
Immediate Loading of Single Implants: A Two-Year...
10
Volume 37, Number 1, 2017 69 ©2017 by Quintessence Publishing Co Inc. 1 Professor, Department of Dental Sciences, University Vita Salute San Raffaele, Milan, Italy. 2 Professor, Department of Periodontology and Oral Implantology, University of Ghent, Ghent, Belgium. 3 Private Practice, Bologna, Italy. 4 Private Practice, Grumo Nevano (Naples), Italy. 5 Private Practice, Naples, Italy. 6 Professor, Department of Oral and Maxillofacial Surgery, Dental School, University of Naples, Naples, Italy. 7 Lecturer, Department of Surgical and Morphological Science, Dental School, University of Varese, Varese, Italy. Correspondence to: Dr Francesco Mangano, Department of Surgical and Morphological Science, Dental School, University of Varese, via G Piatti 10, 21100 Varese, Italy. Fax. +39-0344-530251. Email: [email protected] Immediate Loading of Single Implants: A Two-Year Prospective Multicenter Study The aim of this prospective multicenter study was to evaluate the outcomes of single implants subjected to immediate functional loading. Inclusion criteria were single-tooth placement in postextraction sockets or fully healed sites, and sufficient bone height and width to place an implant of at least 3.5 × 10.0 mm. All implants were functionally loaded immediately after placement and followed for 2 years. Outcome measures were implant survival, complications, and peri- implant marginal bone loss (MBL). A total of 57 implants (38 maxilla, 19 mandible) were placed in 46 patients (23 men, 23 women, aged 18–73 years). Of these, 10 implants were placed in postextraction sockets. One implant failed, in a healed site, giving a patient-based overall 2-year survival rate of 97.6%. The incidence of biologic complications was 1.8%; prosthetic complications amounted to 7.5%. The peri-implant MBL was 0.37 ± 0.22 mm (healed sites: 0.4 mm ± 0.22; post- extraction sockets: 0.3 mm ± 0.22). The immediate functional loading of single implants seems to represent a safe and successful procedure. Long-term follow- up studies on a larger sample of patients are needed to confirm these results. Int J Periodontics Restorative Dent 2017;37:69–78. doi: 10.11607/prd.2986 Dental implants are a proven solu- tion for the rehabilitation of partial and total edentulism, and the sur- vival of fixed implant-supported res- torations is now very high. 1–3 For this reason, more patients are asking to be rehabilitated with implants. Im- plants represent a successful solu- tion even in single-tooth gaps, as demonstrated by a large number of studies 3,4 and systematic reviews. 5,6 In recent years, implantology has increasingly advocated the con- cept of immediate loading, even in the case of rehabilitation with single implants. 6,7 Immediate load- ing is defined as the placement of a prosthetic restoration within 48 to 72 hours of implant placement. 6,7 Among the advantages of immedi- ate loading is an overall reduction of treatment times, with functional, cosmetic, and psychologic benefits for the patient. 6-8 With this proce- dure, the fixed prosthetic restora- tion can be positioned in occlusion (immediate functional loading) 8 or it can be drained by the occlusion (immediate nonfunctional restora- tion). 9,10 The difference between these two procedures is the force ideally exerted on the implant by the fixed prosthetic restoration po- sitioned on it. 10 This is not a trivial matter. On one hand, immediate loading is greatly successful in com- plex rehabilitations that provide for the placement of numerous Carlo Mangano, MD, DDS 1 /Filiep Raes, MD, DDS 2 Carolina Lenzi, DDS 3 /Tammaro Eccellente, MD, DDS 4 Michele Ortolani, MD, DDS 5 /Giuseppe Luongo, MD, DDS 6 Francesco Mangano, DDS 7
Transcript of Immediate Loading of Single Implants: A Two-Year...

Volume 37, Number 1, 2017
69
©2017 by Quintessence Publishing Co Inc.
1 Professor, Department of Dental Sciences, University Vita Salute San Raffaele, Milan, Italy. 2 Professor, Department of Periodontology and Oral Implantology, University of Ghent, Ghent, Belgium.
3 Private Practice, Bologna, Italy.4 Private Practice, Grumo Nevano (Naples), Italy.5 Private Practice, Naples, Italy.6 Professor, Department of Oral and Maxillofacial Surgery, Dental School, University of Naples, Naples, Italy.
7 Lecturer, Department of Surgical and Morphological Science, Dental School, University of Varese, Varese, Italy. Correspondence to: Dr Francesco Mangano, Department of Surgical and Morphological Science, Dental School, University of Varese, via G Piatti 10, 21100 Varese, Italy. Fax. +39-0344-530251. Email: [email protected]
Immediate Loading of Single Implants: A Two-Year Prospective Multicenter Study
The aim of this prospective multicenter study was to evaluate the outcomes of single implants subjected to immediate functional loading. Inclusion criteria were single-tooth placement in postextraction sockets or fully healed sites, and sufficient bone height and width to place an implant of at least 3.5 × 10.0 mm. All implants were functionally loaded immediately after placement and followed for 2 years. Outcome measures were implant survival, complications, and peri-implant marginal bone loss (MBL). A total of 57 implants (38 maxilla, 19 mandible) were placed in 46 patients (23 men, 23 women, aged 18–73 years). Of these, 10 implants were placed in postextraction sockets. One implant failed, in a healed site, giving a patient-based overall 2-year survival rate of 97.6%. The incidence of biologic complications was 1.8%; prosthetic complications amounted to 7.5%. The peri-implant MBL was 0.37 ± 0.22 mm (healed sites: 0.4 mm ± 0.22; post-extraction sockets: 0.3 mm ± 0.22). The immediate functional loading of single implants seems to represent a safe and successful procedure. Long-term follow-up studies on a larger sample of patients are needed to confirm these results. Int J Periodontics Restorative Dent 2017;37:69–78. doi: 10.11607/prd.2986
Dental implants are a proven solu-tion for the rehabilitation of partial and total edentulism, and the sur-vival of fixed implant-supported res-torations is now very high.1–3 For this reason, more patients are asking to be rehabilitated with implants. Im-plants represent a successful solu-tion even in single-tooth gaps, as demonstrated by a large number of studies3,4 and systematic reviews.5,6
In recent years, implantology has increasingly advocated the con-cept of immediate loading, even in the case of rehabilitation with single implants.6,7 Immediate load-ing is defined as the placement of a prosthetic restoration within 48 to 72 hours of implant placement.6,7 Among the advantages of immedi-ate loading is an overall reduction of treatment times, with functional, cosmetic, and psychologic benefits for the patient.6-8 With this proce-dure, the fixed prosthetic restora-tion can be positioned in occlusion (immediate functional loading)8 or it can be drained by the occlusion (immediate nonfunctional restora-tion).9,10 The difference between these two procedures is the force ideally exerted on the implant by the fixed prosthetic restoration po-sitioned on it.10 This is not a trivial matter. On one hand, immediate loading is greatly successful in com-plex rehabilitations that provide for the placement of numerous
Carlo Mangano, MD, DDS1/Filiep Raes, MD, DDS2
Carolina Lenzi, DDS3/Tammaro Eccellente, MD, DDS4
Michele Ortolani, MD, DDS5/Giuseppe Luongo, MD, DDS6
Francesco Mangano, DDS7

The International Journal of Periodontics & Restorative Dentistry
70
implants splinted between them-selves, as shown by numerous clini-cal studies.8,11,12 On the other hand, there is less evidence in the literature regarding the immediate loading of implant-supported single crowns, especially in the posterior region.13 The transmission of the load on the implant during the healing period and immediately after placement could lead to micromovements at the interface between the bone and the implant, compromising healing and osseointegration.14 Immediate nonfunctional restoration provides for the transmission of a certain amount of loading on the underly-ing implant.9,10 Especially in the pos-terior area, the forces of chewing and those determined by muscula-ture (eg, those transmitted by the tongue in the mandibular arch) will act in some way on the implant even in the absence of specific occlusal contacts.15 However, it is evident that immediate functional loading carries a higher risk, especially in the case of implant-supported single crowns in the posterior area.15
Different surgical protocols are now available for the rehabilita-tion of single-tooth gaps with im-plants.15,16 These include immediate implant treatment (IIT) within 48 hours of extraction of the affected tooth, early implant treatment (EIT) 4 to 8 weeks after extraction, and conventional implant treatment (CIT) performed on complete heal-ing of the surgical site 4 to 6 months after extraction.15,16 Although all of these surgical techniques can en-sure high success and survival rates, immediate implant treatment in the postextraction site may represent an
additional risk factor for implant fail-ure, especially where adequate or satisfactory primary implant stability has not been obtained.16,17 To date, few studies have addressed the topic of immediate functional load-ing with implant-supported single crowns,18–25 and even fewer have ad-dressed the issue of single implants placed in postextraction sockets and immediately loaded.21,22,25 The purpose of this prospective multi-center study with 2 years follow-up was therefore to assess survival, complications, and peri-implant marginal bone loss (MBL) of single implants placed in healed sites and in postextraction sockets and subjected to immediate functional loading.
Materials and methods
Patient selection
This prospective study is based on data from patients treated with im-mediately loaded single implants in six different dental centers, under the same protocol. In the period between February 2012 and Feb-ruary 2013, patients were selected for treatment based on the follow-ing inclusion criteria: patients with single-tooth gaps or with a single, compromised, nonrecoverable den-tal element to be replaced with an implant; enough bone to place an implant of at least 10.0 mm in length and 3.5 mm in diameter; aged ≥ 18 years; good general and oral health; ability to sign an informed con-sent; and willingness to participate in annual checkups. The exclusion
criteria were chronic periodontitis with advanced loss of bone sup-port;26 oral diseases; need for ma-jor regenerative techniques before implant placement (minor proce-dures including covering exposed implant threads with granulate or buccal grafting and interproximal procedures were not exclusion cri-teria); active infections in the tooth to be extracted (eg, pain, pus, fistula); severe impairment/dam-age to one of the four walls of the alveolus following extraction; lack of occlusal contacts in the antago-nist arch; parafunction (ie, bruxism/clenching); uncontrolled diabetes; immunocompromised states; che-motherapy; radiotherapy; treatment with intravenous amino-bisphos-phonates; psychiatric disorders; and abuse of drugs/alcohol. The diagno-sis of parafunction was made as a result of careful anamnesis, physical examination, and electromyography of the masticatory muscles.27 Smok-ing was not considered an exclusion criterion for this study; however, patients enrolled in the study were informed in detail about the risks associated with cigarette smoking, which in several studies has been identified as a risk factor for implant failure.28 All patients were informed in detail about the planned therapy and the related risks and signed an informed consent to treatment. This study was conducted in compliance with the principles set out in the Declaration of Helsinki for clinical research on humans in 1975 (revi-sion of 2000) and was approved by the Local Ethical Committee of the Hospital of Varese (protocol number 0034086).

Volume 37, Number 1, 2017
71
Dental implants
The implants inserted in this study (AnyRidge, Megagen) were char-acterized by a tapered design with self-cutting threads (KnifeThread, Megagen).21 These implants pos-sessed an internal hexagon and a 5-mm-deep conical connection (10 degrees) with built-in platform switching. These implants had a nanostructured calcium-incorporat-ed surface (Xpeed, Megagen)29 and were available in different lengths (10.0, 11.5, and 13.0 mm) and diam-eters (3.5, 4.0, and 4.5 mm).
Case study and planning
Patients were subjected to periapi-cal and panoramic radiographs for preliminary study of the residual bone anatomy and to assess the compromised element to be ex-tracted. Where needed, the sur-geon could request a cone beam computed tomography (CBCT) scan for three-dimensional (3D) as-sessment of the surgical site. The files obtained through CBCT were imported into 3D software for re-construction of the crest and evalu-ation of every anatomical detail. The preliminary examinations were completed with generic impressions and development of stone casts for diagnostic wax-up.
Surgical and prosthetic procedures
Two days before surgery, patients were asked to rinse two to three
times daily with chlorhexidine 0.12% mouthrinse for a total time of 1 min-ute. The same procedure was re-peated 15 minutes before surgery. The surgery was performed under local anesthesia obtained by infiltra-tion with articaine with adrenaline 1:100,000. In the case of single-tooth–gap patients, the surgical pro-cedure involved the execution of a crestal incision possibly connected to two short incisions of vestibular relaxation. The mucoperiosteal flap was raised, and the surgeon pro-ceeded with the osteotomy, starting with a 2.0-mm-diameter pilot drill, to the desired depth. The bone quality of the residual crest was assessed ac-cording to the clinician’s judgment4 and the implant site was prepared accordingly. The surgeon then posi-tioned the implant of chosen length and diameter at crestal level. The stability of the implants was deter-mined clinically as the absence of axial or rotational movement by the removal of the implant driver, with-out use of the stabilizing wrench. In patients with severely compromised dental elements, which called for extraction and immediate implant treatment, the procedure was per-formed with the flapless approach. The tooth was gently extracted, with care taken not to damage the re-maining socket walls, particularly the buccal wall (the compromise of even one socket wall excluded patients from this study). The postextraction alveolus was curetted to remove any remaining granulation tissue. The integrity of the residual walls of the alveolus was verified, and the proce-dure continued with the preparation of the implant site.
Again, drill selection was based on the bone quality of the receiv-ing site. The implants were placed in prepared osteotomies, apically pushed 3 to 4 mm to the peak of the postextraction socket. In cases with high esthetic needs, particular atten-tion was paid to placing the implant palatally and avoiding contact with the buccal wall of the alveolus. The implants were manually placed in a slightly subcrestal position, using a hand ratchet. This gave a rough estimate of the maximum insertion torque obtained, after which any spaces between the buccal bone wall and the implant body were filled with hydroxyapatite/beta-tricalcium phosphates granules.
Immediately after implant place-ment, a prefabricated titanium abut-ment was prepared and screwed onto the implant. Temporary resin crowns were adapted from pre-formed shells or obtained from the laboratory; in both cases, they were relined with light-curing flow-able resin. The provisional crowns were finished and polished meticu-lously to obtain the desired emer-gence profiles. In the healed ridge group, the flap was adapted to the emergence profile and sutured; in the extraction sockets group, the temporary restorations sealed the socket and maintained clot forma-tion subgingivally. The provisional restorations were screw retained; each had a hole in the occlusal sur-face, which was closed with compos-ite resin. A careful check of occlusion was conducted using articulating papers. Distributed occlusal con-tacts were obtained, and in all cases articulating papers were firmly held

The International Journal of Periodontics & Restorative Dentistry
72
by the occluding teeth. An intraoral periapical radiograph was taken.
Ice packs were provided and analgesics were prescribed (100 mg nimesulide every 12 hours for 2 days). Patients were prescribed antibiotics (amoxicillin + clavulanic acid, 2 g per day for 6 days) and asked to avoid hard foods, at least in the first weeks after implant placement. All patients were recalled at 10 days, for a control and for removal of sutures, where present. After 3 months, the provi-sional restorations were replaced with the final metal-ceramic or zir-conia-ceramic crowns; these were screwed or cemented, depending on the choice of the prosthodontist. Occlusion was carefully checked and an intraoral periapical radiograph was taken to check final restoration seating. Patients were thereafter enrolled in a maintenance program with professional oral hygiene ses-sions every 6 months.
Outcome variables
The following outcome variables were analyzed at the time of implant insertion and provisionalization (T0), at delivery of the final restoration (3 months after implant insertion, T1) and after 1 (T2) and 2 years (T3) of functional loading:
• Implant survival. The stability of individual implants was checked at delivery of final crowns by applying a reverse torque of 20 Ncm2 with a dedicated wrench. Implant stability was checked again after 2 years of loading.
• Complications. Pain/swelling after surgery, peri-implant mucositis, and peri-implantitis were enlisted as biologic complications; abutment screw loosening/fracture and ceramic/veneer fractures were enlisted as prosthetic complications.
• Peri-implant MBL.21 Intraoral periapical radiographs were taken at different times (T0, T1, T2, and T3) for each implant, using a Rinn alignment system with a rigid film-object X-ray source coupled to a beam-aiming device to achieve reproducible exposure geometry. Customized film holders were fabricated, with polymerized polyvinyl siloxane on the occlusal surfaces of the adjacent teeth. Mesial and distal marginal bone levels of all implants were measured at different times (T0, T1, T2, and T3); an ocular grid (×4.5 magnification) was used for all measurements. The coronal margin of the implant neck and the most coronal bone-to-implant contact point were used as references for the linear measurements. To account for variability, the implant length was measured and compared with the documentation dimensions. Ratios were calculated to adjust for distortion. At the end, peri-implant MBL was calculated as modification in the peri-implant marginal bone level at different times on the mesial and distal implant sides. The average
mesial and distal calculations were averaged to obtain the final value.
Statistical evaluation
Data were collected and analyzed by two independent, experienced observers who were not part of the treating team. All data were entered into a specific statistical sheet, where the analysis was con-ducted. Descriptive statistics were used for the evaluation of patient demographics (sex, age, smoking habit) and implant characteristics/features (site, position, length, di-ameter, bone quality at the recipient site). Absolute and relative frequen-cy distributions were calculated for qualitative variables, means, stan-dard deviations, and medians, and 95% confidence intervals (CI) were estimated for quantitative variables such as peri-implant MBL. Implant survival was calculated at the patient and implant levels; peri-implant MBL was calculated at the patient level.
Results
A total of 46 patients (23 men and 23 women; aged 18–73 years, mean age: 44.5 years) were eligible for the present study. The sex, age, and smoking habits of the enrolled pa-tients, with related survival rates, are reported in Table 1. The site, posi-tion, length, and diameter of the placed implants, together with the quality of the recipient sites and the related survival rates, are reported in Table 2. A total of 47 implants
Volume 37, Number 1, 2017
73
(82.5%) were placed in healed sites, while 10 (17.5%) were placed in fresh extraction sockets. The reasons for extraction of the teeth substituted with immediate implants were root fracture (7 cases; 70%), endodontic failure (2 cases; 20%), and extensive tooth decay (1 case; 10%).
Most of the immediate implants (8/10; 80%) were installed in the anterior maxilla. No buccal bone damage occurred in this group, so no patients were excluded for this. No major augmentation procedures were needed, but minor augmenta-tion to cover exposed threads and/or interproximal/buccal grafting owing to hard tissue deficiency was performed after installation of 15 implants (26.3%).
The final restorations were screwed or cemented metal-ceramic (52 cases; 91.2%) or zirconia-ceramic (5 cases; 8.8%) single crowns. A total of 4 patients (4 implants) withdrew from the study and were conse-quently classified as dropouts, even if their implants were still in function.
At the 2-year follow-up, one im-plant was lost, in the posterior max-illa (second premolar, healed site) of a 48-year-old woman with a smok-ing habit. The failed implant (3.5- mm diameter × 10.0-mm length) was installed in type 3 bone. This implant showed mobility and lack of osseointegration 2 months after surgery and was removed; all the other implants were stable, giving a patient-based 2-year overall survival rate of 97.6% (Figs 1 and 2).
With regard to biologic com-plications, one patient experienced pain and swelling after surgery. This was managed by prescribing an-
algesic medication, and no further complications were reported for this implant.
At the end of the study, the in-cidence of biologic complications was 1.8%. Prosthetic complications
Table 1 Patient Distribution By Sex, Age, and Smoking Habit, as Related to Patient-Based Survival Rate
Patients (n [%])
Dropouts (n)
Failures (n)
Survival rate (2 y) (%)
Sex Men Women
23 (50)23 (50)
31
01
10095.4
Age (y) 16–25 26–35 36–45 46–55 56–65 > 65
7 (15.2)6 (13.0)7 (15.2)
13 (28.2)9 (19.5)4 (8.7)
011011
000100
10010010092.3
100100
Smoking habit Smokers Nonsmokers
17 (37.0)29 (63.0)
13
10
93.7100
Overall All patients 46 (100) 4 1 97.6
Table 2 Distribution of Implants by Site, Position, Length, Diameter, and Bone Type, with Related Survival Rate
Implants (n [%])
Dropouts (n)
Failures (n)
Survival rate (2 y) (%)
Site Maxilla Mandible
38 (66.7)19 (33.3))
22
10
97.2100
Position Incisors Canines Premolars Molars
9 (15.8)3 (5.2)
31 (54.4)14 (24.6)
0022
0010
10010096.5
100
Length (mm) 10 11.5 13
30 (52.7)21 (36.8)6 (10.5)
121
100
96.5100100
Diameter (mm) 3.5 4.0 4.5
25 (43.9)21 (36.8)11 (19.3)
121
100
95.8100100
Bone quality Type 2 Type 3 Type 4
18 (31.6)31 (54.4)8 (14.0)
121
010
10096.5
100
Overall All implants 57 (100) 4 1 98.1

The International Journal of Periodontics & Restorative Dentistry
74
amounted to 7.5%. Three patients had their abutments loosened, two in the posterior mandible and one in the anterior maxilla. All these abut-ments were inserted and screwed in again; however, these mechani-cal complications were recorded as prosthetic complications. In addi-tion, a veneer fracture occurred in a metal-ceramic definitive crown. The damaged restoration was removed, and a new crown was fabricated and provided. Finally, the peri-implant
MBL as calculated at the 1- and 2-year examinations is reported in Table 3.
Discussion
Few studies are available in the lit-erature on immediate functional loading of single implants.18–22,24,25 For the most part, the studies that do exist deal with implants placed in the anterior maxilla,22–25 where
functional loads are reduced. Only a few studies examine the imme-diate loading of implants placed in postextraction sockets.21,22,25 A recent randomized controlled trial compared the survival and suc-cess rates of single implants in im-mediate functional loading placed with the flapless method with those of delayed loading implants positioned after raising a surgi-cal flap.18 At the end of this study, the immediate functional loading
Fig 1 Immediate implant placement in the anterior maxilla (right canine). (a) Extraction of the nonrecoverable root. (b) Placement of the implant in the fresh postextraction socket. (c) The implant in position with the provisional abutment 24 hours after surgery. (d) The provisional restoration positioned within 48 hours of implant placement. (e) At 3 months after implant placement, the final metal-ceramic crown was delivered. (f) Radiographic control at the delivery of the final metal-ceramic crown. (g) Clinical control at 2 years. (h) Radiographic control at 2 years.
a b c
e fd
g h
Volume 37, Number 1, 2017
75
had not compromised the survival and success rates of the implants.18 These results were confirmed by a subsequent clinical trial with 4 years of follow-up, where flapless place-ment of single implants with imme-diate functional loading determined high survival and success rates in the posterior areas of the maxilla and mandible.19 In a prospective study on the immediate functional load-ing of 40 implant-supported single crowns in the posterior mandible of
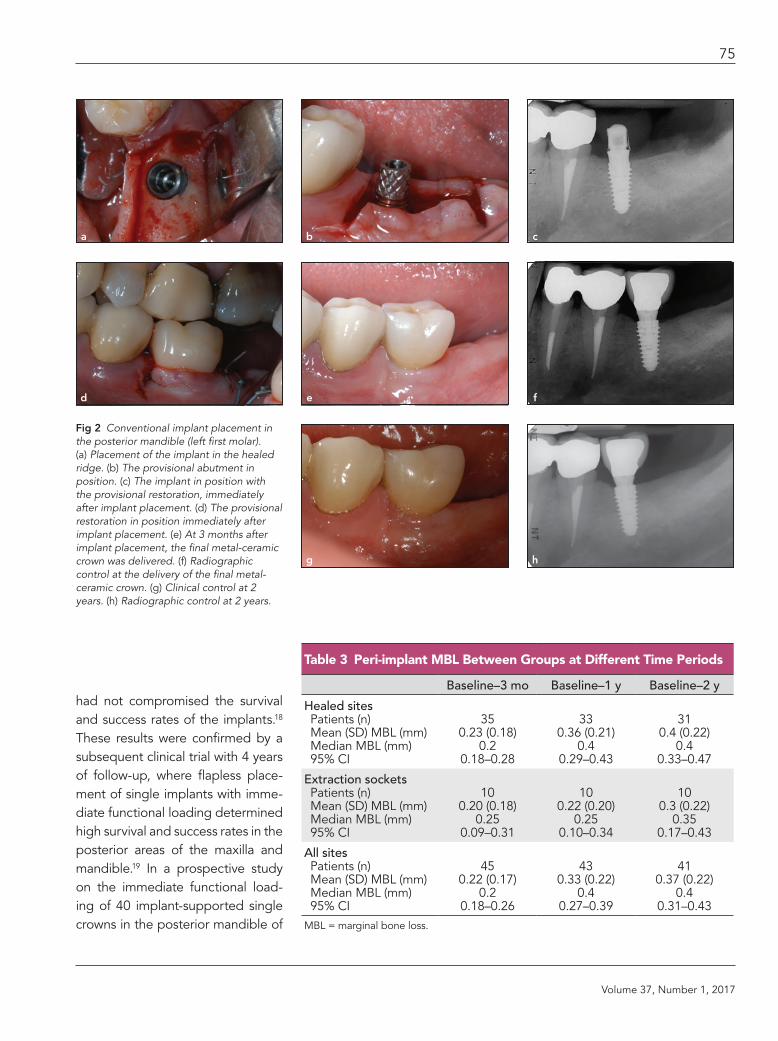
Fig 2 Conventional implant placement in the posterior mandible (left first molar). (a) Placement of the implant in the healed ridge. (b) The provisional abutment in position. (c) The implant in position with the provisional restoration, immediately after implant placement. (d) The provisional restoration in position immediately after implant placement. (e) At 3 months after implant placement, the final metal-ceramic crown was delivered. (f) Radiographic control at the delivery of the final metal-ceramic crown. (g) Clinical control at 2 years. (h) Radiographic control at 2 years.
Table 3 Peri-implant MBL Between Groups at Different Time Periods
Baseline–3 mo Baseline–1 y Baseline–2 y
Healed sites Patients (n) Mean (SD) MBL (mm) Median MBL (mm) 95% CI
350.23 (0.18)
0.20.18–0.28
330.36 (0.21)
0.40.29–0.43
310.4 (0.22)
0.40.33–0.47
Extraction sockets Patients (n) Mean (SD) MBL (mm) Median MBL (mm) 95% CI
100.20 (0.18)
0.250.09–0.31
100.22 (0.20)
0.250.10–0.34
100.3 (0.22)
0.350.17–0.43
All sites Patients (n) Mean (SD) MBL (mm) Median MBL (mm) 95% CI
450.22 (0.17)
0.20.18–0.26
430.33 (0.22)
0.40.27–0.39
410.37 (0.22)
0.40.31–0.43
MBL = marginal bone loss.
a b c
e fd
g h

The International Journal of Periodontics & Restorative Dentistry
76
33 patients with follow-up after 5 years, the cumulative success rate reported was 95% with only 2 im-plant failures.20
Excellent results have been re-ported following the placement of single implants with immediate load-ing in the anterior maxilla.22,24,25 In a study involving 70 patients treated with single implants placed in healed sites (45 implants) and in postextrac-tion sockets (25 implants), 1 year after loading all implants were suc-cessfully osseointegrated.22 Similar excellent results were reported in a clinical study where the placement of single implants subjected to im-mediate functional loading in es-thetic areas had a survival rate of 96.1% at 3 years and minimal peri-implant marginal bone loss.24 This is in agreement with what was re-ported in a previous meta-analysis of the literature relating to single implants positioned in the anterior maxilla, where no significant differ-ences were found in the survival of implants subjected to different load conditions.23
A recent clinical study with fol-low-up at 5 years finally compared the peri-implant MBL of single im-plants placed in healed sites and postextraction sockets of the ante-rior maxilla.25 In this study, the mean MBL after implant placement was 0.26 ± 0.161 mm for 1 year, 0.26 ± 0.171 mm for 3 years, and 0.21 ± 0.185 mm for 5 years in extraction sockets and 0.26 ± 0.176 mm for 1 year, 0.21 ± 0.175 mm for 3 years, and 0.19 ± 0.172 mm for 5 years in the healed ridges group.25 Loss of mar-ginal bone was more pronounced in implants inserted in healed ridges
(P < .041) compared with fresh surgi-cal extraction sockets (P < .540).25
All these results seem to be in agreement with those of the pres-ent study with follow-up at 2 years, where 57 single implants were placed in 46 patients and subjected to immediate functional loading. At the end of the study, only one im-plant was lost, in a healed site, for an overall survival rate of 97.6%. All other implants were in function, with a very low incidence of biologic complications (1.8%); the incidence of prosthetic complications was slightly higher (7.5%). After 2 years of functional loading, the overall peri-implant MBL was 0.37 ± 0.22 mm. In the healed site group, a 2-year MBL of 0.4 ± 0.22 mm was reported, while in postextraction sockets the 2-year MBL amounted to 0.3 ± 0.22 mm. These results seem to suggest that there are no differences in the sur-vival and success rates of immedi-ately loaded single implants placed in healed sites and postextraction sites; however, it must be pointed out that in the present study only 10 implants were placed in postextrac-tion sites.
In procedures with immedi-ate functional loading, success es-sentially depends on the degree of primary implant stabilization, the presence of controlled load condi-tions, and the macro and micro-topographic characteristics of the implant.5–7,10,17,21 Primary stability, defined as the biometric stability achieved immediately after implant insertion by the mechanical locking of the implant to the bone,17 is es-sential. Adequate primary stabiliza-tion of the implant depends on the
surgical protocol used, the experi-ence and skill of the surgeon, the density of the receiving bone site, and the shape and surface of the im-plant.17 A good trick for maximizing primary stability is to underprepare the surgical site. This particularly ap-plies in the case of postextraction sockets, where stabilization is often achieved through an apical fixation of a few millimeters.15–17,21 Use of an aggressive implant with a certain degree of taper may help to obtain a valid primary stabilization.21 In the present study, a strict surgical proto-col was followed in which implants were placed in underprepared osteotomies, particularly in cases where bone quality was poor (types 3 and 4 bone) and in fresh extrac-tion sockets. Moreover, the macro-topographic features of the implant used in this study were designed to provide high insertion torque, with threads of increasing dimension to-ward the coronal end of the implant. This feature may allow for axial and radial bone compression during implant insertion, providing an in-creased primary stability that is use-ful in immediate functional loading, particularly in areas of poor bone quality.21 The receiving bone site is fundamental: primary stabilization is simpler in the anterior areas, where the bone density is higher, and more difficult in the posterior areas, par-ticularly in the posterior maxilla.4,30 In the posterior maxilla, a single implant is more difficult to stabilize and therefore more susceptible to failure in the event of immediate functional loading.5,7,13,16,30 In fact, certain micromovements, beyond a critical threshold, can lead to fibrous

Volume 37, Number 1, 2017
77
encapsulation of the implant, and subsequent failure.5,7,14–17,21 In the present study, most of the implants (26; 45.7%) were placed in the pos-terior maxilla; however, only one fail-ure was reported.
Last but not least, in procedures with immediate functional loading, it is of fundamental importance to use implants with specific microtopog-raphy and surface characteristics capable of stimulating the apposi-tion of new bone and promoting and accelerating healing.5,7,14–17,21,23–30 In the present study, implants with a novel nanostructured calcium-incorporated surface, which is highly osteoconductive21,29 and may pro-mote bone healing, were used. This peculiar microtopographic feature, combined with an implant body de-signed for critical bone conditions and high insertion torques, may have minimized the risk of failure as-sociated with immediate functional loading.
Conclusions
This prospective clinical study with follow-up at 2 years seems to vali-date the hypothesis that immedi-ate functional loading of single implants could represent a safe and effective procedure, character-ized by high survival rates (97.6%), low incidence of biologic compli-cations, and rather limited peri-implant MBL (0.37 ± 0.22 mm). Complications of a prosthetic na-ture occurred at a slightly higher incidence (7.5%). This study has limitations, such as the small num-ber of patients treated and the low
number of implants inserted; fur-ther studies are needed to confirm the results obtained here.
Acknowledgments
The authors reported no conflicts of interest relating to the preparation of this scientific work.
References
1. Mangano C, Iaculli F, Piattelli A, Man-gano F. Fixed restorations supported by Morse-taper connection implants: A retrospective clinical study with 10–20 years of follow-up. Clin Oral Implants Res 2015;26:1229–1236.
2. Kwon T, Bain PA, Levin L. Systematic re-view of short- (5–10 years) and long-term (10 years or more) survival and success of full-arch fixed dental hybrid prosthe-ses and supporting implants. J Dent 2014;42:1228–1241.
3. Mangano F, Macchi A, Caprioglio A, Sammons RL, Piattelli A, Mangano C. Survival and complication rates of fixed restorations supported by locking-taper implants: A prospective study with 1 to 10 years of follow-up. J Prosthodont 2014;23:434–444.
4. Mangano FG, Shibli JA, Sammons RL, Iaculli F, Piattelli A, Mangano C. Short (8-mm) locking-taper implants support-ing single crowns in posterior region: A prospective clinical study with 1-to 10-years of follow-up. Clin Oral Implants Res 2014;25:933–940.
5. Jung RE, Zembic A, Pjetursson BE, Zwahlen M, Thoma DS. Systematic review of the survival rate and the in-cidence of biological, technical, and aes-thetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin Oral Implants Res 2012;23(suppl 6):2–21.
6. Moraschini V, Porto Barboza E. Immedi-ate versus conventional loaded single implants in the posterior mandible: A meta-analysis of randomized controlled trials. Int J Oral Maxillofac Surg 2016; 45:85–92.
7. Ghoul WE, Chidiac JJ. Prosthetic re-quirements for immediate implant load-ing: A review. J Prosthodont 2012;21: 141–154.
8. Boedeker D, Dyer J, Kraut R. Clinical out-come of immediately loaded maxillary implants: A 2-year retrospective study. J Oral Maxillofac Surg 2011;69:1335–1343.
9. Hartlev J, Kohberg P, Ahlmann S, et al. Immediate placement and provisional-ization of single-tooth implants involv-ing a definitive individual abutment: A clinical and radiographic retrospective study. Clin Oral Implants Res 2013;24: 652–658.
10. Takeshita K, Vandeweghe S, Vervack V, Sumi T, De Bruyn H, Jimbo R. immediate implant placement and loading of single implants in the esthetic zone: Clinical outcome and esthetic evaluation in a Japanese population. Int J Periodontics Restorative Dent 2015;35:715–723.
11. Melo AC, Toscano R, Vieira RA, Sartori IA, Bernardes SR, Thomé G. immediate loading of edentulous mandible with prefabricated bars: A long-term study of 7 years. Implant Dent 2015;24:472–476.
12. Crespi R, Capparè P, Gastaldi G, Gher-lone EF. Immediate occlusal loading of full-arch rehabilitations: Screw-retained versus cement-retained prosthesis. An 8-year clinical evaluation. Int J Oral Max-illofac Implants 2014;29:1406–1411.
13. Guidetti LG, Monnazzi MS, Piveta AC, Gabrielli MA, Gabrielli MF, Pereira Filho VA. Evaluation of single implants placed in the posterior mandibular area un-der immediate loading: A prospective study. Int J Oral Maxillofac Surg 2015;44: 1411–1415.
14. Branemark PI, Hansson BO, Adell R, et al. Osseointegrated implants in the treatment of the edentulous jaws. Ex-perience from a 10-year period. Scand J Plast Reconstr Surg Suppl 1977;16:1–132.
15. Benic GI, Mir-Mari J, Hämmerle CH. Loading protocols for single-implant crowns: A systematic review and meta-analysis. Int J Oral Maxillofac Implants 2014;29(suppl):222–238.
16. Chrcanovic BR, Albrektsson T, Wenner-berg A. Dental implants inserted in fresh extraction sockets versus healed sites: A systematic review and meta-analysis. J Dent 2015;43:16–41.
17. Lioubavina-Hack N, Lang NP, Karring T. Significance of primary stability for os-seointegration of dental implants. Clin Oral Implants Res 2006;17:244–250.

The International Journal of Periodontics & Restorative Dentistry
78
18. Cannizzaro G, Leone M, Consolo U, Ferri V, Esposito M. Immediate functional loading of implants placed with flapless surgery versus conventional implants in partially edentulous patients: A 3-year randomized controlled clinical trial. Int J Oral Maxillofac Implants 2008;23: 867–875.
19. Cannizzaro G, Felice P, Leone M, Ferri V, Viola P, Esposito M. Immediate versus early loading of 6.5 mm-long flapless placed single implants: A 4-year after loading report of a split-mouth ran-domised controlled trial. Eur J Oral Im-plantol 2012;5:111–121.
20. Calandriello R, Tomatis M. Immediate occlusal loading of single lower mo-lars using Brånemark System® Wide Platform TiUnite™ implants: a 5-year follow-up report of a prospective clini-cal multicenter study. Clin Implant Dent Related Res 2011;13:311–318.
21. Luongo G, Lenzi C, Raes F, Eccellente T, Ortolani M, Mangano C. Immediate functional loading of single implants: A 1-year interim report of a 5-year pro-spective multicentre study. Eur J Oral Implantol 2014;7:187–199.
22. Di Alberti L, Donnini F, di Alberti C, Camerino M, Sgaramella N, Lo Muzio L. Clinical and radiologic evaluation of 70 immediately loaded single implants in the maxillary esthetic zone: Preliminary results after 1 year of functional load-ing. Int J Oral Maxillofac Implants 2012; 27:181–186.
23. den Hartog L, Slater JJ, Vissink A, Meijer HJ, Raghoebar GM. Treatment outcome of immediate, early and conventional sin-gle-tooth implants in the aesthetic zone: A systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. J Clin Periodontol 2008;35: 1073–1086.
24. Guarnieri R, Grande M, Ippoliti S, Iorio-Siciliano V, Riccitiello F, Farronato D. Influence of a Laser-Lok Surface on Im-mediate Functional Loading of Implants in Single-Tooth Replacement: Three-Year Results of a Prospective Randomized Clinical Study on Soft Tissue Response and Esthetics. Int J Periodontics Restor-ative Dent 2015;35:865–875.
25. Berberi AN, Sabbagh JM, Aboush-elib MN, Noujeim ZF, Salameh ZA. A 5-year comparison of marginal bone level following immediate loading of single-tooth implants placed in healed alveolar ridges and extraction sockets in the maxilla. Front Physiol 2014;31:29.
26. American Academy of Periodontology. Parameters on chronic periodontitis with advanced loss of periodontal support. J Periodontol 2000;71(suppl 5):856–858.
27. Reddy SW, Kumer MP, Sravanthi D, Mohsin AH, Anuhya V. Bruxism: A lit-erature review. J Int Oral Health 2014;6: 105–109.
28. Moraschini V, Barboza ED. Success of dental implants in smokers and non-smokers: a systematic review and meta-analysis [epub ahead of print 15 Sept 2015]. Int J Oral Maxillofac Surg pii: S0901-5027(15)01308-9. doi: 10.1016/j.ijom.2015.08.996.
29. Lee SY, Yang DJ, Yeo S, An HW, Ryoo KH, Park KB. The cytocompatibility and osseointegration of the Ti implants with Xpeed surfaces. Clin Oral Implants Res 2012;23:1283–1289.
30. Javed F, Almas K, Crespi R, Romanos GE. Implant surface morphology and primary stability: Is there a connection? Implant Dent 2011;20:40–46.


















