
Identifying cases & Quality Assurance: Data Completeness & Accreditation The Trauma Audit & Research...
24
Identifying cases & Quality Assurance: Data Completeness & Accreditation The Trauma Audit & Research Network (TARN) Data Collection session
-
Upload
drusilla-lynch -
Category
Documents
-
view
214 -
download
0
Transcript of Identifying cases & Quality Assurance: Data Completeness & Accreditation The Trauma Audit & Research...

Identifying cases&
Quality Assurance:Data Completeness & Accreditation
The Trauma Audit & Research Network (TARN)
Data Collection session

Identifying cases: 2 case studies

System 1: Retrospective Data captureClinical (ICD10) codes
Clinical coding departments use a coding system called ICD10
ICD10: International Classification of Diseases ICD10 codes document: Admission reason (Injury, Medical, Elective, Complication)
ICD10 codes that begin with S or T indicate injury e.g. S82.2: fracture to shaft of tibia S82.21: open shaft of tibia S82.20: closed shaft of tibia T055: Traumatic amputation of both legs

Trust IT dept. can therefore generate weekly spreadsheet showing:
Patients discharged previous week with any S or T ICD10 code Filtering out:
<3 days stay, discharge destination = home 65+ isolated NOF 65+ isolated pubic rami fracture Minor injuries
Full list of all applicable ICD10 codes: www.tarn.ac.uk/resources
Result: List of potential TARN patients
Check imaging reports to ensure inclusion
System 1: Retrospective Data captureClinical (ICD10) codes

System 1: Retrospective Data captureClinical (ICD10) codes

Example ICD10 spreadsheet
Age Admission
DateDischarge
Date Disch. Destination LoS Diag. 1 ICD Diag. 1 TextDiag. 2
ICD Diag. 2 TextDiag. 3
ICDDiag. 4
ICDDiag. 5
ICDDiag. 6
ICD
84 05/06/2010 16/07/2010 NHS NURSING 41 S0650TRAUMATIC SUBDURAL
HAEMATOMA K709 ALCOHOLIC LIVER DAMAGE UNSPECIFIED L031 B181 F102 N179
84 14/12/2010 06/01/2011 USUAL RESIDENCE 23 S825FRACTURE OF MEDIAL
MALLEOLUS S526CLOSED FRACTURE OF RADIUS AND ULNA,
LOWER END V99X
82 26/11/2010 01/12/2010 PATIENT DIED 5 S063CLOSED HINDBRAIN
CONTUSION W199[X]UNSPECIFIED FALL, OCCURRENCE AT
UNSPECIFIED PLACE N390 I48X I120 I258
78 01/06/2010 16/07/2010 USUAL RESIDENCE 45 S323CLOSED FRACTURE OF ILIUM,
UNSPECIFIED N390URINARY TRACT INFECTION, SITE NOT
SPECIFIED NOS I10X F339 F319 E039
78 04/07/2010 09/08/2010 USUAL RESIDENCE 36 S220CLOSED FRACTURE THORACIC
VERTEBRA W190[X]UNSPECIFIED FALL, OCCURRENCE AT
HOME N390 J22X I639 I10X
75 19/09/2010 05/10/2010NON-NHS RUN
RESID. CARE HOME 16 S422CLOSED FRACTURE PROXIMAL
HUMERUS, NECK S721CLOSED FRACTURE OF FEMUR,
INTERTROCHANTERIC W194 N390 D649 E039
75 03/10/2010 03/11/2010NHS NURSING
HOME/ 31 S327MULTIPLE FRACTURES OF
LUMBAR SPINE AND PELVIS S499[X]UNSPECIFIED INJURY OF SHOULDER AND
UPPER ARM W109 N390 R32X I10X
75 03/11/2010 21/12/2010 USUAL RESIDENCE 48 Z501 [X]OTHER PHYSICAL THERAPY S327MULTIPLE FRACTURES OF LUMBAR SPINE
AND PELVIS S499 I350 R32X I10X
Patients potentially have multiple ICD10 (Diagnosis) codes
Ensure your Trust reviews the first 5 diagnosis codes
Reviewing Primary Diagnosis code only – will definitely result in missed cases

System 1: Retrospective Data captureClinical (ICD10) codes: Advantages
Captures patients who bypass ED (transfers in, GP admissions)
TARN can liaise with IT to help set this up: SQL script
Limited staff resource required
Used by most Trauma Units who employ Retrospective data capture
Used as backup to “live” data capture by most Major Trauma Centres

Only admitted patients are assigned an ICD10 code Transfers out from ED Deaths in ED
Separate system required to capture these
Accuracy of Trust ICD10 coding
Use of NOS (not otherwise specified) codes can increase potential cases
Cases admitted for Rehabilitation only – not easily identified
Delay between discharge and clinical coding
System 1: Retrospective Data captureClinical (ICD10) codes: Disadvantages
System 2: Live Data captureEmployed by Royal Stoke University Hospital
Major Trauma CentreNorth West Midlands & North Wales Major Trauma Network
System 2: Live Data captureEmployed by Royal Stoke University Hospital Major Trauma Centre
Diary in Resuscitation completed by ED Consultant.
Data Co-ordinators pagers that receive Trauma Calls.
ED system search: Patients who were imaged & admitted.
Daily contact with relevant Wards: Notification of any trauma patients admitted.
Attend morning Orthopaedic/Neurosurgical case discussion meetings.
Liaise with Rehabilitation Co-ordinators re: Trauma patients seen on wards
When eligible cases identified: Early care data collected on forms by TNC & Data coordinators whilst still inpatient.
Later care data (Operation, ICU, Imaging, Ward, Discharge data) taken from online systems.

System 2: Live Data capture: AdvantagesEmployed by Royal Stoke University Hospital Major Trauma Centre
Very little backlog; patients often dispatched to TARN day after discharge.
Case notes only required for “missed” cases identified post discharge.
Regular communication between Coordinators & Clinicians.
Rehabilitation Co-ordinators involved very early on.
Deaths data: Available from Bereavement office quickly, no waiting for inquest.

System 2: Live Data capture: Disadvantages Employed by Royal Stoke University Hospital Major Trauma Centre
Greater staff resource required
Post discharge ICD10 report required to capture “missed” patients.

Collecting the data
Retrospective Data Entry: Post discharge
Access to electronic Imaging and Theatre systems required
Enter data directly from notes or use Pro-forma
CORE PROFORMA IN REPORTS SECTION OF WEBSITE
DO NOT have to start and finish a submission in one session

Quality Assurance
Data Completeness (quantity)
& Data Accreditation (quality)

Data completeness % Measure of Expected v Submitted number of cases
HES Data used to calculate expected no. of cases per Trust
HES = Hospital Episode Statistics database
HES data contains ICD10 codes assigned by Trusts in previous year: 2013
TARN Inclusion criteria applied to HES data
No. of Expected cases then derived
Expected number of cases used as a guide only. Not a 100% target!
All eligible cases should be submitted to TARN
Data completeness %Measure of Expected v Submitted number of cases
% of expected v submitted cases shown on TARN website
Updated every 4 months: End of March July November
Shown as Trust and individual Hospital figures
Should always be viewed alongside Hospital Survival rate

Data Completeness calculation
Data Completeness
76.1%
Submissions: NUMERATOR 238
Expected submissions: DENOMINATOR 313
Data completeness 76.1%
HES dataset/Denominator
TARN submissions/Numerator
1-49%: May not reflect true practice50-79%: May not reflect true practice80%+: View with confidence

Improving Data completeness
HES v TARN 2013 Data comparison exercise

HES v TARN 2013 comparison exercise Comparison spreadsheet produced:
Green: Cases appear in both datasets (Submission ID shown) Black: Cases appear in HES dataset only (not submitted in TARN)
‘Not TARN eligible’ field: Completed by Trust & Fed-back to TARN Missing cases: Issues identified & entered: Increase in Numerator
Ineligible cases: Removed from expected no. of cases: Decrease in Denominator

HES v TARN 2013 comparison exercise results
Commonly missed groups: Aged 65+ Hip fractures with other (non hand or foot) fracture Traumatic SDH admitted to medical wards Aged 65+ Pelvic fractures Spinal fractures Patients whose LOS is exactly 3 days
Common reasons for the variance between the HES and TARN: Inaccuracies in ICD10 coding Old injuries being coded. Use of NOS (Not Specified) codes, which varies from trust to trust Rehabilitation only admissions Elective admissions
45 Trust participated in exercise >3,700 cases removed from Expected no. of cases 18% reduction & comparable Data Collection increase

Data Accreditation % (quality)Measure of frequency of CORE data field completion
CURRENT ACCREDITATION FIELDSGlasgow Coma Score or Intubation/ventilation
(Pre Hospital or ED)
Incident or Call 999 Date/time
Arrival time
Transfer: Reason & Date of Referral
CT time
Operation: Start time, grade & speciality of surgeon & grade of anaesthetist
ED Doctors: Time seen, grade & speciality
Injury detail – proportion of NFS codes

NEW ADDITIONS TO ACCREDITATION FIELDS*Pre-existing conditions
**Pupil reactivity for patients with AIS 3+ (Serious) head injuries
Data Accreditation%: Recent additionsFrom December 2014 onwards
* New Probability of Survival (Ps)14 model‘Other’ and ‘Not Known’ detrimental to Data Accreditation
** Future Probability of Survival model
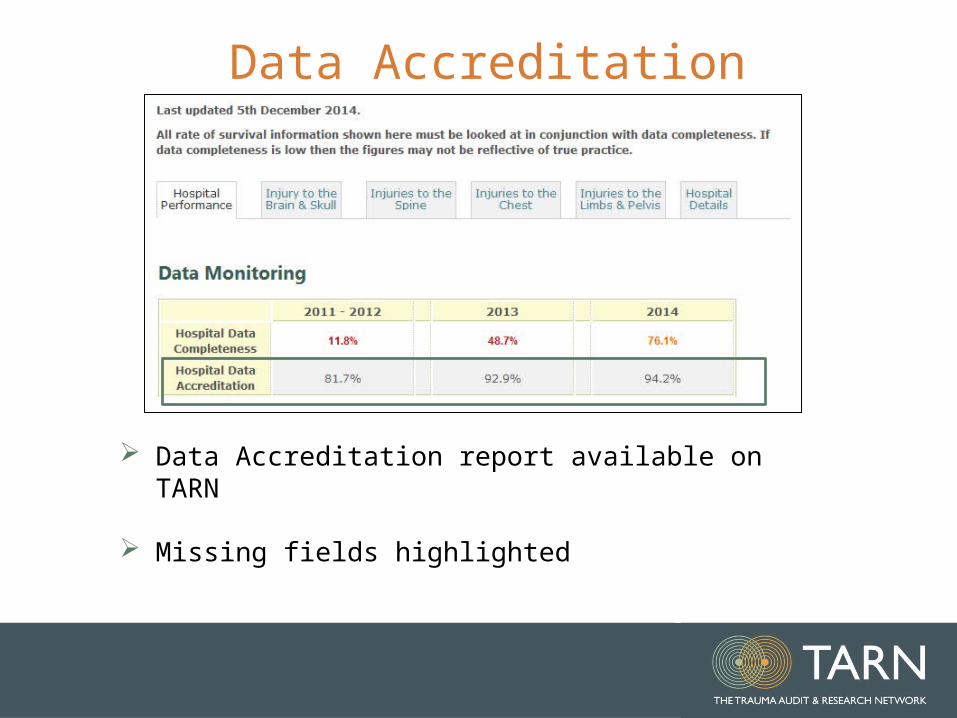
Data Accreditation
Data Accreditation report available on TARN
Missing fields highlighted

Questions?














![MAGIK: Managing Completeness of Data · Completeness is a central aspect of data quality which only re-cently has received increased attention in research (cf. [1, 2]) In particular,](https://static.fdocuments.net/doc/165x107/5fd7b827f1cd553eee1ba8c2/magik-managing-completeness-of-data-completeness-is-a-central-aspect-of-data-quality.jpg)



