IHCA-ICAL 2012 Seating Surface Pressure Ulcer
23
PRESSURE DETECTIVES Seating Surfaces H Raymond Bingham, DPT, MBA, CWS Eastern Idaho Regional Medical Center Idaho Falls, ID
-
Upload
ray-bingham -
Category
Documents
-
view
54 -
download
9
Transcript of IHCA-ICAL 2012 Seating Surface Pressure Ulcer

PRESSURE DETECTIVES
Seating Surfaces
H Raymond Bingham, DPT, MBA, CWSEastern Idaho Regional Medical CenterIdaho Falls, ID

WHAT IS A PRESSURE ULCER?
According to the National Pressure Ulcer Advisory Panel (NPUAP): A pressure ulcer is localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with SHEAR.

WHO IS AT RISK? According to the NPUAP:
Consider all bed-bound and chair-bound persons, or those whose ability to reposition is impaired, to be at risk for pressure ulcers.
Soooo . . . . . Most residents of SNF’s/ALF’s qualify as either bed-bound, chair-bound OR “those whose ability to reposition is impaired”

WHAT ARE THE RISK FACTORS? (CLUES!!!) Pressure Shear Skin Microclimate
Heat Humidity
Friction Immobility Device-Related Pressure

PRESSURE
Google Definition The continuous physical force exerted on or
against an object by something in contact with it. Prolonged pressure impairs blood flow leading
to areas of tissue ischemia => cell death Larger surfaces redistribute pressure better
than smaller surfaces Immersion in the surface without bottoming
out reduces pressure

SHEAR
According to the NPUAP: Shear is a normal mechanic force with
physiological effects. The deformation of the tissues alters
the tissues physiology and increases the risk for pressure ulcer.
Some studies suggest that shear may play more critical role than pressure in ulcer formation.

SKIN MICROCLIMATE
Humidity (Moisture) Includes Incontinence, Sweating, &
External Sources (spilled milk, juice, soup, etc.)
Moistures affects skin by: ↓ the skin’s stiffness ↓ the skins strength ↑ Friction at the skin surface ↑ Adherence to surfaces => ↑ SHEAR

SKIN MICROCLIMATE
Heat Increased temp => Increased metabolic
rate Increases demand on cells for nutrients, O2, etc.
which are in short supply when under pressure Increased temp => Increased Sweating,
leads to increased moisture Encourage patients to wear the least
amount of layers they are comfortable with.
If pt must wear Incontinent Briefs Least bulky that works & breathable if able

FRICTION
Google Definition The resistance that one surface or object
encounters when moving over another. Increased friction will increase the
shear and magnify the pressure on the bony prominences
IMMOBILITY
Patients who lack mobility or who have altered mobility will be at higher risk for pressure ulcers as they will not be able to provide adequate pressure redistribution with assistance
Use Therapy to improve mobility. If therapy is not available/indicated, then
use restorative aides, activity directors, etc.

DEVICE-RELATED PRESSURE
If pt gets pressure ulcer while on pressure redistribution surface, need to assess the surface Flat ROHO example
If pt gets pressure ulcer in an odd place or with an odd appearance, check pt’s environment for sources of device-related pressure

RECOMMENDATIONS
Per NPUAP Reposition chair-bound pt’s at least every
hour Teach pt to do pressure relief activity every
15 minutes for pt’s who are able.
RECOMMENDATIONS
Educate Caregivers/Pt’s/Family Importance of pressure redistribution
surfaces Importance of pressure relief every 15
mins sitting Importance of maintaining posture during
sitting Limit sitting time to 1 hour, 3X/day max for
at risk or those with minor (Stage I or II) ulcers
Avoid pressure on Stage III or IV ulcers as much as possible

RECOMMENDATIONS
Use Therapies (Physical & Occupational) Use for Rehab to improve pt’s strength to
increase ability to reposition self in seating surfaces general posture
Many therapists have obtained specialized skills in assessing and recommending seating surfaces
Therapists will have good ideas on how to alter existing surfaces or postures to improve pressure redistribution

RECOMMENDATIONS
Obtain Specialized Seating Surfaces Foam Gel Air Combination
NO!!!! Donut-type Devices NO!!!! Sheepskin Devices NO!!! Egg Crate Devices

FOAM SURFACES
Use of viscoelastic foam for pressure redistribution

GEL SURFACES
Use of Viscoelastic gel for pressure redistribution

AIR SURFACES
Use of air-filled bladders to provide pressure redistribution
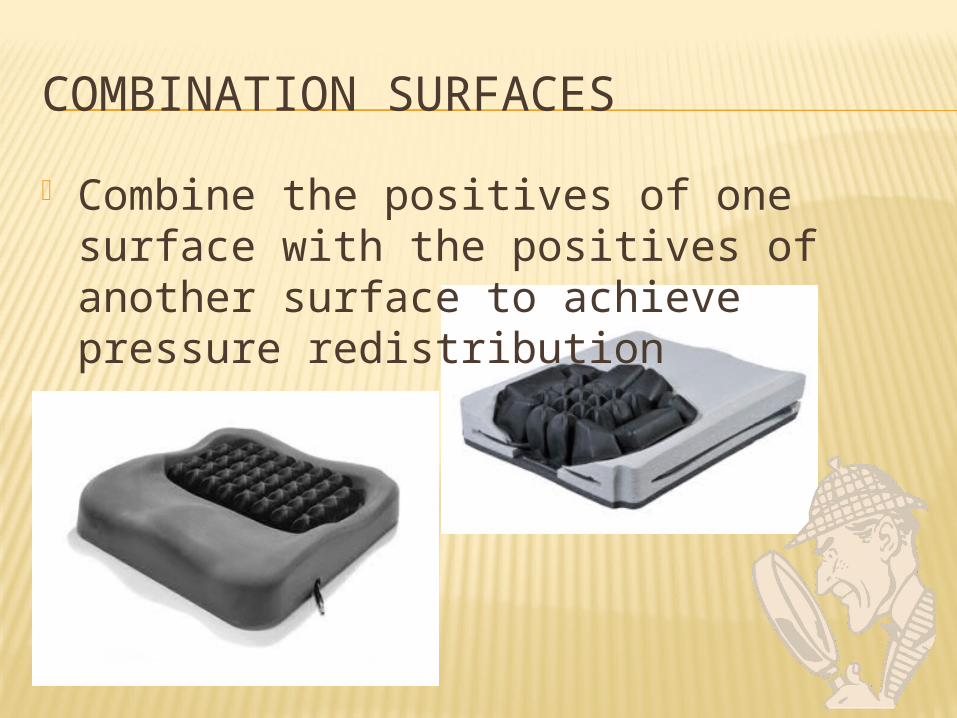
COMBINATION SURFACES
Combine the positives of one surface with the positives of another surface to achieve pressure redistribution

SPECIALTY CUSHIONS
Cushions for special populations or situations

ITEMS TO REMEMBER ON SEATING SURFACES
Purpose of seating surfaces is to REDISTRIBUTE pressure off bony prominences
If surfaces is too rigid, the surface will actually magnify the pressure on the bony prominences
If surface is too soft the bony prominences will rest on the base surfaces leading to increased pressure

ITEMS TO REMEMBER ON SEATING SURFACES
Select cushions based on individual patient characteristics
Patients bodies change over time and their cushion requirements will change too
Donuts, Sheepskin, and Egg Crates are NOT pressure redistribution surfaces
May use pillows/foam to achieve position change on pressure redistribution surface

A FEW TAKE HOME ITEMS
Make connections with a seating specialist (be it a P.T., O.T. or a vendor)
A wheelchair cushion is less expensive than treating a pressure ulcer (Prevention costs less than Treatment)
Do what’s best for your patients








![BOTA ICAL, PHYTOCHEMICAL A D BIOLOGICAL I ... are useful in filariasis, night blindness, helminthiasis, piles, ulcer and tumours [4]. It is reported to possess antifertility, aphrodisiac](https://static.fdocuments.net/doc/165x107/5cc8c6d688c993d63c8dc2b9/bota-ical-phytochemical-a-d-biological-i-are-useful-in-filariasis-night-blindness.jpg)