Humoral Hypercalcemia Complicating Adenocarcinoma of the Sigmoid Colon: Report of a Case
4
Surg Today (2005) 35:692–695 DOI 10.1007/s00595-004-2974-3 Humoral Hypercalcemia Complicating Adenocarcinoma of the Sigmoid Colon: Report of a Case Jun Sakata 1 , Toshifumi Wakai 1 , Yoshio Shirai 1 , Eiko Sakata 1 , Go Hasegawa 2 , and Katsuyoshi Hatakeyama 1 Divisions of 1 Digestive and General Surgery and 2 Pathomorphology, Niigata University Graduate School of Medical and Dental Sciences, 1-757 Asahimachi-dori, Niigata 951-8510, Japan roid hormone-related peptide (PTHrP) produced by tumor cells, and local osteolytic hypercalcemia, caused by extensive skeletal tumor involvement. 1 Humoral hypercalcemia of malignancy complicates a variety of malignancies, most commonly squamous, renal, and urothelial tumors. 1 Primary colorectal malignancies are rarely associated with HHM. In fact, we found only 20 cases reported in the English-language literature (PubMed, National Library of Medicine, Bethesda, MD, USA) up to the end of 2003. 2–18 We reviewed these 20 cases and report a further case, in an attempt to clarify the clinicopathologic features of colorectal carci- noma associated with HHM. Case Report A 52-year-old Japanese woman underwent a radical sigmoidectomy and lateral segmentectomy with partial hepatectomy for primary colonic cancer with synchro- nous liver metastases. The primary tumor was well- differentiated adenocarcinoma, and the resected liver specimen contained ten metastatic deposits of poorly differentiated adenocarcinoma. For 12 months after discharge, she received 5-fluorouracil (500 mg/m 2 per week) and leucovorin (250 mg/m 2 per week) intrave- nously. However, a follow-up computed tomography scan 2 years later showed metachronous metastases in the remnant liver, and she was referred to our department for repeat hepatectomy. Her symptoms on admission included upper abdominal pain, anorexia, constipation, muscle weakness, and lethargy. Labora- tory data showed an elevated serum calcium level of 14.2 mg/dl (reference range, 8.7–10.0 mg/dl) and a low serum phosphorus level of 2.2 mg/dl (reference range, 2.5–4.6 mg/dl). The serum levels of carcinoembryonic antigen and carbohydrate antigen 19-9 were 14.1 ng/ml (reference range, 0–6 ng/ml) and 44 U/ml (reference range, 0–37 U/ml), respectively. A skeletal survey and Abstract Humoral hypercalcemia can arise from a variety of malignancies, but its association with primary colorectal carcinoma is rare, with only 20 such cases documented in the English-language literature to date. We report an additional case to clarify the clinicopathologic features of colorectal carcinoma with humoral hypercalcemia. A 54-year-old woman was admitted with symptomatic hypercalcemia of 14.2 mg/dl and multiple hepatic me- tastases, 2 years after resection of sigmoid colon cancer. The hypercalcemia was caused by the circulating par- athyroid hormone-related peptide (PTHrP) produced by poorly differentiated adenocarcinoma in the liver. The PTHrP level on admission was 13.5 pmol/l. Despite systemic chemotherapy, the patient died of disease pro- gression 3 weeks after the humoral hypercalcemia was diagnosed. A review of the 21 reported cases, including ours, suggests that colorectal carcinoma associated with humoral hypercalcemia is characterized by a poorly differentiated tumor with or without squamous or neu- roendocrine features, distant metastases, and a dismal prognosis. Key words Humoral hypercalcemia of malignancy · Parathyroid hormone-related peptide · Paraneoplastic syndrome · Colorectal neoplasm · Prognosis Introduction Hypercalcemia is a common metabolic manifestation of cancer. Malignancy-associated hypercalcemia is divided into two syndromes: humoral hypercalcemia of malig- nancy (HHM), which results from a circulating parathy- Reprint requests to: T. Wakai Received: January 5, 2004 / Accepted: November 16, 2004
-
Upload
jun-sakata -
Category
Documents
-
view
214 -
download
2
Transcript of Humoral Hypercalcemia Complicating Adenocarcinoma of the Sigmoid Colon: Report of a Case

Surg Today (2005) 35:692–695DOI 10.1007/s00595-004-2974-3
Humoral Hypercalcemia Complicating Adenocarcinoma ofthe Sigmoid Colon: Report of a Case
Jun Sakata1, Toshifumi Wakai1, Yoshio Shirai1, Eiko Sakata1, Go Hasegawa2, and Katsuyoshi Hatakeyama1
Divisions of 1 Digestive and General Surgery and 2 Pathomorphology, Niigata University Graduate School of Medical and Dental Sciences,1-757 Asahimachi-dori, Niigata 951-8510, Japan
roid hormone-related peptide (PTHrP) produced bytumor cells, and local osteolytic hypercalcemia, causedby extensive skeletal tumor involvement.1 Humoralhypercalcemia of malignancy complicates a variety ofmalignancies, most commonly squamous, renal, andurothelial tumors.1 Primary colorectal malignancies arerarely associated with HHM. In fact, we found only20 cases reported in the English-language literature(PubMed, National Library of Medicine, Bethesda,MD, USA) up to the end of 2003.2–18 We reviewed these20 cases and report a further case, in an attempt toclarify the clinicopathologic features of colorectal carci-noma associated with HHM.
Case Report
A 52-year-old Japanese woman underwent a radicalsigmoidectomy and lateral segmentectomy with partialhepatectomy for primary colonic cancer with synchro-nous liver metastases. The primary tumor was well-differentiated adenocarcinoma, and the resected liverspecimen contained ten metastatic deposits of poorlydifferentiated adenocarcinoma. For 12 months afterdischarge, she received 5-fluorouracil (500 mg/m2 perweek) and leucovorin (250mg/m2 per week) intrave-nously. However, a follow-up computed tomographyscan 2 years later showed metachronous metastasesin the remnant liver, and she was referred to ourdepartment for repeat hepatectomy. Her symptoms onadmission included upper abdominal pain, anorexia,constipation, muscle weakness, and lethargy. Labora-tory data showed an elevated serum calcium level of14.2 mg/dl (reference range, 8.7–10.0mg/dl) and a lowserum phosphorus level of 2.2mg/dl (reference range,2.5–4.6 mg/dl). The serum levels of carcinoembryonicantigen and carbohydrate antigen 19-9 were 14.1 ng/ml(reference range, 0–6 ng/ml) and 44U/ml (referencerange, 0–37 U/ml), respectively. A skeletal survey and
AbstractHumoral hypercalcemia can arise from a variety ofmalignancies, but its association with primary colorectalcarcinoma is rare, with only 20 such cases documentedin the English-language literature to date. We report anadditional case to clarify the clinicopathologic featuresof colorectal carcinoma with humoral hypercalcemia. A54-year-old woman was admitted with symptomatichypercalcemia of 14.2 mg/dl and multiple hepatic me-tastases, 2 years after resection of sigmoid colon cancer.The hypercalcemia was caused by the circulating par-athyroid hormone-related peptide (PTHrP) producedby poorly differentiated adenocarcinoma in the liver.The PTHrP level on admission was 13.5 pmol/l. Despitesystemic chemotherapy, the patient died of disease pro-gression 3 weeks after the humoral hypercalcemia wasdiagnosed. A review of the 21 reported cases, includingours, suggests that colorectal carcinoma associated withhumoral hypercalcemia is characterized by a poorlydifferentiated tumor with or without squamous or neu-roendocrine features, distant metastases, and a dismalprognosis.
Key words Humoral hypercalcemia of malignancy ·Parathyroid hormone-related peptide · Paraneoplasticsyndrome · Colorectal neoplasm · Prognosis
Introduction
Hypercalcemia is a common metabolic manifestation ofcancer. Malignancy-associated hypercalcemia is dividedinto two syndromes: humoral hypercalcemia of malig-nancy (HHM), which results from a circulating parathy-
Reprint requests to: T. WakaiReceived: January 5, 2004 / Accepted: November 16, 2004
Used Mac Distiller 5.0.x Job Options
This report was created automatically with help of the Adobe Acrobat Distiller addition "Distiller Secrets v1.0.5" from IMPRESSED GmbH. You can download this startup file for Distiller versions 4.0.5 and 5.0.x for free from http://www.impressed.de. GENERAL ---------------------------------------- File Options: Compatibility: PDF 1.2 Optimize For Fast Web View: Yes Embed Thumbnails: Yes Auto-Rotate Pages: No Distill From Page: 1 Distill To Page: All Pages Binding: Left Resolution: [ 600 600 ] dpi Paper Size: [ 595.3 785.2 ] Point COMPRESSION ---------------------------------------- Color Images: Downsampling: Yes Downsample Type: Bicubic Downsampling Downsample Resolution: 150 dpi Downsampling For Images Above: 225 dpi Compression: Yes Automatic Selection of Compression Type: Yes JPEG Quality: Medium Bits Per Pixel: As Original Bit Grayscale Images: Downsampling: Yes Downsample Type: Bicubic Downsampling Downsample Resolution: 150 dpi Downsampling For Images Above: 225 dpi Compression: Yes Automatic Selection of Compression Type: Yes JPEG Quality: Medium Bits Per Pixel: As Original Bit Monochrome Images: Downsampling: Yes Downsample Type: Bicubic Downsampling Downsample Resolution: 600 dpi Downsampling For Images Above: 900 dpi Compression: Yes Compression Type: CCITT CCITT Group: 4 Anti-Alias To Gray: No Compress Text and Line Art: Yes FONTS ---------------------------------------- Embed All Fonts: Yes Subset Embedded Fonts: No When Embedding Fails: Warn and Continue Embedding: Always Embed: [ ] Never Embed: [ ] COLOR ---------------------------------------- Color Management Policies: Color Conversion Strategy: Convert All Colors to sRGB Intent: Default Working Spaces: Grayscale ICC Profile: RGB ICC Profile: sRGB IEC61966-2.1 CMYK ICC Profile: U.S. Web Coated (SWOP) v2 Device-Dependent Data: Preserve Overprint Settings: Yes Preserve Under Color Removal and Black Generation: Yes Transfer Functions: Apply Preserve Halftone Information: Yes ADVANCED ---------------------------------------- Options: Use Prologue.ps and Epilogue.ps: No Allow PostScript File To Override Job Options: Yes Preserve Level 2 copypage Semantics: Yes Save Portable Job Ticket Inside PDF File: No Illustrator Overprint Mode: Yes Convert Gradients To Smooth Shades: No ASCII Format: No Document Structuring Conventions (DSC): Process DSC Comments: No OTHERS ---------------------------------------- Distiller Core Version: 5000 Use ZIP Compression: Yes Deactivate Optimization: No Image Memory: 524288 Byte Anti-Alias Color Images: No Anti-Alias Grayscale Images: No Convert Images (< 257 Colors) To Indexed Color Space: Yes sRGB ICC Profile: sRGB IEC61966-2.1 END OF REPORT ---------------------------------------- IMPRESSED GmbH Bahrenfelder Chaussee 49 22761 Hamburg, Germany Tel. +49 40 897189-0 Fax +49 40 897189-71 Email: [email protected] Web: www.impressed.de
Adobe Acrobat Distiller 5.0.x Job Option File
<< /ColorSettingsFile () /LockDistillerParams false /DetectBlends false /DoThumbnails true /AntiAliasMonoImages false /MonoImageDownsampleType /Bicubic /GrayImageDownsampleType /Bicubic /MaxSubsetPct 100 /MonoImageFilter /CCITTFaxEncode /ColorImageDownsampleThreshold 1.5 /GrayImageFilter /DCTEncode /ColorConversionStrategy /sRGB /CalGrayProfile () /ColorImageResolution 150 /UsePrologue false /MonoImageResolution 600 /ColorImageDepth -1 /sRGBProfile (sRGB IEC61966-2.1) /PreserveOverprintSettings true /CompatibilityLevel 1.2 /UCRandBGInfo /Preserve /EmitDSCWarnings false /CreateJobTicket false /DownsampleMonoImages true /DownsampleColorImages true /MonoImageDict << /K -1 >> /ColorImageDownsampleType /Bicubic /GrayImageDict << /HSamples [ 2 1 1 2 ] /VSamples [ 2 1 1 2 ] /Blend 1 /QFactor 0.9 >> /CalCMYKProfile (U.S. Web Coated (SWOP) v2) /ParseDSCComments false /PreserveEPSInfo false /MonoImageDepth -1 /AutoFilterGrayImages true /SubsetFonts false /GrayACSImageDict << /VSamples [ 2 1 1 2 ] /HSamples [ 2 1 1 2 ] /Blend 1 /QFactor 0.76 /ColorTransform 1 >> /ColorImageFilter /DCTEncode /AutoRotatePages /None /PreserveCopyPage true /EncodeMonoImages true /ASCII85EncodePages false /PreserveOPIComments false /NeverEmbed [ ] /ColorImageDict << /HSamples [ 2 1 1 2 ] /VSamples [ 2 1 1 2 ] /Blend 1 /QFactor 0.9 >> /AntiAliasGrayImages false /GrayImageDepth -1 /CannotEmbedFontPolicy /Warning /EndPage -1 /TransferFunctionInfo /Apply /CalRGBProfile (sRGB IEC61966-2.1) /EncodeColorImages true /EncodeGrayImages true /ColorACSImageDict << /VSamples [ 2 1 1 2 ] /HSamples [ 2 1 1 2 ] /Blend 1 /QFactor 0.76 /ColorTransform 1 >> /Optimize true /ParseDSCCommentsForDocInfo false /GrayImageDownsampleThreshold 1.5 /MonoImageDownsampleThreshold 1.5 /AutoPositionEPSFiles false /GrayImageResolution 150 /AutoFilterColorImages true /AlwaysEmbed [ ] /ImageMemory 524288 /OPM 1 /DefaultRenderingIntent /Default /EmbedAllFonts true /StartPage 1 /DownsampleGrayImages true /AntiAliasColorImages false /ConvertImagesToIndexed true /PreserveHalftoneInfo true /CompressPages true /Binding /Left >> setdistillerparams << /PageSize [ 576.0 792.0 ] /HWResolution [ 600 600 ] >> setpagedevice

693J. Sakata et al.: Humoral Hypercalcemia from Colonic Cancer
bone scan showed no evidence of bony metastases. Anelevated serum level of PTHrP (Allegro PTHrP kit,Nichols Institute Diagnostics, San Clemente, CA, USA)of 13.5pmol/l (reference range, <0.6pmol/l) and aserum level of intact parathyroid hormone (Allegro in-tact PTH kit, Nichols Institute Diagnostics) of less than5ng/l (reference range, 10–60ng/l) confirmed a diagno-sis of HHM. The patient was treated with intravenoussaline hydration followed by an infusion of 30mg ofpamidronate. Within 5 days, the calcium level de-creased to 11.5mg/dl and her clinical status improved.As computed tomography showed numerous metastaticdeposits throughout the entire liver, repeat hepatec-tomy was not considered. Systemic chemotherapywas started with oral TS-1 200mg/day (Taiho Pharma-ceutical, Tokyo, Japan), which consisted of tegafur 5-chloro-2,4-dihydroxypyridine, and potassium oxonate,in a molar ratio of 1 : 0.4 :1. Despite treatment, the livertumors continued to grow and multiple lung lesionsappeared. The patient died of progressive disease 3weeks after the HHM was diagnosed. Autopsy was notperformed.
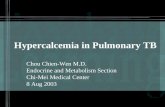
Immunohistochemical examination of the primarysigmoid colon tumor, using a monoclonal antibodyagainst PTHrP (Oncogene Research Product, Cam-bridge, MA, USA) revealed negative staining. In con-trast, the resected liver metastases stained positively(Fig. 1).
Discussion
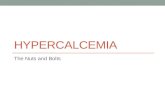
Humoral hypercalcemia of malignancy is a rare mani-festation of colorectal carcinoma. Kubota et al.5 re-ported only two cases of HHM among 1053 patients(0.02%) with colorectal carcinoma. The histopathologictype of both of these cancers was adenosquamous car-cinoma. A review of the 21 reported cases of HHMcomplicating colorectal carcinoma, including that of ourpatient, revealed that poorly differentiated/undifferen-tiated (n = 12) or adenosquamous carcinoma (n = 8)were the dominant histopathologic types (Table 1).Four reported cases also showed neuroendocrine fea-tures.6,13,16,18 In the case we described, immunohis-tochemical analysis revealed that PTHrP was positiveonly in the liver metastases of poorly differentiatedadenocarcinoma, indicating that the dedifferentiationof tumor cells may lead to excessive production ofPTHrP. Taken together, these findings suggest thatcolorectal carcinoma associated with HHM is character-ized by a poorly differentiated tumor with or withoutsquamous or neuroendocrine features.
The symptoms of HHM include nausea, vomiting,anorexia, constipation, muscle weakness, lethargy, andmental confusion,4,7 some of which were experienced byour patient. Thus, we recommend measuring the serumcalcium levels if patients with malignancies have thesesymptoms. Distant metastases are common in patientswith colorectal malignancies and HHM.11,12,16,17 All ofthe 17 patients with documented metastatic disease hadliver metastases. Thus, HHM should be considered
Fig. 1. Immunohistochemical analysis ofa metastatic lesion in the liver, done usinga monoclonal antibody against parathy-roid hormone-related peptide. The cyto-plasm of the poorly differentiated tumorcells was stained positively (¥200)

694 J. Sakata et al.: Humoral Hypercalcemia from Colonic Cancer
Tab
le 1
.R
epor
ted
case
s of
hum
oral
hyp
erca
lcem
ia a
ssoc
iate
d w
ith
colo
rect
al c
arci
nom
a
Out
com
e af
ter
Sex/
age
Pri
mar
yH
isto
logy
Seru
m c
once
ntra
tion
sde
tect
ion
ofF
irst
aut
horR
ef.
Yea
r(y
ears
)si
teSi
tes
of m
etas
tase
sT
ype
Gra
deC
alci
umP
TH
PT
HrP
hype
rcal
cem
ia
Cas
tlem
an2
1963
M/7
7C
olon
HE
P, L
YM
Ade
noG
3-4
14m
g/dl
ND
ND
3 w
eeks
; DO
DM
ozaf
fari
an3
1969
M/4
6C
olon
HE
PA
deno
ND
15m
g/dl
ND
ND
3 w
eeks
; DO
DO
men
n419
69M
/79
Col
onN
DN
DN
D17
.8m
g/dl
ND
ND
ND
; DO
DK
ubot
a519
80M
/43
Col
onH
EP
, PU
L, K
idne
yA
sN
D7.
6m
Eq/
lU
ndet
ecta
ble
ND
<1 m
onth
; DO
DK
ubot
a519
80M
/39
Rec
tum
HE
P, P
ER
As
G3
7.9
mE
q/l
Und
etec
tabl
eN
D1
wee
k; D
OD
Pal
vio6
1985
F/6
7R
ectu
mH
EP
, PU
L, A
DR
, OSS
,A
saG
44.
0m
mol
/lSl
ight
lyN
D2
mon
ths;
DO
DL
YM
, PE
R, P
LE
,el
evat
edT
hyro
idC
hevi
nsky
719
87F
/41
Col
onH
EP
, LY
MA
sG
318
.4m
g/dl
ND
ND
6 da
ys; D
OD
Ber
kelh
amm
er8
1989
M/7
4C
olon
HE
P, P
UL
As
G3
14.5
mg/
dlU
ndet
ecta
ble
ND
2 w
eeks
; DO
DM
arch
919
91M
/58
Rec
tum
HE
PA
deno
ND
17.6
mg/
dl15
ng/l
ND
ND
; DO
DG
urne
y1019
93N
DC
olon
ND
ND
ND
ND
ND
2–10
pmol
/lN
D; N
DG
urne
y1019
93N
DC
olon
ND
ND
ND
ND
ND
>20
pmol
/lN
D; N
DL
inks
1119
94M
/58
Col
onH
EP
As
G3
2.99
mm
ol/l
0.55
ng/m
l25
.5pm
ol/l
7 m
onth
s; D
OD
de S
ouza
1219
95F
/52
Rec
tum
HE
PA
deno
G3
4.52
mm
ol/l
0.3
pmol
/l16
2pm
ol/l
3 w
eeks
; DO
DSi
dler
1319
96M
/75
Col
onH
EP
, LY
MA
deno
aG
33.
3m
mol
/l6
ng/l
36.7
pg/m
l6
mon
ths;
DO
DP
etre
lli14
1996
F/3
7C
olon
HE
P, L
YM
As
ND
ND
ND
ND
ND
; DO
DSe
kine
1519
98M
/47
Col
onN
DN
DN
D16
.0m
g/dl
ND
ND
ND
; ND
Lor
thol
ary16
1999
F/5
4C
olon
HE
P, L
YM
Ade
noa
G3
3.75
mm
ol/l
1ng
/l18
pmol
/l5
wee
ks; D
OD
Lor
thol
ary16
1999
M/6
3R
ectu
mH
EP
, PU
L, L
YM
, SK
IA
deno
G1
4.27
mm
ol/l
12.7
ng/l
9.3
pmol
/l7
wee
ks; D
OD
Tho
mps
on17
2001
F/7
6C
olon
HE
P, L
YM
, SK
IA
sG
413
.6m
g/dl
6pg
/ml
25.7
pmol
/l10
mon
ths;
AW
DL
uh18
2002
M/4
2C
olon
HE
P, L
YM
, OSS
, SK
IA
deno
aG
316
.2m
l/dl
31.8
pg/m
l12
.1pm
ol/l
6 m
onth
s; D
OD
Pre
sent
cas
eF
/54
Col
onH
EP
, LY
M, P
UL
Ade
noG
314
.2m
g/dl
<5ng
/l13
.5pm
ol/l
3 w
eeks
; DO
D
PT
H, p
arat
hyro
id h
orm
one;
PT
HrP
, par
athy
roid
hor
mon
e-re
late
d pe
ptid
e; A
deno
, ade
noca
rcin
oma;
As,
ade
nosq
uam
ous
carc
inom
a; G
1, w
ell d
iffe
rent
iate
d; G
3, p
oorl
y di
ffer
enti
ated
; G4,
undi
ffer
enti
ated
; H
EP
, he
pati
c; L
YM
, ly
mph
nod
es;
PU
L,
pulm
onar
y; P
ER
, pe
rito
neum
; A
DR
, ad
rena
ls;
OSS
, os
seou
s; P
LE
, pl
eura
; SK
I, s
kin;
DO
D,
died
of
dise
ase;
AW
D,
aliv
e w
ith
dise
ase;
ND
, not
des
crib
edaT
hese
spe
cim
ens
also
had
neu
roen
docr
ine
feat
ures

695J. Sakata et al.: Humoral Hypercalcemia from Colonic Cancer
when marked hypercalcemia is found in patients withcolorectal carcinoma and distant metastases.
Pamidronate with intravenous saline hydration is thetreatment of choice for HHM.16,18 Our patient’s symp-toms resolved quickly after this treatment. Gurneyet al.10 reported that patients with serum PTHrP levels≥12 pmol/l had a poor response to pamidronate; how-ever, the combination of calcitonin and pamidronatemay be effective for patients with HHM caused by highlevels of PTHrP.15,19
Patients with colorectal malignancies associatedwith HHM have a very poor prognosis (Table 1).Since most tumors have spread beyond the scope ofsurgical resection at the time of diagnosis of HHM,systemic chemotherapy may be the only option forthese tumors; however, no effective chemotherapeuticregimen for colorectal carcinoma presenting with HHMhas been established.5,11,13,18 Further investigation is war-ranted to find an effective treatment regimen for thiscondition.
In conclusion, colorectal carcinoma associated withhumoral hypercalcemia is characterized by a poorlydifferentiated tumor with or without squamous or neu-roendocrine features, distant metastases, and a dismalprognosis. Although rare, this paraneoplastic syndromeshould be considered in patients with a history ofcolorectal carcinoma who present with distant meta-stases and marked hypercalcemia.
References
1. Wysolmerski JJ, Broadus AE. Hypercalcemia of malignancy: thecentral role of parathyroid hormone-related protein. Annu RevMed 1994:45:189–200.
2. Castleman B, Kibbee BU. Case records of the MassachusettsGeneral Hospital: case 63-1963. N Engl J Med 1963:269:801–8.
3. Mozaffarian G. Hypercalcemia associated with malignanciesunexplained by bone metastasis. Case reports and review ofliterature. J Maine Med Assoc 1969;60:205–7.
4. Omenn GS, Roth SI, Baker WH. Hyperparathyroidism associ-ated with malignant tumors of nonparathyroid origin. Cancer1969;24:1004–12.
5. Kubota H, Koyama Y, Hojo K, Shimamura Y, Onishi T, TanakaM, et al. Adenosquamous cell carcinoma of the colon with severehypercalcemia. Report of two cases. Jpn J Clin Oncol 1980;10:311–20.
6. Palvio DH, Sorensen FB, Klove-Mogensen M. Stem cell carci-noma of the colon and rectum. Report of two cases and review ofthe literature. Dis Colon Rectum 1985;28:440–5.
7. Chevinsky AH, Berelowitz M, Hoover HC Jr. Adenosquamouscarcinoma of the colon presenting with hypercalcemia. Cancer1987;60:1111–6.
8. Berkelhammer CH, Baker AL, Block GE, Bostwick DG,Michelassi F. Humoral hypercalcemia complicating adeno-squamous carcinoma of the proximal colon. Dig Dis Sci 1989;34:142–7.
9. March R, Ulin R, Puccio C, Savino J, Arlin Z, Ahmed T, et al.Hypercalcemia associated with adenocarcinoma of the rectum. Acase report and review of the literature. Anticancer Res 1991;11:2029–30.
10. Gurney H, Grill V, Martin TJ. Parathyroid hormone-related pro-tein and response to pamidronate in tumor-induced hypercalce-mia. Lancet 1993;341:1611–3.
11. Links M, Ho H, Clingan P, Diamond T. Hypercalcemia in apatient with fatal adenosquamous carcinoma of the colon. Med JAust 1994;160:286–7.
12. de Souza PL, Friedlander ML. Humoral hypercalcemia associatedwith adenocarcinoma of the rectum. A case report and review ofthe literature. Am J Clin Oncol 1995;18:126–9.
13. Sidler B, Alpert L, Henderson JE, Deckelbaum R, Amizuka N,Silva JE, et al. Amplification of the parathyroid hormone-relatedpeptide gene in a colonic carcinoma. J Clin Endocrinol Metab1996;81:2841–7.
14. Petrelli NJ, Valle AA, Weber TK, Rodriguez-Bigas M.Adenosquamous carcinoma of the colon and rectum. Dis ColonRectum 1996;39:1265–8.
15. Sekine M, Takami H. Combination of calcitonin and pamidronatefor emergency treatment of malignant hypercalcemia. Oncol Rep1998;5:197–9.
16. Lortholary AH, Cadeau SD, Bertrand GM, Guerin-Meyer VI,Gamelin EC, Audran MJ. Humoral hypercalcemia in patientswith colorectal carcinoma: report of two cases and review of theliterature. Cancer 1999;86:2217–21.
17. Thompson JT, Paschold EH, Levine EA. Paraneoplastic hyper-calcemia in a patient with adenosquamous cancer of the colon.Am Surg 2001;67:585–8.
18. Luh JY, Han ES, Simmons JR, Whitehead RP. Poorlydifferentiated colon carcinoma with neuroendocrine featurespresenting with hypercalcemia and cutaneous metastases: casereport and review of the literature. Am J Clin Oncol 2002;25:160–3.
19. Bilezikian JP. Management of acute hypercalcemia. N Engl J Med1992;326:1196–203.