Hypertensive Retinopathy Signs as Risk Indicators of Cardiovascular Morbidity and Mortality
38
Laporan kasus Myopia Patologi ODS PEMBIMBING Dr. Cut Masdalena, M.Ked (Oph), Sp.M DISUSUN OLEH Cut Rahmi Nadhia Putri, S.ked 080610028 KEPANITRAAN KLINIK ILMU PENYAKIT MATA RUMAH SAKIT UMUM Dr. FAUZIAH BIREUN PROGRAM STUDI PENDIDIKAN DOKTER UNIVERSITAS MALIKUSSALEH TAHUN 2014
description
hypertensive
Transcript of Hypertensive Retinopathy Signs as Risk Indicators of Cardiovascular Morbidity and Mortality

Laporan kasus
Myopia Patologi ODS
PEMBIMBING Dr. Cut Masdalena, M.Ked (Oph), Sp.M
DISUSUN OLEHCut Rahmi Nadhia Putri, S.ked
080610028
KEPANITRAAN KLINIK ILMU PENYAKIT MATARUMAH SAKIT UMUM Dr. FAUZIAH BIREUN
PROGRAM STUDI PENDIDIKAN DOKTER UNIVERSITAS MALIKUSSALEH
TAHUN 2014

Jurnal
Hypertensive retinopathy signs as risk indicators of cardiovascular
morbidity and mortality
PEMBIMBING Dr. Cut Masdalena, M.Ked (Oph), Sp.M
DISUSUN OLEHCut Rahmi Nadhia Putri, S.ked
080610028
KEPANITRAAN KLINIK ILMU PENYAKIT MATARUMAH SAKIT UMUM Dr. FAUZIAH BIREUN
PROGRAM STUDI PENDIDIKAN DOKTER UNIVERSITAS MALIKUSSALEH
TAHUN 2014

Hypertensive retinopathy signs as risk indicators of cardiovascular morbidity and
mortality
Abstract
Hypertensive retinopathy has long been regarded as a risk indicator for systemic morbidity and
mortality. New population-based studies show that hypertensive retinopathy signs are strongly
associated with blood pressure, but inconsistently associated with cholesterol and other risk
factors of atherosclerosis. Mild hypertensive retinopathy signs, such as generalized and focal
retinal arteriolar narrowing and arteriovenous nicking, are weakly associated with systemic
vascular diseases. Moderate hypertensive retinopathy signs, such as isolated microaneurysms,
haemorrhages and cotton-wool spots, are strongly associated with subclinical cerebrovascular
disease and predict incident clinical stroke, congestive heart failure and cardiovascular mortality,
independent of blood pressure and other traditional risk factors. These data support the concept
that an assessment of retinal vascular changes may provide further information for vascular risk
stratification in persons with hypertension.
Introduction
The retinal circulation undergoes a series of pathophysiological changes in response to elevated
blood pressure.1 These changes are manifested clinically as a spectrum of signs commonly
referred to as hypertensive retinopathy.2 Hypertensive retinal vascular signs can be broadly
classified into arteriolar changes (generalized arteriolar narrowing, focal arteriolar narrowing,
arteriovenous nicking and arteriolar wall opacification) and more advanced retinopathy lesions
(microaneurysms, blot and flame-shaped haemorrhages, cotton-wool spots, hard exudates and
optic disk swelling). With the exception of disk swelling, these signs can be detected fairly
frequently in adult populations, even in persons without a known history of hypertension.3
The significance of hypertensive retinopathy signs as risk indicators of systemic morbidity and
mortality has long been recognized since their description in patients with renal and
cerebrovascular disease by Marcus Gunn in the late nineteenth century.4,,5 In fact, an assessment
of hypertensive retinopathy signs for risk stratification is supported by international hypertension
management guidelines, including the US Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood Pressure (JNC) and the British Society of
Hypertension.6,,7 The guidelines emphasize that hypertensive retinopathy, together with left
ventricular hypertrophy and renal impairment, may be considered an indicator of target organ

damage, suggesting that physicians should consider a more aggressive approach in managing
these patients.7
Classification and diagnosis
The traditional classification of hypertensive retinopathy, dating back to 1939, was based on
work by Keith et al.8 Although the modern classification system bears their name, the original
paper8 was not an attempt to classify hypertensive retinopathy signs but to show that severity of
hypertension itself was predictive of mortality. This classification and its modifications typically
consist of four grades of hypertensive retinopathy with increasing severity: grade 1 consists of
‘mild’ generalized retinal arteriolar narrowing; grade 2 consists of ‘more severe’ generalized
narrowing, focal areas of arteriolar narrowing and arteriovenous (AV) nicking; grade 3 consists
of grade 1 and 2 signs plus the presence of retinal haemorrhages, microaneurysms, hard exudates
and cotton-wool spots; grade 4, which is sometimes referred to as accelerated (malignant)
hypertensive retinopathy, consists of signs in the preceding three grades plus optic disk swelling
and macular oedema. Whereas the 3 year survival of persons with grade 1 hypertensive
retinopathy was 70%, the survival was only 6% in those with grade 4 retinopathy.8 The major
limitation of this classification system is the difficulty in distinguishing early hypertensive
retinopathy severity (i.e. grade 1 from grade 2), and several proposals for a new systems have
been made.2,3,,9 A simple three-grade classification is proposed at the end of this article
It is important for the physician to be aware that some of these signs, particularly
microaneurysms, haemorrhages and cotton-wool spots, may also be found in other systemic and
ocular conditions (Table 1). The presence of hard exudates, for example, is more typical of
diabetic retinopathy, while unilateral retinal signs may indicate carotid artery disease. Visual loss
is suggestive of retinal vein occlusion, diabetic retinopathy, accelerated hypertension and other
retinal diseases. Thus, in atypical scenarios, appropriate investigations may be necessary to
exclude these important diseases.
Table 1
Differential diagnoses of isolated retinal haemorrhage, cotton-wool spots and microaneurysms
Epidemiology
Recent population-based studies have provided data on the prevalence of various hypertensive
retinopathy signs in the general population.10–17 Data from these studies indicates that

hypertensive retinopathy signs, defined from retinal photographs, are seen in 3–14% of adult
individuals aged ≥40 years (Fig. 1).
View larger version:
Fig. 1
Prevalence of hypertensive retinopathy: signs and selected population studies.
There are fewer studies of the long-term incidence of new hypertensive retinopathy signs.10 Data
from the Beaver Dam Eye Study, a study of 4926 adults aged 43–86 years in Wisconsin, showed
that the 5 year incidence of focal arteriolar narrowing, AV nicking, retinal haemorrhages and
microaneurysms in people without diabetes ranged from 6% to 10%.
Associations with morbidity and mortality
Blood pressure
An abundance of data from clinical and population-based studies show a strong, graded and
consistent association of hypertensive retinopathy signs with blood pressure (Table 2).10–13,15–17
Both the presence11 and the development of new hypertensive retinopathy signs10 are strongly
related to elevated blood pressure. In the Beaver Dam Eye Study, hypertensive individuals were
50–70% more likely to have retinal haemorrhages and microaneurysms, 30–40% more likely to
have focal arteriolar narrowing and 70–80% more likely to have AV nicking than normotensive
people. In addition, hypertensive persons whose blood pressure was still elevated despite use of
antihypertensive medications, an indication of ‘poorer’ control, were more likely to develop
retinopathy than individuals whose blood pressure was controlled with medication.
Systemic associations of hypertensive retinopathy signs: selected population-based studies
Several recent population-based studies have used standardized retinal photography methods to
define hypertensive retinopathy signs and computer-based imaging methods to measure retinal
arteriolar diameters from photographs. One of these is the Atherosclerosis Risk in Communities
(ARIC) study, a population-based cohort investigation of cardiovascular disease of persons aged
45–64 years selected from four US communities. Retinal photography was added as a component

of the examination and graded for the presence and severity of hypertensive retinal
microvascular changes. The ARIC study demonstrated that generalized retinal arteriolar
narrowing, indicated by narrower arteriolar diameters determined from photographs, was
strongly associated with elevated blood pressure, a finding now confirmed in five other
populations using similar methods.18–22 However, the clinical applicability of these findings is
unclear, as the subtle degree of arteriolar narrowing associated with elevated blood pressure is
difficult to estimate from ophthalmoscopy. For example, each 10 mmHg increase in mean
arterial blood pressure was associated with a reduction of only 6 µm (3%) reduction in retinal
arteriolar diameters in one study.22
Data from ARIC and other studies provides increasing evidence that the pattern of associations
of blood pressure with specific hypertensive retinopathy signs varies. Generalized retinal
arteriolar narrowing and AV nicking appear to be markers of cumulative long-term hypertension
damage, and are independently linked with past blood pressure levels measured 5–8 years before
the retinal assessment.20,21,,23 In contrast, focal arteriolar narrowing, retinal haemorrhages,
microaneurysms and cotton-wool spots reflect more transient changes of acute blood pressure
elevation, and are linked only with concurrent blood pressure measured at the time of the retinal
assessment.20,,21
An important finding in the Beaver Dam Eye Study was the observation that the association
between blood pressure and retinal microvascular signs appears to be weaker with age, 22 possibly
reflecting greater sclerosis of retinal arterioles in older persons.
Atherosclerosis risk factors
In contrast with its strong association with blood pressure, hypertensive retinopathy signs have
not been consistently linked to either direct measures of atherosclerosis, such as carotid artery
stenosis, or atherosclerosis risk factors, such as hyperlipidaemia (Table 2). In the ARIC study,
while controlling for blood pressure, generalized arteriolar narrowing was associated with carotid
artery plaque but not stenosis, AV nicking was associated with carotid artery stenois but not
plaque and focal arteriolar narrowing was not related to either carotid artery measure.12
In the Hoorn Study in The Netherlands hyperglycaemia and abdominal obesity were
independently related to incidence of retinal haemorrhages, microaneurysms, hard exudates and
cotton-wool spots in the non-diabetic general population.24 In the ARIC study, hypertensive
retinopathy signs were related to larger waist circumference, an indicator of abdominal obesity.25

However, not all studies have found associations between hypertensive retinopathy signs and
abdominal obesity or dyslipidaemia.18
The association of hypertensive retinopathy signs with novel atherosclerosis risk factors has also
been investigated. Cross-sectional associations of retinal arteriolar narrowing and AV nicking
with biomarkers of inflammation (e.g. white blood cell counts) and endothelial dysfunction (e.g.
von Willebrand factor) have been reported in the ARIC study12 and by other groups.18
These studies emphasize the fact that typical signs of hypertensive retinopathy may be related to
vascular processes other than blood pressure.
Stroke and cerebrovascular disease
Numerous studies have reported a strong association between various hypertensive retinopathy
signs and both subclinical and clinical cerebrovascular disease26–28 and stroke mortality.29 In the
ARIC study, individuals with retinal haemorrhages, microaneurysms and cotton-wool spots, as
defined from photographs, were two to four times more likely to develop an incident clinical
stroke within 3 years, even when controlling for the effects of blood pressure, cigarette smoking,
lipids and other risk factors.30 Among the participants without stroke or transient ischaemic
attack, hypertensive retinopathy signs were also related to changes in cognitive function, as
defined by standardized neuropsychological tests over a 6 year period,31 and to cerebral white
matter hyperintensity lesions 32 and atrophy, as defined from MRI scans.33
One of the key observations was that the presence of hypertensive retinopathy may offer
additional predictive value of clinical stroke risk in individuals with MRI-defined subclinical
cerebral disease. In the ARIC study, individuals with both MRI-defined white matter lesions and
hypertensive retinopathy were 18 times more likely [relative risk (RR) 18.1; 95% confidence
interval (CI) 5.9–55.4] to develop an incident clinical stroke event than those without either
white matter lesions or hypertensive retinopathy.32
Coronary heart disease and heart failure
Hypertensive retinopathy signs have been linked with both subclinical and clinical coronary
heart disease and congestive heart failure. For example, various hypertensive retinopathy signs
have been associated with ischaemic changes on electrocardiogram,34 severity of coronary artery
stenosis on angiography35 and incident coronary heart disease and myocardial infarction in men36
and women.37

The ARIC study reported that, after controlling for pre-existing risk factors, individuals with
retinal haemorrhages, microaneurysms and cotton-wool spots were twice as likely (RR 1.96;
95% CI 1.52–2.56) to develop congestive heart failure as individuals without retinopathy.38 In
fact, among low-risk individuals (without pre-existing heart disease, diabetes or hypertension),
the presence of hypertensive retinopathy signs predicted a 3-fold increased risk of heart failure
events (RR 2.97, 95% CI 1.49–5.91). This is compatible with the interpretation that
microvascular damage to the myocardium from hypertension and other systemic processes may
be a contributing factor in the development of heart failure.
Other systemic diseases
A number of systemic diseases have been associated with different hypertensive retinopathy
signs (Table 2). In the ARIC study, individuals with AV nicking, retinal haemorrhages,
microaneurysms and cotton-wool spots were more likely to develop renal dysfunction than those
without these signs.39 This association was independent of blood pressure, diabetes and other risk
factors, and was also seen in persons without diabetes or hypertension.
Data from three population-based studies suggest that generalized retinal arteriolar narrowing, a
marker of blood pressure damage, may in fact predict the development of incident
hypertension.40–42 The ARIC study showed that normotensive participants who had generalized
arteriolar narrowing were 60% more likely to be diagnosed with hypertension within a
subsequent 3-year period than normotensive individuals without arteriolar narrowing (RR 1.62;
95% CI 1.21–2.18).41 This association was independent of an individual’s pre-existing blood
pressure levels, body mass index and other known hypertension risk factors.
The ARIC and Beaver Dam Eye Studies have also shown that generalized retinal arteriolar
narrowing predicts the incidence of type 2 diabetes among persons initially free of diabetes,
independent of diabetes risk factors.43,,44 Thus generalized arteriolar narrowing, possibly
reflecting various systemic peripheral arteriolar changes, may be a preclinical marker of overt
hypertension and diabetes.
Cardiovascular mortality
The study by Keith et al.8 was amongst the first to show a dose-dependent increase in mortality
with severity of hypertensive retinopathy changes. Since then, numerous studies conducted in the
1950s and 1960s have further shown that persons with hypertension and retinopathy signs are at
increased risk of mortality.34,45–47 However, inferences from many older studies are limited

because of the subjective evaluation of hypertensive retinopathy signs, the lack of data on cause-
specific mortality rates and inadequate control for potential confounders such as blood pressure
and diabetes.
Nonetheless, more recent studies have provided stronger evidence that hypertensive signs are
markers of mortality risk. In a nested case–control analysis of the Beaver Dam Eye Study,
individuals with retinal microaneurysms and retinal haemorrhages were twice as likely to die
from cardiovascular events as those without these signs.29
Clinical applications
Data from recent studies support the current hypertension guidelines regarding the prognostic
significance of retinopathy signs.6,,7 The information obtained from an assessment of the
retinopathy status appears to be independent of, and qualitatively different from, that of
measuring blood pressure or serum lipids, as the presence of retinopathy signs indicates
susceptibility and the onset of preclinical systemic vascular disease. In particular, it seems that
individuals with certain hypertensive retinopathy signs (e.g. retinal haemorrhages,
microaneurysms and cotton-wool spots) should be more closely monitored for cardiovascular
risk, and may benefit from further investigations (e.g. echocardiogram for heart function) if
clinically indicated.
A three-grade classification system for hypertensive retinopathy is shown in Table 3, and a
suggested approach for patients with various hypertensive retinopathy grades is shown in Figure
2. It is important to emphasize that the management for patients with hypertension and
cardiovascular disease should continue to follow standard risk prediction approaches (i.e. based
on assessment of age and gender of the patient, blood pressure and lipid levels, cigarette smoking
status etc).
Table 3
Classification of hypertensive retinopathy

Fig. 2
Evaluation and management of a patient with hypertensive retinopathy.
The classification in Table 3 groups hypertensive retinopathy signs into mild, moderate and
accelerated (malignant). Patients with mild hypertensive retinopathy signs (Figure 3A) will
probably require routine care, and blood pressure control should be based on established
guidelines.6,,7 Patients with moderate hypertensive retinopathy signs (retinal haemorrhage,
microaneurysm, cotton-wool spots) (Fig. 3B) may benefit from further assessment of vascular
risk (e.g. assessment of cholesterol levels) and, if clinically indicated, appropriate risk reduction
therapy (e.g. cholesterol-lowering agents). Patients with accelerated hypertensive retinopathy
(bilateral disk swelling in the presence of moderate hypertensive retinopathy) (Figure 3C), which
is relatively rare in the general population but may occur in conjunction with severe
hypertension, will continue to need urgent immediate antihypertensive management, including
possible administration of intravenous medication. In such scenarios, physicians should aim for a
small stepwise control of blood pressure over a few hours, and avoid a sudden reduction in blood
pressure which may lead to stroke.

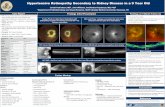
Fig. 3
(A) Mild hypertensive retinopathy: AV nicking (black arrow) and focal narrowing (white arrow).
(B) Moderate hypertensive retinopathy: retinal haemorrhages (black arrows), AV nicking (white
arrow) and generalized retinal arteriolar narrowing. (C) Accelerated (malignant) retinopathy:
swelling of optic disk, retinal haemorrhages and cotton-wool spots.
There have been several experimental studies48,,49 and clinical reports50–52 of regression of
hypertensive retinopathy signs with control of blood pressure. With adequate hypertension
treatment, resolution of hypertensive retinopathy signs may occur over a period of 6 months 52 to
a year.51 Thus follow-up of patients for up to a year after diagnosis may be needed.
These studies also provide some evidence that specifically targeting the microcirculation in
hypertensive individuals may further reduce cardiovascular morbidity and mortality.For
example, certain antihypertensive agents (e.g. ACE inhibitors) have been suggested to have
direct beneficial effects on microvessel structure and function, beyond their primary effect on
lowering blood pressure.52 Therefore such agents may have added therapeutic value in preventing
and treating cardiovascular diseases. However, whether these specific therapies may reverse or
reduce retinopathy changes, and whether this will result in reduced cardiovascular risk, is
currently unclear.
Conclusions
Hypertensive retinopathy signs may differ in their associations with systemic diseases. Isolated
retinal haemorrhages, microaneurysms and cotton-wool spots (moderate hypertensive
retinopathy) appear to be associated with risk of subclinical and clinical stroke, other
cerebrovascular outcomes, congestive heart failure and cardiovascular mortality, independent of
traditional risk factors. In contrast, the systemic associations for generalized retinal arteriolar
narrowing, focal arteriolar narrowing and AV nicking (mild hypertensive retinopathy) appear to
be weaker and less consistent. An assessment of hypertensive retinopathy signs may provide
important information for vascular risk stratification

References
1. Wong TY, Mitchell P (2004) Hypertensive retinopathy. N Engl J Med 351, 2310–17.
2. Tso M, Jampol LM (1982) Pathophysiology of hypertensive retinopathy. Ophthalmology,
89, 1132–45.
3. Wong TY, Klein R, Klein BEK, Tielsch JM, Hubbard LD, Nieto FJ (2001) Retinal
microvascular abnormalities, and their relation to hypertension, cardiovascular diseases
and mortality. Surv Ophthalmol, 46, 59–80.
4. Gunn RM (1892) Ophthalmoscopic evidence of (1) arterial changes associated with
chronic renal diseases and (2) of increased arterial tension. Trans Am Ophthalmol Soc,
12, 124–5.
5. Gunn RM (1898) On ophthalmoscopic evidence of general arterial disease. Trans
Ophthalmol Soc UK, 18, 356–81.
6. Williams B, Poulter NR, Brown MJ, Davis M, McInnes GT, Potter JF, Sever PS, Thom
SM. British Hypertension Society guidelines for hypertension management 2004 (BHS-
IV): summary. Bmj 2004; 328: 634–40
7. Chobanian AV, Bakris GL, Black H.R et al. (2003)The Seventh Report of the Joint
National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood
Pressure: the JNC7 Report. JAMA, 289: 2560–72.
8. Keith NM, Wagener HP, Barker NW (1939) Some different typs of essential hypertension:
their course and prognosis. Am J Med Sci, 197, 332–43.
9. Dodson PM, Lip GY, Eames SM, Gibson JM, Beevers DG (1996) Hypertensive
retinopathy: a review of existing classification systems and a suggestion for a simplified
grading system. J Hum Hypertens, 10, 93–8.
10. Klein R, Klein BEK, Moss SE (1997) The relation of systemic hypertension to changes in
the retinal vasculature. The Beaver Dam Eye Study. Trans Am Ophthalmol Soc, 95, 329–
50.
11. Klein R, Klein BEK, Moss SE, Wang Q (1994) Hypertension and retinopathy, arteriolar
narrowing and arteriovenous nicking in a population. Arch Ophthalmol, 112, 92–8.
12. Klein R, Sharrett AR, Klein BEK et al. Are retinal arteriolar abnormalities related to
atherosclerosis? The Atherosclerosis in Communities Study. Arterioscler Thromb Vasc
Biol, 20, 1644–50.

13. Sharp PS, Chaturvedi N, Wormald R et al. (1995) Hypertensive retinopathy in Afro-
Caribbeans and Europeans. Prevalence and risk factor relationships. Hypertension, 25,
1322–5.
14. Stolk RP, Vingerling JR, de Jong PT et al. Retinopathy, glucose, and insulin in an elderly
population. The Rotterdam Study. Diabetes, 44, 11–15.
15. Wang JJ, Mitchell P, Leung H, Rochtchina E, Wong TY, Klein R (2003) Hypertensive
retinal vessel wall signs in the general older population: the Blue Mountains Eye Study.
Hypertension, 42, 534–41.
16. Wong TY, Klein R, Sharret AR et al. 2003, The prevalence and risk factors of retinal
microvascular abnormalities in older people. The Cardiovascular Health Study.
Ophthalmology, 110, 658–66.
17. Yu T, Mitchell P, Berry G, Li W, Wang JJ (1998) Retinopathy in older persons without
diabetes and its relationship to hypertension. Arch Ophthalmol, 116, 83–9.
18. Ikram MK, de Jong FJ, Vingerling JR et al. (2004) Are retinal arteriolar or venular
diameters associated with markers for cardiovascular disorders? The Rotterdam Study.
Invest Ophthalmol Vis Sci, 45, 2129–34.
19. Leung H, Wang JJ, Rochtchina E et al. (2003) Relationships between age, blood pressure
and retinal vessel diameters in an older population. Invest Ophthalmol Vis Sci, 44, 2900–
4.
20. Sharret AR, Hubbard LD, Cooper LS et al. (1999) Retinal arteriolar diameters and
elevated blood pressure. The Atherosclerosis Risk in Communities Study. Am J
Epidemiol, 150, 263–70.
21. Wong TY, Hubbard LD, Klein R et al. (2002) Retinal microvascular abnormalities and
blood pressure in older people: The Cardiovascular Health Study. Br J Ophthalmol, 86,
1007–13.
22. Wong TY, Klein R, Klein BEK, Meuer SM, Hubbard LD (2003) Retinal vessel diameters
and their associations with age and blood pressure. Invest Ophthalmol Vis Sci, 44, 4644–
50.
23. Leung H, Wang JJ, Rochtchina E, Wong TY, Klein R, Mitchell P (2004) Impact of current
and past blood pressure on retinal arteriolar diameter in an older population. J
Hypertens, 22, 1543–9.

24. van Leiden HA, Dekker JM, Moll AC et al. (2003) Risk factors for incident retinopathy in
a diabetic and nondiabetic population: the Hoorn Study. Arch Ophthalmol, 121, 245–51.
25. Wong TY, Duncan BB, Golden SH et al. (2004) Associations between the metabolic
syndrome and retinal microvascular signs: the Atherosclerosis Risk in Communities
Study. Invest Ophthalmol Vis Sci, 45, 2949–54.
26. Svarsudd K, Wedel H, Aurell E, Tibber G (1978) Hypertensive eye ground changes:
prevalence, relation to blood pressure and prognostic importance. Acta Med Scand,
1978; 204: 159–167.
27. Tanaka H, Hayashi M, Date C et al. (1985) Epidemiolgic studies of stroke in Shibata, a
Japanese provincial cuty: preliminary report on risk factors for cerebral infaction.
Stroke, 16, 773–80.
28. Nakayama T, Date C, Yokoyama T, Yoshiike N, Yamaguchi M, Tanaka H (1997) A 15.5-
year follow-up study of stroke in a Japanese provincial city. The Shibata Study. Stroke,
28, 45–52.
29. Wong TY, Klein R, Nieto FJ et al. (2003) Retinal microvascular abnormalities and ten-
year cardiovascular mortality. A population-based case-control study. Ophthalmology,
110, 933–40.
30. Wong TY, Klein R, Couper DJ et al. (2001) Retinal microvascular abnormalities and
incident clinical strokes. The Atherosclerosis Risk in the Communities Study. Lancet, 258,
1134–40.
31. Wong TY, Klein R, Sharret AR, et al. (2002) Retinal microvascular abnormalities and
cognitive impairment in middle-aged persons: the Atherosclerosis Risk in Communities
Study. Stroke, 33, 1487–92.
32. Wong TY, Klein R, Sharret AR et al. (2002) Cerebral white matter lesion, retinopathy and
risk of clinical stroke: The Atherosclerosis Risk in the Communities Study. JAMA, 288,
67–74.
33. Wong TY, Mosley TH, Klein R (2003). Retinal microvascular abnormalities and MRI
signs of cerebral atrophy in healthy, middle-aged people. Neurology, 61, 806–11.
34. Breslin DJ, Gifford RWJ, Fairbairn JFI (1966) Essential hypertension: a twenty year
follow-up study. Circulation, 33, 87–97.

35. Michelson EL, Morganroth J, Nichols CW, MacVaugh H (1979) Retinal arteriolar
changes as an indicator of coronary artery disease. Arch Intern Med, 139, 1139–41
36. Duncan BB, Wong TY, Tyroler HA, Davis CE, Fuchs FD (2002) Hypertensive
retinopathy and incident coronary heart disease in high risk men. Br J Ophthalmol, 86,
1002–6.
37. Wong TY, Klein R, Sharret AR et al. (2002) Retinal arteriolar narrowing and incident
coronary heart disease in men and women: The Atherosclerosis Risk in the Communities
Study. JAMA, 287, 1153–93
38. Wong TY, Rosamond W, Chang PP et al. (2005) Retinopathy and risk of congestive heart
failure. JAMA, 293, 63–9.
39. Wong TY, Coresh J, Klein R et al. (2004) Retinal microvascular abnormalities and renal
dysfunction in middle-aged people. J Am Soc Nephrol, 15, 2469–76.
40. Smith W, Wang JJ, Wong TY et al. (2004) Retinal arteriolar narrowing is associated with
5-year incident severe hypertension. The Blue Mountains Eye Study. Hypertension, 44,
442–7.
41. Wong TY, Klein R, Sharret AR et al. (2004) Retinal arteriolar diameters and risk of
hypertension. Ann Intern Med, 140, 248–55.
42. Wong TY, Shankar A, Klein R, Klein BEK, Hubbard LD (2004) Prospective cohort study
of retinal vessel diameters and risk of hypertension. BMJ, 329, 79–82.
43. Wong TY, Klein R, Sharret AR et al. (2002) Retinal arteriolar narrowing and risk of
diabetes in middle-aged persons. JAMA, 287, 2528–33.
44. Wong TY, Shankar A, Klein R, Klein BEK, Hubbard LD (2005) Retinal arteriolar
narrowing, hypertension and subsequent risk of diabetes mellitus. Arch Intern Med, 165,
1060–5.
45. Breckenridge A, Dollery CT, Parry EH (1970) Prognosis of treated hypertension.
Changes in life expectancy and causes of death between 1952 and 1967. Q J Med, 155,
411–29.
46. Breslin DJ, Gifford RWJ, Fairbairn JFI, Kearns TP (1966) Prognostic importance of
ophthalmoscopic findings in essential hypertension. JAMA, 195, 335–8.
47. Frant R, Groen J (1950) Prognosis of vascular hypertension: A nine year follow-up study
of four hundred and eighteen cases. Arch Intern Med, 85, 727.

48. Palmer RS, Loofbourow D, Doering CR (1948) Prognosis in essential hypertension:
eight-year follow-up study of 430 patients on conventional medical treatment. N Engl J
Med, 239, 990.
49. Hamada Y, Niisato E, Otori T et al. (1995) Ocular fundus changes in malignant or
precocious stroke-prone spontaneously hypertensive rats after administration of
antihypertensive drugs. Clin Exp Pharmacol Physiol Suppl, 22, S132–3
50. Morishita R, Higaki J, Nakamura F et al. (1992) Regression of hypertension-induced
vascular hypertrophy by an ACE inhibitor and calcium antagonist in the spontaneously
hypertensive rat. Blood Press Suppl, 3, 41–7.
51. Bock KD (1984) Regression of retinal vascular changes by antihypertensive therapy.
Hypertension, 6, 158–62.
52. Strachan MW, McKnight JA (2005) Improvement in hypertensive retinopathy after
treatment of hypertension. N Engl J Med, 352, e17
53. Dahlof B, Stenkula S, Hansson L (1992) Hypertensive retinal vascular changes before
and after treatment. Blood Press, 1, 35–44.

Tanda-tanda retinopati hipertensi sebagai indikator risiko morbiditas dan
mortalitas kardiovaskular
abstrak
Retinopati hipertensi telah lama dianggap sebagai indikator risiko morbiditas dan
mortalitas sistemik . Studi berbasis populasi baru menunjukkan bahwa tanda-tanda
retinopati hipertensi yang berkaitan erat dengan tekanan darah , tapi tidak konsisten
terkait dengan kolesterol dan faktor risiko lain dari aterosklerosis . Tanda-tanda
retinopati hipertensi ringan , seperti umum dan focal arteriol retina penyempitan dan
arteriovenosa nicking , yang lemah terkait dengan penyakit pembuluh darah sistemik.
Tanda-tanda retinopati hipertensi moderat, seperti microaneurysms terisolasi,
perdarahan dan cotton-wool spots, yang berkaitan erat dengan penyakit
serebrovaskular subklinis dan memprediksi langkah klinis kejadian , gagal jantung
kongestif dan kematian kardiovaskular , independen dari tekanan darah dan faktor
risiko lainnya . Data ini mendukung konsep bahwa penilaian terhadap perubahan
vaskular retina dapat memberikan informasi lebih lanjut untuk stratifikasi risiko
vaskular pada orang dengan hipertensi.
Sirkulasi retina mengalami serangkaian perubahan patofisiologi dalam
menanggapi tekanan darah. Perubahan ini diwujudkan secara klinis sebagai
spektrum tanda-tanda yang biasa disebut sebagai hipertensi retinopathy. tanda-tanda
pembuluh darah retina hipertensi dapat secara luas diklasifikasikan menjadi
perubahan arteriol ( umum penyempitan arteriolar , focal penyempitan arteriolar ,
arteriovenous nicking dan arteriol dinding kekeruhan ) dan lesi retinopathy lebih
maju ( microaneurysms , noda dan pendarahan berbentuk api , cotton-wool spots ,
eksudat keras dan disk yang optik bengkak ) . Dengan pengecualian disk bengkak ,
tanda-tanda ini dapat dideteksi cukup sering pada populasi dewasa , bahkan pada
orang tanpa riwayat diketahui hypertensi.
Pentingnya tanda-tanda retinopati hipertensi sebagai indikator risiko morbiditas
dan mortalitas sistemik telah lama dikenal sejak deskripsi mereka pada pasien
dengan penyakit ginjal dan serebrovaskular oleh Marcus Gunn pada akhir century.
Ke 19. Bahkan , penilaian tanda-tanda retinopati hipertensi untuk stratifikasi risiko
didukung oleh pedoman manajemen hipertensi internasional , termasuk Komite

Gabungan AS Nasional Pencegahan, Deteksi , Evaluasi , dan Penanganan Tekanan
Darah Tinggi ( JNC ) dan British Society of Hypertension. pedoman menekankan
bahwa retinopati hipertensi , bersama-sama dengan hipertrofi ventrikel kiri dan
gangguan ginjal , dapat dianggap sebagai indikator kerusakan organ target ,
menunjukkan bahwa dokter harus mempertimbangkan pendekatan yang lebih agresif
dalam mengelola pasien.
Klasifikasi dan diagnosis
Klasifikasi tradisional retinopati hipertensi , dating kembali ke 1939 , didasarkan
pada karya Keith et al.8 Meskipun sistem klasifikasi modern yang menyandang nama
mereka, paper8 asli tidak upaya untuk mengklasifikasikan tanda-tanda retinopati
hipertensi tetapi untuk menunjukkan bahwa keparahan hipertensi itu sendiri adalah
prediksi kematian . Klasifikasi ini dan modifikasi yang biasanya terdiri dari empat
kelas retinopati hipertensi dengan meningkatnya keparahan : kelas 1 terdiri dari '
ringan ' umum arteriol retina penyempitan ; kelas 2 terdiri dari ' lebih parah ' umum
penyempitan , area fokus penyempitan arteriolar dan arteriovenosa ( AV ) nicking ;
kelas 3 terdiri dari kelas 1 dan 2 ditambah tanda-tanda adanya pendarahan retina ,
mikroaneurisma , eksudat keras dan cotton-wool spots , kelas 4 , yang kadang-
kadang disebut sebagai dipercepat ( ganas ) retinopati hipertensi , terdiri dari tanda-
tanda di sebelumnya tiga kelas ditambah cakram optik pembengkakan dan edema
makula . Sedangkan survival 3 tahun orang dengan kelas 1 retinopati hipertensi
adalah 70 % , kelangsungan hidup hanya 6 % pada mereka dengan kelas 4
retinopathy.
Hal ini penting bagi dokter untuk menyadari bahwa beberapa dari tanda-tanda
ini, khususnya microaneurysms , perdarahan dan cotton-wool spots , juga dapat
ditemukan dalam kondisi sistemik dan okular lainnya ( Tabel 1 ) . Kehadiran eksudat
keras , misalnya , lebih khas retinopati diabetes , sedangkan tanda-tanda retina
unilateral dapat menunjukkan penyakit arteri karotid . Kehilangan penglihatan adalah
sugestif dari oklusi vena retina , retinopati diabetes , hipertensi dipercepat dan
penyakit retina lainnya . Dengan demikian , dalam skenario atipikal , penyelidikan
yang tepat mungkin diperlukan untuk mengecualikan penyakit penting ini .
Diagnosis banding perdarahan retina terisolasi , cotton-wool spots dan

mikroaneurisma
Studi berbasis populasi baru-baru ini telah memberikan data prevalensi berbagai
tanda retinopati hipertensi pada umumnya data population.10 - 17 dari studi ini
menunjukkan bahwa tanda-tanda retinopati hipertensi , yang didefinisikan dari foto-
foto retina , terlihat dalam 3-14 % dari individu dewasa berusia ≥ 40 tahun prevalensi
retinopati hipertensi : tanda-tanda dan studi populasi yang dipilih.
Ada penelitian lebih sedikit dari kejadian jangka panjang Data retinopati
hipertensi baru signs.10 dari Beaver Dam Eye Study , sebuah studi dari 4926 orang
dewasa berusia 43-86 tahun di Wisconsin , menunjukkan bahwa kejadian 5 tahun
focal penyempitan arteriolar , AV nicking , perdarahan retina dan mikroaneurisma
pada orang tanpa diabetes berkisar antara 6 % sampai 10 %.
Asosiasi dengan morbiditas dan mortalitas tekanan darah kumpulan data dari studi
klinis dan berbasis populasi menunjukkan kuat , dinilai dan konsisten asosiasi tanda-
tanda retinopati hipertensi dengan tekanan darah ( Tabel 2 ) .10-13,15-17 Baik
presence dan pengembangan retinopati hipertensi baru yang gejala sangat terkait
dengan tekanan darah tinggi . Dalam Beaver Dam Eye Study , individu hipertensi
adalah 50-70 % lebih mungkin untuk memiliki pendarahan retina dan
mikroaneurisma , 30-40 % lebih mungkin untuk memiliki focal penyempitan
arteriolar dan 70-80 % lebih mungkin untuk memiliki AV nicking daripada orang
normotensif . Selain itu, orang-orang yang hipertensi yang tekanan darah masih
tinggi meskipun penggunaan obat antihipertensi , indikasi control ' miskin ' , lebih
mungkin untuk mengembangkan retinopati daripada individu yang tekanan darah
dikendalikan dengan obat-obatan .
Asosiasi sistemik tanda-tanda retinopati hipertensi : studi berbasis populasi yang
dipilih, Beberapa studi berbasis populasi baru-baru ini telah menggunakan metode
fotografi retina standar untuk menentukan tanda-tanda retinopati hipertensi dan
metode pencitraan berbasis komputer untuk mengukur diameter arteriol retina dari
foto . Salah satunya adalah Atherosclerosis Risk in Communities ( ARIC ) studi ,
yang berdasarkan populasi kohort investigasi penyakit kardiovaskular dari orang
yang berusia 45-64 tahun yang dipilih dari empat komunitas AS . Fotografi retinal
ditambahkan sebagai komponen pemeriksaan dan dinilai untuk kehadiran dan tingkat

keparahan hipertensi perubahan mikrovaskuler retina . Penelitian ARIC
menunjukkan bahwa umum retina penyempitan arteriolar , ditunjukkan dengan
diameter arteriol sempit ditentukan dari foto-foto , sangat terkait dengan tekanan
darah tinggi , sebuah temuan sekarang dikonfirmasi dalam lima populasi lain dengan
menggunakan sejenis methods.18 - 22 Namun , penerapan klinis dari temuan ini
tidak jelas , seperti tingkat halus penyempitan arteriolar berhubungan dengan tekanan
darah tinggi adalah sulit untuk memperkirakan dari oftalmoskopi . Sebagai contoh,
setiap peningkatan 10 mmHg tekanan darah arteri rata-rata dikaitkan dengan
penurunan hanya 6 m ( 3 % ) pengurangan diameter arteriol retina dalam satu study.
Data dari ARIC dan studi lain memberikan peningkatan bukti bahwa pola asosiasi
tekanan darah dengan tanda-tanda retinopati hipertensi tertentu bervariasi .
Generalized arteriol retina penyempitan dan AV nicking tampaknya penanda
kerusakan jangka panjang hipertensi kumulatif , dan secara independen terkait
dengan tingkat tekanan darah lalu diukur 5-8 tahun sebelum assessment.20 retina , 21
,Sebaliknya , fokus penyempitan arteriolar , pendarahan retina , dan mikroaneurisma
cotton-wool spots mencerminkan perubahan yang lebih transien peningkatan tekanan
darah akut , dan dihubungkan hanya dengan tekanan darah bersamaan diukur pada
saat assessment. retina
Temuan penting dalam Beaver Dam Eye Study adalah pengamatan bahwa
hubungan antara tekanan darah dan tanda-tanda mikrovaskuler retina tampaknya
lemah dengan usia , 22 mungkin mencerminkan sclerosis lebih besar dari arteriol
retina pada orang tua .
Faktor risiko Aterosklerosis
Berbeda dengan hubungan yang kuat dengan tekanan darah , tanda-tanda
retinopati hipertensi belum konsisten terkait dengan baik langkah-langkah langsung
aterosklerosis , seperti stenosis arteri karotis , atau faktor risiko aterosklerosis ,
seperti hiperlipidemia ( Tabel 2 ) . Dalam studi ARIC , sekaligus mengontrol tekanan
darah , penyempitan arteriolar umum dikaitkan dengan plak arteri karotid tetapi tidak
stenosis , AV nicking dikaitkan dengan stenois arteri karotis tapi tidak plak dan fokus
penyempitan arteriolar tidak terkait dengan baik measure.12 arteri karotid

Dalam Studi Hoorn di Belanda hiperglikemia dan obesitas perut secara
independen terkait dengan kejadian pendarahan retina , mikroaneurisma , eksudat
keras dan cotton-wool spots di population. umum non - diabetes Dalam studi ARIC ,
tanda-tanda retinopati hipertensi terkait dengan lebih besar lingkar pinggang ,
indikator obesitas. Namun, tidak semua studi telah menemukan hubungan antara
tanda-tanda retinopati hipertensi dan obesitas abdominal atau dyslipidaemia.
Hubungan tanda-tanda retinopati hipertensi dengan faktor risiko aterosklerosis
baru juga telah diteliti . Asosiasi cross- sectional dari retina penyempitan arteriolar
dan AV nicking dengan biomarker peradangan ( misalnya jumlah sel darah putih )
dan disfungsi endotel ( misalnya faktor von Willebrand ) telah dilaporkan dalam
study12 ARIC dan oleh groups.
Studi ini menekankan fakta bahwa tanda-tanda khas dari retinopati hipertensi
mungkin berhubungan dengan proses vaskular selain tekanan darah .
Stroke dan penyakit serebrovaskular
Sejumlah penelitian telah melaporkan hubungan yang kuat antara berbagai tanda-
tanda retinopati hipertensi dan kedua subklinis dan klinis serebrovaskular disease26 -
28 dan stroke mortality.29 Dalam studi ARIC , individu dengan pendarahan retina ,
dan mikroaneurisma cotton-wool spots , sebagaimana didefinisikan dari foto , dua
sampai empat kali lebih mungkin untuk mengembangkan stroke klinis insiden dalam
waktu 3 tahun , bahkan ketika mengendalikan untuk efek dari tekanan darah ,
merokok , lipid dan factors.30 risiko lain antara peserta tanpa stroke atau transient
ischemic attack , tanda-tanda retinopati hipertensi juga terkait dengan perubahan
fungsi kognitif , seperti yang didefinisikan oleh tes neuropsikologi standar selama 6
tahun , 31 dan cerebral hyperintensity materi putih lesi 32 dan atrofi , sebagaimana
didefinisikan dari MRI scans.
Salah satu pengamatan penting adalah bahwa kehadiran retinopati hipertensi
mungkin menawarkan nilai prediksi tambahan risiko stroke klinis pada individu
dengan MRI - didefinisikan penyakit otak subklinis . Dalam studi ARIC , individu
dengan baik lesi materi putih MRI - didefinisikan dan retinopati hipertensi adalah 18
kali lebih mungkin [ risiko relatif ( RR ) 18,1 ; selang kepercayaan 95% ( CI ), untuk

kejadian stroke yang klinis insiden dibandingkan tanpa baik lesi materi putih atau
retinopathy.hipertensi. Penyakit jantung koroner dan gagal jantung.
Tanda-tanda retinopati hipertensi telah dikaitkan dengan kedua penyakit jantung
koroner subklinis dan klinis dan gagal jantung kongestif . Sebagai contoh, berbagai
tanda-tanda retinopati hipertensi telah dikaitkan dengan perubahan iskemik pada
elektrokardiogram , 34 keparahan stenosis arteri koroner pada angiography35 dan
insiden penyakit jantung koroner dan infark miokard pada men36 dan women.
Penelitian ARIC melaporkan bahwa , setelah mengendalikan faktor risiko yang
sudah ada sebelumnya , individu dengan pendarahan retina , dan mikroaneurisma
cotton-wool spots dua kali lebih mungkin ( RR 1,96 , 95 % CI 1,52-2,56 ) untuk
mengembangkan gagal jantung kongestif sebagai individu tanpa retinopati .38
Bahkan, di antara individu yang berisiko rendah ( tanpa penyakit jantung yang sudah
ada sebelumnya , diabetes atau hipertensi ) , kehadiran tanda-tanda retinopati
hipertensi memprediksi risiko 3 kali lipat peningkatan kejadian gagal jantung ( RR
2,97 , 95 % CI 1,49-5,91 ) . Ini kompatibel dengan interpretasi bahwa kerusakan
mikrovaskuler ke miokardium dari hipertensi dan proses sistemik lainnya dapat
menjadi faktor yang berkontribusi dalam pengembangan gagal jantung .
Penyakit sistemik lainnya
Sejumlah penyakit sistemik telah dikaitkan dengan tanda-tanda hipertensi
retinopati yang berbeda. Dalam studi ARIC , individu dengan nicking AV ,
pendarahan retina , dan mikroaneurisma cotton-wool spots lebih mungkin untuk
mengembangkan disfungsi ginjal daripada mereka yang tidak ada gejala. Asosiasi ini
adalah independen dari tekanan darah , diabetes dan faktor risiko lain , dan juga
terlihat pada orang tanpa diabetes atau hipertensi .
Data dari tiga studi berbasis populasi menunjukkan bahwa umum penyempitan
arteriol retina , penanda kerusakan tekanan darah , mungkin sebenarnya memprediksi
perkembangan insiden studi hypertension. The ARIC menunjukkan bahwa peserta
normotensif yang umum penyempitan arteriolar adalah 60 % lebih mungkin
didiagnosis dengan hipertensi dalam jangka waktu 3 tahun berikutnya dibandingkan
orang normotensif tanpa penyempitan arteriolar ( RR 1,62 , 95 % CI 1,21-2,18 )
asosiasi ini adalah independen dari yang sudah ada tingkat tekanan darah

individu ,indeks massa tubuh dan faktor lain yang diketahui hipertensi risiko .
The ARIC dan Beaver Dam Eye Studi juga menunjukkan bahwa umum arteriol
retina penyempitan memprediksi kejadian diabetes tipe 2 di antara orang-orang yang
pada awalnya bebas dari diabetes , independen factors. risiko diabetes , Dengan
demikian umumnya penyempitan arteriolar , mungkin mencerminkan berbagai
arteriol perifer sistemik perubahan , dapat menjadi penanda praklinis hipertensi
terbuka dan diabetes mortalitas kardiovaskular.
Penelitian oleh Keith et al.8 adalah di antara yang pertama untuk menunjukkan
peningkatan mortalitas dengan keparahan perubahan retinopati hipertensi . Sejak itu,
sejumlah studi yang dilakukan pada 1950-an dan 1960-an telah lebih lanjut
menunjukkan bahwa orang dengan hipertensi dan retinopathy tanda-tanda berada
pada peningkatan risiko mortality.34 ,45 - 47 Namun , kesimpulan dari banyak studi
yang lebih tua terbatas karena evaluasi subjektif dari retinopati hipertensi tanda-tanda
, kurangnya data pada tingkat penyebab kematian - spesifik dan kontrol yang tidak
memadai untuk pembaur potensial seperti tekanan darah dan diabetes .
Meskipun demikian , penelitian yang lebih baru telah memberikan bukti kuat
bahwa tanda-tanda hipertensi merupakan penanda risiko kematian . Dalam analisis
kasus-kontrol berumber dari Beaver Dam Eye Study , individu dengan
microaneurysms retina dan pendarahan retina dua kali lebih mungkin untuk
meninggal akibat kejadian kardiovaskular seperti yang tanpa gejala.
Data dari studi terbaru mendukung pedoman hipertensi saat ini tentang
pentingnya prognostik retinopati signs. Informasi yang diperoleh dari penilaian status
retinopathy tampaknya independen , dan secara kualitatif berbeda , yang mengukur
tekanan darah atau serum lipid , sebagai tanda-tanda retinopati menunjukkan
kerentanan dan timbulnya penyakit vaskular sistemik praklinis . Secara khusus,
tampaknya bahwa individu dengan tanda-tanda retinopati hipertensi tertentu
( misalnya pendarahan retina , dan mikroaneurisma cotton-wool spots ) harus
dipantau lebih dekat untuk risiko kardiovaskular , dan dapat mengambil manfaat dari
penyelidikan lebih lanjut ( misalnya echocardiogram untuk fungsi jantung ) jika
terindikasi secara klinis .

Sebuah sistem klasifikasi tiga kelas untuk retinopati hipertensi ditunjukkan pada
Tabel 3 , dan pendekatan yang disarankan untuk pasien dengan berbagai kelas
retinopati hipertensi ditunjukkan pada Gambar 2 . Adalah penting untuk menekankan
bahwa manajemen untuk pasien dengan hipertensi dan penyakit kardiovaskular harus
terus mengikuti pendekatan standar prediksi risiko ( yaitu berdasarkan penilaian dari
usia dan jenis kelamin pasien , tekanan darah dan kadar lipid , rokok status merokok
dll ) .
Evaluasi dan pengelolaan pasien dengan retinopati hipertensi.
Klasifikasi pada Tabel 3 kelompok hipertensif tanda-tanda retinopati menjadi
ringan, sedang dan dipercepat ( ganas ) . Pasien dengan tanda-tanda retinopati
hipertensi ringan ( Gambar 3A ) mungkin akan memerlukan perawatan rutin , dan
kontrol tekanan darah harus didasarkan pada didirikan guidelines. Pasien dengan
tanda-tanda retinopati hipertensi sedang ( perdarahan retina , microaneurysm ,
cotton-wool spots ) ( Gambar . 3B ) dapat mengambil manfaat dari penilaian lebih
lanjut dari risiko vaskular ( misalnya penilaian kadar kolesterol ) dan , jika terindikasi
secara klinis , terapi pengurangan risiko yang sesuai (misalnya agen penurun
kolesterol ) . Pasien dengan retinopati hipertensi dipercepat ( bilateral disk yang
bengkak di hadapan hipertensi retinopati moderat ) ( Gambar 3C ) , yang relatif
jarang terjadi di populasi umum tetapi dapat terjadi dalam hubungannya dengan
hipertensi berat , akan terus membutuhkan manajemen antihipertensi segera
mendesak , termasuk kemungkinan pemberian obat intravena. Dalam skenario seperti
ini , dokter harus bertujuan untuk kontrol bertahap kecil tekanan darah selama
beberapa jam , dan menghindari penurunan mendadak tekanan darah yang dapat
menyebabkan stroke.
Ada beberapa studies eksperimental dan laporan klinis regresi tanda-tanda
retinopati hipertensi dengan kontrol tekanan darah . Dengan pengobatan hipertensi
yang memadai , resolusi tanda-tanda retinopati hipertensi dapat terjadi selama
periode 6 bulan hingga tahun yang demikian tindak lanjut dari pasien sampai satu
tahun setelah diagnosis mungkin diperlukan.
Studi ini juga menyediakan beberapa bukti yang secara khusus menargetkan
mikrosirkulasi pada individu hipertensi dapat mengurangi morbiditas kardiovaskular

dan mortality. contoh , agen antihipertensi tertentu (misalnya inhibitor ACE ) telah
disarankan untuk memiliki efek menguntungkan langsung pada struktur microvessel
dan fungsi , di luar utama mereka efek pada menurunkan tekanan darah. Oleh karena
agen tersebut mungkin telah menambahkan nilai terapeutik dalam mencegah dan
mengobati penyakit jantung . Namun, apakah ini terapi khusus dapat membalikkan
atau mengurangi perubahan retinopati , dan apakah ini akan mengakibatkan risiko
kardiovaskular berkurang , saat ini tidak jelas.
kesimpulan
Tanda-tanda retinopati hipertensi mungkin berbeda dalam asosiasi mereka dengan
penyakit sistemik . Pendarahan retina terisolasi , dan mikroaneurisma cotton-wool
spots ( retinopati hipertensi moderat ) tampaknya terkait dengan risiko subklinis dan
klinis stroke, hasil serebrovaskular lainnya , gagal jantung kongestif dan kematian
kardiovaskular , independen dari faktor risiko tradisional . Sebaliknya , asosiasi
sistemik untuk umum penyempitan arteriol retina , focal penyempitan arteriolar dan
AV nicking ( retinopati hipertensi ringan) tampaknya lebih rendah konsisten.
Penilaian terhadap tanda-tanda retinopati hipertensi dapat memberikan informasi
penting untuk stratifikasi risiko vaskular.