
Immunohistochemistry in the Heart: A Protocol Manual IN THE HEART: A PROTOCOL MANUAL ... For this...
26
Keele, JA 1 Immunohistochemistry in the Heart: A Protocol Manual By: Jacque A. Keele and Mark M. Stayton Department of Molecular Biology, University of Wyoming, Laramie, WY, 82071, USA July 2008 IMMUNOHISTOCHEMISTRY IN THE HEART: A PROTOCOL MANUAL ....... 1 PART I: INTRODUCTION AND BACKGROUND .................................................................... 3 PART II: MATERIALS AND METHODS ............................................................................. 19 PART III: DEFINITIONS- FROM THE HANDBOOK IMMUNOCHEMICAL STAINING METHODS 3 RD EDITION, DAKO CORPORATION (1)......................................................................... 23 REFERENCES .................................................................................................................. 26 Figure and Table List Figure 1: Diagrams of the binding of (A) polyclonal and (B) monoclonal antibodies to epitopes of an antigen. Note that polyclonal antibodies bind to many different epitopes while monoclonal antibodies bind to a single specific epitope. (C) The direct method where the primary antibody (green) is directly labeled with a tag (red dot) to the protein of interest (blue). (D) The two-step indirect method of detection. The protein of interest (blue) is first labeled with the primary antibody (green), the secondary antibody (yellow) binds to the primary antibody, and a fluorescent tag (red) is used for detection (1)...................................................................................... 9 Figure 2: Autofluorescence in a chemically fixed heart section. A) TRITC filter, B) FITC filter, C) merged image, 20x magnification .............................................................. 17 Figure 3: Autofluorescence of naïve heart tissue. (A) TRITC filter, (B) FITC filter, (C) Merged, (D) Dapi...................................................................................................... 17
-
Upload
truongthuy -
Category
Documents
-
view
219 -
download
2
Transcript of Immunohistochemistry in the Heart: A Protocol Manual IN THE HEART: A PROTOCOL MANUAL ... For this...

Keele, JA 1
Immunohistochemistry in the Heart: A Protocol Manual
By: Jacque A. Keele and Mark M. Stayton Department of Molecular Biology, University of Wyoming,
Laramie, WY, 82071, USA July 2008
IMMUNOHISTOCHEMISTRY IN THE HEART: A PROTOCOL MANUAL....... 1
PART I: INTRODUCTION AND BACKGROUND .................................................................... 3
PART II: MATERIALS AND METHODS ............................................................................. 19
PART III: DEFINITIONS- FROM THE HANDBOOK IMMUNOCHEMICAL STAINING METHODS
3RD EDITION, DAKO CORPORATION (1)......................................................................... 23
REFERENCES .................................................................................................................. 26
Figure and Table List Figure 1: Diagrams of the binding of (A) polyclonal and (B) monoclonal antibodies to
epitopes of an antigen. Note that polyclonal antibodies bind to many different
epitopes while monoclonal antibodies bind to a single specific epitope. (C) The
direct method where the primary antibody (green) is directly labeled with a tag (red
dot) to the protein of interest (blue). (D) The two-step indirect method of detection.
The protein of interest (blue) is first labeled with the primary antibody (green), the
secondary antibody (yellow) binds to the primary antibody, and a fluorescent tag
(red) is used for detection (1)...................................................................................... 9
Figure 2: Autofluorescence in a chemically fixed heart section. A) TRITC filter, B) FITC
filter, C) merged image, 20x magnification.............................................................. 17
Figure 3: Autofluorescence of naïve heart tissue. (A) TRITC filter, (B) FITC filter, (C)
Merged, (D) Dapi...................................................................................................... 17

Keele, JA 2
Figure 4: 40x Olympus microscope images of ARG2, two different slides. (A) ARG2
with stats, (B) Dapi, (C) merged, (D) ARG2 without stars, (E) Dapi, (F) merged... 18
Figure 5: Naïve expression of N-cadherin (1:2 dilution) of mouse heart using the
Olympus microscope 40X magnification. Changing the exposure time of the digital
camera can result in under or over exposure of the image. (A) Under exposed, (B)
Middle exposure time, (C) Overexposed .................................................................. 18
Figure 6: Selecting an image for publication. Double labeling of ARG1 (red) and SPSY
(green) in naïve mouse heart at 40X magnification.................................................. 18
Figure 7: A) Humidity control box with wet paper towel. B) Microscope slide with the
microscope slide holder in it. Note that one of the microscope slides has PBS on it
(volume approximately 150 µL). C) Washing the slides with PBS. D) Microscope
slide with the cover slide sealed on by nail polish.................................................... 22
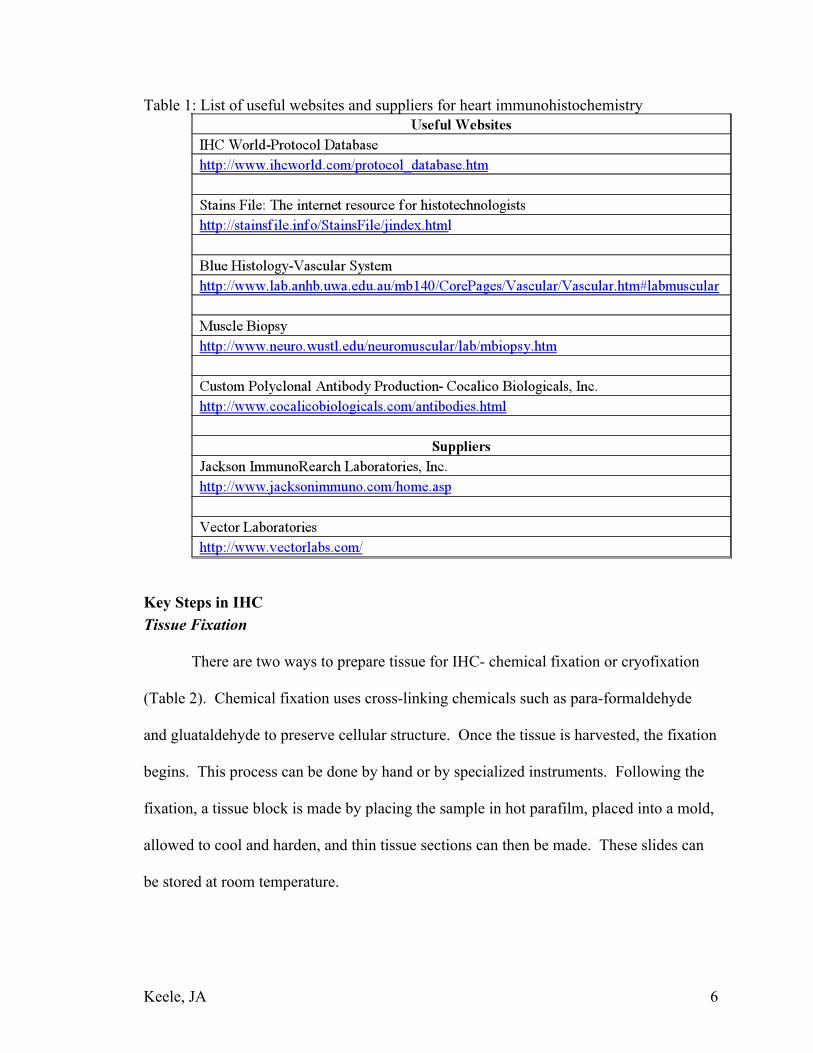
Table 1: List of useful websites and suppliers for heart immunohistochemistry ............... 6
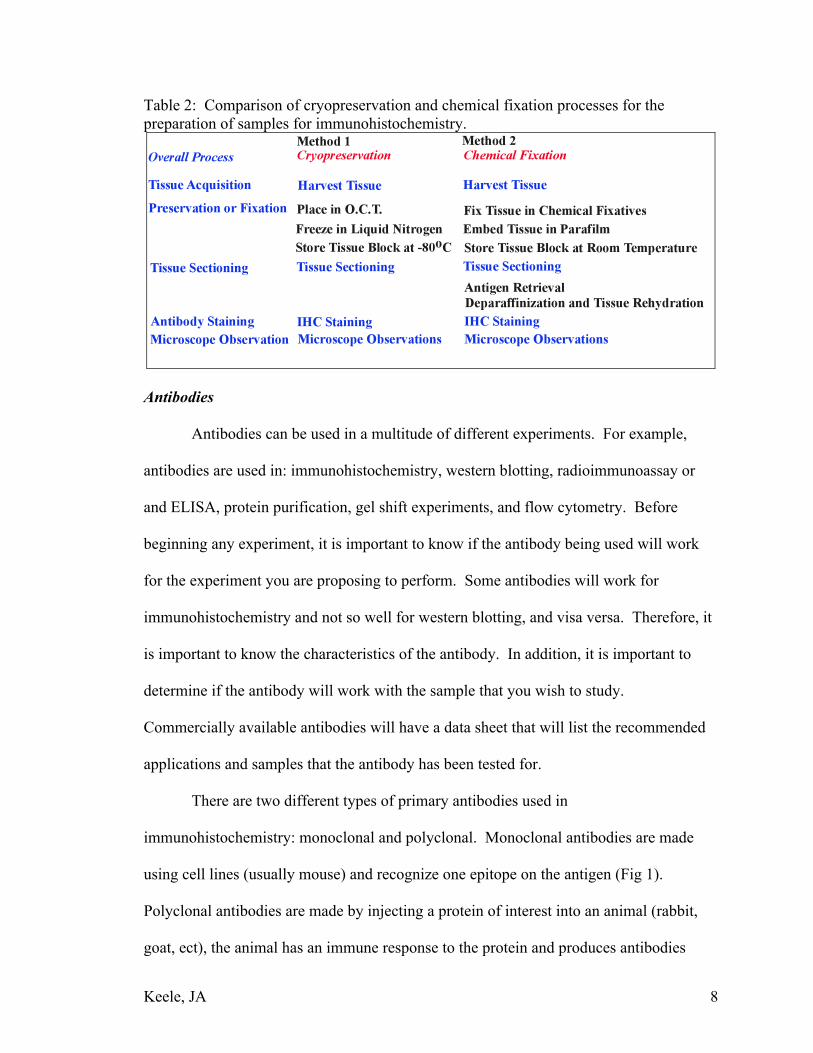
Table 2: Comparison of cryopreservation and chemical fixation processes for the
preparation of samples for immunohistochemistry..................................................... 8
Table 3: Phosphate Buffered Saline (PBS)....................................................................... 19

Keele, JA 3
Part I: Introduction and Background
Scientists have applied immunohistochemistry (IHC) to a wide variety of
organisms, tissues, and cells. The focus of this manual will be on mouse heart because it
is the tissue most studied in the Stayton Lab. The goal of the experiments performed in
the Stayton Lab was to determine the naïve expression pattern and subcellular location of
specific proteins in the heart. In addition, once the naïve expression pattern of the
proteins of interest were determined it was possible to observe changes in expression
patterns following the application of surgical acute myocardial infarction on the heart.
There are many different approaches to performing IHC; therefore, this manuals focus
will be on the general background information, the protocols, and troubleshooting
problems seen when working on mouse hearts. While the focus of this manual is on
mouse heart tissue, the background information in it can be applicable to other tissues
with modifications. The ultimate goal for anyone performing IHC should be
reproducible, reliable results (the three R’s). Obtaining this goal can be a challenge, but
it is possible to do when there is a basic understanding of the IHC process. Often
obtaining this goal can require weeks or sometimes months of trial and error to determine
the optimal conditions for tissue processing, staining, and microscope observations.
Immunohistochemistry (IHC) involves the study of cells and tissue.
Immunocytochemistry applies to the study of the intracellular activities of proteins.
These two words are now being used interchangeably in scientific publications and
presentations. Both of these techniques use antibodies to detect specific antigens in a
sample has been placed on a microscope slide.

Keele, JA 4
IHC is very similar to the method used for western blotting; both of these
methods involve blocking, primary and secondary antibody incubations, and finally
detection as key steps. Another technique that is gaining popularity is the use of green
fluorescent protein (GFP) labeled proteins. For this method, a transgenic animal is
produced that expresses GFP-fusion protein in the animal. The advantage of this method
is that tissue can be harvested from these animals, sectioned, and observed on the
microscope without IHC staining. The GFP will show you where your protein of interest
is located assuming that GFP does not alter the protein localization. While technique is
commonly used in yeast and C. elegans, using it in mice would require the production of
a transgenic animal. The cost of producing a GFP-labeled protein in a mouse when
compared to immunohistochemistry staining is high.
Using the Internet to Find Protocols
The internet is an amazing starting place for finding protocols, antibodies, and
supplies needed to perform IHC (Table 1). It is important to the researcher to find out as
much background information as possible on the antibodies and protocols they will be
using. For starters, you should find out if others have used the antibody for IHC. If they
have, then did they work on the same tissue or organism that you are interested in
studying? If they did, then using the protocol that they developed for the antibody is a
viable starting place for your own experiments. If there are not published data on your
antibody and organism the next step is to determine how others have prepared the sample
you are interested. By looking at how others have approached IHC with your sample,
you can avoid some of the problems and time involved in developing your own protocol.

Keele, JA 5
Protocols that are more detailed than those published in journals are available from the
antibody suppliers and from the website www.IHCworld.com.
Second, realize that getting a published report on both your antibody and sample
of interest can be a challenge. The majority of antibodies used in the Stayton Lab to label
proteins in the heart had very little data available as a starting place. In that case, we had
to develop our own protocols based on the IHC that others had done in the heart and
work our own conditions for staining for each of the antibodies.
Finally, if you purchase commercial antibodies they should come with a data
sheet that will show the methods the antibody can be used for, dilution factors, storage
conditions, and any publications in which the antibody was used. Before purchasing an
antibody, it is important to look at these data sheets and determine if the antibody that
you are thinking of purchasing is usable for IHC and compatible with the sample you are
interested studying. In addition, the data sheet can tell you if there are any special
considerations, you need to make when using the antibody (i.e. buffers, incubation times,
fixed or unfixed tissue).
Keele, JA 6
Table 1: List of useful websites and suppliers for heart immunohistochemistry
Key Steps in IHC Tissue Fixation There are two ways to prepare tissue for IHC- chemical fixation or cryofixation
(Table 2). Chemical fixation uses cross-linking chemicals such as para-formaldehyde
and gluataldehyde to preserve cellular structure. Once the tissue is harvested, the fixation
begins. This process can be done by hand or by specialized instruments. Following the
fixation, a tissue block is made by placing the sample in hot parafilm, placed into a mold,
allowed to cool and harden, and thin tissue sections can then be made. These slides can
be stored at room temperature.

Keele, JA 7
The thin sections on the slides need to be “de-cloaked’, so that antigens are
exposed. De-cloaking methods include heat and pressure treatment, enzyme digest, and
microwaving. Following the de-cloaking, the parafilm on the slides is removed by
baking, and the IHC staining process can begin. With these slides, autofluorescence is a
major concern and de-cloaking the epitopes can be difficult (Fig 2).
Cryofixation does not preserve the cellular structure quite as well as chemical
fixation, but the amount of autofluorescence seen with cryo-fixed tissue is substantially
less than the chemically fixed tissue. Cryofixation for heart muscle (or for any other type
of muscle) is done by using iso-butane cooled by liquid nitrogen. Hearts are placed in a
small mold or boat, and O.C.T. (Optical Cutting Temperature) is pored over the heart.
The boat is then dipped into the cold iso-butane, and the sample is cooled almost
immediately. Once the samples are in this block, they must be stored at -80oC until they
are sectioned. The O.C.T. helps to protect the tissue during the freezing process. Using
this method ensures that the sample is frozen as quickly and thus decreases the likelihood
of ice crystals forming that can damage the tissue.
Tissue sectioning of the heart is performed on a cryostat set at -18oC to -20oC.
Keeping the cryostat as cold as possible is key to obtaining good sections. When the
cryostat gets to warm, the O.C.T. will melt becoming gummy, and it will become
impossible to get clean sections. After the slides are made, they should be set out to air
dry for at least 10 minutes, and then stacked, wrapped in tinfoil, and stored at -80oC until
needed. Sections can be stored for long periods at -80oC if they properly protected.
Keele, JA 8
Table 2: Comparison of cryopreservation and chemical fixation processes for the preparation of samples for immunohistochemistry.
Antibodies
Antibodies can be used in a multitude of different experiments. For example,
antibodies are used in: immunohistochemistry, western blotting, radioimmunoassay or
and ELISA, protein purification, gel shift experiments, and flow cytometry. Before
beginning any experiment, it is important to know if the antibody being used will work
for the experiment you are proposing to perform. Some antibodies will work for
immunohistochemistry and not so well for western blotting, and visa versa. Therefore, it
is important to know the characteristics of the antibody. In addition, it is important to
determine if the antibody will work with the sample that you wish to study.
Commercially available antibodies will have a data sheet that will list the recommended
applications and samples that the antibody has been tested for.
There are two different types of primary antibodies used in
immunohistochemistry: monoclonal and polyclonal. Monoclonal antibodies are made
using cell lines (usually mouse) and recognize one epitope on the antigen (Fig 1).
Polyclonal antibodies are made by injecting a protein of interest into an animal (rabbit,
goat, ect), the animal has an immune response to the protein and produces antibodies

Keele, JA 9
against the protein. The serum is harvested and the antibodies are purified. For both
monoclonal and polyclonal antibodies, it is important to determine the optimal working
dilutions before starting to collect real data.
Detection of the protein is done directly with the primary antibody or indirectly
with a primary antibody that binds to a secondary antibody (Fig 1 c and d). The primary
antibody can be conjugated to a fluorescent tag. There are kits are available for
conjugating primary antibodies to tags. The more common way of detecting epitopes is
to use a labeled secondary antibody that will bind to the protein of interest.
Figure 1: Diagrams of the binding of (A) polyclonal and (B) monoclonal antibodies to epitopes of an antigen. Note that polyclonal antibodies bind to many different epitopes while monoclonal antibodies bind to a single specific epitope. (C) The direct method where the primary antibody (green) is directly labeled with a tag (red dot) to the protein of interest (blue). (D) The two-step indirect method of detection. The protein of interest (blue) is first labeled with the primary antibody (green), the secondary antibody (yellow) binds to the primary antibody, and a fluorescent tag (red) is used for detection (1). Secondary antibodies can be conjugated to an enzyme, biotin, or fluorescent tag.
This manual will focus on fluorescent labeling. When enzymes labeling is done, the
secondary antibody has to undergo a chemical reaction to produce a color product.
Secondary antibodies are usually absorbed against control animal serum to reduce
background staining. Choosing the correct secondary antibody is key to having the
experiment work out well. First, decide how the antibody will be detected, will it be with
fluorescence or the light microscope. Then pick the secondary antibody. There are

Keele, JA 10
companies that specialize in secondary antibodies (Jackson Immuno Research for
example) and have their catalogs posted on line. The variety of different secondary
antibodies can be overwhelming. Companies selling the primary antibodies will usually
have a data sheet where they tell you the recommended secondary antibody to use. In
addition, it is also advisable to call the company’s technical support and get an experts
opinion about the secondary antibody before making the purchase.
It is important plan out IHC experiments prior to purchasing antibodies for several
reasons. First, antibodies are expensive (primary antibodies start at $200 and go up) and
you do not want to buy antibodies that are not compatible with your samples. Second, if
multiple antigen labeling is going to be done it is important to know if the antibodies are
compatible with each other. Third, it is possible to shop around for your antibodies to get
a better price because there are many companies selling primary antibodies. Finally, take
the time to read up on the antibodies that you will buy. Some antibodies work only under
certain conditions (blocking buffer, antibody dilution, and ect.) and it is important to
know these details prior to using the antibody. Purchasing antibodies is an investment
and like all good investments, it is very important to do background research.
Antibodies should be stored according to the manufacturer’s recommendations.
Usually it is advised that the antibodies should be stored at 4oC to avoid freezing and
thawing cycles. It is also possible to aliquot the antibody for long-term storage at -80oC
using instructions provided by the manufacturer.

Keele, JA 11
Immunohistochemistry Staining In Part II, of this appendix, the protocols used for double labeling are laid out in
detail. However, in every protocol, minor details or lessons learned sometimes are left
out that can help to make IHC process work more efficiently. This section will discuss
some of the do’s, don’ts, and why’s of IHC that might seem like common sense, but that
can be forgotten in the rush to get results.
First, it is always important to work with fresh buffers and solutions. The
antibody and blocking buffers should be made fresh every few days to ensure that the
components in these buffers do not degrade. This can lead to a decrease in the quality of
the IHC staining. Second, it is important to determine the optimal antibody dilution for
the experiments. After looking at several different dilutions, you determine which of the
dilutions gives the “best” staining. Finally, the washes done with PBS after the primary
and secondary antibody incubations are very important. If they are not sufficiently
stringent, there can be over-staining, artifacts, and stars (see troubleshooting images).
Quality control is also an important factor to consider when setting up IHC
experiments. If possible, it is important to have a positive tissue control that will show if
the antibody is working correctly. Negative controls, where the primary antibody is
absent, are used to assess if the secondary antibody is binding non-specifically to the
tissue. If non-specific secondary binding is seen then changes in the blocking buffer
must be made. In addition, you want to have consistent results over time. If the
antibody-staining pattern changes every time you do an experiment, then something is
wrong with your experimental set up. The goal for anyone performing these types of

Keele, JA 12
experiments has to be reproducible reliable results (the three R’s) that anyone in the lab
can obtain.
Blocking is a vital step for IHC. Blocking buffer should contain serum from the
animal from which the secondary antibody was raised. This is done to avoid having the
secondary antibody bind non-specifically to the tissue. For example, if the primary
antibody was raised in a rabbit, then your secondary antibody will have to be anti-rabbit.
If the secondary is goat anti-rabbit, then you will need goat serum in the blocking buffer.
The composition of the blocking buffer can change depending on the antibodies that are
being studied. BSA can be in the blocking buffer; however, some secondary antibodies
will bind non-specifically to BSA creating a false-positive result. So with these
antibodies, BSA is omitted from the blocking buffer. Optimizing the blocking buffer can
help you avoid background staining and false-positive results. Knowing about these
simple yet very important details can help to ensure clean reliable reproducible IHC
results.
Microscope Observations, Photography, and Data Analysis
Books have been written about the ways to make microscope observations,
photography and data analysis. This section will briefly discuss several of the common
issues that were encountered and overcome when studying the mouse heart with IHC.
First, all tissue has some natural fluorescence associated with it (Fig 3). Therefore, when
working with the fluorescent microscope it is important to keep in mind that the tissue
will autofluorescence and might give misleading results. To control for this, a slide
without any antibodies on it should be observed to assess the natural fluorescence of the

Keele, JA 13
tissue. In particular, it is important to determine if the autofluorescence is located in a
specific place or is through out the tissue sample.
When making microscope observations it is important to understand what the
unstained sample should look like. Knowing this will help you determine if your sample
looks normal or abnormal when compared to the published images. The process of
cryofixation and then sectioning can damage the tissue. Sectioning can tear the tissue,
the knife can cause ridges and nicks in the sample, and tissue can become folded.
Additionally, there can be trash (hairs, dust, and ect.) on the slide that can cause
interference with the analysis. Sometimes the trash will be fluorescent and give false
results. These are all issues that can be hard to prevent, so it is important to be aware of
them.
There are some key controls that should be done to determine the background
fluorescence on the slides that are being stained. First, a slide without any antibodies
should be done to show the natural fluorescence associated with the tissue of interest.
Second, it is important to determine if the secondary antibody is binding to the tissue. If
this happens adjustments in the blocking buffer must be made to ensure that the results
are true and not due to non-specific binding of the secondary antibody.
It is important to know and understand the sample under observation so
judgments can be made on whether the cryo-fixation or sectioning damaged the tissue.
So finding published images of the sample you are looking at can help you judge if the
sample is undamaged by the steps that went into making the section. In addition, it is
important to use control antibody markers to identify the cell type the protein of interest

Keele, JA 14
co-localizes to. DAPI is also a valuable tool in determining where DNA in the cells is
located.
Once an image is taken, it should be saved with as much identifying information
as possible. For instance, the date, tissue type, antibody dilution, tissue treatment, and
magnification of the microscope are all important information to know that will make
analyzing the images easier. Never make changes to the original image file. When you
begin to analyze the images, always open the image and then do a save as. IHC images
can be analyzed using the free software from the National Institutes of Health, ImageJ
(http://rsb.info.nih.gov/ij/). The website that provides this free software has tutorials on
how to utilize ImageJ. This program will allow you to merge images for double labeling,
and to make adjustment with the brightness and contrast of the images. It is a valuable
tool for analyzing and making the images ready for publication. Quantification of the
signal in IHC images is a recent development, and should be approached with great care
and thought. The software and algorithms needed to perform quantitative
immunohistochemistry have yet to be fully developed (2).
Troubleshooting- Examples of When Things Go Wrong
The following figures illustrate some of the common things that can go wrong with
IHC. Some of these things cannot be avoided (autofluorescence, artifacts, folded tissue)
while others can be controlled (stars, over and under staining, camera exposure). One
simple way to avoid making a time consuming mistake is to start out by doing single
labeling of the antibodies under study. Once the conditions staining have been
determined then it is possible to move into double labeling. If complex multi-labeling

Keele, JA 15
experiments are attempted from the start, mistakes will be made and it will be hard to
diagnose where the missteps are in the experimental design.
The goal should always be clean reproducible reliable results (the three R’s). Taking
clear and complete notes on everything that is done to the sections is important, because
with IHC the little things really do matter. Slight changes in incubation times, buffers,
and antibodies can result in significant changes in the IHC results. Most antibody
companies have tables available for troubleshooting IHC on the internet. In addition, it is
possible to call and discuss troubleshooting issues with the company that you bought the
antibodies from.
Autofluorescence is always a concern. It is important to test the sample to
determine how much the sample fluoresces without any antibodies present. In Fig 3, the
autofluorescence for naïve mouse heart cryo-sectioned sample is shown. When these
images were taken the exposure time on the camera was set at maximum. The images
were processed using ImageJ software. In Fig 3-A and B, it is possible to see that the red
and green filters of the microscope show autofluorescence. The green channel is stronger
than the red channel as shown when the images are merged. When these images were
processed, the brightness and contrast of the picture had to be increased using ImageJ.
Unambiguous staining is shown in Fig 3-D with Dapi labeling. In this image, it is
possible to see what specific staining looks like when compared to autofluorescence.
Another issue that comes up with IHC is artifacts or damage to the tissue due to
sectioning. Artifacts can be very fluorescent and sometimes give false results. They can
also disrupt the analysis of the slide if they are present in a specific region of tissue you
are looking at. Damage to the sample by the sectioning process can result in folded

Keele, JA 16
tissue, rips or tears in the tissue, and knife marks. Artifacts are usually easy to see and
diagnosis.
One artifact that is harder to diagnosis is when there are small fluorescent dots on
the slide that are known as stars. These stars are the result of inadequate washes before
mounting of the sample. They are caused by unbound secondary antibody left on the
slide. To recognize stars, you look at an area on the slide where there is know tissue
section. If there are stars in that area, then you know that the pattern of staining on the
section is false and is not specific binding of your antibody. In Fig 4-A, shows a star
pattern with ARG2 staining. Fig 4-B shows what happened when the washes were made
more stringent.
Changing the exposure time of the camera can have drastic effects on the image
quality (Figure 5). Overexposing or underexposing the section can result in a loss of
information. Finding the right exposure time is vital for getting publication quality
images.
One of the tricky aspects of IHC is selecting an image for publication. Figure 6
shows naïve mouse heart that has been stained with ARG1 (red) and SPSY (green).
These images were analyzed using ImageJ. Looking at this selection of images it is hard
to pick an image that would stand up to the rigors of peer review. The majority of the
images have an inbalance in their color. In addition, there is some starring in figure 6-A
and 6-H. The only one that might be publishable is figure 6-D. When selecting an image
it is important to consider a few things. First, did the IHC staining process work
correctly? Can the results be reproduced on multiple occasions? The staining showed in
Fig 6 was the first attempt at double labeling these two antibodies, therefore the results

Keele, JA 17
are very preliminary and would not be published. Second, which image best represents
the data? How many images are should be taken to ensure that the staining pattern is
consistent over days and different sections of tissue? These questions should be
discussed within the lab and decisions should be made on how to address these issues.
Figure 2: Autofluorescence in a chemically fixed heart section. A) TRITC filter, B) FITC filter, C) merged image, 20x magnification
Figure 3: Autofluorescence of naïve heart tissue. (A) TRITC filter, (B) FITC filter, (C) merged image, (D) DAPI.

Keele, JA 18
Figure 4: 40x Olympus microscope images of ARG2, two different slides. (A) ARG2 with stars, (B) DAPI, (C) Merged, (D) ARG2 without stars, (E) DAPI, (F) Merged
Figure 5: Naïve expression of N-cadherin (1:2 dilution) of mouse heart using the Olympus microscope 40X magnification. Changing the exposure time of the digital camera can result in under or over exposure of the image. (A) Under exposed, (B) Middle exposure time, (C) Overexposed
Figure 6: Selecting an image for publication. Double labeling of ARG1 (red) and SPSY (green) in naïve mouse heart at 40X magnification.

Keele, JA 19
Part II: Materials and Methods Buffers and Chemicals for Immunohistochemistry (All of these solutions are adapted from http://www.IHC.com protocols) Table 3: Main Buffer Used in IHC- Phosphate Buffered Saline (PBS) PBS pH 7.2 10X- 0.1M 20X- 0.2 M Na2HPO4 (anhydrous) 10.9 g 21.8 g NaH2PO4 (anhydrous) 3.2 g 6.4 g NaCl 90 g 180 g Distilled water 1000 mL 1000 mL Store this solution at room temperature. Dilute with distilled water before use, adjust pH to 7.2, and autoclave the solution. Blocking Buffer Normal Serum Blocking Solution: 2% serum (blocking) 1
1% BSA (stabilizer) 2
0.1% cold fish skin gelatin (blocking) 3
0.1% Triton X-100 (penetration enhancer) 0.05% Tween 20 (detergent and surface tension reducer) 0.05% sodium azide (preservative) 4 0.01M PBS, pH 7.2 Mix well and store at 4 ºC. Be aware that every antibody is different and adjustments will most likely be needed for the blocking buffer. Antibody Buffer Primary Antibody Dilution Buffer: 1% BSA (stabilizer and blocking) 0.1% cold fish skin gelatin (blocking)5 0.05% sodium azide (preservative) 6
1 Use serum from the animal that your secondary antibody was raised in. For example, if you are using a goat anti-rabbit secondary antibody then you will block with goat serum. In addition, if you are double labeling, you will block with two different serums. 2 BSA can cause background when used with certain secondary antibodies, so be aware of your secondary antibodies instructions. 3 Knox gelatin can be used in place of fish skin gelatin. 4 By making a small amount of blocking buffer and using it within a week, you can avoid the use of sodium azide. 5 Using Knox gelatin instead of the cold fish skin gelatin does not seem to affect the results obtained. 6 By making fresh dilutions of the primary antibodies right before they are used the addition of sodium azide can be avoided.

Keele, JA 20
0.01M PBS pH 7.2 (TBS pH 7.6 used in primary antibody dilution buffer produces weaker staining) Antibodies diluted using this buffer can be stored at 4 ºC for 6 months without reducing binding activity. This buffer cannot be used for diluting HRP conjugated antibodies since sodium azide is an inhibitor of HRP. Secondary Antibody Dilution Buffer: 0.01M PBS, pH 7.2 0.05% sodium azide (preservative) 7
Antibodies diluted using this buffer can be stored at 4 ºC for 6 months without reducing binding activity. Do not use BSA or other serum containing reagents to dilute secondary antibodies since they may bind to BSA or serum therefore reducing antibody affinity. Using TBS to dilute secondary antibodies often produces weaker staining. So use TBS only for the antibodies with high background staining or for alkaline phosphatase conjugated antibodies since phosphate is an inhibitor of alkaline phosphatase.
Anti-fade Mounting Medium8 2% n-propyl gallate 9 49% PBS pH 7.4 49% glycerol 0.5-1.0 ug/mL Dapi (final concentration)10
7 By making fresh dilutions of the secondary antibodies right before they are used the addition of sodium azide can be avoided. 8 Store the mounting medium at -20oC, wrapped in tin foil. It is light sensitive and will last longer if properly. From Dr. Z.J. Zhang, University of Wyoming 9 To prepare a stock solution of n-propyl gallate: 0.1M solution in 9:1 glycerol: PBS then place 0.1 g n-propyl gallate into 5 ml of glycerol: PBS. 10 Dapi can be left out of the anti-fade medium.

Keele, JA 21
Protocol for Double Labeling with Immunohistochemistry Parallel Approach (Adapted from http://www.IHC background/Immunofluorescence Double Staining Protocol.htm) Prior to perform double labeling, it is important to test each primary antibody individually and select the best pretreatment for each antibody (3). It will be ideal if the two primary antibodies require same pretreatment. Otherwise, one should do a further test by treating sections with both pretreatments and then immunostain for each antibody individually. If both antibodies survive the “double pretreatments”, you are ready for immunohistochemistry double staining. Overall IHC Method11 -Frozen Sections
a. Snap frozen fresh tissues in isopentane pre-cooled in liquid nitrogen, embedded in OCT compound in cryomolds. Store frozen blocks at -80 ºC.
b. Cut 4-8 µm-thick cryostat sections and mount on superfrost plus slides, gelatin-coated slides, or 1% silane coated slides. Store slides at - 80 ºC until needed.
c. Before staining, warm slides at room temperature for 30 minutes and fix in ice-cold acetone for 5 minutes. Air-dry for 30 minutes.
d. Wash in PBS for 2 x 2 minutes -Blocking e. Incubate sections in normal serum blocking solution – species same as secondary
antibody for 20 minutes (for example: primary antibodies are mouse and rabbit, and secondary antibodies are horse anti-mouse, and goat anti-rabbit, so horse and goat serum block should be used).
a. Made sure that the blocking buffer covers the sections, it should take less than 100 µL of liquid.
b. Do not let the slides dry out. Place the slides in a closed container with a damp towel to maintain the humidly. (Figure 7a)
c. Place the slides on the metal rack (Figure 7b) -Primary Antibodies
f. Incubate sections in the mixture of two primary antibodies at appropriate dilution in primary antibody dilution buffer for 1 hour at room temperature or at 4oC overnight.
a. Make sure the antibody mixture covers the sample. It should take less than 100 µL of liquid to cover the sample.
g. Rinse in PBS for 3x2 minutes (raise the metal rack to allow the liquid to drain off Figure 7c)
-Secondary Antibodies h. Incubate sections in a mixture of the two fluorescent conjugated secondary
antibodies for 30 minutes at room temperature. Make sure to do this in the dark. i. Rinse in PBS for 3x2 minutes
11 Sources for the supplies and equipment are listed in Table 5; in addition, materials can be obtained from chemical and equipment supply companies (such as Vector, Sigma-Aldrich, or the on campus Chemical Stock Room).

Keele, JA 22
-Mounting j. Place anti-fade mounting media on the sample- about 10 µL will cover the
sample. k. Place a glass cover slide over the sample l. Use nail polish to seal the cover slide to the microscope slide by painting on at
least two of cover slides sides (figure 7d) m. Store slide in the dark at 4oC
Figure 7: A) Humidity control box with wet paper towel. B) Microscope slide with the microscope slide holder in it. Note that one of the microscope slides has PBS on it (volume approximately 150 µL). C) Washing the slides with PBS. D) Microscope slide with the cover slide sealed on by nail polish.

Keele, JA 23
Part III: Definitions- From the Handbook Immunochemical Staining Methods 3rd Edition, DAKO Corporation (1). Antigen- a molecule that is capable of binding to an antibody Antigen retrieval (AR) - also known by the terms “epitope retrieval” or “target retrieval”, pertains to the restoration of antigenicity (immunoreactivity) to an immungen Antiserum- a serum that contains antibodies Ascites or ascetic fluid- an accumulation of fluid in the abdominal cavity Background- unless defined otherwise, background staining includes all nonspecific staining because of procedural artifacts. Occasionally, it may also include “undesirable” staining, e.g. due to diffused antigen Chromogen- one of a group of chemical species that can form a particular colored material or can be identified by such a reaction with an appropriate reagent Counterstain- a second stain that provides a contrasting effect to another stain Cross-reactivity- the ability of an antibody to react with antigens other that the immunogen. The term should not be used when referring to reactions occurring between an antibody and different cell or tissue components. Epitope- the structural part of an antigen that reacts with an antibody. These are groupings of amino acids in globular proteins and sugar side-chains in polysaccharides. The most critical part is called the immunodominant point. Immunochemistry- the branch of immunology concerned with the chemical substances and reactions of the immuno system, the specific study of antigens and antibodies and their interactions with one another. Immunocytochemistry- immunochemistry applied to the study of intracellular activities. (Now frequently used interchangeably with immunohistochemistry.) Immunogen- any substance capable of generating an immune reaction, in contrast to any substance that binds to an antibody (i.e., an antigen) Immunogencity- the ability of an immunogen to elicit an immune response. Immunogencity depends upon foreignness to the host, the size of the immunogen, the complexity of its molecular structure, the length of time it remains in the host and its ability to reach certain immuno-competent cells in order to generate immunity.

Keele, JA 24
Immunohistochemistry- immunochemistry applies to the study of cells and tissues. (Now frequently used interchangeably with Immunocytochemistry.) In Situ Hybridization- an assay for nucleic acids “on site” in fixed tissue sections by the use of heat to first denature and then to re-anneal with specific DNA, RNA or PNA probes Internal tissue control-a specimen from the patient donor, which contains the target marker, not only in the tumor to be identified, but also in adjacent normal tissue. Thus, no separate positive control sections are needed Ligand-a molecule, ion or atom that is bound to the central atom (usually a metal atom) of a coordination compound or chelate. Monoclonal Antibodies –immunochemically identical antibodies produced by one clone of plasma cells that react with a specific epitope on a given antigen. Produced commercially using hybridomas Monospecific-having an effect only on a particular kind of cell or tissue, or reacting with a single antigen, as a monospecific antiserum Negative tissue control- a tissue specimen from the same organ lacking the target antigen and processed by use of the primary antibody. Nonimmune serum- serum obtained from animals that have not been immunized. Polyclonal antibodies- immunochemically dissimilar antibodies produced by different cells and reacting with various epitopes on a given antigen. Positive tissue control- a specimen previously shown to stain specifically for the target antigen after exposure to primary antibody. Nonspecific background staining should be at a minimum. Note that, for some target antigens (e.g., prostate specific antigen), the staining intensity ideally should be less than maximal to allow monitoring not only for positivity, but also for variation in intensity. Primary antibody- the first antibody used in a staining procedure. Quenching- refers to the inactivation of a chemical activity by an excess of reactants or products. In enzymology, excess substrate or product may inhibit the enzymatic activity. Secondary antibody- the second antibody used in a staining procedure; it reacts with the primary antibody, now the antigen, and forms a bridge between the primary antibody and a subsequent reagent, if any. Also known as “link” antibody. Specific staining- positive staining of tissue or cells by use of primary antiserum. Occasionally this includes diffused, absorbed or phagocytosed antigen, giving rise

Keele, JA 25
to “undesirable” staining. The staining seen due to contaminating antibodies in the primary antiserum should be considered as nonspecific. Standardization- classically, to standardize means to compare with or conform an assay of unknowns to established standards. In quantitative analytical work numbers readily allow for conforming to such standards. In semi-quantitative or qualitative assays such as immunocyto- or immunohistochemistry, which frequently conclude with an opinion, only subjective comparisons to carefully selected tissue and reagent controls can be used to monitor and maintain excellence Titter-in immunohistochemistry, the highest dilution of an antiserum which results in optimal specific staining with the least amount of background.

Keele, JA 26
References (1) Boenisch, T. (2001) Immunochemical staining methods, 3 ed., DAKO
Corporation, Carpinteria, CA.
(2) Matkowskyj, K. S., D, and Benya, R. (2000) Quantitative immunohistochemistry
by measuring cumulative signal strenght using commercially available software
photoshop and Matlab. The Journal of Histochemistry and Cytochemistry 48, 303-
311.
(3) Javois, L. Immunocytochemical methods and protocols, Vol. 115.


















