Approach to Hepatomegaly, Splenomegaly and Hepatosplenomegaly

Imaging of liver and pancreas
. .

•
•
•

Disease of the liver
• Focal liver disease
• Diffusion liver disease

Focal liver disease
Benign
• Cyst
• Abscess
• Hemangioma
• FNH
• Hepatic adenoma
Malignant
• HCC
• Fibrolamellar
carcinoma
• Metastasis
• Cholangiocarcinoma

Diffuse liver disease
• Cirrhosis
• Metabolic disease
– Hemochromatosis
– Wilson’s disease
– Fatty liver

Anatomy of liver



Hemodynamic
• Blood supply
– Portal vein (70%)
– Hepatic artery (30%)
– Hepatic vein

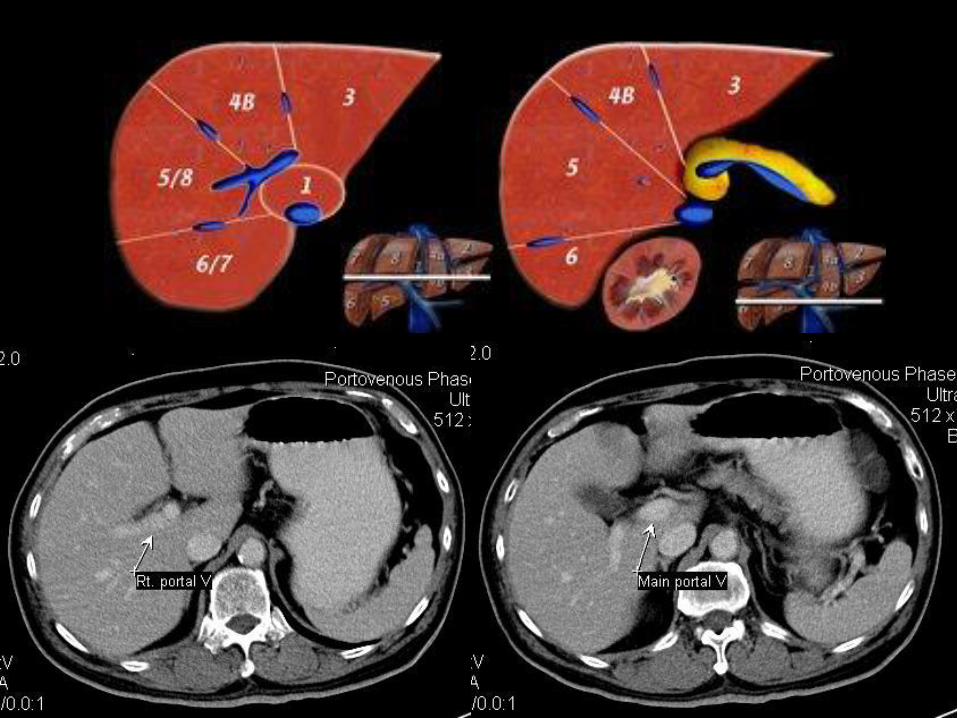
Anatomy of the liver
• Morphological anatomy – 3 lobes
– Right lobe
– Left lobe
– Caudate lobe
• Functional anatomy – 8 segments
– Base on portal and hepatic vein supply


Morphological anatomy
Division between:
• Right lobe and left lobe: Middle hepatic
vein
• Left lobe and caudate lobe: Ligamentum venosum


Caudate lobe

Morphological anatomy

Imaging modality
• Plain film: not useful
• Ultrasound: good screening test, non-
invasive, cheap
• CT: good modality
• MRI: the best at present

Plain film

Ultrasound
Pro:
• Non-invasive method
• Good screening tool
• Not expensive
• Widely available
Con:
• Operator dependent
• Less specificity than CT and MRI


Hemangioma

CT
Pro:
• Good for lesion detection and characterization
• Widely available in most hospital
Con:
• Radiation hazard
• Risk of contrast allergy
• Risk in patient with renal insufficiency

Contrast enhanced CT
• Arterial phase (25-30 sec)
• Portovenous phase (70 sec)
• Delay phase (10-20 min)
• Iodinated or non-iodinated contrast 100-150 cc (6%) rate 2-3 cc/sec
“Multiphasic CT scan”

Blood supply of the liver
• Blood supply
– Portal vein (70%)
– Hepatic artery (30%)
– Hepatic vein

Extracellular contrast agent

Non contrast Arterial phase20-25 sec
Portovenous phase70 sec

Arterial phase
• Scan at 25-30 sec. after injection
• Clearly seen hepatic artery
• Minimal hepatic parenchymal enhancement
Benefit:
• Good for hypervascular tumor detection
• Transient hepatic attenuation difference (THAD)

Arterial phase Portovenous phase
Non-contrast
Hypervascular tumor

No contrast
Arterial phase Portovenous phase

THAD
Arterial phase Portovenous phase

Portovenous phase
• Scan at 70 sec after injection
• Clearly seen hepatic vein and portal vein
• Enhancement of hepatic parenchyma
Benefit: Good for
• Hypovascular tumor
• Biliary tract dilatation
• Hepatic injury

Non contrast
Arterial phase Portovenous phase

THAD
Arterial phase Portovenous phase

Biliary tract dilatation

Portovenous phase
Pitfall:
• 35% miss HCC
• 14% miss hypervascular metastasis (breast,
melanoma, choriocarcinoma, pancreatic islet cell tumor, GIST, etc)

Delay scan (equilibrium phase)
• Scan at 10-20 min after injection
Benefit:
For confirmation of
• Hemangioma
• Intrahepatic cholangiocarcinoma

MRIPro:
• Good for lesion detection and characterization (better than CT)
• No radiation hazard
• No risk for contrast allergy and in patient with renal insufficiency
Con:
• Expensive
• Not widely available
• Cannot perform in patient with metal in body

Liver cyst
Ultrasound
• Anechoic
• Thin wall
• Posterior acoustic enhancement
CT
• Thin wall
• Clear water content

MRI 43219
Benign liver cyst

US, CT: Sharp margin, no internal septation
Clear internal fluid

Liver abscess
Ultrasound
• Irregular wall
• Echogenic content
• May have acoustic enhancement
CT
• Hypodensity collection with irregular peripheral enhancement

Unliquified abscess Liquified abscess

Liver abscess

Non-contrast Arterial phase
Portovenous phase
66M RUQ pain, fever withChill and weight loss
Liver abscess
Solid liver mass
• FNH
• Hepatic adenoma
• HCC
• Fibrolamellar carcinoma
• Metastasis
• Cholangiocarcinoma

Hemangioma
2 months follow up

Hemangioma



Pancreatic mass

Pancreatic mass
• CT is investigation of choice
• CT with dual phase and thin section at pancreas
Staging
• Local invasion: adjacent structure and vascular
• Adenopathy
• Metastasis



Investigation of jaundice

Etiology
1. Hemolysis
2. Bilirubin conjugation problem
3. Obstruction of biliary tract

Etiology
1. Hemolysis
• Overproduction of heme
• High indirect bilirubin
• Thalassemia

Etiology
2. Bilirubin conjugation problem
• Hepatitis (viral, bacterial)
• Sepsis
• Liver failure
• Diffuse liver disease

Etiology
3. Biliary tract obstruction
• Stone
• Stricture
• Tumor: cholangiocarcinoma and
pancreatic carcinoma
• Choledochol cyst

Investigation of jaundice
• US is investigation of choice
Follow by
• CT, ERCP, PTC
• Or MRCP

Ultrasound
- NPO 4-6 hrs
- Biliary tract dilatation
- CBD dilatation- Liver disease



CT
Indication
• Further investigation of site and cause of
jaundice.
• Preparation: oral and IV contrast
• NPO 4-6 hrs
• Good in obesity patient






ERCP

ERCP
Indication
• Inconclusive ultrasound finding
Patient preparation
• NPO 4-6 hrs
• Mild sedation
• Prophylatic antibiotic

ERCP
Post procedure care
• Post sedation care
• Look for infection and pancreatitis
Complication
• Acute pancreatitis



Percutaneous transhepatic
Cholangiography (PTC)

PTC
Indication
• High level of biliary obstruction
• Fail ERCP
• Stent placement
Contraindication
• Bleeding disorder
• Biliary tract infection

PTC
Patient preparation
• Clotting study
• Prophylactic antibiotic
• NPO 4-6 hrs
• Sedation

PTC
Post procedure care
• Observe bleeding and infection
Complication
• Hemorrhage
• Septicemia
• Bile leak, bile peritonitis

T-tube cholangiography
Post cholecystectomy
with T-tube placement

MRCP
Indication
Preoperative
• find cause of obstruction
• fail ERCP
Postperative
• Recurrent jaundice
• symptom of pancreatitis

Portal hypertension

Portal hypertension
• Increase portal venous pressure
• Cause: Intrahepatic, extrahepatic
• Intrahepatic: cirrhosis
• Extraheaptic: hepatic vein obstruction
• Physiology: splenomegaly, collateral
circulation

Imaging of portal hypertension
Indication
• Prove portal hypertension
• Find cause
• Find complication: collateral circulation,
splenomegaly




CT
• Same indication and finding as ultrasound
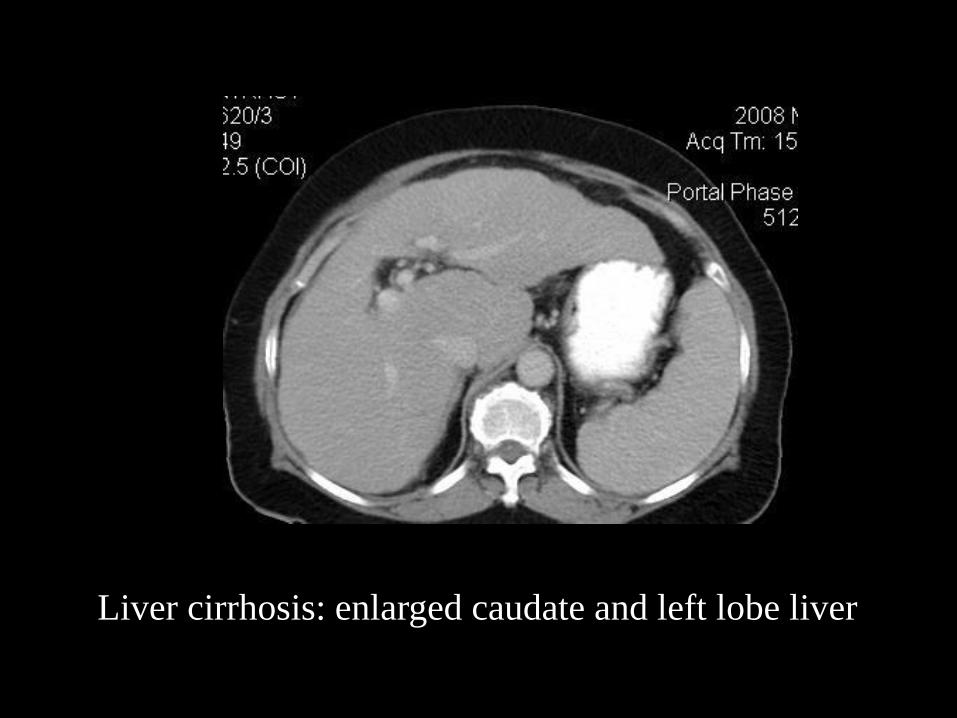
Liver cirrhosis: enlarged caudate and left lobe liver