Hypertension for nurses 29 th October 2008. Cardiovascular disease Blood pressure Heart attack...
43
Hypertension for nurses 29 th October 2008
-
Upload
gertrude-tucker -
Category
Documents
-
view
213 -
download
0
Transcript of Hypertension for nurses 29 th October 2008. Cardiovascular disease Blood pressure Heart attack...

Hypertension for nurses
29th October 2008

Cardiovascular disease
Blood pressure
Heart attack
Cholesterol Atheroma
Vascular narrowing
and/or occlusion
Stroke
Cigarettes Thrombosis Claudication
Diabetes Renal failure

Leading causes of death 2002WHO 2003 & Poole-Wilson. Clin Med JRCPL 2005; 5: 379-84.
478
496
606
735
754
929
1,398
2,399
4,692
5,823
Colo-rectal cancer
Tuberculosis
Stomach cancer
Hypertensive heart disease
Diabetes
Lung cancer
LRTI
COPD
Stroke disease
CHD
Deaths (thousands) 60 years & over

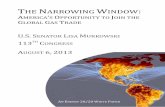
WHO global burden of disease major risk factors
Ezzati et al, Lancet 2002; 360:1347-60.
Total deaths: 55,861,000, year 2000
0 1000 2000 3000 4000 5000 6000 7000 8000
Unsafe water
Alcohol
Inactivity
High BMI
Low fruit and vegetables
Unsafe sex
Underweight
High cholesterol
Tobacco
High blood pressure
Thousands
7,141,000
4,907,000
4,915,000
3,748,000
2,886,000
2,726,000
2,591,000
1,922,000
1,804,000
1,730,000

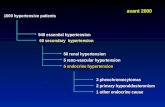
Renfrew 1972. Arbitrary dividing linesHawthorne, Greaves & Beevers, Brit Med J 1978.
Normotensive
(89) 1846 (60.3%)
Mild Hypertensive
(90-109) 1069 (34.9%)
Moderate Hypertensive
(110-129) 130 ( 4.2%)
Severe Hypertensive
(>130) 16 ( 0.5%)

Survival of untreated hypertensionLeishman, Brit Med J 1959; 1: 1361
MHT>150130-149120-129100-119
8%
16%
36%
66%
88%
100
90
80
70
60
50
40
30
20
10
Diastolic blood pressure
Percentdead
in 2 yr

CHD mortality v usual blood pressure Prospective Studies Collaboration, Lancet 2002; 360:1903-13

Stroke mortality v usual blood pressure Prospective Studies Collaboration, Lancet 2002; 360: 1903-13.

JNC 7New classification of hypertension
J Amer Med Ass 2003; 289: 2560-72
Classification of blood pressure for adults aged 18 years or older
Systolic BP Diastolic BP
Normal <120 and <80
Pre-hypertension 120-138 or 80-89
Stage 1 hypertension 140-159 or 90-99
Stage 2 hypertension > 160 or > 100

Cardiovascular risk in “non-hypertensives”Vassan et al, New Eng J Med 2001; 345: 1291-7. Framingham.

Framingham life expectancy 2005Franco et al, Hypertension 2005; 46: 280-6.
0 10 20 30 40
Normal BP
High normal
Hypertension
Normal BP
High normal
Hypertension
Life expectancy at age 50
Free of CVD
With MI
With stroke
With other CVD
Women
Men

Metropolitan Life Insurance Company
A man age 36 with a blood pressure of 150/100 will die before he reaches the retirement age of
65.

FRAMINGHAM
Over the age of 45, systolic blood pressure is a better predictor of risk than diastolic pressure.
Kannel WB, Am J Cardiol 1971; 27: 335.

Systolic versus diastolicWere we taught wrongly?
1970s. Reliable long-term epidemiological surveys in Framingham and elsewhere.
1980s. Cox’s proportional hazard model enables differentiation.
1990s. Computer hardware and software readily available.
So the current views are based on facts rather than opinions.

The definition of hypertension
“Hypertension should be defined in terms of a blood pressure level above which investigation and treatment do
more good than harm”
Grimley Evans & Rose, Br Med Bull 1971

British Hypertension Society-IVJ Human Hypertens 2004;
Thresholds and targets for treatment
Thresholds.1. Low-risk patients: (No end-organ damage or diabetes &
CVD risk < 20%).
160/100.
2. High risk patients. (End-organ damage or diabetes or CVD
risk > 20%):
140/90.
Targets.1. Diabetics:
130//80.
2. All other patients:
140/85.

Prevalence of hypertensionPrimatesta et al, Hypertension 2001;38: 827-32.
Health Survey for England 1998.
0
25
50
75
100
16-19 20-29 30-39 40-49 50-59 60-69 70-79 >80
Men WomenPercent
SBP >140 mmHg
and/or
DBP >90 mmHg
Age

Hypertension control in seven countries
Wolf-Maier et al, Hypertension 2004; 43: 10-7
Age and gender adjusted hypertension control
0
10
20
30
40
50
60
70
USA CAN ITAL SP ENG GER SW USA CAN ITAL SP ENG GER SW
Percent atTarget 160/95
Percent atTarget 140/90

Opportunistic screening in general practiceBarber et al, Brit Med J 1979; i: 843.
Men aged 35-69 years : 1 doctor
0
100
200
300
400
500
40.4%(199)
23.3%(114)
13.9%(68)
77.5%
(381)
Screened
(80)
1st Year
2nd
Year
3rd
Year
Total Eligible
Number of patients screened

Diabetes in a BP clinicSalmasi et al, Amer J Hypertens 2004; 17: 483-8. London.
Normal GTT, n=41
IGT or IFG, n=35
Diabetes, n=24

Prevalence of hypertension and dyslipidaemia in men as a function of glucose tolerance
Isomaa et al, Diabetes Care 2001; 24: 683-9.
0
10
20
30
40
50
60
Normal glucosetolerance
Impaired fastingglucose
Type 2 diabetes
Pat
ien
ts (
%)
Dyslipidaemia
Hypertension

STROKE
38% SD 4
8.7<0.0001
CHD
16% SD 4
38.80.0001
REMAINING VASCULAR
DEATHS
ALL VASCULAR DEATHS*
4.8<0.00021
ALL OTHER
DEATHS
1200
1000
800
600
400
200
T
T
C
C
T C
T C
CT
Total numbers of individuals affected
% reduction in odds:
No. of SD:2P=value
* includes any deaths from unknown causes
= fatal events
T = treatment
C = control
Brit. Med. Bull. 1994: 50: 272-90
525
140
835
234
934
470
1104
560
158 170
768
964
667 670

BP control in general practiceHudson. Practice Nurse 1993; 1: 14. Holmes Chapel
0%
25%
50%
75%
100%
General practitioner Practice nurse
Good (<160/90) Fair (160-180/90-110) Poor (>180/110)

Nurse run BP clinicCurzio et al, J Human Hypertens 1990; 4: 665-70. Western Infirmary, Glasgow
80
100
120
140
160
180
0 1 2 3 4Years follow up
SBP
DBP
Nurse run clinic: (n=198) – drop out rate = 8%Conventional clinic: (n-198) – drop out rate = 34%

Nurse management of hypertensionRudd et al, Amer J Hypertens 2004; 17: 921-7. California
Early counselling and telephone follow-up
p<0.01
p<0.01

Nurse-run hypertension OP clinicCurzio et al. J Human Hypertens 1990; 4: 665.
Nurse-run clinic Conventional clinic
Moved away 4% 0
To other clinic 11% 6%
Discharged 1% 15%
Died 9% 9%
Defaulted 8% 34%
Weight loss 2.8 kg 0.5 kg

Nurse management of hypertensionRudd et al, Amer J Hypertens 2004; 17: 921-7. California
Early counselling and telephone follow-up
P<0.05

Part 2
What causes the bloody thing?

The aetiology of hypertensionRenal disease
Renovascular disease
Secondary hypertension (2-3%) Aldosterone excess
Phaeochromocytoma
Others
Salt
Low fruit & vegetables
High fat diet
Essential hypertension (97-98% Weight
Alcohol
Exercise
Genetic factors

Drug-induced hypertension and interactions with antihypertensive drugs
Oestrogen-only oral contraceptives
LiquoriceOral & topical
corticosteroidsCold cures & nasal
decongestantsCyclosporinErythropoetin
Methysergide
Monoamine oxidase inhibitors
Narcotic abuse
Alcohol excess
Sibutramine
NSAIDS & coxibs
Lithium

Ever popular terms like “ idiopathic” and “essential” are actually
nonsensical as all diseases must have causes
Geoffrey Rose, Reflections on changing times. Brit Med J 1990; 301: 683-7

Family history and hypertensionStamler et al, JAMA 1979; 241: 43-6.
Percent of population with DBP 95 mmHg or more.Whites Blacks
Men Women Men Women All
Positive family history (%)
36.9 33.6 50.5 40.0 35.9
Negative family history (%)
22.1 19.5 36.3 22.2 21.8

Montreal Adoption StudyMongeau et al, Clin Exper Hypertens 1986; 8: 653-60
Correlation coefficients;
* p<0.001, † p<0.01
0.38*
Diastolic BP
0.53*
Systolic BP
0.26*
0.27* 0.29*
0.13†
0.21† 0.10
0.18
0.160.19
0.27*
0.24* 0.08
0.09
AANN
AANN
0.15*

Stress and hypertension
Whilst acutely stressful stimuli cause an acute rise in blood
pressure,
there is no convincing evidence that chronic stress causes
hypertension

Meta-analysis of salt intake v systolic BP Law et al, BMJ 1991; 302: 811
Age 20-29
SBP
Age 40-49
Age 60-69
0 100 200 300 400
Sodium Intake (mmol/24h)
Developed
Underdeveloped100
120
140
160
180
100
120
140
160
100
120
140
160

The effect on systolic BP (A) and diastolic BP (B) of reduced sodium intake and the DASH Diet.
Sacks FM, New Eng J Med 2001; 344: 3-10
412 subjects - normotensive + hypertensive - randomised to diet rich in veg & low fat & 3 levels of salt intake.7.1 mmHg normotensives11.5 mmHg hypertensives

Exercise and blood pressureWallace et al, Amer J Hypertens 1997; 10: 728-34. Indiana
25 untreated mildly hypertensive patients

Kaiser Permanente multiphasic health examination data
Klatsky et al, New Eng J Med 1977; 296 1194-2000.

Effects of obesityWestern Europe
Haslam & James. Lancet 2005; 366: 1197-209.
0 500 1000 1500 2000
Women
Men
Disability-adjusted life-years lost due to obesity x103
CHD
Hypertension
Stroke
Diabetes
Colon cancer
Endometrial cancer
Breast cancer
Osteoarthritis

Obesity and hypertensionHaemodynamic profile
Weir et al, Amer J Med 1991; 90 (suppl A): 5-14
1. High cardiac output2. Expanded plasma volume3. Increased salt sensitivity and intake4. Normal or decreased renin-angiotensin activity5. Normal or decreased peripheral resistance6. Raised sympathetic nervous system activity,
plasma adrenalin & noradrenalin 7. Insulin resistance

Blood pressure change with dietReisin et al, Ann Intern Med 1983; 98: 315-9
-20 -15 -10 -5 0 5 +10 +15
Change in weight (kg)
Change in MAP(mmHg)
+15
+10
+5
0
-5
-10
-15
-20
r = .49p < 0.05

SummaryCauses of hypertension
Unmodifiable
Family history
ModifiableSalt salt salt
Fruit & vegetablesAnimal fatObesity
Alcohol excessLack of exercise
Underlying renal adrenal diseases

Millions of undiagnosed, untreated & undertreated hypertensives
The existing structure of health-care delivery has failed to solve the problem
The primary health-care team can potentially improve things.
It’s time the nurses took over.
……but only if they receive adequate postgraduate training.