
Iatrogenic occlusion of the ophthalmic artery after cosmetic facial filler injections
59
Iatrogenic Occlusion of the Ophthalmic Artery After Cosmetic Facial Filler Injections A National Survey by the Korean Retina Society JAMA Ophthalmology, June 2014
-
Upload
iam-ami -
Category
Healthcare
-
view
120 -
download
0
Transcript of Iatrogenic occlusion of the ophthalmic artery after cosmetic facial filler injections

Iatrogenic Occlusion of the Ophthalmic Artery After Cosmetic Facial
Filler InjectionsA National Survey by the Korean Retina Society
JAMA Ophthalmology, June 2014
AUTHORS
• Kyu Hyung Park, MD, PhD• Yong-Kyu Kim, MD• Se JoonWoo, MD, PhD • SeWoong Kang, MD, PhD• Won Ki Lee,MD, PhD• Kyung Seek Choi, MD, PhD• HyungWoo Kwak, MD, PhD• Ill Han Yoon, MD, PhD• Kuhl Huh, MD, PhD• JongWoo Kim, MD, PhD


INTRODUCTION
• Increasing interest in aesthetics and rejuvenation has led to a recent dramatic increase in the number of aesthetic procedures performed
• Various materials are used for facial filling, with autologous fat, hyaluronic acid, collagen, and biosynthetic polymers


Hyaluronic Acid
• Restylane®– Stabilized hyaluronic acid – Produced from the
fermentation of equine streptococci with 1% cross-linking
– Concentration is 20 mg/ml– Gel particle size is 400 μm
Can block the central retinal artery (Ø160μm), or smaller branch retinal arteries more easily
than the ophthalmic artery (Ø2mm)

Autologous Fat
• Autologous fat has a variable particle size and can block various sized arteries

INTRODUCTION
• Blindness after cosmetic facial filler injections is a rare but severe complication, with only fragmented case reports that was not uniformly designed and did not represent a comprehensive summary of clinical features

OBJECTIVE
• To investigate clinical and angiographic features of iatrogenic occlusion of the ophthalmic artery and its branches caused by cosmetic facial filler injections

DESIGN, SETTING, & PARTICIPANTS
• Retrospective• A national survey by members of the Korean
Retina Society from 27 retinal centers• 44 patients with occlusion of the ophthalmic
artery and its branches after cosmetic facial filler injections

MAIN OUTCOMES
• Visual prognosis and its relationship to angiographic findings and injected filler material

METHODS
• December 1, 2012 May 30, 2013• Survey case report forms

DATA
• Clinic type• Injection site• Injected filler material• Demographic data• Initial symptoms & signs• Examination results
• Fundus photographs• Fluorescein
angiography (FFA)• Indocyanine green
angiography (ICG)• Optical coherence
tomography (OCT)• Visual field tests (VF)• Electroretinography
(ERG)

CLASSIFICATIONS
1. Ophthalmic artery occlusion (OAO)2. Generalized posterior ciliary artery
occlusion (PCAO) with relative central retinal artery sparing
3. Localized PCAO4. Central retinal artery occlusion (CRAO)5. Branch retinal artery occlusion (BRAO)6. Posterior ischemic optic neuropathy (PION)

BCVA LogMAR
• Counting fingers = 2• Hand movements = 2.3• Light perception = 2.6• No light perception = 2.9

STATISTICAL ANALYSES
• Statistical analyses– Mann-Whitney test– Kruskal-Wallis test– χ2 test– Fisher exact test
• SPSS version 18• P < .05 was considered statistically significant

Results

DEMOGRAPHIC DATA
Young women(mean age, 35.8 years; 93% [41 of 44] female)
84% patients sought medical attention within
1 day of symptom onset, which occurred immediately after filler
injections
Autologous fat (50% [22 of 44])
>Hyaluronic acid(30% [13 of 44])
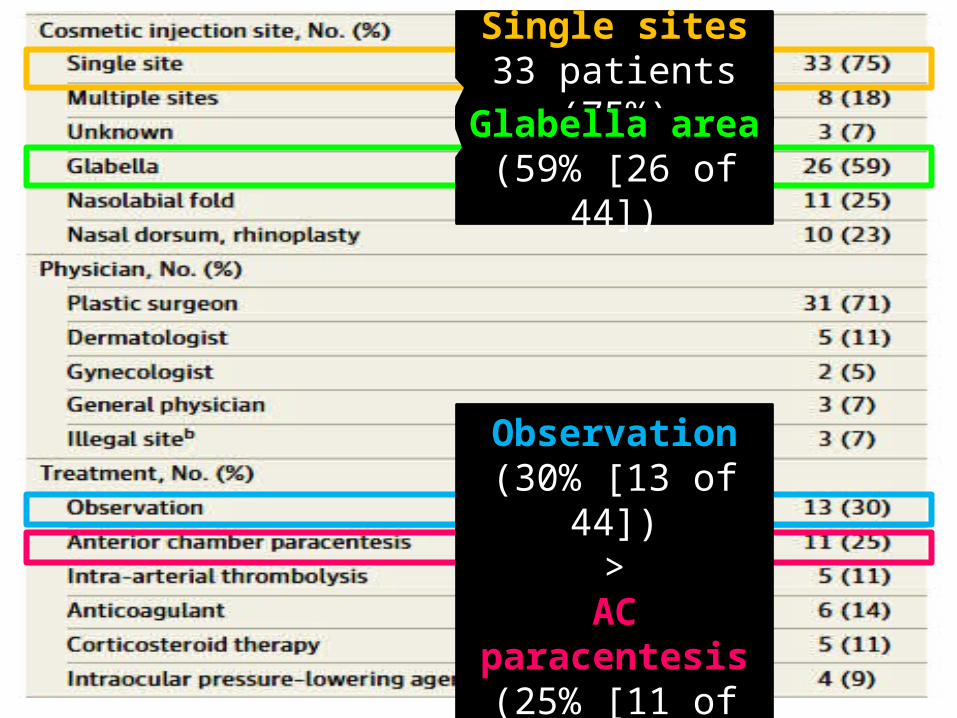
Single sites33 patients (75%)
Glabella area(59% [26 of 44])
Observation(30% [13 of 44])
>AC paracentesis (25% [11 of 44])

Brain infarction(39% [12 of 31])
Poor visual prognosis;27 patients (61%)
final VA = NLP

1. VA decrease [84%]
2. Ophthalmoplegia [50%]3. Ocular pain / Skin lesion
[39%]
1. VA decrease (15 of 21 [71%])
2. Strabismus (7 of 21 [33%]) 3. VF defect (3 of 21 [14%])..6. Phthisis bulbi (1 of 21 (5%)

Ophthalmic Artery Occlusion (OAO)
*

I. Ophthalmic Artery Occlusion (OAO)
• 17 of 44 patients• OAO = both retinal & choroidal insufficiency• Fundus = diffuse retinal whitening• FFA & ICG = severely compromised retinal &
choroidal filling• MRI brain = 60% [9 of 15] showed focal or
diffuse brain infarction

First visit; NPL

ERG
Rod Cone
*
*
*
*
*

FFA ICG
MRIbrain
3 months later; NPL

I. Ophthalmic Artery Occlusion (OAO)
• Poor visual prognosis (after F/U 14.4 ± 15.4 months was NLP in all patients)
• Autologous fat injections (71% [12 of 17])• Ophthalmoplegia or strabismus (77% [13 of
17]), ocular pain (65% [11 of 17])
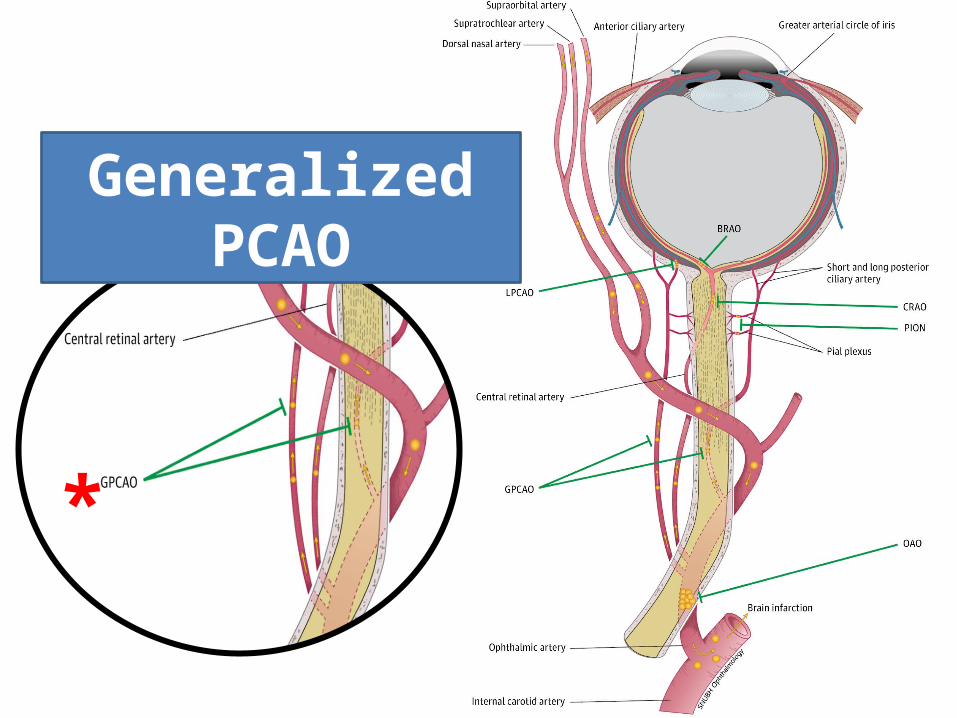
Generalized PCAO
*

II. Generalized PCAO With Relative Central Retinal Artery Sparing
• 3 of 44 patients• GPCAO = generalized choroidal ischemia
with spared retinal circulation• Initially, only focal retinal edema was present• Within 3 days, the inner retina became
compromised, finally optic atrophy• Poor visual outcomes (final BCVA of NLP in
all 3 patients)

First visit; FCFFA
FFA FFA
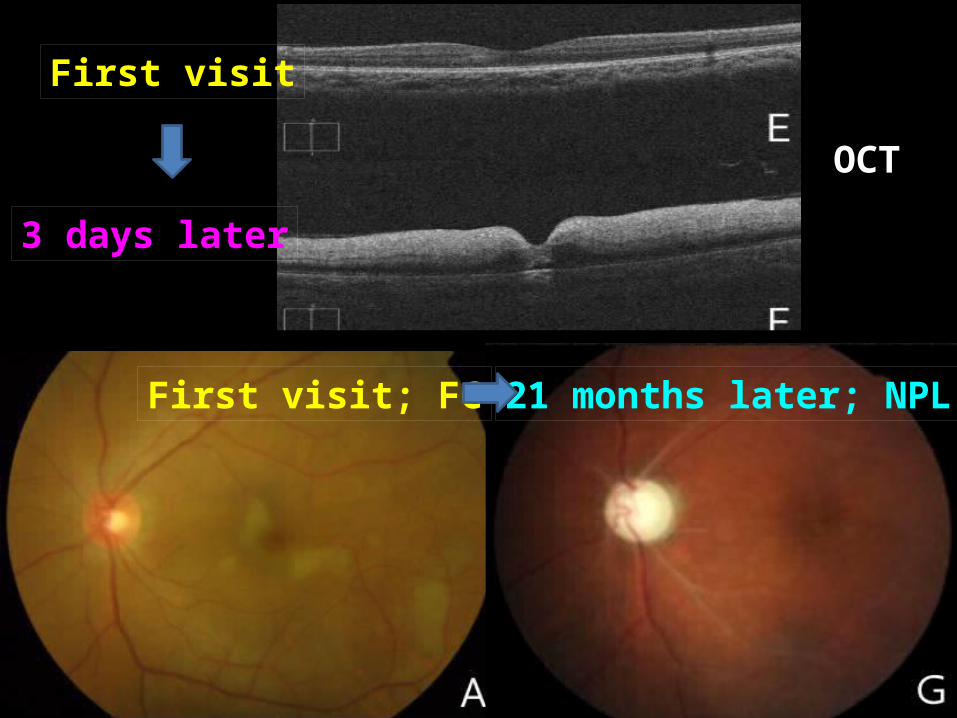
First visit; FC 21 months later; NPL
First visit
3 days later
OCT

Central Retinal Artery Occlusion
(CRAO)
*
III. Central Retinal Artery Occlusion (CRAO)
• 8 of 44 patients• CRAO = compromised retinal circulation
(prominent) & reduced choroidal perfusion• Fundus = “cherry-red spot”• OCT = severe inner retinal edema• Autologous fat injections (75% [6 of 8])• Poor visual prognosis (final BCVA of NLP in 6
of 8 patients)

First visit; NPLFFA
FFA OCT

Localized PCAO
*

IV. Localized PCAO
• 4 of 44 patients• LPCAO = localized choroidal ischemia, with
no compromising of the retinal or remaining choroidal circulations
• Good visual prognosis (unaffected macula)• 2 patients can resolve anterior segment
ischemia (corneal edema & AC reaction)• No cases of autologous fat injections

First visit; 20/32 Final VA 20/25FFA
FFA FFA

Branch Retinal Artery Occlusion
(BRAO)
*

V. Branch Retinal Artery Occlusion (BRAO)
• 10 of 44 patients• BRAO = localized retinal ischemia• Fundus = localized retinal edema• Good visual prognosis in most cases• 2 cases [20%] of autologous fat filler

FFA
OCT VF

Posterior Ischemic Optic Neuropathy
(PION)
*

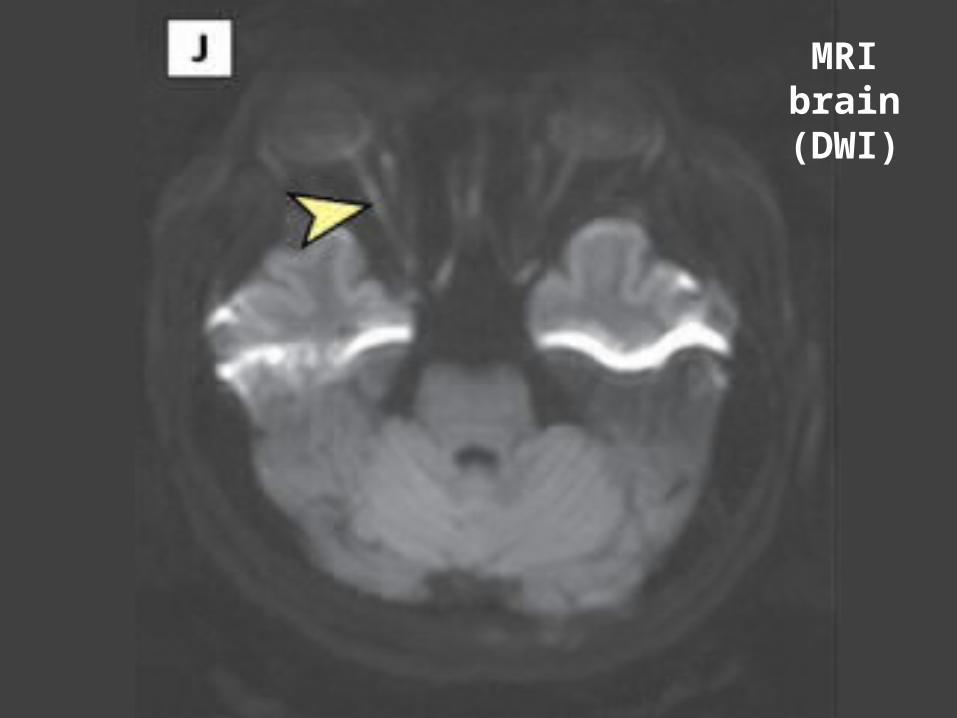
VI. Posterior Ischemic Optic Neuropathy (PION)
• 2 of 44 patients• Sudden onset of eyeball deviated laterally,
diplopia, blurry vision, and eyeball pain• Normal fundus, FFA & ICG, ERG• VEP = delayed latency & reduced signal
amplitude• MRI brain = focal high–signal intensity lesion
at retrobulbar optic nerve• Poor visual outcome

*
MRI brain (DWI)

Diffuse vs Localized Occlusion
• Diffuse (28 patients) OAO, generalized
PCAO, CRAO Generalized
decreases in retinal or choroidal perfusion and involved the retina and choroid as a whole
• Localize (16 patients) Localized PCAO,
BRAO, PION Focal vascular
compromise in the retina or choroid

Diffuse vs Localized Occlusion
• Diffuse occlusions had higher rates of – Autologous fat injections• (68%[19 of 28] vs 19%[3 of 16], P = .002)
– Brain lesion on MRI• (50%[12 of 24] vs 0%[0 of 7], P = .02)
– Ocular pain• (54%[15 of 28] vs 13%[2 of 16], P = .01)
• Visual prognosis was also poor in the diffuse occlusion group (initial, final, and gain VA)

Autologous Fat vs Hyaluronic Acid
• Autologous fat injections had higher rates of – Diffuse occlusions
• (86%[19 of 22] vs 39%[5 of 13], P = .007)– Worse VA
• (mean final BCVA, 2.6±0.8 vs 1.4±1.4; P = .01)– Lower visual gain
• (mean, −0.1±[−0.2] vs 0.3±[0.6]; P = .02)– Long-term visual loss
• (100%[9 of 9] vs 43%[3 of 7], P = .02) – Brain lesions on MRI
• (46%[10 of 22] vs 8%[1 of 13], P = .03)

Autologous Fat vs Hyaluronic Acid
• Hyaluronic acid injections had higher rates of – Anterior segment ischemia• Corneal edema (39%[5 of 13] vs 5%[1 of 22], P = .02)• AC inflammation (54%[7 of 13] vs 0%[0 of 22], P < .001)
• No significant differences were observed between the groups in the number of injections or the site of injection

Discussion

This Study
• This is the largest case series reported to date on ocular complications following cosmetic facial filler injections and includes a comprehensive analysis of clinical characteristics of patients according to their angiographic findings and injected filler material

Mechanical Theory
“Retrograde embolic mechanisms”• Anterograde thromboembolism of filler
material to ophthalmic artery origin retrograde embolic to central retinal artery & posterior ciliary artery particle dispersion into each arterial branch obstruction


Entry Point
• Glabellar region1. Supratrochlear artery2. Supraorbital artery
• Nasolabial fold1. Anastomosis of the dorsal nasal artery2. Angular artery3. Lateral nasal artery

**
*
**

Autologous Fat Injections
• A previous study; size variation in injected particles leads to different occlusion
• Fat is usually injected using a large-bore needle (14G to 18G), aiming to overcorrect the cosmetic defect
• High volume & high pressure of fat injection multifocal & complete obstruction of the ophthalmic artery and its branches

Cerebral Infarction
• Cerebral infarction was more frequently observed in autologous fat–associated retinal artery occlusions
• A previous study; most cases occurred after autologous fat injections
• It seems that fat particles are directly injected into the internal carotid artery system in a retrograde fashion

LIMITATIONS
• Retrospective design– Could not directly calculate the ocular
complication incidence– Not designed to identify risk factors that might
mitigate complications, such as• Type of needle used (sharp vs blunt cannula)• Gauge of the instruments• Depth or total volume of the injection

CONCLUSIONS
• Clinical features of iatrogenic occlusion of the ophthalmic artery and its branches following cosmetic facial filler injections were diverse according to the location and extent of obstruction and the injected filler material
• Autologous fat injections were associated with a worse visual prognosis and a higher incidence of combined cerebral infarction

THANKYOU


















