HYPERCALCEMIA IN MALIGNANCY
33
HYPERCALCEMIA IN MALIGNANCY 報告:PGY 林學群 │指導醫師:VS 吳家兆
Transcript of HYPERCALCEMIA IN MALIGNANCY

HYPERCALCEMIA IN MALIGNANCY
報告:PGY 林學群 │指導醫師:VS 吳家兆

Outline
• Introduction
• Clinical presentation
• Etiology and pathophysiology
• Diagnostic approach
• Management
2

Introduction
• Defined as the level above the upper limit of the normal reference range (usually > 10.5 mg/dl)
• Among all patients presenting to the ER with hypercalcemia Malignancy
Primary hyperparathyroidism
• Among all cancers Multiple myeloma has the highest prevalence
Breast, renal, and SqCC of any origin
• Of the total liquid malignancies Multiple myeloma is the most prevalent
Leukemia and non-Hodgkin lymphoma
3

Clinical presentation
Serum total calcium levels
• Mild (10.5-11.9 mg/dl): asymptomatic
• Moderate (12-13.9 mg/dl)
• Severe (≥ 14 mg/dl): often associated with malignancy
4

Etiology and pathophysiology
There are four mechanisms:
5

Humoral hypercalcemia of malignancy (HHM)
• Parathyroid hormone related peptide (PTHrP) Encoded by Parathyroid Hormone-like Hormone (PTHLH) gene
PTHLH and PTH genes have quite comparable structures The first 13 amino acids are almost identical
A similar secondary structure over the next 21 amino acids
Physiologic role Regulates osteoblast, osteoclast, and chondrocyte differentiation
Highly expressed in the placenta (Embryologic development)
Highly expressed in the breast during lactation (Mammary gland function)
6

Humoral hypercalcemia of malignancy (HHM)
• Parathyroid hormone related peptide (PTHrP) Secreted by
SqCC of skin, head, lung, esophagus, cervix
Adenocarcinoma of breast, prostate, ovary
Renal cell carcinoma
Bind to PTH1R despite differences in protein structure Mimic the effects of PTH: trigger RANKL expression in osteoblast
7

Humoral hypercalcemia of malignancy (HHM)
PTH PTHrP Same
• Increased bone turnover with greater increase in bone resorption than formation
• Increased Ca reabsorption in AL of Henle and DCT • Inhibition of P reabsorption in PCT
Difference • Increase renal 1α-hydroxylase activity Elevated level of 1,25 (OH)2D
• No native PTH secretion in patients with cancer, except parathyroid cancer
8

Local osteolytic hypercalcemia
• Common causes Multiple myeloma
Metastatic breast and lung cancer
• Local cytokines released from the tumor and surrounding cells (e.g., macrophages or endothelial cells) Include IL-1, IL-3, IL-6, TNF-α, TNF-β, etc.
Act similarly to PTH and PTHrp Increased secretion of RANKL by osteoblasts
Inhibit osteoblast function
9

Excess production of extra-renal 1,25-dihydroxyvitamin D • The cancer cells recruit the adjacent macrophages and stimulate
them to express 1α-hydroxylase Production by lymphomas (Hodgkin, non-Hodgkin, multiple myeloma)
Conversion of endogenous 25-hydroxyvitamin D into 1,25-dihydroxyvitamin D Bind to the receptors in the gut (increased intestine calcium absorption)
Normal to high phosphorus level
Suppressed level of PTH (negative feedback)
10

Ectopic secretion of parathyroid hormone
• Malignant cells can also produce ectopic PTH Pulmonary, thyroid, ovarian, pancreatic malignancies
Parathyroid adenoma or hyperplasia can also occur concomitantly
11

Diagnostic approach
• Verify with repeat measurement Albumin-calcium correction
Hyperalbuminemia (eg, severe dehydration): pseudohypercalcemia
Hypoalbuminemia (eg, chonic illness)
• Clinical clues Symptoms: more symptomatic in malignancy
Diet and Medication: thiazide, lithium, etc.
Family history: hyperparathyroidism
12

Diagnostic approach
• Laboratory evaluation: to differentiate PTH or non-PTH mediated Check serum intact PTH (35 to 65 pg/mL)
Elevated or minimally elevated
Low-normal or low (<20 pg/mL)
13

Diagnostic approach
• Non-PTH mediated
PTH related peptide: humoral hypercalcemia of malignancy
Serum phosphate concentration
1,25-dihydroxyvitamin D (calcitriol): lymphoma, granulomatous disease, etc.
25-hydroxyvitamin D: vitamin D intoxication
Urinary calcium excretion < 100 mg/day [2.5 mmol/day]
Milk-alkali syndrome
Thiazide diuretics
Familial hypocalciuric hypercalcemia
Multiple myeloma: SPEP, UPEP
Thyrotoxicosis: TSH
Vitamin A intoxication
14

15

Management
• Primary goal: treatment of underlying malignancy
• The type and timing of therapy Mild, asymptomatic: delay until a diagnosis has been made
Moderate to severe: start immediately Especially severe renal and neurologic symptoms
16

Management
Isotonic saline • Initial treatment of choice
Restore renal perfusion and increase renal calcium excretion
• The addition of furosemide is not recommended Reserved for symptoms of volume overload or oliguric renal failure
• The rate: depend on the severity, the age, and the comorbidities (eg, CHF) Usually, bolus 1-2 L followed by maintenance 100-150ml/hr titrated to ensure urine output of
100ml/hr
17

Management
Calcitonin • Adjunctive initial therapy
Inhibit osteoclastic bone resorption and renal calcium reabsorption
• The addition of bisphosphonate: lower calcium level more rapidly
• The addition of glucocorticoids: enhance the effect (upregulating surface receptors)
• Disadvantage: Tachyphylaxis within 3 days (downregulation of receptors)
• Minimal side effects
18

Management
Bisphosphonates (pyrophosphate analogues) • First line therapy and should be given within 48h of diagnosis (2-4 days to take
effect) Target osteoclasts inducing their apoptosis
Proliferation and differentiation of osteoblast
19

Management
Corticosteroid • Clinical effect in multiple myeloma and other hematological malignancies
associated with 1, 25(OH)2D overproduction Inhibit conversion of 1α-hydroxylase
Decrease tumor production of locally active cytokines
Inhibit osteoclast resorption
20

Management
Denosumab (human monoclonal antibody to RANKL) • Inhibits osteoclasts activity
• More pronounced in patients with renal failure
21

Management
Cinacalcet (calcimimetic agent) • Increase the sensitivity of the calcium sensing receptor (CaSR) to extracellular
calcium level Effect a reduction in PTH and therefore a reduction in serum calcium level
22

Management
Hemodialysis
• Recommended for GFR < 10-20ml/min
Severe congestive heart failure
Treatment failure (hydration, bisphosphonates)
23

Management
24

Take home message
• Hypercalcemia of malignancy is a common finding in patients with advanced stage cancers.
• There are four mechanisms which are responsible for the development of hypercalcemia of malignancy.
Humoral hypercalcemia of malignancy
Local osteolytic hypercalcemia
Excess production of extra-renal 1,25-dihydroxyvitamin D
Ectopic secretion of parathyroid hormone
25

Take home message
• Clinical evaluation, including presence or absence of symptoms, family history, and medications, may help determine the etiology of hypercalcemia.
• Measurement of intact PTH is important to distinguish PTH-mediated from non-PTH-mediated causes of hypercalcemia.
• Treatment includes i. v. hydration, calcitonin, bisphosphonates, denosumab, corticosteroids, and cinacalcet depending on the cause of hypercalcemia. Hemodialysis should be considered for advanced underlying kidney disease and/or refractory
severe hypercalcemia
26

References
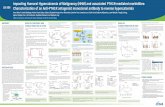
• Diagnosis, Pathophysiology and Management of Hypercalcemia in Malignancy: A Review of the Literature
- Horm Metab Res. 2019 Dec -
• Hypercalcemia and Cancer: Differential Diagnosis and Treatment - CA Cancer J Clin. 2018 Sep -
• Diagnostic approach to hypercalcemia - UpToDate -
27

Progression of a Solitary
Plasmacytoma to Multiple Myeloma Left pelvic mass in this patient
28

Plasmacytomas
A mass composed of neoplastic monoclonal plasma cells
• Solitary plasmacytoma of bone (SBP): Occur solely in the bone
• Extramedullary plasmacytoma (EMP): arise outside bone in soft tissues
Differentiation criteria for both SBP and EMP from myeloma
• Lack of CRAB features (not systemic)
• Normal bone marrow with no evidence of clonal plasma cells BM may show <10% plasma cells in 4% of patients due to patchy BM involvement
• Normal imaging except for the primary lesion
29

SBP versus EMP
SBP EMP
Presentation A single, typically painful bone lesion Space-occupying lesions
Site • Axial skeleton (83%) • Appendicular skeleton (17%) (e.g,
pelvic bones)
• Soft tissue (usually in nasal cavity and nasopharynx)
Treatment RT (highly radiosensitive disease) even after gross total excision
RT instead of radical surgery due to head and neck region
30

Our case
31
• Biopsy of soft tissue, left pelvis: Plasma cell myeloma, with kappa monoclonality
• Biopsy of bone marrow: Slightly increased small T cells without aggregation
No increase or clusters of B cells
• Abdomen CT: multiple osteolytic lesions involving the T-L vertebrae, pelvic bones and bilateral femurs
• Bone scan: suspected multiple bony metastasis
• Lab tests: no significant biomarker of malignancy
Suspicion: SBP progresses to MM

References
• Plasmacytoma (Solitary bone plasmacytoma, extramedullary plasmacytoma) - Atlas Genet Cytogenet Oncol Haematol. 2019 -
• A Review for Solitary Plasmacytoma of Bone and Extramedullary Plasmacytoma - The Scientific World Journal 2012 -
32

Thanks for your attention
33