Hypertrophic Cardiomyopathy: A Contemporary And...
75
Barry J. Maron, MD Director, Hypertrophic Cardiomyopathy Center Minneapolis Heart Institute Foundation Minneapolis, Minnesota Disclosures: Medtronic (Grantee) GeneDx (Consultant) Hypertrophic Cardiomyopathy: A Contemporary And Treatable Disease in 2015
Transcript of Hypertrophic Cardiomyopathy: A Contemporary And...
Barry J. Maron, MD
Director, Hypertrophic Cardiomyopathy CenterMinneapolis Heart Institute Foundation
Minneapolis, Minnesota
Disclosures:Medtronic (Grantee)GeneDx (Consultant)
Hypertrophic Cardiomyopathy:
A Contemporary
And Treatable Disease in 2015

General
Population
1:500
700,000 people
in U.S.
AT RISK:
50,000 – 100,000 ?
Amer Indians
N=3,501;51-77 y
0.2%
CARDIA
N=4,111;23-35 y
0.17%
China
N=8,080;18-74 y
0.16%
Rural Minnesota
N=15,137;16-87 y
0.19%
Japan
N=3,354;20-77 y
0.17%
Tanzania
N=6,680;22-91 y
0.2%
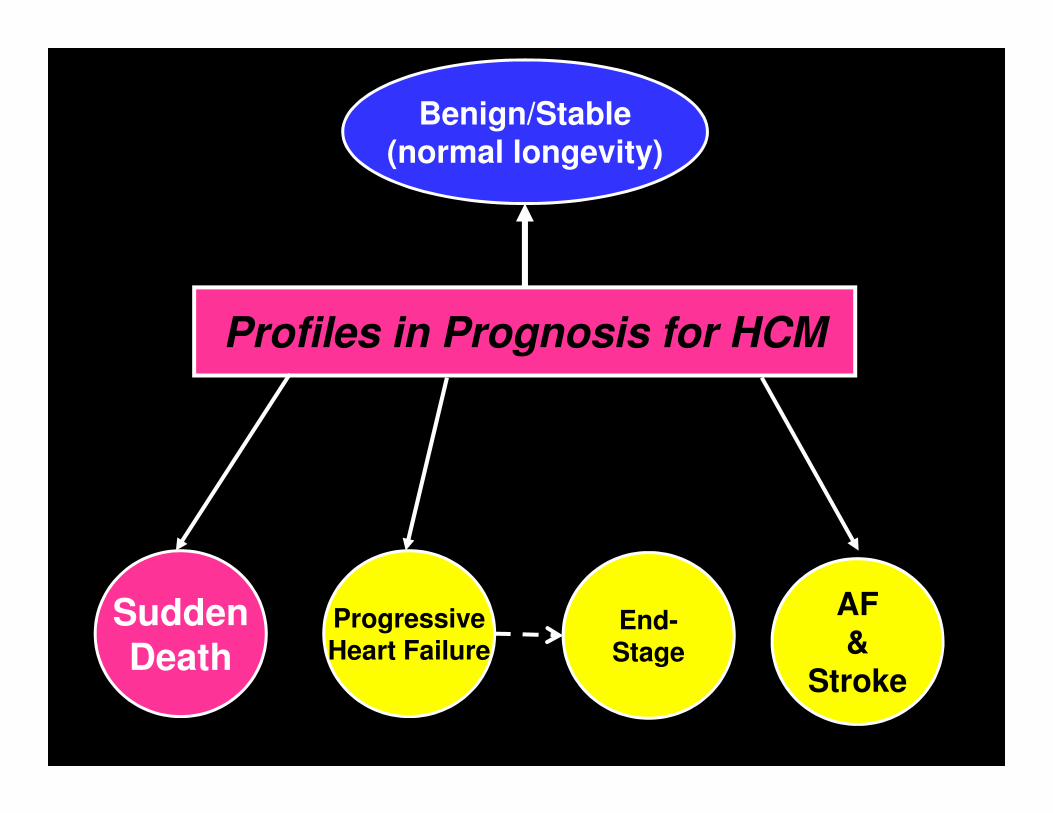
SuddenDeath
ProgressiveHeart Failure
AF&
Stroke
End-Stage
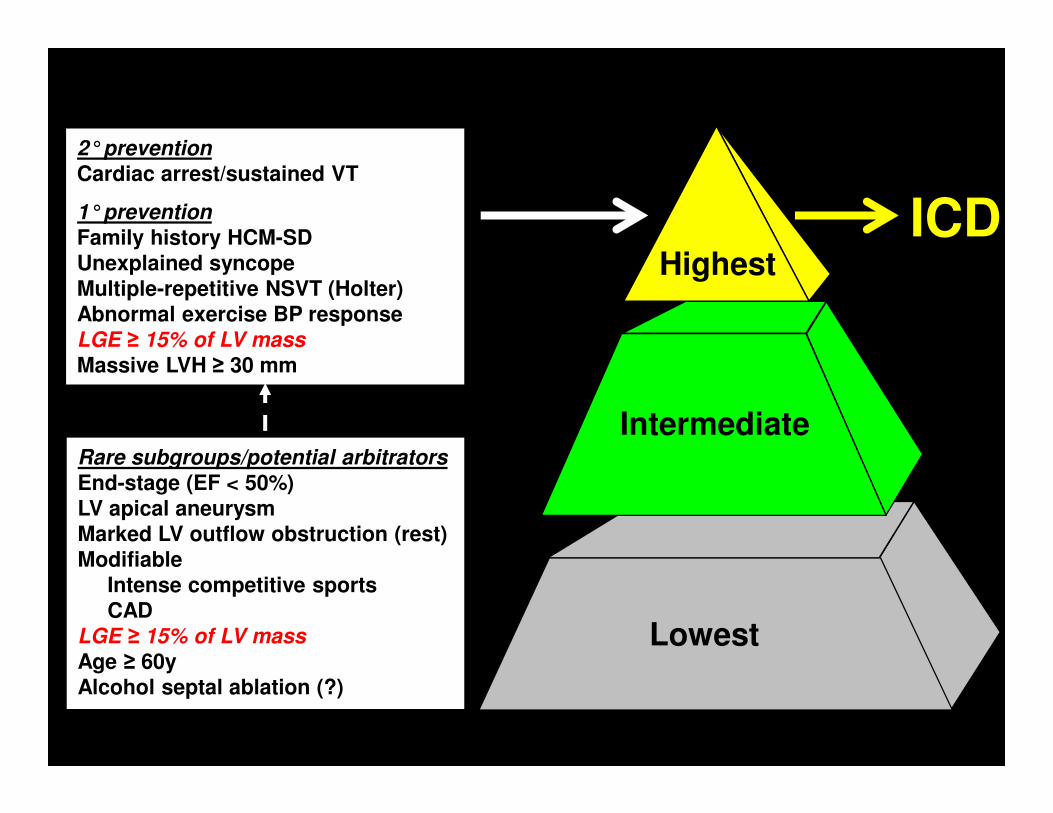
Profiles in Prognosis for HCM
Benign/Stable(normal longevity)
Highest
Intermediate
Lowest
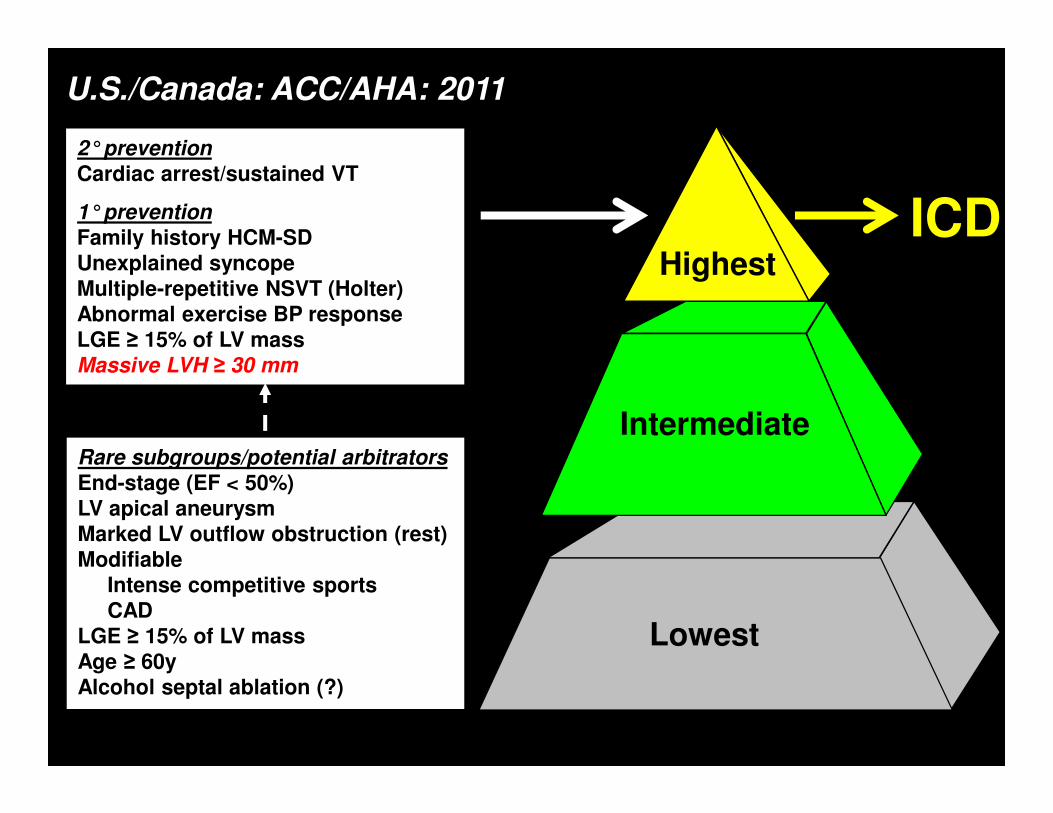
2°prevention
Cardiac arrest/sustained VT
1°prevention
Family history HCM-SDUnexplained syncopeMultiple-repetitive NSVT (Holter)Abnormal exercise BP responseLGE ≥ 15% of LV massMassive LVH ≥ 30 mm
Rare subgroups/potential arbitrators
End-stage (EF < 50%)LV apical aneurysmMarked LV outflow obstruction (rest)Modifiable
Intense competitive sportsCAD
LGE ≥ 15% of LV massAge ≥ 60yAlcohol septal ablation (?)
ICD
U.S./Canada: ACC/AHA: 2011

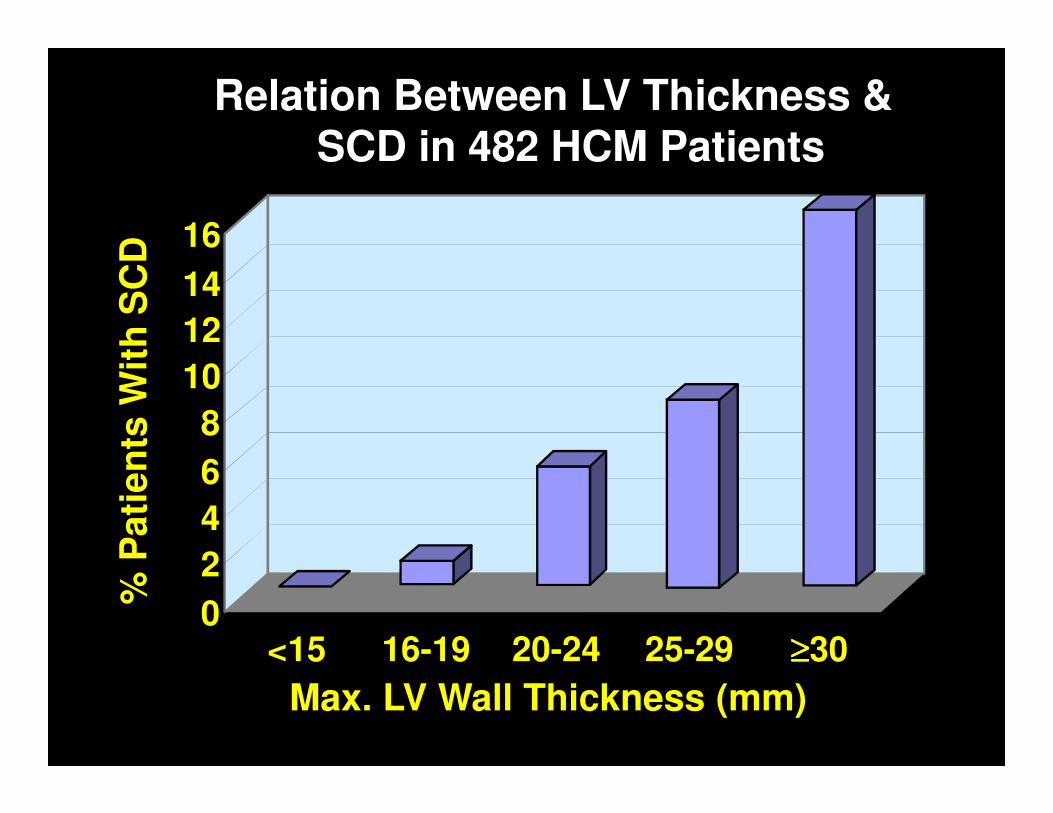
0
2
4
6
8
10
12
14
16
<15 16-19 20-24 25-29 ≥≥≥≥30
Max. LV Wall Thickness (mm)
% P
ati
en
ts W
ith
SC
DRelation Between LV Thickness &
SCD in 482 HCM Patients
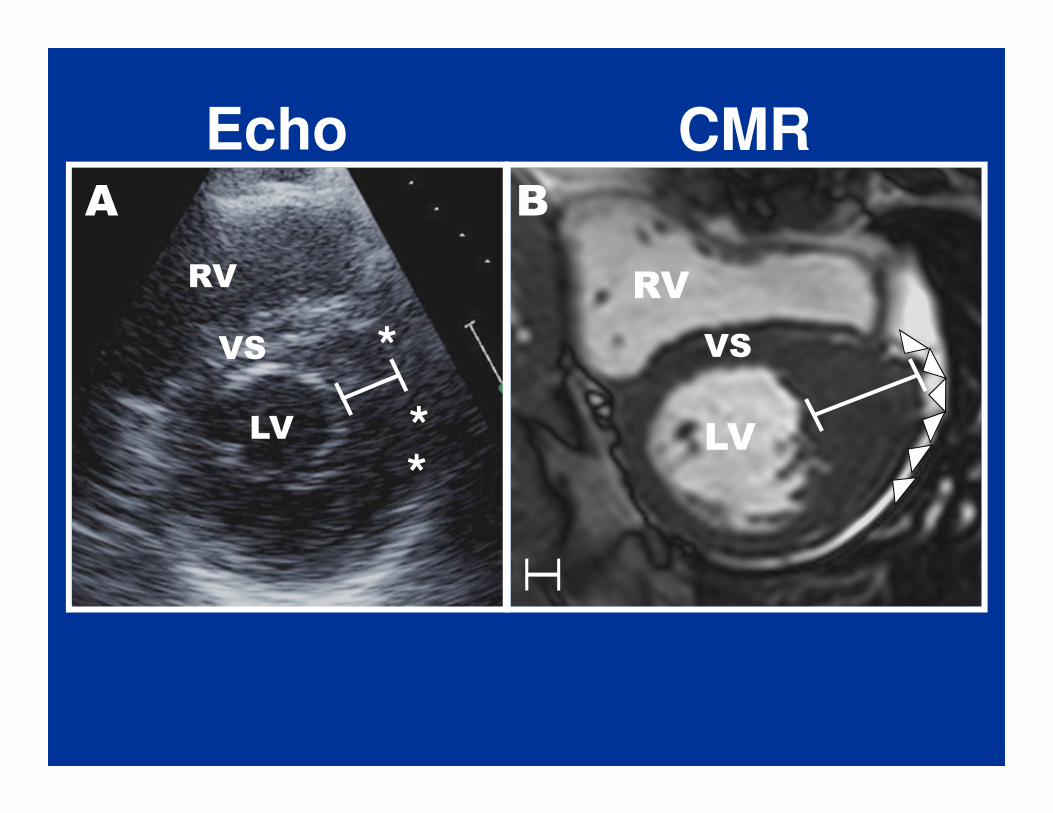
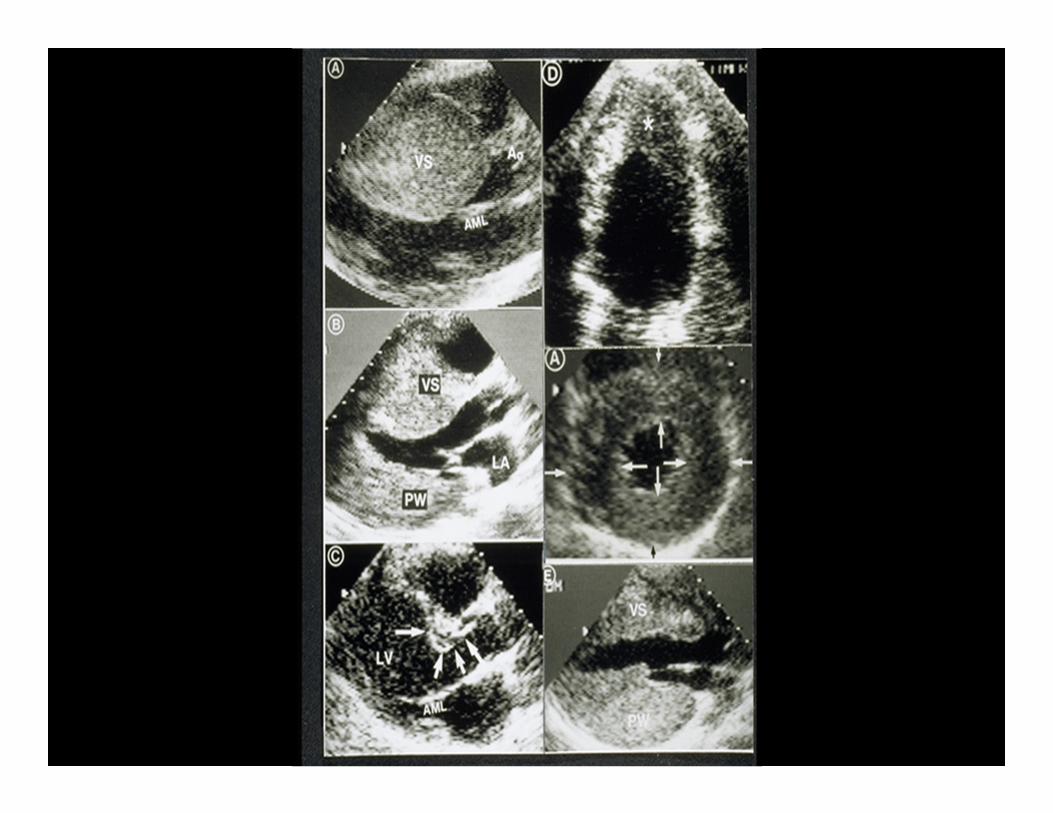
A
RV
LV
VS
*
*
*
RV
VS
LV
B
Echo CMR
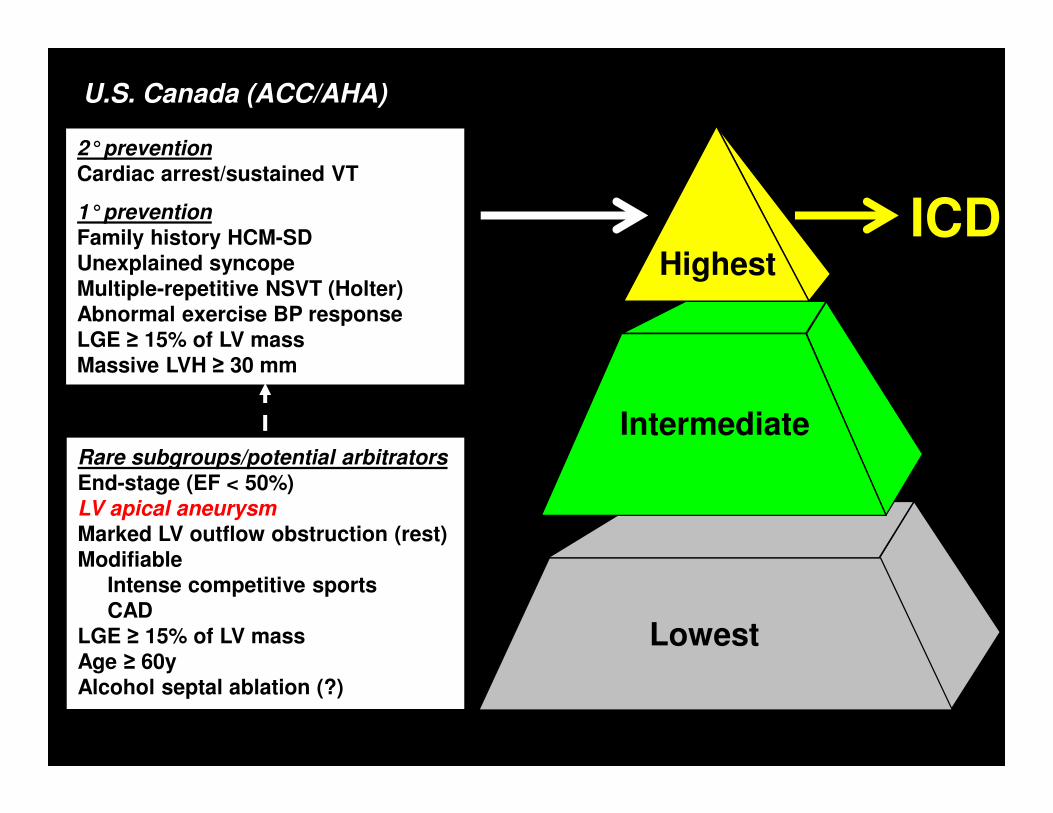
Highest
Intermediate
Lowest
2°prevention
Cardiac arrest/sustained VT
1°prevention
Family history HCM-SDUnexplained syncopeMultiple-repetitive NSVT (Holter)Abnormal exercise BP responseLGE ≥ 15% of LV massMassive LVH ≥ 30 mm
Rare subgroups/potential arbitrators
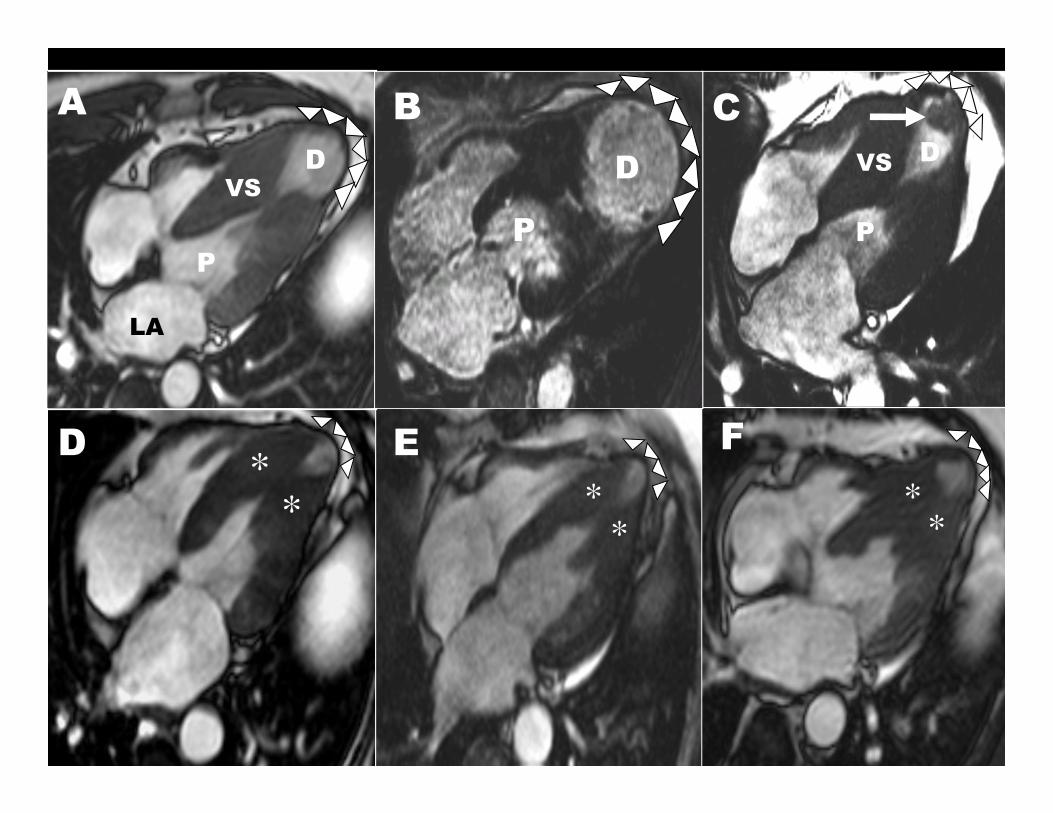
End-stage (EF < 50%)LV apical aneurysm
Marked LV outflow obstruction (rest)Modifiable
Intense competitive sportsCAD
LGE ≥ 15% of LV massAge ≥ 60yAlcohol septal ablation (?)
ICD
U.S. Canada (ACC/AHA)
A C
D E F
LA
P
D D
P
VSVS
B
P
D
*
**
*
**
Figure 1.
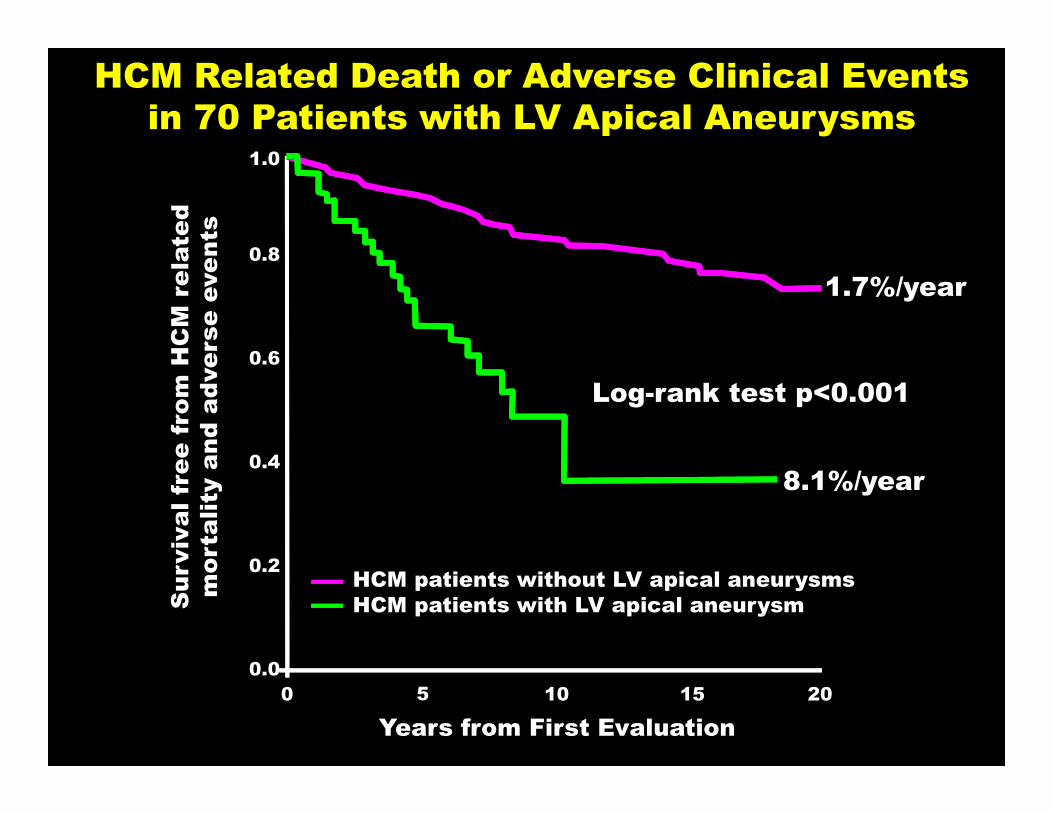
1.0
0.8
0.6
0.4
0.0
0 5 1510 20
HCM patients without LV apical aneurysms
HCM patients with LV apical aneurysm
Log-rank test p<0.001
Years from First Evaluation
Survival free from HCM related
mortality and adverse events
0.2
HCM Related Death or Adverse Clinical Events
in 70 Patients with LV Apical Aneurysms
8.1%/year
1.7%/year

Highest
Intermediate
Lowest
2°prevention
Cardiac arrest/sustained VT
1°prevention
Family history HCM-SDUnexplained syncopeMultiple-repetitive NSVT (Holter)Abnormal exercise BP responseLGE ≥ 15% of LV massMassive LVH ≥ 30 mm
Rare subgroups/potential arbitrators
End-stage (EF < 50%)LV apical aneurysmMarked LV outflow obstruction (rest)Modifiable
Intense competitive sportsCAD
LGE ≥ 15% of LV massAge ≥ 60y
Alcohol septal ablation (?)
ICD
U.S./Canada: ACC/AHA

0
10
20
30
40
50
60
70
Alive Non-
Cardiac
Death
Non-HCM
Cardiac
Death
Embolic
Stroke
Heart
Failure
SCD
% o
f H
CM
Co
ho
rt
65%
13% 12%
2% 1%
0.2%/y
Outcome of HCM Patients First Evaluated ≥ 60 Years
1%
HCM Death
Aging is Good in HCM
Maron BJ et. al. Circ 2013; 127: 585
Intermediate
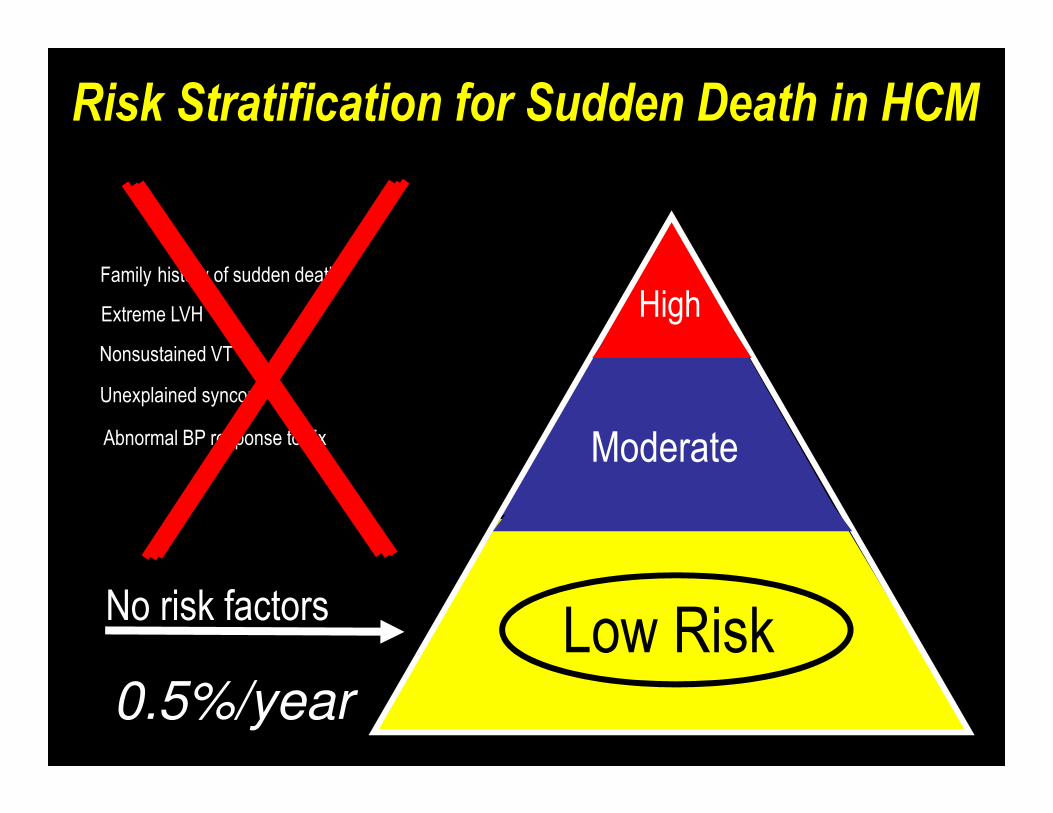
Low Risk
Risk Stratification for Sudden Death in HCM
Moderate
High
No risk factors
Family history of sudden death
Nonsustained VT
Unexplained syncope
Extreme LVH
Abnormal BP response to Ex
0.5%/year

LA
LA
VS
RV
LV VS
A B C
D E F
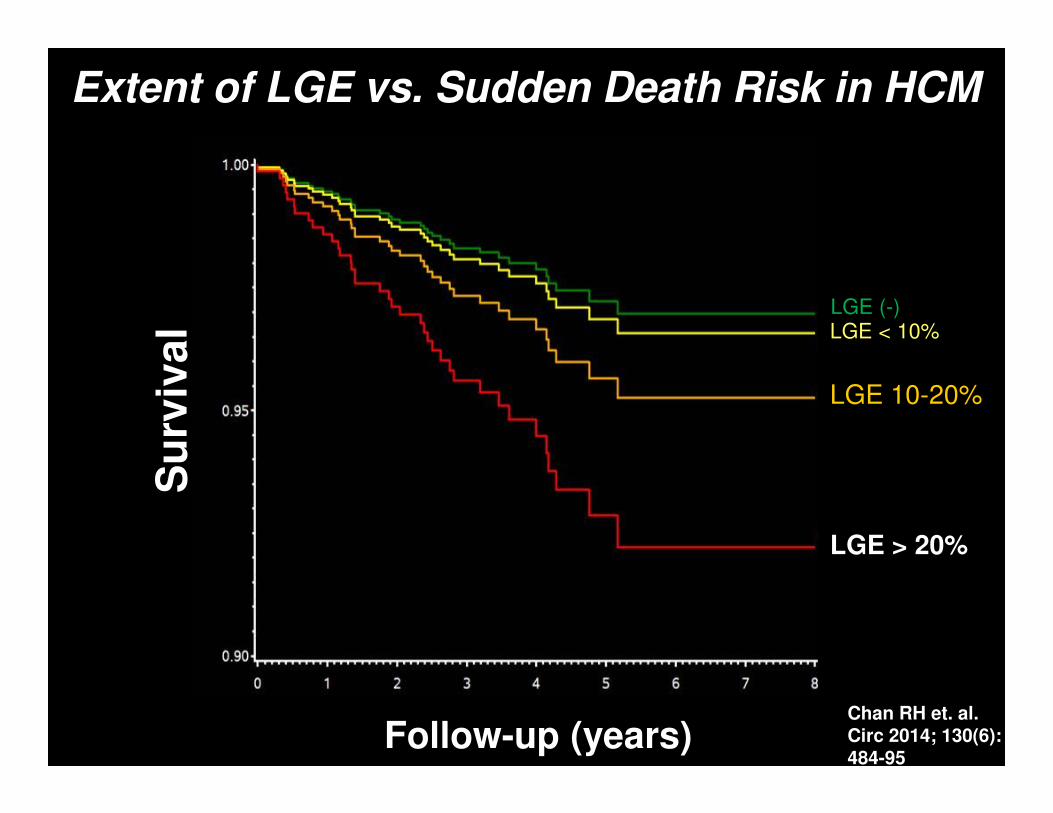
Prevalence
of LGE = 55-70%
L
G
E
LGELGE
Extent of LGE vs. Sudden Death Risk in HCM
Follow-up (years)
Su
rviv
al
LGE (-)LGE < 10%
LGE 10-20%
LGE > 20%
Chan RH et. al.Circ 2014; 130(6):484-95
Highest
Intermediate
Lowest
2°prevention
Cardiac arrest/sustained VT
1°prevention
Family history HCM-SDUnexplained syncopeMultiple-repetitive NSVT (Holter)Abnormal exercise BP responseLGE ≥ 15% of LV mass
Massive LVH ≥ 30 mm
Rare subgroups/potential arbitrators
End-stage (EF < 50%)LV apical aneurysmMarked LV outflow obstruction (rest)Modifiable
Intense competitive sportsCAD
LGE ≥ 15% of LV mass
Age ≥ 60yAlcohol septal ablation (?)
ICD
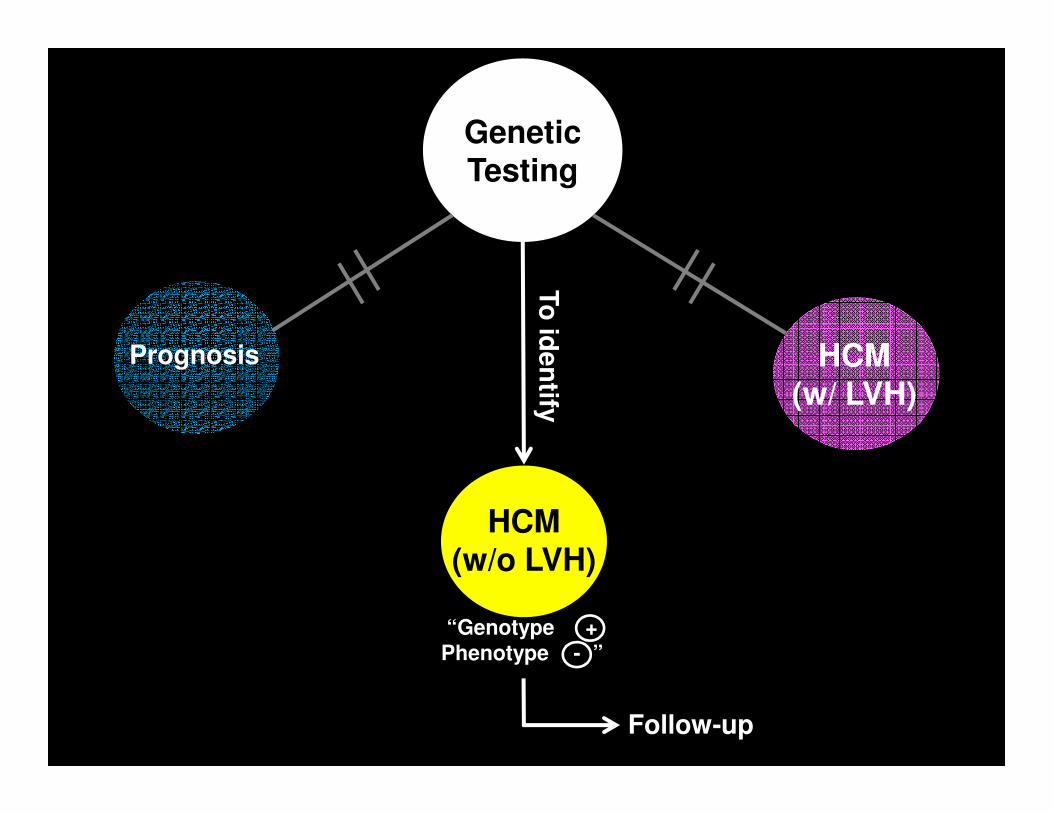
GeneticTesting
Prognosis
HCM(w/o LVH)
HCM(w/ LVH)
To
ide
ntify
“Genotype +Phenotype - ”
Follow-up

Prevention of Sudden Death
in HCM

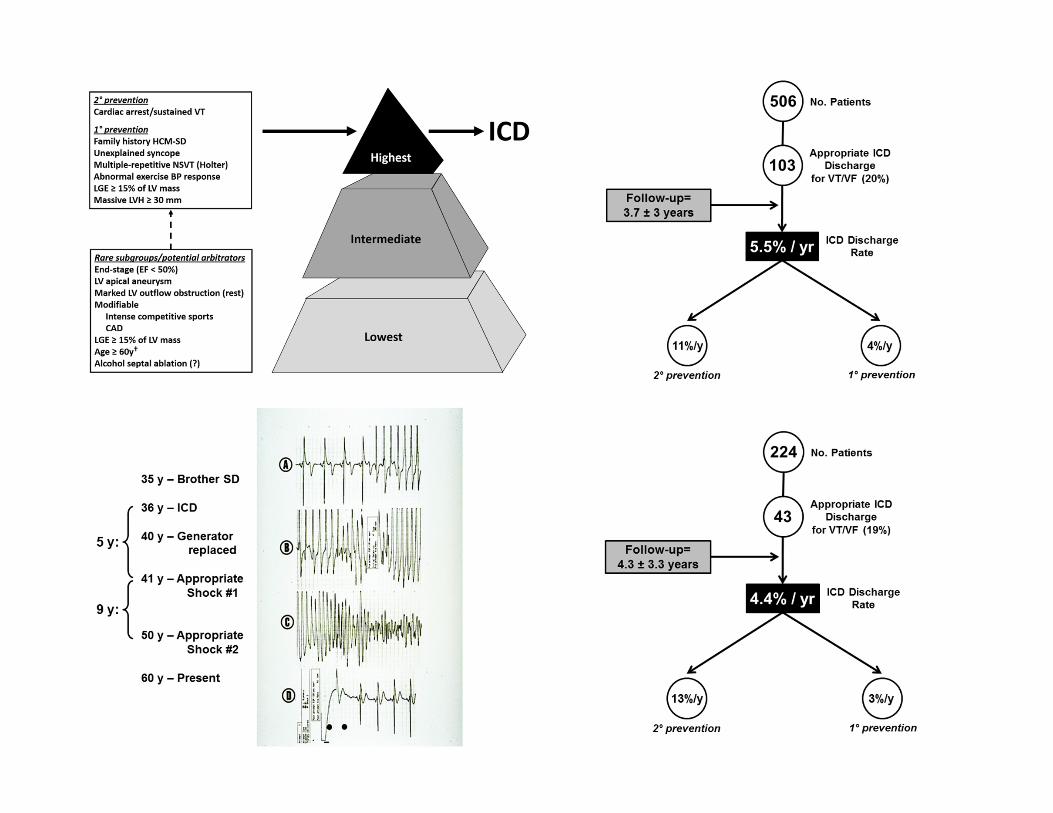
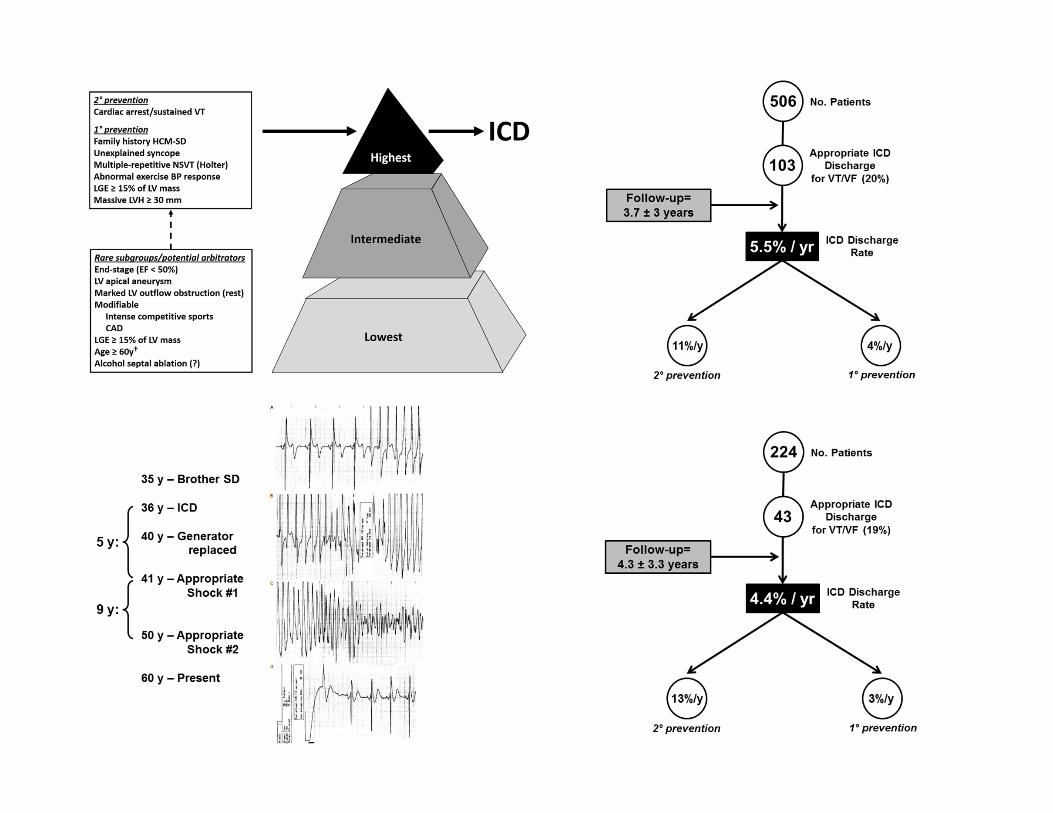
ICD Performance in HCM
506
103
5.5%/y
Follow-up = 3.7 ± 3 years
ICD dischargerate
AppropriateShocks (20%)
11%/y 4%/y
2º prevention 1º prevention
VT/VF
Maron BJ et. al. JAMA 2007;298:405-412
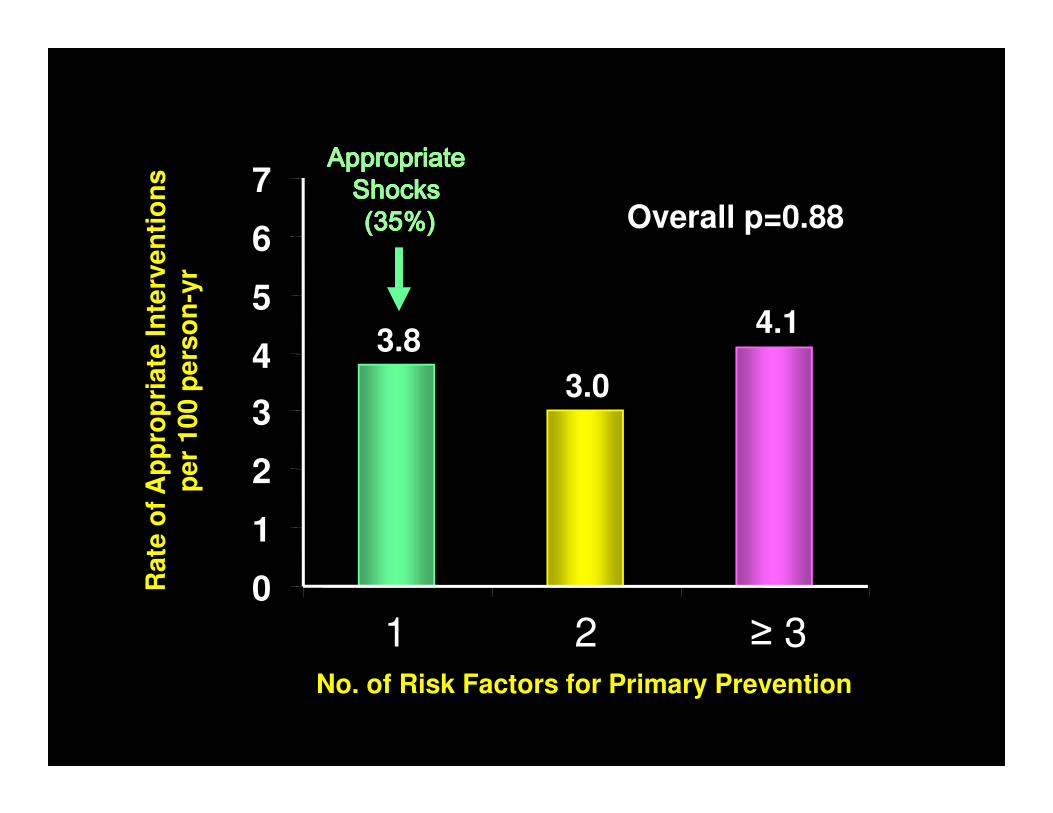
0
1
2
3
4
5
6
7
1 2 ≥ 3No. of Risk Factors for Primary Prevention
Ra
te o
f A
pp
rop
ria
te In
terv
en
tio
ns
pe
r 1
00
pe
rso
n-y
r
3.8
3.0
4.1
Overall p=0.88
AppropriateAppropriateAppropriateAppropriate
ShocksShocksShocksShocks
(35%)(35%)(35%)(35%)
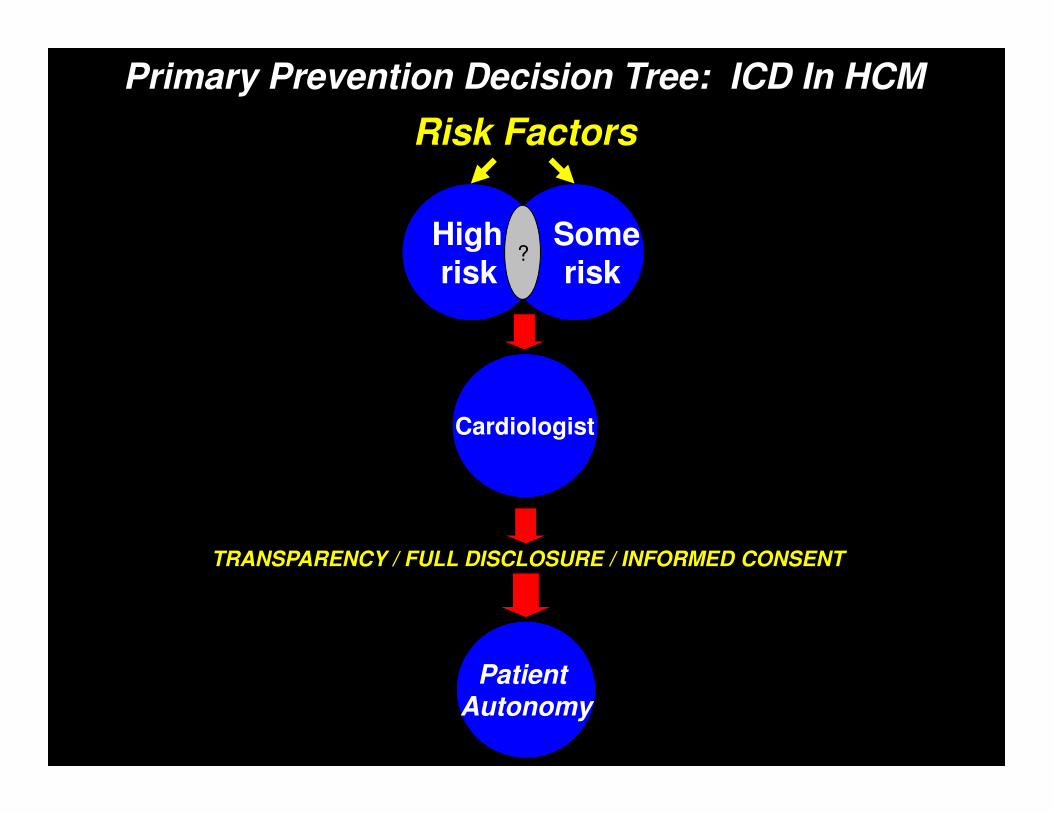
Highrisk
Somerisk
Cardiologist
Patient Autonomy
TRANSPARENCY / FULL DISCLOSURE / INFORMED CONSENT
?
Risk Factors
Primary Prevention Decision Tree: ICD In HCM
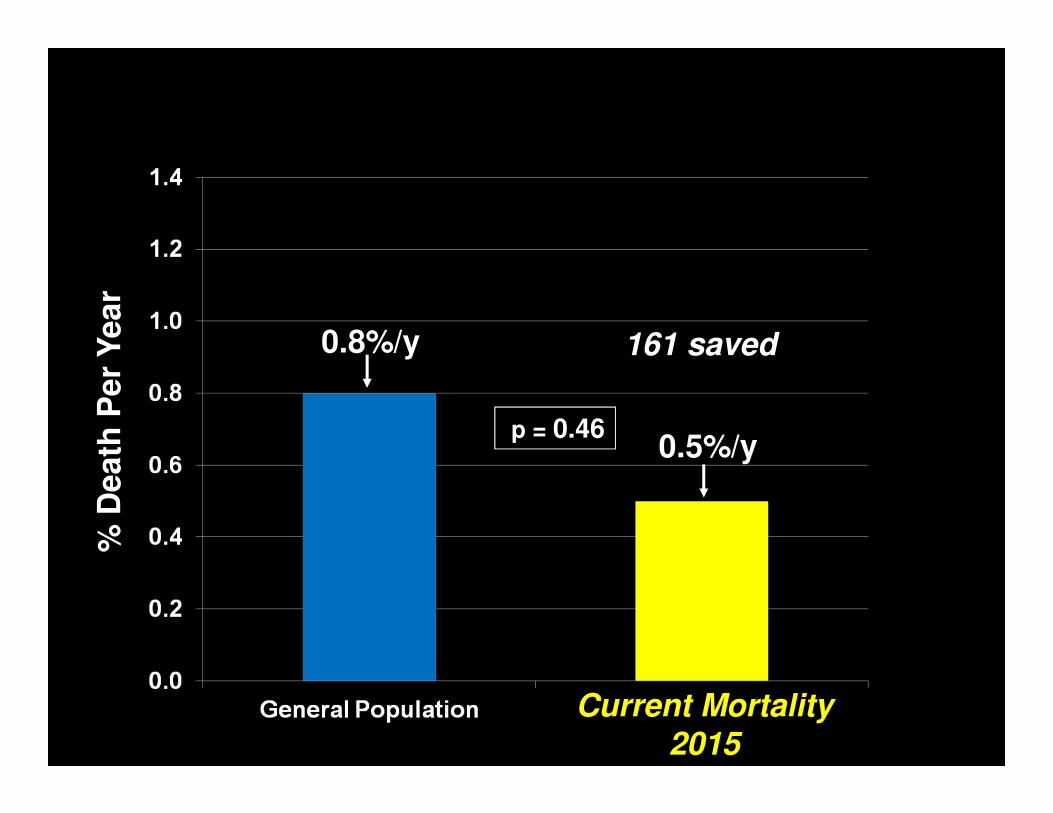
Evidence for Decreased HCM Mortality:
2000 Patients Presenting 10-70 years Old
MHIF/Tufts
What is Possible…..

0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
General Population "Historic Mortality"
0.8%/y
86 ICDinterventions
% D
eath
Per
Year
1.5%/y
Maron BJ et. al.JACC 2015
Pre-ICD era

0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
General Population "Historic Mortality"
0.8%/y
% D
eath
Per
Year
0.8%/y
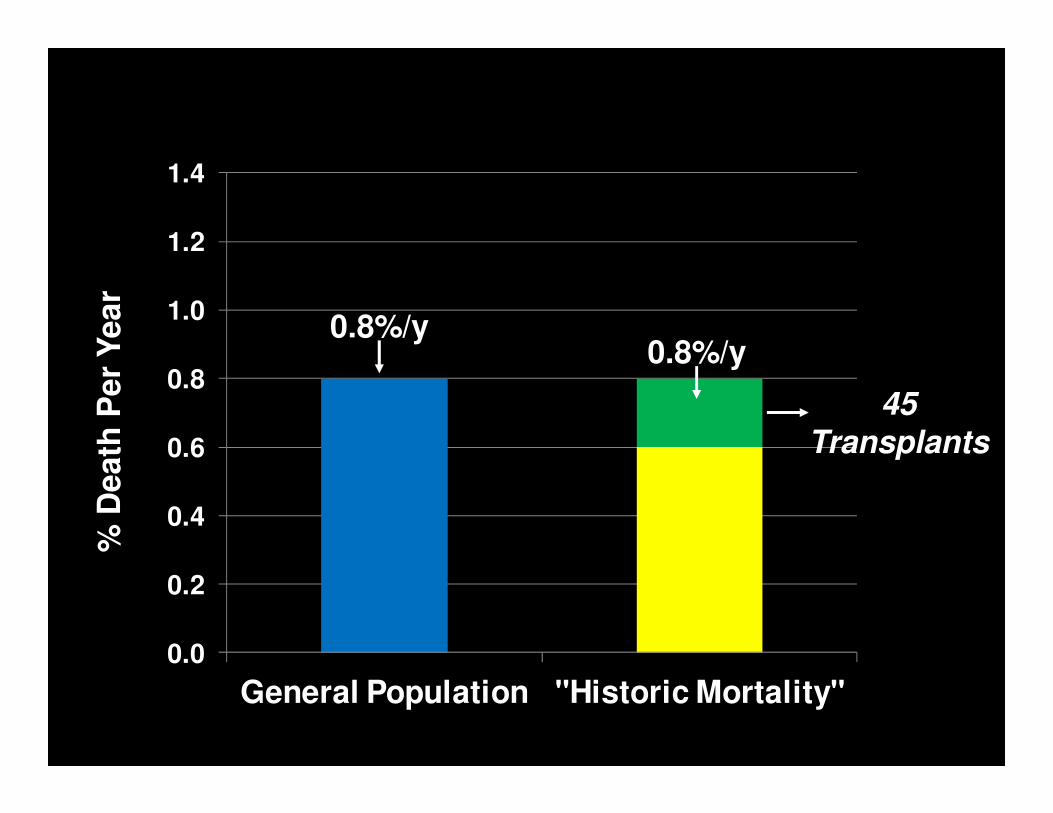
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
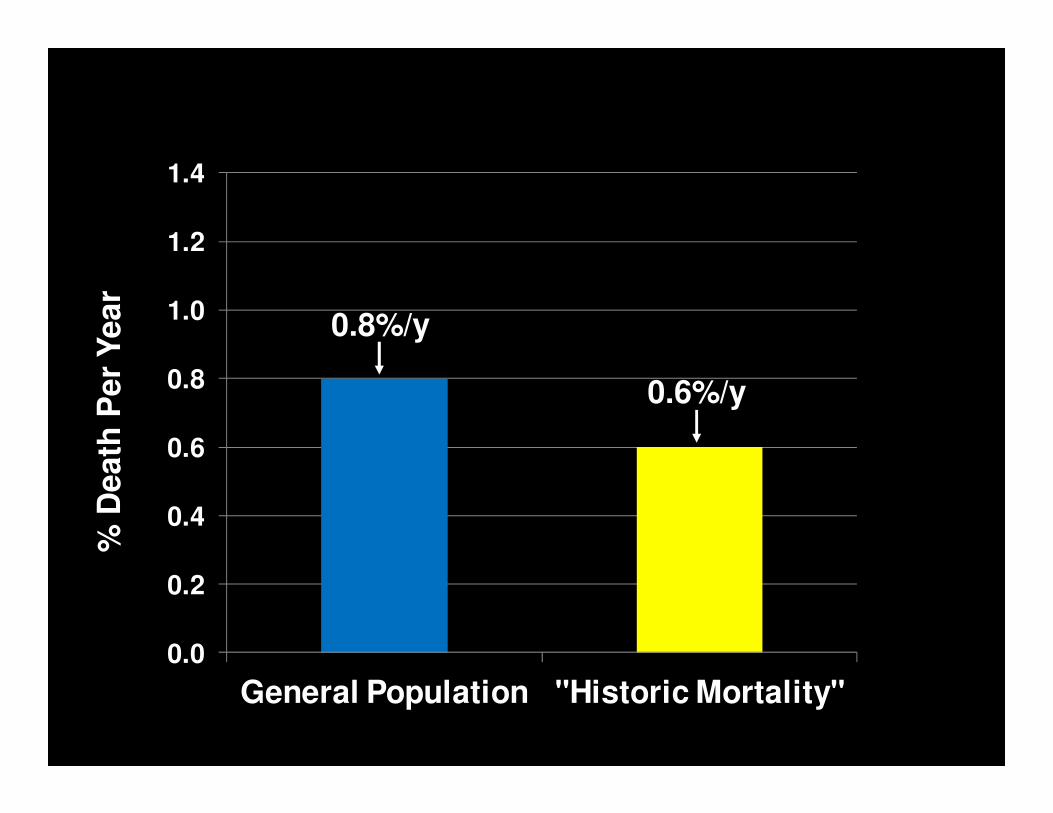
General Population "Historic Mortality"
0.8%/y
45Transplants
% D
eath
Per
Year
0.8%/y
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
General Population "Historic Mortality"
% D
eath
Per
Year
0.8%/y
0.6%/y
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
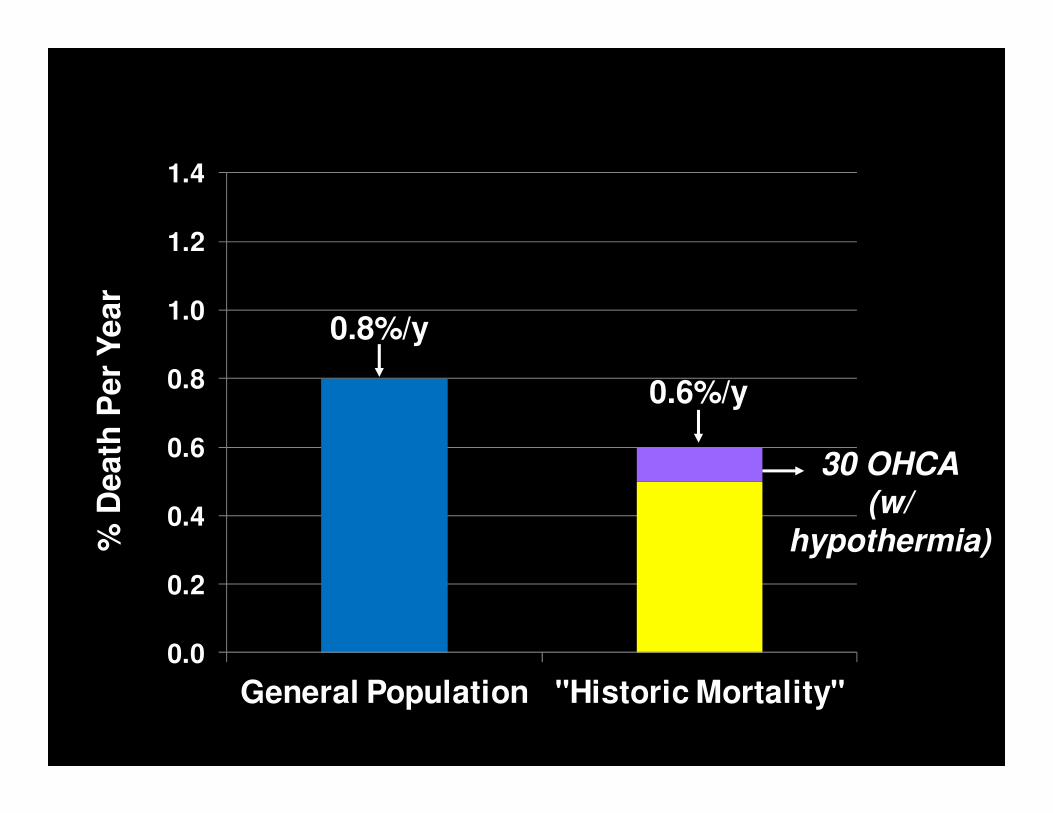
General Population "Historic Mortality"
0.8%/y
30 OHCA(w/
hypothermia)% D
eath
Per
Year
0.6%/y
0.8%/y
0.5%/y
Current Mortality2015
% D
eath
Per
Year
p = 0.46
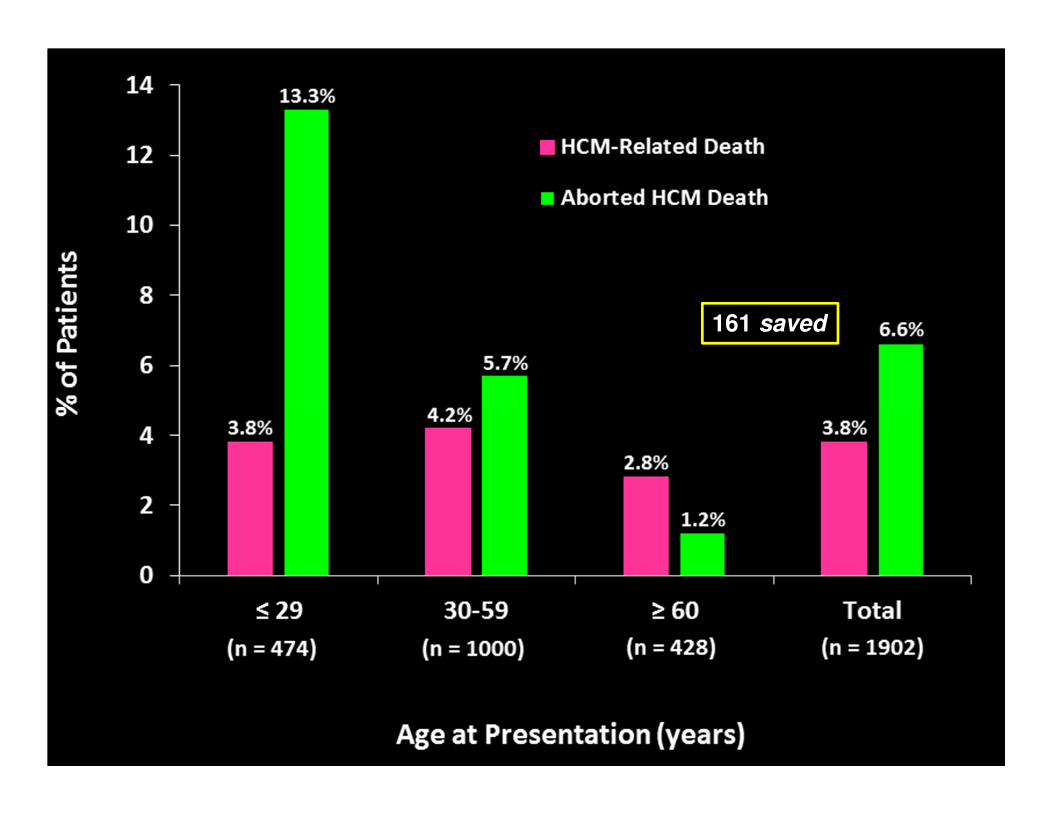
161 saved
161 saved
0
0.1
0.2
0.3
0.4
0.5
0.6
≤ 29 30-59 ≥ 60
(n = 474) (n = 1000) (n = 428)
Age in Years—Initial Evaluation
HC
M-R
ela
ted
Mo
rtali
ty
0.500.54
0.60
SuddenDeath
AdvancedHF
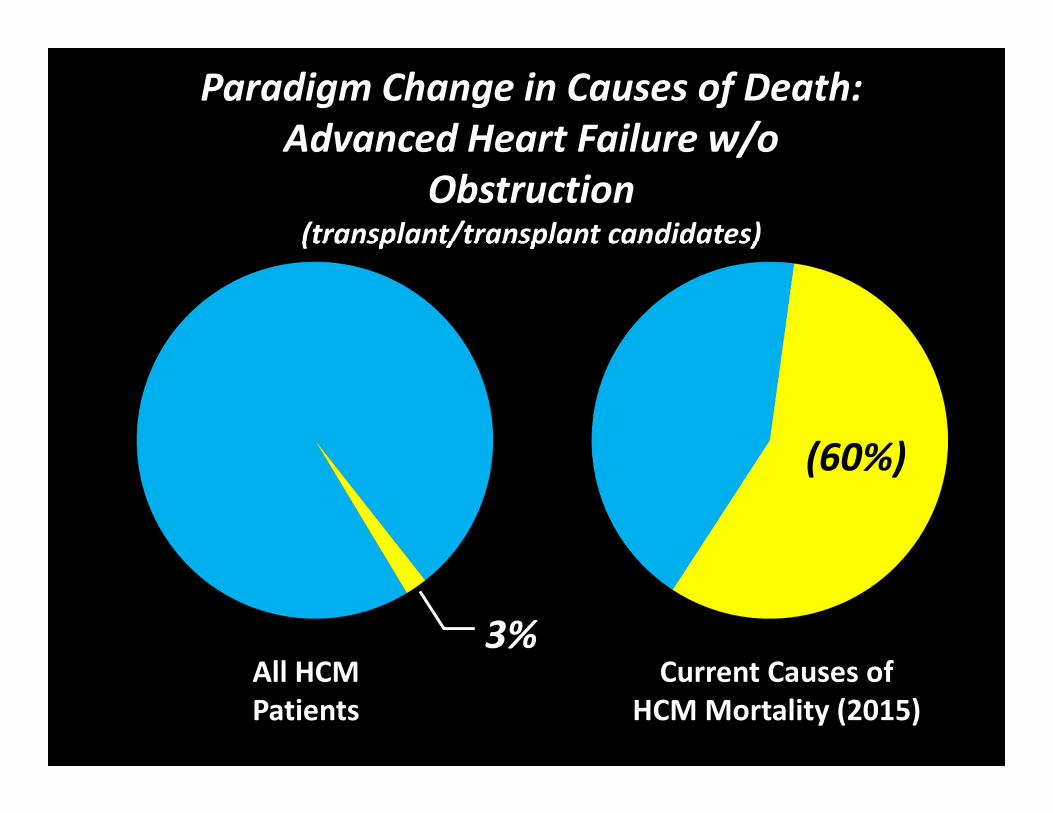
Paradigm Change in Causes of Death:
Advanced Heart Failure w/o
Obstruction (transplant/transplant candidates)
All HCM
Patients
Current Causes of
HCM Mortality (2015)
3%
(60%)
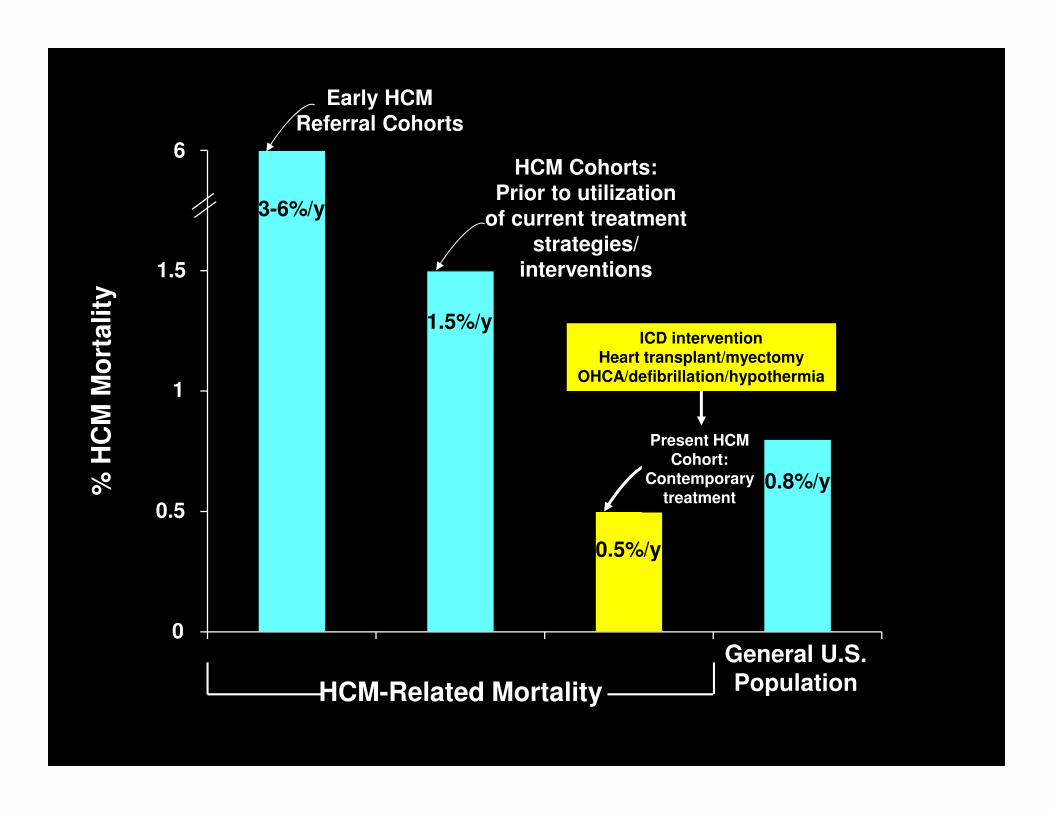
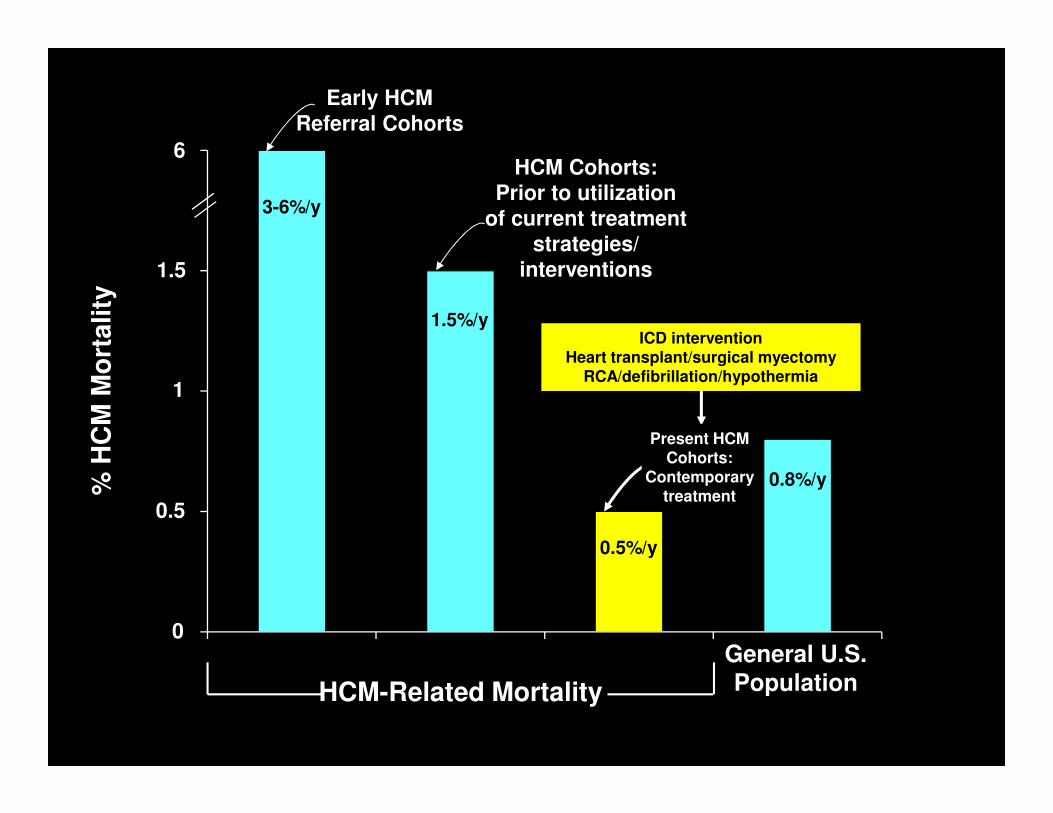
0
0.5
1
1.5
2
% H
CM
Mo
rta
lity
HCM-Related Mortality
0
0.5
1.5
1
6
General U.S.Population
0.8%/y
0.5%/y
1.5%/y
3-6%/y
Early HCMReferral Cohorts
HCM Cohorts:Prior to utilization
of current treatmentstrategies/
interventions
ICD interventionHeart transplant/myectomy
OHCA/defibrillation/hypothermia
Present HCMCohort:
Contemporarytreatment

ICD
Sudden Death
ProgressiveHeart
Failure(obstructive)
AdvancedHeart Failure& End Stage
(non-obstructive)
AF &
Stroke
Benign/Stable(normal longevity)
DrugsSeptal Myectomy(Alcohol Ablation)
Transplant DrugsAnticoagulants
Ablation
Profiles in Prognosis for HCM

New HCM Paradigms:
1. Contemporary Treatable Disease
Compatible w/ Low Mortality &
Extended/Normal Longevity
2. Rx Interventions available to
Change Clinical Course of
Disease
“At this time we are aware of no method of management that can specifically and
favorably influence the course of a patient with idiopathic ventricular hypertrophy.”
Eugene BraunwaldEdwin C. BrockenbroughAndrew G. Morrow
Circulation, Volume XXVI, August 1962


% P
ati
en
ts W
ith
/Wit
ho
ut
ICD
In
terv
en
tio
n/S
ud
de
n D
ea
th
AppropriateICD
Intervention
No AppropriateICD
Intervention
ESC Risk Score
<4%<4% 4-6%4-6% >6%>6%
Risk/5y Risk/5y
<4% 4-6% >6%
Risk/5y
Sudden Death
Assessment of ESC Sudden Death Risk Score(n = 1649)
60%
26%
63%
9%
161 saved

The ESC-HCM prediction formula for SD is as follows:
Probability SCD at 5 years = 1 – 0.998 exp (Prognostic index);
where Prognostic index = [0.15939858 x maximal LV wall
thickness (mm)] – [0.00294271 x LV maximal wall thick-
ness2 (mm2)] + [0.0259082 x left atrial diameter (mm)] +
[0.00446131 x maximal (rest/Valsalva) LV outflow tract
gradient (mm Hg)] + [0.4583082 x family history SCD] +
[0.82639195 x NSVT] + [0.71650361 x unexplained
syncope] – [0.01799934 x age at clinical evaluation (years)].
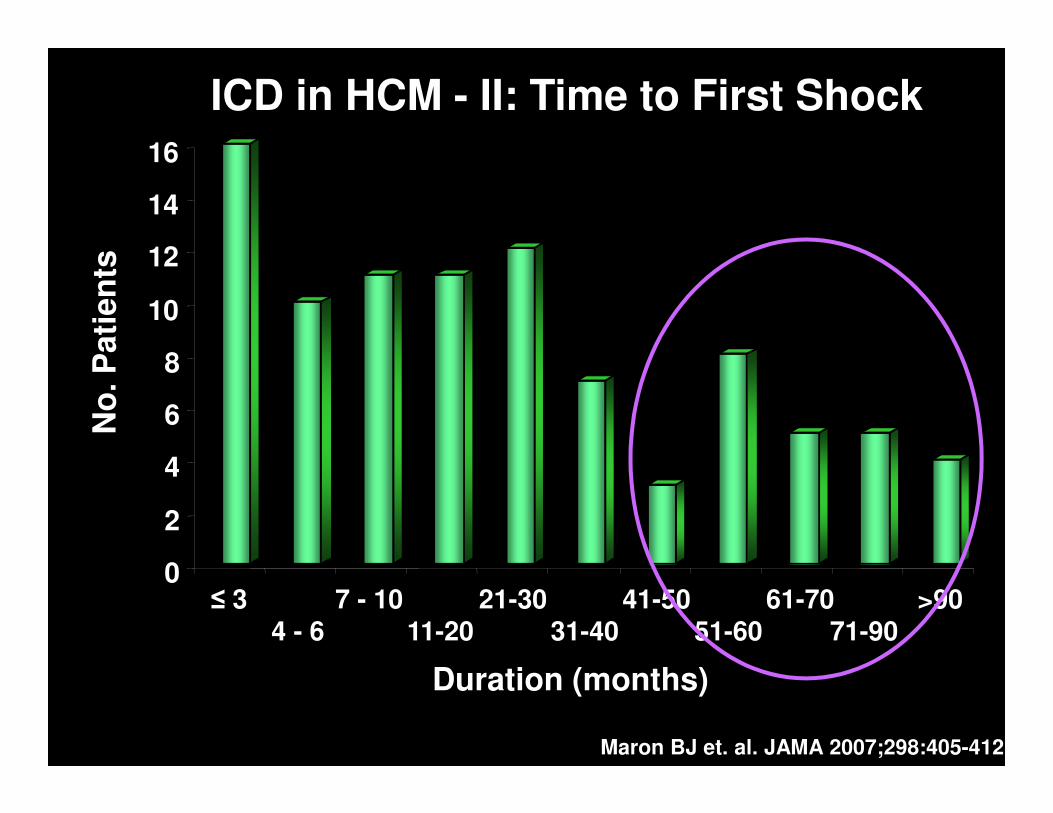
≤ 34 - 6
7 - 1011-20
21-3031-40 51-60
>90
Duration (months)
No
. P
ati
en
ts
0
2
4
6
8
10
12
14
16
61-7071-90
41-50
ICD in HCM - II: Time to First Shock
Maron BJ et. al. JAMA 2007;298:405-412
HCM is Unpredictable


Surgical Septal Myectomy:Quality of Life/Survival
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8 9 10
Years Post-op
Su
rviv
al
Isolated MyectomyNonoperated obstructiveExpected ---US population P<0.001
83%
61%
Ommen S et. al.JACC 2006
(Operative mortality: 0.4%)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
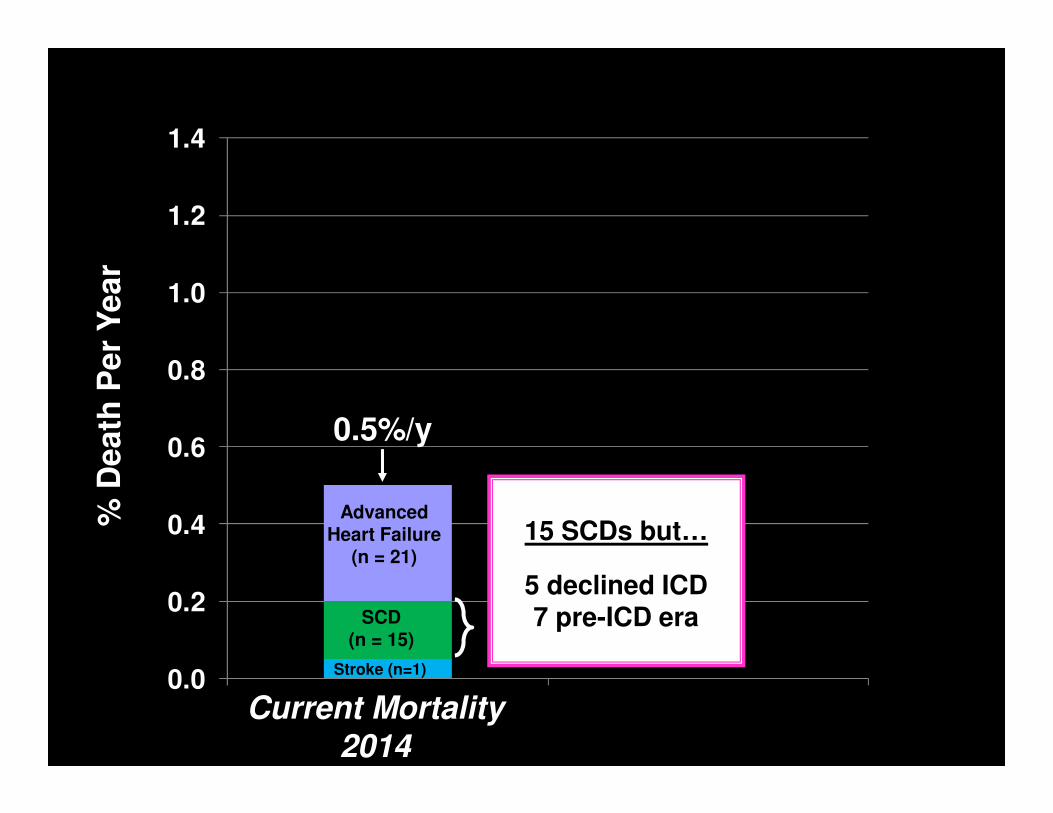
0.5%/y
Current Mortality2014
Advanced Heart Failure
(n = 21)
SCD(n = 15)
% D
eath
Per
Year
Stroke (n=1)
15 SCDs but…
5 declined ICD7 pre-ICD era
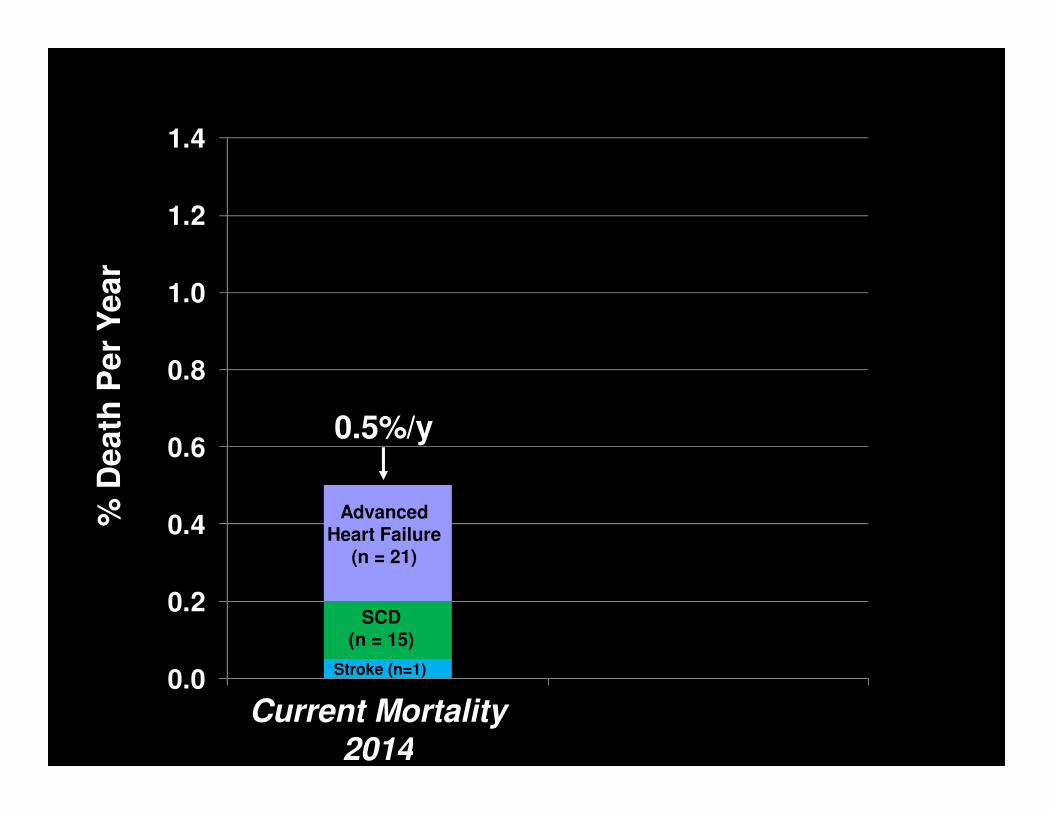
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
0.5%/y
Current Mortality2014
Advanced Heart Failure
(n = 21)
SCD(n = 15)
% D
eath
Per
Year
Stroke (n=1)
Evidence for Decreased HCM Mortality:
2000 Patients Presenting in Mid-Life (30-59y)
MHIF/Tufts
What is Possible…..
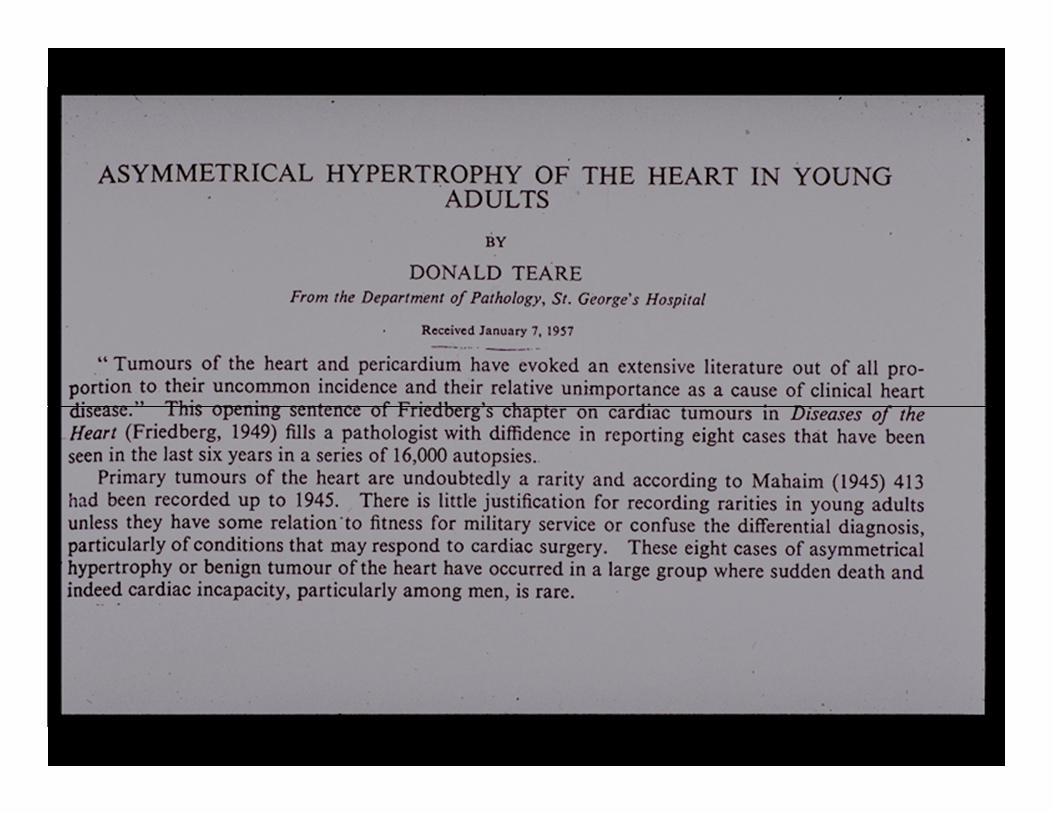
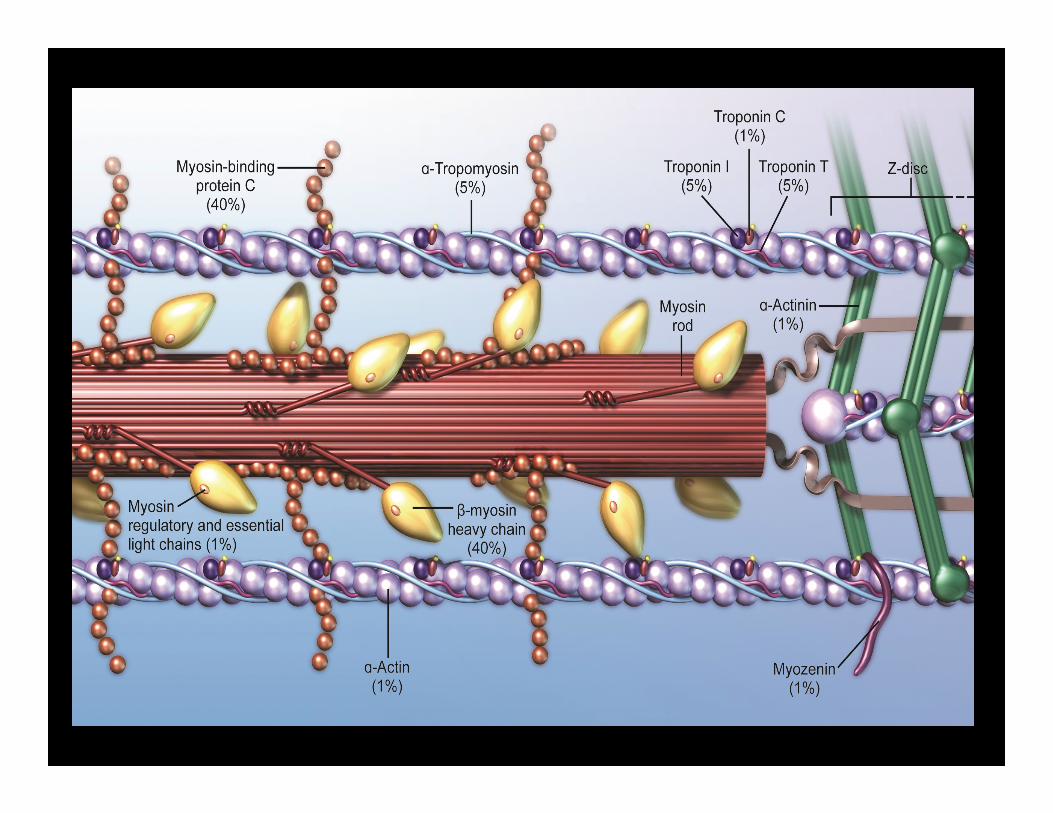
HCM : The Tip Of The Iceberg
Identified
Unidentified
?

Unexplained LVH
Sarcomeric ProteinMutations
Non-SarcomericMutations
AMP-Kinase(PRKAG2)
Lamp2(Danon)
Storage Diseases
~ 11 Genes---or more?
> 1500 mutations
FabryDisease
HCM Is A Global Disease
50 countries….all continents
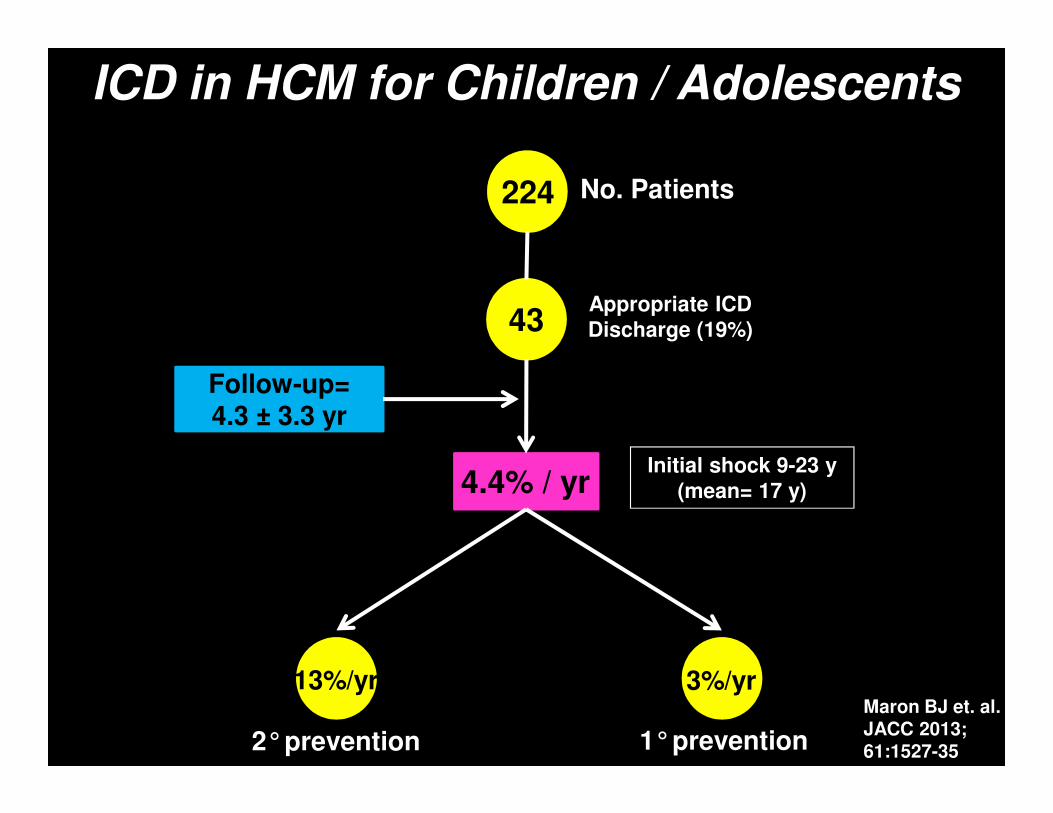
ICD in HCM for Children / Adolescents
224
43
4.4% / yr
13%/yr 3%/yr
No. Patients
Appropriate ICDDischarge (19%)
2°prevention 1°prevention
Follow-up=4.3 ± 3.3 yr
Initial shock 9-23 y (mean= 17 y)
Maron BJ et. al. JACC 2013;61:1527-35
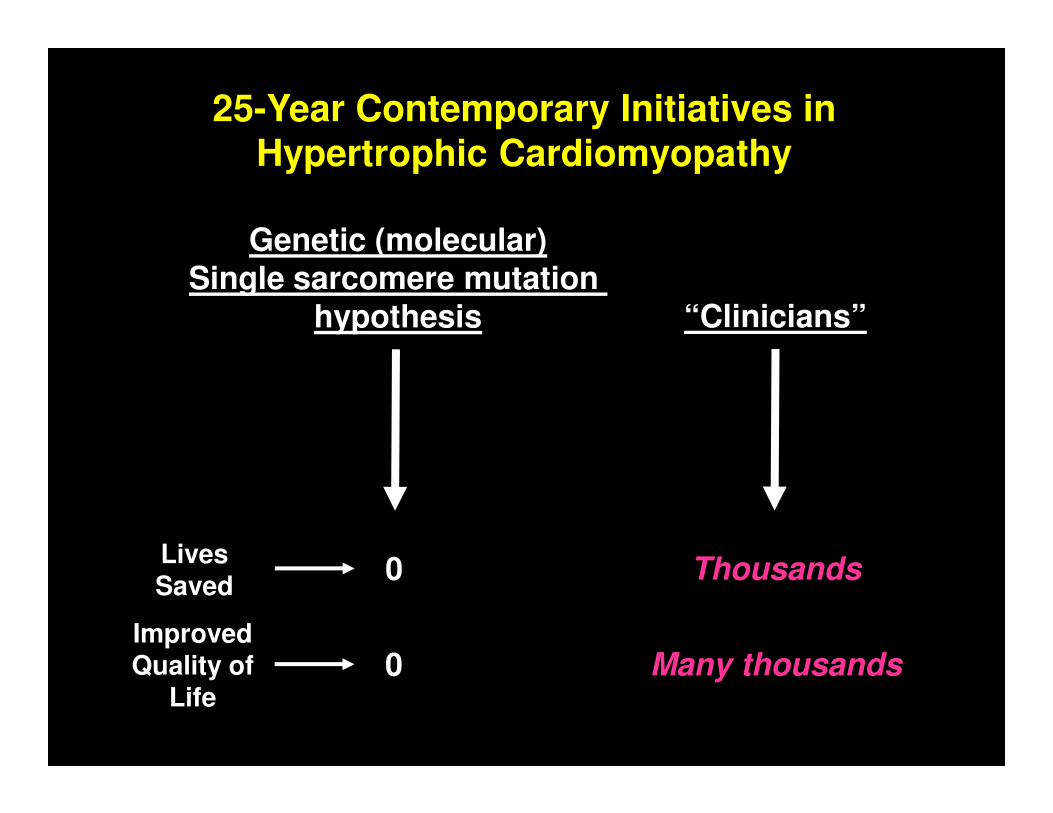
25-Year Contemporary Initiatives inHypertrophic Cardiomyopathy
Genetic (molecular)Single sarcomere mutation
hypothesis “Clinicians”
0 ThousandsLivesSaved
0 Many thousandsImprovedQuality of
Life
N Engl J Med 1980;303:322.
Dr. Michele Mirowski
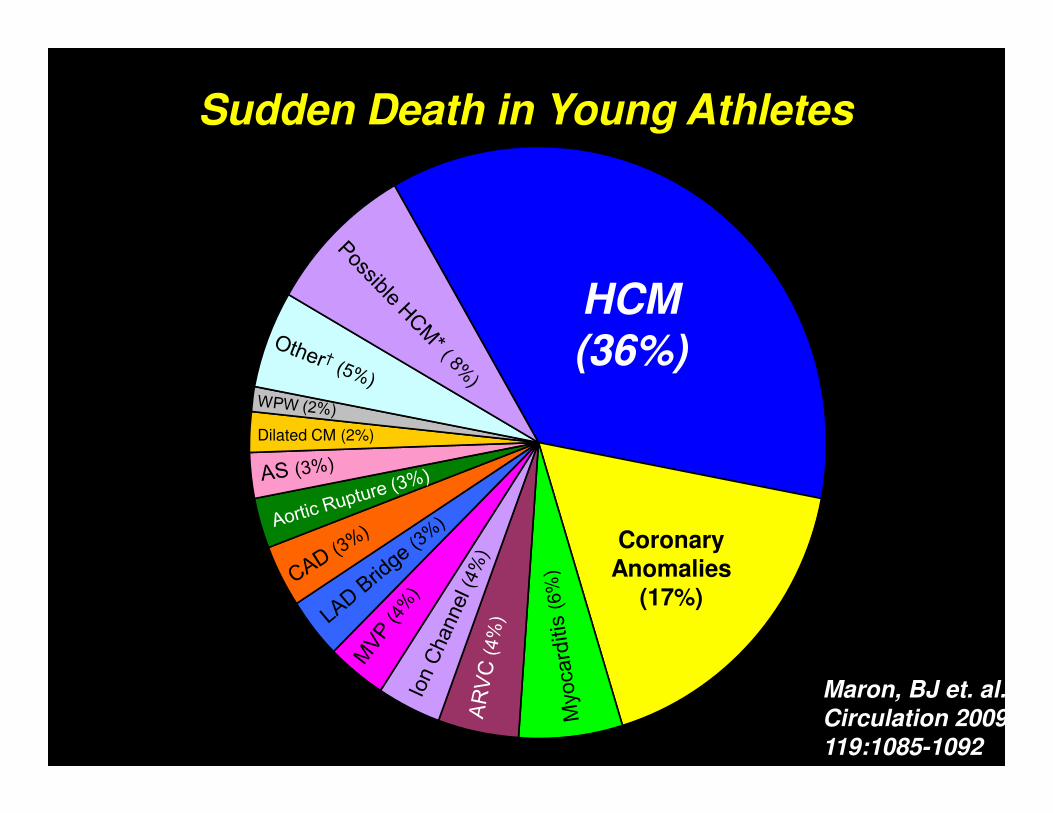
HCM(36%)
CoronaryAnomalies
(17%)
Dilated CM (2%)
Sudden Death in Young Athletes
Maron, BJ et. al. Circulation 2009;119:1085-1092

K.K. 23 Years with ICD and HCM
* preceded by asymptomatic
AF on ICD (3 weeks)
BrotherSD
(HCM)
36 504135 58 60
ICDimplant
ShockPolymorphic
VT(203/min)
VF x2shocks
(2 mo. apart)
AF*(cardioverted)
Amio200 mg
Xeralto
5 y 9 y 8 y
BD:2/19/56

Septal Scarring
Septal Scar No Scar
Post-ablation Post-myectomy
VS=30%LV 10%
Valeti et. al. JACC 2007;49:350
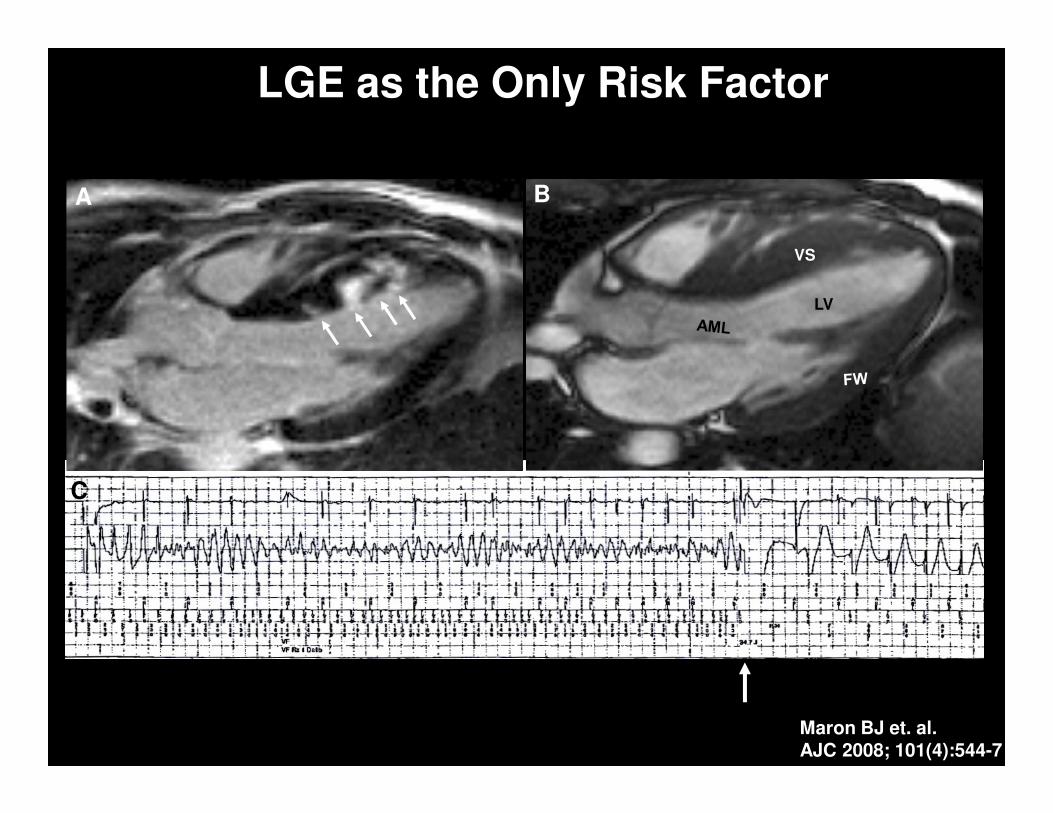
VS
LV
A B
C
LGE as the Only Risk Factor
Maron BJ et. al.AJC 2008; 101(4):544-7

HCM—ICD Registry
29(6%)
14
14
1
Deaths
ICDMalfunction
End-stage
Embolic stroke
Cancer, sepsis,
renal diseases,
suicide, CAD,
accidents
No HCM
HCM
HCM-Arrhythmias
(nl EF)
Maron, BJ et. al. JAMA 2007;298:405
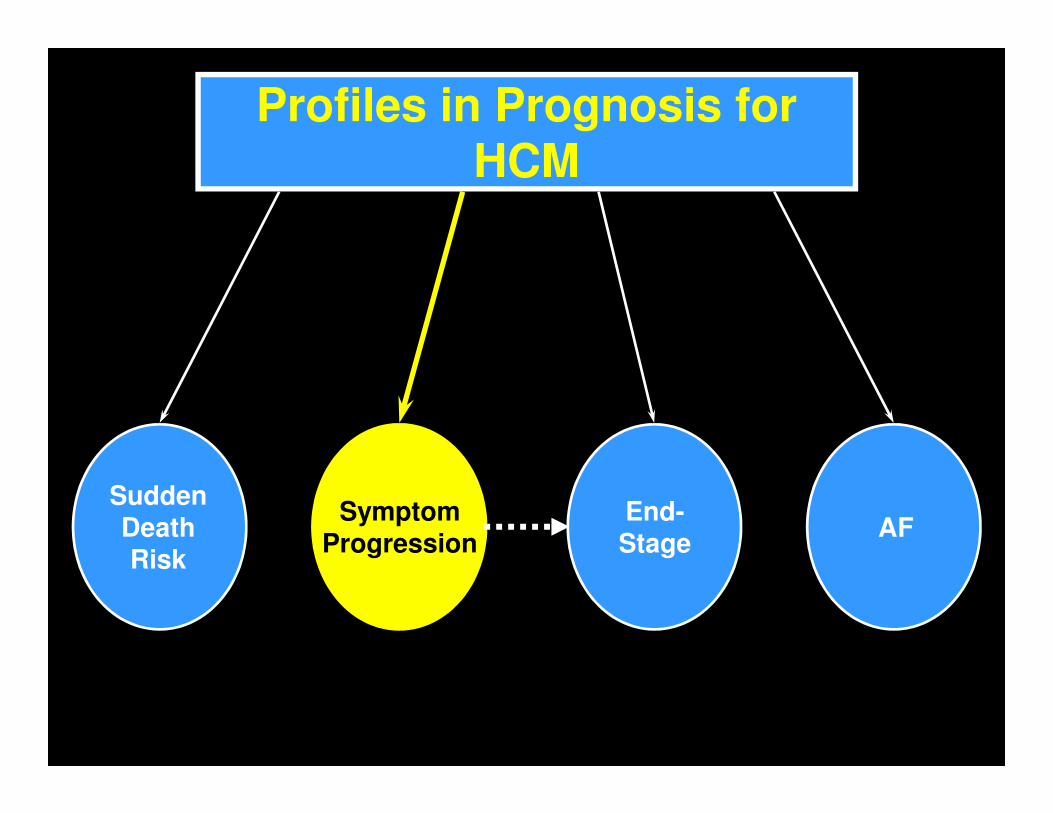
Profiles in Prognosis for HCM
SuddenDeathRisk
SymptomProgression
End-Stage
AF
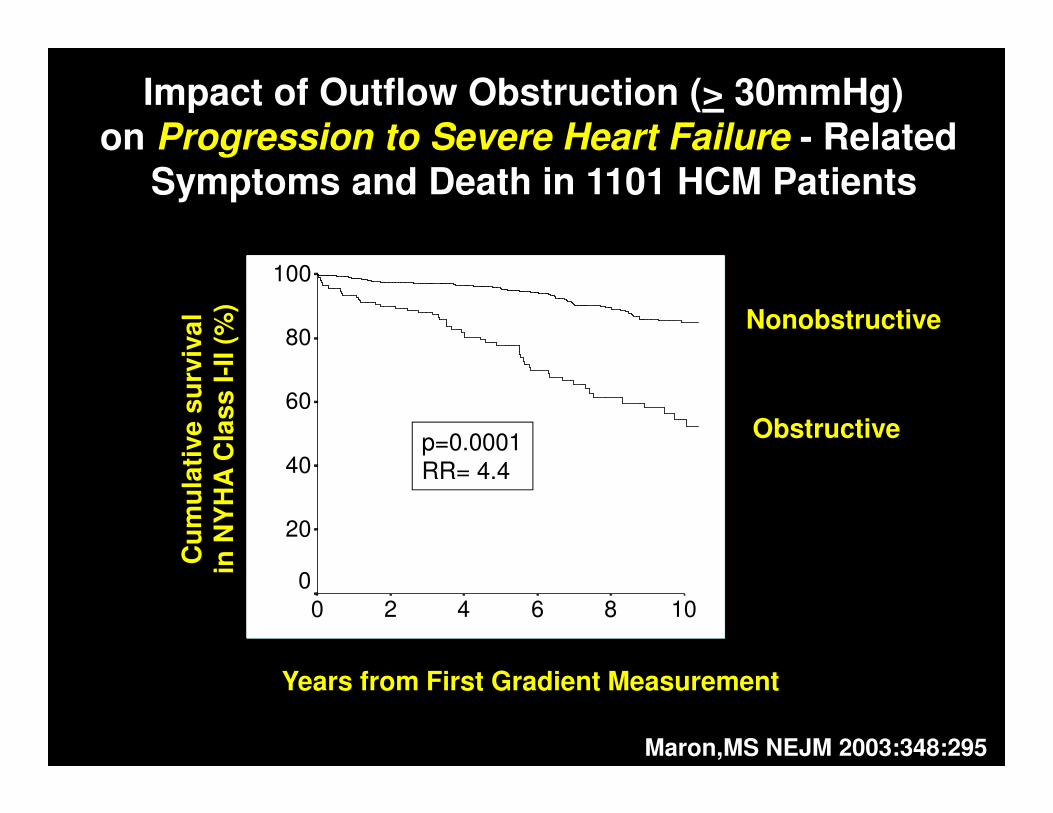
1086420
100
80
60
40
20
0
Nonobstructive
Obstructive
Years from First Gradient Measurement
Cu
mu
lati
ve
su
rviv
al
in N
YH
A C
las
s I-I
I (%
)
p=0.0001
RR= 4.4
Impact of Outflow Obstruction (> 30mmHg) on Progression to Severe Heart Failure - Related
Symptoms and Death in 1101 HCM Patients
Maron,MS NEJM 2003:348:295

Cardiovascular Societies &HCM Consensus Panels for
Myectomy vs. Alcohol Ablation
ACC 2003
ESC 2003
ACC 2011
AHA 2011
Myectomy
Myectomy
Myectomy
Myectomy
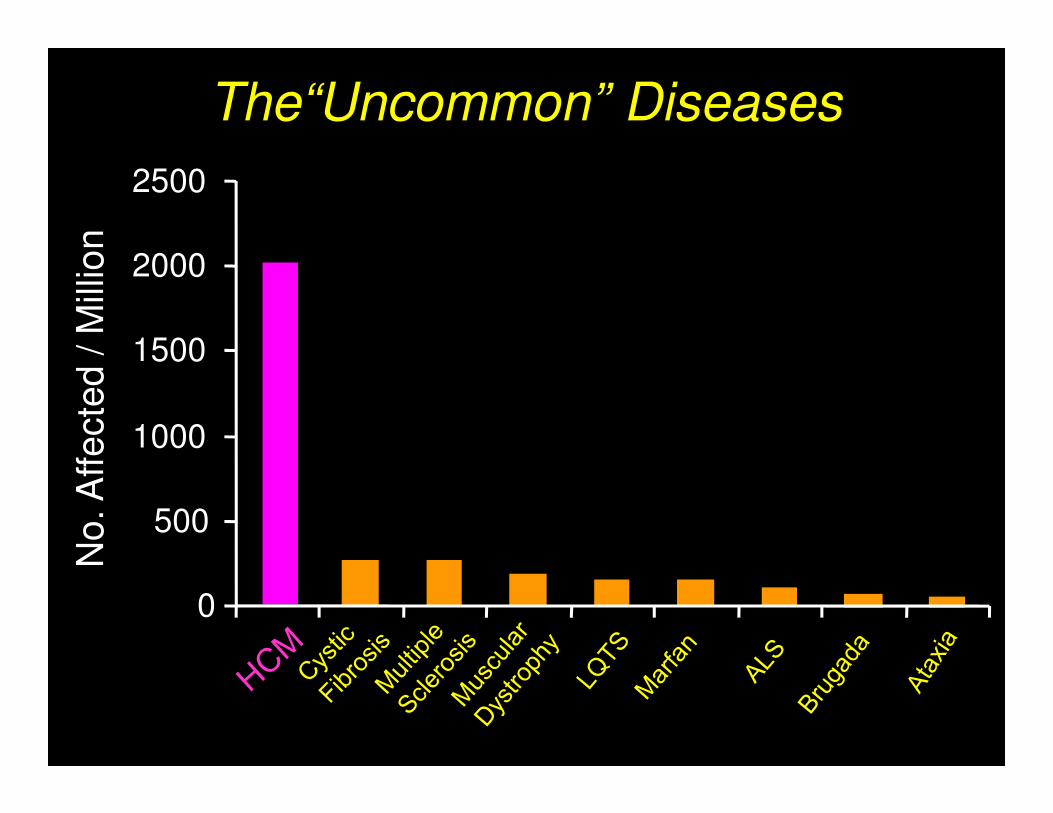
0
500
1000
1500
2000
2500
No
. A
ffe
cte
d / M
illio
nThe“Uncommon” Diseases

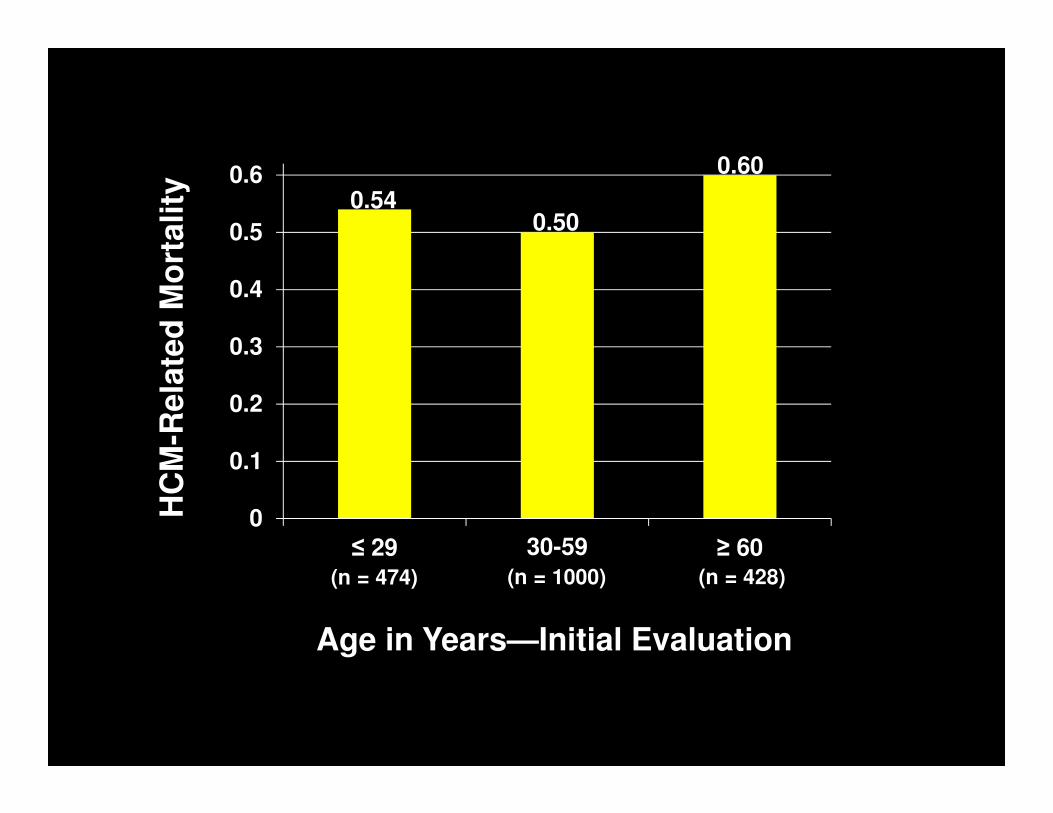
CONTEMPORARY HCM MORTALITY BY AGE: MHIF/Tufts
2015
<29 y 30-59 y >60 y Total
No. Patients
474 1000 428 1902
HCM Mortality
0.5%/y 0.5%/y 0.6%/y 0.5%/y
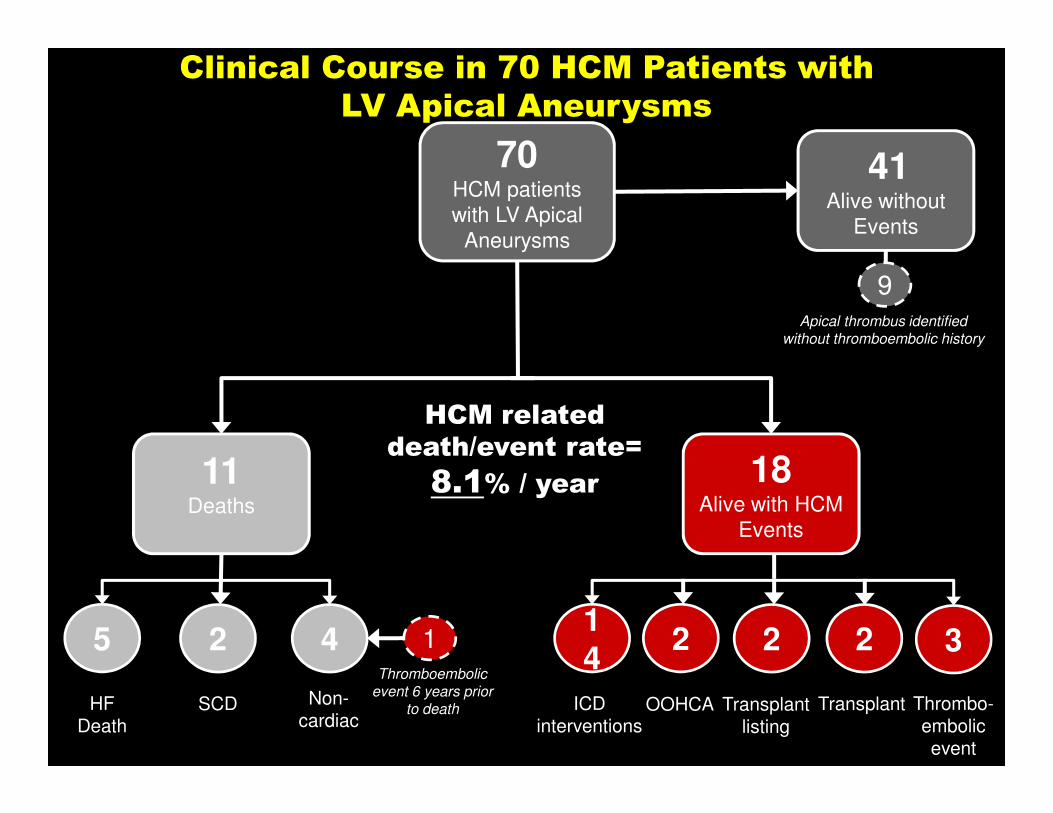
70HCM patients
with LV Apical
Aneurysms
11 Deaths
18Alive with HCM
Events
HCM related
death/event rate=
8.1% / year
5
HF Death
2
SCD
4
Non-cardiac
14
2
Transplant listing
2
Transplant
3
Thrombo-embolic event
ICD interventions
41Alive without
Events
2
OOHCA
1Thromboembolic
event 6 years prior
to death
Apical thrombus identified
without thromboembolic history
9
Clinical Course in 70 HCM Patients with
LV Apical Aneurysms

Operative Deaths**
Institution No. Myectomies Age (years) % Male No. %
Mayo Clinic (Rochester, MN) 1411 51 ±±±± 14 55 4† 0.3
Cleveland Clinic 1470Δ 55 ±±±± 14 55 6 0.4
Tufts Medical Center‡ (Boston) 348 52 ±±±± 15 56 4 1.1
Toronto General 306 49 ±±±± 13 62 2 0.6
Mount Sinai-St. Luke’s (NYC) 160 53 ± 14 48 1 0.6
Totals 3,695 54 ±±±± 14 55 17 0.4
Symbols:
* does not include myectomy associated with valve replacement, coronary artery bypass grafting
or resection of a subaortic membrane
** within 30 days of the myectomy
† includes 2 paIents with prior alcohol septal ablaIon; with these 2 paIents considered non-pure
myectomies, the Mayo mortality rate would be only 0.15%
‡ newest myectomy center with operations performed over only 11 years with first procedure
in 2004, while data for the other centers encompasses 15 yearsΔ includes 19% of patients with mitral valve repair
Abbreviations:
MN = Minnesota; NYC = New York City
Operative Mortality Associated with Septal Myectomy* at North American
Hypertrophic Cardiomyopathy Centers, 2000-2014

HCM is Unpredictable
(15%)
(15%)
(7%)
(7%)
(<1%)
(<1%)
(<1%)
(<1%)
(<1%)
(<1%)
0
0.5
1
1.5
2
% H
CM
Mo
rta
lity
HCM-Related Mortality
0
0.5
1.5
1
6
General U.S.Population
0.8%/y
0.5%/y
1.5%/y
3-6%/y
Early HCMReferral Cohorts
HCM Cohorts:Prior to utilization
of current treatmentstrategies/
interventions
ICD interventionHeart transplant/surgical myectomy
RCA/defibrillation/hypothermia
Present HCMCohorts:
Contemporarytreatment
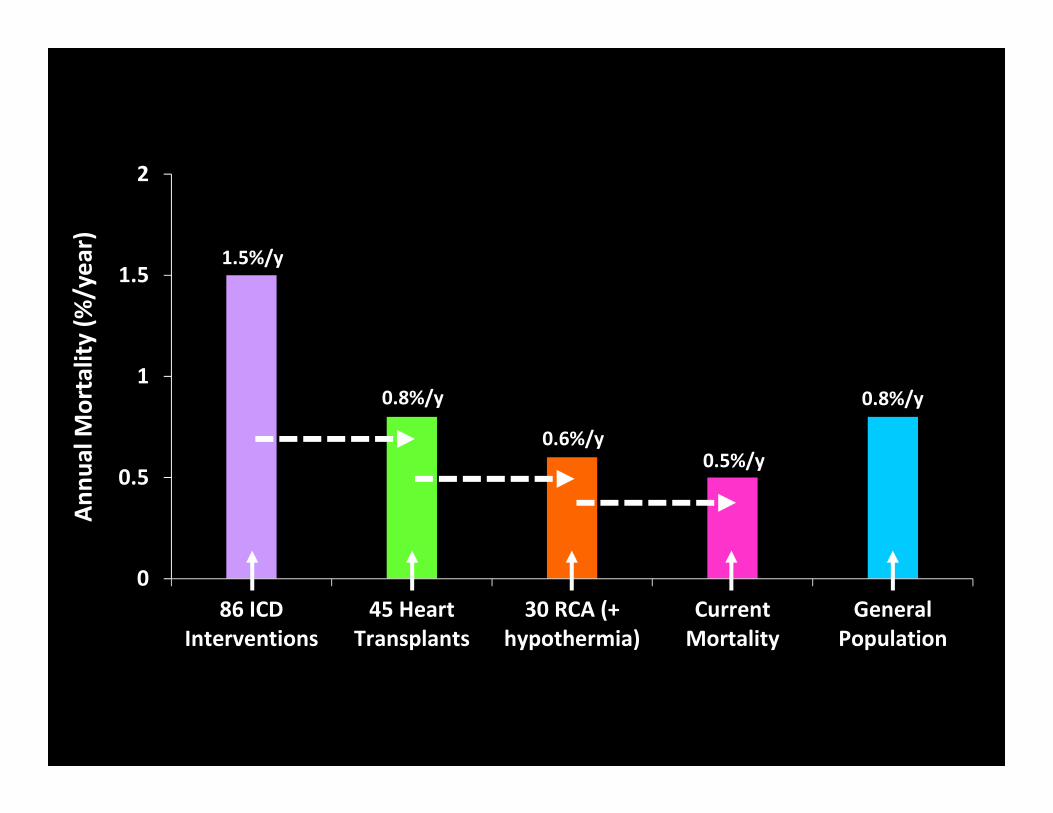
0
0.5
1
1.5
2
86 ICD
Interventions
45 Heart
Transplants
30 RCA (+
hypothermia)
Current
Mortality
General
Population
An
nu
al
Mo
rta
lity
(%
/ye
ar)
1.5%/y
0.8%/y
0.6%/y0.5%/y
0.8%/y
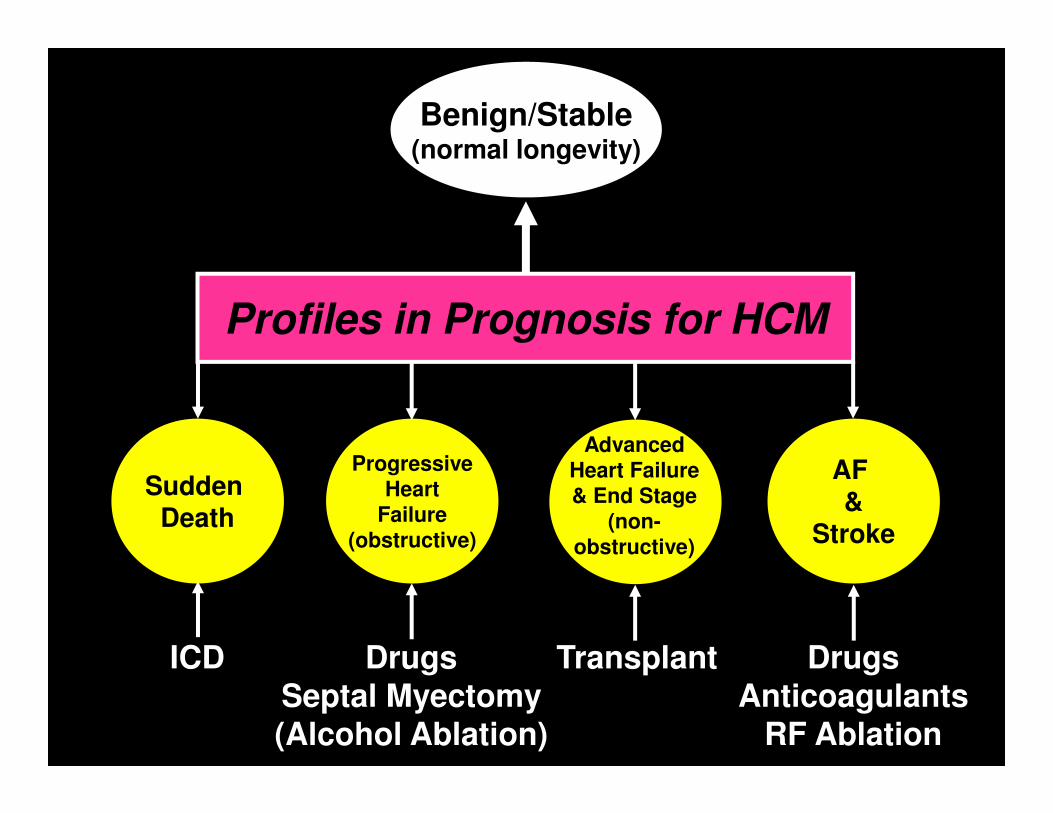
ICD
Sudden Death
ProgressiveHeart
Failure(obstructive)
AF &
Stroke
Benign/Stable(normal longevity)
DrugsSeptal Myectomy(Alcohol Ablation)
Transplant DrugsAnticoagulants
RF Ablation
Profiles in Prognosis for HCM
AdvancedHeart Failure& End Stage
(non-obstructive)

Highest
Intermediate
Lowest
2°prevention
Cardiac arrest/sustained VT
1°prevention
Family history HCM-SDUnexplained syncopeMultiple-repetitive NSVT (Holter)Abnormal exercise BP responseLGE ≥ 15% of LV massMassive LVH ≥ 30 mm
Rare subgroups/potential arbitrators
End-stage (EF < 50%)LV apical aneurysmMarked LV outflow obstruction (rest)Modifiable
Intense competitive sports
CADLGE ≥ 15% of LV massAge ≥ 60yAlcohol septal ablation (?)
ICD