Human Immunodeficiency Virus: An Overview Elizabeth W. Delamater, Ph.D. Manager, Microbiological...
71
Human Immunodeficiency Virus: An Overview Elizabeth W. Delamater, Ph.D. Manager, Microbiological Sciences Division Laboratory Services Section Texas Department of State Health Services
-
Upload
suzan-cecily-jones -
Category
Documents
-
view
217 -
download
3
Transcript of Human Immunodeficiency Virus: An Overview Elizabeth W. Delamater, Ph.D. Manager, Microbiological...

Human Immunodeficiency Virus: An Overview
Elizabeth W. Delamater, Ph.D.
Manager, Microbiological Sciences Division
Laboratory Services Section
Texas Department of State Health Services

Common Ancestor
(STLV-I)
HTLV-I
HTLV-II
HIV-1
HIV-2
(SIV)
Transforming Viruses
Cell Proliferation
Cytopathic Viruses
Cell Death

Human Retroviruses - Nomenclature
Human Immunodeficiency Viruses¤ HIV-1 (1983)
• HIV, HTLV III, LAV, ARV– AIDS and related conditions
¤ HIV-2 (1986)• LAV-2, HTLV IV
– AIDS (primarily in West Africa)

Human Retrovirus – Characteristics
RNA Tumor (transforming) and immunodeficiency (cytopathic) viruses
Reverse Transcriptase Integration of the viral genome into the host
DNA as a provirus Primarily infect T-lymphocytes and some
neural cells Exogenous (transmisssible, infectious agents) Latency (long incubation period)

Brief History of Retroviruses
Transmissible agents capable of causing leukemias and solid-tissue tumors were discovered¤ 1970 – Reverse transcriptase was discovered¤ 1980 – HTLV-I and HTLV-II were isolated¤ 1981 – First AIDS case was discovered¤ 1983 – HIV-1 was isolated¤ 1985 – EIA test for anti-HIV-1 antibodies was
licensed by the FDA

Where did HIV come from?
• Estimated origin around 1930.• Estimated origin in Africa.• Thought to come from SIV in
primates (blood exposure)• Change in travel and social norms
caused the world wide epidemic.




HIV Subtypes
HIV isolates are classified into three different groups¤ Major group (M)¤ Outlier group (O)¤ Non-M / non-O (N)
Groups N and O restricted to West Africa Based on the analysis of the envelope gene,
there are at least nine pure subtypes or clades A-D, F-H, J and K



HIV Transmission
Requires:
1) Infected body fluid.
2) Entry into the body.
Blood, Semen, Vaginal Secretions & Breast Milk
Mucous Membrane--Anal, Oral or Vaginal Sex
Blood to Blood--Needle or Broken Skin
Perinatal- In utero, During birth, Breastfeeding
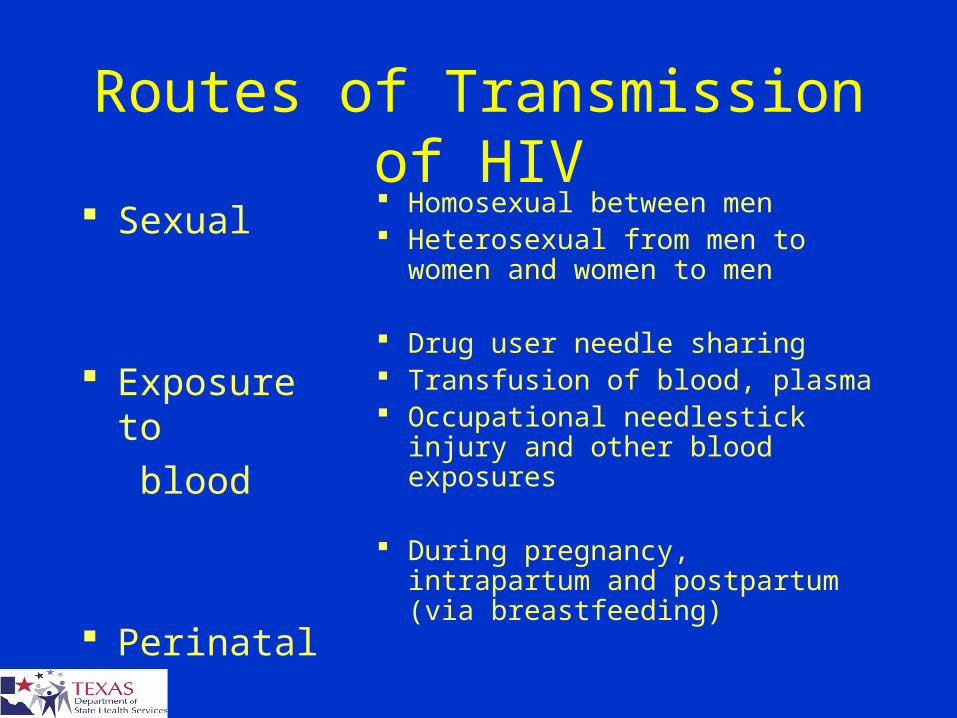
Routes of Transmission of HIV Sexual
Exposure to
blood
Perinatal
Homosexual between men Heterosexual from men to
women and women to men
Drug user needle sharing Transfusion of blood, plasma Occupational needlestick injury
and other blood exposures
During pregnancy, intrapartum and postpartum (via breastfeeding)

Perinatal transmission
Greatly reduced due to use of antiretroviral therapy during pregnancy¤ decrease from 24 to 8% vertical transmission with
AZT
Trials using high doses of new antiretrovirals during labor and to newborn--success of Nevirapine
Women with higher viral loads more likely to transmit

Factors Affecting Transmission
STD Co-infectionMore likely to become
infectedMore likely to transmit
infection
Viral Load Stage of infectionTreatment

Disease Progression
Infection
Primary Infection/Antibody Development
Asymptomatic Period (10-12 yrs average)
AIDS (Opportunistic infections, CD4 200 or below)

AIDS
AIDS Defining IllnessesPnuemocystis pnuemonia
ToxoplasmosisKaposi’s sarcoma
Mycobacterium avium complexInvasive cervical cancer
etc...
HIV infected + immune system breakdown
(CD4 count < 200 or AIDS Defining illness)

Antiretroviral Treatment
Triple Drug Cocktail--Attack the virus at different points in the replication process•Difficult Drug Regimens
•Importance of Adherence•Side Effects•Expensive


Other Treatment
Prophylaxis for Opportunistic Infections
Treatment of Opportunistic Infections
Vaccines (future)
Alternative Treatment
Immune Therapy

Difficulties in Treatment
Access to Care Family Care Burdens Language Barriers Fragmentation of Care Fears / Myths About Medical Care

Post Exposure Prophylaxis
Treatment with antiretroviral drugs after an exposure to HIV.
Must be started within 72 hours (sooner the better) and continued for a month.
PEP showed a 80% reduction in HIV infections for occupational exposures.
Concerns for drug and sexual exposures

Estimated Number of AIDS Cases, Deaths, and Persons Living with AIDS,1985-2004, United States
Note. Data adjusted for reporting delays.
No.
of c
ases
and
dea
ths
(in th
ousa
nds)
Year of diagnosis or death
Prevalence (in thousands)
0 0
90400
450
10
20
50
30
100
40150
50
200
60
250
70
300
80350
19851986198719881989199019911992199319941995199619971998199920002001200220032004
DeathsPrevalence
AIDS 1993 definitionimplementation

Number HIV infected 1,039,000 – 1,185,000
Number unaware of their HIV infection 252,000 - 312,000 (24%-27%)
Estimated new infections 40,000 annually
Awareness of HIV Status among Persons with HIV, United States
Glynn M, Rhodes P. 2005 HIV Prevention Conference

Awareness of Serostatus Among People with HIV and Estimates of Transmission
~25% Unaware
of Infection
~75% Aware of Infection
People Living with HIV/AIDS: 1,039,000-1,185,000
New Sexual Infections Each Year: ~32,000
Accounting for: ~54% of New
Infections
~46% of New
Infections
Marks, et alAIDS 2006;20:1447-50

HIV/AIDS Diagnoses among Adults and Adolescents, by Transmission Category — 33 States, 2001–2004
MSM61%IDU
16%
Heterosexual17%
MSM/IDU 5% Other 1%
Males(n ≈ 112,000)
Females(n ≈ 45,000)
Heterosexual76%
IDU21%
Other 3%
MMWR, Nov 18, 2005



USA
Numbers of AIDS deaths are falling Number of AIDS diagnosis are falling Rates of HIV infection have NOT changed Trends
¤ Younger People (25% under age 25)¤ Low Socioeconomic Status ¤ IDU¤ Disease of the Marginalized

Knowing You Are Infected:
Primary Infection• 2-6 wks average• 75 -90% have symptoms
Only way to know for sure: HIV Antibody Test
“Window Period”: time to develop antibodies• 3-6 weeks 85% • 3 months >99%

Testing Technology
Technologies More accurate
serum EIA Oral fluids test Home test system Rapid test Urine test
Strategies Phone results Augmented
counseling Outreach
¤ Bars, coffee shops, bath houses
¤ Syringe exchanges¤ Street (vans)

TDH HIV-1 Testing AlgorithmPatient Specimen – EIA Screen
Nonreactive Reactive
No further
Testing
Report as
Nonreactive
Repeat screen 2X
Reactive 2XReactive
Nonreactive
Nonreactive 2X
Western Blot Confirmation No further
Testing
Report as
Nonreactive
Reactive NonreactiveIndeterminate
Report Reactive
Retest
8 weeks
Report Nonreactive

HIV Screening
Enzyme Immunoassay
EIA or ELISA

EIA or ELISAAdvantages
Simple Sensitive Rapid Can be Automated Suitable for High Volume Testing

EIA or ELISALimitations
Potential for False Positives Initial High Reactives must be Repeated

Types of Specimens for Testing
Serum or Plasma

Plate with Antigen coated wells Add patient serum sample containing anti-HIV-1 antibodies
Wash, add enzyme conjugated anti-human antibodies

Wash, add appropriate substrate for the conjugated enzyme
Enzyme acts on substrate, causing a color change









Types of Specimens for Testing
Serum or Plasma
Dried Blood Spots


Types of Specimens for Testing
Serum or Plasma
Dried Blood Spots
Oral Fluid

Types of Specimens for Testing
Serum or Plasma
Dried Blood Spots
Oral Fluid
Urine

HIV Confirmation
Western Blot
Immunofluorescent Assay
Laboratory Only

gp160
gp120
p66
gp41
p24
p17


What about HIV-2?
Not common in the United States
Only about 72 cases confirmed as of 2000

gp160gp120
gp41
HIV-2 confirmed by the CDC
HIV Rapid Tests

Public Health Need for Rapid HIV Tests
High rates of non-return for test results¤ In 2000, 31% did not return for results of
HIV-positive conventional tests at publicly funded sites
Need for immediate information or referral for treatment choices¤ Perinatal settings¤ Post-exposure treatment settings
Screening in high-volume, high-prevalence settings

Uni-Gold Recombigen
Multispot HIV-1/HIV-2
Reveal G2 OraQuick
Advance

Four FDA-approved Rapid HIV Tests
99.7 (99.0 – 100)
99.8 (99.3 – 100)
100 (99.5 – 100)
100 (99.5 – 100)
Uni-Gold Recombigen
- whole blood
- serum/plasma
100 (99.7-100)
99.8 (99.6 – 99.9)
99.9 (99.6 – 99.9)
99.6 (98.5 - 99.9)
99.3 (98.4 - 99.7)
99.6 (98.5 - 99.9)
OraQuick Advance
- whole blood
- oral fluid
- plasma
Specificity
(95% C.I.)
Sensitivity
(95% C.I.)

Four FDA-approved Rapid HIV Tests
99.9 (99.8 – 100)100 (99.9 – 100)
100 (99.7 – 100)
Multispot
serum/plasma
HIV-2
99.1 (98.8 – 99.4)
98.6 (98.4 – 98.8)
99.8(99.2 – 100)
99.8(99.0 – 100)
Reveal G2
serum
plasma
Specificity
(95% C.I.)
Sensitivity
(95% C.I.)

Revised RecommendationsAdults and Adolescents - I
Routine, voluntary HIV screening for all persons 13-64 in health care settings, not based on risk
Repeat HIV screening of persons with known risk at least annually
Opt-out HIV screening with the opportunity to ask questions and the option to decline
Include HIV consent with general consent for care; separate signed informed consent not recommended
Prevention counseling in conjunctions with HIV screening in health care settings is not required

Opt-Out Screening
Prenatal HIV testing for pregnant women: RCT of 4 counseling models with opt-in consent:
¤ 35% accepted testing¤ Some women felt accepting an HIV test
indicated high risk behavior
Testing offered as routine, opportunity to decline¤ 88% accepted testing¤ Significantly less anxious about testing
Simpson W, et al, BMJ June,1999

Routine Opt-Out HIV TestingTexas STD Clinics, 1996-97
Texas Department of State Health Services, 2005
Opt-In Opt-Out N (%) N (%) % change
STD Visits 31,558 34,533 +9Eligible Clients 19,184 (61) 23,686 (69) +23Pre-test counsel 15,038 (78) 11,466 (48) -24Tested 14,927 (78) 23,020 (97) +54
Post-test counsel 6,014 (40) 4,406 (19) -27HIV-positive 168 (1.1) 268 (1.2) +59

Revised RecommendationsAdults and Adolescents - II
Intended for all health care settings, including inpatient services, EDs, urgent care clinics, STD clinics, TB clinics, public health clinics, community clinics, substance abuse treatment centers, correctional health facilities, primary care settings
Communicate test results in same manner as other diagnostic/screening tests
Provide clinical HIV care or establish reliable referral to qualified providers

Revised RecommendationsAdults and Adolescents - III
Low prevalence settings:¤ Initiate screening¤ If yield from screening is less than 1 per 1000,
continued screening is not warranted
Steps should be considered to resolve conflicts between the recommendations and state or local regulations

Revised RecommendationsPregnant Women - I
Universal opt-out HIV screening¤ Include HIV in routine panel of prenatal
screening tests¤ Consent for prenatal care includes HIV testing¤ Notification and option to decline
Second test in 3rd trimester for pregnant women:¤ Known to be at risk for HIV¤ In jurisdictions with elevated HIV incidence¤ In high HIV prevalence health care facilities

Revised RecommendationsPregnant Women - II
Opt-out rapid testing with option to decline for women with undocumented HIV status in L&D¤ Initiate ARV prophylaxis on basis of rapid
test result
Rapid testing of newborn recommended if mother’s status unknown at delivery¤ Initiate ARV prophylaxis within 12 hours of
birth on basis of rapid test result
Summary
There is an urgent need to increase the proportion of persons who are aware of their HIV-infection status
Expanded, routine, voluntary, opt-out screening in health care settings is needed
Such screening is cost-effective Recommendations Revised: September 2006 Several jurisdictions have already begun

Key Messages
The large majority of people with HIV continue to be men who have sex with men. People of color are disproportionately represented among new infections
The basic modes of transmission and prevention of HIV have not changed in 20 years
The AIDS epidemic is not over, but there is more hope than ever for those that are infected