
Hypertension in Pregnancy - UNT Health Science Centerce.unthsc.edu/assets/71/11 - Bleich.pdf · •...
46
Hypertension in Pregnancy April Bleich, MD, FACOG 26 th Annual Pelham P. Staples, Jr, MD Symposium October 17, 2014
Transcript of Hypertension in Pregnancy - UNT Health Science Centerce.unthsc.edu/assets/71/11 - Bleich.pdf · •...
HypertensioninPregnancy
April Bleich, MD, FACOG26th Annual Pelham P. Staples, Jr, MD Symposium
October 17, 2014
Objectives• Define types of hypertension in pregnancy
• Chronic hypertension• Gestational hypertension• Preeclampsia• Super imposed preeclampsia
• Review diagnosis of each of the above conditions• Discuss recommended management for hypertension in pregnancy including timing of delivery
HypertensiveDisorders• Complicate 5‐10% of all pregnancies• Preeclampsia occurs in 4% of pregnancies• World Health Organization, 2006
• 16% of maternal deaths in developed countries attributed to hypertensive disorders
• Over of half of these deaths are deemed preventable
History• Eclampsia was described as early as 2200 BC• Many translations of Hippocrates refer to what is believed to be eclampsia • “in pregnancy, the onset of drowsy headaches with heaviness is bad; such cases are perhaps liable to some sort of fits at the same time”
• Described in 1694 edition of a textbook by Mauriceau• “the mortal danger to mother and fetus is greatest when mother does not recover consciousness between convulsions”
• “Primigravidas are at far greater risk of convulsions than are multiparas”
Chelsey’s Hypertensive Disorders in Pregnancy, 3rd Edition, 2009.
History• Early treatments
• Phlebotomy• Purging
• Eclampsia was not differentiated from epilepsy until 1739 and the theory was not widely accepted for another 100 years
Chelsey’s Hypertensive Disorders in Pregnancy, 3rd Edition, 2009.
Definitions• Chronic hypertension• Gestational hypertension
• Preeclampsia• Preeclampsia with severe features
• Chronic hypertension with superimposed preeclampsia

Mild preeclampsia
ChronicHypertension• Diagnosis of HTN that predates pregnancy OR is detected prior to 20 weeks gestation
• Gestational HTN that does not normalize by 12 weeks postpartum
GestationalHypertension• New onset HTN after 20 weeks gestation in the absence of proteinuria

Preeclampsia• Elevated BP
• >140 mm Hg systolic or >90 mm Hg diastolic• Proteinuria
• >300 mg protein in 24‐hour urine• Protein/creatinine ratio > 0.3 mg/dL• If other testing modalities unavailable, may use 1+ on urine dip
• Massive proteinuria (>5 grams) has been eliminated from diagnostic criteria for severe preeclampsia
Preeclampsia• In the absence of proteinuria, new onset HTN with new onset of any of the following
• Platelet count <100,000/microliter• Creatinine >1.1 mg/dL or doubling of creatinine in absence of other renal disease
• Transaminases >2 x upper limit of normal• Pulmonary edema• Cerebral or visual symptoms
Preeclampsia• Severe features of preeclampsia
• Systolic BP >160 mm Hg or diastolic BP >110 mmHg• Platelet count <100,000/microliter• Impaired liver function
• AST/ALT at twice normal levels• Severe persistent RUQ or epigastric pain unresponsive to meds
• Renal insufficiency (creatinine > 1.1 mg/dL or doubling of creatinine)
• Pulmonary edema• New‐onset cerebral or visual disturbances
CHTNwithsuperimposedpreeclampsia
• New onset proteinuria and:• Worsening of HTN• Increased transaminases• Thrombocytopenia• Elevated creatinine• RUQ pain/HA• Pulmonary edema
• OR an increase in proteinuria with any of the above
Eclampsia• New onset grand mal seizures in a woman with preeclampsia
• Need to consider other causes
• Fetal growth restriction is no longer considered an indication of severe disease
• Degree of proteinuria is no longer indicative of severe disease
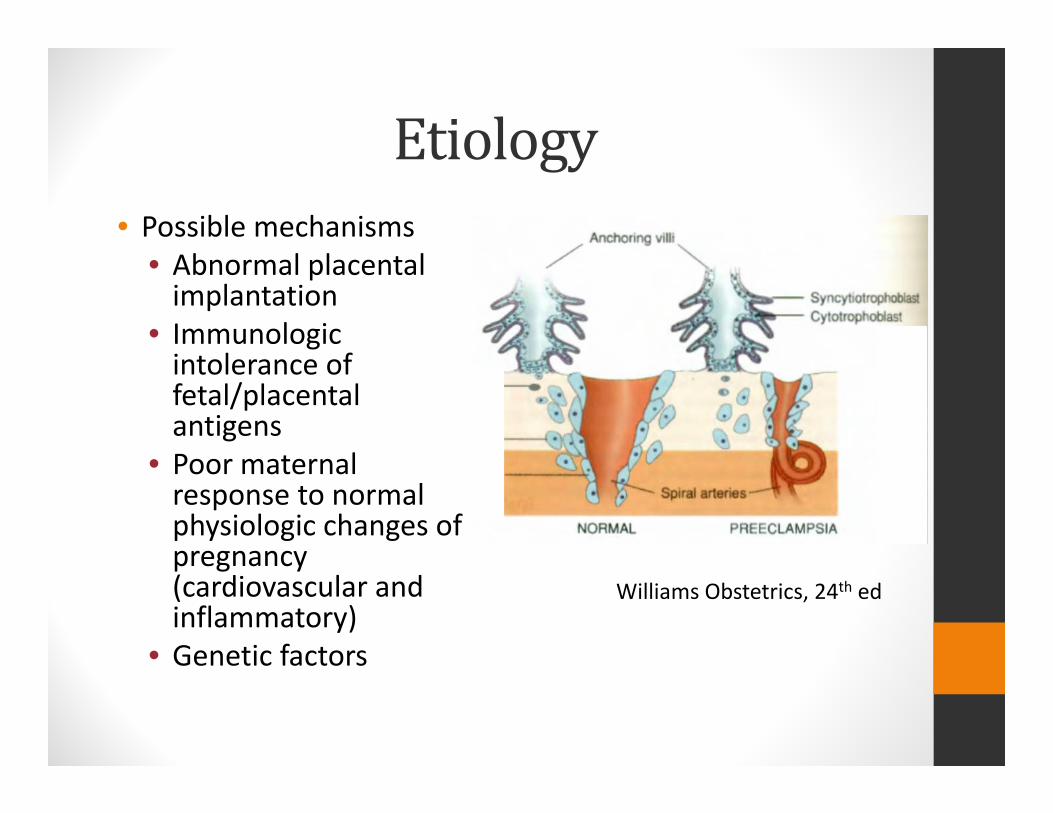
Etiology• Possible mechanisms
• Abnormal placental implantation
• Immunologic intolerance of fetal/placental antigens
• Poor maternal response to normal physiologic changes of pregnancy (cardiovascular and inflammatory)
• Genetic factors
Williams Obstetrics, 24th ed

Management
CHTNManagement• Baseline 24 hr urine protein• Initiation of medications if indicated• Serial growth ultrasounds• Weekly antenatal testing if on medications• Timing of delivery
• Per consensus statement, if uncomplicated, not before 38 weeks
ChronicHypertension• When to initiate treatment?
• Systolic >160 mmHg or diastolic >105 mmHg (I say if persistently in upper 150s or 100s)
• Reason for treatment of BP is for maternal benefit, not fetal
• BP goal on meds is >120/80• What medication should I use?
• Labetalol• Nifedipine• Methyldopa • Avoid ACE inhibitors or ARBs
Methyldopa(Aldomet)• Centrally acting alpha‐2 adrenergic agonist
• Pregnancy category B• Side effects: hemolytic anemia (rare), dry mouth, sedation, dizziness, hepatic dysfunction
• Less effective for severe HTN than beta blocker or CCB in Cochrane review
Labetalol• Nonselective β‐blocker with vascular α‐receptor blocking ability
• Side effects: lethargy, fatigue, sleep disturbances, bronchoconstriction
• Avoid if asthma, CHF, or heart disease• May be associated with SGA infants when compared to placebo or no treatment (RR 1.3)
Procardia• Calcium channel blocker• Not as well studied in pregnancy but no known adverse outcomes
• Does not appear to adversely affect uterine or umbilical blood flow
• Avoid sublingual form
AntihypertensiveTherapy• Used to prevent severe HTN and hemorrhagic stroke
• Treatment may decrease risk of progressing to severe HTN but may also impair fetal growth
• Therapy vs placebo• ↓ severe HTN (RR 0.5)• No effect on risk of progressing to preeclampsia, eclampsia, pulmonary edema, PTB, SGA or NND
• Beta blockers associated with increased risk SGA (RR1.36)
MedsforUrgentBPControl• Labetalol
• First line agent• 10‐20 mg IV, then 20‐80 mg q20‐30 min to max of 300 mg
• Hydralazine• Higher doses can be associated with hypotension, HA, and fetal distress
• 5 mg IV or IM, then 5‐10 mg IV q20‐40 min• Nifedipine
• Side effects‐tachycardia, HA• 10‐20 mg orally, repeat in 30 min if needed, then 10‐20 mg q2‐6 hours
Management• Gestational HTN and Preeclampsia without severe features
• Outpatient • Twice weekly BP checks• Consideration of weekly CBC/CMP• If GHTN, weekly urine protein• Antenatal surveillance• Corticosteroids for fetal lung maturity if <34 weeks
• Antihypertensives should NOT be started if systolic is <160 mmHg or <110 mmHg
• Strict bedrest should not be prescribed ***• Expectant management until 37 0/7 weeks gestation
Antenatalsurveillance
• Daily kick counts• NST/BPP
• GHTN‐weekly• Preeclampsia without severe features‐twice weekly• Preeclampsia with severe features‐should be admitted
• Weekly fluid check• Growth q3 weeks• Uterine artery dopplers if FGR present
Management‐Severe• Preeclampsia with severe features
• Expectant management until 34 weeks• This should only be done in center with adequate maternal and NICU resources
• If pre‐viable, expectant management is not recommended
• Corticosteroids for fetal lung maturity• Antihypertensive therapy if BP sustained >160 mmHg and/or >110 mmHg
• Decisions regarding delivery should NOT be made based on degree of proteinuria
• Deliver at 34 0/7 weeks
Management‐Severe• Vitals, intake/output q8 hours• Monitor for symptoms q8 hours• CBC, AST/ALT, Creatinine daily (can be spaced out if remain stable)
• Antenatal surveillance• NST/kick count daily• BPP twice weekly• Growth ultrasound q2 weeks with UA dopplers if growth restriction
Steroidsandseveredisease• Should always be given, but when should delivery be delayed????
Steroidsandseveredisease• Delivery should NOT be delayed if:• Uncontrollable severe HTN
• Eclampsia• Pulmonary edema• Abruption• DIC• Nonreassuring fetal status
• IUFD• Nonviable fetus
Steroidsandseveredisease• ***It is suggested, that delivery should be deferred for 48 hours if maternal and fetal conditions remain stable, if***:• Preterm premature ROM• Labor• Platelets <100,000/microliter• HELLP• Abnormal transaminases (>2 x upper limit normal)• Fetal growth restriction (<5%ile)• Severe oligohydramnios (AFI <5 cm)• Reversed end diastolic flow on UA dopplers• New‐onset renal dysfunction or increasing renal dysfunction• Persistent symptoms
• “Delivery should also be considered for women whose health is declining...”
WhentoDeliver• Gestational HTN and preeclampsia without severe features
• >37 weeks• Worsening maternal or fetal condition• Suspected abruption
• >34 weeks with any of the following• Labor or PROM• Fetal growth restriction (EFW <5%ile)• Oligohydramnios (AFI <5 cm)• Persistent BPP 6/10 or less or abnormal maternal/fetal testing
Risksofexpectantmanagement
• Severe HTN (10‐15%)• Eclampsia (0.2‐0.5%)• HELLP (1‐2%)• Abruption (0.5‐2%)• FGR (10‐12%)• Fetal demise (0.2‐0.5%)

RouteofDelivery• Mode of delivery should be determined by gestational age, fetal presentation, cervical status, and maternal and fetal conditions
• These women do NOT have to deliver via cesarean
• With induction, likelihood of cesarean delivery increases with decreasing gestational age

Magnesiumsulfate• Indications
• Eclampsia • Severe disease• Should be considered in women with certain signs/sx (HA, scotomata, blurry vision, RUQ pain)
• Infusion should continue in the OR• 4‐6 gm loading dose followed by maintenance of 1‐2 gm/hr
• If continue to have seizures, can give an additional 2 gm dose (20% solution)
• Therapeutic at 4‐7 mEq/L OR 4.8‐8.4 mg/dL• Magnesium sulfate is NOT given to treat HTN
PreviableManagement• Associated with high fetal morbidity and mortality
• Expectant management is not recommended
Postpartum• BP should be monitored for 72 hours in the hospital (or equivalent outpatient) and again 7‐10 days postpartum
• If BP persistently >/=150 mm Hg systolic or >/=100 mmHg diastolic, meds should be started
• If >/=160/110 mmHg, should be treated within 1 hour!
RiskFactors• Primiparous• Previous pregnancy with preeclampsia• CHTN or chronic renal disease• Thrombophilia• Multifetal gestation• IVF• Family history of preeclampsia• Overt diabetes (type I or II)• Obesity• Lupus• AMA >40 years
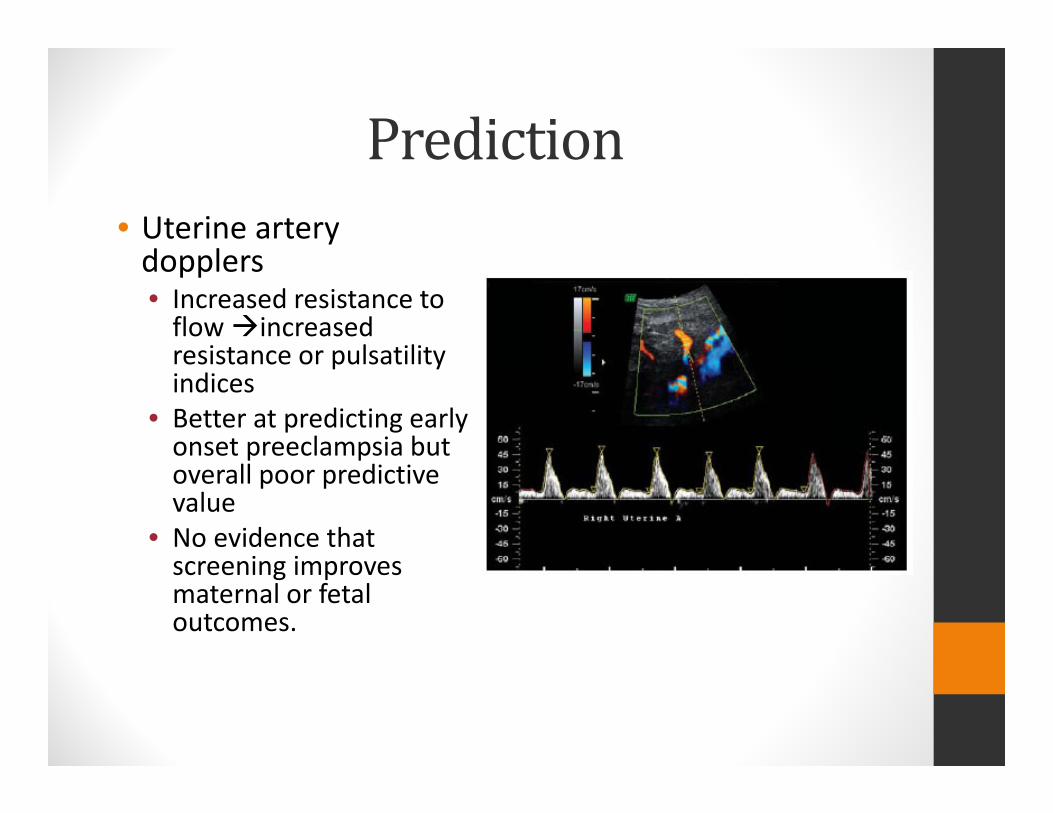
Prediction• Uterine artery dopplers• Increased resistance to flow increased resistance or pulsatilityindices
• Better at predicting early onset preeclampsia but overall poor predictive value
• No evidence that screening improves maternal or fetal outcomes.
Prediction• Biomarkers
• sFlt‐1 (soluble fms‐like tyrosine kinase 1)
• PIGF (placenta growth factor)
• VEGF (vascular endothelial growth factor)
• Promising but no evidence of improved outcomes
Prevention• Things that are NOT effective in preventing preeclampsia• Antioxidants‐vitamin C and vitamin E
• Bedrest• Salt restriction
Prevention• Low dose daily ASA (60‐80 mg)• history of early onset preeclampsia and preterm delivery <34 weeks gestation OR preeclampsia in more than one pregnancy
• Initiate in late first trimester
• Moderate quality of evidence
BestEvidence• Recommendations with the strongest evidence
• Vitamin E and C should not be used for preeclampsia prevention• Women with severe disease that is being expectantly managed <34 weeks should be given steroids (even if superimposed)
• Give magnesium sulfate for eclampsia• Women with severe preeclampsia should also be given magnesium sulfate
• Women with HELLP before viability should be delivered as soon as mother is stabilized
References• Cunningham, Leveno, Bloom et al (2014). Williams Obstetrics, 24th Ed. New York, NY: McGraw‐Hill.
• Hypertension in Pregnancy. The American College of Obstetricians and Gynecologists. 2013.
• Lindheimer, Roberts, Cunningham (2009). Chesley’sHypertensive Disorders in Pregnancy, 3rd Ed. San Diego, CA: Elsevier.














