Hyponatremia- Fishing in troubled waters.
58
Hyponatremia – Fishing in troubled waters K.SAMPATHKUMAR . MD, DNB, DM, FISN,FRCP ( Glasgow) MEENAKSHI MISSION HOSPITAL MADURAI, INDIA
-
Upload
drk-sampath-kumar -
Category
Health & Medicine
-
view
165 -
download
1
Transcript of Hyponatremia- Fishing in troubled waters.
Hyponatremia – Fishing in troubled waters
K.SAMPATHKUMAR . MD, DNB, DM, FISN,FRCP ( Glasgow)
MEENAKSHI MISSION HOSPITAL MADURAI, INDIA

Homer Smith

Crucial role of Kidneys in evolution‘Mileu interior’
Danger of osmotic lysis
Kidneys provide “milieu interior”

Hyponatremia < 135 mEq/L
True = Hypo osmolar Plasma
Water excess state


Osmolality of various body fluid compartments govern the fluid and solute distribution
• Plasma Osmolality:Calculated
Posm = 2 (Na) + glucose + urea
Normal = 2 (140) + 5 + 5 = 290 (275-290 )• Effective Osm= Remove urea from eq.• Measured Osmolality- Osmometer- Freezing point
depression
• Osmolal gap= Mannitol,urea,glycine etc

S.Na ~ Na e + K e
TBW
K 140 Na – 140
280 mOsm
280 mOsm
25 L 17 L
H2O balance – ICF VolumeNa balance – ECF Volume
Na,KATPase

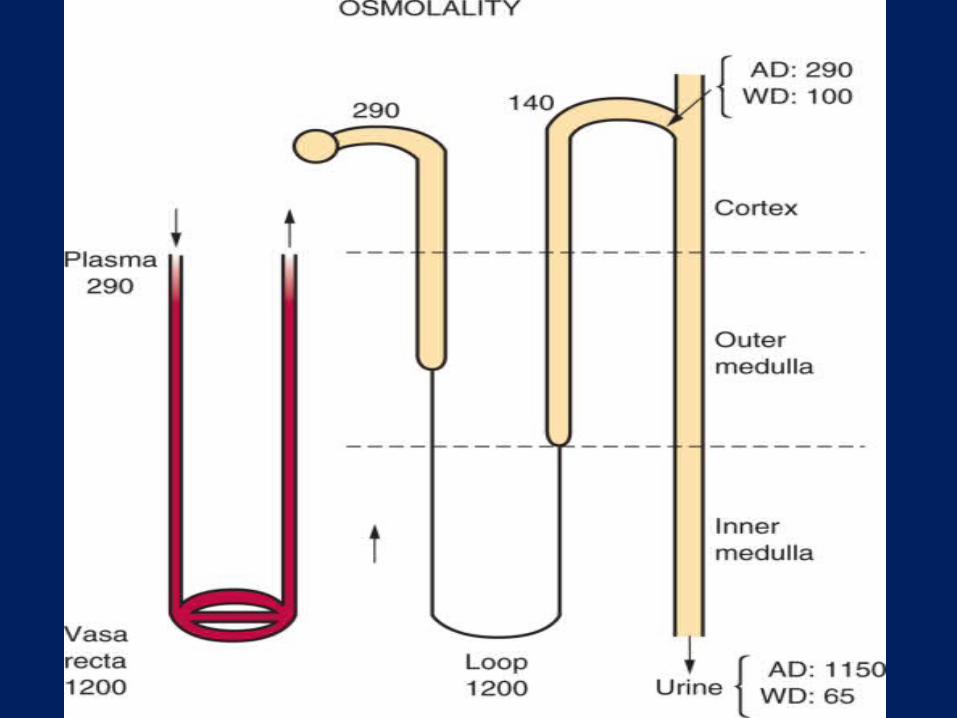
Kidney’s capacity to concentrate and dilute the urine
AVERAGE U Osm = 400. 1.5 L of Urine to excrete 600 mOsm

Hyponatremia – Basics
Na + K
Total Body Water
Loss of Na,K
Excess water IntakeRetention
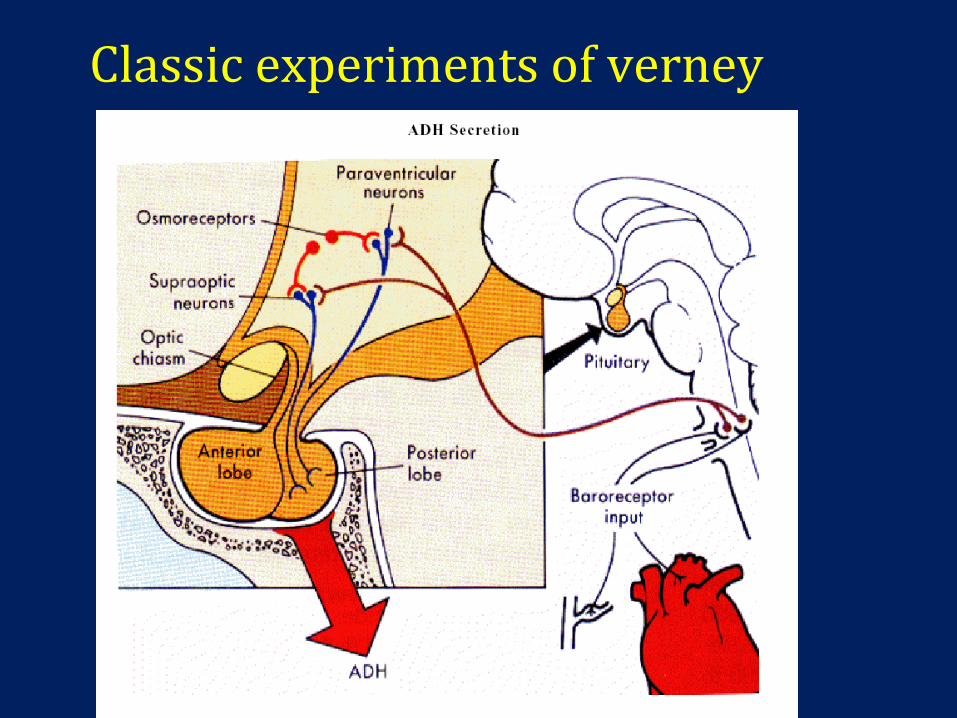
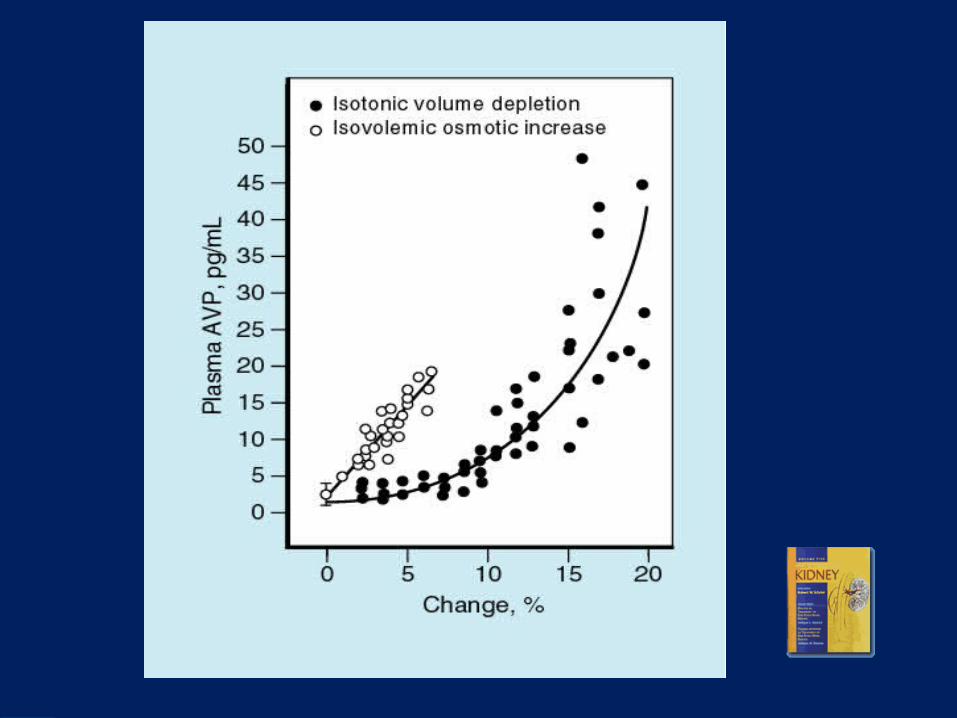
Classic experiments of verney

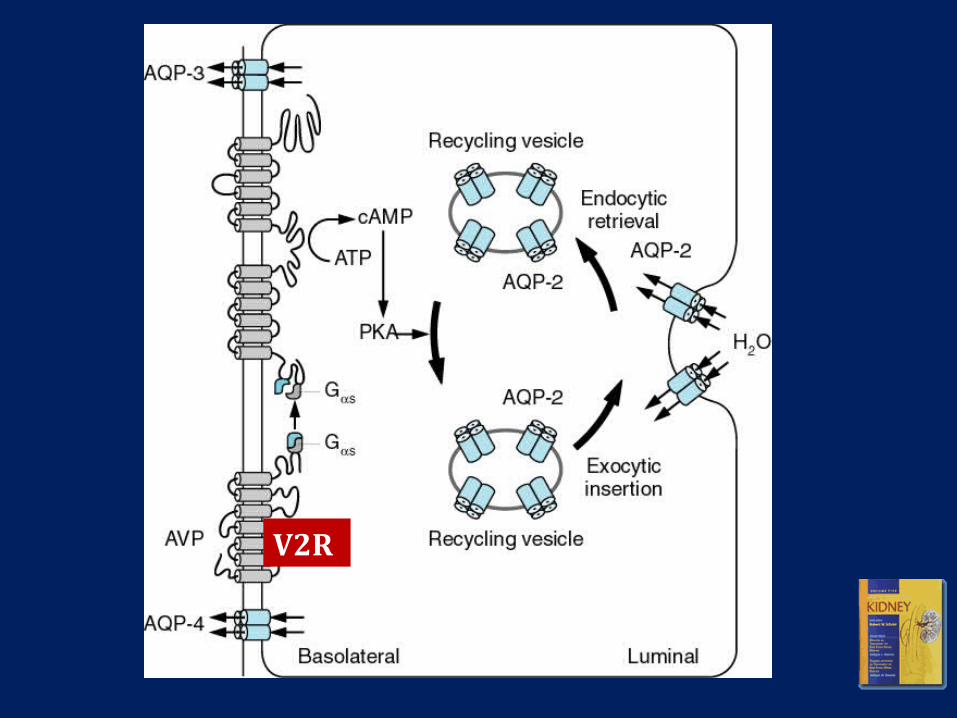
V2R

5
0
1200
50
140
130
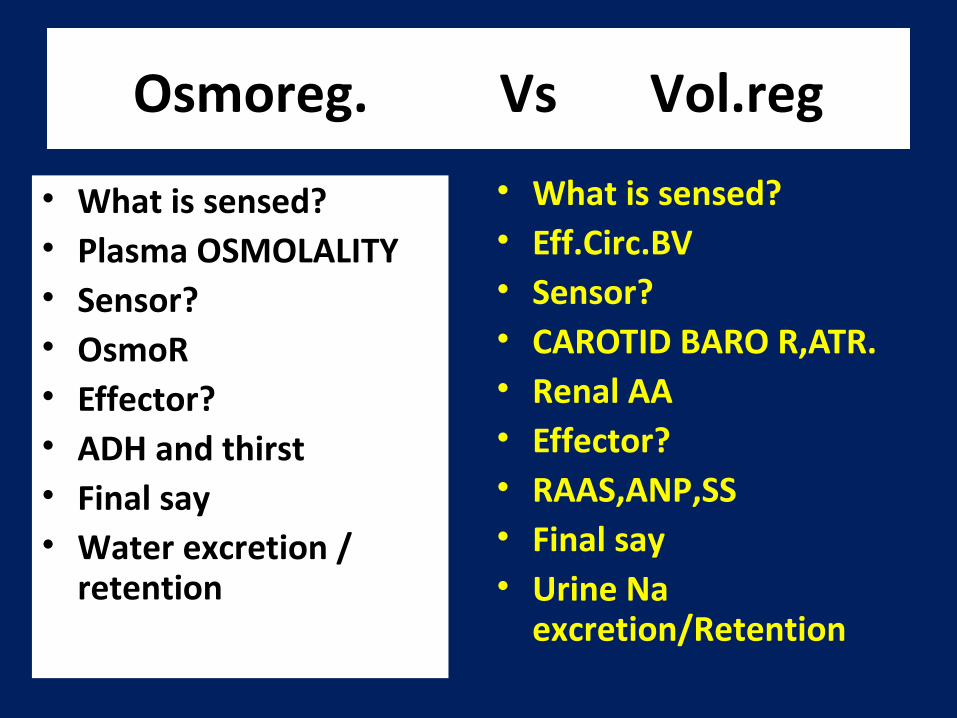
Osmoreg. Vs Vol.reg
• What is sensed?• Plasma OSMOLALITY• Sensor?• OsmoR • Effector?• ADH and thirst• Final say• Water excretion /
retention
• What is sensed?• Eff.Circ.BV • Sensor?• CAROTID BARO R,ATR.• Renal AA• Effector?• RAAS,ANP,SS• Final say• Urine Na
excretion/Retention

In volume depletion states when ADH is stimulated which takes
precedence ?
Water is retained more and serum sodium lowered

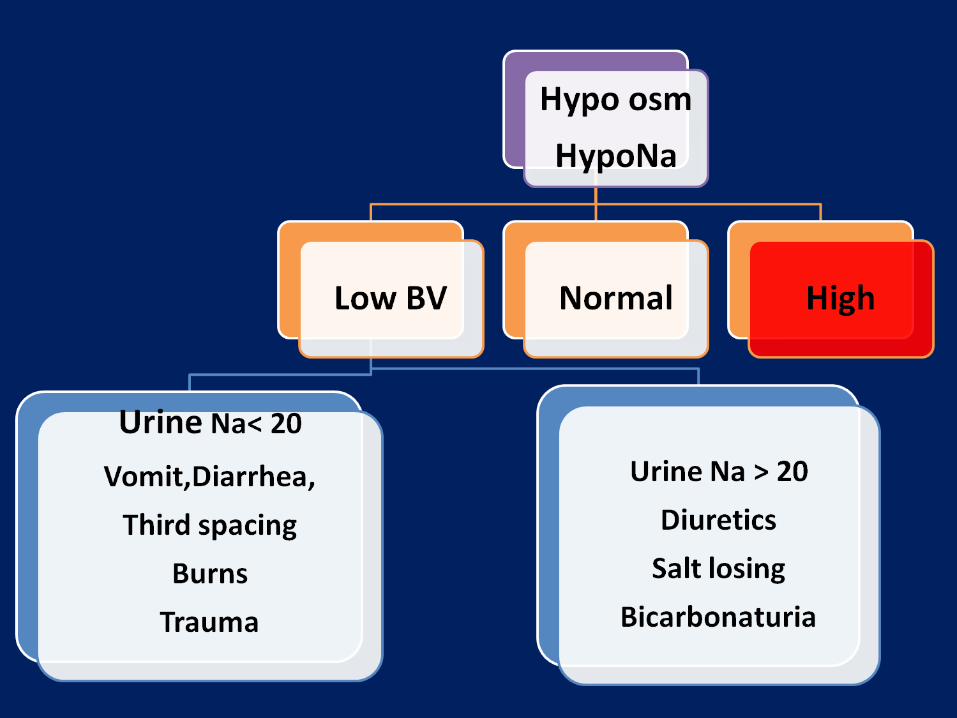
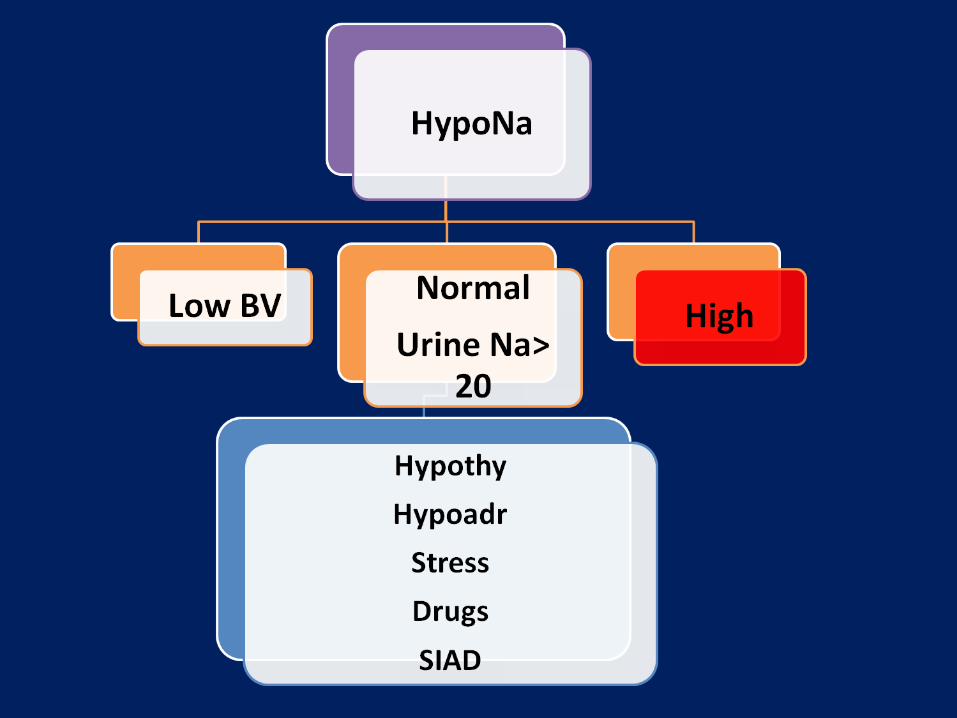
Clinical approach to HypoNa
•1% of healthy population
•5-8 % of hospitalised patients
•30% of ICU patients
Is it serious ?• Marker of severity of underlying disease• CCF.• Cirrhosis.• Advanced cancer.
• Marker of increased mortality
• Treatment may be more deleterious in some !
4 essentials
1. History
2. Plasma osm.
3. Volume status
4. Urine Sodium


Don’t jump to treatment!!Avoid misdiagnosis !
• Sampling error ? Common • Hyperlipidemia ? Use ISE ( Not Flame
Photometer)• Multiple Myeloma ? Use ISE ( - do - )• Hyperglycemia ? Every 100 mg increase in glucose
reduces serum Sodium by 1.6 - 2.4 mEq/L
• Drugs and chemicals? Glycine,Mannitol.

Hyperglycemia – Hyperosmolar hyponatremia
Water
Glucose is osmotically Active
Translocational hyponatremia
Serum osmolality will be high

LOOP D block both conc.and dilution
THIAZIDES BLOCK DILUTION ALONE
Urine Na and K very high Urine Na and K moderate



Management and special situations

Therapeutic Strategy Based On
• 1. Volume Status of Patient• 2. Presence of Absence of Symptoms• 3. Duration of Hypoosmolality• 4. Presence of absence of risk factors for
development of neurological complication
(Osmotic demyelination is rare in patients with initial Na+ > 120mEq/L)
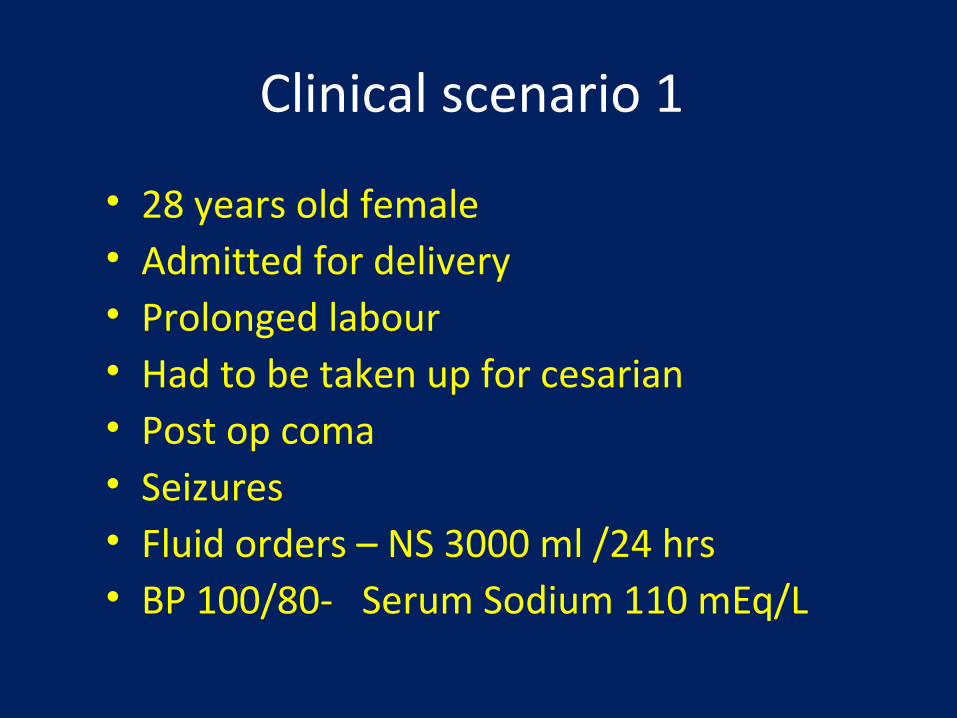
Clinical scenario 1
• 28 years old female • Admitted for delivery• Prolonged labour• Had to be taken up for cesarian• Post op coma • Seizures • Fluid orders – NS 3000 ml /24 hrs• BP 100/80- Serum Sodium 110 mEq/L

Why hyponatremia
Source of free water
Was given Normal saline3 Litres /24 hours
Free water intake due to anxiety
ADH is acting
Post op painAnxietyNausea due to analgesics
DESALINATION syndrome

e- 300 mOsm x 3
900 Mosm
ADH CONCENTRATES
URINE
600 Mosm /L = 1.5 L of urine
3 L of Saline
Thus 1.5 Litres of free water is retained in body !

1.5 L WATER
K 135 Na – 135
270 mOsm
270 mOsm
26 L 17 .5 L
1L
0.5L

Cerebral edema and Brain herniation
36
CNS ENCASED IN SKULL
Neuronal edemaTentorial herniationNeurog.Pul.edema
Acute water excess
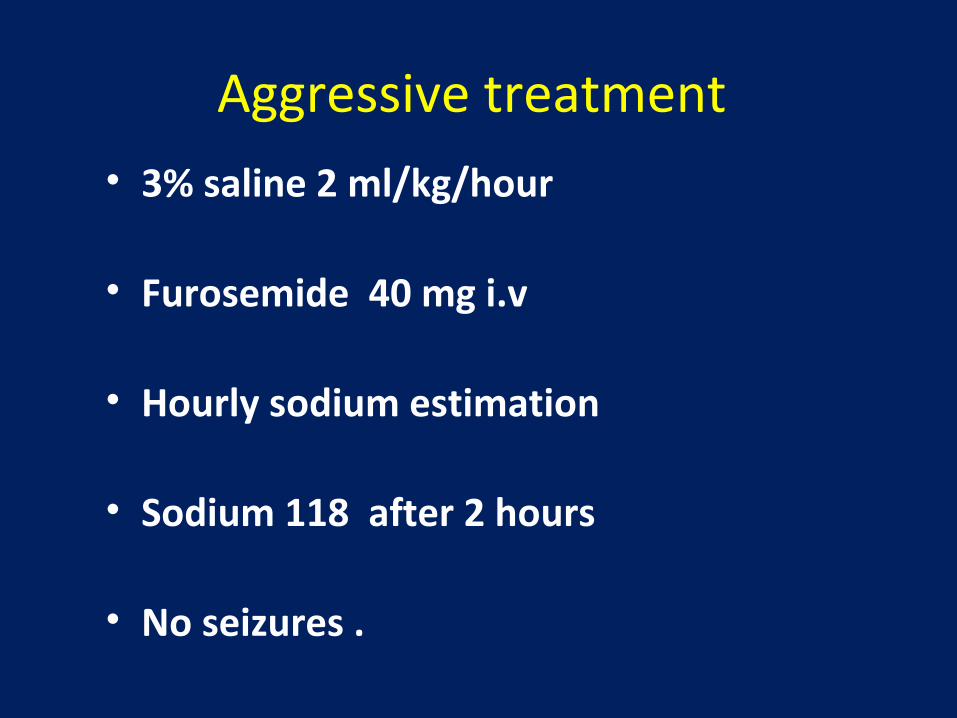
Aggressive treatment • 3% saline 2 ml/kg/hour
• Furosemide 40 mg i.v
• Hourly sodium estimation
• Sodium 118 after 2 hours
• No seizures .

Scenario 2 56 years old maleAlcoholic cirrhosisEdema , AscitesOliguriaSleepinessS.Sodium 113/K 2.3 ?Chronic hyponatremia – beware!
38
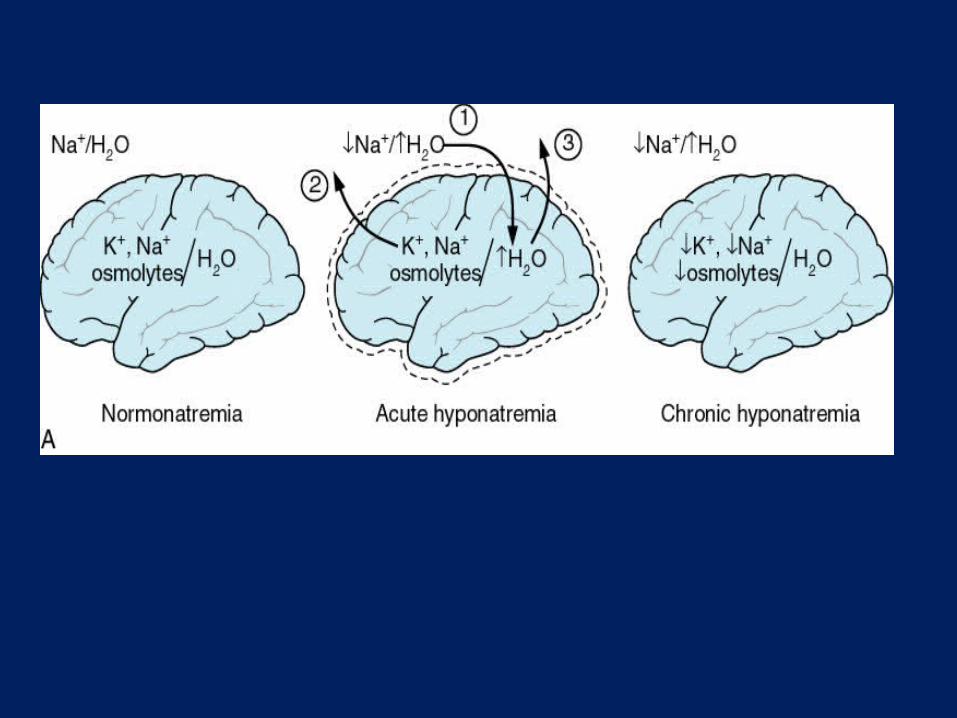
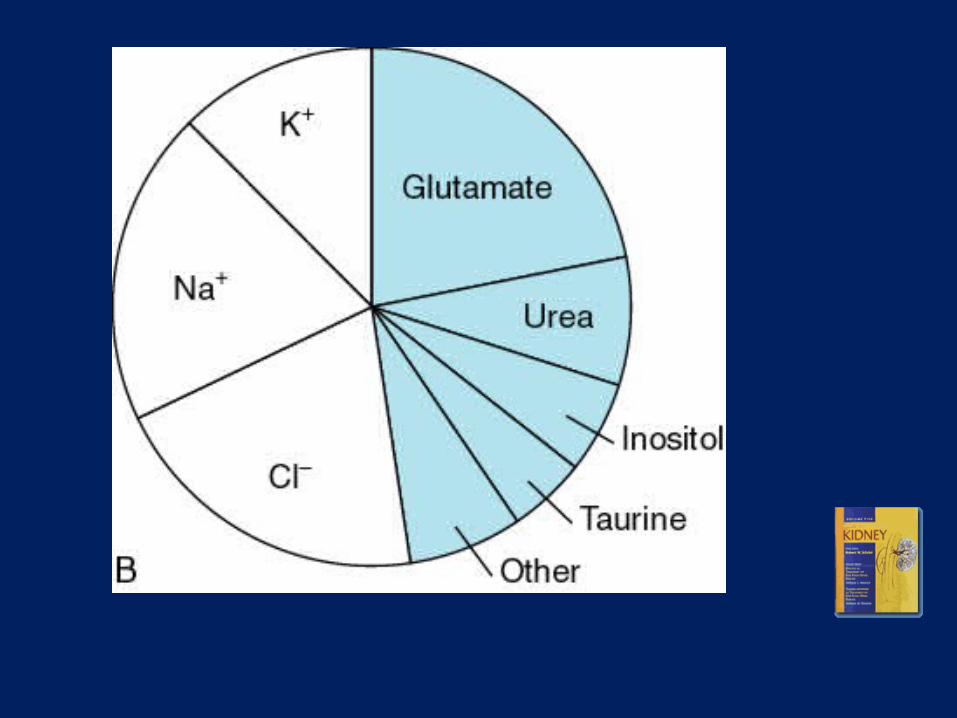

Chronic hyponatremia – Brain adapts to keep the edema within limits
Aminoacids.Myoinositol
Rapid correction leads on to cell shrinkage and Demyelination.

Calculation• 60% of body weight is water • 65 x 0.6 = 39 L• 123-113 = 8 • 39x 8 = 312 Meq needed• 1ml of 3% saline = 0.5 mEq of Na• Sodium deficit = 624 ml• 624 /24 hours = 26 ml/hr• Serum Na measure q2-4 hrs
42
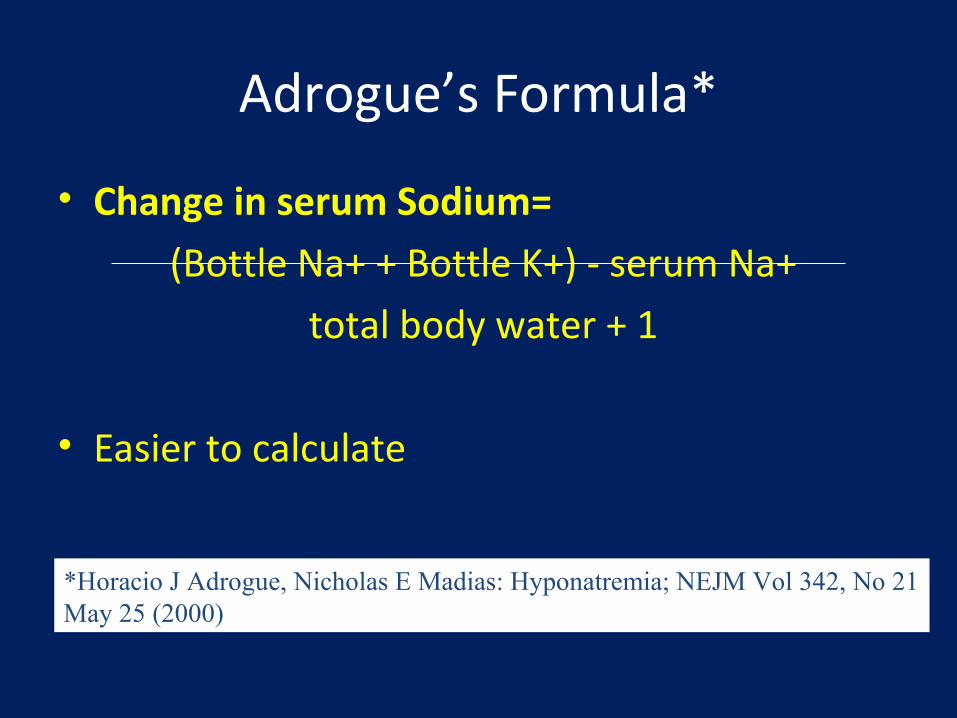
Adrogue’s Formula*
• Change in serum Sodium=
(Bottle Na+ + Bottle K+) - serum Na+
total body water + 1
• Easier to calculate
*Horacio J Adrogue, Nicholas E Madias: Hyponatremia; NEJM Vol 342, No 21May 25 (2000)

Janinic and Verbalis formula
• Rate ml/Kg/Hr = Goal rate of rise mmol/Kg/Hr
• 1ml/kg/hr = 1ml/kg/hr rise in Serum Na
• Ideal for those allergic to Math !!

Chronic hyponatremia
• Water restriction• Demeclorcycline 300 -600 mg tid• Lithium • Oral urea • VAPTANS

K
Na moves into cell producing hyponatremia
19/9/2010
46
Tirunelveli API , TVMC Auditorium

Treat with Intravenous potassium Replenish the IC deficit of Potassium . Sodium automatically comes up If not replaced , then there is danger of
osmotic demyelination.
19/9/2010
47
Tirunelveli API , TVMC Auditorium
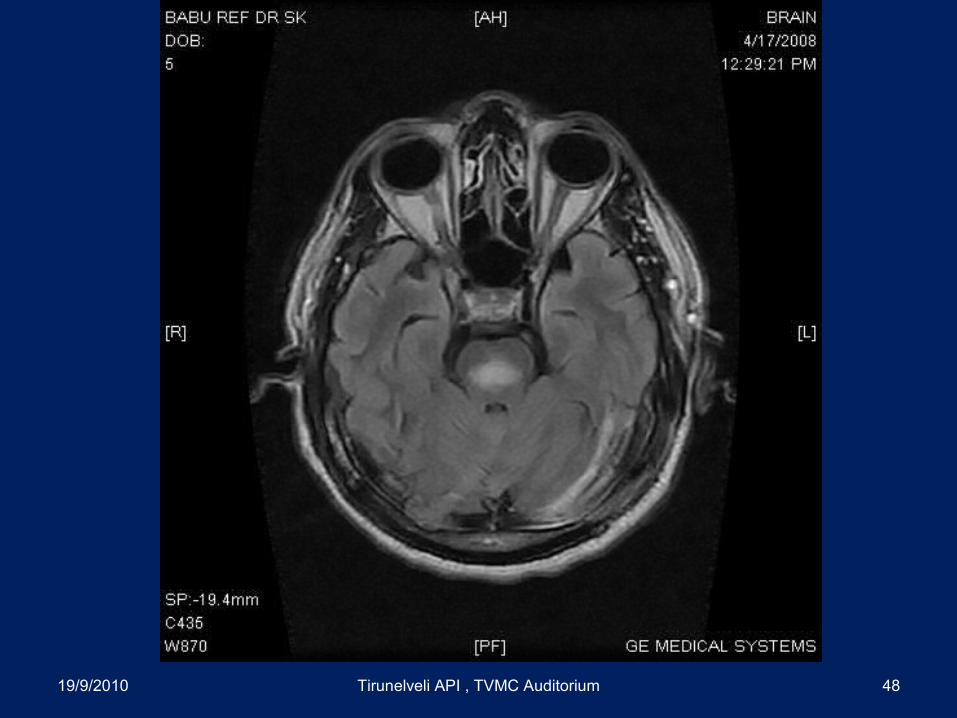
19/9/2010 Tirunelveli API , TVMC Auditorium 48
Insufficient Correction
CEREBRAL EDEMA Herniation
Too Rapid Correction
OSMOTICDEMYELINATION
19/9/2010
49
Tirunelveli API , TVMC Auditorium

Vasopressin receptor antagonists

Vasopressin-Receptor Antagonists.
Ellison DH, Berl T. N Engl J Med 2007;356:2064-2072.

SALT -1 ,SALT-2 and SALTWATER
• Oral Tolvaptan increased the serum sodium levels significantly and safely in CCF,SIAD and Cirrhosis.
• NOT USED IN ACUTE SYMPTOMATIC HYPONATREMIA
• 2 CONCERNS• INCREASED THIRST• OVERLY RAPID CORRECTION OCCURRED in 1.8%• No ODM ENCOUNTERED
VAPTANS –PURE WATER EXCRETION
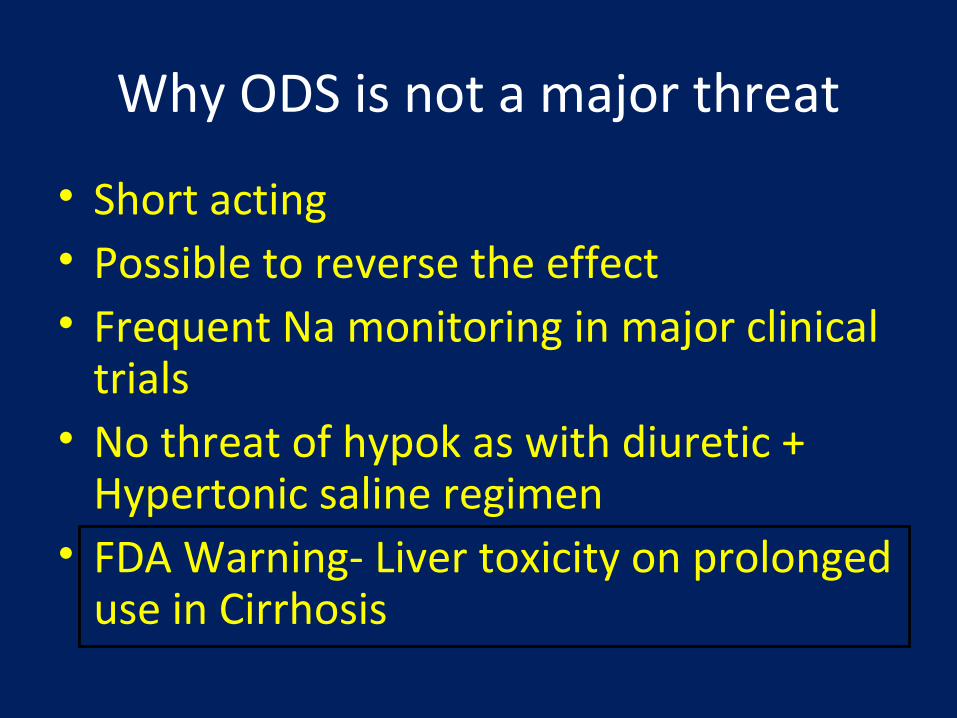
Why ODS is not a major threat
• Short acting • Possible to reverse the effect • Frequent Na monitoring in major clinical
trials• No threat of hypok as with diuretic +
Hypertonic saline regimen• FDA Warning- Liver toxicity on prolonged
use in Cirrhosis

Who should be treated with vaptans
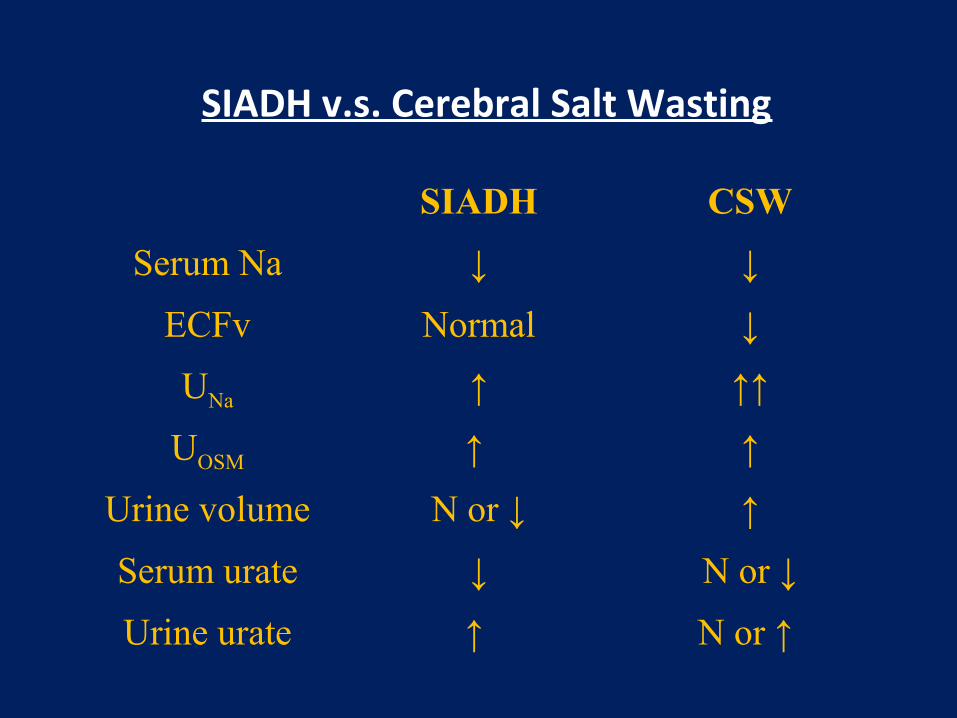
SIADH v.s. Cerebral Salt Wasting
SIADH CSW
Serum Na ↓ ↓
ECFv Normal ↓
UNa ↑ ↑↑
UOSM ↑ ↑
Urine volume N or ↓ ↑
Serum urate ↓ N or ↓
Urine urate ↑ N or ↑

Some Interesting Issues not discussed
• Reset Osmostat• Beer Potomania• Glycine in TURP• Exertional hyponatremia• Ecstacy and hyponatremia

THANK YOU