ILSI EUROPE CONCISE MONOGRAPHS...Food allergy Allergic reaction to a food caused by an...
30
Transcript of ILSI EUROPE CONCISE MONOGRAPHS...Food allergy Allergic reaction to a food caused by an...


ILSI EUROPE CONCISE MONOGRAPHS
This booklet is one in a series of ILSI Europe concisemonographs. The monographs are written for those witha general background in the life sciences. However, thestyle and content of the monographs wifi also appeal to awider audience who seek up-to-date and authoritativereviews on a variety of important topics relating tonutrition, health and food safety.
Concise monographs are based on the proceedingsof a conference or workshop on a topic presented byleading experts. The text of each concise monograph ispeer reviewed by academic scientists of high standing.The concise monographs make important results andconclusions available to a wider audience. The first
published concise monographs are entitled Starches andSugars: A Comparison of Their Metabolism in Man and ASimple Guide to Understanding and Applying the HazardAnalysis Critical Control Point Concept.
Titles of other monographs in preparation include:• Diet and Health in Europe• Food Biotechnology• Efficacy of Caries Preventive Strategies• Dietary Fat and Health• Light Products• Sweetness• Dietary Fibre: Nutritional Function in Health and Disease
INTERNATIONAL LIFE SCIENCES INSTITUTE AND ILSI EUROPE
The International Life Sciences Institute (ILSI) is aworldwide, public, non-profit scientific foundationheadquartered in Washington, DC, USA, with branches inArgentina, Australia, Brazil, Europe, Japan, Mexico, NorthAmerica and Southeast Asia, with a focal point in China.
ILSI is affiliated with the World Health Organizationas a non-governmental organization (NGO) and hasspecialised consultative status with the Food andAgriculture Organization of the United Nations.
ILSI Europe was established in 1986 to provide aneutral forum through which members of industry andexperts from academic, medical and public institutionscan address topics related to health, nutrition and foodsafety throughout Europe in order to advance the
understanding and resolution of scientific issues in theseareas. ILSI Europe is active in the fields of nutrition,toxicology and food microbiology. It sponsors research,conferences, workshops and publications.
For more infonnation about its programmes andactivities, please contact:
ILSI EuropeAvenue F. Mounier 83, Box 6
B-1200 BRUSSELSBelgium
Telephone (32) 2 771-0014Telefax (32) 2 762-0044

FOOD ALLERGY AND OTHER ADVERSE
REACTIONS TO FOOD
by M. H. Lessof
ILSI
InternationalLife SciencesIN5TITUTE
ILSI Europe

Copyright © 1994 by the International Life Sciences Institute
All rights n’served. No part of this publication may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise,without the prior written permission of the copyright holder.
ILSI Press1126 Sixteenth Street, N.W.Washington, D.C. 20036 USATelephone (202) 659-0074Telefax (202) 659-8654
ILSI EuropeAvenue E. Mounier 83, Box 6B-1200 BRUSSELSBelgiumTelephone (32) 2771-0014Telefax (32) 2 762-0044
l’rinted in the United States of America.
ISBN 0-944395-19-7

FOREWORD
Many foods are capable of eliciting allergic or other adversereactions, causing a wide range of symptoms in sensitivesubjects. Recognising the importance of the topic to publichealth, the Group of European Nutritionists chose as thesubject of its 28th Symposium “Food Allergy and FoodIntolerance: Nutritional Aspects and Developments”. ILSIEurope was pleased to make a contribution to the conference,
which took place at Scheveningen, the Netherlands, in June1990, and to collaborate in its organisation. The full conferenceproceedings were published by Karger in 1991 (ISSN 3-8055-5363-3).
This booklet, written by Prof. M. H. Lessof, is based onthat conference, with some additional background materialto help explain the topic to the non-specialist.
Author: M. H. LessofScientific Editor: R. J. J. Hermus
Series Editor: N. Jardine

CONTENTS
Introduction 1
Symptoms and Syndromes Caused by Adverse Reactions to Foods 1
Food Aflergy 3
Non-allergic Reactions to Foods 9
Diagnosis of Adverse Reactions to Foods 11
Allergy to Cows Milk 13
Coeliac Disease 14
Food Additives: Are They an Important Cause of Adverse Reactions to Foods7 16
Living with Adverse Reactions to Foods 18
Summary 20
Glossary 21

Food Allergy 1
INTRODUCTION
There has been a steady increase in public interest in theimportance of diet and its relevance to health. At the sametime, however, the public has become concerned thatadverse reactions to foods, food additives and drinks maybe common and that they can cause a wide range ofdistressing physical and psychological problems andchronic, disabling diseases.
Adverse reactions to foods certainly do exist, but thelabel of “food allergy” applied to many of these reactions isoften incorrect. Unfounded and inaccurate claims for adiagnosis of food allergy have created unnecessary alarmamong the public and have diverted attention from somebasic problems.
There are a number of reasons why it is difficult todiagnose and study adverse reactions to food:• They are caused by a wide range of foods and food
additives, many of them common components of the diet.• They give rise to a wide variety of symptoms, many of
which are not specific to adverse food reactions, andwhich may appear at a variable time after ingestion of afood.
• They are caused by a diverse range of mechanisms.• Some adverse reactions are psychologically based.• Diagnostic methods can be cumbersome.
In this monograph, we will put adverse reactions tofoods into perspective. These reactions are not as commonas popularly thought, and the symptoms are often mild.Excluding psychologically based symptoms, probably nomore than one person in 50 is affected. Many foods arecapable of provoking a variety of symptoms in susceptibleindividuals, but the most common reactions are restrictedto a few common foods. Demonstrable reactions to foodadditives are about 10 times less common than to foodsthemselves.
SYMPTOMS AND SYNDROMESCAUSED BYAD VERSE REACTIONSTO FOODS
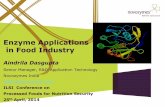
The diagnosis of adverse reactions is complicated by thefact that many foods are involved (Table 1), causing a widerange of symptoms by a variety of different mechanisms. Asingle food may give rise to different symptoms, butlikewise the same symptoms may have a number ofdifferent causes.
For example, identical symptoms may be elicited by anumber of foods: eczema may be caused by milk, egg andmany other foods in one and the same person. Asthma canoccur as an allergic response to milk, but it can also betriggered by the irritant effects on the air passages ofpreservatives such as sodium metabisuiphite.
Even where a single food is involved and a single partof the body affected, different mechanisms may be responsible in different individuals. For example, diarrhoea ininfants receiving soya formulas can be caused by a reactionto the protein in soya, or by an inability to digest disaccharides, especially in formulas containing sucrose.
A single food can give rise to a wide spectrum ofadverse reactions. For example, wheat can cause diarrhoea,urticaria and baker’s asthma, due to allergic reactions towheat protems. In individuals who suffer from coeliacdisease, there is a reaction in the intestine against one of theproteins found in wheat, causing diarrhoea and malabsorption. Bread made from wheat can affect intestinalphysiology causing effects which may appear abnormal tosome individuals (discussed further in Diagnosing IrritableBowel Syndrome, below).
Symptoms in Children
Many symptoms have been associated with adverse foodreactions in children, including diarrhoea, vomiting andblood loss from the digestive tract, eczema, asthma, whealsof the skin (hives or urticaria), swelling of the tissues

2 Concise Monograph Series
(angioedema), migraine and anaphylaxis, as well as someless well-defined conditions especially in severely affectedchildren who are irritable or fail to thrive. An estimatedthree-quarters of these cases develop by the age of one year.
Some of the conditions which occur in infancy andearly childhood are predominantly diseases of early life, butothers remain lifelong problems. Recovery rates varyaccording to the food. Children with an apparent intolerance to cow’s milk protein can often tolerate milk withinmonths of diagnosis. However, recovery is least likely tooccur in children with allergies to other foods such aspeanuts, nuts and fish.
Certain foods are capable of damaging the lining ofthe small intestine, the best-known example being thedamage arising from consumption of wheat products incoeliac disease (discussed in detail in the section on CoeliacDisease, page 16). Coeliac disease affects all ages, hut someother, less common, reactions are seen only in children,such as when they are caused by a sensitivity to cow’s milkprotein or to soy, chicken, rice, fish and egg.
Symptoms in Adults
In adults, the classic allergic symptoms of urticaria, asthmaor anaphylaxis may be seen. Some foods provoke
Type of Reaction Cause Foods/food compounds involved
Food allergy Allergic reaction to a food caused by an over-sensitive Eggs, milk, wheat, fish, shellfish, nuts,reaction of the body’s immune system peanuts, soybean, rice
Pharmacological Absorption of certain amines from foods containing Fermented foods (cheese, red wine,high amounts sauerkraut, fermented sausages);
fish productsOther substances with pharmacological type of action Caffeine
Enzyme defects Failure of normal enzymatic breakdown after absorption Alcohol, fructose, aminesFailure to digest, so that unabsorbed substances reach Lactose (in milk), fatsthe lower intestine, where they are fermented
Irritant Often made worse by acid which refluxes from the top Strong spices and flavours; suiphitesend of the stomach to cause heartburn
Toxic Toxins Some shellfish, badly stored food (e.g.,green potatoes), and some vegetables,some fungi
TABLE 1
Adverse Reactions: Causes and Foods Commonly Involved
Psychological foodintolerance
Emotional reaction to a food (reaction does not occurif food is unrecognised)
V

Food Allergy 3
gastrointestinal symptoms. Overactive movements of thegastrointestinal tract and increased secretion of mucus seenin allergic reactions often result in nausea, vomiting,abdominal pain and diarrhoea.
Similar but often milder episodes of nausea, bloating,abdominal pain, constipation or diarrhoea occur in patientssuffering from the irritable bowel syndrome. Symptomsoccur when there is an abnormal response of the intestine after food is consumed, but in some cases there is astrong psychological component to the perception of thesymptoms.
It has been suggested that migraine may sometimesresult from intolerance to certain foods (cheese, chocolateand red wine have been cited). However, the relationship offood to migraine is poorly understood.
FOOD ALLERGY
Food allergy is not the most common cause of adversereactions to foods, but it is one of the best understood. Thereis a wide range of symptoms caused by food allergy,affecting many parts of the body (Table 2), and reactions aresometimes serious. These reactions can occur very quickly,often within minutes, and hence are termed immediatereactions. In the oral allergy syndrome, the lips, cheeks,tongue or throat may swell or itch within minutes of contactwith such foods as eggs, nuts or peanuts. Similar reactionscan affect the skin, the lungs or the digestive tract, causingsymptoms such as skin wheals (urticaria), wheezing(asthma), vomiting and diarrhoea.
Such allergies are more common in children than inadults. Foods commonly involved include eggs, peanuts,cow’s milk, soy, wheat, peas, fish, shellfish and nuts, butreactions can also occur to spices such as mustard andsesame or to vegetables, for example, celery and tomato.
Allergy is essentially “immunity gone wrong” wherea normally harmless substance is perceived as a threat—anallergen—and attacked by the body’s immunologicaldefences. Food allergy involves the reaction of a foodprotein with antibodies produced against it by the immune
system. The accompanying symptoms are the result of thisinappropriate immune response.
The operation of the immune system is complex andmuch remains to be learnt about it. The following gives anoutline of our knowledge in order to provide an insight intowhy and how allergic reactions arise.
The Immune System and Its Role in FoodAllergy
The body’s immune system provides a vital defence
TABLE 2
Symptoms of food allergyGastrointestinal
NauseaVomitingColicDiarrhoeaAbdominal crampsBloating
RespiratoryRhinitisSneezingAsthmaRecurrent coughWheezingLaryngeal oedema
DermatologicalAngiooedemaUrticariaEczemaPruritisErythema (skin inflammation)
OtherAnaphylaxis

4 Concise Monograph Series
FIGURE 1The structure of gE antibodies
mechanism against harmful substances and againstinfection. Immunological reactions to polio vaccine, forexample, provide an individual with long-lastingprotection against infection with the polio virus.
Defensive cells in the body produce antibodies ofdifferent types which react specifically with foreignmicroorganisms, viruses or foreign substances such asproteins. Antibodies are specific proteins produced by thebody which fit onto foreign molecules in a lock-and-keyfashion. Although the body’s defensive cells can potentiallyproduce a vast variety of immunoglobulins (Ig’s), immunereactions trigger the production of specific antibodies inresponse to particular foreign substances or proteins. Oncea particular antibody has been formed (against polio virus,for example), it can be mass-produced by the bodywhenever it is needed.
Antibody structures all follow a basically similarpattern (Fig. 1). Although there are other classes ofantibodies (IgG, IgA, 1gM), it is IgE which is important in
mucous membrane epithelium)lining the intestine, respiratorytract, etc.
zzz B cell
T cell
tgE
lgE secreted by B cells circulates throughout the bodyvyvy
immediate allergic reactions. Antibodies bind to foreignproteins or other foreign substances known as antigens,thus neutralising their effect. The antigen may be part of thecoat of an invading bacterium or virus or a free molecule,for example, a protein from cow’s milk. The antigens infoods which provoke an IgE response are mostly proteinsor glycoproteins (proteins with sugar groups attached).
FIGURE 2Production of IgE antibodies
Antigen attaclres to receptors on the surface of a I cell. Antibody on the surface of m Bcell also recognises the antigen, arrd after contact with the T cell, the B cell and itsdaughter cells are primed to produce IgE. lrrterleukin 2 llL-2), secreted by I cells,promotes proliferation of B cells. Interleukin 4 )lL-4), also secreted by T cells,promotes IgE production.
TIns part of the gE antibody bindsantigen. It has a variable structuresvhich is urrique for the specificantigen.
6’This part of the gE antibsrdy is culledthe “fixed” region. It binds to variouscells of the immune system, includingmast cells.
lL-4
antigen
daughter B cells
B cells are stimulated toproduce lgE by 11.4secreted by I cells

Food Allergy 5
B cells and T cellsB cells and T cells are types of mobile white
cells called lymphocytes. They develop andcongregate in the organs of the immune system.B cells ongrnate from stem cells in the bone marrowand elsewhere. Each B cell produces one type ofantibody which is capable of reacting with onespecific antigen in a lock-and-key fashion.Collectively, B cells produce the many thousands ofdifferent antibodies needed to counteract the manyantigens which may be encountered in a lifetime.(Those clones of B cells which could act against thebody’s own proteins are eliminated in early life.)When a particular foreign antigen enters the systemfor the first time, the B cells that produce theantibody against the antigen are primed andactivated, so that thereafter they (and their daughtercells) can mass-produce the appropriate antibodieswhen required. B cells carry samples of their specificantibody on their surfaces, thus permitting theirproliferation following interaction with specificantigens. T cells control the activity of B cells (Fig. 2).
T cells also originate from stem cells, notably inthe thvmus. They do not secrete antibody but like Bcells they can recognise a legion of antigens throughreceptors present on their surfaces—the “T cellreceptor”. Part of the T cell receptor comprises anantigen-specific molecule related to immunoglobulin. This acts like an antibody, binding to aspecific antigen. The combination of an antigen withits specific T cell receptor enables the T cell to controlthe activity of B cells which recognise the sameantigen. “Helper” T cells stimulate the corresponding B cells to secrete antibody against thatantigen. “Suppressor” T cells can reduce the activityof corresponding B cells, inhibiting lgE production.T cells also have other regulating effects on theimmune response, mainly through the chemicalsignalling substances—interleukins——which theysecrete.
FIGURE 3Sensitisation of mast cells
IgE is produced by white cells known as Blymphocytes or B cells. Another type of lymphocyte, the“helper” T cell, is also involved in the process. It is asecretion of this cell—interleukin 4 (IL-4)——whichinfluences B cells (see box) to produce IgE rather thananother class of antibody (Fig. 2).
The IgE secreted by B cells circulates throughout thebody. One part of IgE has a particular affinity for receptorson the surface of mast cells found in body tissues. Mast cellsbind the tail of IgE molecules, which thereby sensitise thosecells to specific antigens (Fig. 3).
if, in a subsequent encounter with the sensitised mastcell, the antigen forms a bridge between two adjacent IgEmolecules, this acts as the signal for the release of a varietyof substances which either have been stored in granules inthe mast cell (for example, histamine) or are newlysynthesised at the cell surface (such as prostaglandin D2 andleukotriene C4) (Fig. 4). Release of these substances causesan inflammatory reaction (see box, page 7) capable of
V V
The receptor-specific ends of gEmolecules attach to receptoss onmast cells, The antigen-specific endis free to react wish antigen.V
sensitizedmast cell

6 Concise Monograph Series
FIGURE 4Inflammatory reaction initiated by the mast cell
FIGURE 5The defence barriers of the intestine
damaging, destroying or otherwise facilitating the removalof the foreign material.
Mast cells are scattered below the skin surface andbelow the mucous surfaces in eyes, nose, mouth,respiratory tract and intestine. A food-allergic individualcan therefore have a widespread reaction when mast cellscoated with the appropriate IgE are triggered into activityafter encountering the corresponding antigen from thefood. On rare occasions, the intensity of the reaction can beextreme, manifested by oedema (swelling), breathingdifficulties, a drop in blood pressure and even heart failure.Known as anaphylactic shock, this severe reaction issometimes fatal.
The presence of sensitised mast cells in the skin can bedemonstrated by a simple test in which a small patch of skinis coated with a diluted food solution and then pricked witha needle. The development of a local wheal providesindirect evidence of histamine release and, therefore, of aspecific triggering of the local mast cells by a food antigencombining with the IgE on mast cell surfaces.
The Immunological Defences of the Intestine
Many potentially harmful substances and microbialorganisms are present in the tonne or so of food eaten by anindividual each year, but their penetration is largelyprevented by defensive barriers in the intestine (Fig. 5).Viscous mucus, produced by specialised intestinal liningcells forming the mucous membranes, behaves like anantiseptic paint. This “paint” contains various protectivesubstances including s-IgA and s-IgM antibodies, thes-prefix indicating that they are specifically modified topermit their secretion across the intestinal wall. Suchsecretory antibodies help counteract the entry of solubleantigens, for example, from food residues—a process calledimmune exclusion. Behind the mucous membrane is theepithelial cell layer. Histamine and other reactive substances are normally bound and destroyed by the mucosaand its enzymes. Substances that penetrate further than thismay encounter IgG antibody in the tissues or may triggermast cells primed with the appropriate IgE.
antigen
mucous membrane lepithelium) lining theintestine, respiratory tract, etc.
(lumen of the intestine J
.
protective mucous containing 1gM, gA and other bdingprotein
Mast cell degranulates, releasinginflammatory chemicals includinghistamine and producing other chemicalsfrom its surface, including prostaglandinsand leukotrienes
.0
I •.Ow ..
Eiiilary with IgG :
IDeepertissues containing T and B lymphocytes, macrophages (scavenger cells)

Food Allergy 7
FIGURE 6The Peyer’s patch of the intestine
A number of factors, some of which are inherited,determine whether a food antigen causes an allergic ratherthan another type of immune response. The presence ofregulatory molecules is important, for example, IL-4favours an allergic response. In susceptible people,intestmal allergy can occur when small amounts of antigenpenetrate the intestinal wall. Penetration of antigen isincreased when there is damage to the intestinal barrier.1-lowever, mechanisms in the immune system, both insideand outside the intestine, help to discriminate betweenthose antigens which wifi be “tolerated” and those whichwill start an immune reaction.
The importance of the immune system in the intestineis demonstrated by the fact that it contains about 80 billionlymphocytes, compared to a total of approximately 20billion in the important immune system organs of the bonemarrow, spleen and lymph nodes combined. Mostlymphocytes in the intestine are found in specialised areasknown as Peyer’s patches (Fig. 6). Each of these patchescontains some 30-40 groups of cells, mostly T and Blymphocytes, clustered in fofficles. In addition to theseconcentrated patches, there are much smaller areas of
lymphocyte-rich tissue, and many individual lymphocytesare also scattered along the Lining layers of the intestinewhere they can migrate to areas of inflammation.
Scattered over the surface of Peyer’s patches arespecialised cells (M cells) through which samples of theantigens present in the intestinal lumen penetrate into thelymphoid tissues of Peyer’s patches. Lymphocytes primedto produce antibodies by contact with an antigen throughthe M cells of the Peyer’s patches eventually reach the locallymph nodes and the circulating blood. From there theyseed themselves back to the wall of the intestine in manymore places, and are also spread to other mucosal sites,notably in the breast and the lung airways. In this way, thelocal effects of an immune response in the intestine can bespread to all the mucosal surfaces of the body by means ofrecirculation and distant seeding of T and B lymphocytes.
Why Do Some People Suffer from FoodAllergy?
The regulation of the mucosal immune response has topermit reactions against harmful organisms while ensuringtolerance to food antigens as well as to the normal
lumen of the intestine sampling cells (M cellsl
follicle lgerminal B cells T cells(entrei of B cells
Both food antigens and microorganisms can penetrate into the M cells and arebrought into contact with migrating lymphocytes. The Peyer’s patch caninduce either immune tolerance or an immune reaction, depending on thesolubility, concentration and other features of the antigen it encounters.
The inflammatory responseThe inflammatory reaction, which follows injury tothe body, increases the blood supply to the area andbrings protective white cells and components of theimmune system to the site of the injury. The scale ofthe reaction can be boosted by a series of enzymesand other blood constituents known as complement.These can also increase the permeabffity of bloodvessels. Prolonged reactions involve T lymphocyteswhich can infiltrate virtually all tissues. By releasingcompounds called lymphokines, T cells can attractyet more cells, leading to a further crescendo ofinflammatory activity.

8 Concise Monograph Series
(harmless) bacteria which reside in the gastrointestinaltract. The soluble antigens of food brought into contactwith lymphocytes within the sampling cells of Peyer’spatches seem to be able to induce a state of immuneunresponsiveness termed oral tolerance. This may bemediated by suppressor T cells which block the activationof specific lymphocytes. Thus, in most circumstances, theantigens present in food are recognised as harmless and donot trigger protective immune mechanisms.
Long-lasting oral tolerance is most easily induced ininfancy and childhood when the lymphatic tissues of theintestine first encounter the soluble antigens in new foods.This is also the most common time for defects in thedeveloping immune system to reveal themselves and forallergy to develop, indicating the finely balanced nature ofthe mechanism.
Food allergy appears to be an excessive response ofthe immune defences. There are a number of factors whichneed to be considered to understand why some peoplesuffer from food allergy:
• the patient’s genetic predisposition,• exposure to food and other allergens, and• the state of the gastrointestinal barrier.
IgE reactions may have originally evolved as adefence against parasites. With improvements in foodhygiene, such reactions may be less necessary for health,and those people who inherit a natural tendency to reactvigorously may actually be at a disadvantage. In allergicfamilies, it is known that suppression of the IgE responsedoes not occur as readily as in other people, possiblybecause of an inherited defect which leads to overproduction of IL-4 or because of a failure to produce thesuppressor substances known as interferons. These defectsmay explain why those with food allergy have a tendencyto suffer from other allergies such as asthma.
The tendency to develop allergy may be especiallymarked in children if both parents are affected. Manypatients with food allergy have large quantities of IgE onthe surfaces of their mucosal mast cells, and their children
sometimes have high blood levels of IgE at birth.Furthermore, the intestinal mucosa of some (but not all) ofthese children contains a reduced number of IgAproducing cells. It is possible that this IgA deficiency eitherallows intestinal infections to occur or permits food antigens to penetrate the intestinal wall more easily and thusstimulate IgE production as part of a “second line defence”.
In the newborn, the risk of developing an allergy is40—60% if both parents are allergic, 20—40% if one parent isallergic, and 5—15% if nobody in the immediate family isaffected.
Exposure to a potential food allergen can to someextent determine the likelihood of developing sensitivity.For example, allergy to fish is more common inScandinavia, as is rice allergy in Japan and allergy topeanuts in the United States.
The reaction to food antigens passing through theintestinal wall is affected by the state of the wall, whosepermeabifity may be greater when immature or increasedby inflammation following intestinal infection, allowingmore antigens to pass through. Passage of antigens isaffected by such diverse factors as degree of digestion (forexample, lack of stomach acid will reduce digestion);selective IgA deficiency; amount of antigen consumed andwhether it is ingested alone or with other foods; and thedegree to which food is cooked.
Delayed Reactions of Food Allergy
There is another type of allergic reaction to food where theonset of symptoms of inflammation is delayed. In the largemajority of such delayed reactions, IgE is not in evidence.This type of food allergy is less well understood andcharacterised than “immediate” IgE-mediated reactions.Delayed reactions involve other components of theimmune system including migrating cells of the T cell typeand various types of scavenger cells.
Delayed reactions may account for the occasionalcases of children with symptoms of a similar pattern whichappear to be provoked by cow’s milk, soya, fish, chicken orrice, and for some of the reactions which occur in babies

Food Allergy 9
sensitive to cow’s milk. Such reactions of delayedhypersensitivity also account for at least some of theintestinal problems which occur in coeliac disease (see page15).
NON-ALLERGIC REACTIONS TOFOODS
The symptoms of a number of adverse reactions to foodsmimic allergic reactions but nevertheless do not have animmunological basis. These include certain urticarial skinreactions and other manifestations similar to the symptomsof true allergy. Many of these patients also have abdominalcomplaints, including abdominal pain and intermittentdiarrhoea. Such reactions are due to a variety ofmechanisms (see Table 1). For example, it has beenestimated that food allergy is demonstrable in fewer than3% of cases of chronic urticaria but some of the remainderare due to non-allergic reactions to food.
Food Constituents with PharmacologicalEffects: Adverse Reactions Involving AminesIn many cases of non-allergic reactions to food, substancesknown as amines are responsible. Such amines are oftentermed biogenic amines owing to their physiologicallypowerful effects and are the same or similar to thosereleased by mast cells as a result of an IgE-mediatedreaction. This may explain the similarity of the symptoms tothose found in food allergy.
There are at least four major mechanisms whereamines are involved in adverse reactions to foods:
• Absorption of biogenic amines such as histamine andtyramine from the intestine, due to either abnormallyhigh levels in food or, more controversially, resultingfrom synthesis of amines in the intestine by bacteria.
• The enzymes that normally degrade the amines presentin food may be absent or partially inactivated.
• The nervous system may regulate the release of histaminefrom, for example, mucosal mast cells. Some irritants likealcohol or spices may affect nerve endings, thusstimulating histamine release in the mucosa.
• Components in food may directly stimulate the release ofhistamine and other chemical mediators from mast cells.
Biogenic amines are normal constituents of manyfoods, but they can also develop during cooking andstorage. The largest amounts of histamine and tyramine arefound in fermented foods such as cheese, alcoholic drinks,tinned fish and fish products, sauerkraut, pork andfermented sausage products. Scombroid fish (tuna ormackerel) is sometimes stored at temperatures high enoughto allow the generation of histamine and otherphysiologically active amines.
The bacteria normally present in the intestine maysynthesize histamine from foods rich in the amino acidhistidine. Histamine may be absorbed from the intestine,especially where inflammation or other damage hasincreased the permeability of the intestine. If histaminepenetrates as far as the bloodstream, it can cause flushing bydilating the blood vessels, increasing capillary permeabilityand causing constriction of the smooth muscle of bronchiand intestine. Experimental infusion of histamine into thebloodstream has been shown to stimulate gastric secretion,and above certain levels there are adverse effects on bloodpressure, the pulse rate rises and headache occurs. Stillhigher levels can lead to asthma and the danger of heartfailure.
Besides being absorbed from the intestine, histaminemay also be released directly from mast cells and basophils(white blood cells which contribute to symptoms of allergy)by constituents of certain foods. The mechanism is poorlyunderstood but does not involve IgE. Foods involved mayinclude indude strawberries, fish and shellfish, but thisrequires confirmation.
Tyramine also has a number of significant effects. Itmakes the arteries constrict, raises the blood pressure andcan cause migraine headaches.

10 Concise Monograph Series
Other types of amines in food have also beenimplicated in adverse reactions. Diamines such asputrescine and cadaverine are present in wines, andspermidine occurs in pork and in cereal grains. Other activesubstances include catecholamines present in variousvegetables, tryptamine in tomatoes, and 5-hydroxytryp-tamine in bananas and avocados.
How does the body defend against amines in foods?Specific types of proteins present in the mucus of thestomach and intestine (Fig. 5) normally bind and inactivatehistamine. This protective effect can be lost. For example,the amines putrescine and cadaverine bind strongly tothese proteins, leaving fewer binding sites for histamine.Nevertheless, most of the histamine which passes throughthe epitheium is degraded by the enzyme diamine oxidasewhich is located in the wall of the intestine. However,putrescine and cadaverine also have a high affinity fordiamine oxidase and can inhibit this breakdown ofhistamine.
Histamine is also inactivated by another enzyme,histamine methyltransferase. Although present in theintestine, especially the colon and rectum, its activity isgreatest in the liver. Liver disease (for example, acutehepatitis) can interfere with the activity of the enzyme.
As a result of these defence mechanisms, the amountof free histamine absorbed from food and reaching theblood is normally very low. There is evidence, however,that recurrent reactions to food rich in histamine may bedue to a number of mechanisms. These include increasedintestinal permeability to histamine, or a defect in themechanism which breaks down histamine.
Other Food Constituents withPharmacological EffectsExcessive drinking of coffee or tea has been associated insome individuals with side effects such as heartburn,gastrointestinal disturbances, anxiety, tremor, irregularheartbeats and sleeplessness. Some of these effects can beascribed to the effects of caffeine. Pharmacological effects
can also be caused by unusually high quantities of sodiumnitrite, an antioxidant used as a bactericidal agent in curedmeats. Nitrites dilate the blood vessels and cause flushingand headache, urticaria or intestinal symptoms.
Enzyme Defects as a Cause of AdverseReactions
Enzyme defects have a genetic origin. The best-knownexample is alactasia, a common form of intolerance to cow’smilk found in people who have a partial or more seldom atotal deficiency of the enzyme lactase, which digests themilk sugar lactose. Alactasia affects up to 80% of the adultpopulation in many parts of the world where a normal andprogressive loss of lactase is experienced during childhoodas milk consumption declines. In individuals with alactasia,most of the undigested, unabsorbed lactose that reaches thelarge intestine is fermented by bacteria there, formingcarbon dioxide and lactic and propionic acids. The resultinggaseous distension and irritation may cause considerablesymptoms (Fig. 7). The symptoms of alactasia mimic thoseseen in cases of the irritable bowel syndrome, which mayalso be due to the fermentation of unabsorbed foodresidues. Alactasia is also sometimes found as a geneticdefect in babies where it has serious implications as milk issuch an important part of the infant diet.
Other enzyme deficiencies can have more generalisedeffects. For example, people of Asian origin commonly havea deficiency of the enzyme aldehyde dehydrogenase andcannot metabolise alcohol as readily without theaccumulation of toxic aldehydes.
Adverse Reactions Due to Toxins in Foods
Toxic effects are to blame in some cases where allergicreactions are suspected. For example, reactions to shellfishcan be caused by poisonous dinoflagellates on which theshellfish fed. Toxins can occur naturally in some commonfoods, for example, glycoalkaloids in badly stored or greenpotatoes. Toxins may also be present in lima beans and

Food Allergy 11
FIGURE 7Digestive tract and adverse reactions to foods
pharmacological and irritant effectscausing acid reflex
intestinal hurry due to lactoseintolerance or tat malabsorption
irritable bowel syndrome
millet sprouts. Cassava roots need careful processing toprevent toxicity arising from the cyanide-generatingglycosides. Toxins capable of causing ifiness also arise fromfungal or bacterial contamination of food or bydegenerative changes in poorly stored food.
DIAGNOSIS OF ADVERSEREACTIONS TO FOODSDoctors who are aware of the dangers of overdiagnosis offood allergy and the consequent use of inappropriatedietary restriction are sometimes sceptical that a genuineproblem exists. By the same token, patients with adversereactions to foods may be unaware of the relevance of foodto their symptoms. Greater awareness is therefore neededby doctors about the symptoms of adverse reactions tofoods and the diagnosis and management of the manyrelated conditions.
There is a wide range of both clinical and laboratorytests for the diagnosis of food intolerance, but they vary intheir validity and interpretation. In patients with animmediate type of allergic reaction, skin prick tests orlaboratory tests for IgE against food antigens are useful.Biopsies of the small intestinal mucosa in patients withcoeliac disease can also aid diagnosis. The value of otherlaboratory tests and diagnostic procedures is limited.
An adverse reaction to a food can only be confirmed ifthe symptoms disappear after elimination of the suspectfood from the diet and reappear following a challenge test,where the food is reintroduced into the diet. Such testsshould always be used to confirm an adverse reactionexcept in those people whose reactions are so severe that achallenge could be dangerous. If the test is to be convincing,the reintroduction of the suspected food should be in a formunrecognised by the patient.
The most convincing form of challenge test is thedouble-blind, placebo-controlled food challenge. The firststep is to control the patient’s symptoms by eliminating oneor more suspect foods from the diet. “Challenges” are thenperformed by administering to the patient either a
Symptoms and syndromes
oral allergy syndrome

12 Concise Monograph Series
Controversies Surroundingthe Diagnosis of AdverseReadions to Foods
An entire repertoire of diagnoses and treatments isbased on unsubstantiated theories concerning foodreactions. These include the placement of food dropsunder the tongue, either for diagnosis or treatment,and tests where different dilutions of a suspectmatenal are applied to the skin, looking for a“neutralisation point”. The so-called cytotoxic testdepends on exposing the patient’s blood to differentfood solutions to assess, for example, how quicklythe blood cells die. Hair analysis and a variety ofelectrical tests are other examples of tests offered tothe public which have not been objectivelyvalidated.
Commercial laboratories which advertise“allergy” diagnosis may fail to distinguish betweenadverse reactions with an immunologicalmechanism, for which useful tests are available, andthose which have other causes. In one study, ninefish-allergic and ten healthy individuals providedblood samples which, after coding, were sent to fivecommercial laboratories and to a hospital laboratory.One of the commercial laboratories requiredspecimens of hair. Widely discrepant results werereported by the commercial laboratories betweenpairs of blood or hair samples taken from the sameindividual. Non-existent allergies were alsodiagnosed in virtually all the normal subjects. Thehospital laboratory tested for IgE antibodies andobtained 37 correct results out of the 38 samples sentfor testing (19 coded pairs).
suspected food or a placebo so that neither the patient northe clinical observer knows what is being received. Theobject of such a “double-blind” procedure is to avoid abiased perception of symptoms. Reactions are frequentlyreported when a challenge contains no food but onlyplacebo, so challenge tests carried out in this way areessential in order to eliminate the possibility ofpsychologically based symptoms. Many early studies ofadverse reactions to foods did not employ this technique,and the results are consequently questionable.
Diagnosing Irritable Bowel Syndrome
Symptoms of the irritable bowel syndrome include nausea,bloating, abdominal pain, constipation and diarrhoea.These features are thought to result from abnormal motilityof the gastrointestinal tract, and it is now accepted that insome cases there is an adverse reaction to a food. There havebeen several reports that the exclusion of specific foods canabolish symptoms of the irritable bowel syndrome,especially in cases associated with diarrhoea. Theassociation between these symptoms and consumption ofmilk is clear in patients with alactasia, but in other cases ofthe syndrome the cause is not known.
Diagnosis of the irritable bowel syndrome iscomplicated by the fact that some individuals are undulysensitive to the feelings associated with the normalcontraction or distension of the intestine. Changes in diet,for example a change from white to wholemeal bread, canspeed up mouth-to-anus transit rate, influence intestinalmovement, increase stool weight, produce a softer stool,increase frequency of defecation and increase the quantityof flaWs. Likewise, some food residues, for example, starchfrom wheat flour, may not be fully broken down by thedigestive process. In the large intestine it can act as asubstrate for bacterial metabolism and thereby produce gas.These normal effects are considerably more obvious to thepatient than to the outside observer and may even coincidewith the symptoms of the irritable bowel syndrome.
It is therefore difficult to evaluate these symptomsand to distinguish those which have a psychological origin.

Food Allergy 13
Diagnosing Psychological Reactions to Foods
People’s attitudes to food vary widely and can result indieting, overeating and food fads. Adults with eatingdisorders such as anorexia nervosa may seize on thesuggestion that their problem could be “allergic” in order toavoid the stigma of a primarily psychiatric diagnosis. Manypeople who go to the doctor complaining of adversereactions to food are undoubtedly over-anxious, but thisdoes not necessarily mean that the symptoms are imagined.For example, apprehensive patients may overhreathe(hyper-ventilate) and thereby develop giddiness, a rapidpulse, nausea, weakness, tingling of the hands and feet, andthought disturbances. Once they have been shown thathyper-ventilation reproduces their symptoms, thesepatients will generally respond to appropriate treatment.
Patients who have psychologically based symptomswithout organic disease may diagnose themselves assuffering from any one of a number of “fad” diagnoses,which may include food “allergy,” leading to the use ofinappropriately restricted diets. Parents who describe theirchild’s adverse reaction to a food may be reflecting theirown psychological state rather than the illness of the child.In a well-recognised form of child abuse, the so-calledMünchausen’s disease by proxy, such parents invent storiesabout a child’s symptoms or physical abnormalities as areason for imposing dietary or other restrictions on thechild.
Even when carefully conducted tests give negativeresults, many patients with symptoms may still refuse toaccept that organic disease is absent. Because suchdiagnoses fail to address the patient’s problem, many suchindividuals lead limited, disabled lives while denying thepossibility of a psychiatric component to their ill health.These patients are in need of a sympathetic hearing,appropriate investigation and much patience and supportfrom their physicians. Without this, many wifi seek therapyfrom unorthodox practitioners.
ALLERGY TO COW’S MILK
More than 2000 years ago Hippocrates observed that cow’smilk could cause both stomach upset and urticaria. Cow’smilk can cause an allergic response in infants as well as
other adverse reactions by a variety of mechanisms,including lactose intolerance due to alactasia. Allergy tocow’s milk occurs in 0.5—4% of infants and is the mostfrequent allergy seen in newborn babies, perhaps becausecow’s milk proteins are among the first foreign antigensthey encounter. The infant is usually sensitised by beingbottle fed and develops symptoms at any time between aweek and six months after birth. Less commonly, thesensitising protein comes from the mother duringpregnancy and the child is already sensitive at birth.Sensitisation can also occur through breast-feeding, whentraces of cow’s milk protein ingested by the mother findtheir way into breast milk.
The diagnosis of cow’s milk allergy is based on thehistory of milk-related symptoms, sometimes supported bylaboratory tests. An allergic cause is particularly likely if thesymptoms include eczema or urticaria, or if the milk hasbeen well tolerated for a period before the svmptonis began.As in other types of adverse reactions to foods, the results ofan oral challenge test can be conclusive. The condition isoften found in children with atopy, that is, where there is agenetic predisposition to allergic reactions as shown by afamily history of allergy.
The most dramatic symptom of allergy to cow’s milkis the immediate type of IgE-mediated allergic responseresulting in anaphylactic shock. This can be very severe andeven result in death if untreated. Other IgE-mediatedsymptoms may also occur, for example, the so-called oralallergy syndrome characterised by oral irritation, lip andthroat tightness, and lip swelling as well as a wide variety ofother symptoms typical of food allergy, occurring in anycombination.

14 Concise Monograph Series
Mild cases of cow’s milk allergy can easily be missed
when symptoms occur in an irritable child who does notsleep well or who has relatively mild diarrhoea or eczema,or when milk allergy causes gastrointestinal blood lossleading to anaemia. Differentiating between allergy and anon-allergic reaction to cow’s milk can be difficult, as in thechild who sometimes vomits and who develops colic afterfeeding but has no other specific symptoms.
Allergy to cow’s milk is not always permanent. Of
those who are sensitised before three months, 40% lose theirsymptoms by three to four years of age. However, of thosewho are sensitised after three months of age, 80% stifi havecow’s milk allergy when followed to three to four years ofage.
The Allergens of Cow’s Milk
There are numerous cow’s milk proteins, but the majorallergens are -lactoglohuIin, a- and -casein, and alactalbumin. Most affected children are sensitised to severalproteins of cow’s milk, but -lactoglobulin stimulates thehighest antibody levels even though if accounts for only10% of the total protein. Its potency as an allergen may bebecause it is the only type of protein in cow’s milk which isnot present in human milk and because it appears to besomewhat resistant to digestion in the stomach, allowingsome to he absorbed undigested.
Several cow’s milk proteins including -lactoglobulinstimulate the production of 1gM antibody, and sometimeslgG antibody, in most normal children and adults. But it isnot known how or in what circumstances these milkproteins stimulate the production of IgE antibody—andhence allergic reactions.
Making Milk Formula for Infants LessAllergenic
It is vital to find alternative feeds for infants who reactagainst cow’s milk. Formulae based on soy protein havebeen tried extensively, both in the prevention and in the
treatment of allergy to cow’s milk. F-lowever, 7—10% ofbabies showing allergy to cow’s milk protein also havereactions to soy formulae.
An alternative for these allergic babies are infantformulae where the protein has been partially digested withenzymes called proteases. These formulae have been in use
for several decades, especially where food allergy is likelyto occur in the first few months of life. Trials indicate thatnewborns babies with a family history of allergy experience
a significantly lower incidence of allergy when given milkproducts treated to produce the smallest size of proteinfragments compared with infants fed cow’s milk or soyapreparations. This benefit continues during the six-monthfeeding period and beyond.
Allergenicity of Milk and Milk Products
Milk remains an important dietary component beyondinfancy, and it is therefore important for those who remainsensitive to milk to know whether processing of milk can
reduce its ability to provoke a reaction. Of the standardmethods of dairy processing, only heat processing andfermentation are known to affect the allergeriicity of milk.
High temperatures reduce the allergenicity of themajor whey proteins such as a-lactalbumin and 13-lactoglobulin. This reduction of allergenicity maybe helpfulin some cases of milk allergy but not in others, because heatdenaturation does not reduce the allergenic potential of allmilk proteins, for example, casein, which is remarkablyheat insensitive.
In fermented milk products like yoghurt and kefir, thestructure of the milk proteins may remain largely intactafter fermentation, thereby maintaining their allergenicity.Although a greater degradation of milk proteins may occurduring cheese manufacture, this is not consistent, and it istherefore not safe to assume that all cheeses have lowallergenic potential, especially fresh cheese or cheeses witha very short ripening period.

Food Allergy 15
COELIA C DISEASE
Coeliac disease, first described as a clinical entity a centuryago, gives insight into how our ideas on adverse reactions tofoods have developed. The classical description of patientswith coeiac disease is of children under the age of threeyears who fail to thrive and who have striking fattydiarrhoea, an enlarged abdomen, limp muscles, weaknessand a bad temper. In younger children, loss of appetite is aprominent symptom, whereas the older ones mostly eatnomally. Infants tend to vomit after feeding and, as theygrow, may be so weak that they cannot walk or even standup. Some have severe malnutrition, anaemia and theswelling of the legs and abdomen that is characteristic ofprotein deficiency. They fail to gain weight. In olderchildren growth retardation is the most prominent andsometimes the only clinical symptom. Severe and typicalcases are now likely to be identified at an early stage, but inmany instances the effects of the disease may be relativelymild and the symptoms vague, making diagnosis difficult.
The characteristic feah.mre of coeliac disease is thechange in the appearance of the viffi of the intestine (Fig. 8).Demonstrating this entails taking a sample of the cellswhich line the intestine and is now the cornerstone in thediagnosis of coeiac disease. It is not a simple test procedure,and for this reason there may stifi be delays in reaching adiagnosis. These changes in the vffli greatly reduce theability of the intestine to absorb fat and other nutrients, suchas fat-soluble vitamins and calcium, thus causing thecharacteristic symptoms.
Identifying the Causes of Coeliac Disease
During the Dutch famine at the end of World War II, it wasnoted that the condition of children with coeliac diseaseparadoxically improved on the diet of mostly potatoes,tulip bulbs and cabbage, whereas most other children lostweight. This observation together with another one thatbiscuits, bread and flour-containing meals could cause an
exacerbation of symptoms in children with coeliac diseaseled Dutch investigators to search for a factor in wheat whichwas toxic to these patients. They identified it as a proteincalled gliadin, which is an important component of gluten,the major group of proteins found in wheat. Similarproteins from rye, oats and barley, but not those of moredistantly related cereals like maize or rice, were also foundto be toxic to these children.
Susceptibility to coeliac disease is genetically determined. Between one in 350 and one in 2000 in the Europeanpopulation suffers from the disease. The highest prevalenceis seen in closed regions such as the Gaiway area in Irelandor in Austria, suggesting that genetic susceptibility varies.However, the incidence in North America is much lower
FIGURE 8Changes in the intestinal absorptivesurfaces in coeliac disease
In the normal intestine, the absorptivesurfaces have pencil-like villi withhair.like microvilli, providing a largeabsorptive surface.
normalvillus
normalcrypt {
In coeliac disease, there is a loss of villi,greatly reducing the absorptive surface. Thecryptu are enlarged and the epithelium isinfiltrated with T lymphocytes.

16 Concise Monograph Series
than in Europe among people of the same ethnic origin, so itis believed that environmental factors also influence thedevelopment of the disease.
Why Are Coeliac Patients Sensitive to Gluten?
It is still uncertain why sufferers of coeliac disease aresensitive to the gliadin found in gluten. Many abnormalitieshave been recorded but it is difficult to disentangle thosewhich are of primary importance in causing the diseasefrom those which are simply a result of the disease process.
A leading hypothesis is that an abnormality in theimmune system underlies coeliac disease, since increasedlevels of IgA, 1gM and IgG antibodies against gliadin arefound together with strikingly increased numbers of B andespecially T cells infiltrating the flattened epithelium. It ispresumed that there is a defect at some point in the immunemechanism which results in sensitisation to gliadin ratherthan tolerance. However, the changes that are seen maysimply be a reaction to undigested food proteins which seepacross the damaged intestinal wall. Even if this is the case,delayed-type immune reactions may still be an importantpart of the disease process, since a gluten challenge given topatients in remission leads rapidly to the appearance oftypes of T cells which are involved with cell destruction andto activation of mast cells and B cells.
Other hypotheses not yet completely ruled outpostulate that a defect in the structure of the epithelial cellmembrane is the primary cause of coeliac disease or thatimportant enzymes in the surface cells of the intestine arelacking.
Dietary Control of Coeliac Disease
Currently the only help for coeliac patients is a gluten-freediet. This is difficult to achieve because gluten is found inmany important cereal-based foods but also less obviouslyin numerous thickeners, emulsifiers and substitutes foranimal proteins. By adolescence, the discipline of a gluten-free diet may be difficult to enforce. Many children who donot strictly adhere to their diet experience no symptoms, so
it is difficult to assess the long-term effects of thisliberalisation of their diet. Some evidence suggests that thisnon-adherence to a gluten-free diet may increase the risk ofbowel cancer in later life.
Attempts are being made to identify the exactsequence of amino acids in gliadin which is toxic to coeliacpatients. This could lead to improvements in the antibodiesused in the analysis of gluten-free food. Furthermore, thisknowledge will be essential for the application ofbiotechnology in the future development of cereal cropscontaining non-toxic gliadin.
FOOD ADDITIVES: ARE THEY ANIMPORTANT CAUSE OF ADVERSEREACTIONS TO FOODS?Food additives serve technological functions in manyfoods. They are used to modify keeping quality, texture,consistency, taste, odour, alkalinity or acidity, or to assistthe process of manufacture.
Even traditional food processing involves the use ofadditives, whether the end product is a loaf of bread or abottle of wine. About 4000 of these ingredients are nowpermitted, a large proportion of which are flavourings usedin very small quantities. Other food additives ensure thesafety of foods or promote convenience, attractiveness andconsistent appearance and quality. Additives with “E”numbers have been approved as safe by the EuropeanCommunity. Any new ingredient must be approved byspecialist committees which consider whether there is aneed for the new material and whether it is safe.
There has been much public concern that additivescause adverse reactions. For example, 7% of a recentpopulation sample in the United Kingdom claimed to reactto food additives. In fact, the frequency of intolerance tofood additives appears to be low. In the above survey,careful investigation using double-blind challenge testsshowed that probably only 0.01-0.23% of the populationwere actually affected. It is clear from this study that public

Food Allergy 17
concern about food additive intolerance is often based onmisconception rather than on identifiable reactions.Adverse reactions to foods appear to be far more commonthan reactions to food additives.
Many earlier studies of adverse reactions to foodadditives used unrealistically high challenge doses or werenot confirmed with double-blind challenges. However,reactions to food additives can certainly occur. For example,sulphites can provoke asthma in certain asthmaticindividuals. This can follow when volatile sulphur dioxidein acidic drinks is inhaled or when suiphite is used topreserve the freshness of fruits and vegetables. More rarely,other food additives have been implicated in asthma. Foodcolours can cause urticaria in an occasional patient. Hyperactivity in children usually has quite different causes butmay perhaps on occasion be caused by food additives (seebelow).
There is therefore uncertainty about some of theearlier claims of adverse reactions to food additives. Wherethey have an effect, food additives appear to exacerbate apre-existing condition rather than induce it. Despiteinvestigation, there is little insight into how additivesproduce a reaction. Allergic mechanisms are rarelyinvolved, although IgE may be implicated in some suiphitesensitive asthmatics. It has been suggested that food coloursrelease histamine and prostaglandins in urticaria, mostlikely because of a direct pharmacological effect in thesesensitive individuals rather than by an allergic mechanism.Other additives may act in a pharmacological manner.
In assessing the risks and benefits of food additives, itis worth remembering that food poisoning from microbiological contamination is several thousand times morelikely to cause adverse effects due to food than is theoccasional asthmatic or urticarial episode provoked by thepresence of a preservative or other food additive. Since onlya very small minority of people are susceptible to foodadditives, informative labelling about the ingredients infood products is regarded as the best protection. As long asthere is a substantial safety margin for the population ingeneral, no other measures need be taken. Ir addition, in
the Netherlands, the United Kingdom and a few othercountries, doctors and dietitians now have access to databanks providing lists of food preparations which are free ofcertain foods or food additives known to he capable ofcausing adverse effects in susceptible individuals. lt hasbeen suggested that such information could usefully beextended to the additives present in antihistamines andother medicines.
Hyperactivity and Food Additives
It should not be surprising that some foods are capable ofaffecting behaviour. Art example is the effect of caffeine onalertness.
Children with allergic disorders such as asthma andeczema can become restless and irritable after eating foodsto which they are sensitive. There is little convincingevidence, however, that behaviour problems are the resultof adverse reactions to foods. Nevertheless, in recent years,physicians have seen an increasing number of parents whoclaim that their children become “hyperactive” as a result ofeating foods that contain food additives.
Hyperactivity is characterised by constantrestlessness, disorganization and inattention. However,agreed-upon norms for measuring activity levels andattention are lacking, and there is disagreement overwhether hyperactivity is a discrete condition or simply acollection of non-specific features present in manybehaviour disorders.
Confusion has also arisen because child psychiatristsin North America and Europe use different terminology.Many children diagnosed as hyperactive in some countriesmay be labelled as having a conduct disorder in others. Thefollowing definitions are often used in Europe: overactivityimplies an excess of physical activity which is neverthelesswithin the wide boundaries of normal; hyperactivity orattention deficit disorder with hyperactivity consists ofexcessive overactivity, short attention span and impulsivebehaviour. Young children with severe, intractablerestlessness and delayed development are sometimes

18 Concise Monograph Series
considered to be suffering from the hyperkinetic syndrome.Estimates of the numbers of hyperactive children also
vary depending on whether the figures are derived fromteacher questionnaire surveys (5—20%) or from clinicallydiagnosed children attending psychiatric clinics (0.1—1%).There is general agreement that four boys are affected forevery girl. Complaints about a child’s hyperactivebehaviour are common reasons for a child to be referred to achild psychiatrist. Brain damage and brain malfunction,zinc or vitamin deficiency, and sugar intolerance have allbeen proposed as causes of hyperactivity. However, theonly hypothesis that has been systematically tested hasbeen the proposal by B. Feingold in 1975 that hyperactivityin children is caused by food additives and salicylates(aspirin-like chemicals which occur naturally in somevegetables and fruit). Although unsupported by scientificdata, Feingold’s anecdotal reports led to widespreadpublicity and uncritical public acceptance, resulting in theformation of numerous support groups advocatingadditive elimination diets for hyperactive children.
Many of the studies of hyperactivity are open tocriticisms which reduce the validity of their findings. Itappears that there is a large placebo effect when diets areused to treat hyperactivity, and any significant effect of foodadditives on behaviour is much more difficult to reproducein properly conducted studies using double-blind challenges than would be expected from the claims of parents.There have been a number of well-designed trials, fromwhich there is limited evidence suggesting a possible effecton the behaviour of a small minority of young hyperactivechildren. These studies show that parents who believe thattheir children are hyperactive because of an effect of foodadditives are nearly always mistaken.
In conclusion, there is only limited evidence that foodadditives or any other dietary factor can produce more thana small and possibly transient effect on behaviour in someyoung children with hyperactivity.
Treatment of Hyperactivity
parents the many factors which may contribute tohyperactivity and give a reassurance that special diets arenot needed. Only in cases when behaviour problems aresevere or associated with learning problems will the childrequire assessment by a clinical psychologist or psychiatrist. In these cases, psychological and sometimes drugtreatment may be used.
An additive elimination diet is not usually indicatedand should not be used without good reason. Such diets areoften socially restricting. Very restricted diets carry thedanger of nutritional deficiencies, and the avoidance of fruitand vegetables containing “natural salicylates” as part ofthe “Feingold diet” is undesirable. Embarking on aninappropriate diet may also neglect other potentialmethods of treatment.
LIVING WITH ADVERSEREACTIONS TO FOODSHow Widespread Are Adverse Reactions toFoods?Accurate information on the numbers of people affected byadverse reactions to foods is difficult to obtain. Manypeople who react to a particular food never see a doctor butsimply avoid the food. Questionnaire surveys of representative samples of the general population find that from4.5% to 33% of the population believe they are affected byadverse reactions to foods. But such questionnaires includeall the built-in errors of self-diagnosis. Ideally, questionnaires should be followed up with challenge testswhere those who believe they react adversely to foods orfood additives are given the appropriate substances in anunidentifiable form and the response compared with that toa placebo. When this is done, a reaction to a food can beconfirmed in only about 20% of those who believe theysuffer from an adverse reaction to a food. This is in strikingcontrast to the study on additives mentioned above where7% of a population believed they reacted to additives: inonly one person in 25 of the 7% could a reaction to anadditive be confirmed.Often all that is required to allay anxieties is to explain to the

Food Allergy 19
Overall, the frequency of adverse reactions to foodsincluding food additives probably lies between the figurerecently proposed of at least 1.4% and about 2% (lactoseintolerance excluded).
Patient Self-Help Groups
Coeliac societies in various countries have built on theenthusiasm of non-medical people who, from experience,have learned the difficulties of getting good advice ondealing with the health problems and disabifities whicharise from coeliac disease. These societies compile andregularly update lists of manufactured foods which are freeof gluten. Excellent advice may also be available for patientssuffering from other adverse reactions to foods. One groupin the Netherlands has a medical board of advisers, invitescomments from an “alternative medicine” board andproduces its own quarterly publication. It also has supportgroups which meet regularly, a dietary advice group and atelephone service run by volunteers.
Identifying Allergens in Food
The identification of allergens in purchased foods is greatlyhelped by food labelling information and by food lists, databanks and advice offered by dietitians, patient self-helpgroups, government departments and food manufacturers.Such lists of foods that are free of milk, egg or gluten areinvaluable, particularly if backed by professional advice onhow to avoid mineral and vitamin deficiencies. The role ofthe dietitian can be crucial. Government requirements forfood labelling have also been of great help to those whomust face the practical difficulties of keeping to a rigorousdiet.
Meals eaten outside the home may pose the problemof the “hidden” allergen and cause reactions in highlysensitive people. Problems can arise with sauces ofunknown composition, the addition of peanut products incooking, or cross-contamination of a cooking utensil thatcontains residual proteins from a food to which anindividual is sensitive.
Controlling Adverse Reactions to Foods
The control of adverse reactions to foods can be approachedin four main ways: prevention, dietary manipulation, drugtreatment, and making foods less allergenic. The first twomethods are the main ones in use and are considered inmore detail below.
The treatment of adverse reactions to foods withdrugs has been largely unsuccessful. For example,disodium cromoglycate has been used in an occasionallysuccessful attempt to prevent reactions, but the results havemostly been disappointing. In severe cases corticosteroidsor adrenaline (epinephrine) are useful in giving symptomrelief. Administration of adrenaline and an antihistamine incases of anaphylactic shock can be life-saving.
Preventing and Treating Food Allergy in theInfant
Breast-feeding is commonly recommended as one of thebest ways to prevent, or at least delay, the development ininfants of allergy, especially to cow’s milk. However,because antigens from food eaten by the mother may enterbreast milk, breast-feeding can very occasionally provokefood allergy in babies where there is a strong family historyof allergy. It has also been suggested that it is beneficial tomodify the mother’s own diet in the last three months ofpregnancy by eliminating or greatly reducing the intake ofmajor food allergens such as milk products, eggs and peanuts. It is highly doubtful if such regimes are worthwhile.
While not uncommon, reactions to cow’s milk are notalways easy to recognize. The mother of an irritable babywho has a skin rash and diarrhoea and vomits cow’s milkmay find it hard to decide whether this is normal. Sincemilk is so vital, there are practical reasons for acceptingminor upsets caused by cow’s milk if the baby is notvomiting.
Protein hydrolysates or soy preparations can beoffered as alternatives in more severe cases of allergy tomilk. The development of less allergenic infant formulas is apromising approach.

20 Concise Monograph Series
Social Adjustments
Adverse reactions to foods can be a “hidden handicap” in achild with a perfectly healthy appearance. A family with afood-intolerant child has to surmount a number ofdifficulties. It may be necessary to convince familymembers that unpopular measures are necessary for thewell-being of the child and that they do not indicate awithdrawal of parental love. The change in eating habitsrequired of the child may be radical, and providing a dailyor weekly menu can be a formidable task. Compliance bythe child wifi be assisted if the whole family can eat a similarrange of foods, although restrictions on other familymembers cannot be carried too far. It may be helpful toleave a “forbidden” cake on the table in the hope that thiswifi habituate the child to confrontations with “forbidden”food outside the home. Possession of an emergency kitcontaining adrenaline may be vital where eating aprohibited food could cause a serious reaction.
Contacts outside the home, such as school personnelor friends’ families, should be alerted to the child’s allergyand the possible severity of an allergic response. An allergicchild out visiting can ease some of the problems by takingalong special food and drinks “just in case”.
It is never easy to keep rigidly to a diet, but themaintenance of good health is an adequate reward for thetrials and tribulations of a restricted food choice. Mostchildren can get used to a diet, however strict. From time totime, new foodstuffs should be tried, preferably under thesupervision of a doctor and dietitian.
SUMMARY
“Food allergy” has become almost a cult health preoccupation. Unfounded claims for its diagnosis or self-diagnosishave diverted attention from some very real medicalproblems and may lead to the omission of nutritious foodsfrom the diet.
Adverse reactions to foods are important in a widerange of conditions, including coeliac disease, cow’s milkreactions in infants, various types of food allergy andreactions caused by toxic substances, enzyme deficienciesand the pharmacological effects of some food constituents.
Confirmation of an adverse reaction to a fooddepends on the demonstration that reintroduction of thefood causes symptoms to recur that are not the result ofpsychological factors. Tests for IgE antibodies to food or forenzyme deficiencies or damage to the intestinal lining canprovide strong supporting evidence of an adverse reactionto that food.
The term allergy implies a reaction of the immunesystem involving among other events an IgE-triggereddischarge of histamine from the body’s mast cells. In thecase of coeliac disease, another form of immune reactionwith a delayed response may be involved.
There are various symptoms associated with adversereactions to foods. They include lip swelling, tightening ofthe throat, asthma, eczema, urticaria, headache, vomiting,diarrhoea and, in the most severe cases, a state of shock withother features of anaphylaxis. The most commonsymptoms in infants with cow’s milk allergy are vomiting,diarrhoea, eczema and failure to thrive. Children withcoeiac disease may have diarrhoea associated with otherfeatures such as weakness, a prominent abdomen and badtemper. This results from a reaction against wheat productsin the diet which causes damage to the intestinalepitheium.
Adverse reactions which do not have an allergicmechanism may produce symptoms similar to those offood allergy. For example, asthma may result from theeffects of the preservative sodium metabisuiphite, or

Food Allergy 21
diarrhoea may be caused by lactase deficiency and theconsequent fermentation of unabsorbed and undigestedlactose in the large intestine.
The overall frequency of food reactions is uncertain,because the majority of people who react to an individualfood never see a doctor. Apart from enzyme deficienciesthat lead to difficulty metabolising lactose in somepopulations and alcohol in others, adverse reactions tofoods affect only a small percentage of the population—probably less than 2%. Small children are the mostcommonly affected, and allergy to cow’s milk can beparticularly troublesome in the children of allergic parents.Reactions caused by food additives are infrequent, andmuch unnecessary anxiety has been caused by claims thatadditives are hanriful and that they are a frequent cause ofallergy or childhood hyperactivity.
It is therefore important that current knowledge aboutadverse reactions to foods be made widely available andthat physicians treat with sympathy and appropriatetesting patients who complain of food or additiveintoLerance. It is unwise to ignore the real or imaginaryproblems caused by adverse reactions to foods but equallyunwise to cause unnecessary alarm. Neither extreme ishelpful.
GLOSSARY
Allergen: A substance which provokes an allergicresponse.
Allergy: An inappropriate and exaggerated immuneresponse.
Amines: Organic compounds, usually derived fromamino acids, that contain nitrogen and hydrogen and
play a prominent role in biochemical systems.
Anaphylaxis: A generalized inflammatory immunereaction to a foreign protein in a sensitised individual
which may be severe enough to be life-threatening.
Angioedema: Swelling of the skin or mucous membrane
and underlying tissue.
Antibody: A protein molecule produced and secreted by
B cells in response to an antigen, which is capable ofbinding to that specific antigen.
Antigen: A foreign substance or protein that, whenintroduced into the body, is recognised by the immune
system.
Asthma: Breathing difficulty caused by narrowing of theair passages that is reversible.
Atopy: A genetic predisposition to allergic reaction.
B cells: (B lymphocytes) White blood cells derived fromstem cells in bone marrow and elsewhere that produceantibodies.
Basophil: A type of white blood cell that contributes toinflammatory reactions and symptoms of allergy.
Challenge test: Reintroduction of a food previouslyeliminated from the diet on suspicion that it caused anadverse reaction.
Complement: Blood proteins that amplify the action ofantibodies.

22 Concise Monograph Series
Double-blind food challenge: Food challenge test whereneither the patient nor the clinical investigator knowsthe identity of the administered substance.
Eczema: An itching red rash, often on the face, hands orskin folds, which oozes and crusts if scratched.
Enzymes: Proteins that facilitate metabolic reactions.Each enzyme is specific for a given substance.
Epithelium: The surface layer of the skin or the lininglayer of the intestinal mucosa or air passages of thelungs.
Fermented foods: Foods that have been subjected toprocessing involving the action of yeasts or bacteria.
Histamine: An amine found in all tissues of the body.Large amounts are released by mast cells when the bodyencounters a substance to which it is sensitive, therebytriggering symptoms of inflammation.
Immunoglobulins: Large proteins from which antibodies are formed, and which are then capable ofcombining with foreign substances (antigens).
Interleukins: Molecules which relay signals betweencells of the imniune system.
Leukotrienes: Chemical mediators of the inflammatoryresponse, released by various white blood cells and bymast cells.
Lumen: The channel within a tubular organ, for example,the lumen of the intestine.
Lymphocytes: White blood cells crucial to the body’simmune defence.
Malabsorption: Failure to absorb nutrients completely.
Mast cells: Granule-containing cells found in tissuewhose inflammatory responses contribute to thesymptoms of allergy.
Metabolism: The body’s highly integrated network ofchemical reactions catalysed by enzymes.
Migraine: Recurrent headaches, often mainly one-sidedand often preceded by flashing lights, nausea or otherwarning symptoms.
Mucosa: The lining membrane of tubular organs.
Permeability: Degree of leakiness of membranes.
Pharmacological: Pertains to drug-like actions ofchemical substances.
Placebo: A harmless and pharmacologically inactivesubstance, usually disguised, given to compare its effectwith that of an active material.
Prostaglandins: Fatty acids synthesised by various whiteblood cells and at the surface of mast cells, that can causeeither contraction or relaxation of smooth muscles in theairways and in certain blood vessels.
Protease: Enzyme that breaks down proteins.
Stem cell: Precursor cell in various systems which iscapable of producing the various functional cells of thatsystem by cell division and differentiation, e.g., stemcells which differentiate into lymphocytes.
Suiphites: Preservatives commonly used in, for example,wine.
T cells (T lymphocytes): White blood cells involved in theimmune response.
Toxin: Poisonous substance.
Urticaria: A raised, itching rash, often with well-circumscribed areas (wheaLs).
Wheal: A well-circumscribed raised area of skin.

Other Publications from ILSI EuropeDietary Starches and Sugars in Man:A Comparison1989. Edited by 1. DobbingILSI Human Nutrition Reviews SeriesAvailable from ILSI Press (originally published bySpringer-Verlag). ISBN 3-540-19560-2
Re-evaluation of Current Methodology ofToxicity Testing Including Gross Nutrients1990. Edited by R. Kroes and R.M. HicksFood and Chemical Toxicology, Vol. 28, No. 11.Published by Pergamon Press. ISSN 0278-6915
Recommended Daily Amounts of Vitamins &Minerals in Europe1990. Nutrition Abstracts and Reviews, Series A, Vol.60, No. 10.Published by C.A.B. International
Starches and Sugars: A Comparison of theirMetabolism in Man1991. ILSI Europe Concise Monograph SeriesPublished by Springer-Verlag.
Diet and Health in Europe—the Evidence1991. Edited by G.B. BrubacherAnnals of Nutrition and Metabolism, Vol. 35,supplement 1.Published by Karger. ISBN 3-8055-5400-1
Food Packaging: a Burden or an Achievement?(2 volumes)1991.Published by Symposia Paris. ISBN 2-9506203-0-2
Monitoring Dietary Intakes1991. Edited by I. MacdonaldILSI MonographsAvailable from ILSI Press (originally published bySpringer-Verlag). ISBN 3-540-19645-5
Food Policy Trends in Europe: nutrition,technology, analysis and safety1991. Edited by H. Deelstra, M. Fondu, W. Ooghe and R.van HavereEllis Horwood Series in Food Science and TechnologyPublished by Ellis Horwood. ISBN 0-7476-0075-9
Modern Lifestyles, Lower Energy Intake andMicronutrient Status1991. Edited by K. PietrzikILSI Human Nutrition Reviews SeriesAvailable from ILSI Press (originally published bySpringer-Verlag). ISBN 3-540-19629-3
Dietary Fibre—A Component of Food:Nutritional Function in Health and Disease1992. Edited by T. F. Schweizer and C.A. EdwardsILSI Human Nutrition Reviews SeriesAvailable from ILSI Press (originally published bySpringer-Verlag). ISBN 3-540-19718-4
Health Issues Related to Alcohol Consumption1993. Paulus M. Verschuren, Executive EditorPublished by ILSI Press. ISBN 0-944398-17-0
ILSI Europe Workshop on Nutrition and PhysicalPerformance1993. Edited by P.O. AstrandInternational Journal of Sports Medicine, Vol. 14,No. 5.Published by Thieme. ISSN 0172-4622
Scientific Evaluation of the Safety Factor for theAcceptable Daily Intake1993. Edited by R. Kroes, I. Munro and E. PoulsenFood Additives and Contaminants, Vol. 10, No. 3.Published by Taylor & Francis. ISSN 0265-203X
A Simple Guide to Understanding and Applyingthe Hazard Analysis Critical Control PointConcept1993. ILSI Europe Concise Monograph SeriesPublished by ILSI Press. ISBN 0-944398-18-9
High Temperature Testing of Food ContactMaterials1993. Edited by 1. GilbertFood Additives and Contaminants, in pressPublished by Taylor & Francis. ISSN 0265-203X
Nutritional Appraisal of Novel Foods1993. Edited by A. Bruce, N. Binns and A. JacksonInternahonal Journal of Food Science and Nutrition (inpress)Published by The Macmillan Press
European Directory of Food Packaging andMigration Research1993. Edited by J. GilbertPublished by PIRA/ILSI Europe (in press)