
Hypertension in Women Living in Africa JESSICA TAYLOR CHUKWUDI OKEKE KIM DOBSON.
17
Hypertension in Women Living in Africa JESSICA TAYLOR CHUKWUDI OKEKE KIM DOBSON
-
Upload
terence-roberts -
Category
Documents
-
view
216 -
download
0
Transcript of Hypertension in Women Living in Africa JESSICA TAYLOR CHUKWUDI OKEKE KIM DOBSON.

Hypertension in Women Living in AfricaJESSICA TAYLOR
CHUKWUDI OKEKE
KIM DOBSON
The World Health Organization (WHO)
The WHO is a non-profit organization est. April 7, 1948Headquartered in Geneva, Switzerland
Private and Public Partnerships to Improve Health InternationallyIt is a Specialized Agency of the United Nations
Made up of over 7,000 people from more than 150 countries150 WHO offices are located around the world
THE WHO: Governed by the World Health Assembly (WHA) Staffed by: Doctors, public health specialists,
scientists, epidemiologists, administrative, financial, information systems, experts in health
statistics, economics & emergency relief The WHA approves major policies, work
programs, & budgets. Elects the Director-General
THE WHA Consists of:
194 Member States The Executive BoardThe Director-General
The Constitution: Signed by 61 countries
(WHO, 2015)
The WHO’s Global Health Focus
The WHO has published several reports with action plans regarding non-communicable diseases (NCD’s), Cardiovascular disease (CVD), and Hypertension:• The Global brief on Hypertension (2013): This report describes how HTN
contributes to CVD, Stroke, & Kidney Failure, as well as Premature Death & Disability. It explains how governments, health care workers, civil society, the private sector, families and individuals can prevent and reduce HTN.
• “Global Action Plan for the Prevention & Control of NCD’s 2013-2020” – There are 9 global targets. #6 calls for 25% reduction in hypertension.
• “Global Status Report on NCD’s 2014” countries will set national targets & measure progress on the 2010 baseline.
• The UN General Assembly will convene in 2018 on NCD’s to assess global targets progress towards the 2025 goals.

WHO Facts on Hypertension
Untreated HTN Results in CVD’s
CVD #1 cause of death globally
An est. 17.5 million died from CVD’s in 2012
Most CVD is preventable
Early Detection is vital to survival rates
Over ¾ of CVD deaths occur in low & middle income
countries
What are CVD’s
Coronary Heart Disease
Cerebrovascular Disease
Peripheral Arterial Disease
Rheumatic Heart Disease
Congenital Heart Disease
Deep Vein Thrombosis
Pulmonary Embolism

Vulnerable Population
▪ Hypertension (HTN) has been a consistent outcome among cultures and regions that have low income, minimal healthcare access, and low education
▪ Africa has had the highest high blood pressure rating when compared to the Americas at 32% versus the African region combined at 46% suffering form hypertension. Prevalence rates in Africa run over 40%. (WHO, 2015)
▪ HTN has caused 46,888 deaths and 390, 860 disabilities in South Africa, Women have had the high occurrence at 60% in the year 2,000 and has only grown with resistance from African cultures (Peltzer &Phaswana 2013)
▪ Various factors have been found to be associated with hypertension, including socio-demographics (older age, female gender, lower education level, lower household income. (Peltzer &Phaswana 2013)
▪ The prevalence rate in South African study of 2008 concluded that 79% were hypertensive women that suffered from low fruits and vegetables, low income, over weight, tobacco use, and were middle aged of 30-50 years old
▪ Niger Africa has the highest female HTN population at 35%, 31% males and mixed 34.5% Norman, 2007)

African Females aged 35-40 years have a higher prevalence than males for HYPERTENSION
Determinant Factors
▪ Genetics
▪ Personal Characteristics
▪ Autonomic Nervous System functions (higher plasma sodium & lower potassium, calcium, magnesium concentrations)
▪ Cardiac Function
▪ Environmental Factors
▪ Cultural bias towards premium on obesity in women
There were higher levels of prevalence in women than men such countries as in Algeria 31.6 percent vs. 25.7 percent in 2003, Botswana 37.0 percent vs. 28.8 percent in 2006 and Mali 25.8 percent vs. 16.6 percent in 2007, for women and men, respectively.
Factors Contributing to Hypertension (HTN)
▪ High salt intakes: salt used to preserve foods like fish & make food tastier. Processed food are rare.
▪ Obesity
▪ Aging population is increasing
▪ Smoking among younger women
▪ Lifestyle: insufficient physical activity
▪ Socioeconomic status
▪ Smoking and Hypertension lead to Coronary Heart Disease and Ischemia heart Disease
▪ Congestive Heart Failure
▪ Cardiomyopathy
▪ Renal Disease: End Stage Renal Disease common cause HTN
▪ Strokes
▪ Uncontrolled Diabetes
In Africa, increased salt intake and the aging population are among the main causes of hypertension. Africa has the highest prevalence of HTN in the world 38.1 % of men and 35.5 % women are affected. The number of people affected with HTN in the region is projected to reach 150million by 2025 ( WHO, 2014).
The History of Hypertension
Salt being the primary cause of hypertension. Iodization in the country was introduced in 1954 in an effort to supply iodine. It failed to eliminate endemic
goiter and iodine deficiency. Voluntary salt recommendations in South Africa failed then they attempted to eliminate the iodine deficiency by
introducing mandatory iodization of table salt at 40–60 ppm in 1995
Hypertension, once rare in rural parts of West Africa, has now emerged as a critical health concern and the
trajectory is upward and factors are complex. For example, recent findings from Ghana report a high prevalence of hypertension among rural agrarian
farmers that may not be easily attributed to western diet given their reliance on traditional home-cooked meals. It was suggested that differential exposure to stress may trigger a chain of neuroendocrine events
cumulating in a high prevalence of hypertension (Iwelunmor, et al, 2014)
Endemic goiter was reported for the first time in South Africa in the Langkloof area of
the Eastern Province in 1927. 32 Subsequent investigations found
widespread endemic goiter during the following years, culminating in the
appointment of the South African Goiter Research Committee under the auspices of
the Medical Faculty of the University of Pretoria in 1948. On recommendation of
this committee, optional iodization of salt with potassium iodate was legally
introduced in South Africa at a level of 10–20 ppm of iodine in 1954. For the following
four decades virtually no new goiter or iodine information was produced in the
country and the Goiter Research Committee was disbanded (Jooste & Zimmermann,
2008, p.11)
History: Salt the Cure for Iodine Deficiency
Median urinary iodine concentrations is the measure used to determine suffiency (median urinary iodine 100–199 µg/L)
Closer collaboration between the South African Iodine Deficiency Disorders Network and the salt industry resulted in improved accuracy of salt iodization.
Knowledge of iodine nutrition amongst adults is low, particularly in low socioeconomic households, leading to the vulnerability of these groups to obtain
non-iodized salt for cooking via unconventional sources.
Iodine Deficiency Lead to Increased Salt Intake
Iodine is an essential substrate for the synthesis of the two thyroid hormones,
thyroxine (T4) and triiodothyronine (T3). Deficiency leads to the impairment of thyroid
hormone synthesis, resulting in hypothyroidism, functional and
developmental abnormalities called iodine deficiency disorders (IDDs). These IDDs include thyroid function abnormalities,
endemic goiter, mental retardation, cretinism, reproductive failure, and perinatal
and infant mortality. The most damaging disorder resulting from iodine deficiency
(Jooste & Zimmermann, 2008)
Awareness Campaigns in Africa
▪ Across Africa , WHO is partnering with local agencies to promote awareness of hypertension.In South Africa, they have initiated a
population-based community education on harmful effects of alcohol
Introduced taxes on alcoholic drinks
▪ In Nigeria, the organization’s efforts:free hypertension screening programs educating the public on hypertension
through advertisements on newspapers

Across Africa, WHO’s campaign Entails:
Banning smoking in public places in 28 countries
Banning and restricting of tobacco advertisement
Introduction of tobacco taxes
Implementation of national guidelines on physical activity by Rwanda, Togo, Lesotho and other countries in the region
Banning of sugary drinks and unhealthy snacks in school cafes’ at Mauritius
Plans to reduced salt contents in bread and processed foods in Mauritius
Campaigns Continued
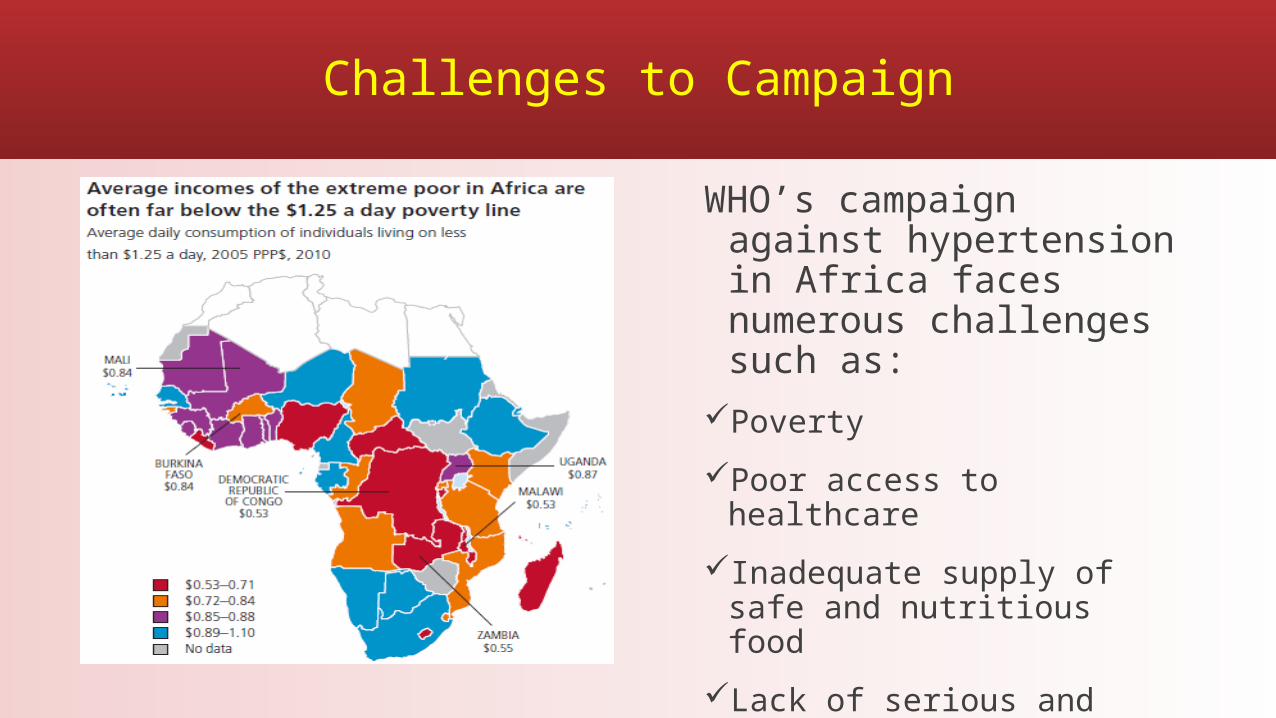
Challenges to Campaign
WHO’s campaign against hypertension in Africa faces numerous challenges such as:
Poverty
Poor access to healthcare
Inadequate supply of safe and nutritious food
Lack of serious and sustained governmental cooperation
Impact on Health Care Delivery
▪ The Effect Treating Hypertension has on Nursing in Africa
The nursing shortage is in crisis especially, doctoral prepared nurses who would carry out much needed clinical research. Columbia university School of Nursing concluded areas of study were associated by funding sources (Sun & Larson, 2014)
Non-Communicable Diseases (NCD’s) overwhelm an already limited health care system and staff shortages.
More than 500,000 Women between the ages of 19 – 49 have died in developing countries each year due to hypertensive-related causes
(Oyedi-Kofi, 2011)

How Nurses in Africa are Combating Hypertension in Women
▪ Nurses in Africa are using teaching and education as essential tools to combat hypertension and cardiovascular disease. ▪ Educate the public on the effects and prevention of hypertension ▪ Educating women/men on healthy diet and nutrition to reduce BMI▪ Educating on medications used to treat hypertension & adherence. The most frequently used are diuretics and ace inhibitors ▪ Monitoring through screenings and encourage daily weights ▪ Encouraging patient to increase daily physical activity▪ Smoking cessation for patients ▪ Educate patients on the limits of alcohol ▪ Educate on stress relief ▪ Empowering women to take control over their health ▪ Using technology to educate and communicate with patients (reminders to take medications to cell phones) in some parts of the country
▪ Limiting Factors: ▪ Poor data availability to evaluate or measure practices because of resource poor countries. ▪ Guidelines are not being followed in some health settings. Failure to follow guidelines has increased the cost of health care by 19%. ▪ Gender Inequality reduces access to health care. ▪ Rural areas: limited access and long distances to travel therefore, the use of herbal medications and traditional medicine is common ▪ Limited continuing education for nurses due to lack of resources. Education contributes to knowledge, skills and attitudes towards prevention,
treatment, and management it could lead to a reduction in visits (Gaziano, Bertram, Tollman, & Hofman, 2014). One gender related barrier related which is harmful to Women: Women cannot receive needed health care because of cultural community norms prevent women from travelling alone to a clinic to seek treatment. (WHO, n.d.)
ODU Honor Code
Honor Code“I pledge to support the honor system of Old Dominion University. I will refrain from any form of academic dishonesty or deception, such as cheating or plagiarism. I am aware that as a member of the academic community, it is my responsibility to turn in all suspected violators of the honor system. I will report to Honor Council hearings if summoned.”
Signed by :Jessica Taylor,
Chukwudi Okeke Kim Dobson

References
Gaziano, T., Bertram, M., Tollman, S. and Hofman, K. (2014). Hypertension education and adherence in South Africa: A cost effectiveness analysis of community health workers. BMC Public Health, 14(240).
Jooste, P., & Zimmermann, M. (2008). Progress towards eliminating iodine deficiency in South Africa. South African Journal Of Clinical Nutrition, 21(1), 8-14.
Iwelunmor, J., Airhihenbuwa, C. O., Cooper, R., Tayo, B., Plange-Rhule, J., Adanu, R., & Ogedegbe, G. (2014). Prevalence, determinants and systems-thinking approaches to optimal hypertension control in West Africa. Globalization & Health, 10(1), 1-15. doi:10.1186/1744-8603-10-42
Norman, R. (2007, August 1). Estimating the burden of disease attributable to high blood pressure in South Africa in 2000.(Original Articles)(Survey). South African Medical Journal, 32-40.
Oyedi-Kofi, J. (2011). Prevention and management of hypertension: A study on knowledge and attitudes of women of childbearing age (Thesis) . Central Ostrobothnia: University of applied sciences, Ghana.
Peltzer, K., & Phaswana-Mafuya, N. (2013). Hypertension and associated factors in older adults in South Africa. Cardiovascular Journal of Africa, 24(3), 66–72. doi:10.5830/CVJA-2013-002.
Seedat, Y. (2013). Ethnicity, hypertension, coronary heart disease and renal diseases in South Africa. Ethnicity and Health, 1(4), 349-357.
Van de Vijver, S., Akinyi, H., Otis, S., Olajide, A., Agyemang, C., Aboderin, I., and Kyobutungi, C. (2013). Status report on hypertension in Africa - Consultative review for the 6th session of the African union conference of ministers of health on NCD’s. The Pan African Medical Journal, 16(38). Retrieved from: http://www.panafrican-med- journal.com/content/article/16/38/full/
World Health Organization (WHO). (2015). Global statistics. Retrieved from: http://www.who.int/gho/countries/dza/country_profiles/en/
World Health Organization (WHO). (n.d.). Gender, women, and health. Retrieved from: www.who.int/gender/genderandhealth/en/


















