Hypersensitivity dr. agale
46
DR. SHUBHANGI V. AGALE ASSOCIATE PROFESSOR GRANT GOVT MEDICAL COOLEGE MUMBAI HYPERSENSITIVITY
-
Upload
shubhangi-agale -
Category
Health & Medicine
-
view
63 -
download
1
Transcript of Hypersensitivity dr. agale
DR. SHUBHANGI V. AGALE
ASSOCIATE PROFESSOR
GRANT GOVT MEDICAL
COOLEGE
MUMBAI
HYPERSENSITIVITY
HYPERSENSITIVITY
All forms of immune-mediated injuries are collectively denoted as hypersensitivity reactions.
Subdivided into four types:
TYPE 1
Allergy and Anaphylaxis.
Allergen cross-links Ig-E ab---
release of vaso-active amines and
other mediators from mast cells and
basophils—recruitment of
inflammatory cells
eg Anaphylaxis, Br.asthama.

TYPE 2
Ab to fixed Ag:IgG or IgM binds to
Ag on cell surface --- phagocytosis
of target cell by complement or
ADCC.AIHA. Erythroblastisis
foetalis,GP synrome.

TYPE 3
Immune –complex disease: Ag-Ab
complex –activate complement---
attracts neutrophils---release of
lysosomal enzymes, oxygen free
radicals. Serum
sickness,SLE,Arthus.

TYPE 4
Cell mediated (delayed)
hypersensitivity: Sensitised T
lymphocytes---release of cytokines
& T cell mediated cytotoxicity.
Tuberculosis, contact dermatitis,
transplant rejection.
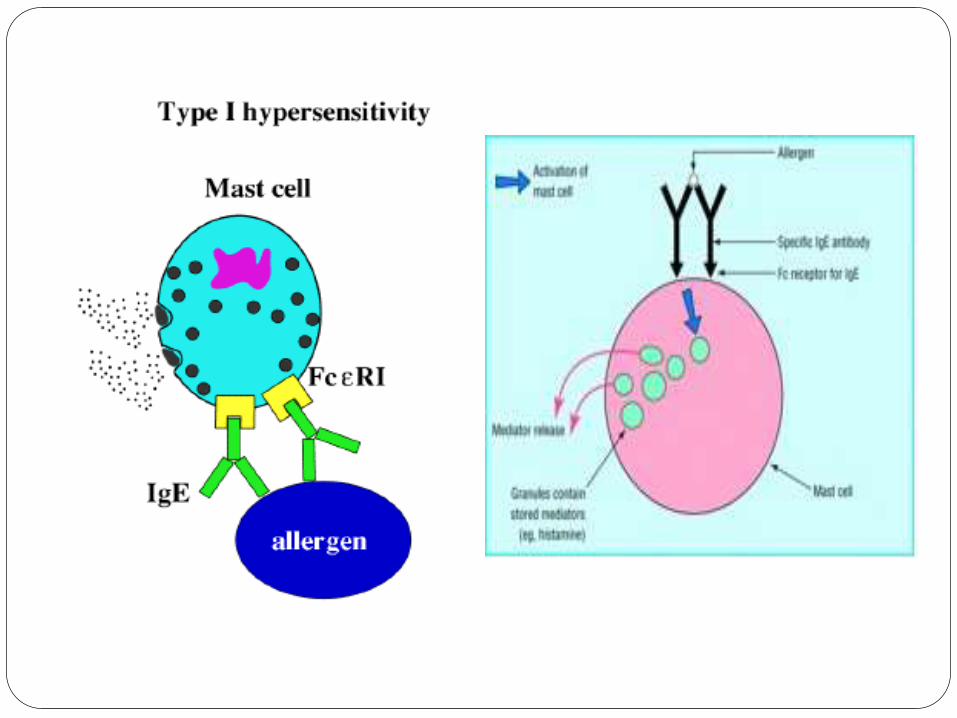
Type 1 hypersensitivity
reaction
Rapidly developing immunologic reaction occurring within minutes after the combination of an Antigen with Antibody bound to mast cells in an individual previously sensitized to the antigen.
Reaction ---- Allergy
Antigen ----- Allergen
Two reactions---- 1.systemic 2. local
Type 1 hypersensitivity
reaction
• Initial response---primary
mediators
• Late phase reaction—sec
mediators
1. Systemic reaction
Follows injection of an antigen to which host has become sensitized
Within minutes , state of fatal shock develop.
Ig G mediated antibody reaction
Mast cells
Primary mediators- histamine, enzymes (chymase, tryptase), proteoglycans
Secondary mediators- leukotriensC4,D4,B4, PG D2 , PAF, Interlukins

2. Local reaction
Skin allergy
Allergic rhinitis
Allergic conjunctivitis
Bronchial asthma
Food allergy
Hay fever
Immediate response
Evident within 5 to 30 minutes
Vasodilatation
Vascular leakage
Smooth muscle contraction
Glandular secretion
Subside within 60 minutes
Late phase reaction
Sets in 2 to 24 hrs after exposure
Without additional exposure to antigen
May last for several days
Infiltration of tissues by eosinophils
/neutrophils /monocytes/ lympocytes.
Tissue destruction, mucosal damage
E.g.- Bronchial asthma, allergic rhinitis

Type 1 hypersensitivity reaction
ATOPY
Genetically predisposed - local type
- I reaction to inhaled or ingested
allergens
E.g. pollen, house dust, food.
High Ig E levels
Family history - positive
PATHOGENESIS
Ig E mediated antibody reaction
Mast cells
Primary mediators- histamine, enzymes (chymase, tryptase), proteoglycans
Secondary mediators- leukotriensC4,D4,B4, PG D2 , PAF, Interleukins

Type 1 hypersensitivity reaction
PATHOLOGIC LESIONS
Vasodilatation
Smooth muscle spasm
Cellular infiltration
Inflammation
Mucus production
Oedema

Type-1
TYPE II - ANTIBODY MEDIATED
Mediated by Ab directed against Ag present on cell surface / extra-cellular matrix.
Secreted antibodies participate directly in injury to cells.
phagocytosis
lysis
injury to tissue by inducing inflammation.
Antibodies may also interfere with cellular functions & cause disease without tissue injury.
Type 2 hypersensitivity
reaction
Three different mechanisms
Complement---direct lysis or opsonisation.Transfusion reactions, erythroblastosis foetalis,AIHA,drugreactions,pemphigus vulgaris.
ADCC—leukocytes—neutrophils, eosinophils, macrophages & mast cells.
Ab mediated cellular dysfunction.e.g: myasthenia graves,greaves disease.
PATHOGENESIS
Production of Ig G / Ig M antibodies
Antibodies bind to antigen on target cell or tissue
Phagocytosis or lysis of target cell by complement activation
Leukocyte recruitment & inflammation

Type 2 hypersensitivity reaction
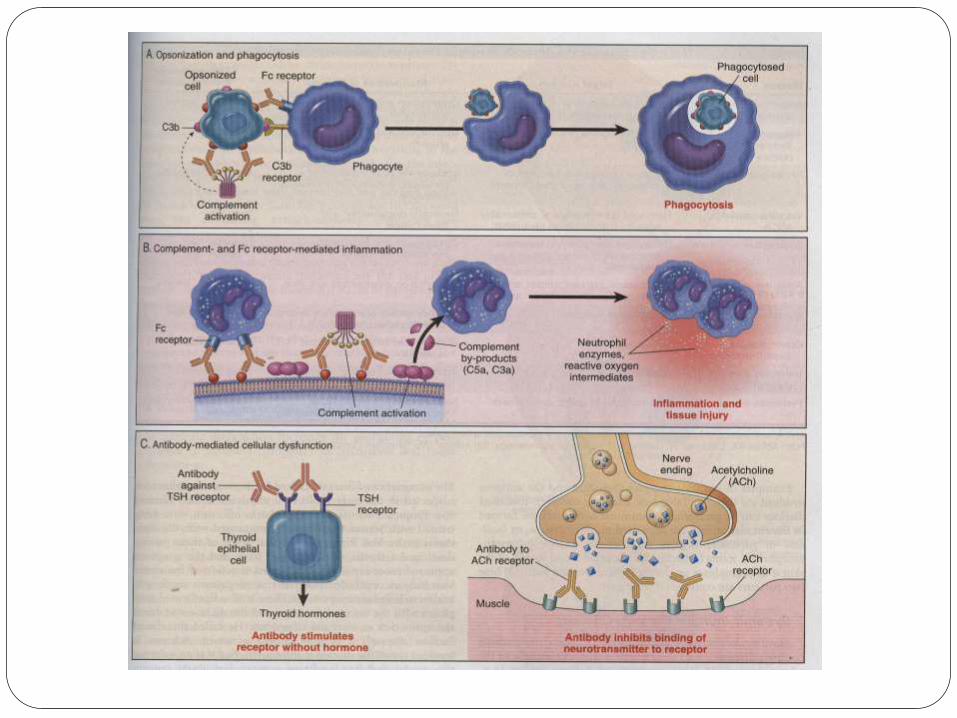
1. Opsonisation & complement
mediated cell destruction and
phagocytosis
Mismatched (Incompatible) blood transfusion- lysis of RBC (ABO incompatibility)
ERYTHROBLASTOSIS FETALIS -there is antigenic difference between mother and fetus. Ig G isoantibodies from mother cross placenta and cause destruction of fetal red cells (Rh incompatibility)
2. COMPLEMENT – AND FC
RECEPTOR MEDIATED
INFLAMMATION
Antibody deposition in extracellular matrix
Complement activation
Recruitment of neutrophils and monocytes
Release of injurious substances by activated leukocytes
Damage to tissue. e.g.-vascular rejection in organ graft.
No phagocytosis or lyses of cells.

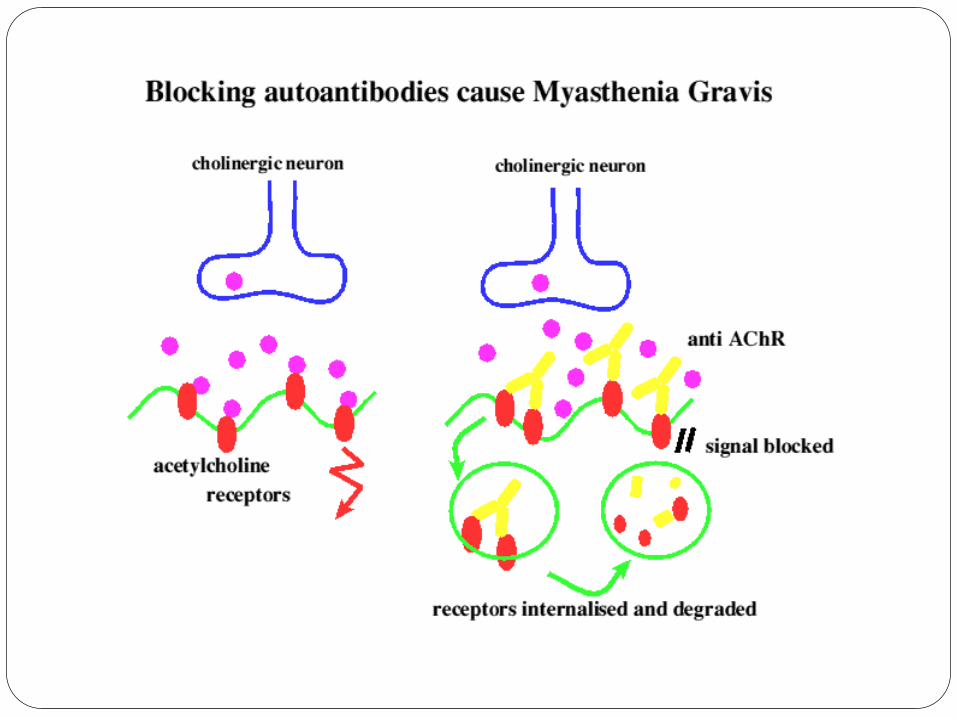
3. ANTIBODY MEDIATED
CELLULAR DYSFUNCTION
Antibodies directed against cell-surface receptors impair or dysregulate function. Both cells & antibodies take part In diseases. (ADCC)
Examples –Myasthenia Gravis
Pemphigus vulgaris
Graves disease
Pernicious Anemia
Rheumatic fever
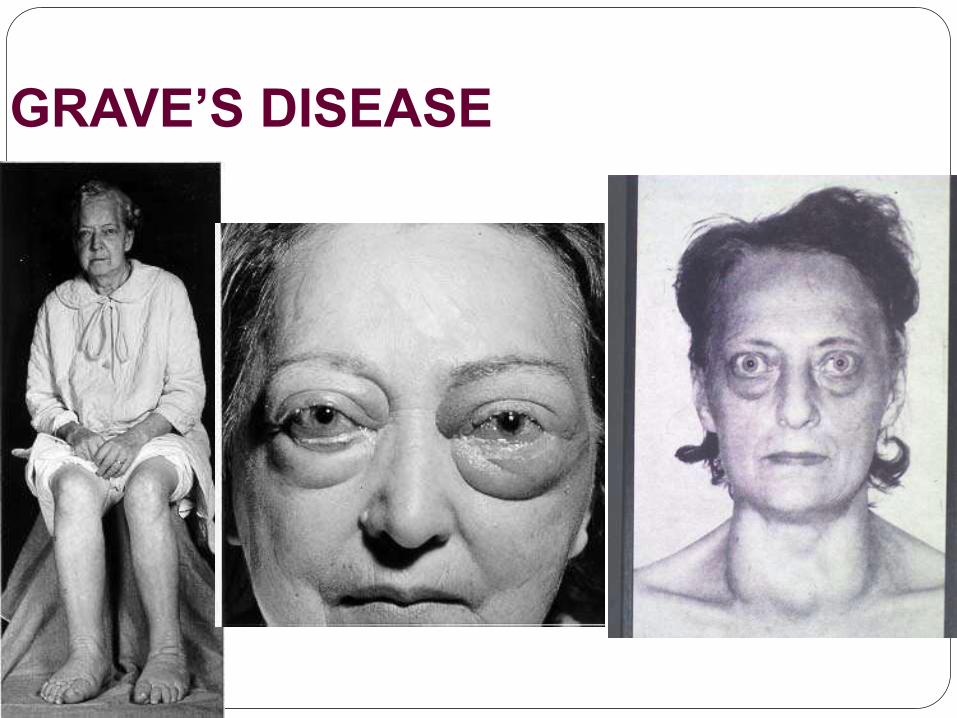
GRAVE’S DISEASE
Type III – IMMUNE COMPLEX
MEDIATED REACTION
Antigen – antibody complexes produce tissue damage mainly by eliciting inflammation at the site of deposition.
Antigen combines with antibody - circulate and are deposited in vessel walls, kidney & other sites.
Ag-Ab complexes are formed at extra-vascular sites where antigen may have been previously deposited.
Two types of antigens = exogenous (streptococci) and endogenous (DNA)
1. GENERALIZED (SYSTEMIC) ICD
Immune complexes are formed in circulation & are deposited in many organs.
Acute serum sickness Early 1900 Clemens von Pirquet
Pts with Diphtheria infection were being treated with serum from horses immunized with diphtheria toxin.
Pts developed fever ,skin rash & arthritis.
Symptoms appeared more rapidly with repeated injections of serum.
Conclusion : Treated pts made antibodies to horse serum proteins, & formed complexes with injected proteins.
PATHOGENESIS
Formation of ag-ab complexes in
circulation
Deposited in various tissues.
- An inflammatory reaction at the sites of
immune complex deposition. Neutrophilic
lysosomal enzyme degradation
-Complement activation
-Platelet aggregation- Micro thrombi-
ischemia- fibrinoid necrosis- vasculitis
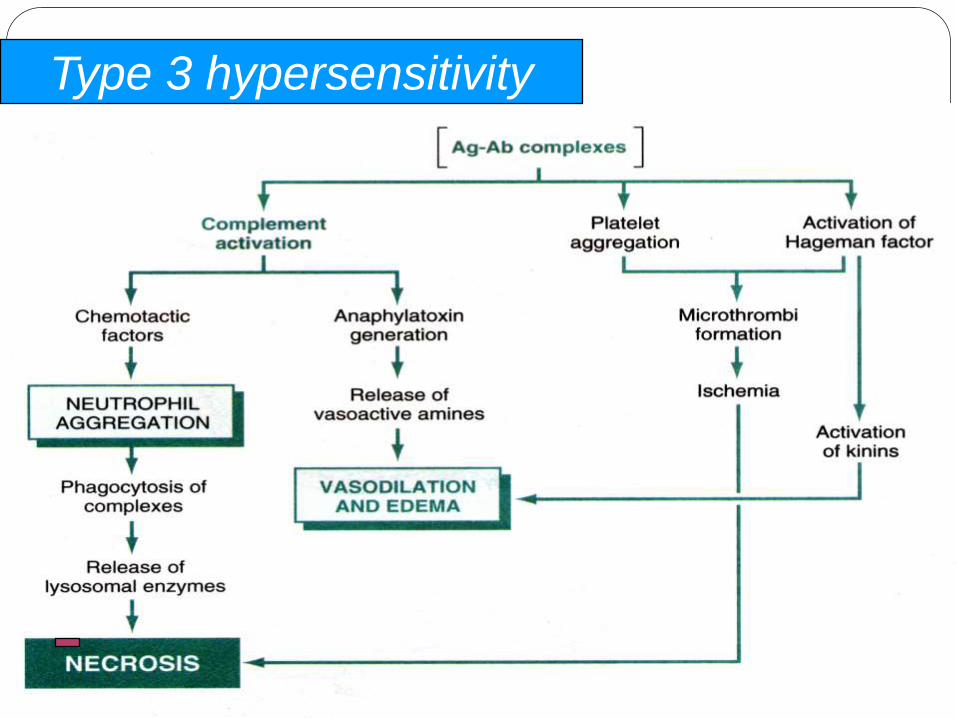
Type 3 hypersensitivity
EXAMPLES
Systemic lupus erythematous
Acute post-streptococcal GM
Poly arteritis nodosa (PAN)
Arthus reaction
Rheumatoid arthritis
Farmer’s Lung
Henoch schonlein purpura.
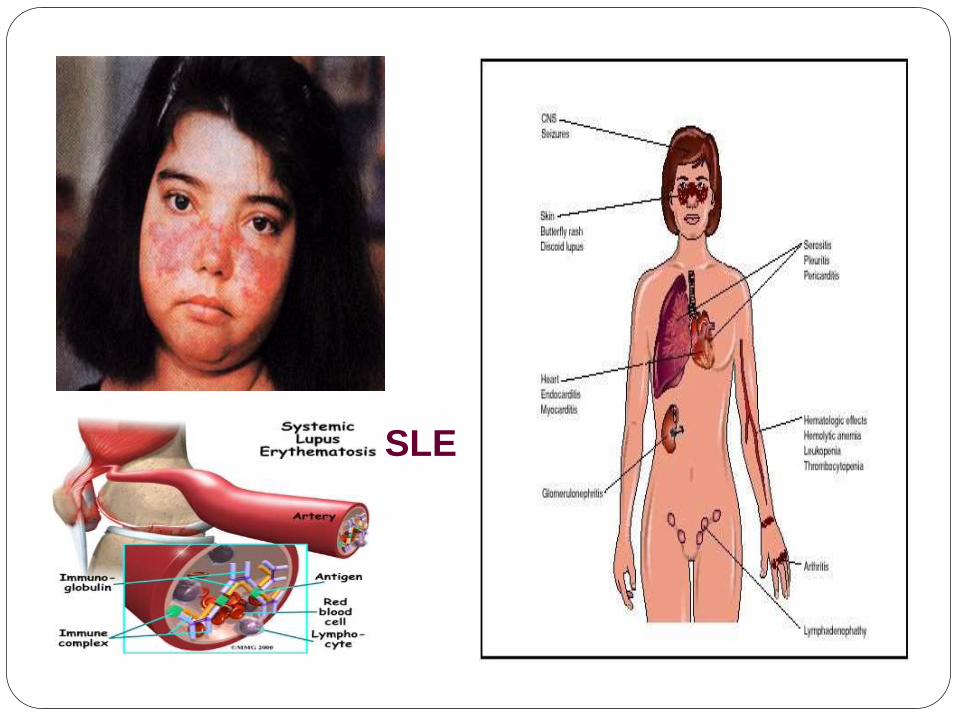
SLE

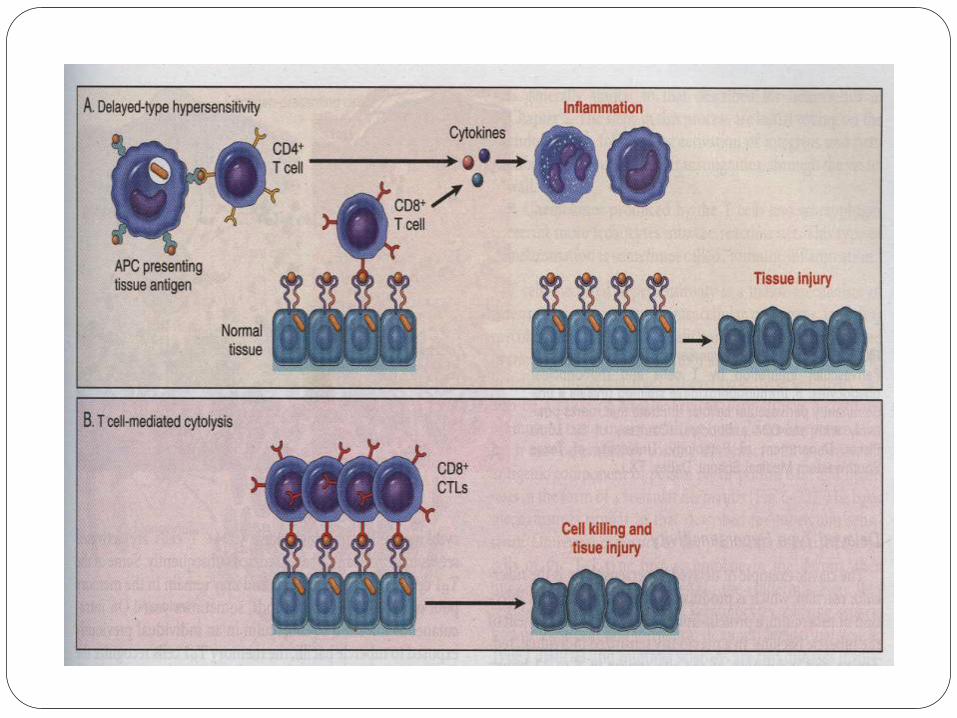
Type IV –T CELL MEDIATED
(DELAYED HYPERSENSITIVITY)
Initiated by antigen-activated (sensitized)
T – lymphocytes
Delayed type reaction – CD 4 +
Direct cell cytotoxicity - CD 8 + (CTL)
Principle pattern of immunologic response
to intracellular microbiologic agents
Mycobacterium tuberculosis, viruses, fungi,
parasites & protozoa.
Tuberculosis & Leprosy

TUBERCULIN REACTION
Intracutaneous injection of tuberculin, a protein lipopolysacharide component of the tubercle bacillus.
In previously sensitized individual reddening and induration of site appear in 8 to 12 hours, & reach a peak in 24 to 72 hours.

PROCEDURE
POSITIVE REACTION
Transplant rejection
Rejection is a complex process in
which both cell mediated immunity
and circulating antibodies have a
role to play.
Transplant rejection
T cell mediated rejection: in direct recognition (activates DTH) & direct recognition. –dendriticcells express high levels of MHC1 & MHC2 mole.
Antibody mediated rejection:Anti-HLA humoralabs develop concurrently with T cell mediated rejection.
Hyperacute rejection –where preformed anti-donor abs are present.
Acute rejection: within days to weeks.combinedprocess of cellular & humoral mech contribute.
Acute cellular rejection: c/f of renal failure.Extensive CD4+ & CD8+T cells with oedema & interstitial haemorrhage.
Acute rejection vasculitis: necrotising vasculitiswith endothelial cell necrosis.
Chronic rejection ---renal ischemia.
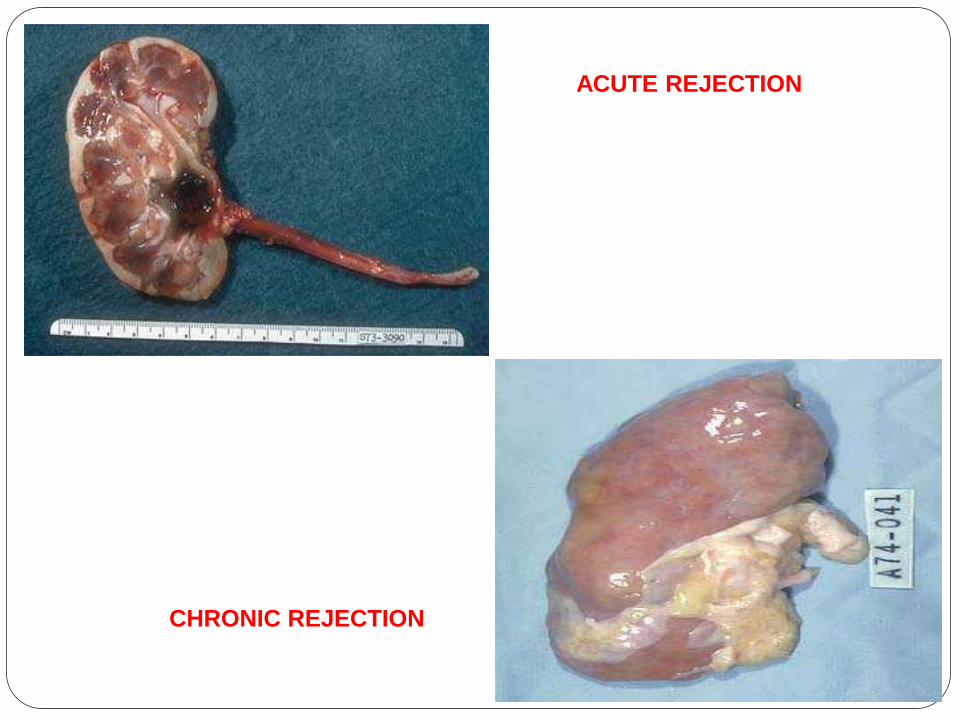
Rejection
Rejection
ACUTE REJECTION
CHRONIC REJECTION

SUMMARY
WHAT IS HYPERSENSITIVITY?
TYPES OF HYPERSENSITIVITY?
TYPE 1
TYPE 2
TYPE 3
TYPE 4
TUBERCULIN TEST
TRANSPLANT REJECTION

THANK
YOU