IBM Patient-Centered Medical Home Pre Launch Briefing
29
© Copyright IBM Corporation 2009 Patient-Centered Medical Home What, Why and How? Pre-Launch Briefing May 27, 2009
-
Upload
ibm-ibv-institute-for-business-value -
Category
Business
-
view
3.526 -
download
0
Transcript of IBM Patient-Centered Medical Home Pre Launch Briefing

© Copyright IBM Corporation 2009
Patient-Centered Medical Home
What, Why and How?
Pre-Launch Briefing
May 27, 2009

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 2 © Copyright IBM Corporation 2009
Today’s speakers
F. Daniel Duffy, MD, MACPSenior Associate Dean for Academics,University of Oklahoma School of Community Medicine
Martin S. Kohn, MD, MS, FACEP, CPESenior Managing Consultant, IBM Healthcare Strategy and Change Practice
Edgar L. Mounib, MBA, MPHGlobal Healthcare Lead, IBM Institute for Business Value
Beginning May 28th, download study atwww.ibm.com/healthcare/medicalhome

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 3 © Copyright IBM Corporation 2009
Abstract
The patient-centered medical home (PCMH) can serve as a foundation for transformation of the U.S. healthcare system – if appropriately conceived and properly implemented. But it can also suffer from unfettered expectations. This study makes the realistic case for why and how stakeholders can participate in PCMH initiatives, identifies critical issues and makes recommendations for best practices to increase the likelihood of initial success and sustainability.
Preface

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 4 © Copyright IBM Corporation 2009
Agenda
Introduction
The medical home: What is it? What isn’t it?
Why should it be done now?
How should it be done?
Conclusion
Agenda

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 5 © Copyright IBM Corporation 2009
Despite having many fine care delivery organizations and caregivers, the U.S. healthcare system is badly broken
High, rapidly rising costs
US$2.5 trillion (17.6% of GDP) will be spent in 2009-US$4.0 trillion (almost 20% of GDP) will be spent in 2015
Highest per capita spend among OECD countries in 2006-48% more than Norway, which spends the third-most-2.4x the OECD average per capita spend
No link between higher costs and quality or safety
98,000 to 195,000 people killed per year by medical mistakes57,000+ dying from inadequate care2 million hospital-acquired infections with 90,000 dying per year4-fold variation in costs with similar qualityRanked 37th in overall health system performance by WHO22nd in life expectancy, 28th in infant mortality and 30th in obesity among the 30 OECD countries
Access issues45+ million uninsured15+ million under-insured, most who are working
Introduction
“Let there be no doubt ... Healthcare reform cannot wait, it must not wait, and it will not wait another year.”- U.S. President Barack Obama, 24 Feb 2009
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 6 © Copyright IBM Corporation 2009
Foundational to healthcare transformation is a primary care system that provides comprehensive and timely care
Primary care offers demonstrable benefits that leads to – - Better health outcomes1
- Lower costs1
- Greater equity in health1
For example, Patients who have a regular primary care provider (PCP) – - Incur about ⅓ less healthcare expenditure2
- Have 19% lower mortality2
- Are 7% more likely to stop smoking3
- Are 12% less likely to be obese3
Majority of patients prefer initial care from a PCP, rather than a specialist
Introduction
Source: 1) B Starfield, Milbank Quarterly, 2003; B Starfield, “The best care is primary care” presented at WONCA 2004; The Future of Family Medicine Study; 2) Franks, Peter and Kevin Fiscella. “Primary Care Physicians and Specialists as Personal Physicians: Health Care Expenditures and Mortality Experience.” Journal of Family Practice. August 1998; 3) Arora, Vineet, Sandeep Gangireddy, Amit Mehrotra, Ranjan Ginde, Megan Tormey, et al. “Ability of hospitalized patients to identify their in-hospital physicians.” Archives ofInternal Medicine. January 26, 2009.

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 7 © Copyright IBM Corporation 2009
From 1998-2008, 57% fewer
medical school graduates entered family practice residencies3
In 2004, the median income for primary care physicians was about
½ that of specialists2
Exacerbating this is a primary care system – the foundation to any healthcare system – that is also broken
PCP shortage is worsening: 35K-44K by 2025- Failure to attract new residents1
- Reimbursement is relatively low and based on quantity2
- Growing levels of frustration
Current primary care practice is geared to treating acute, episodic interventions- Emphasis on triage, not on coordinating care - Minimal communication between providers- Minimal focus on education and self-management - Slow to adopt evidence-based medicine
No tools and support in place such as EMRs Even with tools, evidenced based medicine is more difficult
for PCPs than for specialists because facing more comorbidities or in preventive mode
- Generally lower level of support structure (EMR, support staff, etc.)
Challenge Highlights
Introduction
Source: 1) P.A. Pugno et al., "Results of the 2006 National Resident Matching Program: Family Medicine," Family Medicine 38, no. 9 (2006): 637–646; and T. Bodenheimer, "Primary Care—Will It Survive?" New England Journal of Medicine 355, no. 9 (2006): 861–864; 2) T. Bodenheimer, R.A. Berenson, and P. Rudolf, "The Primary Care–Specialty Income Gap: Why It Matters," Annals of Internal Medicine 146, no. 4 (2007): 301–306; 3) American Academy of Family Physicians. "2008 National Resident Matching Program."

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 8 © Copyright IBM Corporation 2009
Agenda
Introduction
The medical home: What is it? What isn’t it?
Why should it be done now?
How should it be done?
Conclusion
Agenda

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 9 © Copyright IBM Corporation 20099
Patient-centric/Personal PCP PCP-directed medical “team” Whole person orientation Care is coordinated and/or integrated Emphasis on quality and safety Enhanced access Appropriate reimbursement
Patient-Centered Medical Home (PCMH) is an approach to deliver comprehensive care, coordinated by a PCP-led extended care team
Brief history of the evolution of the PCMH- 1967: American Academy of Pediatrics defined medical home
concepts related to children with special needs- 2000-present: AAFP and ACP developed and extended the
concept to include care for all patients with chronic illness and patient centeredness
- 2006-07: AAFP, AAP, ACP and AOA develop a common definition of “patient-centered medical home” and link PCMH to reform of payment for physicians
Principles of PCMH
Technology, Services & Applications to Support the
New Collaborative Care Model
Technology, Services & Applications to Support the
New Collaborative Care Model++Personal Relationship with a
PCP and Care TeamPersonal Relationship with a
PCP and Care Team
Proactive Focus on Health, Care Intervention and Chronic
Disease Management
Proactive Focus on Health, Care Intervention and Chronic
Disease Management
“The Patient-Centered Medical Home (PCMH) provides care that is “accessible, continuous, comprehensive and coordinated and delivered in the context of family and community.”1
Source: 1) www.medicalhomeinfo.org/join%20statementpdf
The medical home: What is it? What isn’t it?

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 10 © Copyright IBM Corporation 200910
Today’s CareToday’s Care Medical Home CareMedical Home Care
Our patients are those who are registered in our medical home
Care is determined by today’s problem and time available today
Care is determined by a proactive plan to meet health needs, with or without visits
Care varies by scheduled time and memory or skill of the doctor
Care is standardized according to evidence-based guidelines
Patients are responsible for coordinating their own care
A prepared team of professionals coordinates all patients’ care
I know I deliver high quality care because I’m well trained
We measure our quality and make rapid changes to improve it
It’s up to the patient to tell us what happened to them
We track tests and consultations, and follow-up after ED and hospital
Clinic operations center on meeting the doctor’s needs
An interdisciplinary team works at the top of our licenses to serve patients
My patients are those who make appointments to see me
The PCMH concept advocates enhanced access to comprehensive, coordinated, evidence-based, interdisciplinary care
Source: Adapted with permission from F. Daniel Duffy, MD, MACP, Senior Associate Dean for Academics, University of Oklahoma School of Community Medicine
The medical home: What is it? What isn’t it?

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 11 © Copyright IBM Corporation 2009
While other approaches have addressed some PCMH Principles, none have addressed them all
Factor/Principle PCMH Non-integrated
managed carePay for
performanceDisease
managementChronic care
model
Purpose/focusFacilitate partnership between PCP and patient
Ideally: cost, quality; Actually: control utilization
Meet operational goals with financial incentives
Meet specific management targets for chronic disease
Org. framework for chronic care mgt and practice improvement
Patient centric/ personal physician
Yes No NoMaybe, often led by actors independent of primary care
Yes, for chronic illness
Physician directed medical “team”
Yes No No No Yes
Whole person orientation
Yes No No No Yes
Care is coordinated and/or integrated
YesNo incentive for coordination
No incentive for coordination
MaybeYes
Emphasis on quality and safety
Yes, evidence-based and best practice; improved outcomes rewarded
No, reduced utilization rewarded
Indirectly; process targets rather than outcome ones
Yes, particularly for diseases
Yes, for chronic illnesses
Enhanced access Yes No, reduced access No Maybe No
Appropriate reimbursement
Yes for PCPs, unclear for others
Potential conflict in motivation
No, still volume driven
Partially, if evidence-base used
No
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value
Aligned Mixed alignment Not alignedAlignment with PCMH Principle:
The medical home: What is it? What isn’t it?

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 12 © Copyright IBM Corporation 2009
Nevertheless, the PCMH model needs additional support
Better clinical content- Evidence-based or personalized health and care/ability to incorporate into practice- Tools to help with correct and complete diagnosis
Changes with and support from other stakeholders since the PCMH model cannot be dropped into the current system for optimal results; examples include:- Consumer responsibility/changing consumer behaviors- Reimbursement changes/payment system reform- Alignment, coordination or integration with care delivered by others outside the medical home (e.g. specialists) in other care settings (e.g. ambulatory surgery centers or hospitals); this has been called the “medical neighborhood.”
- Policy reform to allow payers to collaborate in designing incentive systems- Universal coverage/coverage decisions
Infrastructure to support PCMH model (IT and other services) targeting the consumer/patient and the clinicians (see next slide)
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value
The medical home: What is it? What isn’t it?

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 13 © Copyright IBM Corporation 2009
For example, Health Plans or other entities could offer a variety of services or tools both to members and to providers
Providers• Tools and resources for virtual interdisciplinary care delivery teams
• Tools to support better access to clinical and patient information
• Tools to support cost/quality transparency
• Tools or services to provide coordinated, integrated care
• Tools to enhance access (e-visits, telemedicine)
• Tools to streamline administrative processes
Individuals• Health/wealth planning and management
• Risk assessment• Personal Health Records• Connected personal medical devices
• Trusted clinical information
• Collaboration tools and trusted sites
• Benefits selection• Provider selection
Examples of Tools and Services
• Health coaching • Value coaching
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value
The medical home: What is it? What isn’t it?

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 14 © Copyright IBM Corporation 2009
Agenda
Introduction
The medical home: What is it? What isn’t it?
Why should it be done now?
How should it be done?
Conclusion
Agenda

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 15 © Copyright IBM Corporation 2009
Great majority of patients prefer to seek initial care from PCPs rather than specialists, but their unhappiness with their PCP experience is growing.
50% of patients leave office
visits not understanding what the physician told them
Why PCMH should be done now? The current system does not work and key to its reform is primary care
Increasing unsustainability of healthcare system – mounting cost, quality and access issues- Impacting economic viability of industries, governments- Impacting resources for other investments needed for sustainable economic growth
- Studies estimate that if every American had access to PCMH, national healthcare expenditures would drop 5.6%, or a savings of at least $67B per year
Increasing focus on wellness/prevention – pillars of primary care- For example, $1B in the “American Recovery and Reinvestment Act”
Can be done now without robust IT infrastructure but not scalable
Challenge Highlights
Why should it be done now?
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 16 © Copyright IBM Corporation 2009
Patient Outcomes/Loyalty Patient Satisfaction/Activation Physician Leadership/Ownership Chronic Disease Management Patient Centered Focus Patient Compliance Employee Productivity
PCMH helps address systemic cost, quality, and access issues
Costs ED Visits PMPY Redundant Tests Unnecessary treatment Hospital stays and readmits PMPY Overall mortality
Potential impacts of PCMH
Why should it be done now?
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 17 © Copyright IBM Corporation 2009
Why it can be done now? There is a growing evidence that PCMH can work
Others have done it and demonstrated success- Various focused, regional approaches have worked (next slide)
Technology/IT can support and enable- Integrate and synthesize data from multiple sources into actionable information
- Ability to disseminate data and standards- Guidelines/best practice work flows/ coordination
- Clinicians and patients are using technology today
Momentum and public awareness of need for change- Increasing awareness that change is inevitable- Dichotomy between cost and outcomes
Why should it be done now?
If the U.S. is serious about closing the quality chasm, it will need a strong primary care system, which requires fundamentally reforming provider payment, encouraging all patients to enroll in a patient-centered medical home, and supporting physician practices that serve as medical homes with the information technology and technical assistance for redesigning care processes.
- Karen Davis, President, Commonwealth Fund
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 18 © Copyright IBM Corporation 2009
RI
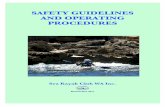
To date, more than 30 PCMH pilots have been initiated and many are demonstrating cost, quality and access improvements
Multi-Payer pilot discussions/activity
Identified pilot activity
No identified pilot activity
“Voice of Detroit Initiative” – 25K uninsured•Reduced ED use by over 60%. •Reduced costs from uncompensated care by 42%•Among homeless and substance abuse patients, reduced hospitalizations by 55% and reduced cost of care by 24%
Community Care of NC (CCNC) – 785K Medicaid enrollees• Asthma: 34% lower hospital admission rate; 8% lower ED rate;
average episode cost for enrolled children was 24% lower; 93% received appropriate inhaled steroid
• Diabetes: 15% increase in quality measures• Program savings: 13% lower ED rate; ~$150M in last fiscal year
BCBS of North Dakota - Diabetes care management• Reduced hospital admissions by 6%, reduced ED visits by 24%• Improved patient satisfaction with care, • Program savings of $1213 per patient ($233,000 total) (2006)
Geisinger Health System – Integrated delivery network in Western Pennsylvania
• Reduced hospital admissions by 20%• Reported medical cost savings of 7%
Why should it be done now?
Horizon BCBS New Jersey•7300 diabetics
•Improved compliance•Reduced costs 10%
BCBS Michigan – new •1,000 physicians•Increased payments•2 million patients•$30 million in incentives
Source: Patient Centered Primary Care Collaborative (http://pcpcc.net/), IBM Healthcare and Life Sciences, IBM Institute for Business Value

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 19 © Copyright IBM Corporation 2009
PCMH is also drawing support from key stakeholder groups and is being bolstered by lawmakers
PROVIDERS•Primary care associations (333,000 physicians)•Associations representing integrated delivery networks, academic medical centers, community hospitals (4,000)
PURCHASERS•Most Fortune 500 (100M lives)•Federal, State Governments
Medicare: Demonstrations from H.R. 6111 – “Tax Relief and Health Care Act”; more Medicare implementations
Medicaid: NC, MO, LA already planning and implementing; Transformation Grants
S-CHIP: Language to encourage transition to medical home model
Health IT Legislation and SGR Reform: Medical home language, encouragement for PCPs to adopt support systems
Quality Improvement Organization 9th Scope of Work Language
Medicaid Transformation Grants
Legislation Highlights
SUPPLIERS•Pharmaceutical and medical device companies •Solution providers
HEALTH PLANS•Health plans including Aetna, BC/BS, Cigna, Humana, MVP Health Care and United Healthcare
CONSUMER ADVOCATES•Unions•Special interest groups
Supporters of the Patient Centered Primary Care Collaborative
Why should it be done now?
Source: Patient Centered Primary Care Collaborative (http://pcpcc.net/), IBM Healthcare and Life Sciences, IBM Institute for Business Value

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 20 © Copyright IBM Corporation 2009
There are demonstrable benefits to the Patient, as well as to caregivers who work at the “top of license” in an integrated team
Patient- Help from a trusted resource to navigate healthcare system- Empowered to make better-informed healthcare decisions- Receive safe, effective care with compassion- Achieve healthier outcomes collaboratively with extended
care delivery team- Improved relationship with PCP, health plan
Primary care provider- Redefine patient relationship to deliver more
comprehensive, coordinated care- Fair compensation for PCMH services, as well as rewards
for improved clinical outcomes- Through a shift in incentives, able to more effectively
provide wellness and preventative care- Better supported to deliver quality care to patients
Nurse- Develop better relationship with patients- More involvement with patient care and support (for
example, patient education, behavioral change, preventive care, proactive care planning)
Pharmacist- Participate fully in team-based care (for example, help
determine medication and reasonable formularies)
Social worker- More integrated role to address key patient needs (for
example, Medicaid)
Hospital- Serve PCMH patients whose conditions may not be as
severe as non-PCMH patients- Potentially reduce admissions from patients who cannot
pay- Potentially reduce number of re-admissions, for which
there may no or reduced payment.
Specialist- Receive higher quality referrals, with more complete
documentation- Improved focus on area of expertise without having to
assume management of patient’s primary care- Opportunity to offset income losses by participating in
financial incentives for coordination and quality (for example, telephone consultations).
Potential benefits by stakeholder
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value
Why should it be done now?

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 21 © Copyright IBM Corporation 2009
PCMH also offers potential benefits to Payers, the Life Sciences, and Governments
Health plan- Improved member and employer satisfaction- Expend healthcare resources with less waste and
greater effectiveness though coordinated evidence-based care.
Employer- Purchase healthcare based on value and
potentially see medical cost savings- Maintaining more present and productive
workforce, in part, through improved wellness and prevention.
Pharmaceutical and other life sciences- Improved appropriateness of and compliance with
therapeutics- Enhanced pharmacovigilance of products, post
clinical trials.
Government- Potential to improve care quality, reduce wasteful
healthcare expenditures- Address frustration with the current uncoordinated
and impersonal system.
Communities and society- Potential for a healthier, more productive citizenry- Potential to allocate dollars so that they have
greater return.
Potential benefits by stakeholder (continued)
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value
Why should it be done now?

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 22 © Copyright IBM Corporation 2009
Agenda
Introduction
The medical home: What is it? What isn’t it?
Why should it be done now?
How should it be done?
Conclusion
Agenda

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 23 © Copyright IBM Corporation 2009
When correctly implementing a PCMH pilot, key steps must be taken to help ensure consistent alignment with the problem at hand
What is the problemWhat is the Problem?
• What cost/quality/ access issue(s) are you targeting?
• Near, long term?• What are your vision, guiding principles?
What are CommonImplementation
Issues?
• Incentives to participate
• Members/patients• Initial funding• Governance• Key metrics• Reimbursement• Physician practice transformation
• Technology infrastructure
• Patient attribution• Sustainability
What is the problemWhat are the Best Practices?
• Who else has addressed our problem?
• What can we learn from them to address our key implementation issues?
Is Our ApproachConsistently Aligned
With Problem We are Trying
to Solve?
•Do you have…• An appropriate
governance structure with the right participants?
• An agreed-upon project plan and strong project manager?
• Capabilities to support the patient cohort?
• Metrics to measure alignment with and progress toward original objectives?
How should it be done?
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 24 © Copyright IBM Corporation 2009
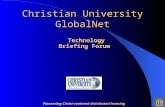
Registration, MH assignment, billing, contracting, compliance with contract
Access to appointments, non-visit advice and help
Clinical Preventive services
Acute Care, ER and UCC Management
Patient Activation & Behavior Change
Social & Mental Health Services
Medication Monitoring
Diagnosis and Drug Management
Specialists
High-risk Care Management
0% 25% 50% 75% 100%
Medical Home Multidisciplinary Team
Clerical
Nursing
Physician, PA, NP
Social Work
Pharmacy & Nursing
Volume of services
All team members collaboratively contribute at the “top of their licenses,” helping the overall practice operate more efficiently and effectively
Source: Adapted with permission by IBM from F. Daniel Duffy, MD, MACP, Senior Associate Dean for Academics, University of Oklahoma School of Community Medicine
How should it be done?
Sample medical home PCP practice
Sample Implementation Issue

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 25 © Copyright IBM Corporation 2009
Key Metrics – Measurement and evaluation processes are critical because of their effects on incentives, resulting organizational learning and other factors
To date, medical home efforts have used a combination of the following types of key metrics:- Costs: Impacted by things like the types and number of patients, as well as duration of initiative- Process of care: Include appropriate screening for traditional conditions, alignment with NCQA
accreditation measures or targeted conditions that are endemic to local population- Outcomes of care: Measures change in health for a patient or a cohort, such as individual
conditions and patient compliance (e.g., tracking HbA1c) or utilization (e.g., ER visits)- Service: Have focused on operational aspects, such as the wait until the next appointment- Patient and caregiver satisfaction: Demonstrates the PCMH initiative’s commitment to quality
and in improvements by assessing the satisfaction of patients and clinicians- Coordination of care: Are more innovative but require a sophisticated tracking system
University of Oklahoma is developing a set of measures that accounts for the rapidity of referrals and getting the referral and includes quality and process measures
Sample assessment questions for include the following:- Is there an agreed-upon set of metrics that are aligned with your original problem?
Pilot phase? Full roll out?Regular updates?
- Is the data needed easy to collect, analyze, report, and act upon?
How should it be done?
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value
Sample Implementation Issue

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 26 © Copyright IBM Corporation 2009
Agenda
Introduction
The medical home: What is it? What isn’t it?
Why should it be done now?
How should it be done?
Conclusion
Agenda

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 27 © Copyright IBM Corporation 2009
There is no reason to wait to invest in the medical home but invest wisely
The medical home is not a “silver bullet” but can become a cornerstone for revamping primary care – an essential component of the overall transformation of U.S. healthcare
To support medical homes, we need better clinical evidence, changes in responsibilities of key stakeholders, and a cross-organizational infrastructure to support coordinated care
It will not be easy to implement medical homes on a large scale even with the current momentum behind them, given challenges such as funding and the level of change required
Fortunately, best practices are emerging for common issues related to planning and implementation - When appropriately applied, they can help increase the likelihood of success for an initial
rollout and for a sustainable model
Source: IBM Healthcare and Life Sciences, IBM Institute for Business Value
Conclusion

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 28 © Copyright IBM Corporation 2009
For more information, please contact
AuthorsJim Adams, MBA
Executive Director, IBM Center for Healthcare ManagementE-mail: [email protected]
Paul Grundy, MD, MPH, FACOEM, FACPMGlobal Director of Healthcare Transformation, IBM
E-mail: [email protected]
Martin S. Kohn, MD, MS, FACEP, CPESenior Managing Consultant,
IBM Healthcare Strategy and Change practiceE-mail: [email protected]
Edgar L. Mounib, MBA, MPHGlobal Healthcare Lead, IBM Institute for Business Value
E-mail: [email protected]
Guest SpeakerF. Daniel Duffy, MD, MACP
Senior Associate Dean for Academics,University of Oklahoma School of Community Medicine
E-mail: [email protected]
Beginning May 28th, download study atwww.ibm.com/healthcare/medicalhome

Patient-Centered Medical Home: What, why and how? | Briefing | Apr 11, 2023 29 © Copyright IBM Corporation 2009
Thank you!