
How to Understand and Treat Cancer with Molecular Markers
54
How to Treat Cancer with Molecular Markers How to Treat Cancer with Molecular Markers How to Treat Cancer with Molecular Markers How to Treat Cancer with Molecular Markers Presented by Professor Serge Jurasunas Presented by Professor Serge Jurasunas Presented by Professor Serge Jurasunas Presented by Professor Serge Jurasunas Lisbon, Portugal Lisbon, Portugal Lisbon, Portugal Lisbon, Portugal www.sergejurasunas.com www.sergejurasunas.com www.sergejurasunas.com www.sergejurasunas.com 1
-
Upload
sheldon-stein -
Category
Health & Medicine
-
view
109 -
download
1
Transcript of How to Understand and Treat Cancer with Molecular Markers
How to Treat Cancer with Molecular MarkersHow to Treat Cancer with Molecular MarkersHow to Treat Cancer with Molecular MarkersHow to Treat Cancer with Molecular Markers
Presented by Professor Serge JurasunasPresented by Professor Serge JurasunasPresented by Professor Serge JurasunasPresented by Professor Serge Jurasunas
Lisbon, PortugalLisbon, PortugalLisbon, PortugalLisbon, Portugal
www.sergejurasunas.comwww.sergejurasunas.comwww.sergejurasunas.comwww.sergejurasunas.com
1
1st of a Series on Naturopathic Oncology
How to Understand and Treat
Cancer with Molecular Markers
Presented by:
Serge Jurasunas N.D., M.D. (HOM)
www.sergejurasunas.com
Member of the Society of Integrative Oncology
American Naturopathic Medical Association2
Lecture Overview
→ What is cancer?
→ What metastasis means?
→ The need for new diagnostics
→ P53 Tumor supressor gene
→ Novel approach to cancer with dietary agents
→ Clinical cases
3
1938 American Society for the
Control of Cancer poster
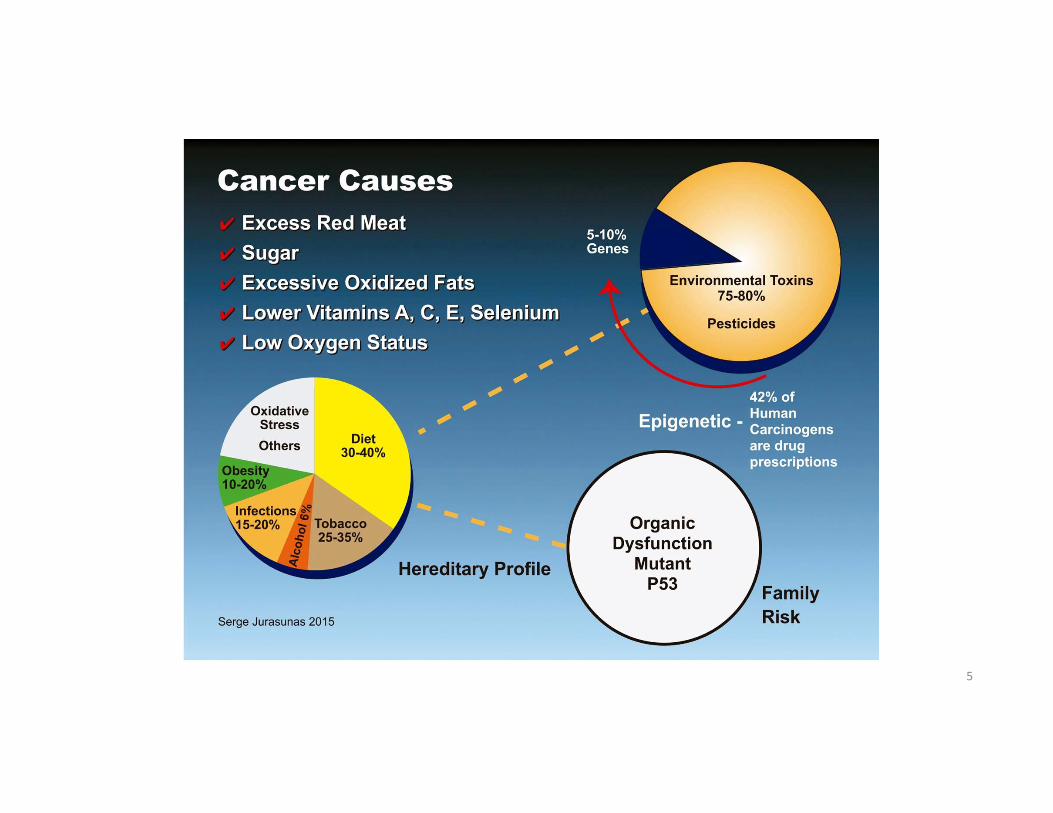
What is Cancer?
What causes cancer?
Why cancer cannot be
cured?
What is the link between
environment, food and
cancer?
How cancer can be
diagnosed?
Can cancer be prevented?
What is the link between
genes and cancer?
4
5
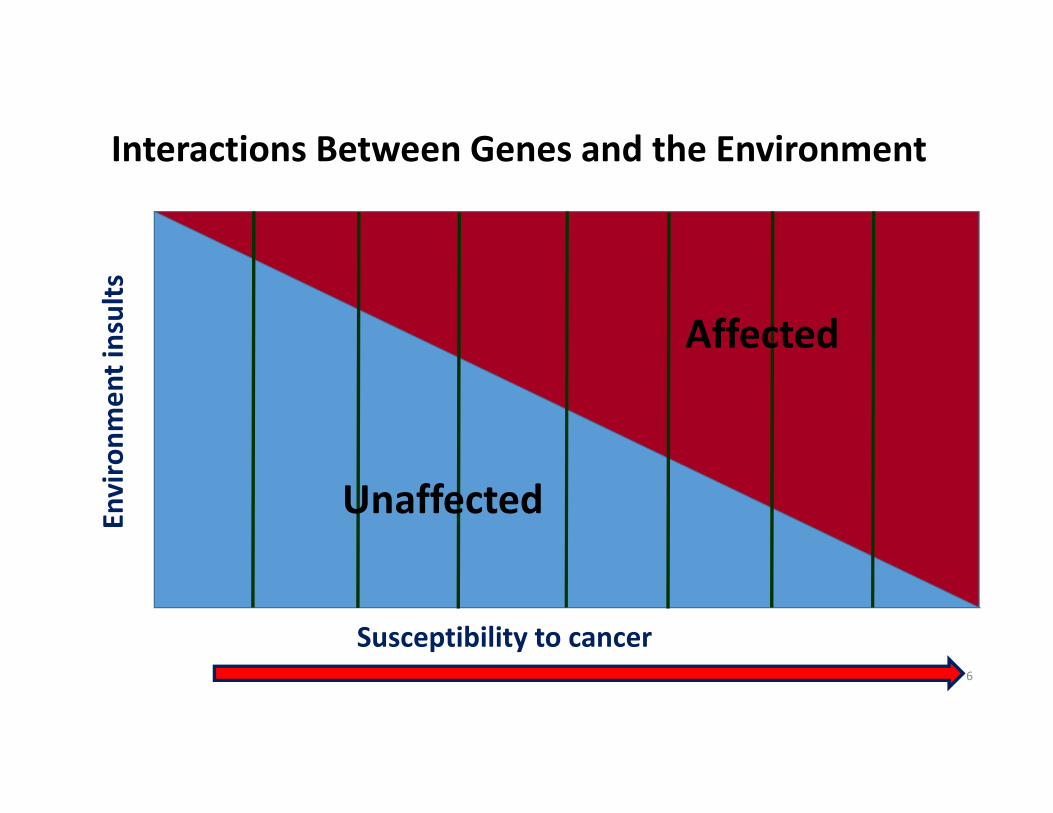
Interactions Between Genes and the Environment
Susceptibility to cancer
En
vir
on
me
nt
insu
lts
Affected
Unaffected
6
Where are We Today with Cancer?
Despite continuing improvement in conventional
diagnosis, local management and some progress in
chemotherapy...
There has been no significant increase in survival
rate over the past 35 years.
Resistance to chemotherapeutic drugs is
considered the greatest obstacle to the successful
management of cancer patients.
Cancer recurrence is still too high.
7
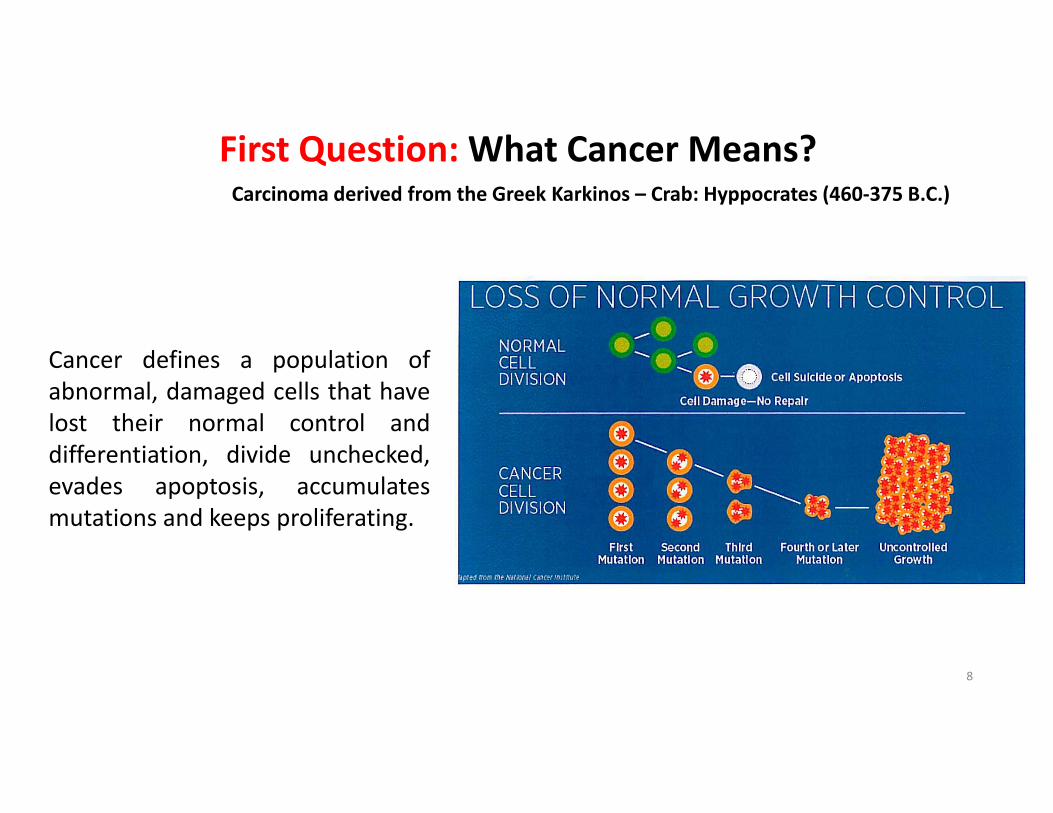
First Question: What Cancer Means?Carcinoma derived from the Greek Karkinos – Crab: Hyppocrates (460-375 B.C.)
Cancer defines a population of
abnormal, damaged cells that have
lost their normal control and
differentiation, divide unchecked,
evades apoptosis, accumulates
mutations and keeps proliferating.
8
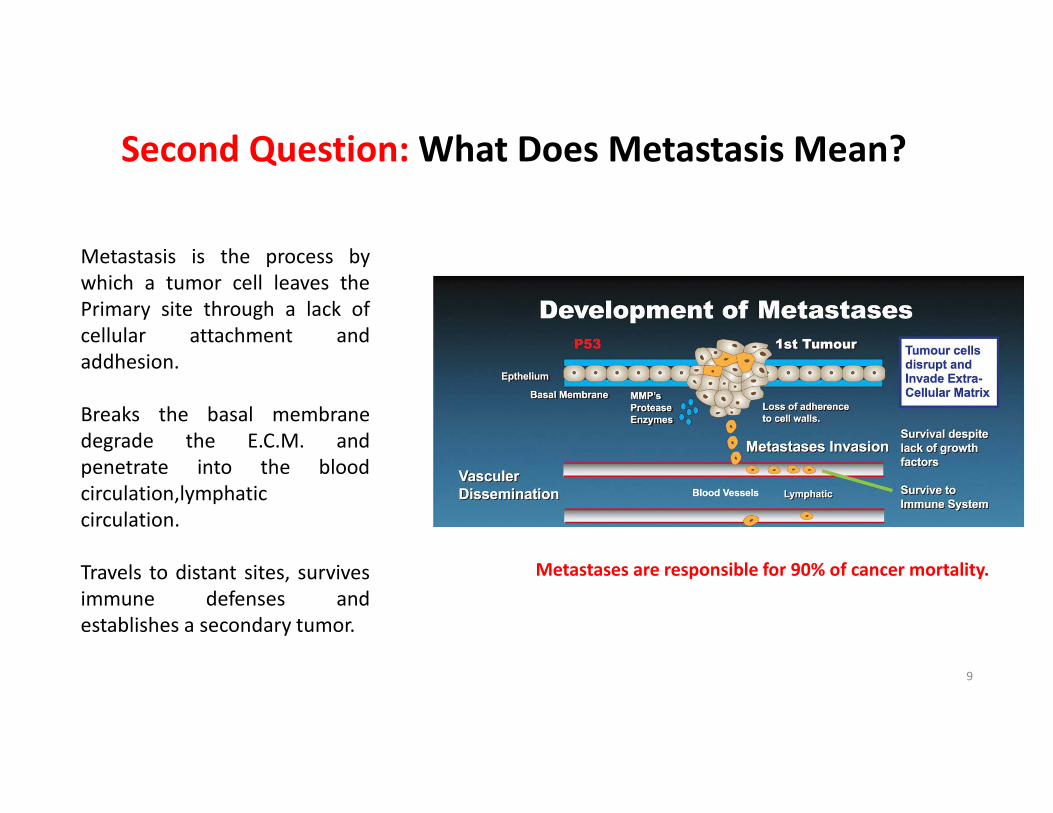
Second Question: What Does Metastasis Mean?
Metastasis is the process by
which a tumor cell leaves the
Primary site through a lack of
cellular attachment and
addhesion.
Breaks the basal membrane
degrade the E.C.M. and
penetrate into the blood
circulation,lymphatic
circulation.
Travels to distant sites, survives
immune defenses and
establishes a secondary tumor.
Metastases are responsible for 90% of cancer mortality.
9
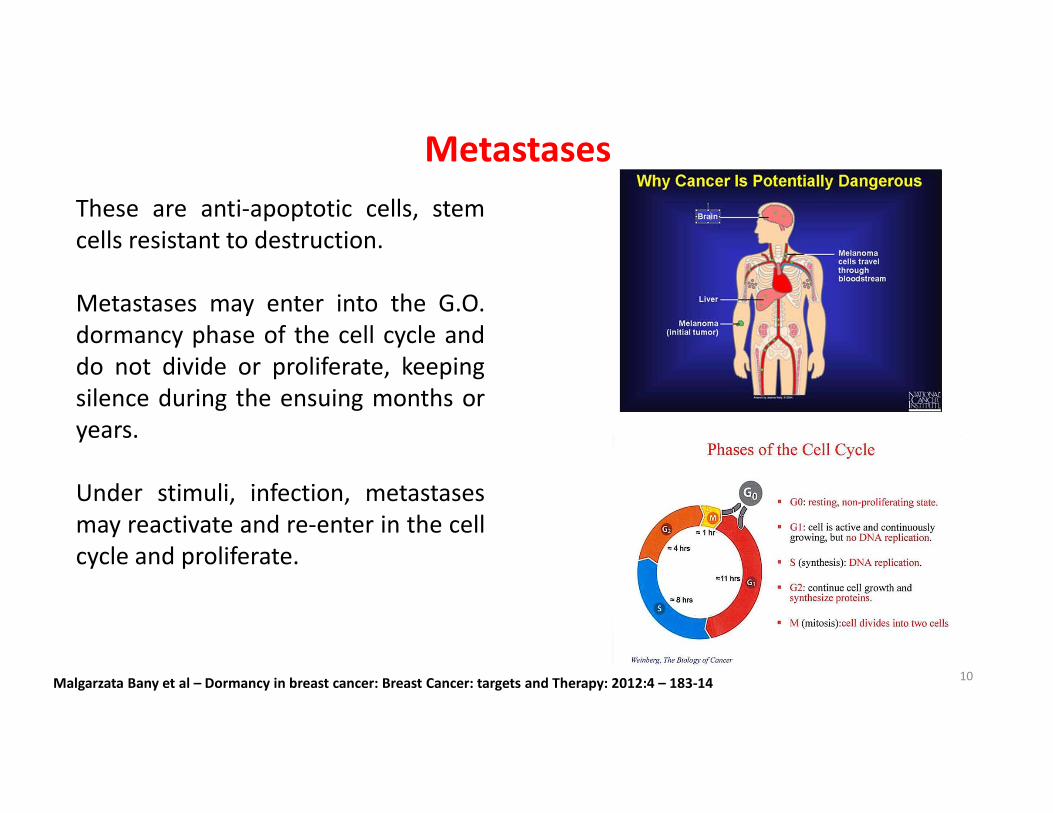
These are anti-apoptotic cells, stem
cells resistant to destruction.
Metastases may enter into the G.O.
dormancy phase of the cell cycle and
do not divide or proliferate, keeping
silence during the ensuing months or
years.
Under stimuli, infection, metastases
may reactivate and re-enter in the cell
cycle and proliferate.
Metastases
Malgarzata Bany et al – Dormancy in breast cancer: Breast Cancer: targets and Therapy: 2012:4 – 183-1410
11
Conventional Diagnostics
1. Inefficient in cancer prevention.
2. Many cancer and pre-malignant forms
go undetected, asymptomatic for
many years .
3. Inefficient to monitor cancer cell
resistance to chemo/radiation.
4. Does not select the best adapted
treatment.
5. Inefficient to predict disease
recurrence.
12
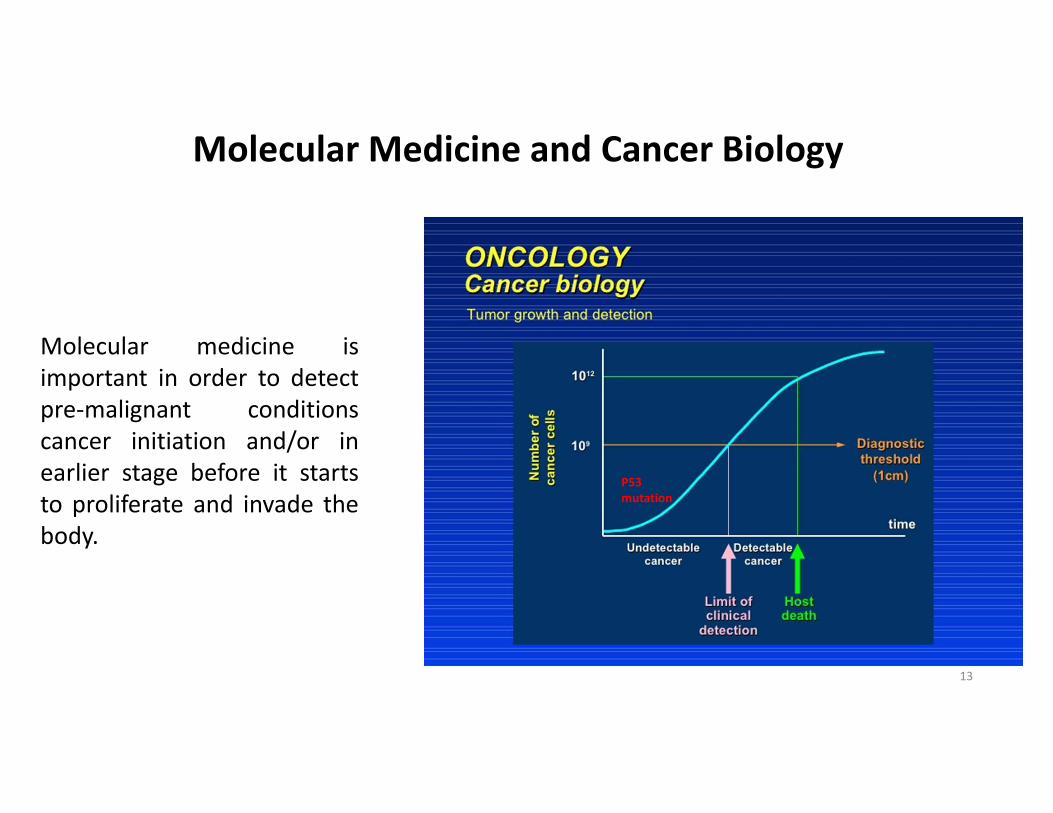
Molecular Medicine and Cancer Biology
Molecular medicine is
important in order to detect
pre-malignant conditions
cancer initiation and/or in
earlier stage before it starts
to proliferate and invade the
body.
P53
mutation
13
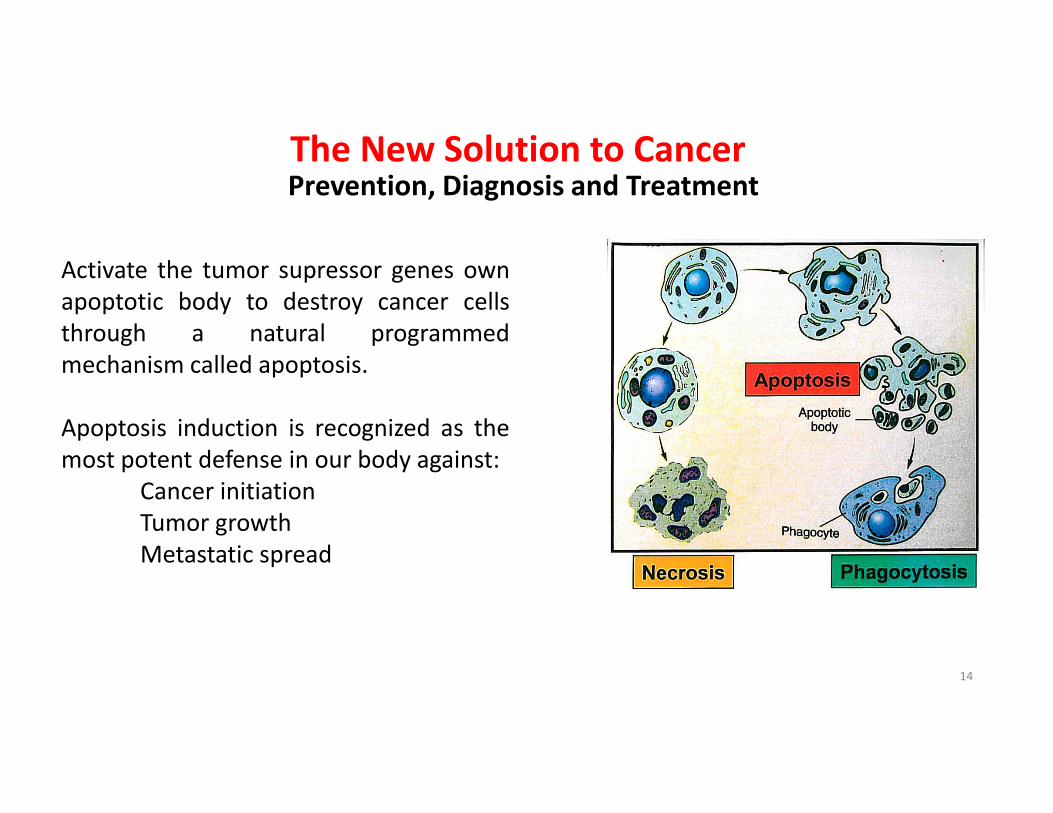
The New Solution to Cancer
Activate the tumor supressor genes own
apoptotic body to destroy cancer cells
through a natural programmed
mechanism called apoptosis.
Apoptosis induction is recognized as the
most potent defense in our body against:
Cancer initiation
Tumor growth
Metastatic spread
Prevention, Diagnosis and Treatment
14
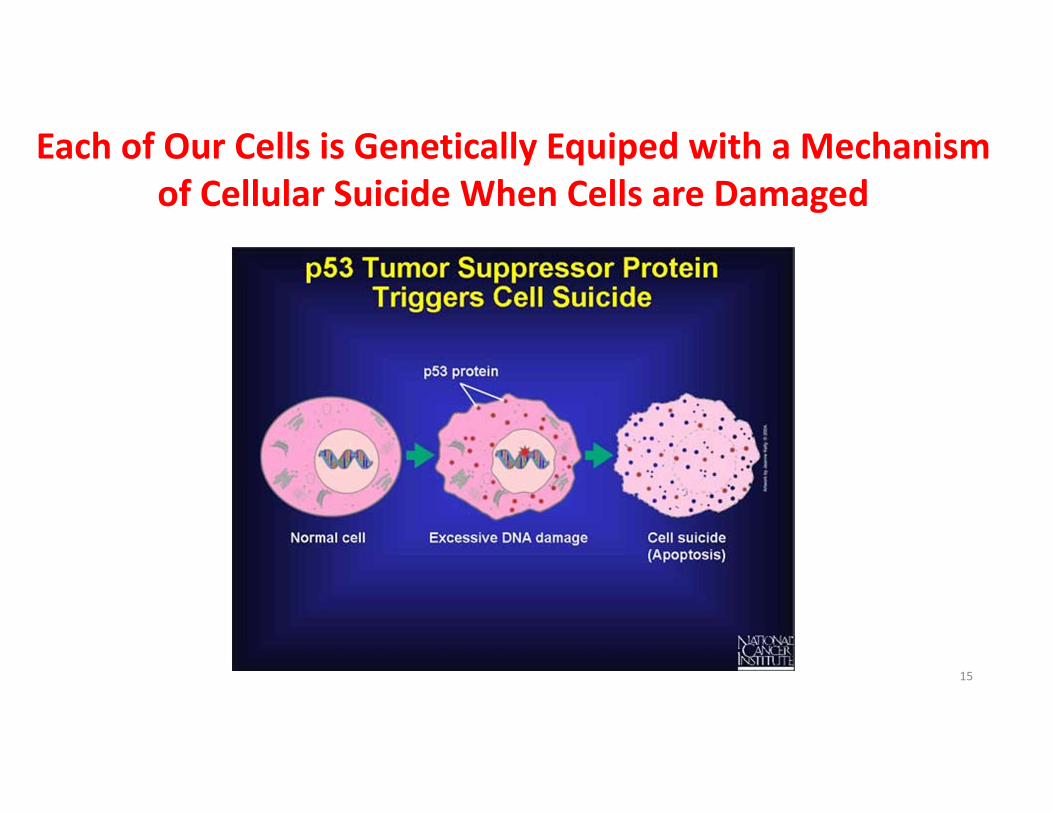
Each of Our Cells is Genetically Equiped with a Mechanism
of Cellular Suicide When Cells are Damaged
15
16
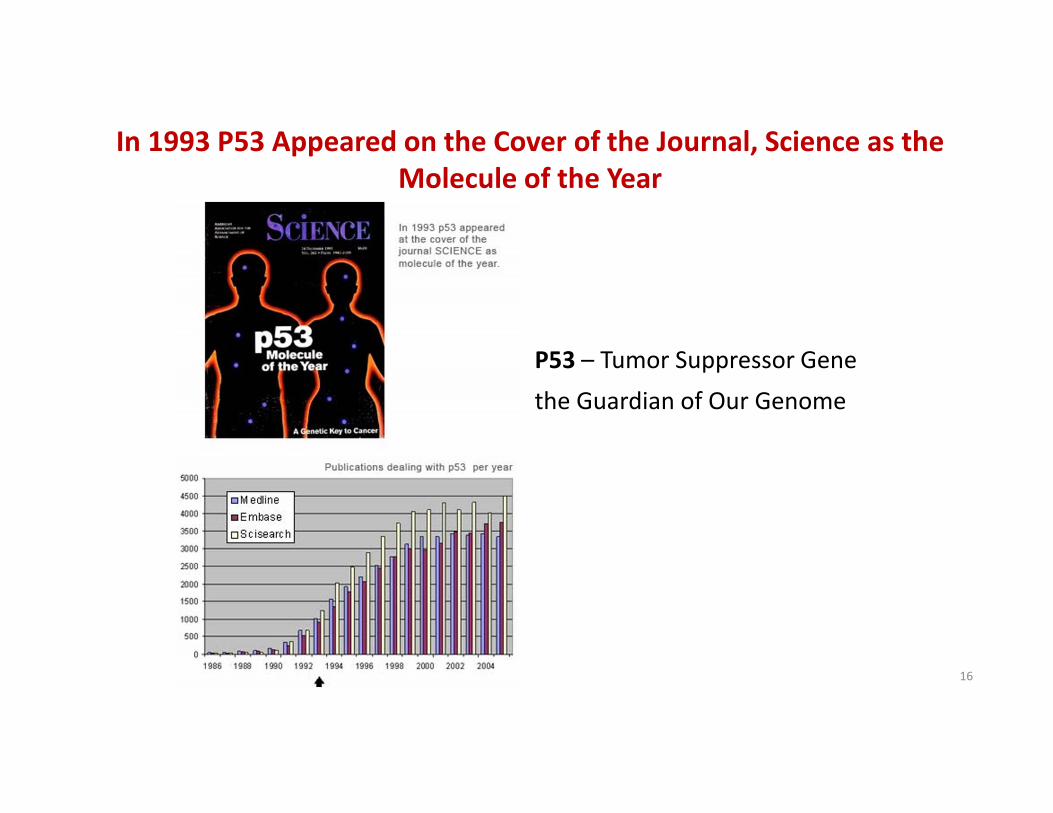
In 1993 P53 Appeared on the Cover of the Journal, Science as the
Molecule of the Year
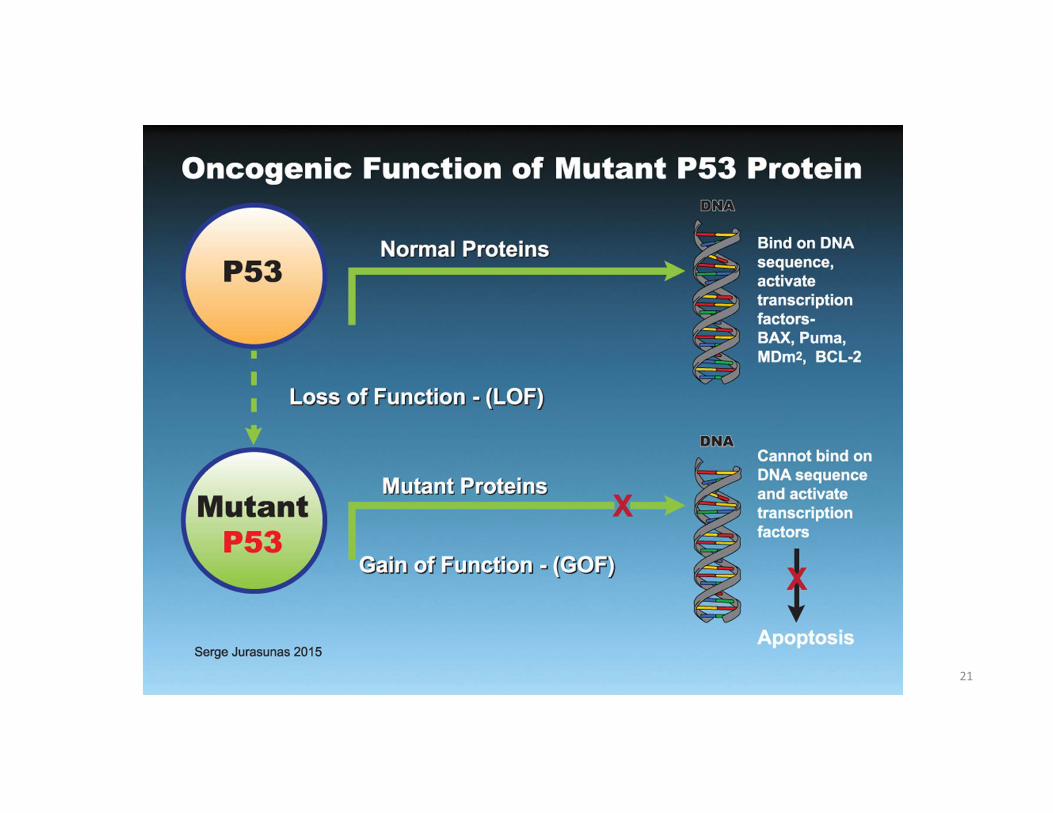
P53 – Tumor Suppressor Gene
the Guardian of Our Genome
Over 60,000 publications
17
January 13, 1997
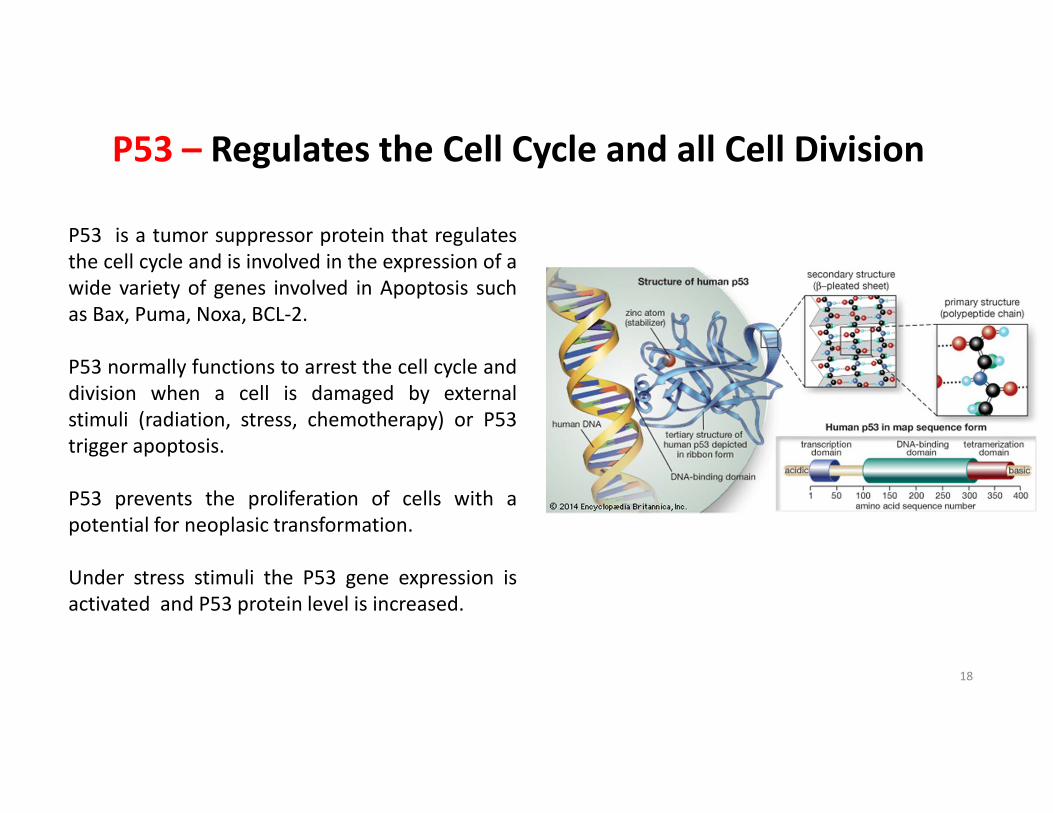
P53 – Regulates the Cell Cycle and all Cell Division
P53 is a tumor suppressor protein that regulates
the cell cycle and is involved in the expression of a
wide variety of genes involved in Apoptosis such
as Bax, Puma, Noxa, BCL-2.
P53 normally functions to arrest the cell cycle and
division when a cell is damaged by external
stimuli (radiation, stress, chemotherapy) or P53
trigger apoptosis.
P53 prevents the proliferation of cells with a
potential for neoplasic transformation.
Under stress stimuli the P53 gene expression is
activated and P53 protein level is increased.
18
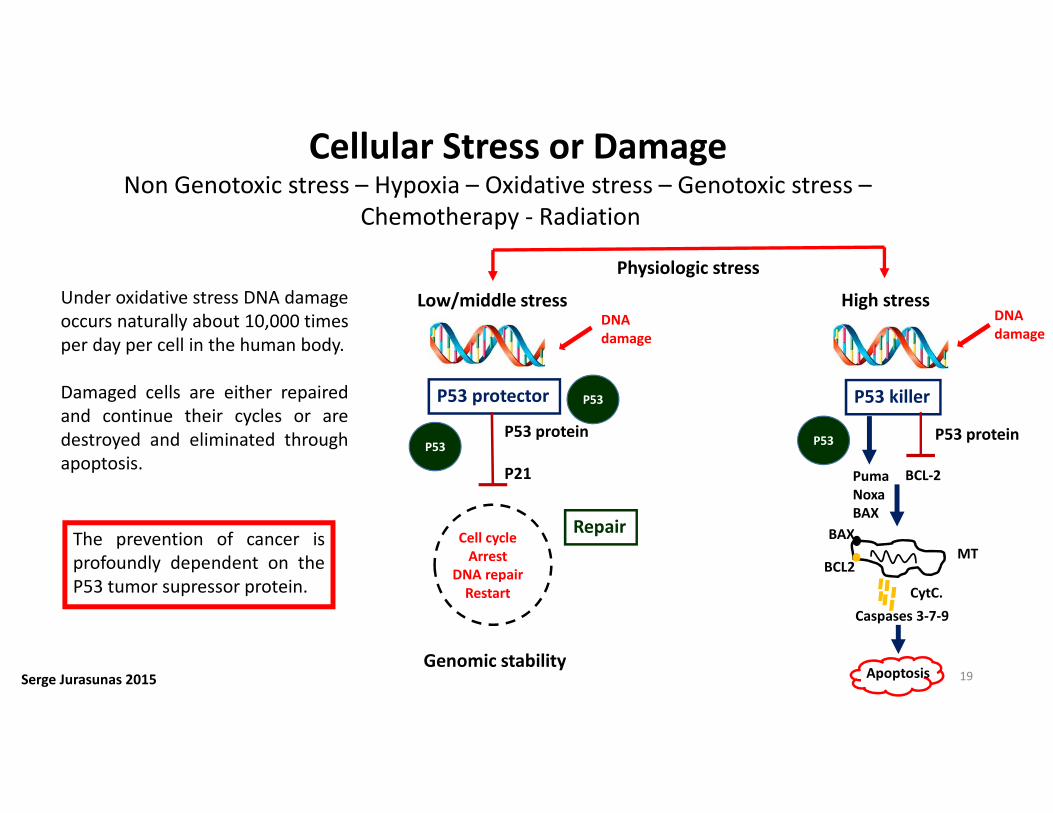
Cellular Stress or DamageNon Genotoxic stress – Hypoxia – Oxidative stress – Genotoxic stress –
Chemotherapy - Radiation
Under oxidative stress DNA damage
occurs naturally about 10,000 times
per day per cell in the human body.
Damaged cells are either repaired
and continue their cycles or are
destroyed and eliminated through
apoptosis.
The prevention of cancer is
profoundly dependent on the
P53 tumor supressor protein.
Serge Jurasunas 2015
Physiologic stress
Low/middle stress High stressDNA
damage
DNA
damage
P53 protector P53 killer
P53 protein
P21
P53 protein
Puma
Noxa
BAX
Apoptosis
Cell cycle
Arrest
DNA repair
Restart
Genomic stability
Repair
P53
P53P53
BCL-2
Caspases 3-7-9
BAX
BCL2MT
CytC.
19
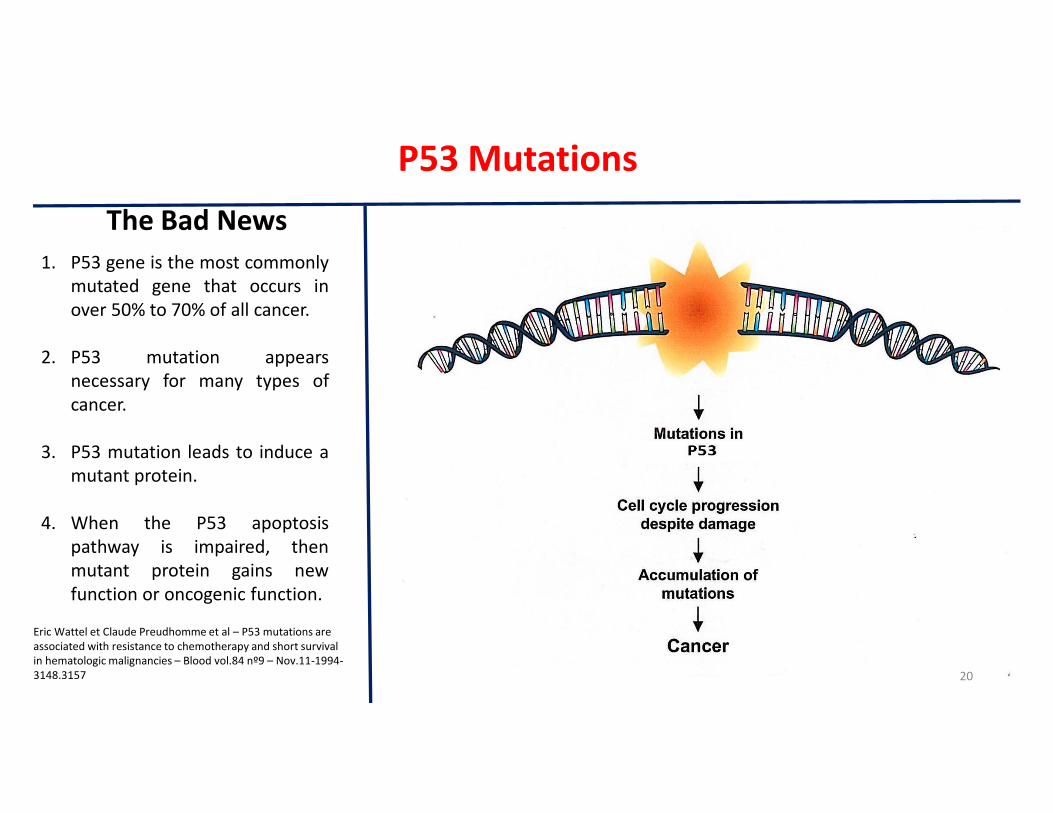
P53 Mutations
1. P53 gene is the most commonly
mutated gene that occurs in
over 50% to 70% of all cancer.
2. P53 mutation appears
necessary for many types of
cancer.
3. P53 mutation leads to induce a
mutant protein.
4. When the P53 apoptosis
pathway is impaired, then
mutant protein gains new
function or oncogenic function.
Eric Wattel et Claude Preudhomme et al – P53 mutations are
associated with resistance to chemotherapy and short survival
in hematologic malignancies – Blood vol.84 nº9 – Nov.11-1994-
3148.3157 20
The Bad News
21
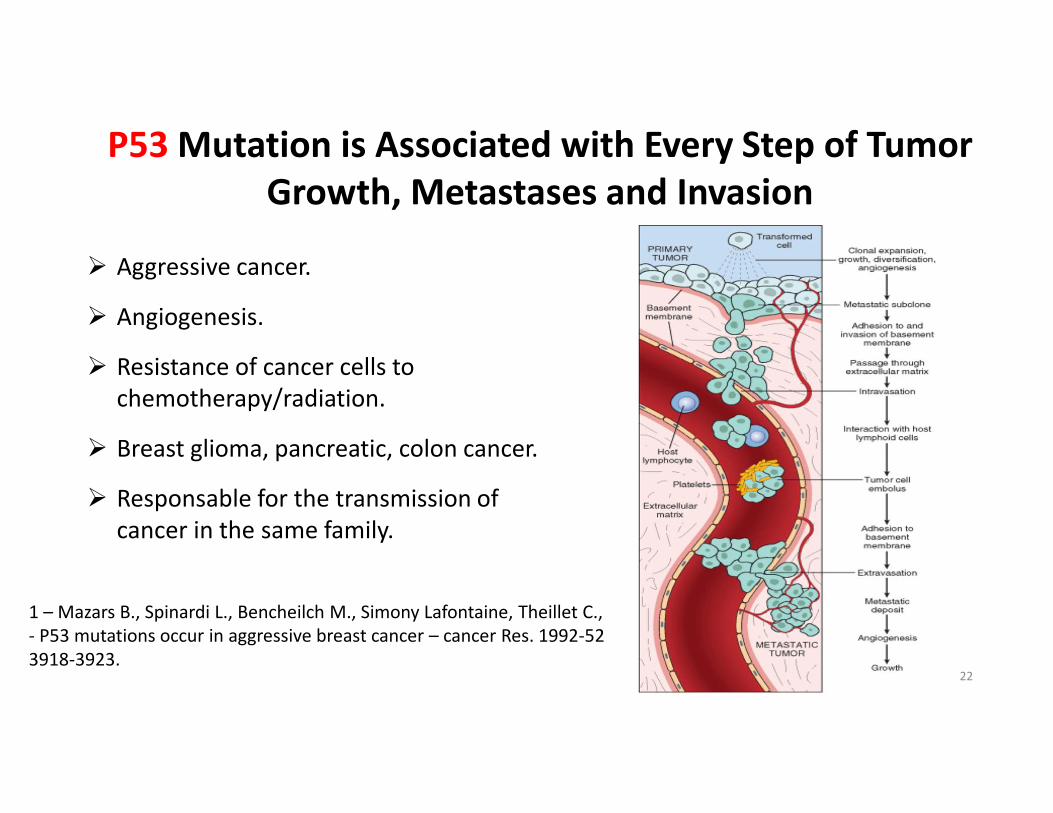
P53 Mutation is Associated with Every Step of Tumor
Growth, Metastases and Invasion
� Aggressive cancer.
� Angiogenesis.
� Resistance of cancer cells to
chemotherapy/radiation.
� Breast glioma, pancreatic, colon cancer.
� Responsable for the transmission of
cancer in the same family.
1 – Mazars B., Spinardi L., Bencheilch M., Simony Lafontaine, Theillet C.,
- P53 mutations occur in aggressive breast cancer – cancer Res. 1992-52
3918-3923.22
23
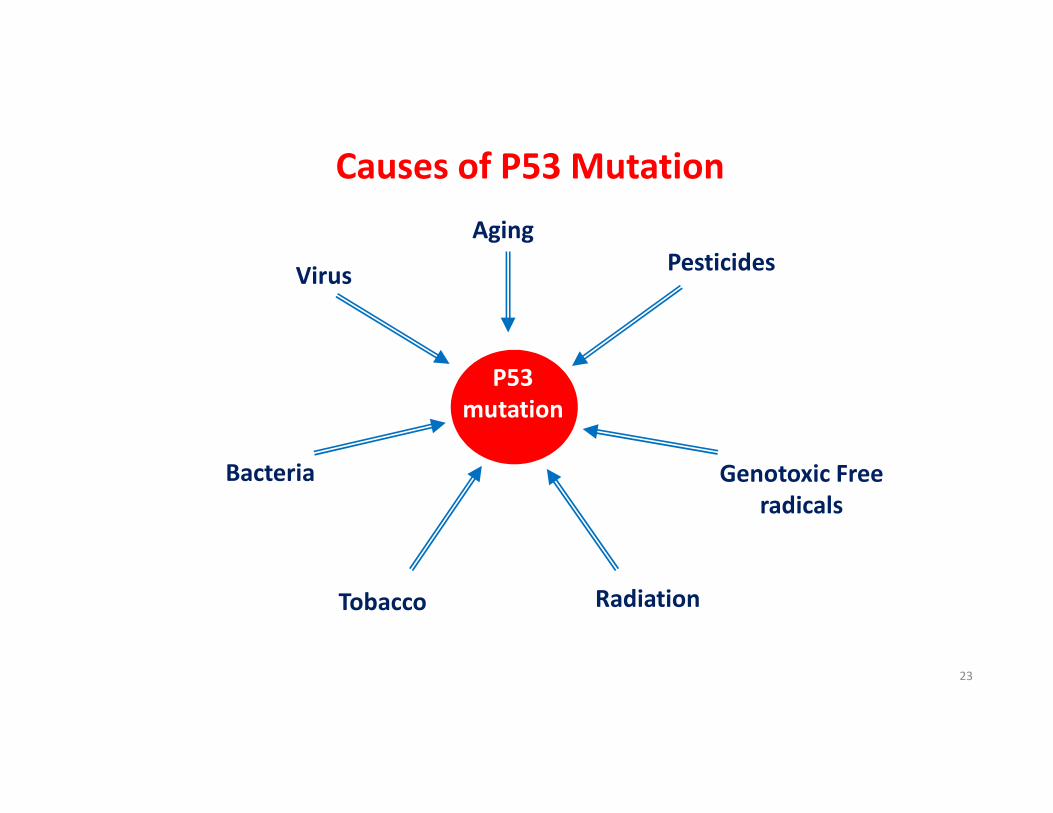
Causes of P53 Mutation
P53
mutation
Aging
Tobacco
Pesticides
Genotoxic Free
radicals
Virus
Bacteria
Radiation
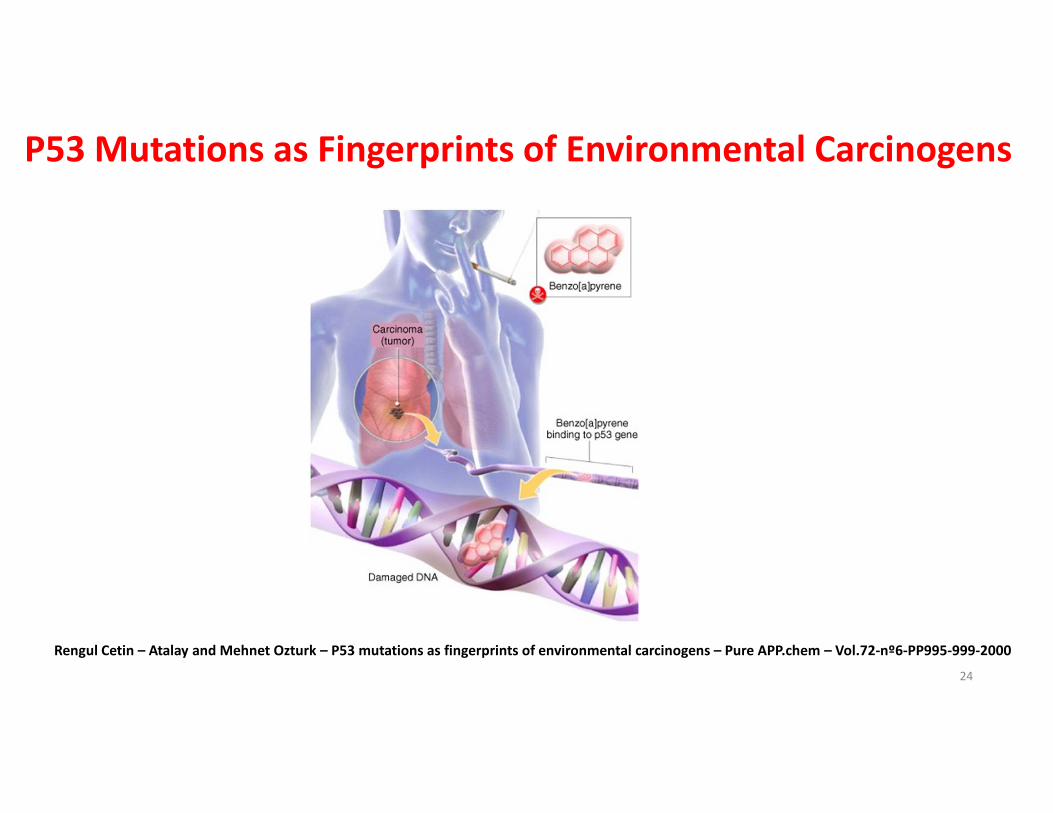
P53 Mutations as Fingerprints of Environmental Carcinogens
Rengul Cetin – Atalay and Mehnet Ozturk – P53 mutations as fingerprints of environmental carcinogens – Pure APP.chem – Vol.72-nº6-PP995-999-2000
24
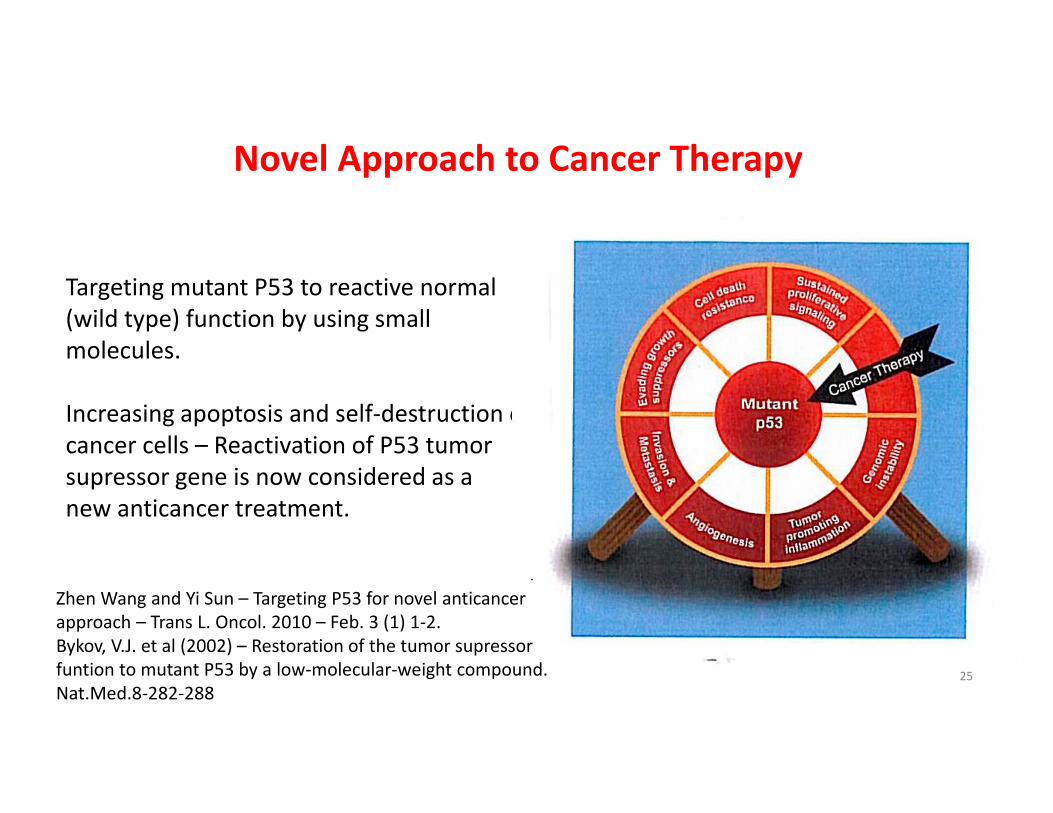
Novel Approach to Cancer Therapy
Targeting mutant P53 to reactive normal
(wild type) function by using small
molecules.
Increasing apoptosis and self-destruction of
cancer cells – Reactivation of P53 tumor
supressor gene is now considered as a
new anticancer treatment.
Zhen Wang and Yi Sun – Targeting P53 for novel anticancer
approach – Trans L. Oncol. 2010 – Feb. 3 (1) 1-2.
Bykov, V.J. et al (2002) – Restoration of the tumor supressor
funtion to mutant P53 by a low-molecular-weight compound.
Nat.Med.8-282-28825
P53 and Chemotherapy
P53 mutation Chemotherapy Prognosis ?
P53 mutation increase the resistance of cancer cells to
numerous chemotherapy agents that fail to destroy. Cancer
cells can accumulate and invade other tissue.
Eric Wattel, Claude Preudhomme et al… - P53 mutations are associated with resistance to chemotherapy and short
survival in hematologic malignancies – Blood Vol.84 – N.9 – Nov.11 – (1994) 3148 – 3157.26
P53 Mutations Predict Outcome in Advance
65/93 Studies found that P53 is a statistically significant factor of poor prognosis in various cancer.
Studies have found that the presence of a mutation was associated with a poor response to various
chemotherapy or radiotherapy regimens in breast, colorectal, ovarian, stomach and soft tissues
carcinoma.
Texas researchers have found that high levels of P53 mutated protein accumulation are associated
with a significantly increased local recurrence rate in 1,500 breast cancer patients treated with
mastectomy.
P53 – positive patients 21.5%
negative patients 9.3%
14/19
27
28
29
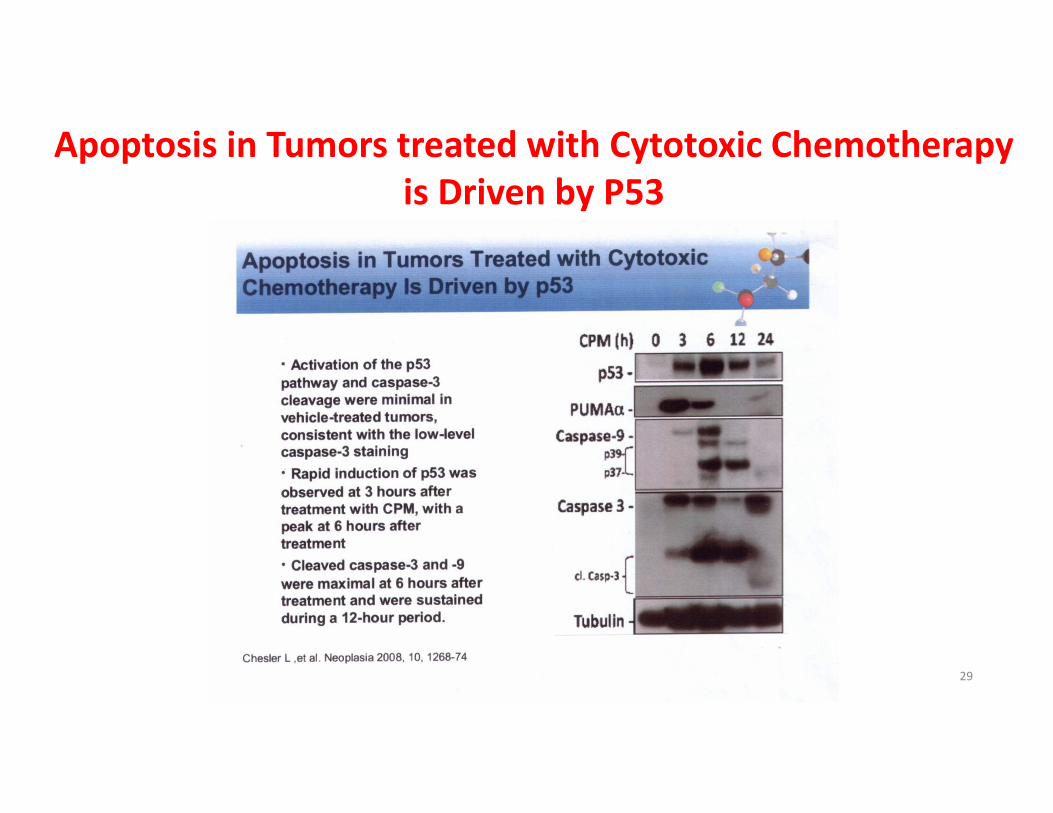
Apoptosis in Tumors treated with Cytotoxic Chemotherapy
is Driven by P53
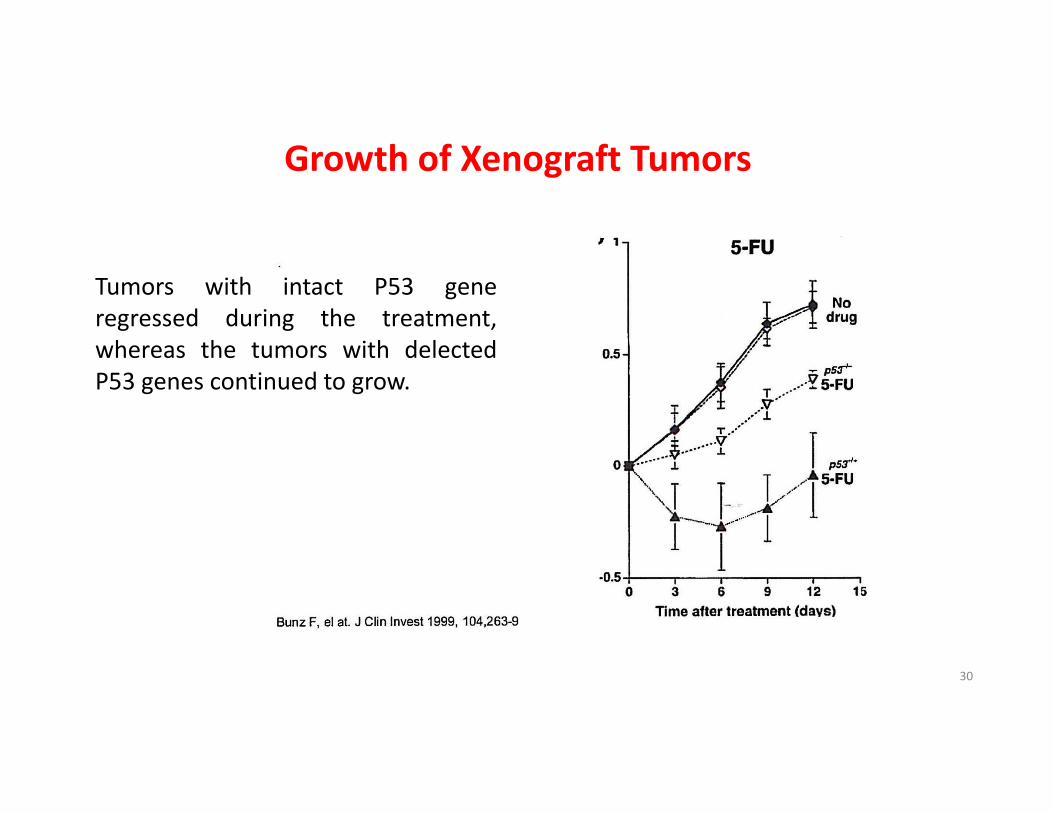
Growth of Xenograft Tumors
Tumors with intact P53 gene
regressed during the treatment,
whereas the tumors with delected
P53 genes continued to grow.
30
We Need to Overcome the Toxicity of Anticancer
agents, radiotherapy, etc.
Toxic toHealthy Cells
31
32
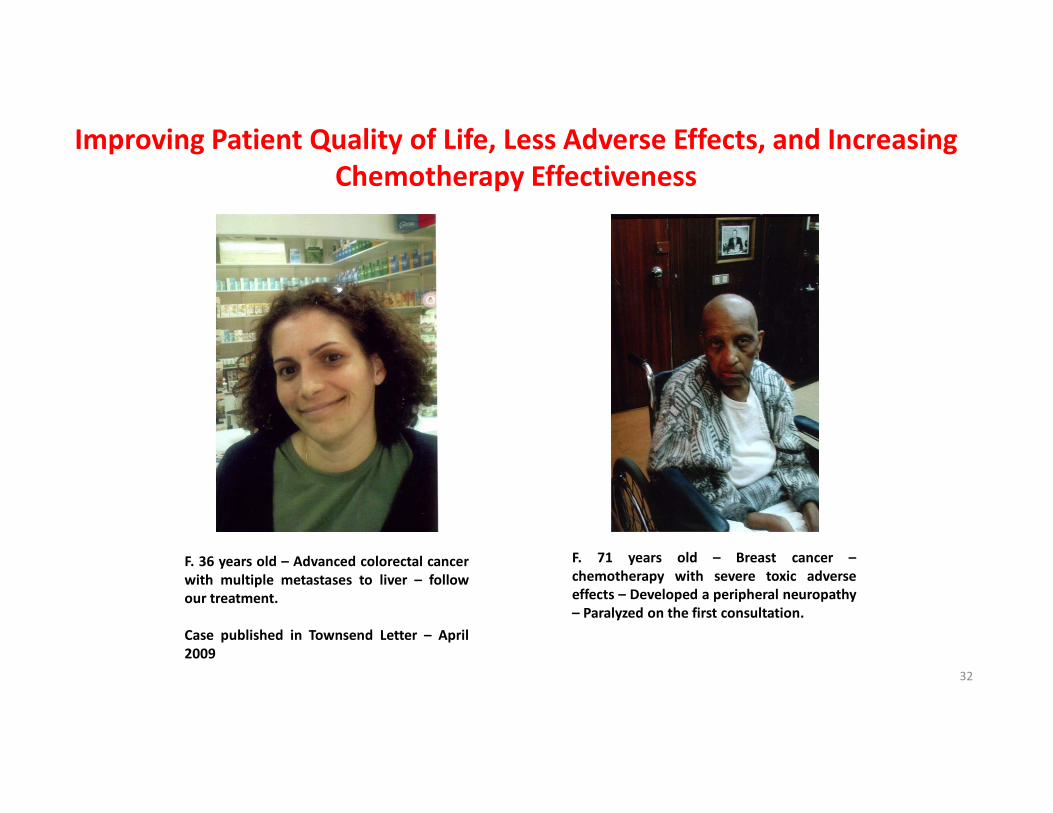
Improving Patient Quality of Life, Less Adverse Effects, and Increasing
Chemotherapy Effectiveness
F. 36 years old – Advanced colorectal cancer
with multiple metastases to liver – follow
our treatment.
Case published in Townsend Letter – April
2009
F. 71 years old – Breast cancer –
chemotherapy with severe toxic adverse
effects – Developed a peripheral neuropathy
– Paralyzed on the first consultation.
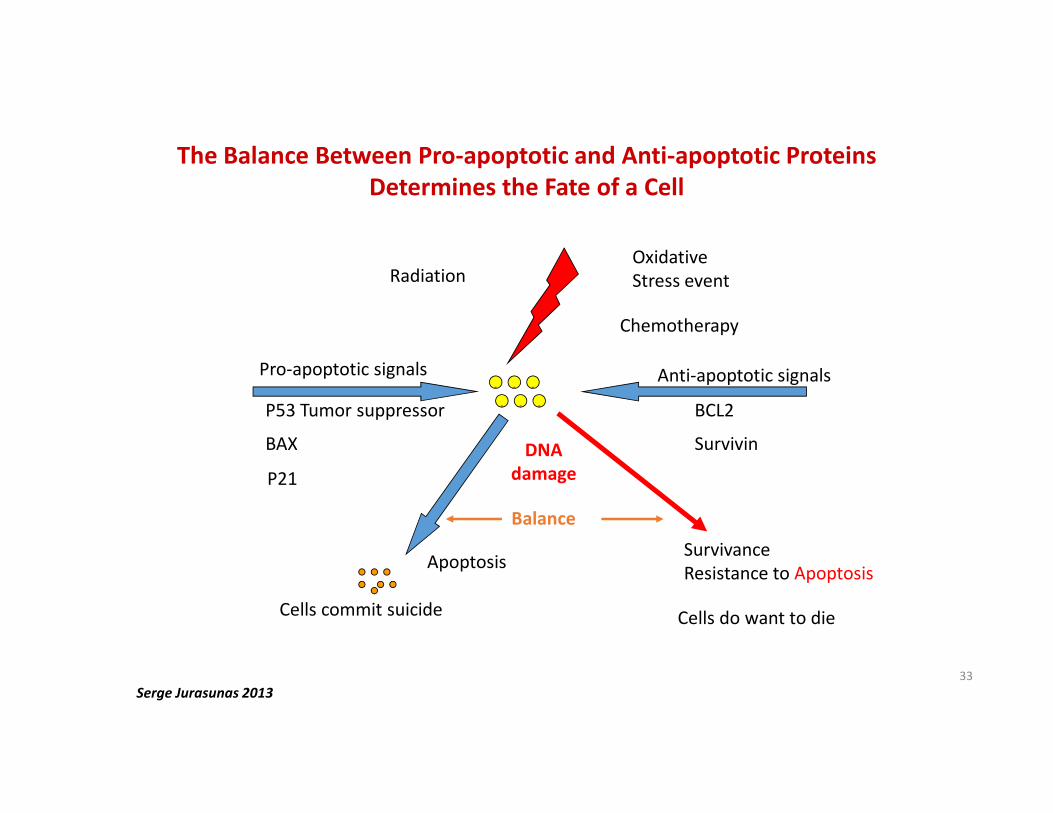
The Balance Between Pro-apoptotic and Anti-apoptotic Proteins
Determines the Fate of a Cell
Serge Jurasunas 2013
Cells commit suicide
RadiationOxidative
Stress event
Chemotherapy
Anti-apoptotic signals
BCL2
Survivin
Pro-apoptotic signals
P53 Tumor suppressor
BAX
P21
Apoptosis
DNA
damage
Balance
Survivance
Resistance to Apoptosis
Cells do want to die
... . .
.
33
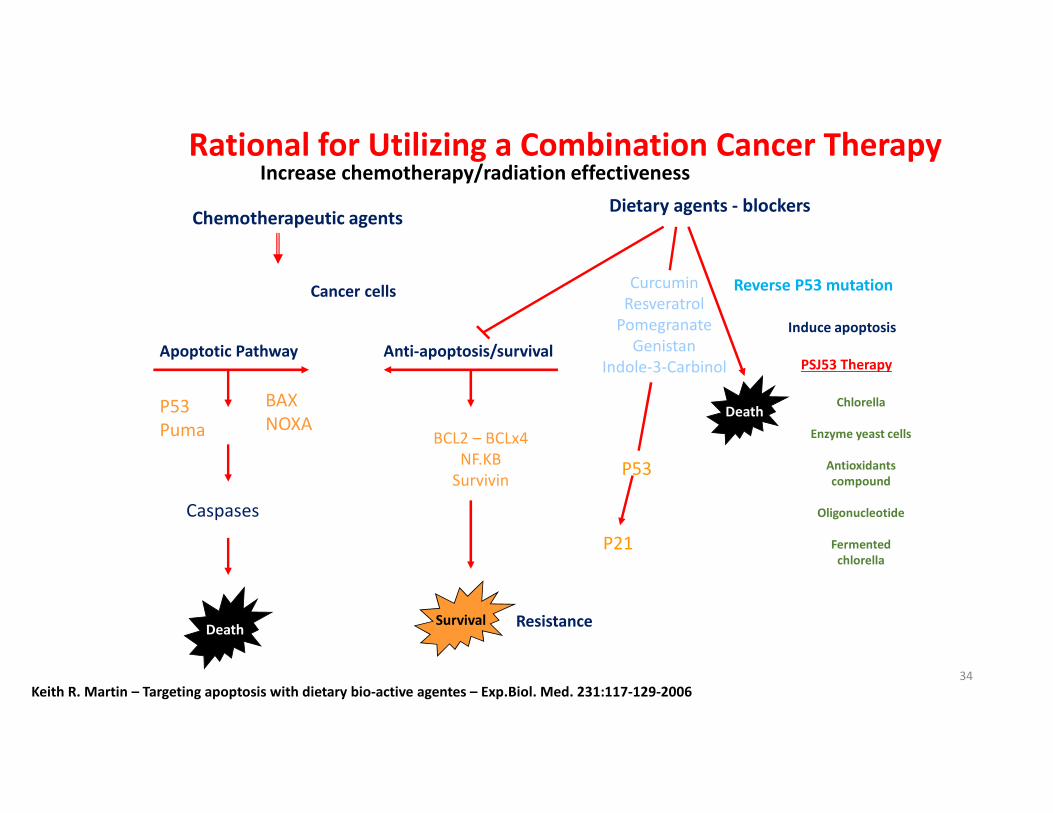
Rational for Utilizing a Combination Cancer TherapyIncrease chemotherapy/radiation effectiveness
Chemotherapeutic agents
Cancer cells
Apoptotic Pathway
P53
Puma
BAX
NOXA
Caspases
Death
Dietary agents - blockers
Anti-apoptosis/survival
BCL2 – BCLx4
NF.KB
Survivin
Survival Resistance
Curcumin
Resveratrol
Pomegranate
Genistan
Indole-3-Carbinol
P53
P21
Reverse P53 mutation
Death
Induce apoptosis
PSJ53 Therapy
Chlorella
Enzyme yeast cells
Antioxidants
compound
Oligonucleotide
Fermented
chlorella
Keith R. Martin – Targeting apoptosis with dietary bio-active agentes – Exp.Biol. Med. 231:117-129-200634
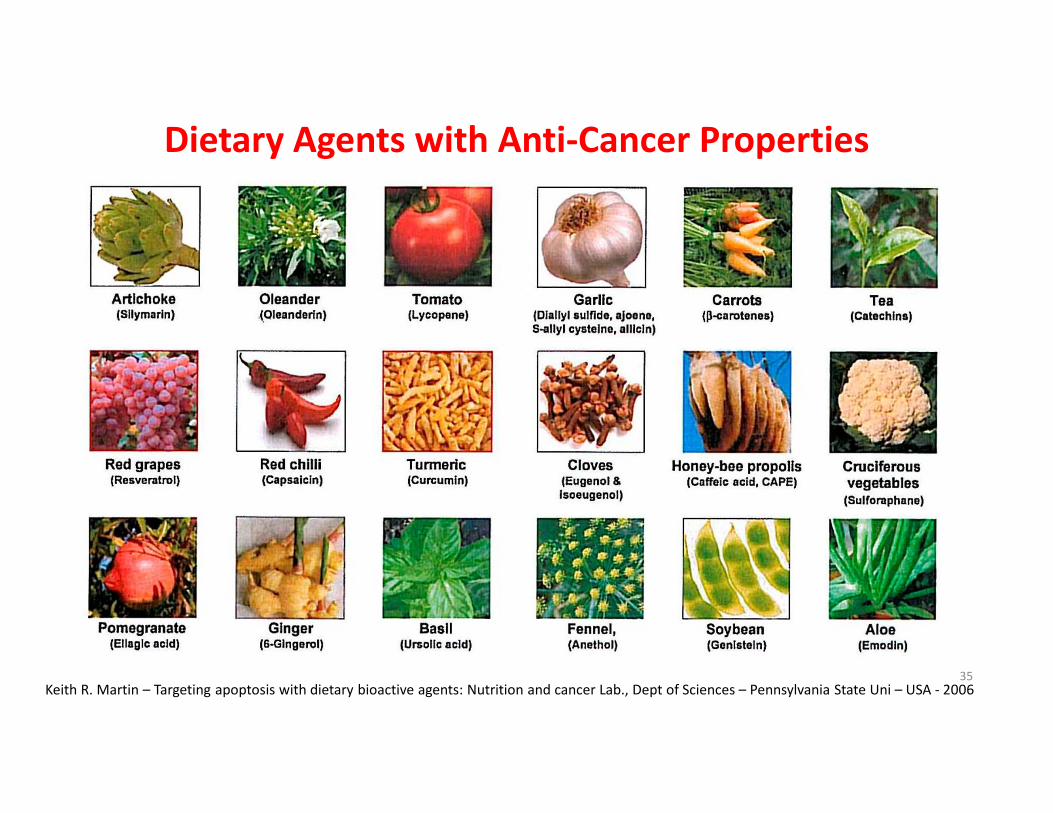
Dietary Agents with Anti-Cancer Properties
Keith R. Martin – Targeting apoptosis with dietary bioactive agents: Nutrition and cancer Lab., Dept of Sciences – Pennsylvania State Uni – USA - 200635
36
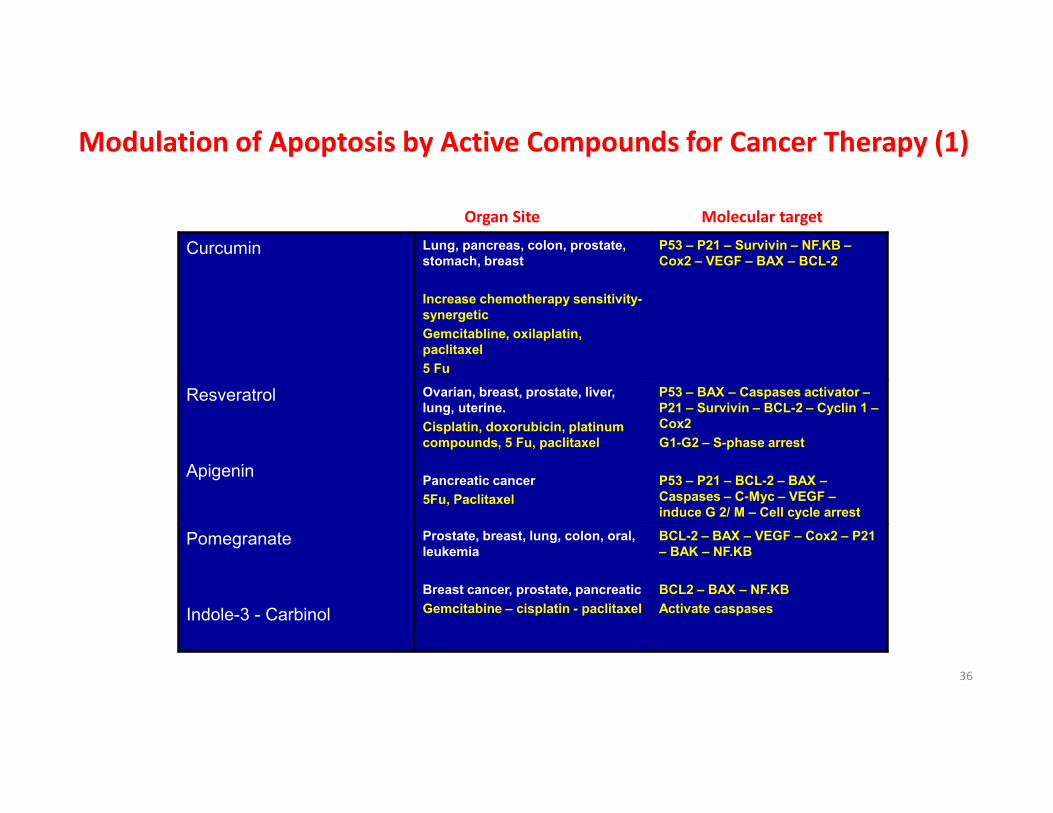
Modulation of Apoptosis by Active Compounds for Cancer Therapy (1)
Curcumin Lung, pancreas, colon, prostate,
stomach, breast.
Increase chemotherapy sensitivity-
synergetic
Gemcitabline, oxilaplatin,
paclitaxel
5 Fu
P53 – P21 – Survivin – NF.KB –
Cox2 – VEGF – BAX – BCL-2
Resveratrol
Apigenin
Ovarian, breast, prostate, liver,
lung, uterine.
Cisplatin, doxorubicin, platinum
compounds, 5 Fu, paclitaxel
Pancreatic cancer
5Fu, Paclitaxel
P53 – BAX – Caspases activator –
P21 – Survivin – BCL-2 – Cyclin 1 –
Cox2
G1-G2 – S-phase arrest
P53 – P21 – BCL-2 – BAX –
Caspases – C-Myc – VEGF –
induce G 2/ M – Cell cycle arrest
Pomegranate
Indole-3 - Carbinol
Prostate, breast, lung, colon, oral,
leukemia
Breast cancer, prostate, pancreatic
Gemcitabine – cisplatin - paclitaxel
BCL-2 – BAX – VEGF – Cox2 – P21
– BAK – NF.KB
BCL2 – BAX – NF.KB
Activate caspases
Organ Site Molecular target
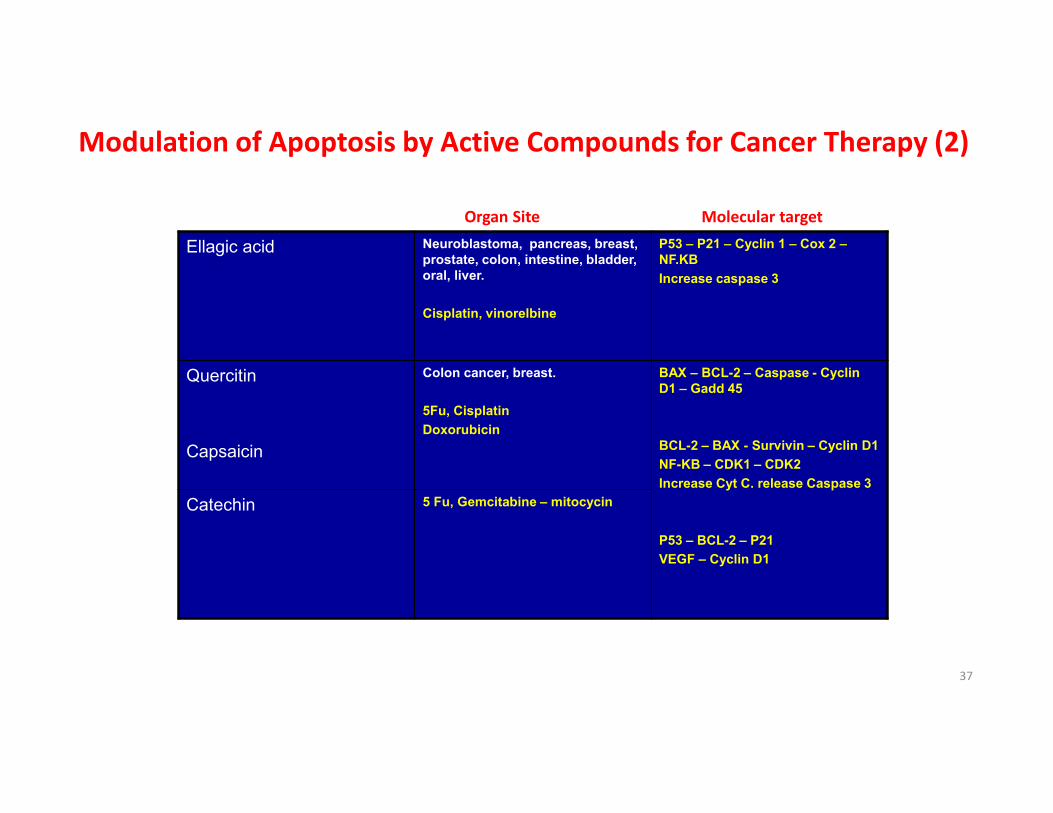
Ellagic acid Neuroblastoma, pancreas, breast,
prostate, colon, intestine, bladder,
oral, liver.
Cisplatin, vinorelbine
P53 – P21 – Cyclin 1 – Cox 2 –
NF.KB
Increase caspase 3
Quercitin
Capsaicin
Colon cancer, breast.
5Fu, Cisplatin
Doxorubicin
BAX – BCL-2 – Caspase - Cyclin
D1 – Gadd 45
BCL-2 – BAX - Survivin – Cyclin D1
NF-KB – CDK1 – CDK2
Increase Cyt C. release Caspase 3
P53 – BCL-2 – P21
VEGF – Cyclin D1
Catechin 5 Fu, Gemcitabine – mitocycin
Modulation of Apoptosis by Active Compounds for Cancer Therapy (2)
Organ Site Molecular target
37

Green tea
Polyphenols and EGCG
Lung, oral, stomach, liver,
pancreas, colon, bladder, prostate,
breast.
Tamoxifen – cisplatin –
adriamycin, dacarbazine
P53 – P21 – BAX – BCL-2 – NF.KB
– Cyclin 1 - Cox2 – VEGF _
increase Xiap
Isithiocyanates (ITC’s)
Sulforaphane
(Cruciferous vegetables)
Prostate, breast
Docetaxel
Adriamycin
Cisplatin
BCL-2 – Survivin – NF.KB – Cyclin
1 – P53 – caspase activation
Licopene Prostate, lung, breast, gastric,
liver, pancreas colorectal
Adriamycin
Cisplatin
Cyclin D1 - BCL-2 – BCL-4 AKT –
NF.KB – MMP9
Organ Site Molecular target
Modulation of Apoptosis by Active Compounds for Cancer Therapy (3)
38
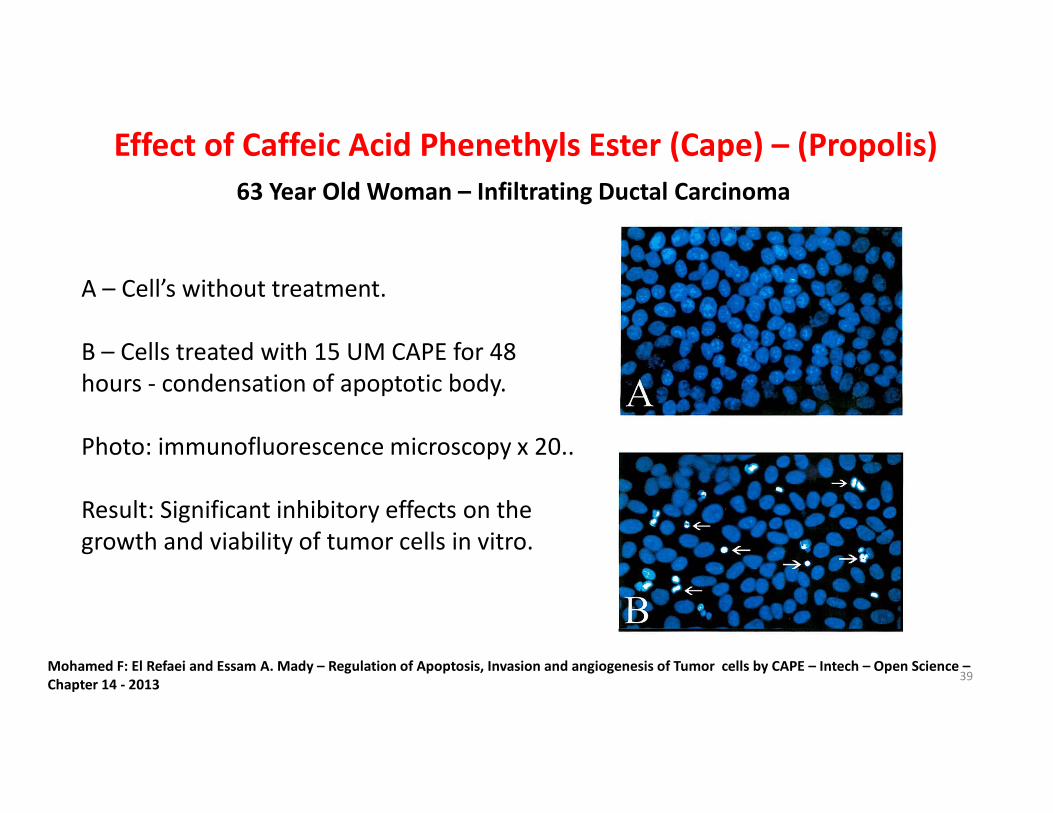
Effect of Caffeic Acid Phenethyls Ester (Cape) – (Propolis)
63 Year Old Woman – Infiltrating Ductal Carcinoma
A – Cell’s without treatment.
B – Cells treated with 15 UM CAPE for 48
hours - condensation of apoptotic body.
Photo: immunofluorescence microscopy x 20..
Result: Significant inhibitory effects on the
growth and viability of tumor cells in vitro.
Mohamed F: El Refaei and Essam A. Mady – Regulation of Apoptosis, Invasion and angiogenesis of Tumor cells by CAPE – Intech – Open Science –
Chapter 14 - 201339
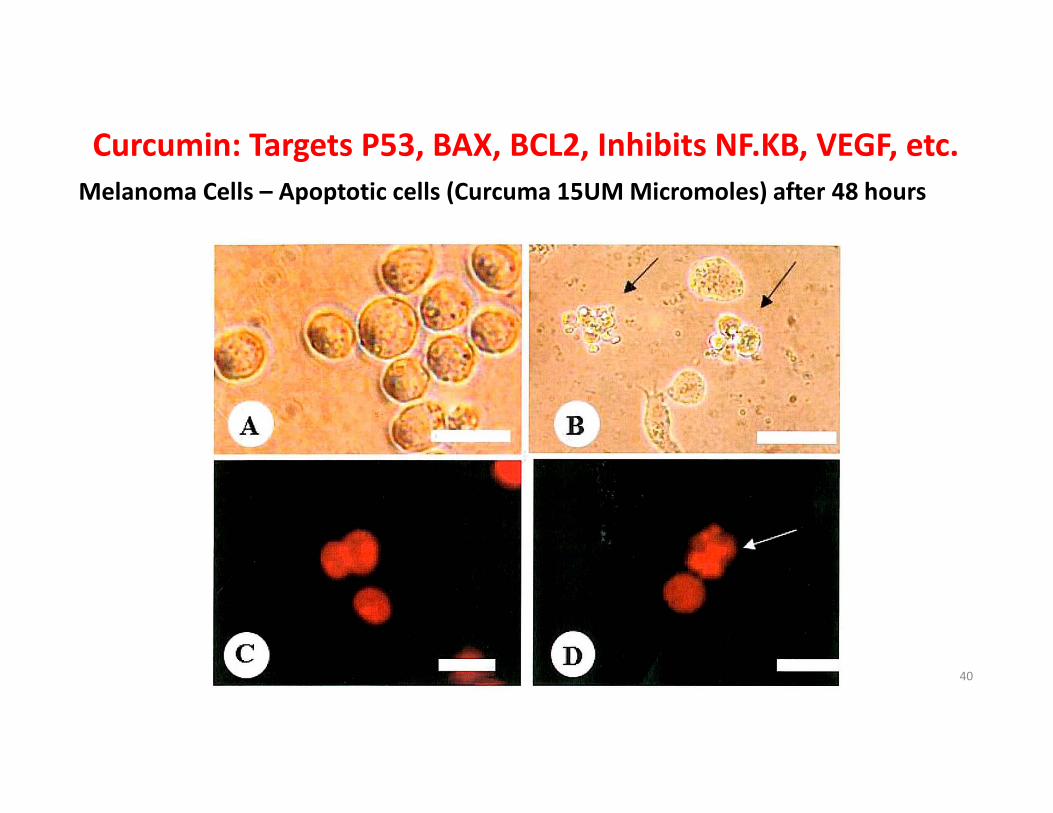
Curcumin: Targets P53, BAX, BCL2, Inhibits NF.KB, VEGF, etc.
Melanoma Cells – Apoptotic cells (Curcuma 15UM Micromoles) after 48 hours
40
Anticancer Properties of Foods
Apoptosis – Angiogenesis – Inflammation – Immune Defense
“Let food your medicine and medicine be your food.”
Hyppocrates 460-370 B.C.41
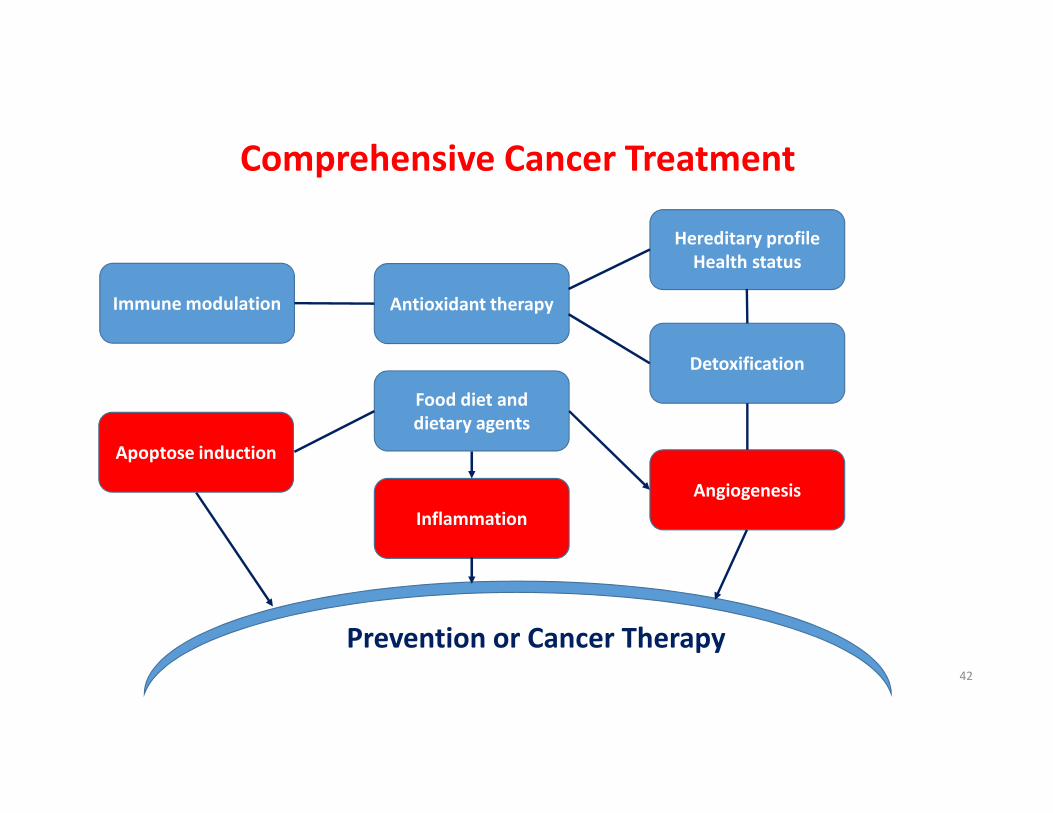
Comprehensive Cancer Treatment
Prevention or Cancer Therapy
Immune modulation Antioxidant therapy
Hereditary profile
Health status
Detoxification
Food diet and
dietary agents
Apoptose induction
Inflammation
Angiogenesis
42

Patients Undergoing Molecular Markers Tests
Method: Elisa Assay
Quantitative Polymer Chain Reactional (P.C.R.)
43
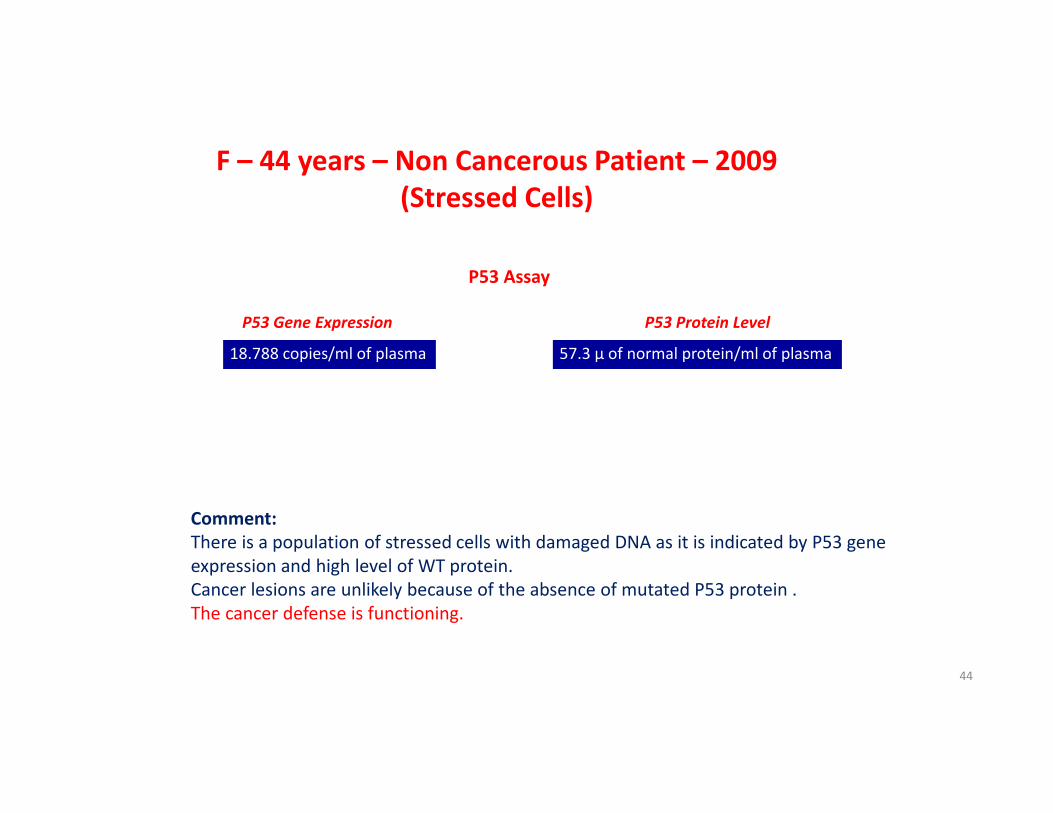
P53 Gene Expression P53 Protein Level
18.788 copies/ml of plasma 57.3 µ of normal protein/ml of plasma
Reference range
50 copies
F – 44 years – Non Cancerous Patient – 2009
(Stressed Cells)
Reference range
0.33 units
Comment:
There is a population of stressed cells with damaged DNA as it is indicated by P53 gene
expression and high level of WT protein.
Cancer lesions are unlikely because of the absence of mutated P53 protein .
The cancer defense is functioning.
P53 Assay
44
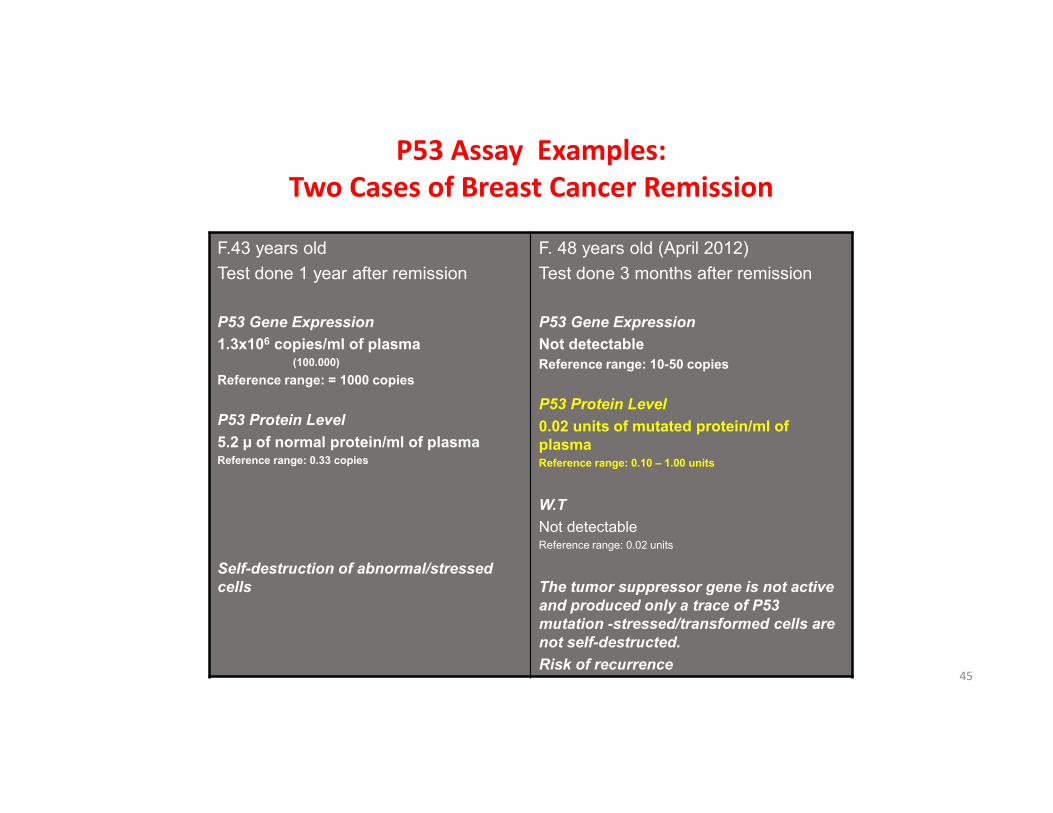
P53 Assay Examples:
Two Cases of Breast Cancer Remission
F.43 years old
Test done 1 year after remission
P53 Gene Expression
1.3x106 copies/ml of plasma(100.000)
Reference range: = 1000 copies
P53 Protein Level
5.2 µ of normal protein/ml of plasmaReference range: 0.33 copies
Self-destruction of abnormal/stressed
cells
F. 48 years old (April 2012)
Test done 3 months after remission
P53 Gene Expression
Not detectable
Reference range: 10-50 copies
P53 Protein Level
0.02 units of mutated protein/ml of
plasmaReference range: 0.10 – 1.00 units
W.T
Not detectableReference range: 0.02 units
The tumor suppressor gene is not active
and produced only a trace of P53
mutation -stressed/transformed cells are
not self-destructed.
Risk of recurrence45
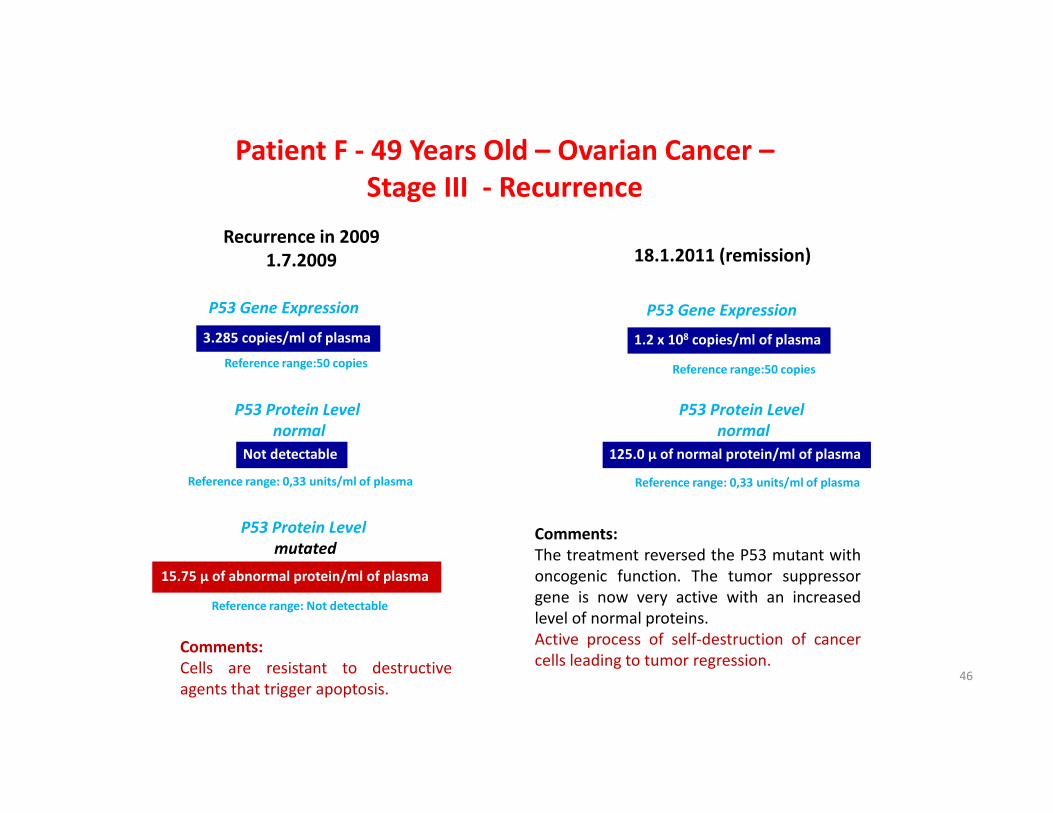
P53 Gene Expression
P53 Protein Level
mutated
3.285 copies/ml of plasma
15.75 µ of abnormal protein/ml of plasma
Reference range:50 copies
Reference range: 0,33 units/ml of plasma
Patient F - 49 Years Old – Ovarian Cancer –
Stage III - Recurrence
Recurrence in 2009
1.7.2009 18.1.2011 (remission)
P53 Gene Expression
1.2 x 108 copies/ml of plasma
P53 Protein Level
normal
125.0 µ of normal protein/ml of plasma
Reference range: Not detectable
Comments:
Cells are resistant to destructive
agents that trigger apoptosis.
Comments:
The treatment reversed the P53 mutant with
oncogenic function. The tumor suppressor
gene is now very active with an increased
level of normal proteins.
Active process of self-destruction of cancer
cells leading to tumor regression.
P53 Protein Level
normal
Not detectable
Reference range: 0,33 units/ml of plasma
Reference range:50 copies
46
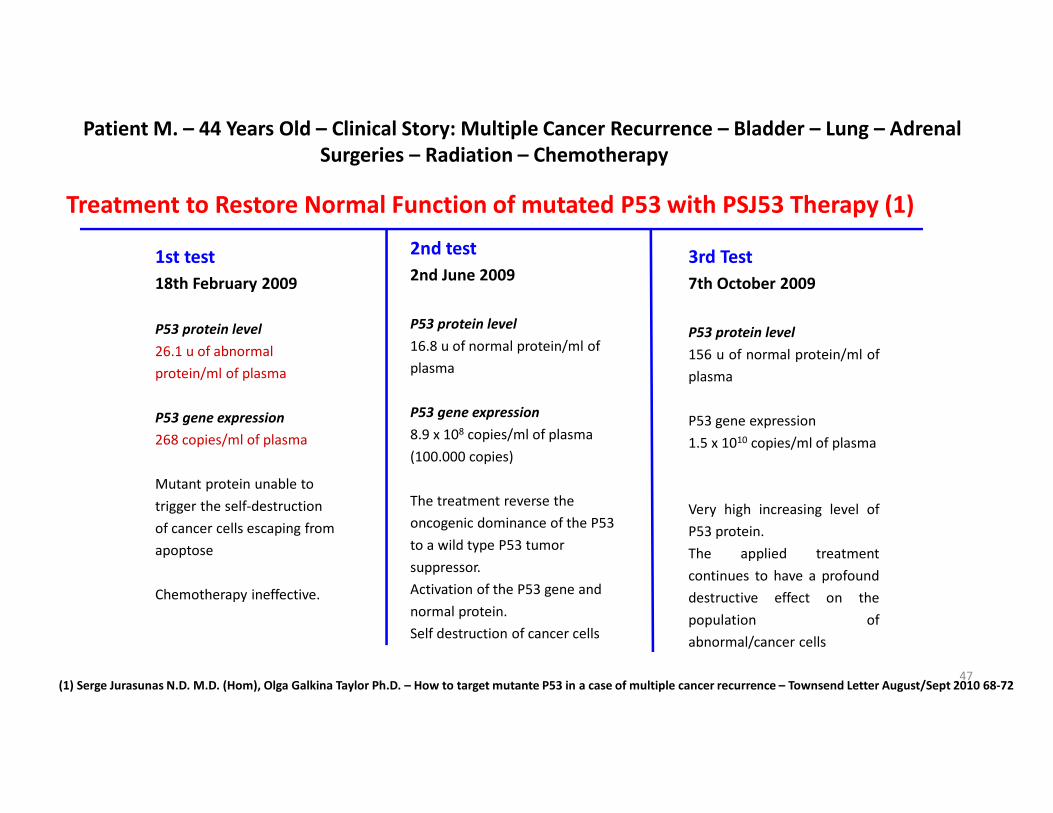
Patient M. – 44 Years Old – Clinical Story: Multiple Cancer Recurrence – Bladder – Lung – Adrenal
Surgeries – Radiation – Chemotherapy
1st test
18th February 2009
P53 protein level
26.1 u of abnormal
protein/ml of plasma
P53 gene expression
268 copies/ml of plasma
Mutant protein unable to
trigger the self-destruction
of cancer cells escaping from
apoptose
Chemotherapy ineffective.
2nd test
2nd June 2009
P53 protein level
16.8 u of normal protein/ml of
plasma
P53 gene expression
8.9 x 108 copies/ml of plasma
(100.000 copies)
The treatment reverse the
oncogenic dominance of the P53
to a wild type P53 tumor
suppressor.
Activation of the P53 gene and
normal protein.
Self destruction of cancer cells
3rd Test
7th October 2009
P53 protein level
156 u of normal protein/ml of
plasma
P53 gene expression
1.5 x 1010 copies/ml of plasma
Very high increasing level of
P53 protein.
The applied treatment
continues to have a profound
destructive effect on the
population of
abnormal/cancer cells
Treatment to Restore Normal Function of mutated P53 with PSJ53 Therapy (1)
(1) Serge Jurasunas N.D. M.D. (Hom), Olga Galkina Taylor Ph.D. – How to target mutante P53 in a case of multiple cancer recurrence – Townsend Letter August/Sept 2010 68-7247
48
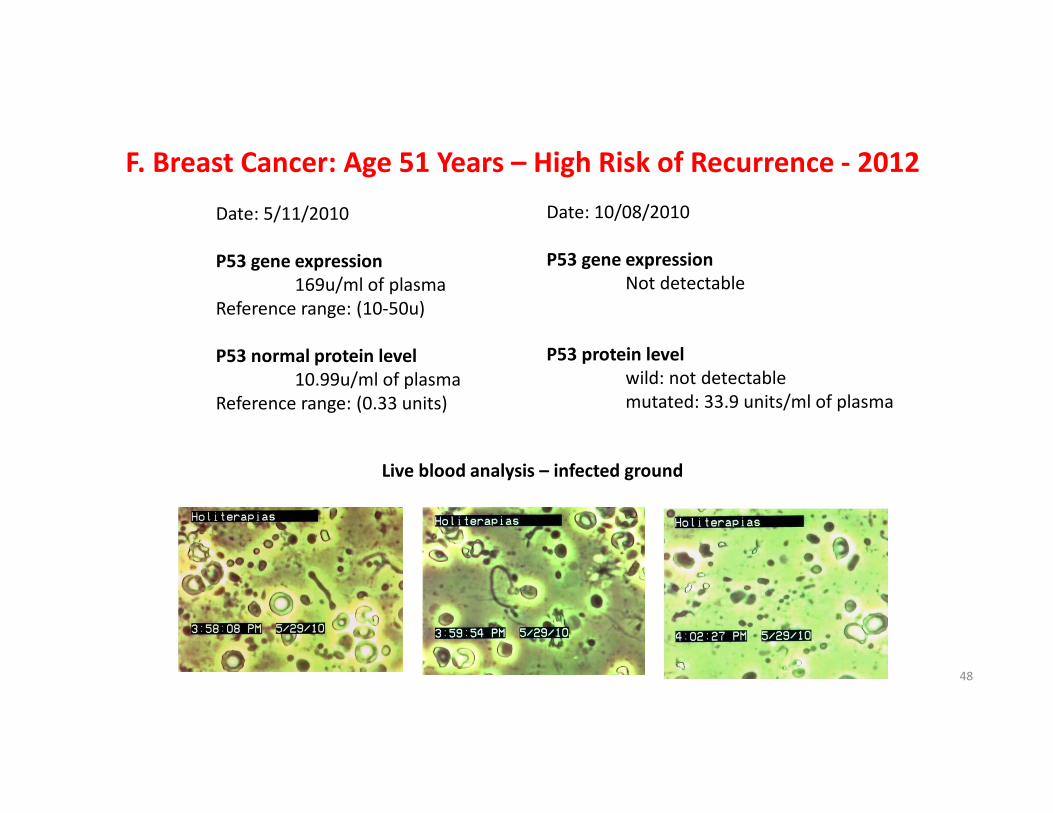
F. Breast Cancer: Age 51 Years – High Risk of Recurrence - 2012
Date: 5/11/2010
P53 gene expression
169u/ml of plasma
Reference range: (10-50u)
P53 normal protein level
10.99u/ml of plasma
Reference range: (0.33 units)
Date: 10/08/2010
P53 gene expression
Not detectable
P53 protein level
wild: not detectable
mutated: 33.9 units/ml of plasma
Live blood analysis – infected ground
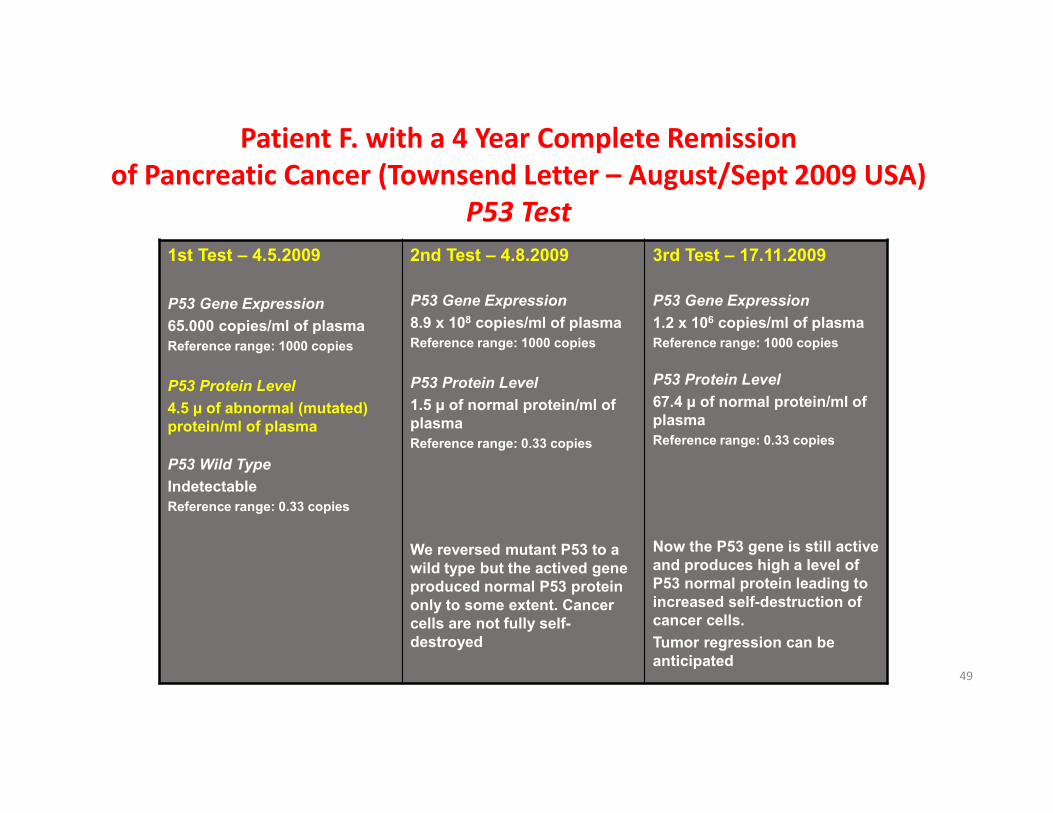
Patient F. with a 4 Year Complete Remission
of Pancreatic Cancer (Townsend Letter – August/Sept 2009 USA)
P53 Test
1st Test – 4.5.2009
P53 Gene Expression
65.000 copies/ml of plasma
Reference range: 1000 copies
P53 Protein Level
4.5 µ of abnormal (mutated)
protein/ml of plasma
P53 Wild Type
Indetectable
Reference range: 0.33 copies
2nd Test – 4.8.2009
P53 Gene Expression
8.9 x 108 copies/ml of plasma
Reference range: 1000 copies
P53 Protein Level
1.5 µ of normal protein/ml of
plasma
Reference range: 0.33 copies
We reversed mutant P53 to a
wild type but the actived gene
produced normal P53 protein
only to some extent. Cancer
cells are not fully self-
destroyed
3rd Test – 17.11.2009
P53 Gene Expression
1.2 x 106 copies/ml of plasma
Reference range: 1000 copies
P53 Protein Level
67.4 µ of normal protein/ml of
plasma
Reference range: 0.33 copies
Now the P53 gene is still active
and produces high a level of
P53 normal protein leading to
increased self-destruction of
cancer cells.
Tumor regression can be
anticipated49
50
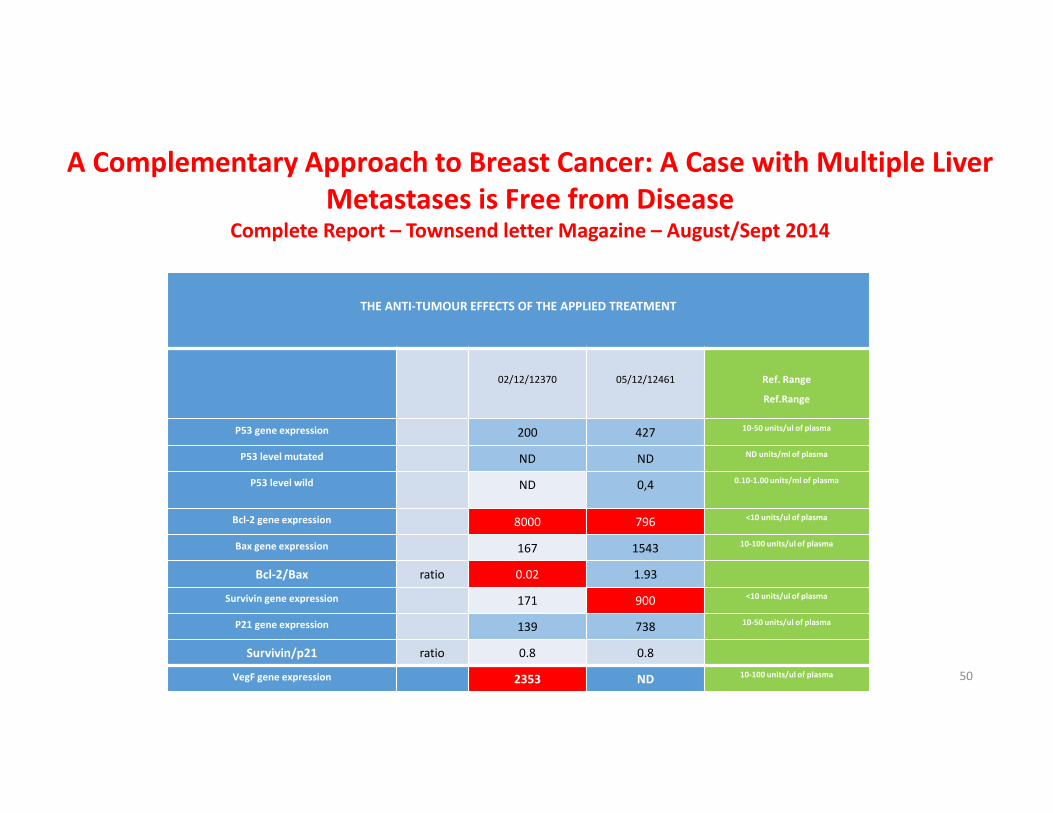
THE ANTI-TUMOUR EFFECTS OF THE APPLIED TREATMENT
02/12/12370 05/12/12461 Ref. Range
Ref.Range
P53 gene expression 200 427 10-50 units/ul of plasma
P53 level mutated ND ND ND units/ml of plasma
P53 level wild ND 0,4 0.10-1.00 units/ml of plasma
Bcl-2 gene expression 8000 796 <10 units/ul of plasma
Bax gene expression 167 1543 10-100 units/ul of plasma
Bcl-2/Bax ratio 0.02 1.93
Survivin gene expression 171 900 <10 units/ul of plasma
P21 gene expression 139 738 10-50 units/ul of plasma
Survivin/p21 ratio 0.8 0.8
VegF gene expression 2353 ND 10-100 units/ul of plasma
A Complementary Approach to Breast Cancer: A Case with Multiple Liver
Metastases is Free from Disease Complete Report – Townsend letter Magazine – August/Sept 2014
51
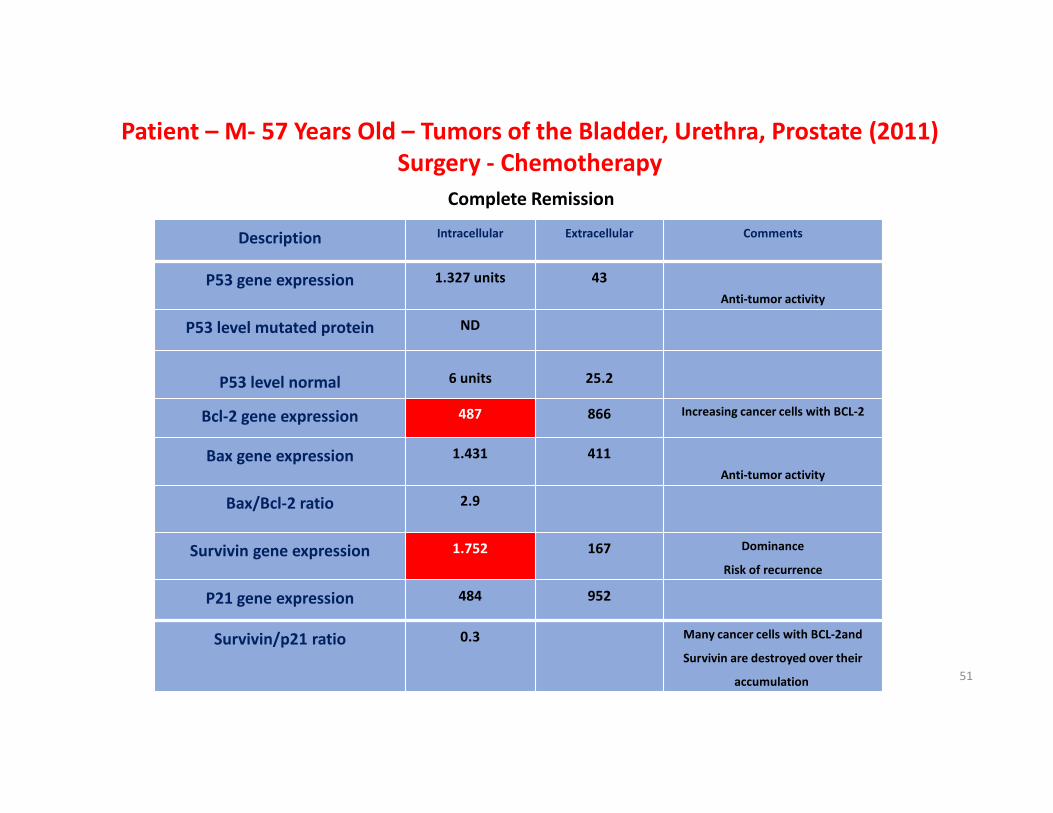
Description Intracellular Extracellular Comments
P53 gene expression 1.327 units 43
Anti-tumor activity
P53 level mutated protein ND
P53 level normal 6 units 25.2
Bcl-2 gene expression 487 866 Increasing cancer cells with BCL-2
Bax gene expression 1.431 411
Anti-tumor activity
Bax/Bcl-2 ratio 2.9
Survivin gene expression 1.752 167 Dominance
Risk of recurrence
P21 gene expression 484 952
Survivin/p21 ratio 0.3 Many cancer cells with BCL-2and
Survivin are destroyed over their
accumulation
Patient – M- 57 Years Old – Tumors of the Bladder, Urethra, Prostate (2011)
Surgery - Chemotherapy
Complete Remission
More Information
Modulation of Apoptosis by active dietary compounds
and their synergistic effects with chemotherapy in
cancer treatment.
Articles on cellular respiration and cancer,
mitochondria, P53 and other molecular markers.
Clinical cases.
Integrative cancer treatment.
www.sergejurasunas.com
Email: [email protected]
52
Thank You for
Your Attention!
Don’t Let the Cancer Kill You, but rather Kill the Cancer.
53
www.sergejurasunas.comwww.sergejurasunas.comwww.sergejurasunas.comwww.sergejurasunas.com
Please visit our website for further information
54


















