Hyponatremia - Boston College · 22nd Annual Northeast Regional Nurse Practitioner Conference –...
43
22nd Annual Northeast Regional Nurse Practitioner Conference – May 6-8, 2015 Hyponatremia Kara M. Olivier, NP
Transcript of Hyponatremia - Boston College · 22nd Annual Northeast Regional Nurse Practitioner Conference –...

22nd Annual Northeast Regional Nurse Practitioner Conference – May 6-8, 2015
HyponatremiaKara M. Olivier, NP

D I S C L O S U R E S
• There has been no commercial support or sponsorship for this program.
• The planners and presenters have declared that no conflicts of interest exist.
• The program co-sponsors do not endorse any products in conjunction with any educational activity.

A C C R E D I TAT I O N
Boston College Connell School of Nursing Continuing Education Program is accredited as a provider of continuing nursing education by the American Nurses Association Massachusetts, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.

22nd Annual Northeast Regional Nurse Practitioner Conference – May 6-8, 2015
S E S S I O N O B J E C T I V E S
• Describe the etiology of SIADH.• Discuss the clinical manifestations and
medical management of patients with SIADH.
• Discuss the nursing implications in the care of patients with SIADH.

The Bare Essentials of Hyponatremia and SIADH
Kara M. Olivier, NP

Objectives
Describe the etiology of hyponatremia and SIADH.
Discuss the clinical manifestations and medical management.
Discuss the nursing implications in the care of patients.

Overview
What is the difference between hyponatremia and SIADH? Hyponatremia – Low serum Na
SIADH – Low serum Na and low osmolality
Result of excess water not Na deficiency

Defining Hyponatremia
Abnormally low sodium level
Electrolyte regulates water in and out of cells
Normal serum sodium 135-145 meq/L
Hyponatremia is typically defined as a serum sodium concentration below 135 meq/L

Causes of Hyponatremia
Poor oral/IV intake
Over hydration
Paraneoplastic syndrome from malignancy
Medications or street drugs
Adrenal insufficiency
SIADH

Symptoms
Serum 125 range Mild CNS symptoms
Fatigue
Lethargy
Anorexia
Nausea
Muscle cramps
Symptoms
Serum Na <125 Confusion
Seizures
Coma
Assessment
Past and recent medical/surgical history Poor oral intake, thirsty
Fevers, sweating
Recent vomiting or diarrhea
Urine output
Orthostatic vital signs

Assessment
Physical exam Skin turgor
Mood changes
Mucous membranes
Axillary sweat
Cardiovascular status
Should hospitalization be considered?
Is the patient symptomatic (confused, seizures)?
Is the hyponatremia severe ( <120 mEq/ml)?
Is the hyponatremia acute (was Na 145 several days ago and 125 now)?
Repeat labs to confirm

Assessment
Laboratory Urinalysis – presence of hyaline casts
or specific gravity >1.010 suggestive of intravascular hypovolemia
Urine electrolytes –urine sodium, urine creatinine and urine osmolality
Urine Na <25 suggestive of hypovolemia with exception of patients on diuretics
Assessment
Laboratory Cont’d Serum BUN/Creatinine - >2.0
suggestive of intravascular hypovolemia
None of the above are perfect.
Consider all when deciding whether patient is intravasculary hypovolemic, euvolemic, hypervolemic
The Hypovolemic Patient
Most frequently occurs in patients taking diuretics with recent decrease in PO intake.
To manage patient Hold diuretics
Hydrate intravascularly (oral and IV)
Treat underlying cause

IV Hydration Tips
Wait for lab results of serum Na prior to ordering aggressive IV hydration
Rapid administration of IV fluid in setting of severe hyponatremia can lead to seizure, destruction of myelin sheath covering nerve cells in brain stem
The Hypervolemic Patient
Most frequently seen in patients with congestive heart failure, cirrhosis, renal failure, psychogenic polydipsia.
To manage this patient: Diuresis with loop diuretic (lasix,
bumex)
Consider ACE inhibitor based on patient tolerability

The Euvolemic Patient
Most frequently seen in patients with SIADH, hypothyroidism, adrenal insufficiency, patients s/p stroke.
To manage patient: Check serum osmolality, TSH, and
serum cortisol
The Euvolemic Patient
Management Continued: If urine osmolality >serum osmolality,
then patient has SIADH
If TSH high hypothyroidism should be considered
If cortisol level is <18 consider adrenal insufficiency
The Euvolemic Patient
Restrict free water to <1500 ml/day for mild abnormalities
Restrict free water to <1000 ml/day for severe abnormalities
If there is no response in two days consider further restriction
Consult Endocrinology and/or Renal colleagues

SIADH
SIADH causes include malignancy, recent surgery, medications
Syndrome of inappropriate antidiuretic hormone (SIADH) is a disorder of water intoxication
SIADH describes the inappropriate production and secretion of antidiuretic hormone (ADH)

Pathophysiology
Abnormal metabolism of ADH causes increased water reabsorption in the renal tubules which leads to increased water retention and dilution

Pathophysiology
Vasopressin is the biologically active form of ADH in humans
Synthesized in the hypothalamus
After synthesis transferred to posterior pituitary
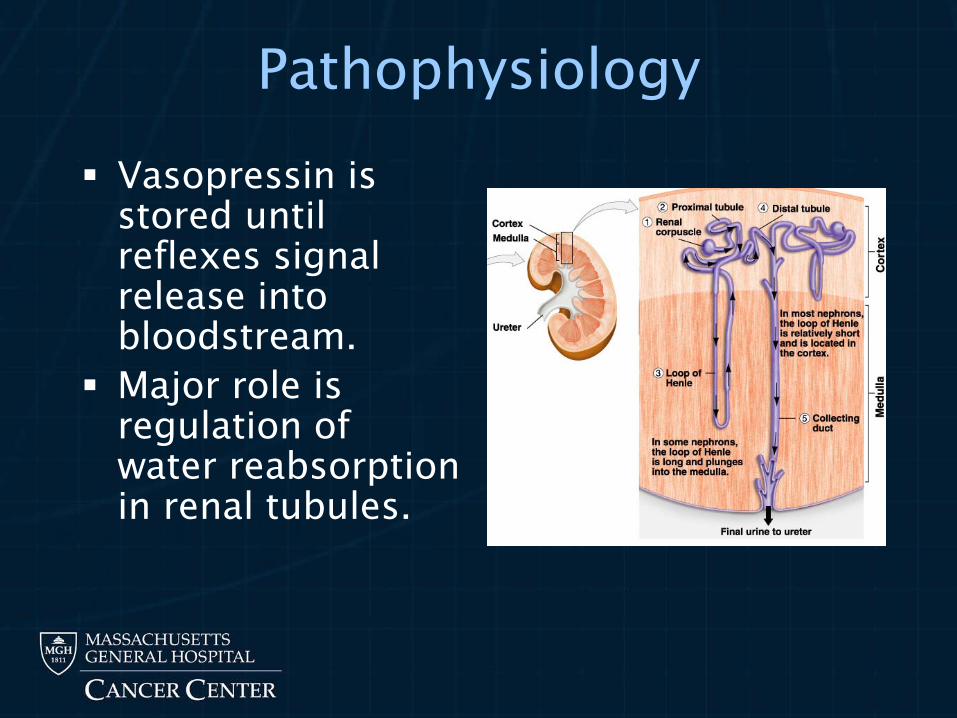
Pathophysiology
Vasopressin is stored until reflexes signal release into bloodstream.
Major role is regulation of water reabsorption in renal tubules.
Pathophysiology
Total body water is regulated primarily by reflexes that stimulate or inhibit ADH.
Venous, cardiac and arterial baroreceptors sense pressure changes that control ADH secretion and to restore extravascular volume.

Pathophysiology
In SIADH , receptors are overridden with the production and secretion of ADH that is not appropriate for homeostasis.
The mechanism in SIADH is ectopic production of ADH which interferes with ability to stop thirst mechanism

Signs and Symptoms
General Weakness, fatigue
Neurologic Altered mental status, headache, lethargy,
irritability, delirium, psychosis, personality changes, gait disturbance
Cardiovascular Normotensive, regular rate, rhythm

Signs and Symptoms
Gastrointestinal Anorexia, nausea, vomiting, diarrhea,
excessive thirst, abdominal cramping.
Renal Oliguria (<400 cc/24 hours), weight
gain, incontinence.
Signs and Symptoms
Musculoskeletal Muscle cramps
Hypoactive reflexes
Myoclonus
Physical Exam
Absence of patient reported symptoms
Dilution occurs on intravascular level
Normal skin turgor
Euvolemic
Normotensive
No peripheral or interstitial edema
Diagnostics Studies
Electrolytes, BUN, creatinine, albumin and uric acid.
Studies to r/o cardiac, hepatic, adrenal and thyroid causes should be considered.
Laboratory Values
Serum sodium <130 mEq/L
Serum osmolality <280 mOsm/kg
Urine osmolality >500 mOsm/kg
Urine sodium >20 mEq/L
Medical Management of SIADH
Directed at treating the underlying pathology.
Discontinuation of contributing medications
In setting of malignancy goal is treatment with surgery, chemotherapy or radiation.

Medical Management of SIADH
Treatment for mild SIADH (serum Na >125 mEq/l) includes fluid restriction of 800-1000 ml/day. Fluid restriction often increases Na
within 3-10 days. Loop diuretic when SIADH
confirmed

Medical Management
Demeclocycline acts on renal tubules as vasopressin antagonist Contraindicated with cirrhosis
Increases Na within 3-4 days
Eases strict fluid restriction

Medical Management
Aquaretics Vasopressin receptor antagonist
Promotes electrolyte sparing diuresis
Approved in hospital setting
Contraindicated hypovolemic patient
Use mostly limited to heart failure patients and best use still in early studies

Medical Management
Consider hypertonic saline (3%) for acute and symptomatic (seizures, coma) low Na Hypertonic saline 513 mEq NaCl
1L NS 154 mEq NaCl
Administered over two to three hours.

Nursing Management
Assessment of neuromuscular, cardiac, gastrointestinal and renal systems.
Evaluation of fluid and electrolyte status
Assess for signs and symptoms of hypovolemia or hypervolemia
Review medications
Monitor blood and urine chemistries

Key Take Home Points
Recent medical and surgical history is going to be best first tool
Wait for repeat serum Na before deciding on role and rate of rehydration
Goal is to treat underlying cause

References
Up-to-Date
Harrison’s Online