvovirus B19 acute infection
and a reactivation of cytomegalovirus and herpesvirus 6 in a chronic myeloid leukemia patient during treatment with dasatinib
(BMS-354825)," Leukemia & lymphoma 48(12):2461-2464, 2007.
[138] S. Mustjoki, M. Ekblom, T. P. Arstila, I. Dybedal, P. K. Epling-Burnette, F. Guilhot, H. Hjorth-Hansen, M. Hoglund, P.
Kovanen, T. Laurinolli et al "Clonal expansion of T/NK-cells
during tyrosine kinase inhibitor dasatinib therapy," Leukemia 23(8):1398-1405, 2009.
[139] H. Tanaka, S. Nakashima, M. Usuda "Rapid and sustained increase
of large granular lymphocytes and rare cytomegalovirus reactivation during dasatinib treatment in chronic myelogenous
leukemia patients," International journal of hematology
96(3):308-319, 2012. [140] P. Rohon, K. Porkka, S. Mustjoki "Immunoprofiling of patients
with chronic myeloid leukemia at diagnosis and during tyrosine
kinase inhibitor therapy," Eur J Haematol 85(5):387-398, 2010.

INTERNATIONAL TRENDS IN IMMUNITY VOL.1 NO.3 JULY 2013 ISSN
ISSN 2326-3121 (Print) ISSN 2326-313X (Online) http://www.researchpub.org/journal/iti/iti.html
28
[141] I. Hus, J. Tabarkiewicz, M. Lewandowska, M. Wasiak, P. Wdowiak, M. Kusz, M. Legiec, A. Dmoszynska, J. Rolinski "Evaluation of
monocyte-derived dendritic cells, T regulatory and Th17 cells in
chronic myeloid leukemia patients treated with tyrosine kinase inhibitors," Folia Histochem Cytobiol 49(1):153-160, 2011.
[142] A. Kreutzman, V. Juvonen, V. Kairisto, M. Ekblom, L. Stenke, R.
Seggewiss, K. Porkka, S. Mustjoki "Mono/oligoclonal T and NK cells are common in chronic myeloid leukemia patients at diagnosis
and expand during dasatinib therapy," Blood 116(5):772-782, 2010.
[143] D. Marin, I. H. Gabriel, S. Ahmad, L. Foroni, H. Lavallade, R. Clark, S. O'Brien, R. Sergeant, C. Hedgley, D. Milojkovic et al "KIR2DS1
genotype predicts for complete cytogenetic response and survival in
newly diagnosed chronic myeloid leukemia patients treated with imatinib," Leukemia 26(2):296-302, 2012.
[144] S. Ali, R. Sergeant, S. G. O'Brien, L. Foroni, C. Hedgley, G. Gerrard,
D. Milojkovic, K. Stringaris, A. Khoder, A. Alsuliman et al "Dasatinib may overcome the negative prognostic impact of
KIR2DS1 in newly diagnosed patients with chronic myeloid
leukemia," Blood 120(3):697-698, 2012. [145] A. Kreutzman, T. Jaatinen, D. Greco, E. Vakkila, J. Richter, M.
Ekblom, H. Hjorth-Hansen, L. Stenke, T. Melo, R. Paquette et al
"Killer-cell immunoglobulin-like receptor gene profile predicts good molecular response to dasatinib therapy in chronic myeloid
leukemia," Experimental hematology 40(11):906-913 e901, 2012.
[146] G. La Nasa, G. Caocci, R. Littera, S. Atzeni, A. Vacca, O. Mulas, M. Langiu, M. Greco, S. Orru, N. Orru et al "Homozygosity for killer
immunoglobin-like receptor haplotype A predicts complete
molecular response to treatment with tyrosine kinase inhibitors in chronic myeloid leukemia patients," Experimental hematology
41(5):424-431, 2013.
[147] S. Mustjoki, T. Lundan, S. Knuutila, K. Porkka "Appearance of bone marrow lymphocytosis predicts an optimal response to
imatinib therapy in patients with chronic myeloid leukemia,"
Leukemia 21(11):2363-2368, 2007. [148] J. N. Valent, C. A. Schiffer "Prevalence of large granular
lymphocytosis in patients with chronic myelogenous leukemia
(CML) treated with dasatinib," Leukemia research 35(1):e1-3, 2011.
[149] S. J. Lee, C. W. Jung, D. Y. Kim, K. H. Lee, S. K. Sohn, J. Y. Kwak,
H. J. Kim, I. H. Kim, S. Park, D. H. Kim "Retrospective multicenter study on the development of peripheral lymphocytosis following
second-line dasatinib therapy for chronic myeloid leukemia,"
American journal of hematology 86(4):346-350, 2011. [150] K. Porkka, H. J. Khoury, R. L. Paquette, Y. Matloub, R. Sinha, J. E.
Cortes "Dasatinib 100 mg once daily minimizes the occurrence of
pleural effusion in patients with chronic myeloid leukemia in chronic phase and efficacy is unaffected in patients who develop
pleural effusion," Cancer 116(2):377-386, 2010. [151] H. Narumi, K. Kojima, Y. Matsuo, H. Shikata, K. Sekiya, T. Niiya,
S. Bando, H. Niiya, T. Azuma, Y. Yakushijin et al "T-cell large
granular lymphocytic leukemia occurring after autologous peripheral blood stem cell transplantation," Bone marrow
transplantation 33(1):99-101, 2004.
[152] R. Leskinen "CD4 and CD8 expression of large granular lymphocytes after bone marrow transplantation and its effect on
lymphocyte CD4/CD8 ratio," APMIS 101(2):149-153, 1993.
[153] G. Rondon, S. Giralt, Y. Huh, I. Khouri, B. Andersson, M. Andreeff, R. Champlin "Graft-versus-leukemia effect after allogeneic bone
marrow transplantation for chronic lymphocytic leukemia," Bone
marrow transplantation 18(3):669-672, 1996. [154] W. Y. Au, C. C. Lam, A. K. Lie, A. Pang, Y. L. Kwong "T-cell large
granular lymphocyte leukemia of donor origin after allogeneic bone
marrow transplantation," American journal of clinical pathology 120(4):626-630, 2003.
[155] H. Chang, S. Kamel-Reid, N. Hussain, J. Lipton, H. A. Messner
"T-cell large granular lymphocytic leukemia of donor origin occurring after allogeneic bone marrow transplantation for B-cell
lymphoproliferative disorders," American journal of clinical
pathology 123(2):196-199, 2005. [156] S. Mustjoki, K. Auvinen, A. Kreutzman, P. Rousselot, S.
Hernesniemi, T. Melo, A. M. Lahesmaa-Korpinen, S. Hautaniemi, S.
Bouchet, M. Molimard et al "Rapid mobilization of cytotoxic lymphocytes induced by dasatinib therapy," Leukemia
27(4):914-924, 2013.
[157] H. Joensuu "Adjuvant treatment of GIST: patient selection and treatment strategies," Nature reviews Clinical oncology
9(6):351-358, 2012.
[158] A. Sawaki, T. Nishida, T. Doi, Y. Yamada, Y. Komatsu, T. Kanda, Y. Kakeji, Y. Onozawa, M. Yamasaki, A. Ohtsu "Phase 2 study of
nilotinib as third-line therapy for patients with gastrointestinal
stromal tumor," Cancer 117(20):4633-4641, 2011. [159] K. Adekola, M. Agulnik "Advances in adjuvant therapy of
gastrointestinal stromal tumors," Current oncology reports
14(4):327-332, 2012. [160] V. P. Balachandran, M. J. Cavnar, S. Zeng, Z. M. Bamboat, L. M.
Ocuin, H. Obaid, E. C. Sorenson, R. Popow, C. Ariyan, F. Rossi et
al "Imatinib potentiates antitumor T cell responses in gastrointestinal stromal tumor through the inhibition of Ido," Nat
Med 17(9):1094-1100, 2011.
[161] N. P. Shah, F. Y. Lee, R. Luo, Y. Jiang, M. Donker, C. Akin "Dasatinib (BMS-354825) inhibits KITD816V, an
imatinib-resistant activating mutation that triggers neoplastic
growth in most patients with systemic mastocytosis," Blood 108(1):286-291, 2006.
[162] Y. Yang, C. Liu, W. Peng, G. Lizee, W. W. Overwijk, Y. Liu, S. E.
Woodman, P. Hwu "Antitumor T-cell responses contribute to the effects of dasatinib on c-KIT mutant murine mastocytoma and are
potentiated by anti-OX40," Blood 120(23):4533-4543, 2012.
[163] T. P. Hughes, S. Branford "Monitoring disease response to tyrosine kinase inhibitor therapy in CML," Hematology / the Education
Program of the American Society of Hematology American Society
of Hematology Education Program:477-487, 2009. [164] S. Mustjoki, J. Richter, G. Barbany, H. Ehrencrona, T. Fioretos, T.
Gedde-Dahl, B. T. Gjertsen, R. Hovland, S. Hernesniemi, D.
Josefsen et al "Impact of malignant stem cell burden on therapy outcome in newly diagnosed chronic myeloid leukemia patients,"
Leukemia, 2013.
[165] C. Preudhomme, J. Guilhot, F. E. Nicolini, A. Guerci-Bresler, F. Rigal-Huguet, F. Maloisel, V. Coiteux, M. Gardembas, C. Berthou,
A. Vekhoff et al "Imatinib plus peginterferon alfa-2a in chronic
myeloid leukemia," The New England journal of medicine 363(26):2511-2521, 2010.
[166] B. Simonsson, T. Gedde-Dahl, B. Markevarn, K. Remes, J. Stentoft,
A. Almqvist, M. Bjoreman, M. Flogegard, P. Koskenvesa, A. Lindblom et al "Combination of pegylated IFN-alpha2b with
imatinib increases molecular response rates in patients with low- or
intermediate-risk chronic myeloid leukemia," Blood 118(12):3228-3235, 2011.
[167] A. Burchert, M. C. Muller, P. Kostrewa, P. Erben, T. Bostel, S. Liebler, R. Hehlmann, A. Neubauer, A. Hochhaus "Sustained
molecular response with interferon alfa maintenance after induction
therapy with imatinib plus interferon alfa in patients with chronic myeloid leukemia," J Clin Oncol 28(8):1429-1435, 2010.
[168] M. Bocchia, S. Gentili, E. Abruzzese, A. Fanelli, F. Iuliano, A.
Tabilio, M. Amabile, F. Forconi, A. Gozzetti, D. Raspadori et al "Effect of a p210 multipeptide vaccine associated with imatinib or
interferon in patients with chronic myeloid leukaemia and persistent
residual disease: a multicentre observational trial," Lancet 365(9460):657-662, 2005.
[169] F. S. Hodi, S. J. O'Day, D. F. McDermott, R. W. Weber, J. A.
Sosman, J. B. Haanen, R. Gonzalez, C. Robert, D. Schadendorf, J. C. Hassel et al "Improved survival with ipilimumab in patients with
metastatic melanoma," The New England journal of medicine
363(8):711-723, 2010. [170] S. L. Topalian, F. S. Hodi, J. R. Brahmer, S. N. Gettinger, D. C.
Smith, D. F. McDermott, J. D. Powderly, R. D. Carvajal, J. A.
Sosman, M. B. Atkins et al "Safety, activity, and immune correlates of anti-PD-1 antibody in cancer," The New England journal of
medicine 366(26):2443-2454, 2012.