ICH:n ennustetta parantavat hoitokeinot - neuro.fi · EPIDEMIOLOGIA. Meretoja 2017...
72
ICH:n ennustetta parantavat hoitokeinot Atte Meretoja
Transcript of ICH:n ennustetta parantavat hoitokeinot - neuro.fi · EPIDEMIOLOGIA. Meretoja 2017...

ICH:n ennustetta parantavat hoitokeinotAtte Meretoja
Meretoja 2017
SidonnaisuudetAtte Meretoja, LKT, MSc(StrokeMed), FRACP
• TYÖANTAJA– HUS, HYKS Pää- ja kaulakeskus, hallinnollinen ylilääkäri– University of Melbourne, Department of Medicine, Associate Professor
• MUU PÄÄTÖSVALLAN KÄYTTÖ– World Stroke Organisation: hallituksen jäsen– European Stroke Organisation: hallituksen jäsen
• YRITYSYHTEISTYÖ– Boehringer Ingelheim: puhujapalkkiot, matkakorvaukset, konsultointi– Stryker: puhujapalkkiot, matkakorvaukset, konsultointi

Meretoja 2017
EPIDEMIOLOGIA
Meretoja 2017
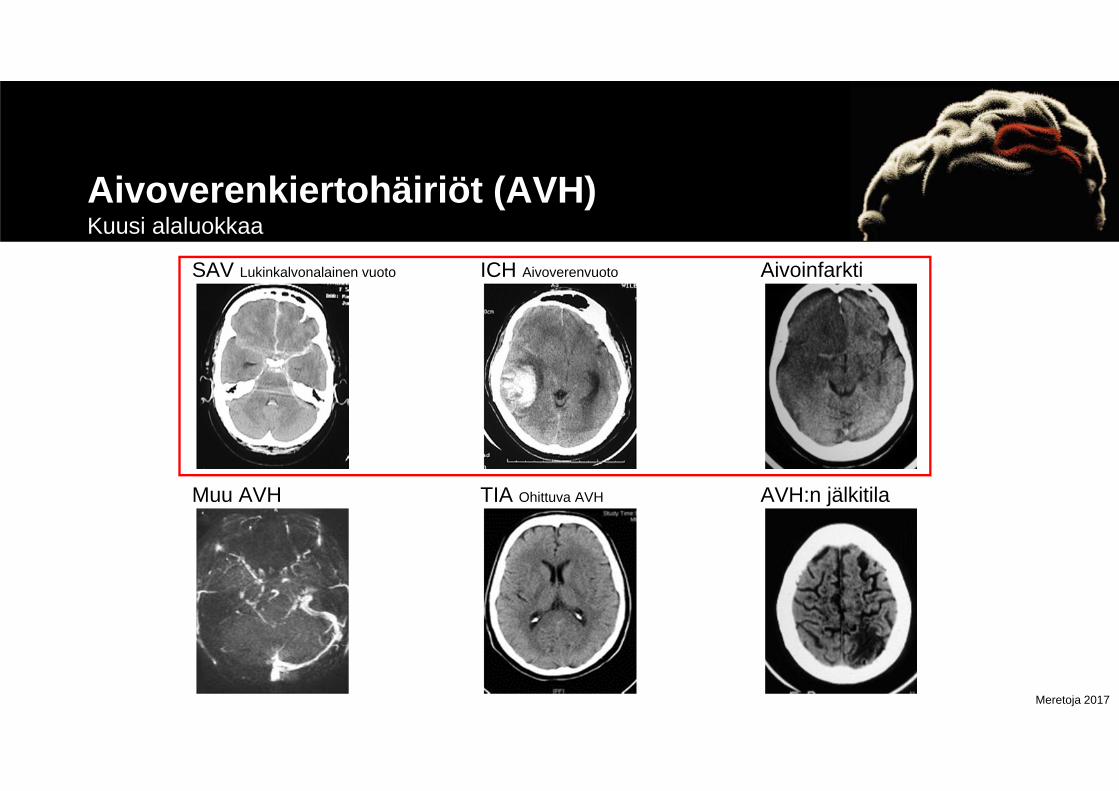
Aivoverenkiertohäiriöt (AVH)Kuusi alaluokkaa
SAV Lukinkalvonalainen vuoto ICH Aivoverenvuoto Aivoinfarkti
Muu AVH TIA Ohittuva AVH AVH:n jälkitila

Meretoja 2017
Mistä EI puhuta tänään
EPIDURAALIVUOTO SUBDURAALIVUOTO AIVOKONTUUSIO

Meretoja 2017
Vuonna 2016 kuoli 55 miljoonaa ihmistäNäistä 2,8 miljonaa aivoverenvuotoihin
Naghavi M, … Meretoja A, … Murray CJL. Global Burden of Disease 2016 Causes of Death Collaboration. Lancet 2017; 390: 1151–210.

Meretoja 2017
Vuonna 2016 menetettiin 2,4 miljardia DALYaNäistä 65 miljoonaa aivoverenvuotojen vuoksi
Hay SI, …, Meretoja A, …, Murray CJL. Global Burden of Disease 2016 DALY Collaboration. Lancet 2017; 390: 1260–344.
Meretoja 2017
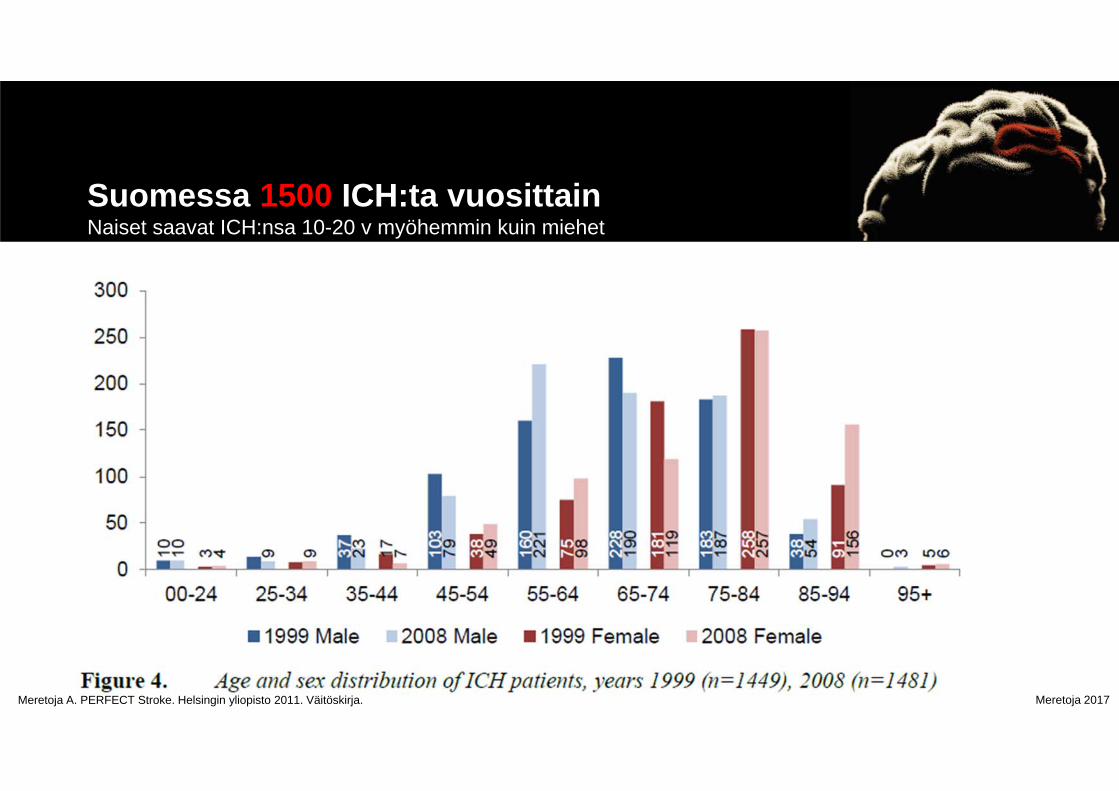
Suomessa 1500 ICH:ta vuosittain Naiset saavat ICH:nsa 10-20 v myöhemmin kuin miehet
Meretoja A. PERFECT Stroke. Helsingin yliopisto 2011. Väitöskirja.
Meretoja 2017
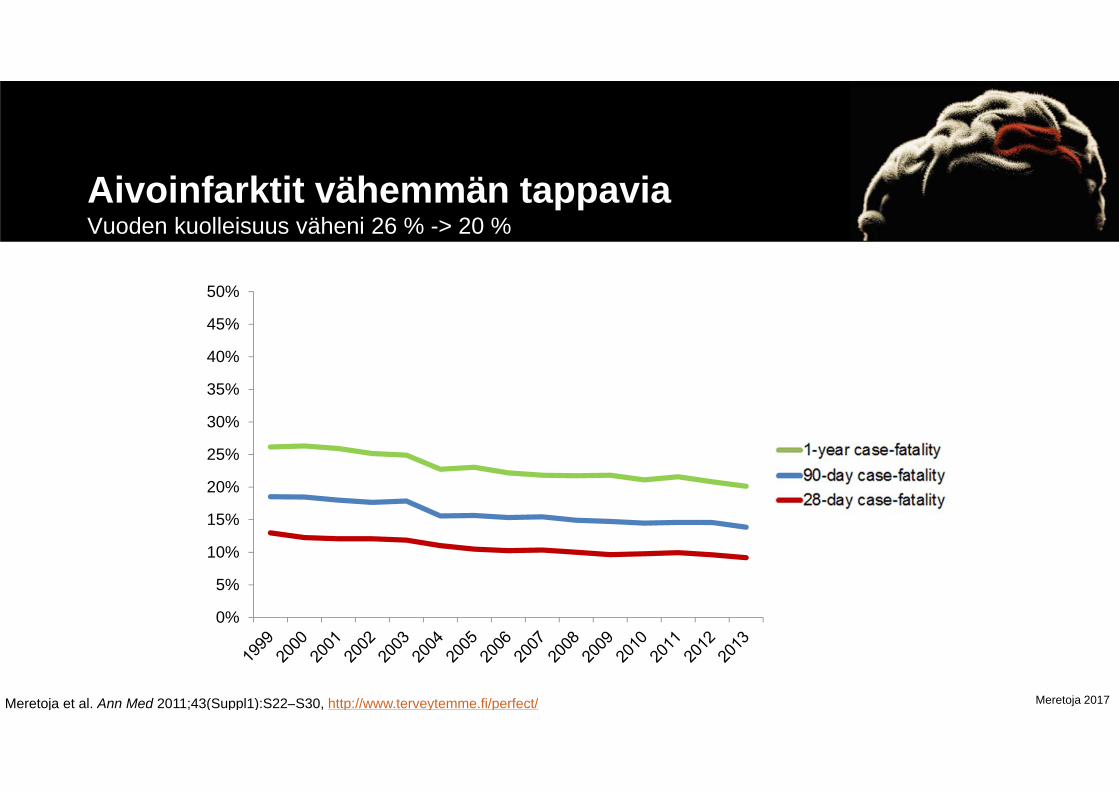
Aivoinfarktit vähemmän tappaviaVuoden kuolleisuus väheni 26 % -> 20 %
Meretoja et al. Ann Med 2011;43(Suppl1):S22–S30, http://www.terveytemme.fi/perfect/
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
28-day case-fatality90-day case-fatality1-year case-fatality

Meretoja 2017
Aivoverenvuodoissa – ei muutostaVuoden kuolleisuus 43 % -> 42 %
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
1-year case-fatality90-day case-fatality28-day case-fatality
Meretoja et al. Ann Med 2011;43(Suppl1):S22–S30, http://www.terveytemme.fi/perfect/

Meretoja 2017
ICH-kuolleisuus tasaista Suomessa 20 v aikana
050
100150200250300350400450500
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
Miehet Naiset
95 -85 - 9475 - 8465 - 7455 - 6445 - 54- 44
Suomen virallinen tilasto (SVT): Kuolemansyyt [verkkojulkaisu].ISSN=1799-5051. Helsinki: Tilastokeskus [viitattu: 24.10.2017].Saantitapa: http://www.stat.fi/til/ksyyt/

Meretoja 2017
HOITOHOITOSUOSITUKSET

Meretoja 2017
European Stroke Organisation GuidelinesSteiner et al. Int J Stroke 2014

Meretoja 2017
Class I Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015

Meretoja 2017
DIAGNOOSI JA ENNUSTEARVIO

Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusDiagnoosi ja ennustearvio
• Rapid neuroimaging with CT or MRI is recommended to distinguish ischemic stroke from ICH (Class I; Level of Evidence A). (Unchanged from the previous guideline)
• A baseline severity score should be performed as part of the initial evaluation of patients with ICH (Class I; Level of Evidence B).(New recommendation)
Meretoja 2017
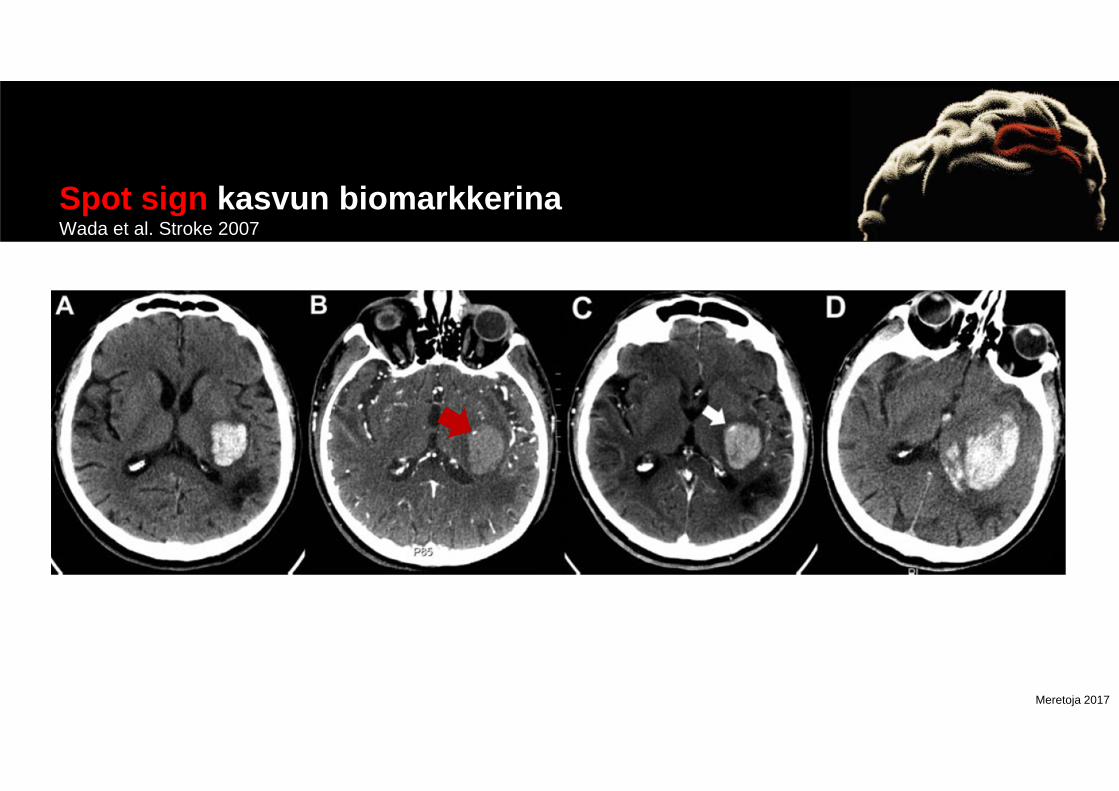
Spot sign kasvun biomarkkerinaWada et al. Stroke 2007

Meretoja 2017
Sekundaarinen etiologia neljäsosalla potilaistaSMASH-U Classification, n=1013
AVM/kavernooman=505 %
Systeemisairausn=485 %
Antikoagulaation=14314 %
Amyloidiangiopatian=20520 %
Hypertensiivinenangiopatian=35435 %
Määrittämätönn=21321 %
Meretoja et al. Stroke 2012;43(10):2592-2597.
Meretoja 2017
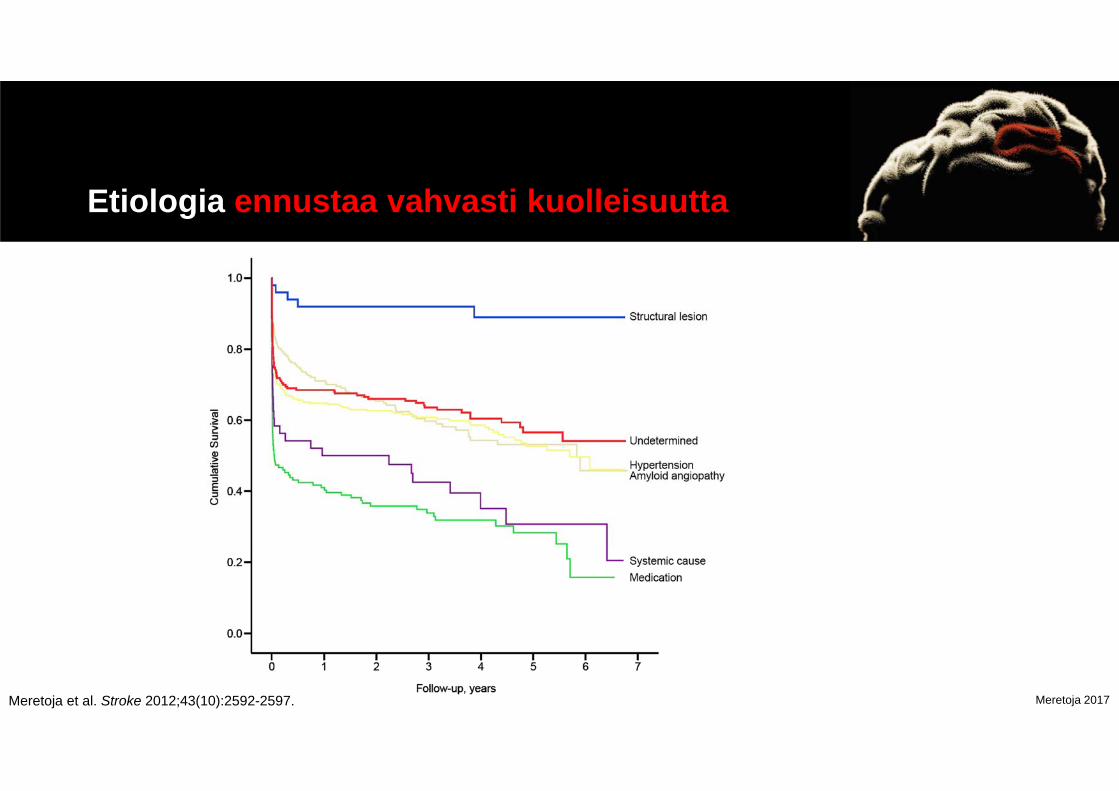
Etiologia ennustaa vahvasti kuolleisuutta
Meretoja et al. Stroke 2012;43(10):2592-2597.
Meretoja 2017
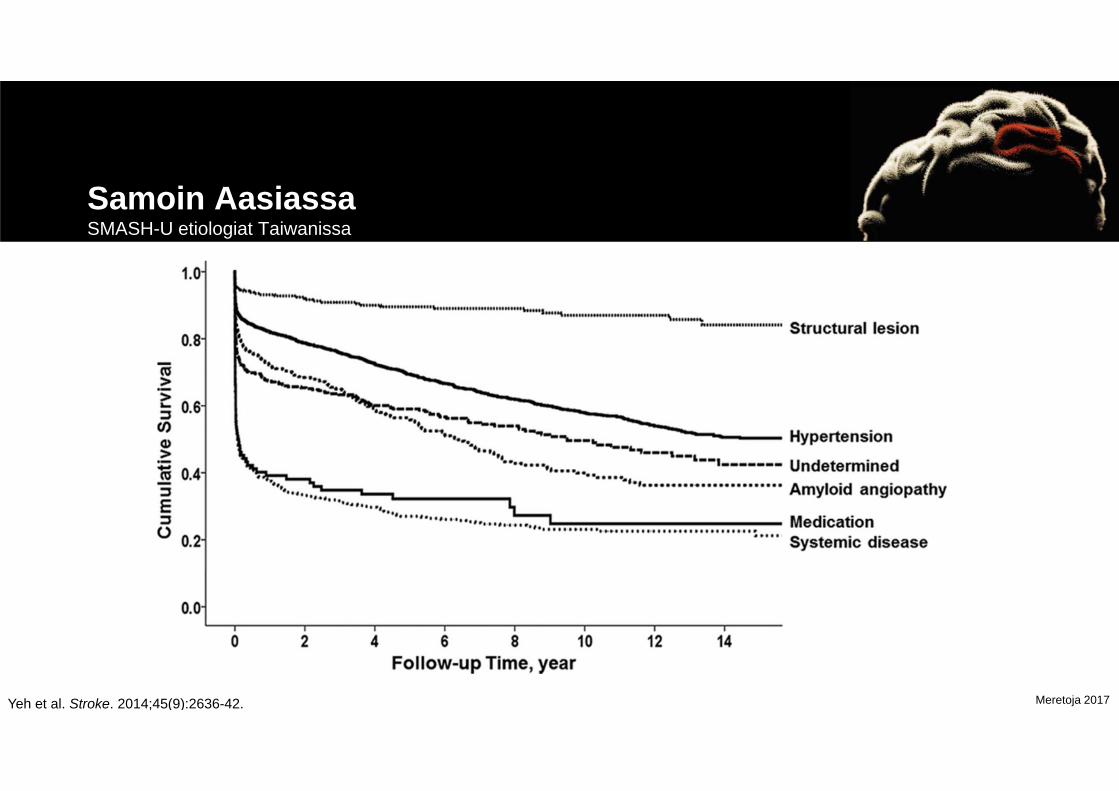
Samoin AasiassaSMASH-U etiologiat Taiwanissa
Yeh et al. Stroke. 2014;45(9):2636-42.
Meretoja 2017
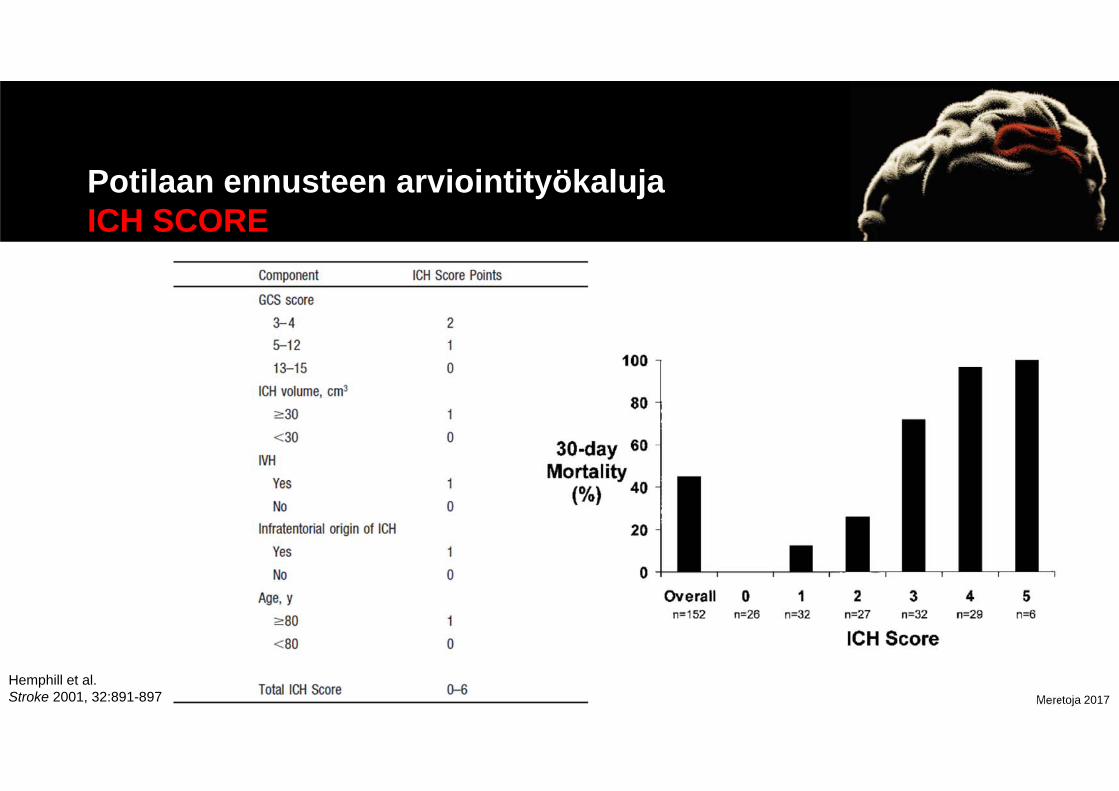
Potilaan ennusteen arviointityökalujaICH SCORE
Hemphill et al. Stroke 2001, 32:891-897

Meretoja 2017Satopää, Mustanoja, Meretoja et al. J Neurol Sci 2017;379:103–108.
Meretoja 2017
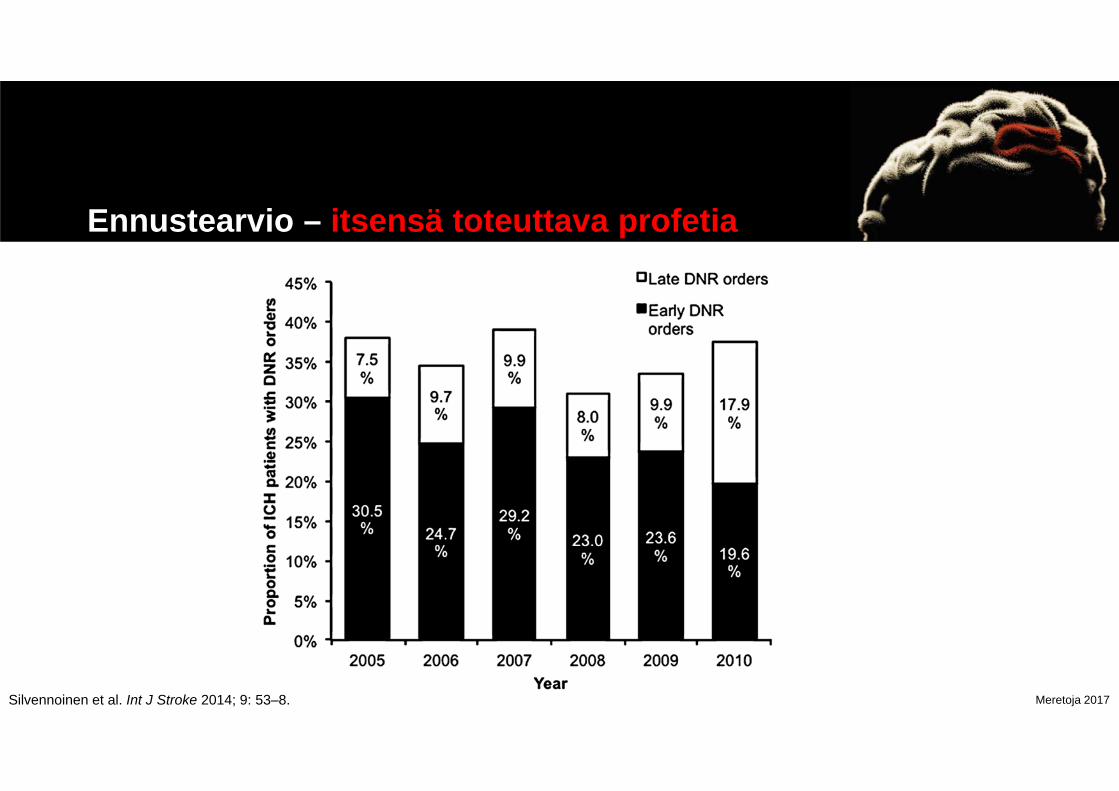
Ennustearvio – itsensä toteuttava profetia
Silvennoinen et al. Int J Stroke 2014; 9: 53–8.
Meretoja 2017
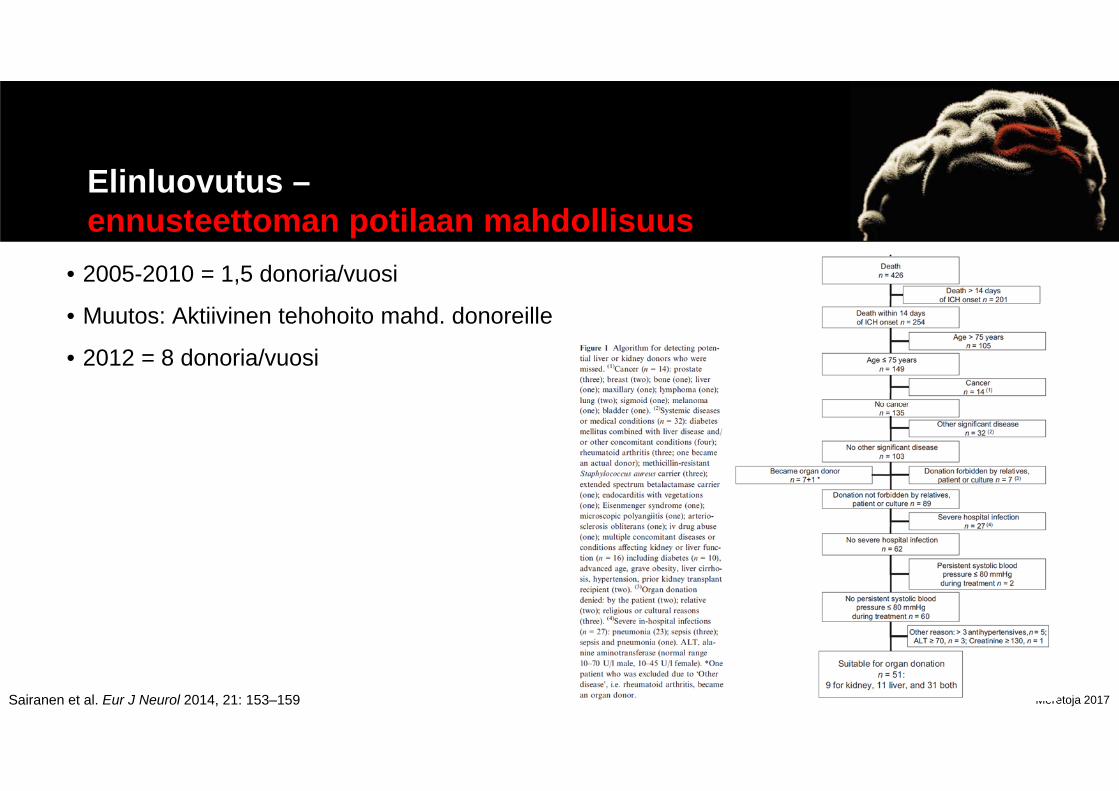
Elinluovutus –ennusteettoman potilaan mahdollisuus
• 2005-2010 = 1,5 donoria/vuosi
• Muutos: Aktiivinen tehohoito mahd. donoreille
• 2012 = 8 donoria/vuosi
Sairanen et al. Eur J Neurol 2014, 21: 153–159

Meretoja 2017
Missä ICH-potilaat viettävätensimmäisen vuotensa?
Jatkohoitoon, sieltä kotiin (34%)
Suoraan kotiin (23%)
Pysyvä laitoshoito (6%)
Kuoli jatkohoito-paikassa (14%)
Kuoli ensimmäisessälaitoksessa (23%)
Ensimmäinen sairaala
Jatkohoitopaikka
Koti Kuollut
Muu laitoshoito
Meretoja A. PERFECT Stroke. Julkaisematon.

Meretoja 2017
HOITOPAIKKA JA KOMPLIKAATIOT

Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusMonitorointi ja hoitopaikka
• Initial monitoring and management of ICH patients should take place in an intensive care unit or dedicated stroke unit with physician and nursing neuroscience acute care expertise (Class I; Level of Evidence B). (Revised from the previous guideline)

Meretoja 2017Langhorne et al. Stroke 2013;44:3044-9.

Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusKomplikaatioiden esto ja Kuntoutus
• A formal screening procedure for dysphagia should be performed in all patients before the initiation of oral intake to reduce the risk of pneumonia (Class I; Level of Evidence B). (New recommendation)
• Patients with ICH should have intermittent pneumatic compression for prevention of venous thromboembolism beginning the day of hospital admission (Class I; Level of Evidence A). (Revised from the previous guideline)
• Given the potentially serious nature and complex pattern of evolving disability and the increasing evidence for efficacy, it is recommended that all patients with ICH have access to multidisciplinary rehabilitation (Class I; Level of Evidence A). (Revised from the previous guideline)

Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusVerensokeri
• Glucose should be monitored. Both hyperglycemia and hypoglycemia should be avoided (Class I; Level of Evidence C). (Revised from the previous guideline)
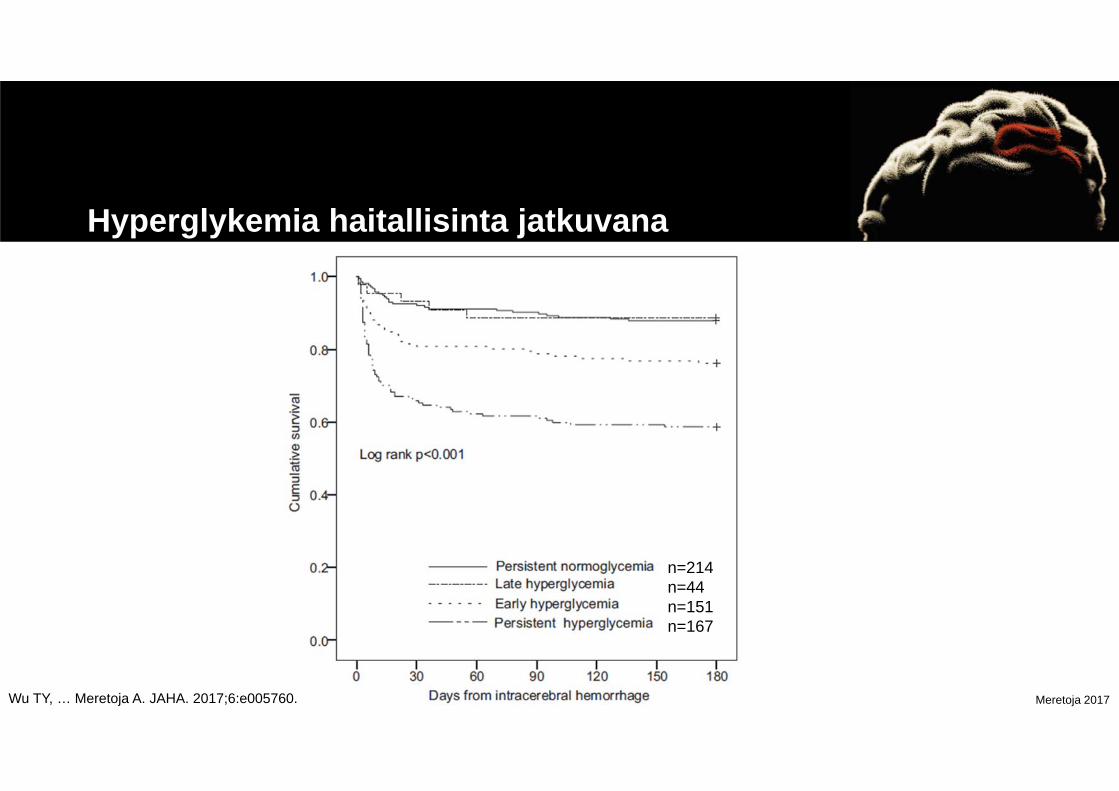
Meretoja 2017Wu TY, … Meretoja A. JAHA. 2017;6:e005760.
Hyperglykemia haitallisinta jatkuvana
n=214n=44n=151n=167
Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusKouristukset
• Clinical seizures should be treated with antiseizure drugs (Class I; Level of Evidence A). (Unchanged from the previous guideline)
• Patients with a change in mental status who are found to have electrographic seizures on EEG should be treated with antiseizure drugs (Class I; Level of Evidence C). (Unchanged from the previous guideline)
Meretoja 2017
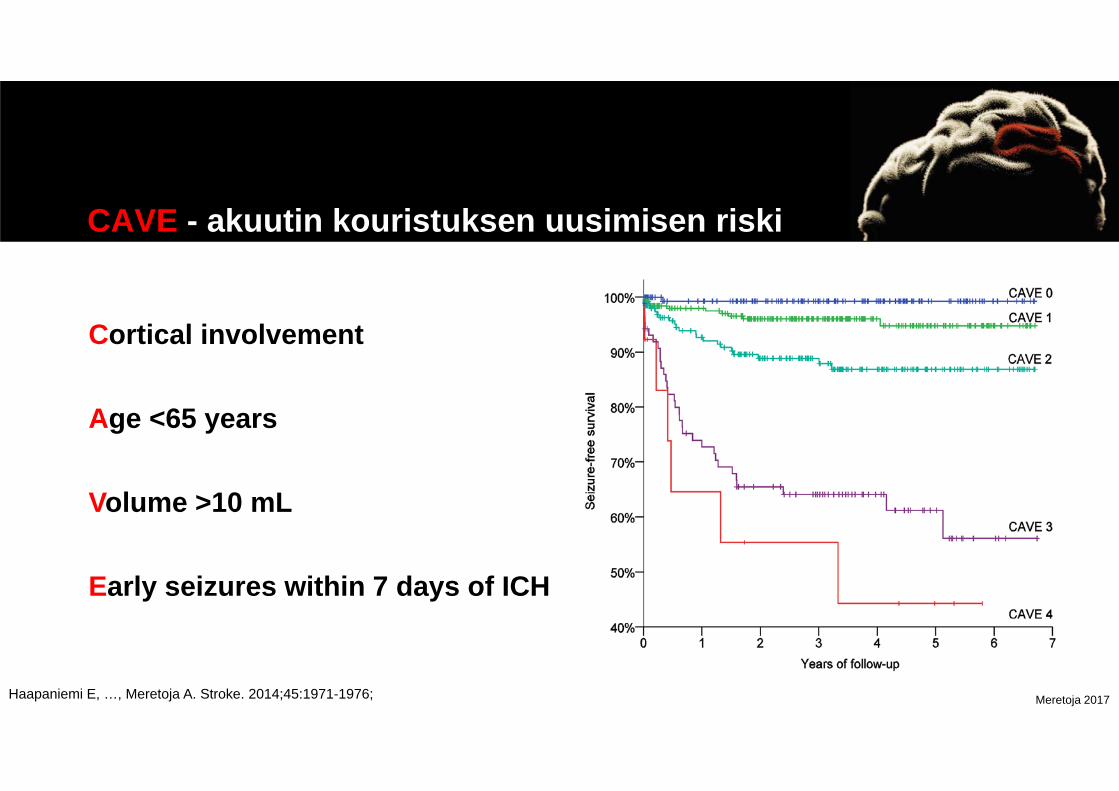
CAVE - akuutin kouristuksen uusimisen riski
Cortical involvement
Age <65 years
Volume >10 mL
Early seizures within 7 days of ICH
Haapaniemi E, …, Meretoja A. Stroke. 2014;45:1971-1976;

Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusSekundaaripreventio
• BP should be controlled in all ICH patients (Class I; Level of Evidence A). (Revised from the previous guideline)
• Measures to control BP should begin immediately after ICH onset (Class I; Level of Evidence A). (New recommendation)

Meretoja 2017
Verenpaineen hoito sekundaaripreventiossa (n=611)
Chapman N et al. PROGRESS trial Stroke 2004;35:116-121
Meretoja 2017
HEMOSTAASI ja ANTIKOAGULAATIO
Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusHemostaasi ja antikoagulaatio
• Patients with a severe coagulation factor deficiency or severe thrombocytopenia should receive appropriate factor replacement therapy or platelets, respectively (Class I; Level of Evidence C). (Unchanged from the previous guideline)
• Patients with ICH whose INR is elevated because of VKA should have their VKA withheld, receive therapy to replace vitamin K–dependent factors and correct the INR, and receive intravenous vitamin K (Class I; Level of Evidence C). (Unchanged from the previous guideline)

Meretoja 2017
PATCH (n=190)trombosyytti-infuusio lisää kuolleisuutta
Baharoglu et al. Lancet 2016; 387: 2605–13
Meretoja 2017
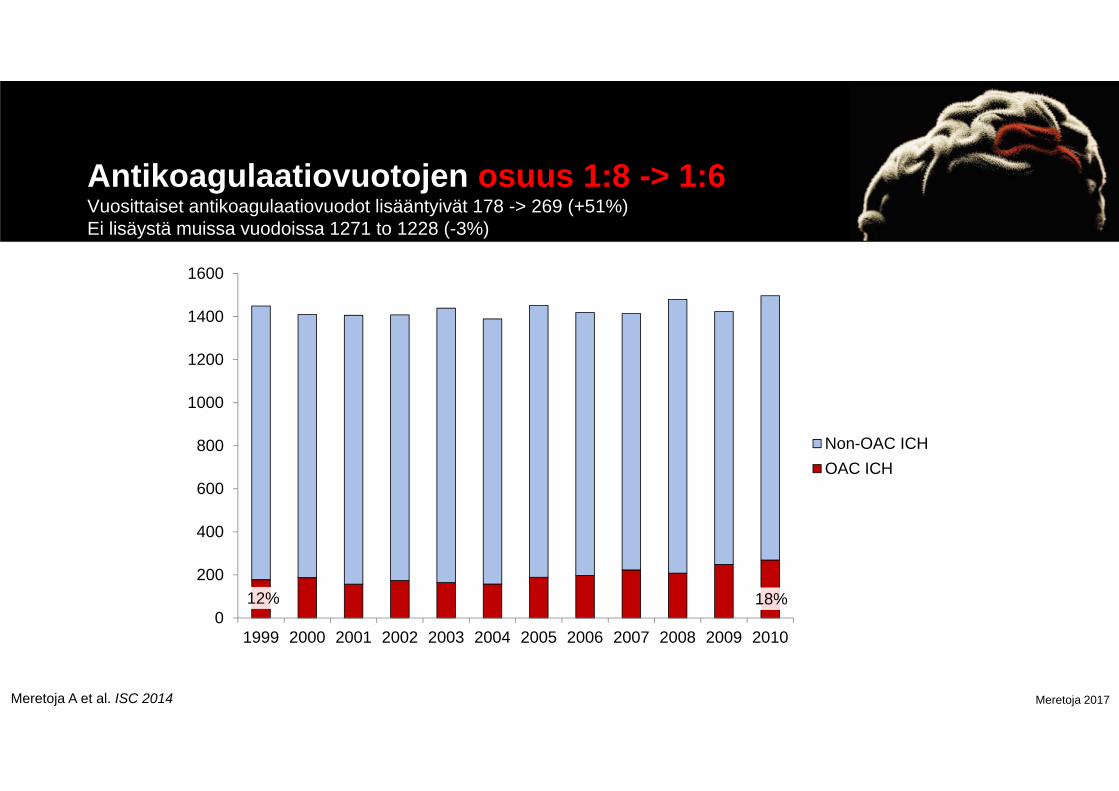
Antikoagulaatiovuotojen osuus 1:8 -> 1:6Vuosittaiset antikoagulaatiovuodot lisääntyivät 178 -> 269 (+51%) Ei lisäystä muissa vuodoissa 1271 to 1228 (-3%)
12% 18%0
200
400
600
800
1000
1200
1400
1600
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Non-OAC ICHOAC ICH
Meretoja A et al. ISC 2014
Meretoja 2017
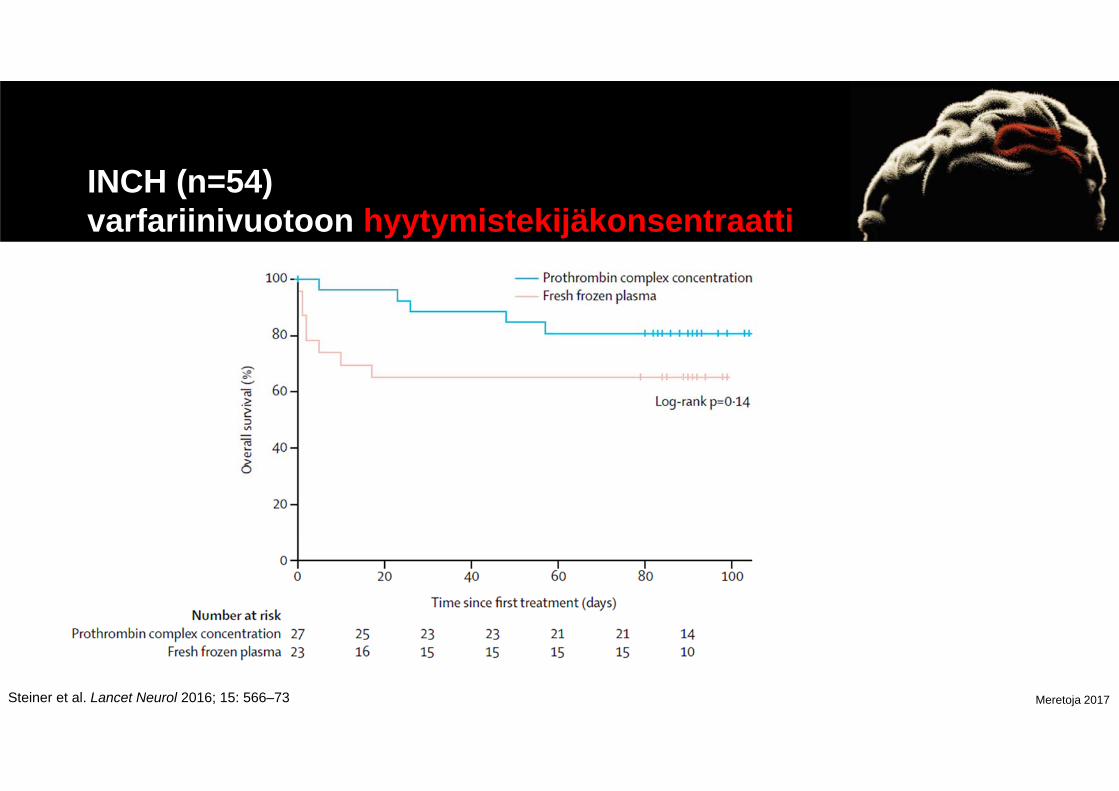
INCH (n=54) varfariinivuotoon hyytymistekijäkonsentraatti
Steiner et al. Lancet Neurol 2016; 15: 566–73

Meretoja 2017
Suorat antikoagulantit vs MarevanICH jälkeen ei kuolleisuuseroa (13 keskusta, n=500)
Wilson D, …, Meretoja A, Werring D. Neurology 2017;88:1693–1700
Meretoja 2017
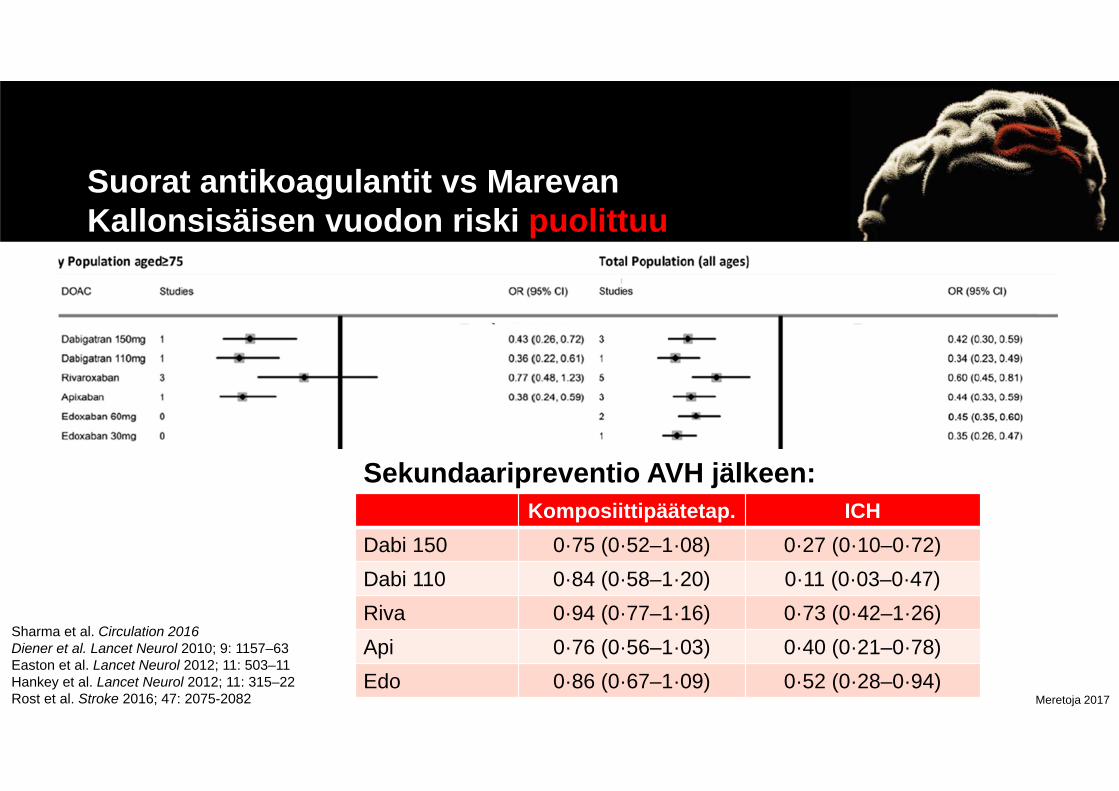
Suorat antikoagulantit vs MarevanKallonsisäisen vuodon riski puolittuu
Sharma et al. Circulation 2016Diener et al. Lancet Neurol 2010; 9: 1157–63Easton et al. Lancet Neurol 2012; 11: 503–11Hankey et al. Lancet Neurol 2012; 11: 315–22Rost et al. Stroke 2016; 47: 2075-2082
Komposiittipäätetap. ICHDabi 150 0·75 (0·52–1·08) 0·27 (0·10–0·72)Dabi 110 0·84 (0·58–1·20) 0·11 (0·03–0·47)Riva 0·94 (0·77–1·16) 0·73 (0·42–1·26)Api 0·76 (0·56–1·03) 0·40 (0·21–0·78)Edo 0·86 (0·67–1·09) 0·52 (0·28–0·94)
Sekundaaripreventio AVH jälkeen:

Meretoja 2017
HEMOSTAATIT
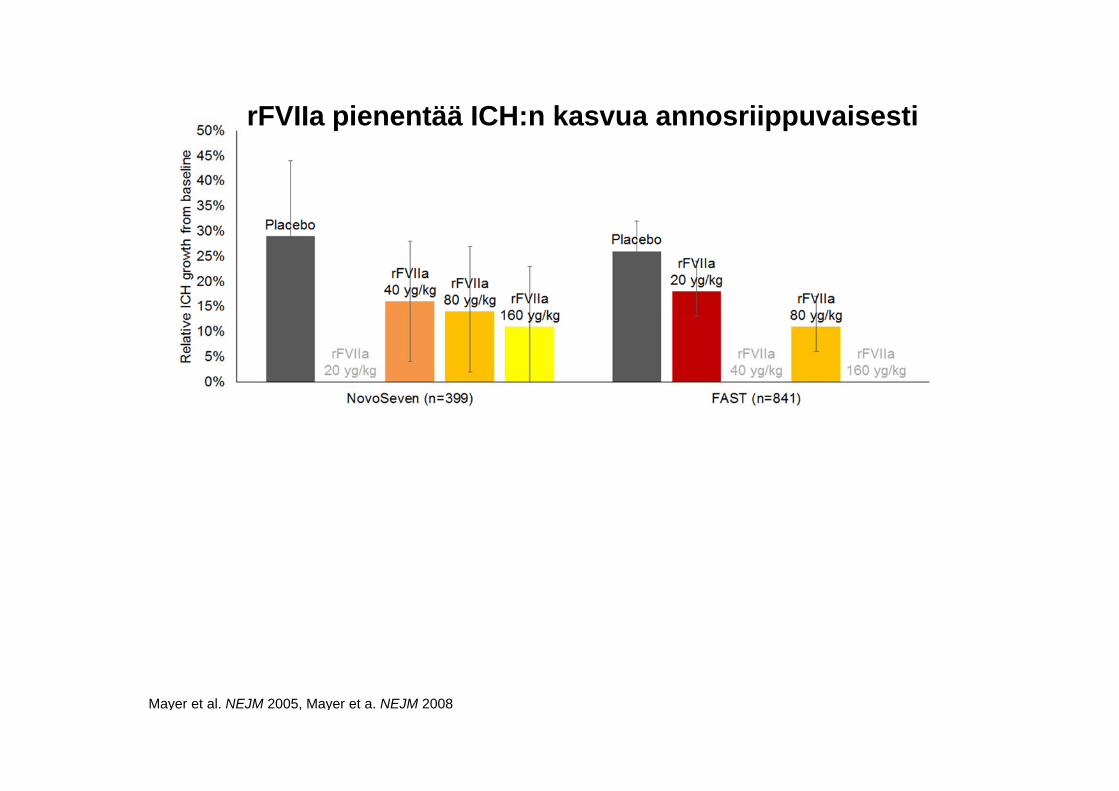
Mayer et al. NEJM 2005, Mayer et a. NEJM 2008
rFVIIa pienentää ICH:n kasvua annosriippuvaisesti

Mayer et al. NEJM 2005, Mayer et a. NEJM 2008
rFVIIa pienentää ICH:n kasvua annosriippuvaisesti

Meretoja 2017
rFVIIa - hemostaatti
Meretoja 2017
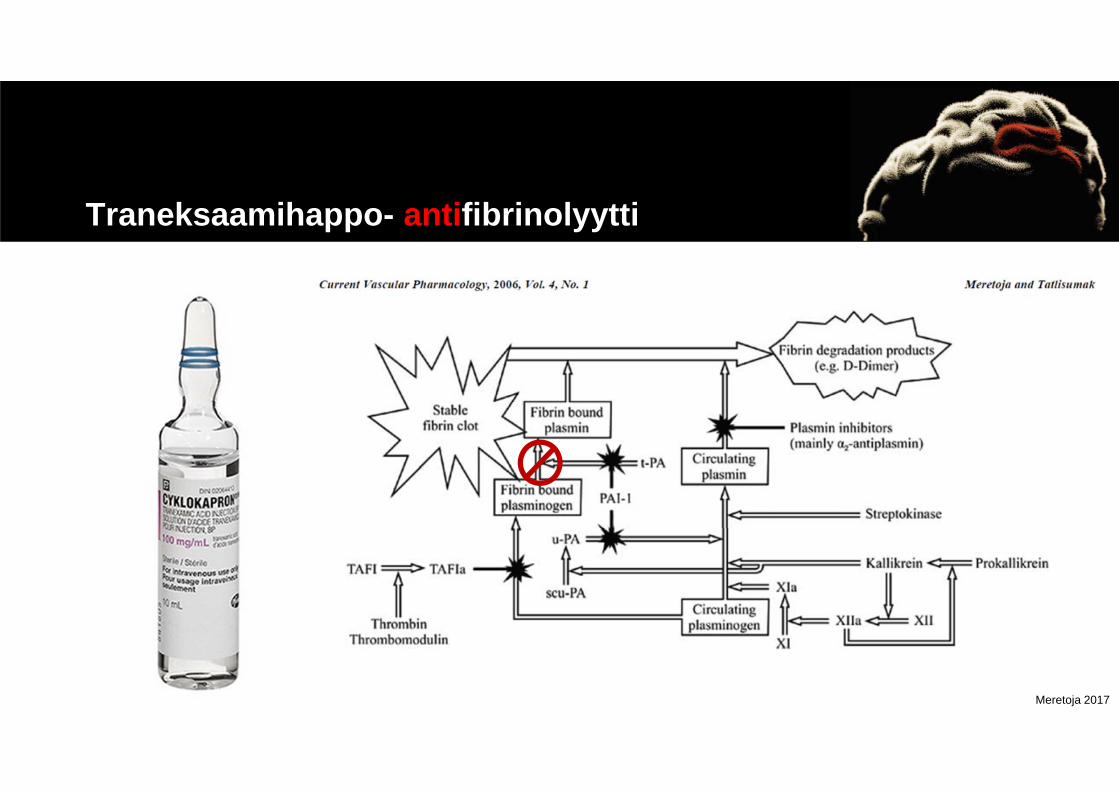
Traneksaamihappo- antifibrinolyytti

Meretoja 2017
VERENPAINE

Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusVerenpaine
• For ICH patients presenting with SBP between 150 and 220 mm Hg and without contraindication to acute BP treatment, acute lowering of SBP to 140 mm Hg is safe (Class I; Level of Evidence A) and can be effective for improving functional outcome (Class IIa; Level of Evidence B). (Revised from the previous guideline)
Meretoja 2017
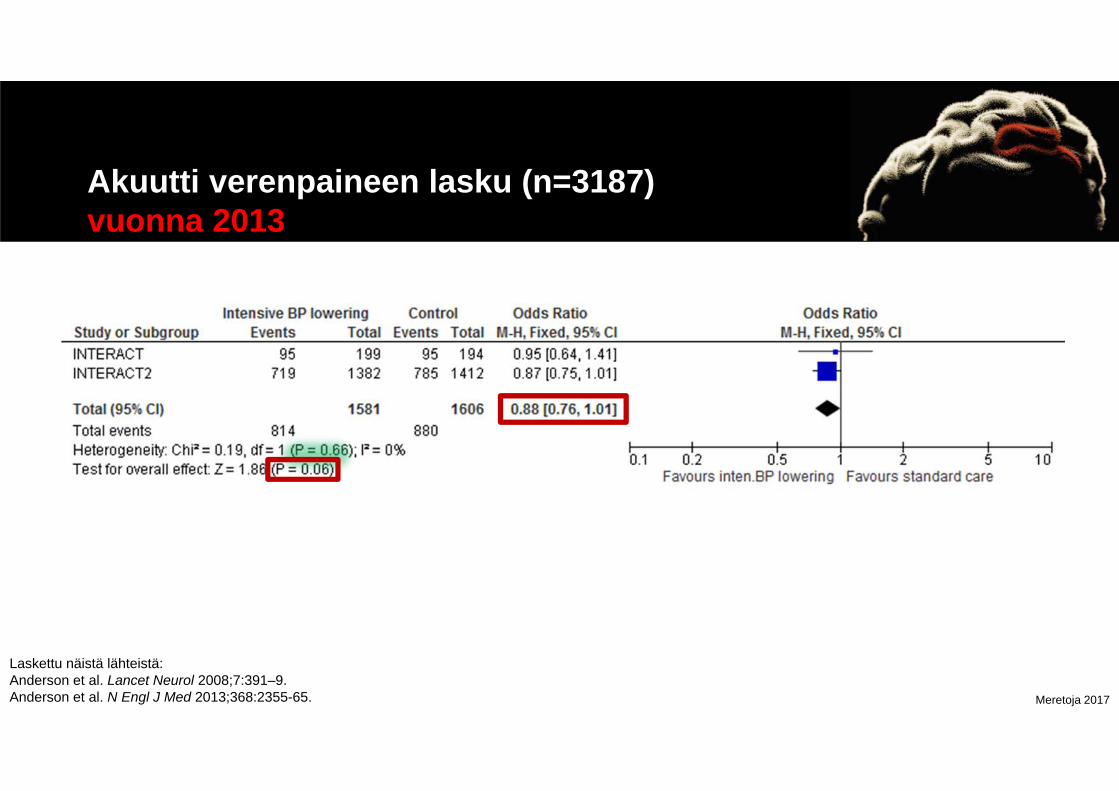
Akuutti verenpaineen lasku (n=3187)vuonna 2013
Laskettu näistä lähteistä:Anderson et al. Lancet Neurol 2008;7:391–9.Anderson et al. N Engl J Med 2013;368:2355-65.
Meretoja 2017
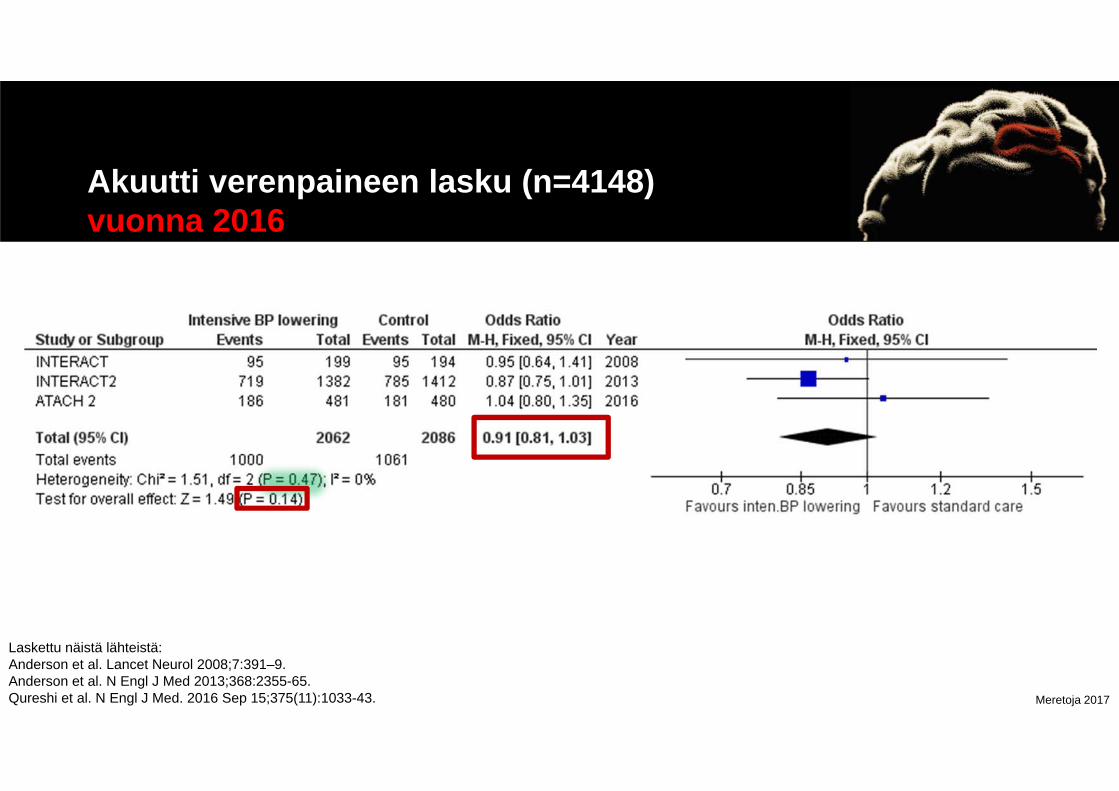
Akuutti verenpaineen lasku (n=4148)vuonna 2016
Laskettu näistä lähteistä:Anderson et al. Lancet Neurol 2008;7:391–9.Anderson et al. N Engl J Med 2013;368:2355-65.Qureshi et al. N Engl J Med. 2016 Sep 15;375(11):1033-43.

Meretoja 2017
Intensiivinen akuutti verenpaineen laskuei vähentänyt kasvua
p=0.06 p=0.27 p=0.05 p=0.90
Anderson et al. Lancet Neurol 2008;7:391–9.Anderson et al. N Engl J Med 2013;368:2355-65.
Meretoja 2017
KIRURGIA
Meretoja 2017
American Heart Association/American Stroke AssociationHemphill et al.Stroke 2015
AHA SuositusVuodon evakuaatio
• Patients with cerebellar hemorrhage who are deteriorating neurologically or who have brainstem compression and/or hydrocephalus from ventricular obstruction should undergo surgical removal of the hemorrhage as soon as possible (Class I; Level of Evidence B). (Unchanged from the previous guideline)
Meretoja 2017
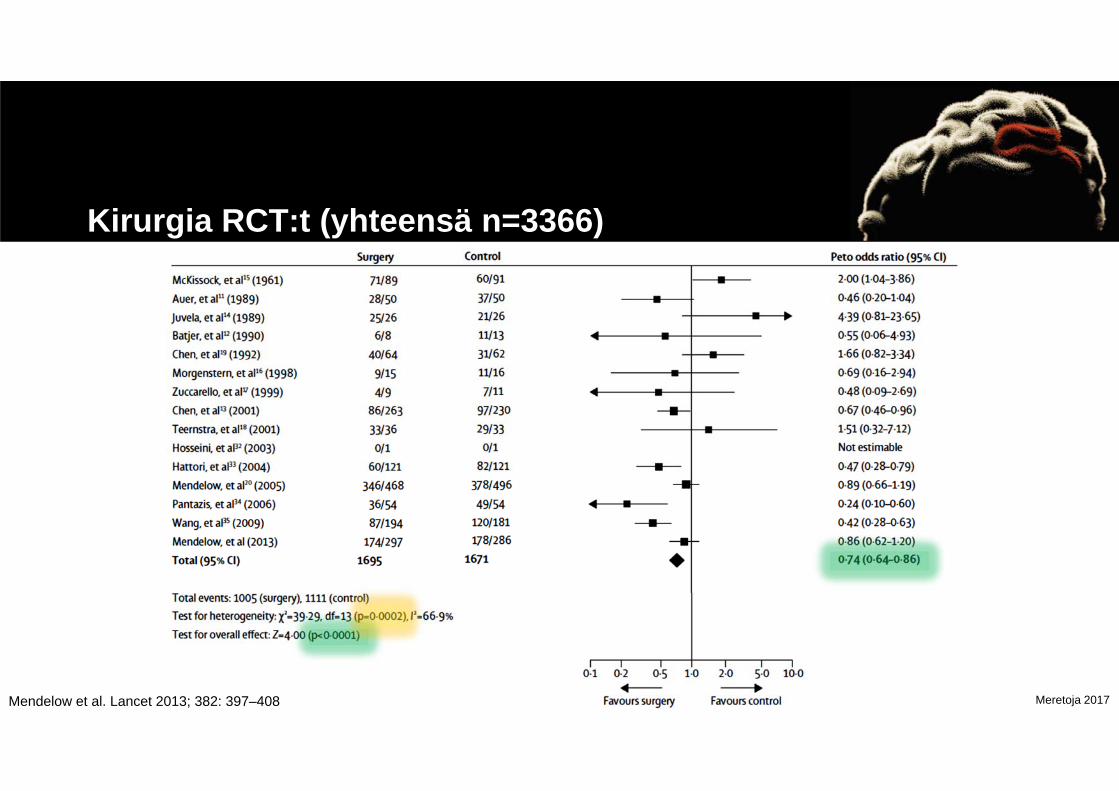
Kirurgia RCT:t (yhteensä n=3366)
Mendelow et al. Lancet 2013; 382: 397–408
Meretoja 2017
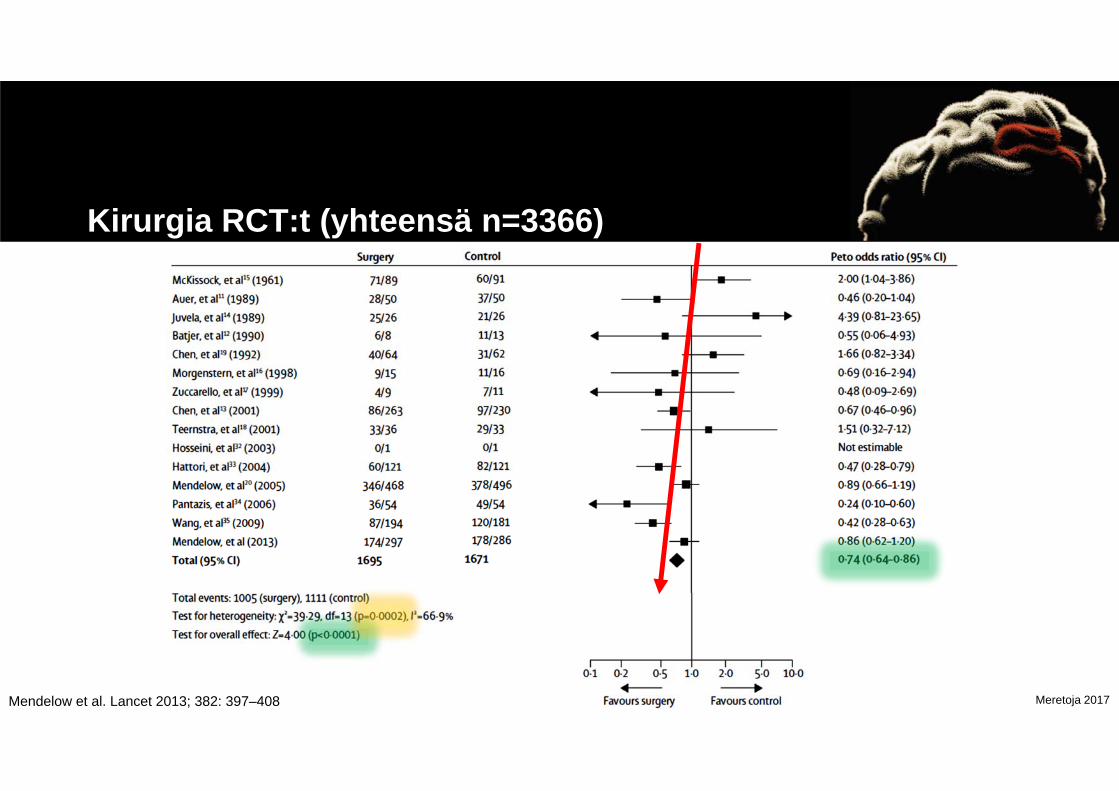
Kirurgia RCT:t (yhteensä n=3366)
Mendelow et al. Lancet 2013; 382: 397–408
Meretoja 2017
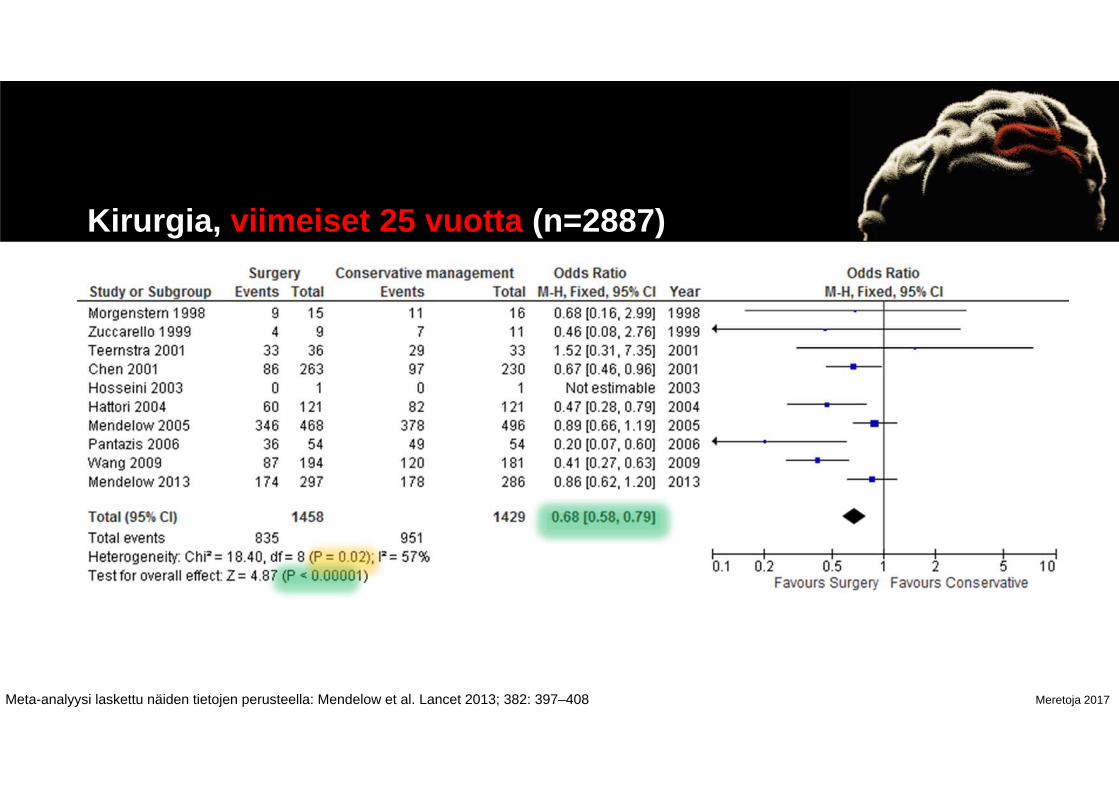
Kirurgia, viimeiset 25 vuotta (n=2887)
Meta-analyysi laskettu näiden tietojen perusteella: Mendelow et al. Lancet 2013; 382: 397–408

Minimally invasive surgery: stereotactic intra-clot EVD + tPA

Meretoja 2017
Kirurgia, viimeiset 25 vuotta (n=2887)
Calculated from: Mendelow et al. Lancet 2013; 382: 397–408

Meretoja 2017
“In recent years, an innovative minimally invasive craniopuncture technique has been widely used to treat spontaneous ICH in China because fewer skills are required ... …. In the past few years, over 150 000 cases of spontaneous ICH have been treated with this technique.”
Wang et al. Int J Stroke. 2009 Feb;4(1):11-6
Meretoja 2017
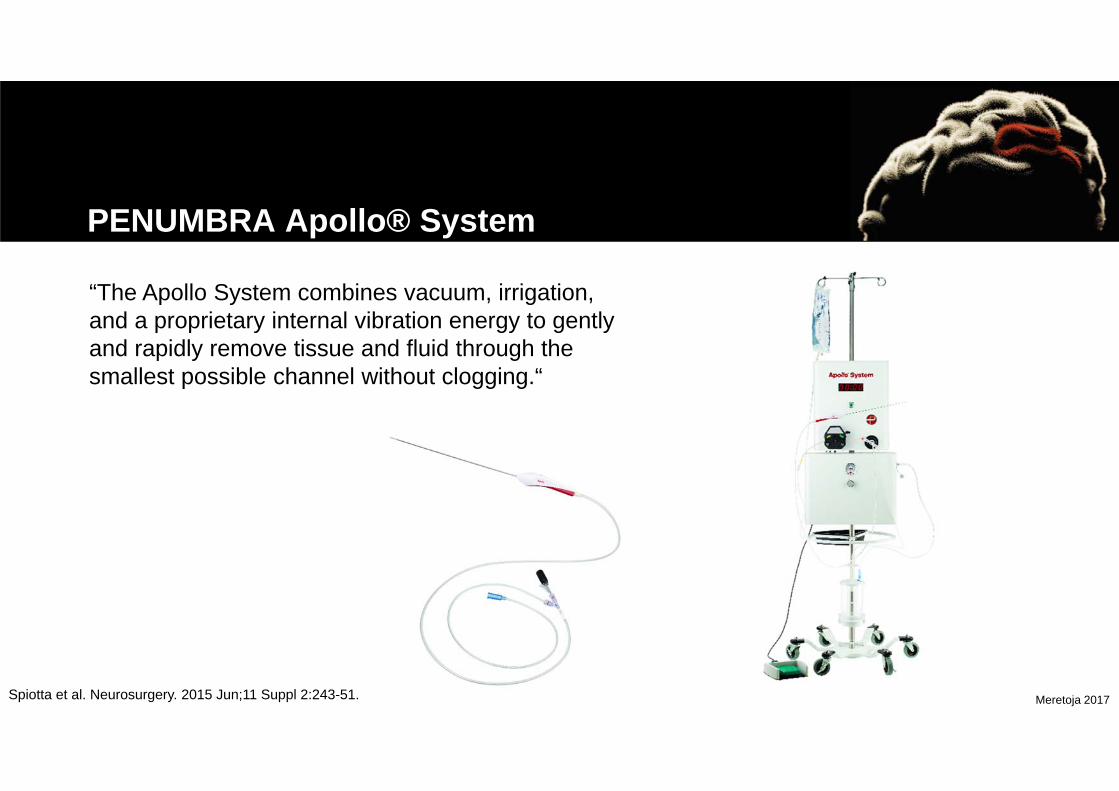
PENUMBRA Apollo® System
Spiotta et al. Neurosurgery. 2015 Jun;11 Suppl 2:243-51.
“The Apollo System combines vacuum, irrigation, and a proprietary internal vibration energy to gently and rapidly remove tissue and fluid through the smallest possible channel without clogging.“
Meretoja 2017
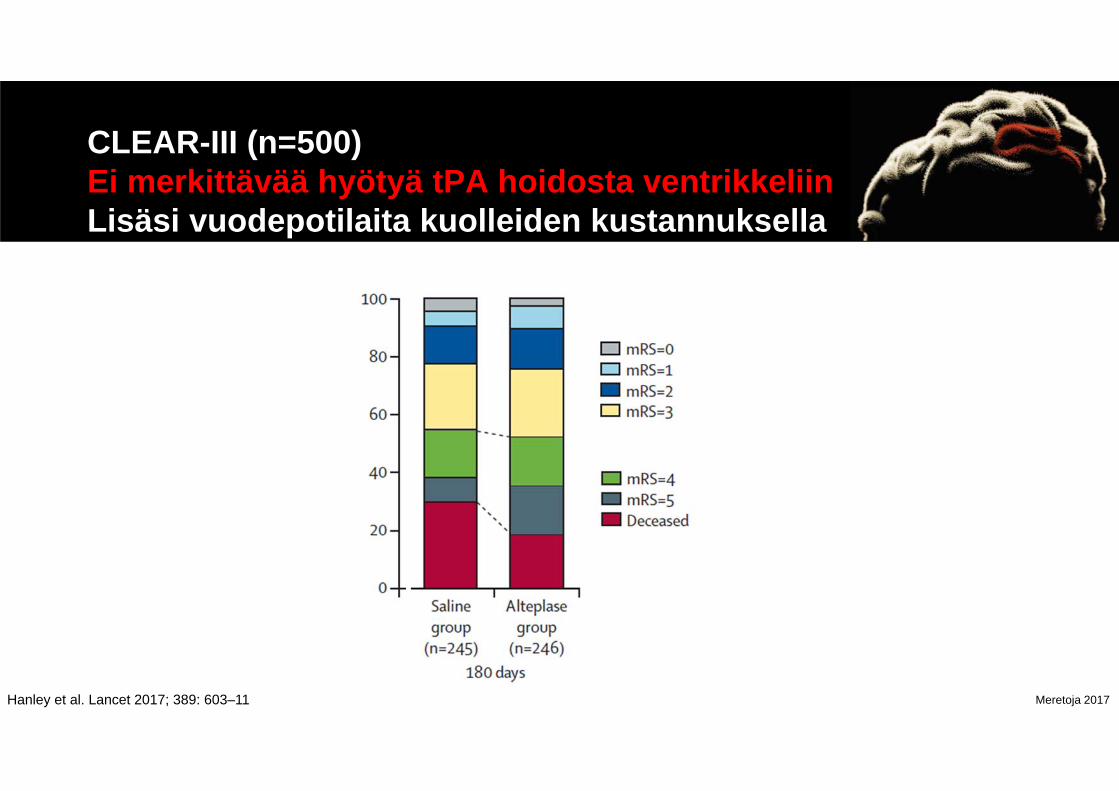
CLEAR-III (n=500)Ei merkittävää hyötyä tPA hoidosta ventrikkeliinLisäsi vuodepotilaita kuolleiden kustannuksella
Hanley et al. Lancet 2017; 389: 603–11

Meretoja 2017
ICH: n hoitava erikoisala vaihtelee maailmalla
Meretoja et al. Int J Stroke 2017 Oct;12(8):858-868

Meretoja 2017
Meilahden evakuoidut ICH:t 2005-2010n = 61 / 1013 (6%)
514
17
316
32
60 1157 1
0 %
10 %
20 %
30 %
40 %
50 %
60 %
70 %
80 %
90 %
100 %
Konservatiivinen Evakuoitu
Brain stemCerebellumLobarDeep
Konser-vatiivinen Evakuoitu
Ikä, mediaani 69 60
Vuodon koko,mediaani 14 mL 44 mL
Rupturoitunutventrikkeliin 43 % 56 %
Kuolleisuus,3 kk 33,2 % 16,4 %

Meretoja 2017
Yhteenveto• Aivoverenvuoto = tärkein kuolleisuutta ja vammaisuutta aiheuttava neurologinen sairaus
• Antikoagulaatioon liittyvä vuodot lisääntyvät
• Vain aivohalvausyksiköt ja sekundaarinen verenpaineen hoito perustuvat vahvaan näyttöön
• Kirurgiaa käytetään todennäköisesti liian vähän
• Tulossa lähivuosina– mini-invasiivinen kirurgia?– toivottavasti antifibrinolyytit?

Meretoja 2017
KIITOS!ICH yhteistyötahot
Daniel Augustin Godoy Sanatorio Pasteur, Catamarca, ArgentinaMatthew Lee-Archer, Helen Dewey Austin Hospital, Heidelberg, AustraliaLuke Perry, Philip Choi Box Hill Hospital, Box Hill, AustraliaCraig Anderson The Royal Prince Alfred Hospital, Camperdown, AustraliaTeddy Wu, Bernard Yan, Stephen M. Davis The Royal Melbourne Hospital, Parkville, AustraliaDaniel Strbian, Jukka Putaala, Sami Curtze, Gerli Sibolt, Tiina Sairanen, Satu Mustanoja, Turgut Tatlisumak, Jarno Satopää, Hanne Sallinen, Mika Niemelä, Markku Kaste
Helsinki University Hospital, Helsinki, Finland
Juha Huhtakangas, Sami Tetri Oulu University Hospital, Oulu, FinlandCharlotte Cordonnier, Nelly Dequatre-Ponchelle Lille University Hospital, Lille, FranceSolveig Horstmann, Roland Veltkamp Heidelberg University Hospital, Heidelberg, GermanyFabrizio Meligeni, Mario Di Napoli San Camillo de'Lellis General Hospital Stroke, Rieti, ItalyPaolo Pennati, Luca Masotti Cecina Hospital Stroke Registry, Cecina, ItalyLuigi Fenoglio, Fulvio Pomero S. Croce e Carle’ Hospital, Cuneo, ItalyRik Houben, Julie Stalls, Floris Schreuder Maastricht University Medical Center, Maastricht, the NetherlandsKoen M. van Nieuwenhuizen, Karin Klijn University Medical Center Utrecht, Utrecht, the NetherlandsShin-Joe Yeh, Jiann-Shing Jeng National Taiwan University Hospital, Taipei, TaiwanAdrian Parry-Jones, Seun Sobowale Salford Royal NHS Foundation Trust, Manchester, UKDuncan Wilson, David Werring University College London (CROMIS 2 Study), London, UKKristiina Rannikmäe, Rustam Al-Shahi Salman Univesity of Edinburgh (LATCH), Edinburgh, UKJoshua Goldstein, Abigail Cohen, Jonathan Rosand Massachusetts General Hospital, Boston, USA+KAIKKI STOP-AUST tiimit ja tutkijat

Meretoja 2017
Pitkäaikaiskustannukset korkeatViiden vuoden vuotuiset kustannukset, vuoden 2003 potilaat
0 €
5 000 €
10 000 €
15 000 €
20 000 €
25 000 €
30 000 €
Ischemic stroke ICH SAH Total for averagestroke patient alive at
start of each year
Previous year 1st year 2nd year 3rd year 4th year 5th year
Meretoja A et al. Stroke. 2011;42:2007-2012.
Meretoja 2017
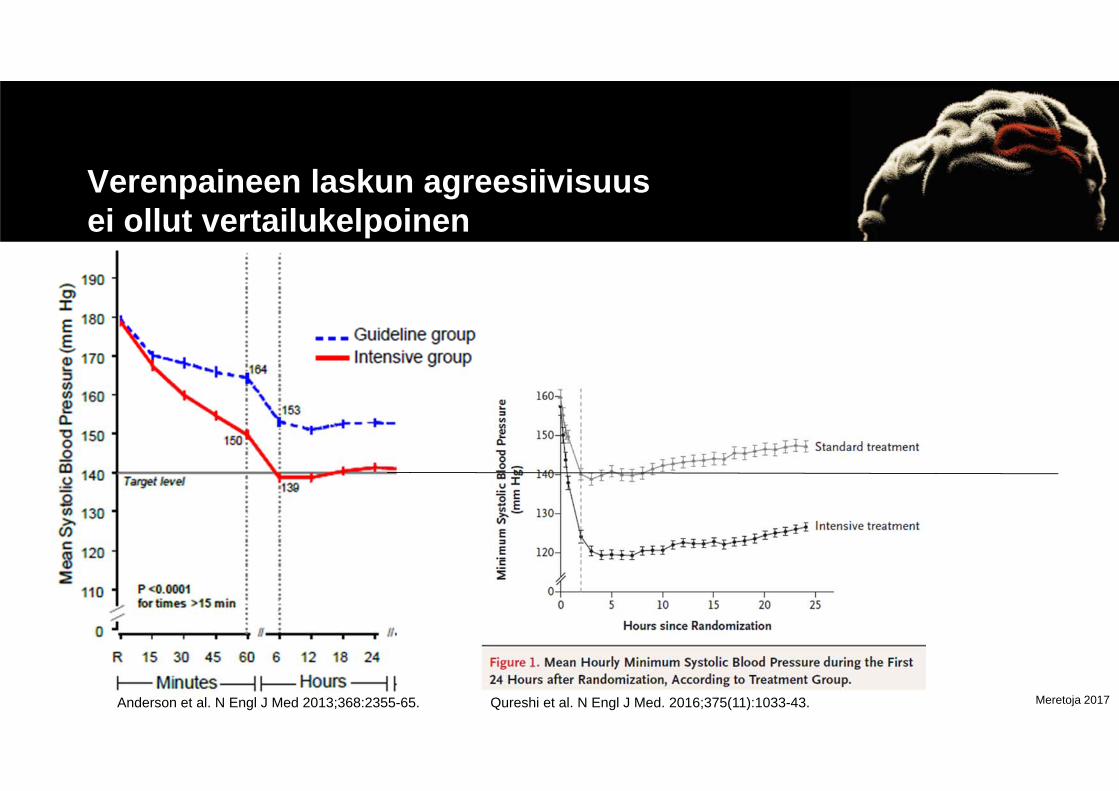
Verenpaineen laskun agreesiivisuusei ollut vertailukelpoinen
Anderson et al. N Engl J Med 2013;368:2355-65. Qureshi et al. N Engl J Med. 2016;375(11):1033-43.
Meretoja 2017
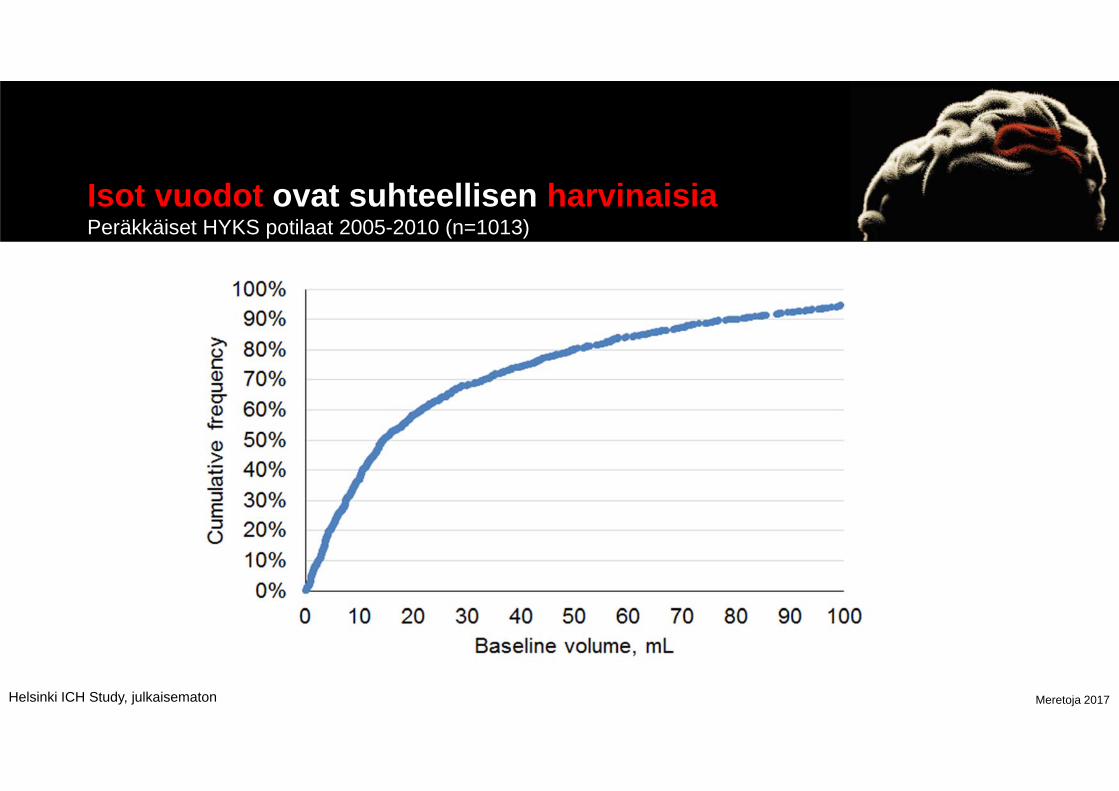
Isot vuodot ovat suhteellisen harvinaisiaPeräkkäiset HYKS potilaat 2005-2010 (n=1013)
Helsinki ICH Study, julkaisematon
Meretoja 2017
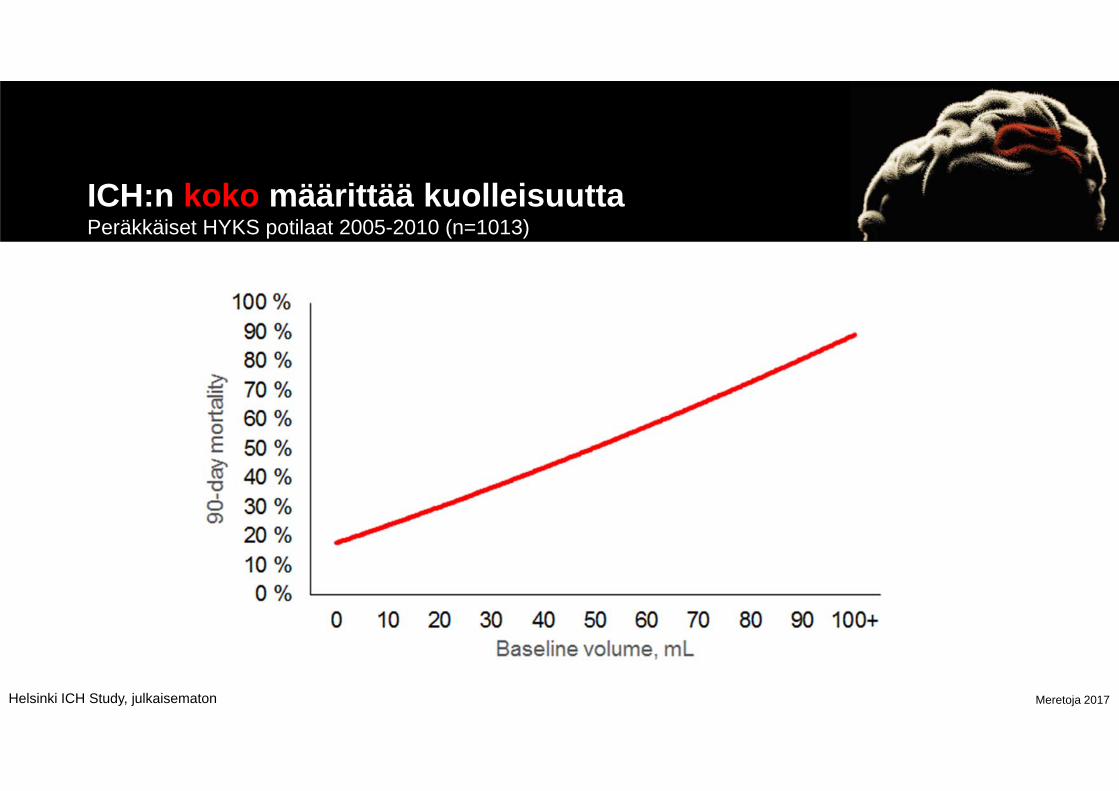
ICH:n koko määrittää kuolleisuuttaPeräkkäiset HYKS potilaat 2005-2010 (n=1013)
Helsinki ICH Study, julkaisematon
Meretoja 2017

Meretoja 2017
Koon kuolleisuussuhde riippuu sijainnistaPeräkkäiset HYKS potilaat 2005-2010 (n=1013)
Aivorunko Pikkuaivot Tyvitumakkeet Kortikaaliset
Helsinki ICH Study, julkaisematon