Human milk fortifier: An occult cause of bowel obstruction in extremely premature neonates
3
Human milk fortifier: An occult cause of bowel obstruction in extremely premature neonates Jennifer Stanger a , Kelley Zwicker b , Susan Albersheim b , James J. Murphy III a, ⁎ a Department of Surgery, Division of Pediatric Surgery, BC Children’s Hospital, University of British Columbia, Vancouver, BC, Canada b Department of Pediatrics, BC Children’s Hospital, University of British Columbia, Vancouver, BC, Canada abstract article info Article history: Received 3 February 2014 Accepted 13 February 2014 Key words: Human milk fortifier Neonatal bowel obstruction Lactobezoar Premature infants Background: Human milk fortifier (HMF) is used in neonatal units throughout North America to facilitate growth of preterm infants. Little data is available on the gastrointestinal side effects and potential adverse events. The purpose of this paper was to present a series of infants presenting with bowel obstruction associated with HMF. Methods: Cases of HMF obstruction were collected between January 2010 and December 2012. Charts were reviewed and relevant data was collected. Results: During the study period, 7 premature infants presented with bowel obstruction secondary to intestinal concretions of HMF. All babies were premature with gestational ages from 25 to 27 weeks. Birth weight was less than 1000 grams in all patients. Patients presented with feeding intolerance, bilious aspirates, abdominal distension, and obstipation. Four of the patients presented with acute deterioration and required urgent surgical intervention. Conclusions: HMF is an important source of nutritional support in infants, which is felt to be safe. We present a series of infants where its use has resulted in significant complications. HMF should be used with caution in infants, especially those with a history of necrotizing enterocolitis. Further research should examine the calcium, protein, and fatty acid concentration tolerable in the gastrointestinal tract of infants. © 2014 Elsevier Inc. All rights reserved. Human breast milk is recognized as an advantageous nutrition source for infants. Infants who are breastfed have improved immune and gastrointestinal function and decreased rates of necrotizing enterocolitis compared to infants that receive formu- la [1,2]. However human milk does not provide sufficient protein, sodium and micronutrients to meet the increased metabolic demands of preterm infants [3]. Several commercially prepared fortifiers have been developed to improve the nutritional content of human milk (human milk fortifier, HMF). In several studies, HMF has been shown to result in improved weight gain [4,5]. However there is insufficient data to conclude that there are no deleterious effects [6]. There have been a few case reports of lactobezoar related to formula ingestion in infants [7,8]. Recently there has been a single case report of calcium stone ileus in a premature infant because of human milk fortifier [9]. The purpose of this paper was to present a series of patients with bowel obstruction following the administration of human milk fortifier. 1. Methods Patients undergoing treatment for bowel obstructions related to human milk fortifier ingestion between January 2010 and December 2012 were identified. All patient charts were reviewed and relevant data was collected. Data collected included demographic (gestational age, birth weight, gender), clinical (presentation, diagnostic variables, radiographic findings), nutritional and pathologic factors. Infants admitted to the Neonatal Intensive Care Unit (NICU) at our institution are started on enteral nutrition as soon as clinically possible. Breast milk (both maternal expressed and donor milk) is the first choice of enteral support. HMF is introduced once feeds are established and there are concerns over adequate growth. Similac Human Milk Fortifier (Abbott Nutrition) was used during the study period. In our institution, HMF is only used in infants who are less than 34 weeks gestation or less than 2500 grams at birth. Once an infant is tolerating breast milk at a rate of 100 mL per kilogram per day, HMF will then be added if growth remains inadequate. Patients are initially started on half-strength HMF (created by adding one package of Similac HMF powder to 50 mL of expressed breast milk (EBM)), and once tolerance has been established patients advance to full strength HMF (two packets per 50 mL of EBM). Each packet provides 1 gram of protein, 14 calories, 117 mg of calcium with a total osmolality of 11.2 mOsm [10]. Full strength HMF fortification provides 24 kcal per Journal of Pediatric Surgery 49 (2014) 724–726 ⁎ Corresponding author at: Division of Pediatric Surgery, BCCH, K0-110 ACB, 4480 Oak Street, Vancouver, BC, Canada V6J 4K7. Tel.: +1 604 875 2810; fax: +1 604 875 2721. E-mail address: [email protected] (J.J. Murphy). http://dx.doi.org/10.1016/j.jpedsurg.2014.02.054 0022-3468/© 2014 Elsevier Inc. All rights reserved. Contents lists available at ScienceDirect Journal of Pediatric Surgery journal homepage: www.elsevier.com/locate/jpedsurg
Transcript of Human milk fortifier: An occult cause of bowel obstruction in extremely premature neonates

Journal of Pediatric Surgery 49 (2014) 724–726
Contents lists available at ScienceDirect
Journal of Pediatric Surgery
j ourna l homepage: www.e lsev ie r .com/ locate / jpedsurg
Humanmilk fortifier: An occult cause of bowel obstruction in extremely
premature neonatesJennifer Stanger a, Kelley Zwicker b, Susan Albersheim b, James J. Murphy III a,⁎a Department of Surgery, Division of Pediatric Surgery, BC Children’s Hospital, University of British Columbia, Vancouver, BC, Canadab Department of Pediatrics, BC Children’s Hospital, University of British Columbia, Vancouver, BC, Canada
a b s t r a c ta r t i c l e i n f o
⁎ Corresponding author at: Division of Pediatric SurgerStreet, Vancouver, BC, Canada V6J 4K7. Tel.: +1 604 875
E-mail address: [email protected] (J.J. Murphy).
http://dx.doi.org/10.1016/j.jpedsurg.2014.02.0540022-3468/© 2014 Elsevier Inc. All rights reserved.
Article history:
Received 3 February 2014Accepted 13 February 2014Key words:Human milk fortifierNeonatal bowel obstructionLactobezoarPremature infants
Background: Human milk fortifier (HMF) is used in neonatal units throughout North America to facilitategrowth of preterm infants. Little data is available on the gastrointestinal side effects and potential adverseevents. The purpose of this paper was to present a series of infants presenting with bowel obstructionassociated with HMF.Methods: Cases of HMF obstruction were collected between January 2010 and December 2012. Charts werereviewed and relevant data was collected.Results: During the study period, 7 premature infants presented with bowel obstruction secondary tointestinal concretions of HMF. All babies were premature with gestational ages from 25 to 27 weeks. Birth
weight was less than 1000 grams in all patients. Patients presented with feeding intolerance, bilious aspirates,abdominal distension, and obstipation. Four of the patients presented with acute deterioration and requiredurgent surgical intervention.Conclusions: HMF is an important source of nutritional support in infants, which is felt to be safe. We present aseries of infants where its use has resulted in significant complications. HMF should be used with caution ininfants, especially those with a history of necrotizing enterocolitis. Further research should examine thecalcium, protein, and fatty acid concentration tolerable in the gastrointestinal tract of infants.© 2014 Elsevier Inc. All rights reserved.
Human breast milk is recognized as an advantageous nutritionsource for infants. Infants who are breastfed have improvedimmune and gastrointestinal function and decreased rates ofnecrotizing enterocolitis compared to infants that receive formu-la [1,2]. However human milk does not provide sufficient protein,sodium and micronutrients to meet the increased metabolicdemands of preterm infants [3]. Several commercially preparedfortifiers have been developed to improve the nutritional content ofhuman milk (human milk fortifier, HMF). In several studies, HMFhas been shown to result in improved weight gain [4,5]. Howeverthere is insufficient data to conclude that there are no deleteriouseffects [6].
There have been a few case reports of lactobezoar related toformula ingestion in infants [7,8]. Recently there has been a singlecase report of calcium stone ileus in a premature infant because ofhuman milk fortifier [9]. The purpose of this paper was to present aseries of patients with bowel obstruction following the administrationof human milk fortifier.
y, BCCH, K0-110 ACB, 4480 Oak2810; fax: +1 604 875 2721.
1. Methods
Patients undergoing treatment for bowel obstructions related tohuman milk fortifier ingestion between January 2010 and December2012 were identified. All patient charts were reviewed and relevantdata was collected. Data collected included demographic (gestationalage, birth weight, gender), clinical (presentation, diagnostic variables,radiographic findings), nutritional and pathologic factors.
Infants admitted to the Neonatal Intensive Care Unit (NICU) at ourinstitution are started on enteral nutrition as soon as clinicallypossible. Breast milk (both maternal expressed and donor milk) is thefirst choice of enteral support. HMF is introduced once feeds areestablished and there are concerns over adequate growth. SimilacHuman Milk Fortifier (Abbott Nutrition) was used during the studyperiod. In our institution, HMF is only used in infantswho are less than34 weeks gestation or less than 2500 grams at birth. Once an infant istolerating breast milk at a rate of 100 mL per kilogram per day, HMFwill then be added if growth remains inadequate. Patients are initiallystarted on half-strength HMF (created by adding one package ofSimilac HMF powder to 50 mL of expressed breast milk (EBM)), andonce tolerance has been established patients advance to full strengthHMF (two packets per 50 mL of EBM). Each packet provides 1 gram ofprotein, 14 calories, 117 mg of calcium with a total osmolality of11.2 mOsm [10]. Full strength HMF fortification provides 24 kcal per

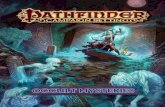
Fig. 1. Photo of intraoperative findings of HMF obstruction.
725J. Stanger et al. / Journal of Pediatric Surgery 49 (2014) 724–726
ounce of milk. Patients will be given a maximum of 20 packets of HMFper day. The protocol for preparing HMF breast milk at our institutionrequires that HMF be added to milk that is at room temperature, thatprepared HMF is remixed prior to each feeding and that HMF fortifiedmilk is not kept for longer than 24 hours.
2. Results
During the three year study period 8 premature infants wereidentified with HMF obstruction. One infant was initially treated at anoutside institution and because of insufficient medical records wasexcluded from the current study. There were 7 males and 1 female.The median gestational age was 25 weeks plus 1 day and the meanbirth weight was 743 grams (Table 1). Owing to the extremeprematurity of the cohort the patients had significant comorbiditiesincluding bronchopulmonary dysplasia (BPD), patent ductus arter-iosus (PDA) and intraventricular hemorrhage (IVH).
Four of the 7 infants in the study had a documented history ofnecrotizing enterocolitis (NEC), all of which had been managednonoperatively. These patients presented with the bowel obstructionat a mean of 27 days (range 18–34 days) after the initial episodeof NEC. All of these patients had tolerated feeds of more than100 mL/kg prior to the development of the obstructive symptoms.Of the remaining three patients, two had no previous gastrointes-tinal issues prior to development of the obstructive symptoms. Theremaining patient (case 6) had a history of early feeding intoleranceand delayed passage of meconium. Subsequent work up, includingcystic fibrosis screening and suction rectal biopsy (performed whenthe patient was 39 weeks corrected gestational age), was negative.The average time to onset of obstruction was at 34 days of life, withall infants having had a delay in the establishment of enteralnutrition. The patients received greater than 5 days of HMFexposure, with the average duration of HMF ingestion prior tosymptoms being 9.1 days.
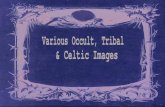
Patients typically presented with obstructive type symptoms,including new onset feeding intolerance, abdominal distension,bilious nasogastric (NG) aspirations and decreased stooling. Four ofthe patients (cases 1, 3, 5, 7) presented with sudden deterioration inaddition to the obstructive symptoms and underwent emergentoperative intervention. In all 4 patients a perforation was found withevidence of inspissated milk (Fig. 1). Two of these patientsdeteriorated and ultimately passed away. Of the three patientspresenting nonacutely, two underwent contrast enema whichshowed evidence of small bowel obstruction with filling defectsbecause of milk/HMF concretions. One patient resolved theirobstruction without surgery with N-acetylcysteine instilled via theNG tube and cessation of HMF. The other patient had three contrastenemas each of which returned a large volume of HMF concretions.Despite N-acetylcysteine via the NG and repeated enemas theobstruction never resolved and operative intervention was required.The final patient presented with obstructive symptoms and anabdominal radiograph (Fig. 2) that showed obstruction after anepisode of NEC and was presumed to have a stricture. Electiveoperative intervention was planned and at the OR the patient wasfound to have inspissated HMF concretions. Two of the 7 patients
Table 1Patients with bowel obstruction because of human milk fortifier ingestion.
Case Gender GA (weeks) BW (gm) Comorbidity NEC Start of SBO (DOL) Type of nutrition Days of HMF Management Outcome
1 Male 25 675 BPD, PDA No 36 EBM 9 Laparotomy, ileostomy Alive2 Male 25 + 5 910 BPD, anemia Yes 53 EBM 7 Laparotomy, decompression Alive3 Male 25 + 5 978 PDA Yes 45 EBM 11 Laparotomy, ileostomy Died4 Male 25 505 Ischemic limb, BPD, No 26 EBM 10 Mucomyst Alive5 Male 25 + 1 570 IVH, PDA Yes 28 EBM 7 Laparotomy, ileostomy Died6 Female 26 + 4 855 BPD, PDA No 29 EBM 11 Laparotomy, ileostomy Alive7 Male 25 + 1 711 PDA, IVH, BPD Yes 21 EBM n/a Laparotomy, ileostomy Alive
passed away. The surviving patients went on to have their stoma’sclosed and achieved enteral autonomy.
During the study period 1896 patients were admitted to our NICU,of which 451 received HMF. Of the 451 patients, 7 developed bowelobstructions involving HMF concretions, resulting in an incidence rateof 0.02%. During the same time period there were 30 confirmed casesof necrotizing enterocolitis. Of the patients with NEC, 17 receivedHMF, with 4 developing complications related to the HMF resulting inan incidence of 23% among this sub group of patients.
3. Discussion
Lactobezoar refers to a coagulum of milk curds in the stomach orthe small bowel, causing intestinal obstruction. Many of the reportedcases have occurred in low birth weight and preterm infants whoreceived high-caloric density formulas rich in casein and calcium[7,8,11]. Rarely does this occur in infants who receive breast milk. Inthe past three years, we have treated 7 infants with obstructionsecondary to lactobezoar from concretions of breast milk with addedhuman milk fortifier.
While human milk remains the preferred form of nutrition forinfants, those who are extremely premature and/or small forgestational age require more calories and macronutrients than canbe provided by breast milk [3]. Consequently, humanmilk fortifier hasbeen developed to provide added calories, protein andmicronutrientsincluding calcium. HMF has been widely adopted in NICUs acrossNorth America. The studies supporting HMF have shown that itpromotes improved growth in premature infants and does not resultin increased rates of NEC or sepsis [1,2]. A recent Cochrane reviewconcluded that while HMF did result in short term improvements inweight gain, there was no evidence to support long term benefits fromits use and insufficient evidence to be reassured that there were nodeleterious effects [6].
We describe 7 patients who present with bowel obstructionsecondary to HMF bezoar. All but one of the patients required operativeintervention to relieve the obstruction and two of the patients died as

Fig. 2. Abdominal x-ray of patient with HMF obstruction.
726 J. Stanger et al. / Journal of Pediatric Surgery 49 (2014) 724–726
a complication of the obstruction and its management. There had beenan antecedent history of NEC in 4 patients. Those patients that did nothave NEC appeared to have a more indolent course; one was able tobe successfully managed without surgery. Those patients that sur-vived went on to successful stoma closure and the resumption of fullenteral feeding.
The cause of bezoars in premature infants is unknown, but is likelyrelated to factors of gastrointestinal immaturity and function as wellas feeding regimens. It has been suggested that precipitation of fattyacids and calcium may be responsible [11]. To date, there have beentwo other single patient case reports of HMF obstruction [9,11]. In thecase reported by Murase et al., the impacted material was analyzedand found to be fatty acid calcium stones. Human milk fortifier mayalter the solubility of calcium contributing to the formation ofconcretions [12]. In all reported cases the infants were prematureand had low birth weight (all less than 1000 grams) suggesting thatthis patient population may be more prone to inspissation. Conse-quences of HMF bezoar in this population can be especially harmful. Inour series two patients died and the patient reported by Murase et al.also died as a consequence of the obstruction.
While the presentation of the patients in our study is significant,our study does represent the limitations of a retrospective case series.
Given the complicated and multifactorial etiology of bowel obstruc-tion in premature infants it is impossible to determine if HMF was thecausative agent in our population. It is possible that among thepatients with NEC the presence of a stricture confounded theirpresentation. However all patients in the study demonstratedtolerance of enteral nutrition prior to introduction of HMF and thepresentation of bowel obstruction, suggesting that the addition ofHMF was a potential factor contributing to bowel obstruction.Chemical analysis was not able to be completed on the concretionsfound in the patients in this study. It is unknown if there is aconcentration of nutritional components (especially calcium andprotein), osmolality or pH that results in the formation of concretionsof HMF in the neonatal gastrointestinal tract. This is an area for furtherresearch. Finally the infants in our study only received a single type ofpowdered HMF. To date we have not encountered patients withbowel obstructions when liquid HMF is utilized, suggesting that itmay be a safer alternative in high risk patients.
Human milk fortifier is an important source of nutritional supportto promote growth in premature infants. While it is largely felt to besafe we present a series of infants where its use has resulted ininfrequent but significant harm. Human milk fortifier should be usedwith caution in premature and small infants. Further research isrequired to determine the ideal calcium, protein and fatty acidconcentration tolerable in the gastrointestinal tract of prematureinfants, and the ideal modality and preparation of supplementalfortifiers. HMF should be avoided in infants with a history ofnecrotizing enterocolitis, until an associated stricture has beenexcluded.
References
[1] Sullivan S, Schanler R, Kim JH, et al. An exclusively human milk-based diet isassociated with a lower rate of necrotizing enterocolitis than a diet of human milkand bovine milk-based products. J Pediatr 2010;156:562–7.
[2] Lucas A, Cole TJ. Breast milk and neonatal necrotizing enterocolitis. Lancet1990;336:1519–23.
[3] Schanler RJ. The use of human milk for premature infants. Pediatr Clin North Am2001;48:207–19.
[4] Reis BB, Hall RT, Schanler RJ, et al. Enhanced growth of preterm infants fed a newpowdered human milk fortifier: a randomized controlled trial. Pediatrics2000;106:581–8.
[5] Berseth CL, Van Aerde JE, Gross S, et al. Growth, efficacy and safety of feeding aniron-fortified human milk fortifier. Pediatrics 2004;114:e699–706.
[6] Kuschel CA, Harding JE. Multicomponent fortified human milk for promotinggrowth in preterm infants. Cochrane Database Syst Rev 2004(1). http://dx.doi.org/10.1002/14651858.CD000343.pub2 [Art No.: CD000343].
[7] Reddy ER, Joseph S. Lactobezoar in a low-birth-weight neonate. Can Med Assoc J1985;133:297.
[8] Lowichik A, Matlak M, Nuttall K, et al. Intestinal lactobezoars in twins receivingreconstituted elemental formula. J Pediatr Gastroenterol Nutr 1999;28:104–7.
[9] MuraseM, Miyazawa T, Taki M, et al. Development of fatty acid calcium stone ileusafter initiation of human milk fortifier. Pediatr Int 2013:114–6.
[10] Abbott Nutrition. http://abbottnutrition.com/brands/products/similac-human-milk-fortifier. Accessed June 25, 2013.
[11] Flikweert ER, La Hei ER, De Rijke YB, et al. Return of the milk curd syndrome.Pediatr Surg Int 2003;19:628–31.
[12] Fogleman AD, Cohen RS, Sakamoto P, et al. Effect of added calcium, phosphorus,and infant formula on calcium and phosphorus dialyzability in preterm donorhuman milk. JPGN 2012;55:390–7.