Icsi preparation
64
‘ ‘ Preparation of Preparation of patients for ICSI: patients for ICSI: an evidence –based an evidence –based approach’ approach’ Dr. Ahmed Abd El Aziz Dr. Ahmed Abd El Aziz Professor of Gynecology and Professor of Gynecology and Obstetrics Obstetrics Alexandria University Alexandria University
-
Upload
nermine-amin -
Category
Health & Medicine
-
view
89 -
download
0
Transcript of Icsi preparation
‘‘Preparation of Preparation of patients for ICSI: patients for ICSI:
an evidence –based an evidence –based approach’approach’
Dr. Ahmed Abd El Aziz Dr. Ahmed Abd El Aziz Professor of Gynecology and Professor of Gynecology and
Obstetrics Obstetrics Alexandria UniversityAlexandria University
Alexandria Alexandria (c. 300 B.C.)(c. 300 B.C.)
ART ART are sometimes misused to are sometimes misused to treat incompletely-evaluated treat incompletely-evaluated patients.patients.
The rising pregnancy rates for The rising pregnancy rates for ICSI may reflect a change in ICSI may reflect a change in patient selection criteriapatient selection criteria and not and not just an improvement in ART.just an improvement in ART.
Investigations of infertile coupleInvestigations of infertile couple Evidence Medicine Based Era Evidence Medicine Based Era
National Evidence-Based Clinical Guidelines“Assessment and treatment for people with fertility problems
developed by the National Collaborating Centre forWomen and Children's Health on behalf of
the National Institute for Clinical Excellence (NICE)”February 2004
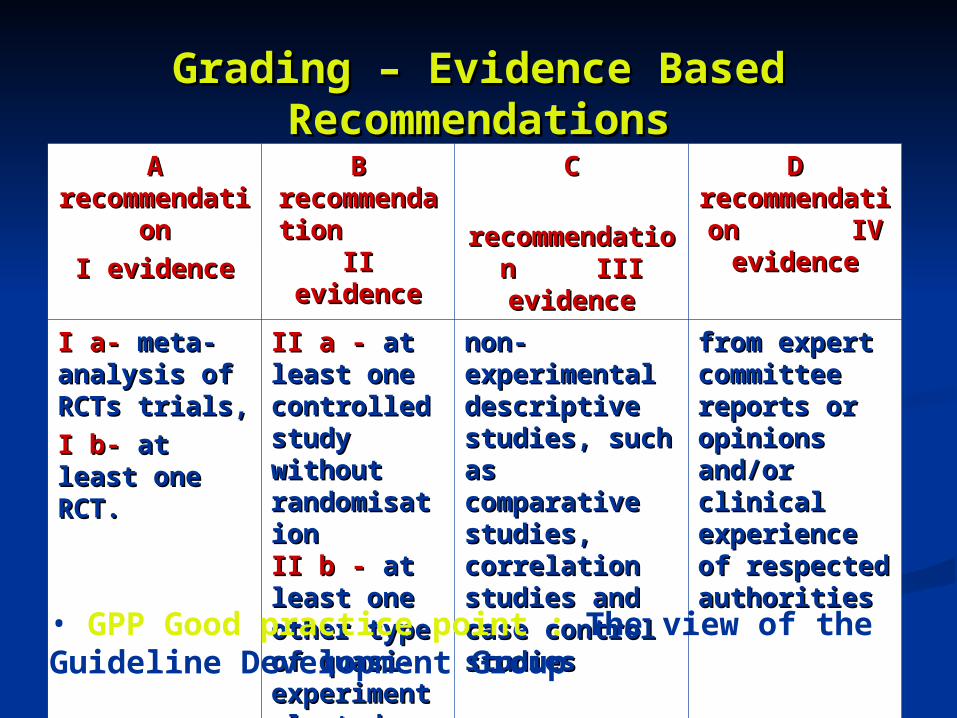
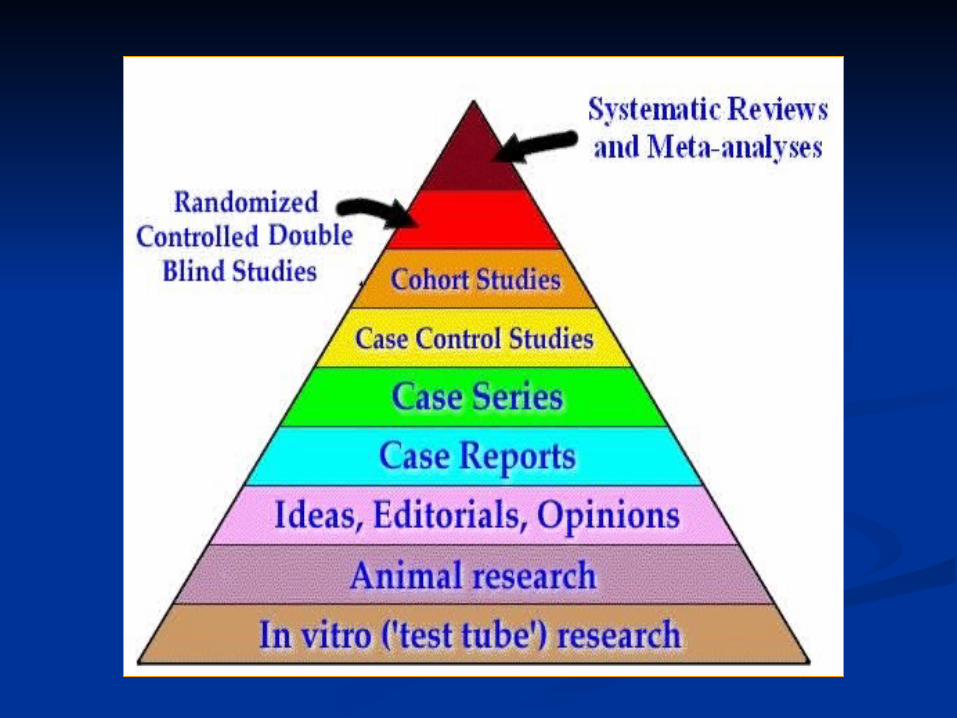
Grading – Evidence Based RecommendationsGrading – Evidence Based RecommendationsA A
recommendationrecommendationI evidenceI evidence
B B recommendatiorecommendation II evidencen II evidence
CC recommendation recommendation
III evidenceIII evidence
D D recommendation recommendation
IV evidence IV evidence
I a-I a- meta-analysis meta-analysis of RCTs trials,of RCTs trials,I b- I b- at least one at least one RCT.RCT.
II a -II a - at least one at least one controlled study controlled study without without randomisation randomisation II b -II b - at least at least one other type one other type of quasi-of quasi-experimental experimental studystudy
non-experimental non-experimental descriptive studies, descriptive studies, such as such as comparative comparative studies, correlation studies, correlation studies and case studies and case control studiescontrol studies
from expert from expert committee reports committee reports or opinions and/or or opinions and/or clinical experience clinical experience of respected of respected authoritiesauthorities
• GPP Good practice point : The view of the Guideline Development Group
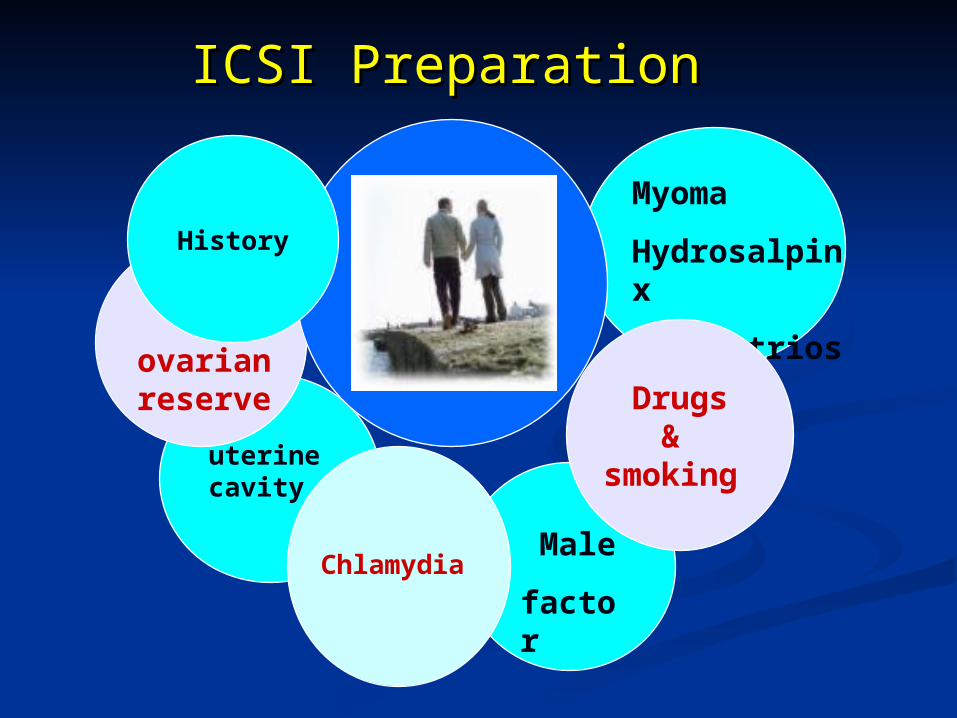
ICSI PreparationICSI Preparation
uterine cavity
ovarian reserve
Chlamydia
Myoma
Hydrosalpinx
Endometriosis
Male
factor
Drugs&
smoking
History
Centers for Disease Control and PreventionNational Center for
Chronic Disease Prevention and Health
PromotionDivision of Reproductive
HealthAtlanta, Georgia
American Society for Reproductive
MedicineSociety for Assisted
Reproductive Technology
Birmingham, Alabama
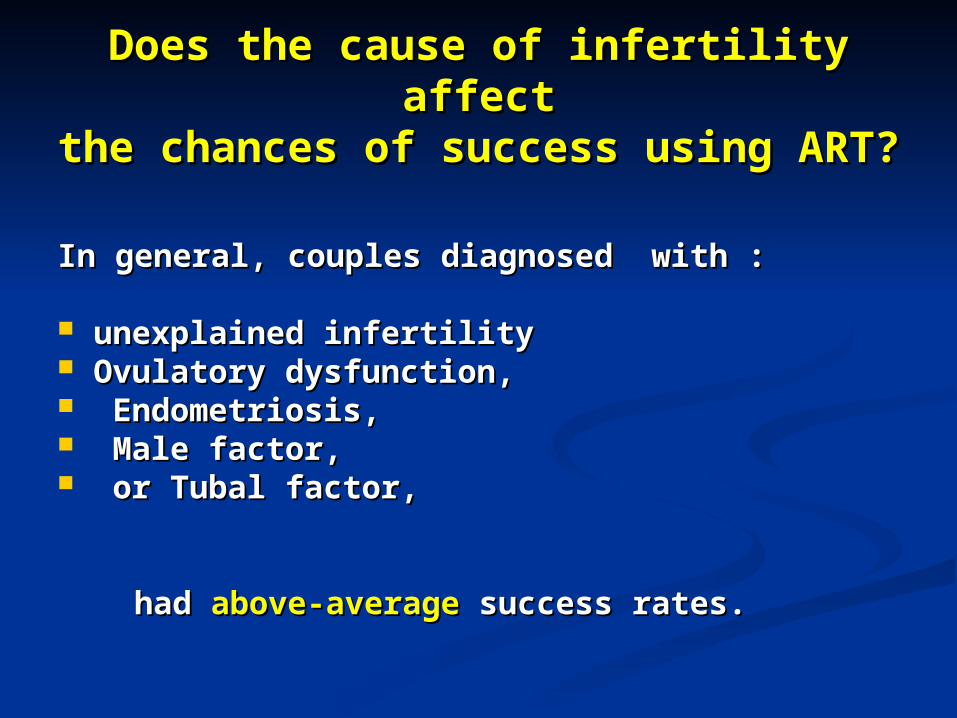
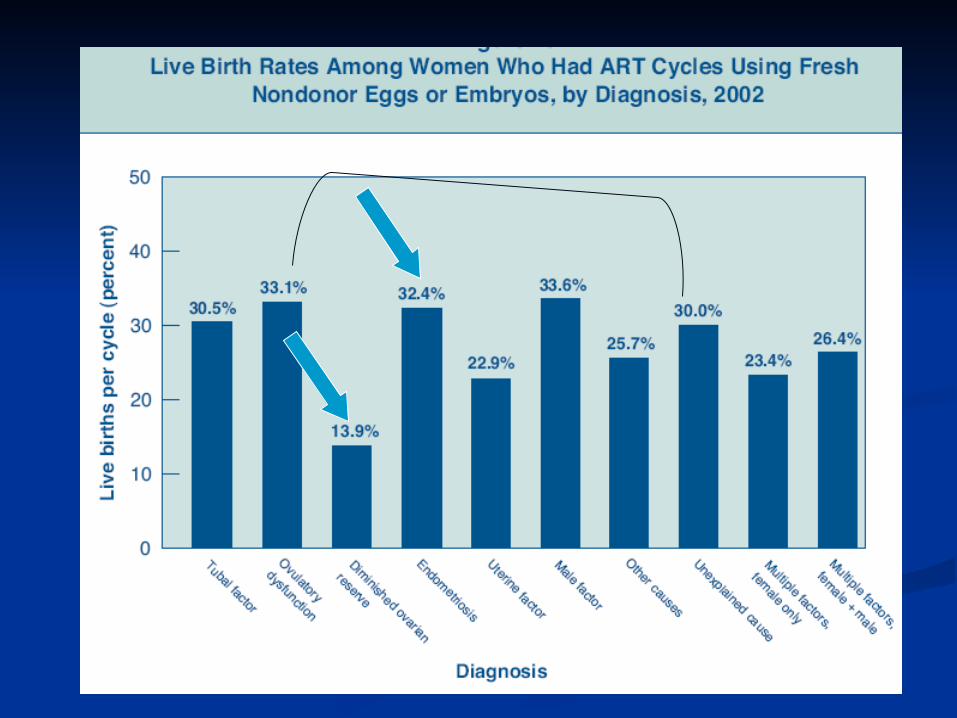
Does the cause of infertility affectDoes the cause of infertility affectthe chances of success using ART?the chances of success using ART?
In general, couples diagnosed with :In general, couples diagnosed with :
unexplained infertility unexplained infertility Ovulatory dysfunction,Ovulatory dysfunction, Endometriosis,Endometriosis, Male factor,Male factor, or Tubal factor, or Tubal factor,
had had above-averageabove-average success rates. success rates.
The The lowest success ratelowest success rate was was observed for those with observed for those with diminished ovarian reserve. [Age]diminished ovarian reserve. [Age]
Below-averageBelow-average success rate was in: success rate was in: uterine factor, uterine factor, ““other” causes, other” causes, or multiple infertility factorsor multiple infertility factors
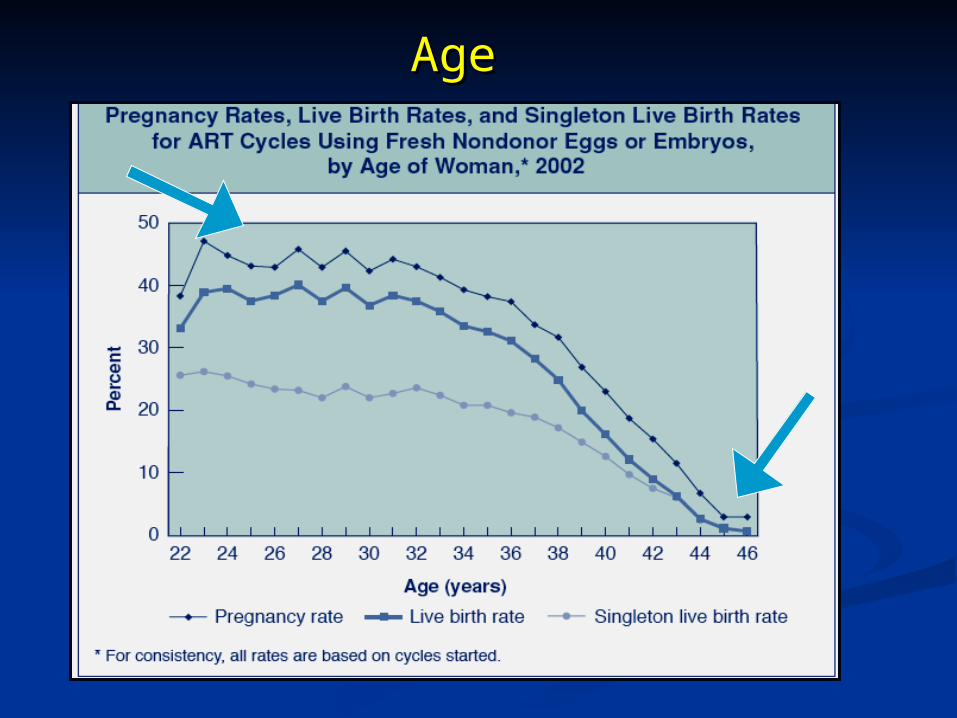
AgeAge
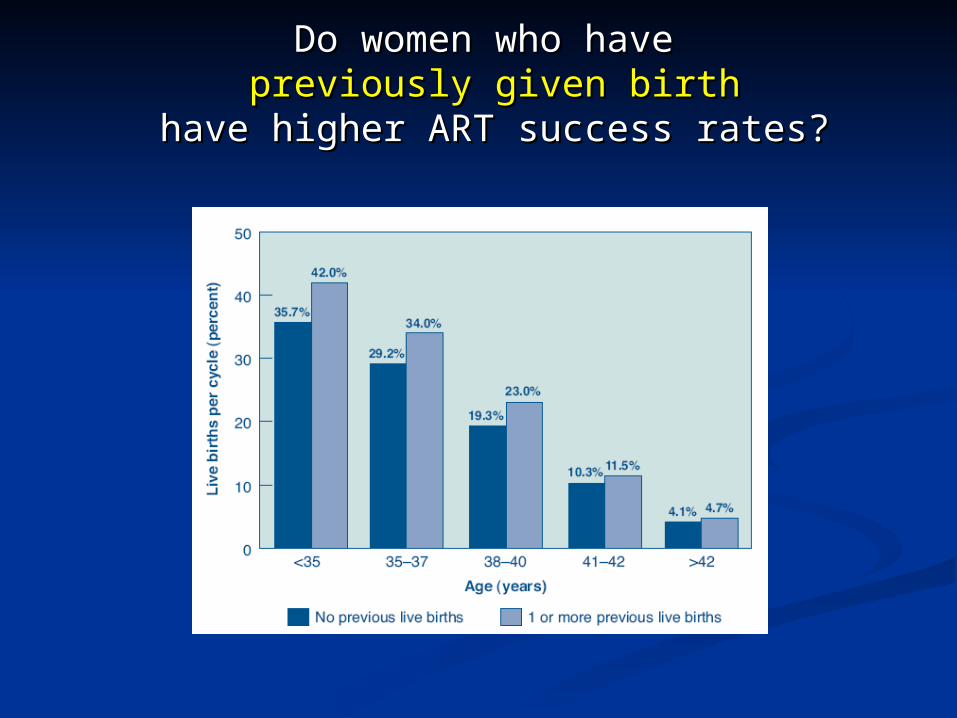
Do women who have Do women who have previously given birthpreviously given birth
have higher ART success rates?have higher ART success rates?
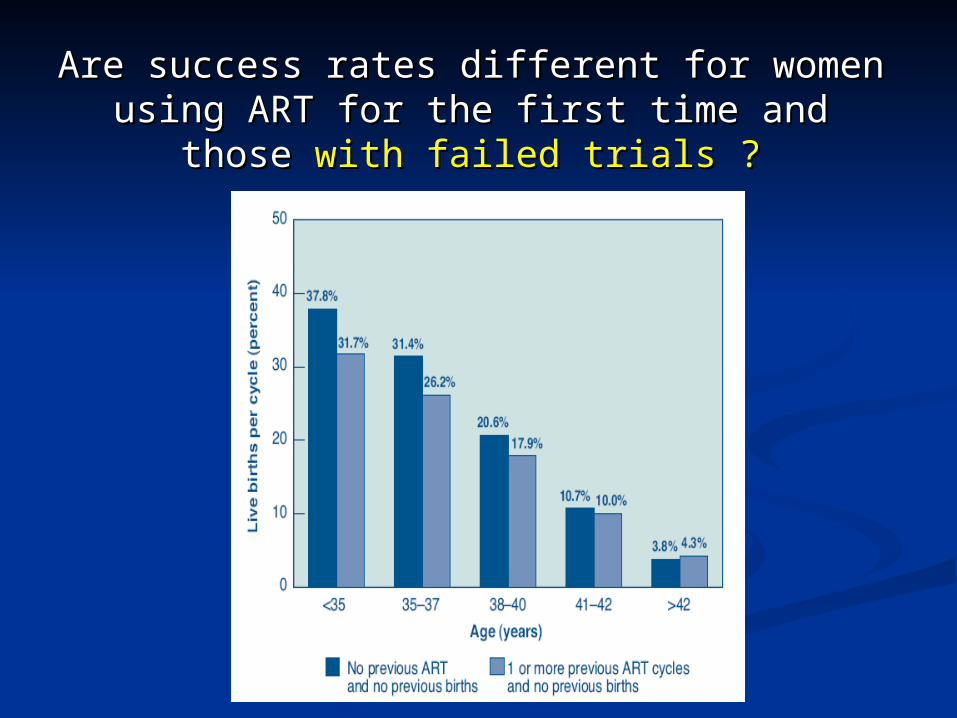
Are success rates different for womenAre success rates different for womenusing ART for the first time and those using ART for the first time and those with with
failed trials ?failed trials ?
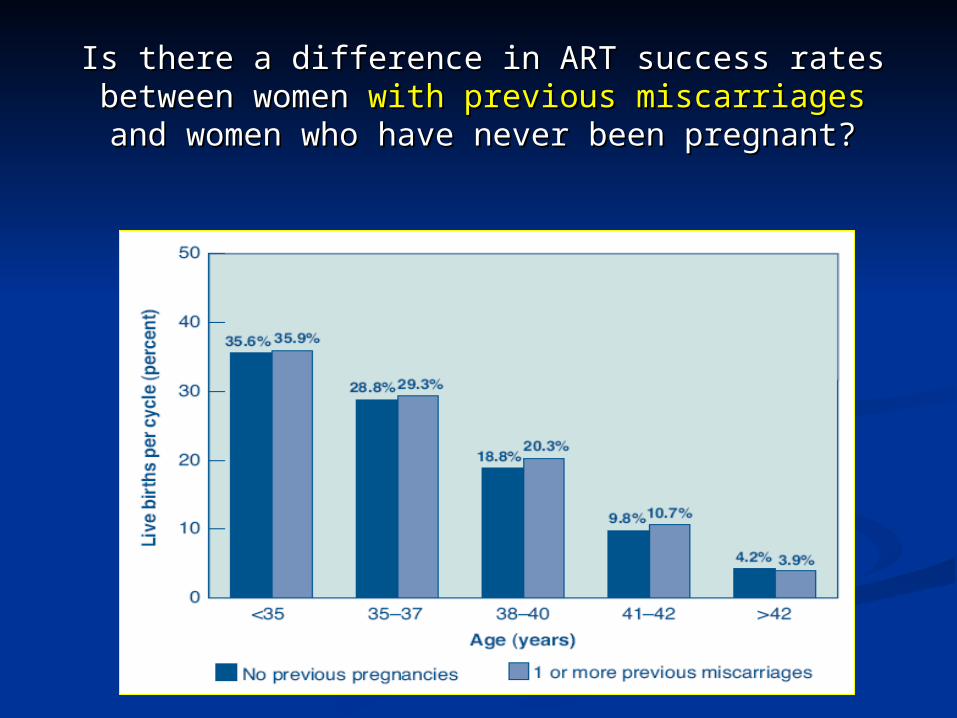
Is there a difference in ART success ratesIs there a difference in ART success ratesbetween women between women with previous miscarriageswith previous miscarriagesand women who have never been pregnant?and women who have never been pregnant?
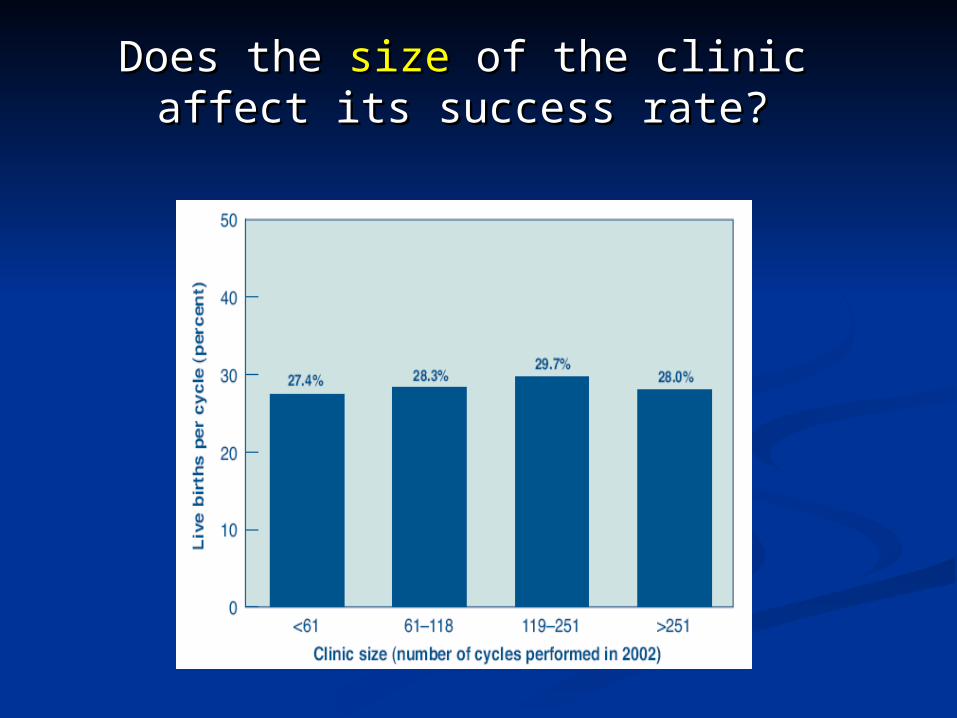
Does the Does the sizesize of the clinic affect its of the clinic affect its success rate?success rate?
Ovarian ReserveOvarian Reserve 1-Day 3 (FSH) and Estradiol 2. Basal Antral follicles Count by US 3. Serum AMH . 4.Intra-ovarian vascularity by Intra-ovarian vascularity by
doppler USdoppler US 5. ovarian volume5. ovarian volume
Day 3 (FSH) and EstradiolDay 3 (FSH) and Estradiol Day 3 FSH values Day 3 FSH values > 15> 15 microIU/LmicroIU/L ;carry a poor potential. ;carry a poor potential.
Day 3 FSH values Day 3 FSH values < 10 microIU/L< 10 microIU/L represent normal represent normal follicular potential (especially if day 3 estradiol values are follicular potential (especially if day 3 estradiol values are less than 40 pg/mL).less than 40 pg/mL).
Values Values between 10 to 15 microIU/Lbetween 10 to 15 microIU/L probably represent an probably represent an effect of aging on fecundity. effect of aging on fecundity.
class: D Evidence.class: D Evidence.
It is possible that It is possible that deficient intra-deficient intra-ovarianovarian vascularity vascularity may serve as the may serve as the initial markerinitial marker of reduced ovarian of reduced ovarian reserve which precedes an increased reserve which precedes an increased FSH level and reduction of the ovarian FSH level and reduction of the ovarian volume .volume .
(Engmann (Engmann et alet al., 1999 ). ., 1999 ).
Ovarian ReserveOvarian Reserve
Ovarian ReserveOvarian Reserve
A mean A mean ovarian volume of <3 cm3ovarian volume of <3 cm3 have a poor response to have a poor response to exogenously applied stimuli.exogenously applied stimuli.
(Syrop (Syrop et alet al., 1995).., 1995).
Assessment of the uterine cavityAssessment of the uterine cavity Any lesion of the Any lesion of the
uterine cavity should be uterine cavity should be treated priortreated prior to an IVF to an IVF cycle to optimize cycle to optimize reproductive success. reproductive success.
This would includeThis would include submucosal myomas, submucosal myomas, endometrial polyps, a endometrial polyps, a uterine septum, and uterine septum, and intracavitary adhesions. intracavitary adhesions.
The most popular techniques used to identify lesions in the uterine
cavity
Hysterosalpingography (HSG),
Hysteroscopy
3D Ultrasound

HysterosalpingogramHysterosalpingogram
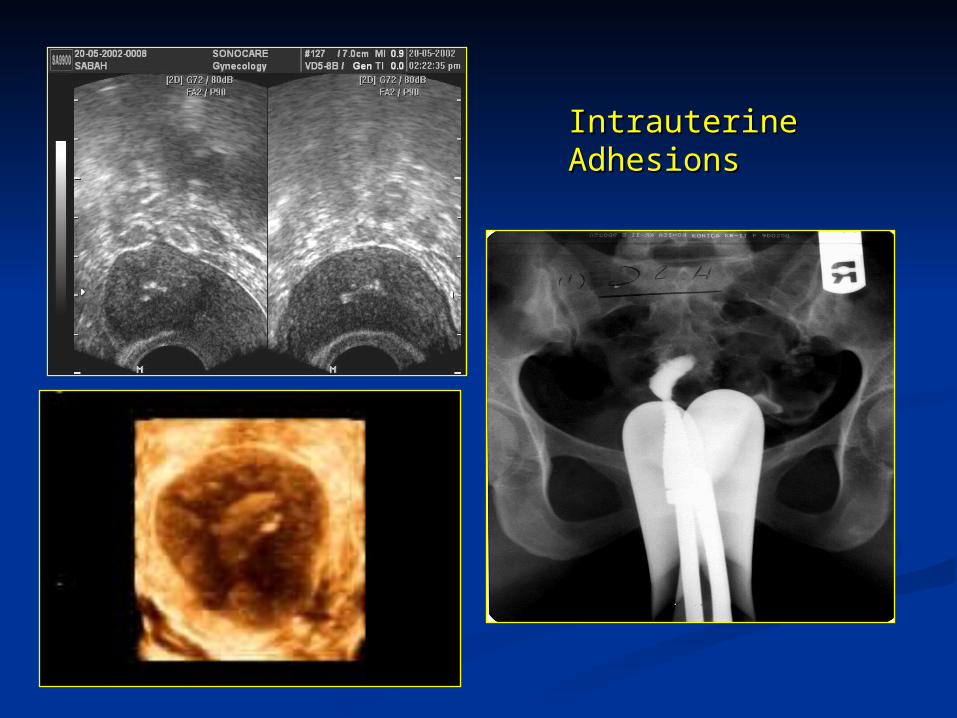
Intrauterine Intrauterine AdhesionsAdhesions
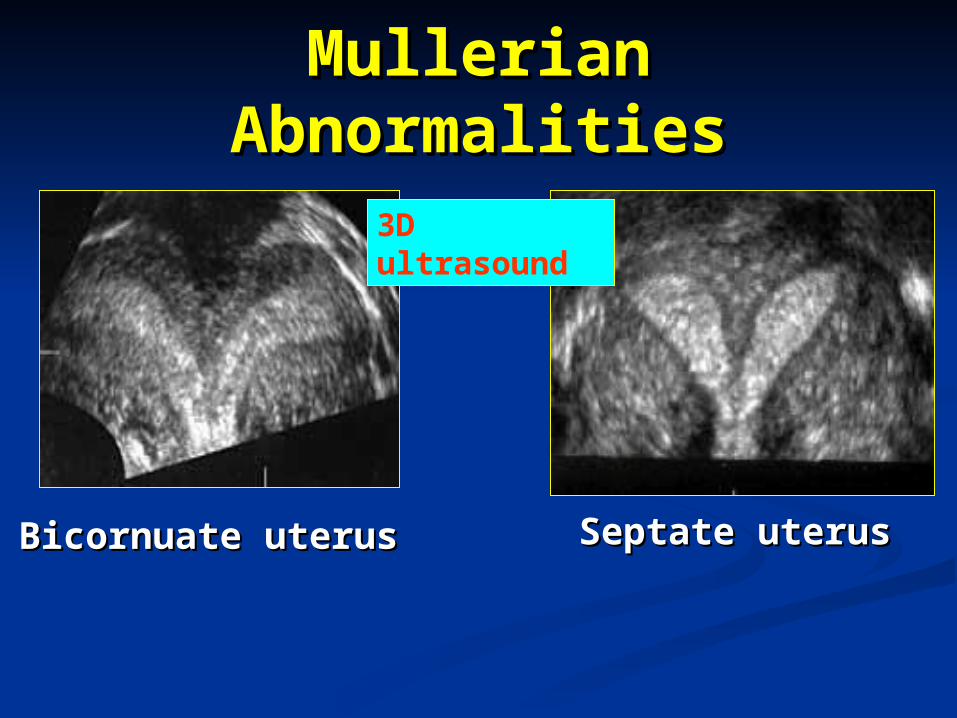
Mullerian Mullerian AbnormalitiesAbnormalities
Bicornuate uterusBicornuate uterus Septate uterus Septate uterus
3D ultrasound
The routine performance of a pelvic ultrasound scan to establish ovarian (and uterine) morphology is a useful tool to identify women with risk factors for pregnancy loss .
RCOG Guidelines : Grade C Recommendation
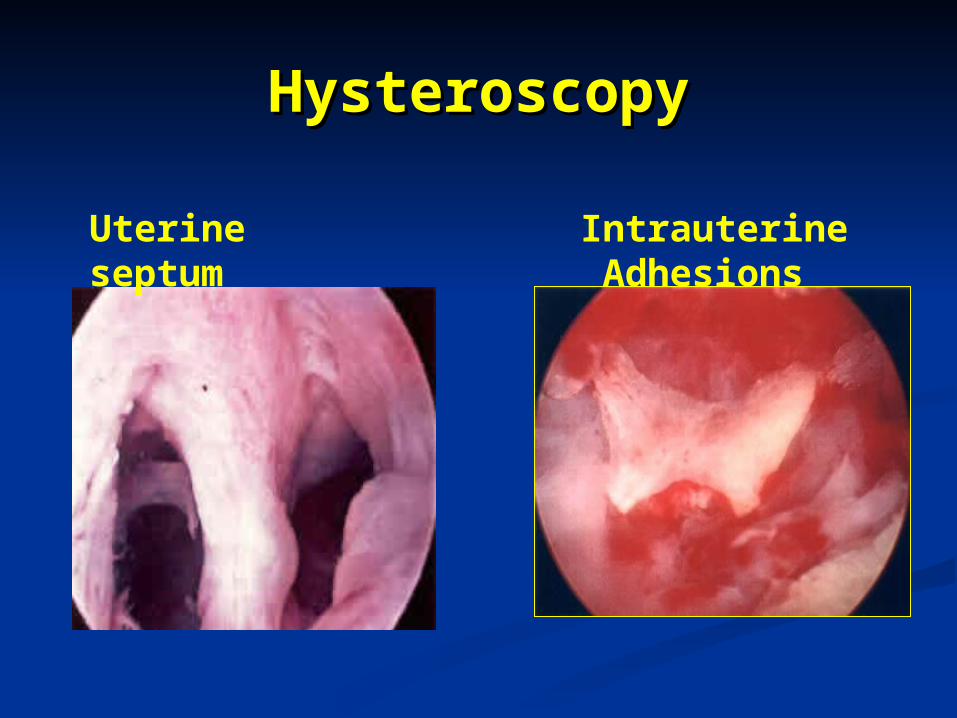
HysteroscopyHysteroscopy
Intrauterine Adhesions Uterine septum
Uterine cavityUterine cavity Women should not be offered
hysteroscopy on its own as part of the initial investigation unless clinically indicated, because the effectiveness of surgical treatment of uterine abnormalities on improving pregnancy rates has not been established. .
RCOG Guidelines : Grade B Recommendation
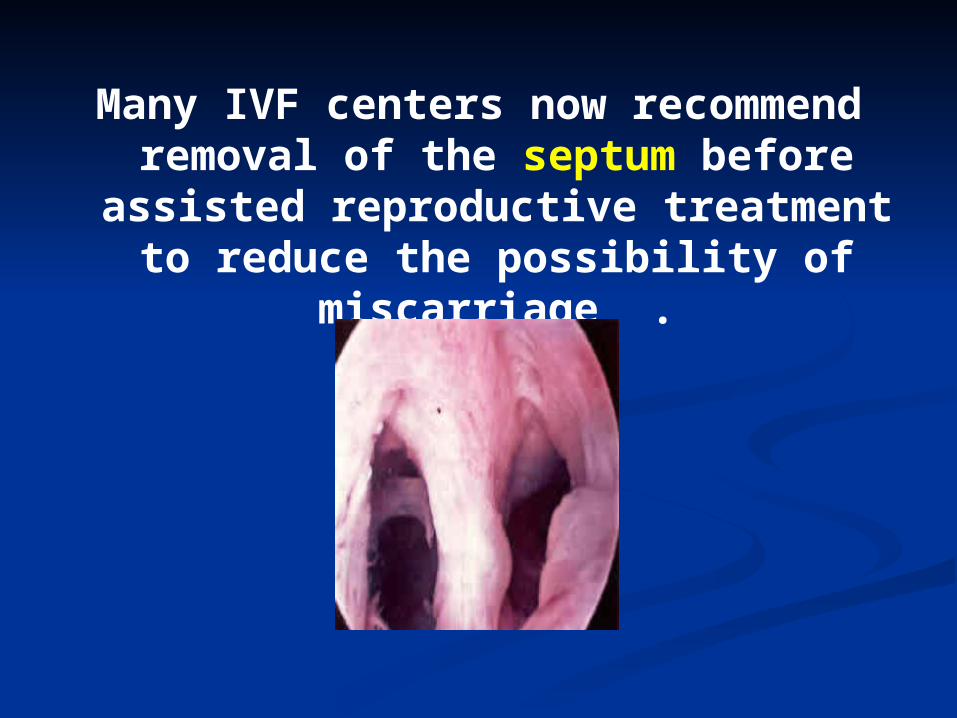
Many IVF centers now recommend removal of the septum before
assisted reproductive treatment to reduce the possibility of
miscarriage .
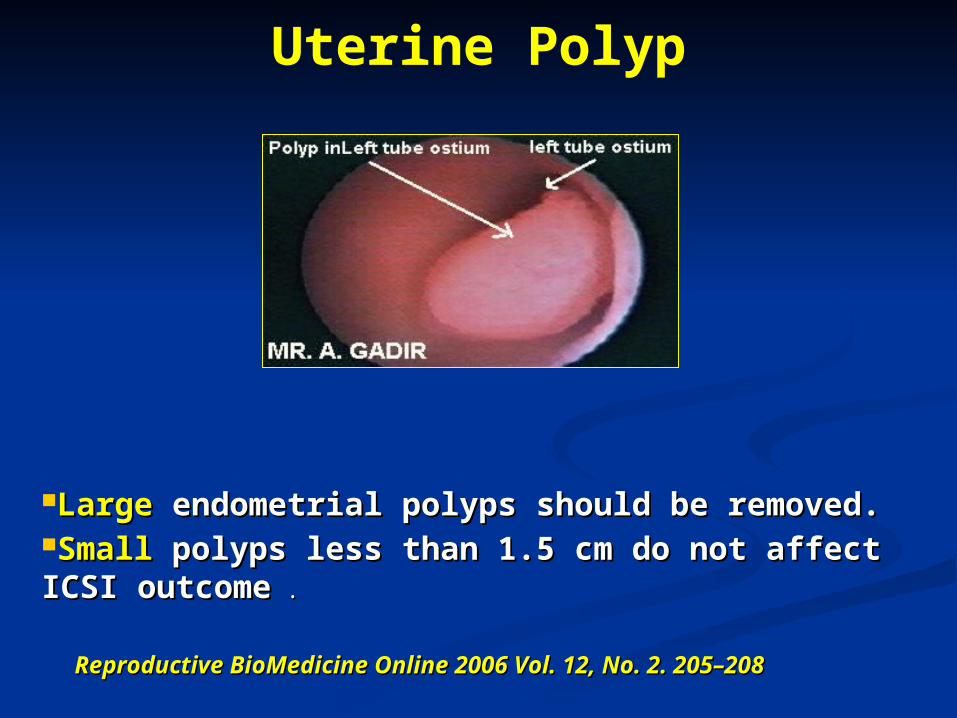
Uterine Polyp
Reproductive BioMedicine Online 2006 Vol. 12, No. 2. 205–208Reproductive BioMedicine Online 2006 Vol. 12, No. 2. 205–208
Large Large endometrial polyps should be removed.endometrial polyps should be removed.Small Small polyps less than 1.5 cm do not affect ICSI polyps less than 1.5 cm do not affect ICSI outcomeoutcome . .
Endometrial receptivity Good Good endometrial and subendometrial endometrial and subendometrial
blood flowblood flow assessed by transvaginal assessed by transvaginal Color DopplerColor Doppler before ET is indicative of before ET is indicative of good endometrial receptivity.good endometrial receptivity.
Poor blood flowPoor blood flow [old women] represents [old women] represents a bad uterine environment. a bad uterine environment.
(Chien LW , et al 2002 , prospective clinical study. 600 patients undergoung ICSI , FOR PREGNANCY RATE )
Chlamydial infectionChlamydial infection Women without Chlamydia
trachomatis antibodies have higher implantation rates, higher pregnancy rates, fewer early abortions, and more normal deliveries .
Women with Chlamydia trachomatis antibodies should be treated before an IVF cycle to give higher pregnancy rates.
TuberculosisTuberculosis
Anti-bacterial treatment of pelvic Anti-bacterial treatment of pelvic tuberculosis prior to IVF tuberculosis prior to IVF increases the success rate; increases the success rate; provided that the tuberculous provided that the tuberculous process has not destroyed the process has not destroyed the endometriumendometrium..
Alcohol, smoking and Alcohol, smoking and caffeine caffeine consumption consumption reduces the success rate reduces the success rate of ICSI .of ICSI .
RCOG Guidelines : Grade C Recommendation
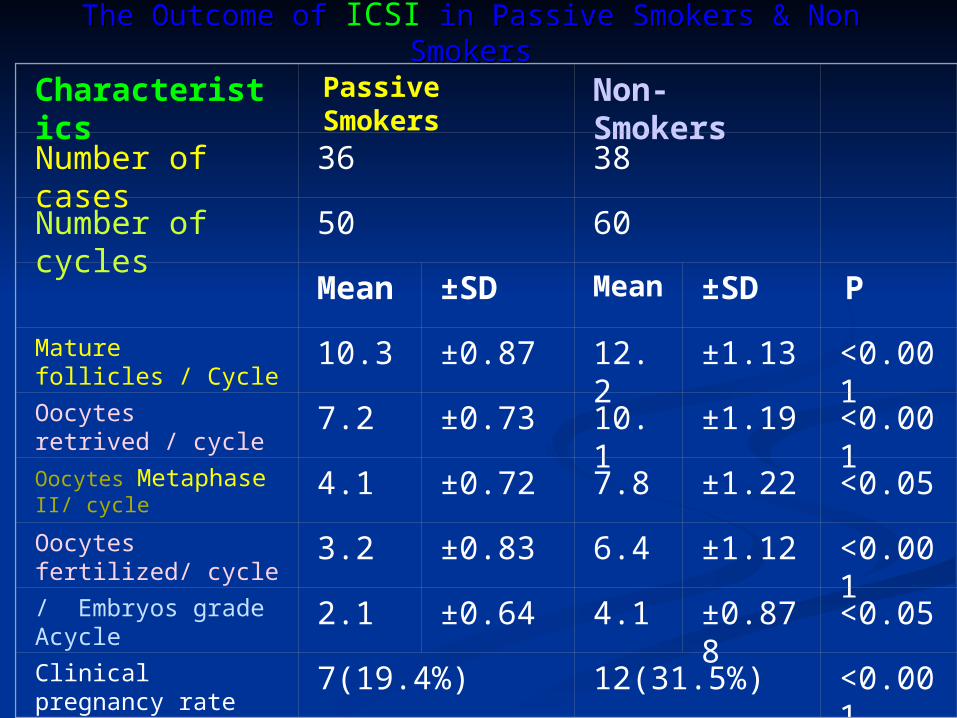
Characteristics Passive Smokers Non-Smokers
Number of cases 36 38
Number of cycles 50 60
Mean ±SD Mean
±SD P
Mature follicles / Cycle 10.3 ±0.87 12.2 ±1.13 <0.001
Oocytes retrived / cycle
7.2 ±0.73 10.1 ±1.19 <0.001
Oocytes Metaphase II/ cycle
4.1 ±0.72 7.8 ±1.22 <0.05
Oocytes fertilized/ cycle 3.2 ±0.83 6.4 ±1.12 <0.001
/ Embryos grade Acycle 2.1 ±0.64 4.1 ±0.878 <0.05
Clinical pregnancy rate (%)
7(19.4%) 12(31.5%) <0.001
The Outcome of The Outcome of ICSI in Passive Smokers & Non in Passive Smokers & Non SmokersSmokers
Body weightBody weight
Body mass index [19–Body mass index [19–30 ]:30 ]:
is optimal for ICSI is optimal for ICSI success.success.
RCOG Guidelines : Grade B Recommendation
DrugsDrugs
1.1. Metformin .Metformin .2.2. Aspirin.Aspirin.3.3. Combined Aspirin and Combined Aspirin and
heparin.heparin.4.4. Luteal phase supportLuteal phase support . .
Metformin TherapyMetformin Therapy Metformin therapy Metformin therapy
improves improves ovarian ovarian stimulation and IVF stimulation and IVF outcomes in -outcomes in -resistant polycystic resistant polycystic ovarian syndrome ovarian syndrome (PCOS).(PCOS).
Jones Institute for Reproductive Medicine, USA , 2002
AspirinAspirin Low-dose aspirin Low-dose aspirin does notdoes not improve improve
ovarian responsiveness or ovarian responsiveness or pregnancy rate in IVF and ICSI pregnancy rate in IVF and ICSI patients: patients:
in a randomized, placebo-in a randomized, placebo-controlled double-blind study.controlled double-blind study.
(Päkkilä M(Päkkilä M , et al , et al Hum Reprod. 2005; 20(8):2211-4 )
Combined low dose Aspirin & Combined low dose Aspirin & HeparinHeparin increases success increases success rate in women with repeated rate in women with repeated IVF failures .IVF failures .
Pacific Fertility Medical Centers of Pacific Fertility Medical Centers of CaliforniaCalifornia ,20002000
luteal supportluteal supporthCG or progesteronehCG or progesterone is is
essential in women essential in women treated with treated with Gn-Rh Gn-Rh
agonists agonists during Ivf & during Ivf & ICSI cycles.ICSI cycles.
RCOG Guidelines : Grade A Recommendation
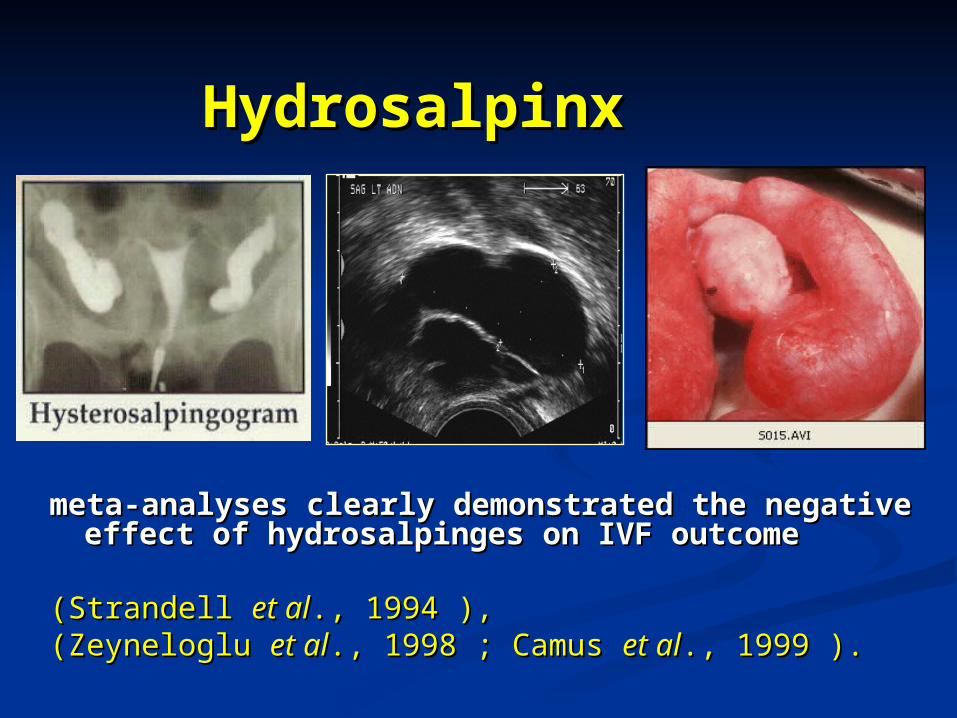
HydrosalpinxHydrosalpinx
meta-analyses clearly demonstrated the negative meta-analyses clearly demonstrated the negative effect of hydrosalpinges on IVF outcome effect of hydrosalpinges on IVF outcome
(Strandell (Strandell et alet al., 1994 ),., 1994 ),(Zeyneloglu (Zeyneloglu et alet al., 1998 ; Camus ., 1998 ; Camus et alet al., 1999 ).., 1999 ).
Laparoscopic Laparoscopic salpingectomysalpingectomy
Should be considered for all Should be considered for all women with hydrosalpinx who women with hydrosalpinx who undergo IVFundergo IVF..
Johnson NP Mars ,2002. systematic review Johnson NP Mars ,2002. systematic review (Cochrane review)(Cochrane review)
Further research is requiredFurther research is required to to assess other pre-IVF surgical assess other pre-IVF surgical interventions,interventions, such as :such as :
needle aspiration of needle aspiration of hydrosalpinx fluid hydrosalpinx fluid
laparoscopic proximal tubal laparoscopic proximal tubal occlusionocclusion
laparoscopic salpingostomylaparoscopic salpingostomy
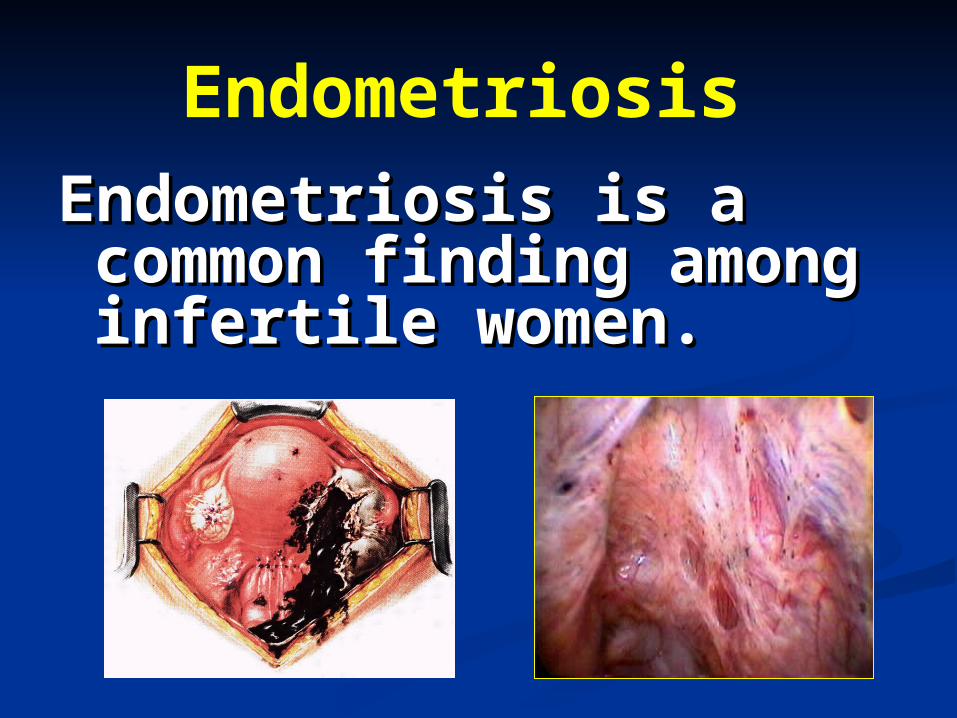
Endometriosis Endometriosis is a Endometriosis is a common finding common finding among infertile among infertile women. women.
Management of Management of endometriosis-associated endometriosis-associated
infertilityinfertility1.1. Surgical treatment Surgical treatment 2. Medical treatment2. Medical treatment
3. Combined medical and surgical therapy 3. Combined medical and surgical therapy 4. Controlled ovarian hyperstimulation +/- IUI4. Controlled ovarian hyperstimulation +/- IUI
5.5. Assisted reproductive techniquesAssisted reproductive techniques
EEndometriosisndometriosis : Mild : Mild Surgical ablation or , or , ovarian stimulation with IUI .ovarian stimulation with IUI .
RCOG Guidelines : Grade A Recommendation
EEndometriosisndometriosis :Moderate to :Moderate to SevereSevere
Surgical treatment may improve fertility .
RCOG Guidelines : Grade B Recommendation
Endometriosis
In more advanced stages of In more advanced stages of endometriosis, endometriosis, ART ART is the is the recommended treatment.recommended treatment.
The use of The use of GnRH agonistGnRH agonist during during stimulation further improves the stimulation further improves the outcome. outcome.
RCOG Guidelines : Grade A Recommendation
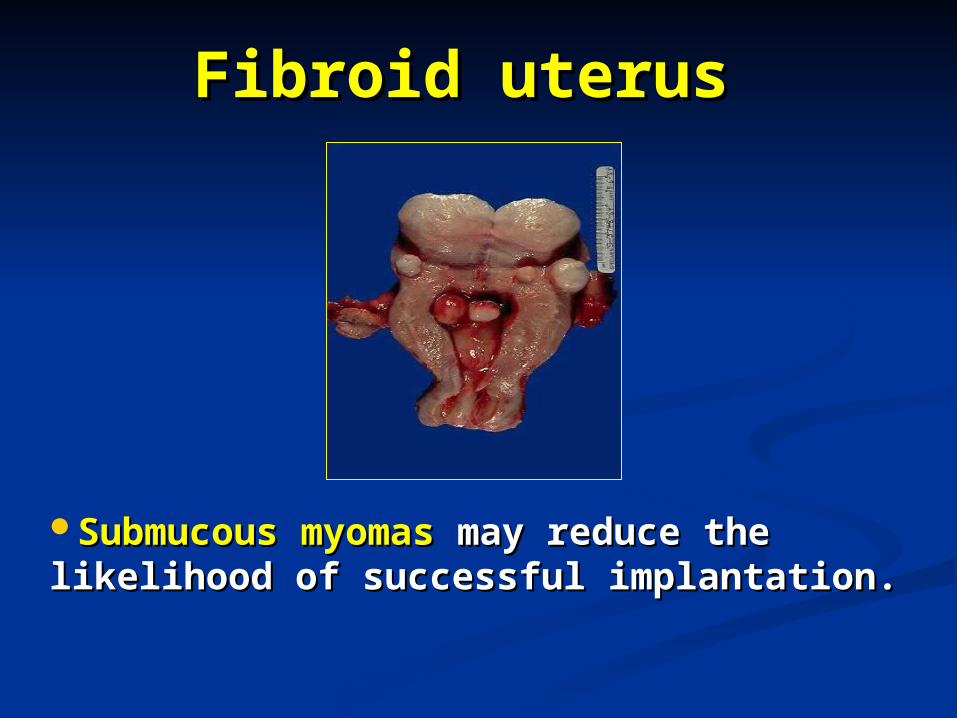
Fibroid uterusFibroid uterus
Submucous myomasSubmucous myomas may reduce the may reduce the likelihood of successful implantation.likelihood of successful implantation.
Fibroid uterusFibroid uterus Patients having Patients having subserosal or intramuralsubserosal or intramural
myomas of <4 cm not encroaching on the myomas of <4 cm not encroaching on the uterine cavity have IVF-ICSI outcomes uterine cavity have IVF-ICSI outcomes comparable to those of patients without comparable to those of patients without such leiomyomas. such leiomyomas.
Oliveira et al , fertil steril , 2004. BrazilOliveira et al , fertil steril , 2004. Brazil
Positive factorsPositive factors
1. Younger age of woman .1. Younger age of woman .2. History of previous pregnancy .2. History of previous pregnancy .3. History of recurrent miscarriage 3. History of recurrent miscarriage
..4. Non-smoker .4. Non-smoker .
Negative factorsNegative factors
1. Old age. 1. Old age.
2. Combined male and female 2. Combined male and female infertility .infertility .
3. Previous history of failed trials (3 3. Previous history of failed trials (3 or more cyclesor more cycles))
Negative factorsNegative factors 4. Uterine abnormality (DES, 4. Uterine abnormality (DES,
fibroids) fibroids) 5. Certain types of ovarian 5. Certain types of ovarian
dysfunction (High FSH level) .dysfunction (High FSH level) . 6. Hydrosalpinx .6. Hydrosalpinx .
Semen analysisSemen analysis
CASA is not superior to conventional semen analysis
RCOG Guidelines : Grade A Recommendation
Semen analysis
Abnormal Azospermia and severe oligospermia
Repeat after 3 monthsRepeat as soon as posible
RCOG Guidelines : Grade B Recommendation
Male SubfertilityOligo/asthenospermia
Gonadotrophin is effective in the treatment of male hypogonadotrophic hypogonadism,but ineffective in idiopathic male infertility.
RCOG Guidelines : Grade B Recommendation
Obstructive Obstructive AzoospermiaAzoospermia
Microsurgical correction of vas deferens occlusion and epididymal blockage can be considered .
RCOG Guidelines : Grade B Recommendation
ICSIICSIIntracytoplasmic sperm injection Intracytoplasmic sperm injection
(ICSI) is indicated in(ICSI) is indicated in SSevere deficits in semen quality evere deficits in semen quality OObstructivebstructive azoospermia . azoospermia . NNon-obstructive azoospermia . on-obstructive azoospermia . PPrevious IVF cycle revious IVF cycle withwith failed or failed or
very poor fertilisation. very poor fertilisation. RCOG Guidelines : Grade A Recommendation
Sperm aneuploidy frequency Sperm aneuploidy frequency and ICSIand ICSI
Increased frequency is associated with :Increased frequency is associated with : lower implantation rates lower implantation rates higher miscarriage rates.higher miscarriage rates.
Future development of methods to identify Future development of methods to identify genetically abnormal sperm may allow for genetically abnormal sperm may allow for better selection and improved ICSI outcomes. better selection and improved ICSI outcomes.
Nunziatina Burrello, et al .Human Reproduction, Vol. 18, No. 7, 1371-1376, July 2003
ICSI PreparationICSI Preparation
uterine cavity
ovarian reserve
Chlamydia
Myoma
Hydrosalpinx
Endometriosis
Male
factor
Drugs&
smoking
History

ICSI 3.mpg