How to Keep Your Surgeon Out of Trouble: Perioperative Medicine ...
94
How to Keep Your Surgeon Out of Trouble: Perioperative Medicine: Risk Stratification Jalal K. Ghali, M.D., F.A.C.C. Professor of Medicine Associate Chair for Clinical Research Chief, Division of Cardiology Department of Medicine Mercer University School of Medicine Macon, GA
Transcript of How to Keep Your Surgeon Out of Trouble: Perioperative Medicine ...

How to Keep Your Surgeon Out of
Trouble: Perioperative Medicine:
Risk Stratification
Jalal K. Ghali, M.D., F.A.C.C.
Professor of Medicine
Associate Chair for Clinical Research
Chief, Division of Cardiology
Department of Medicine
Mercer University School of Medicine
Macon, GA
How to Make Your Surgeon
Happy

Dear Dr. GS,
Your patient Mr. MC has been “cleared” for
the planned surgery.
I would like to assure you that no medical
complications will arise from the planned
surgery and furthermore, should they arise, I
take full responsibility for managing them.
Our commitment extends for full 30 days post
op.
How to Keep Your Surgeon Out of
Trouble:
Impossible

Disclosures
Internists: Know everything
Surgeons: Know nothing
Psychiatrists: Have no clue
Pathologists: Know everything, one day late
do everything…
and do no procedures
and do everything

Definition of the
Medical Consultant
Magnitude of the problem
Is there a need for medical consultation?
Pathophysiology
Predictive models
Revised Cardiac Risk Index
Thoracic Revised Cardiac Risk Index
Vascular Study Group of New England
Surgical Mortality Probability Model
Risk Calculator for Prediction of Cardiac Risk
Perioperative Medicine

Clinical Recommendations
Special considerations
Biomarkers
Hypertension
PCI
Statins
Beta Blockers
Summary
Definition of the medical consultant
Perioperative Medicine

10 million major noncardiac surgery
4 million in patients ≥65 years
High risk account for 80% of death
250 million procedures worldwide
Common preventable complications after non-cardiac surgery
that may be prevented by enhanced perioperative care
Pneumonia
Superficial and deep wound infection
Myocardial infarction
Arrhythmias
Severe pain
Pulmonary embolism
Acute kidney injury
Stroke
Respiratory failure
Acute confusion or delirium
Cardiac arrest
Pearse RM, et al. BMJ 2011;343:d5759.

84,730 patients who had undergone inpatient
general and vascular surgery 2005 - 2007
Very low mortality Very high mortality
3.5% 6.9%
Ghaferi AA. N Engl J Med 2009;361:1368-75
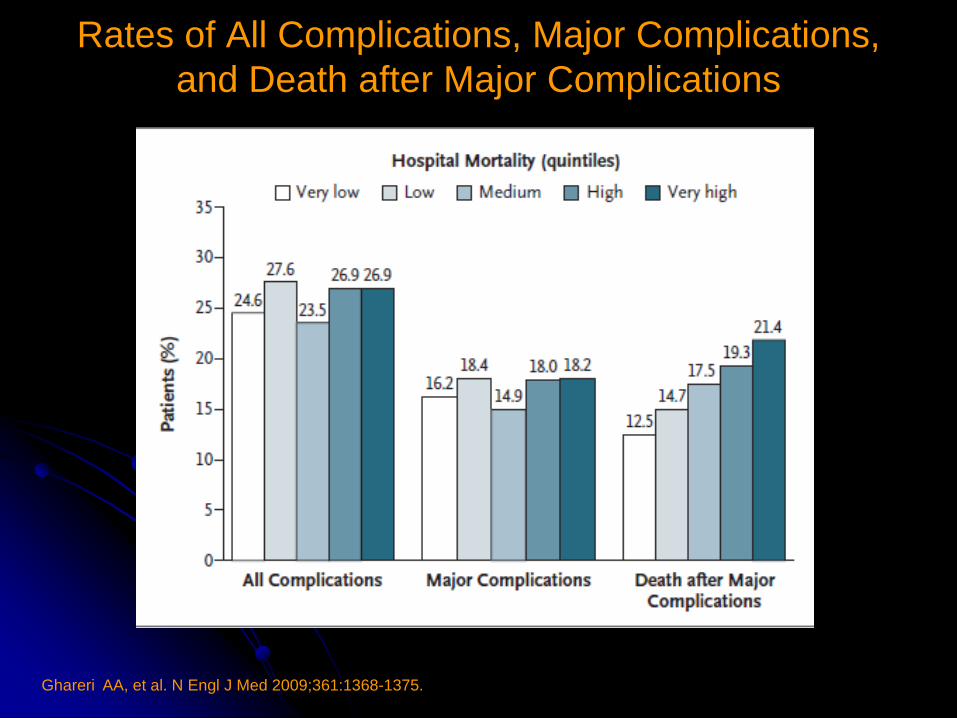
Ghareri AA, et al. N Engl J Med 2009;361:1368-1375.
Rates of All Complications, Major Complications,
and Death after Major Complications
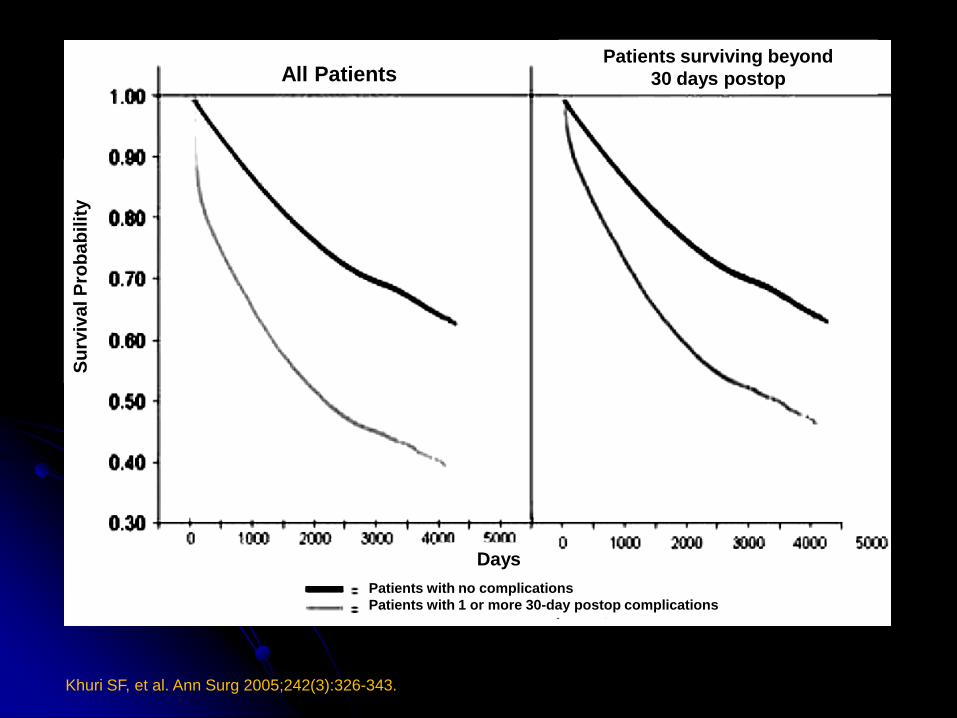
Khuri SF, et al. Ann Surg 2005;242(3):326-343.
Patients with no complications
Patients with 1 or more 30-day postop complications
Patients surviving beyond
30 days postop All Patients
Days
Su
rviv
al P
rob
ab
ilit
y

Hospital-specific rates of preoperative medical
consultation for major elective noncardiac surgery
Wijeysundera DN, et al. Anesthesiology 2012;116:25-34.
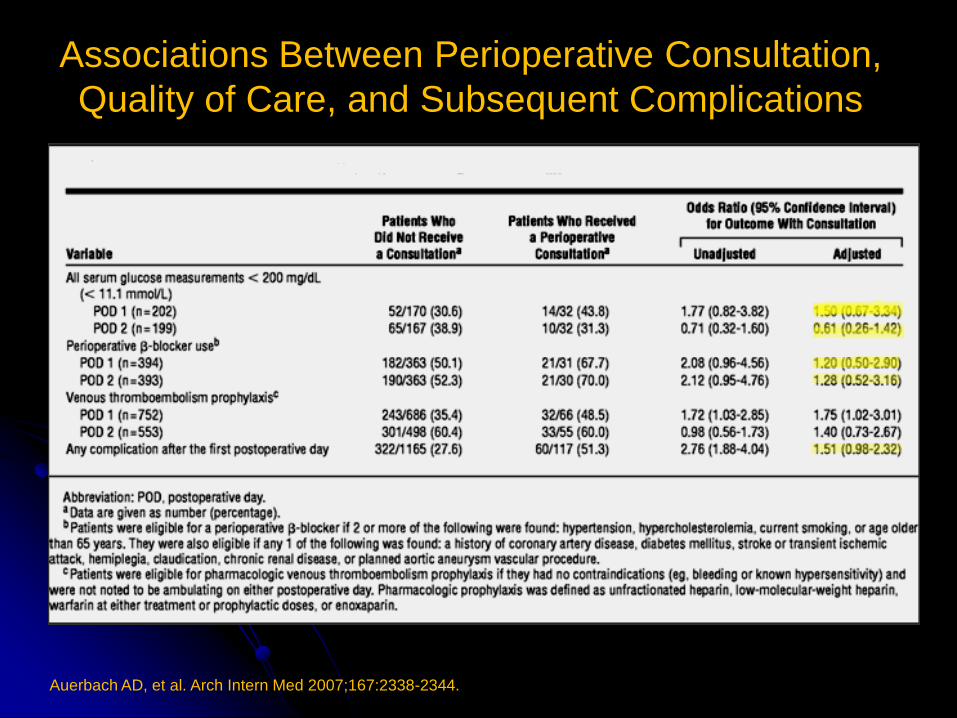
Associations Between Perioperative Consultation,
Quality of Care, and Subsequent Complications
Auerbach AD, et al. Arch Intern Med 2007;167:2338-2344.

Wijeysundera DN, et al. Arch Intern Med 2009;169(6):595-602.
217,082 39% (n = 104,716) underwent
anesthesia consultations
- Reduced mean hospital length of stay
8.17 vs 8.52 day
- No reduction of 30 day or 1 year mortality
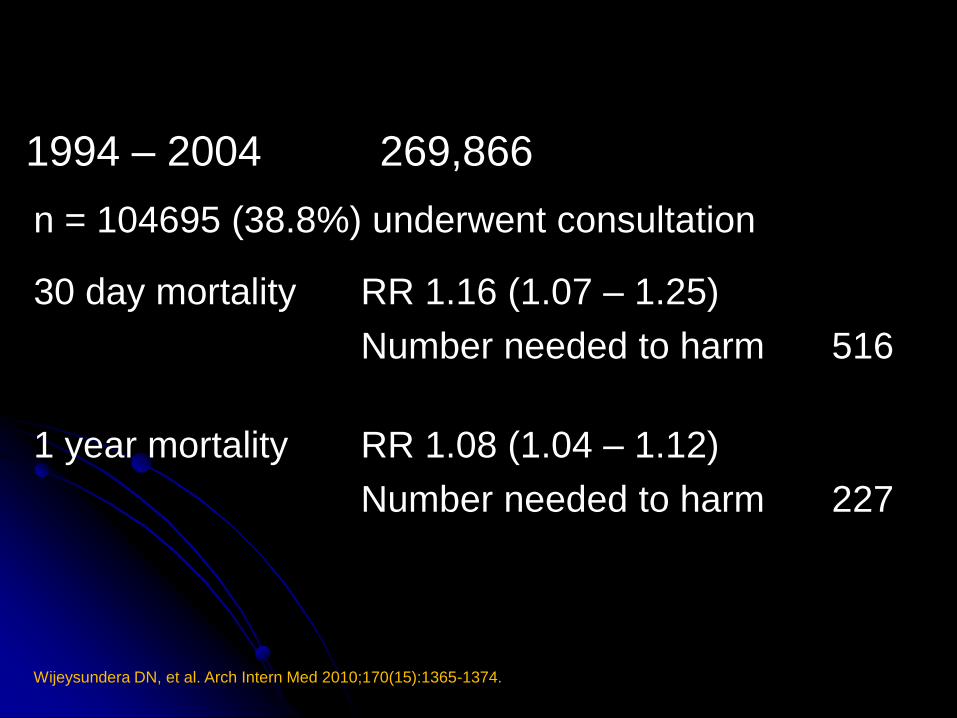
n = 104695 (38.8%) underwent consultation
30 day mortality RR 1.16 (1.07 – 1.25)
Number needed to harm
516
1 year mortality RR 1.08 (1.04 – 1.12)
Number needed to harm
227
Wijeysundera DN, et al. Arch Intern Med 2010;170(15):1365-1374.
1994 – 2004 269,866
Pathophysiology
Emotional stress
Pain
Surgical trauma
Tissue injury
Hypothermia
Hypoxemia
Immobility
Bleeding and anemia
Fasting
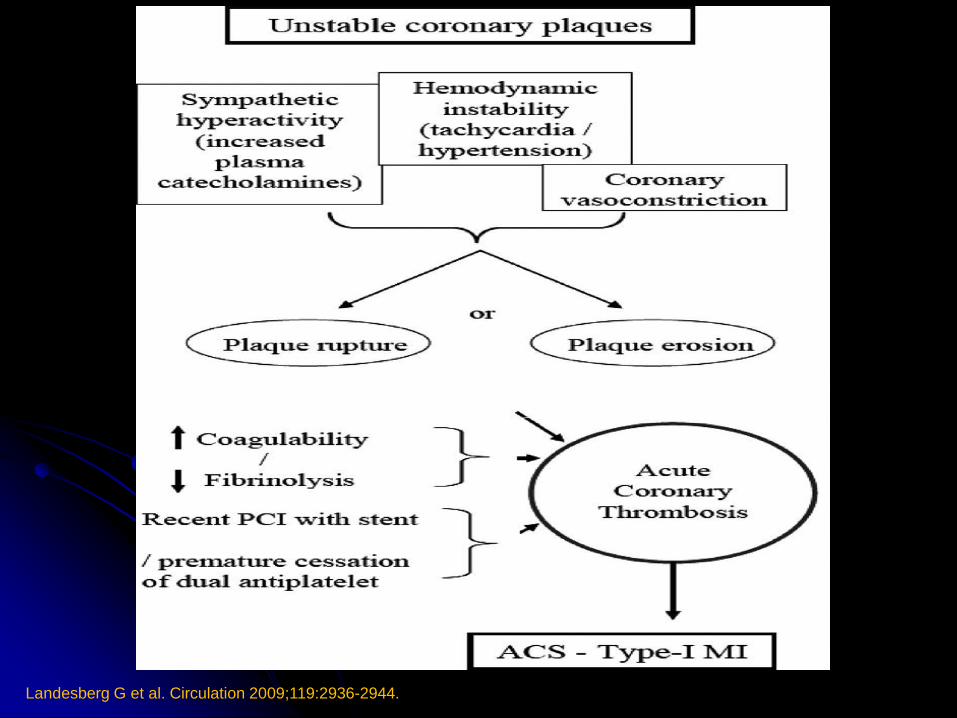
Landesberg G et al. Circulation 2009;119:2936-2944.

Landesberg G et al. Circulation 2009;119:2936-2944.

Devereaux PJ, et al. CMAJ 2005;173(6):627-634.
Potential triggers of states associated with perioperative
elevations in troponin levels, arterial thrombosis and fatal
myocardial infarction

Risk Prediction Models

Revised Cardiac Risk Index
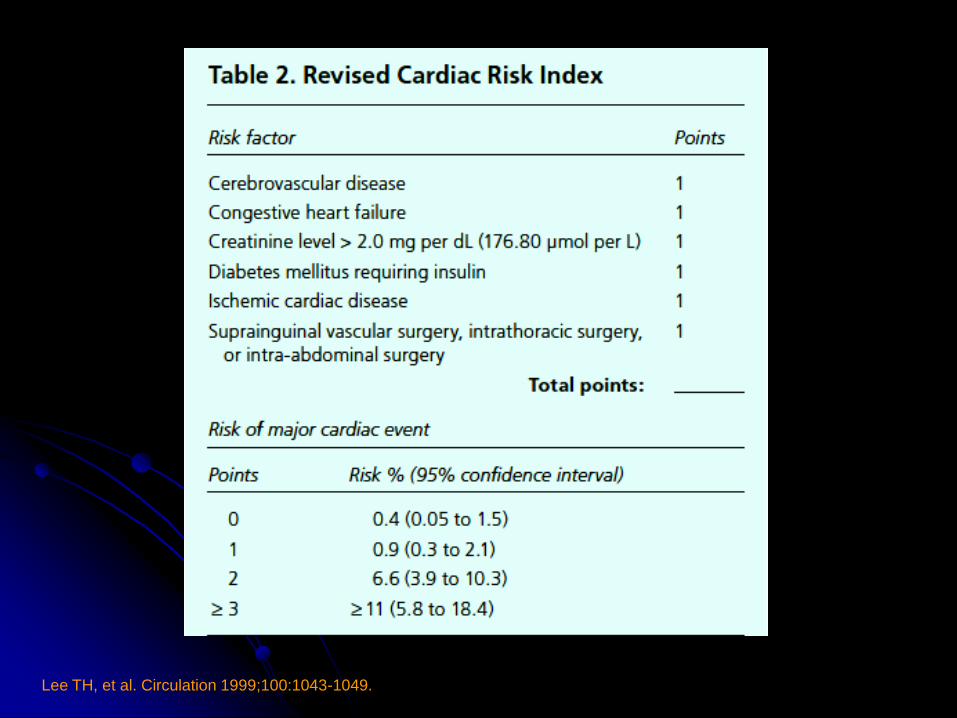
Lee TH, et al. Circulation 1999;100:1043-1049.
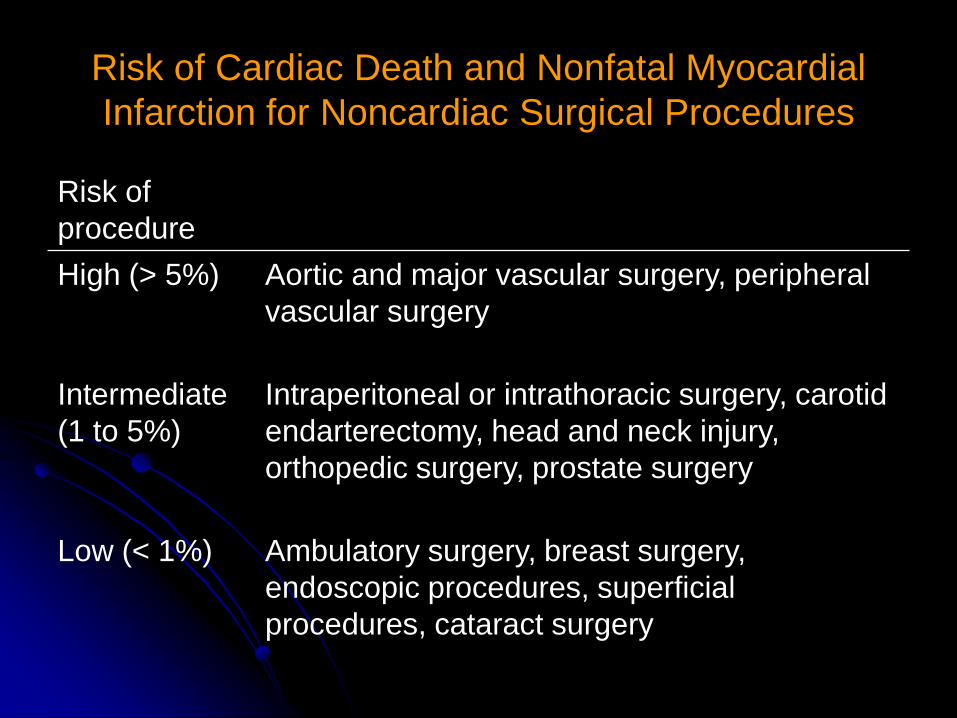
Risk of Cardiac Death and Nonfatal Myocardial
Infarction for Noncardiac Surgical Procedures
Risk of
procedure
High (> 5%) Aortic and major vascular surgery, peripheral
vascular surgery
Intermediate
(1 to 5%)
Intraperitoneal or intrathoracic surgery, carotid
endarterectomy, head and neck injury,
orthopedic surgery, prostate surgery
Low (< 1%) Ambulatory surgery, breast surgery,
endoscopic procedures, superficial
procedures, cataract surgery
Thoracic Revised Cardiac
Risk Index
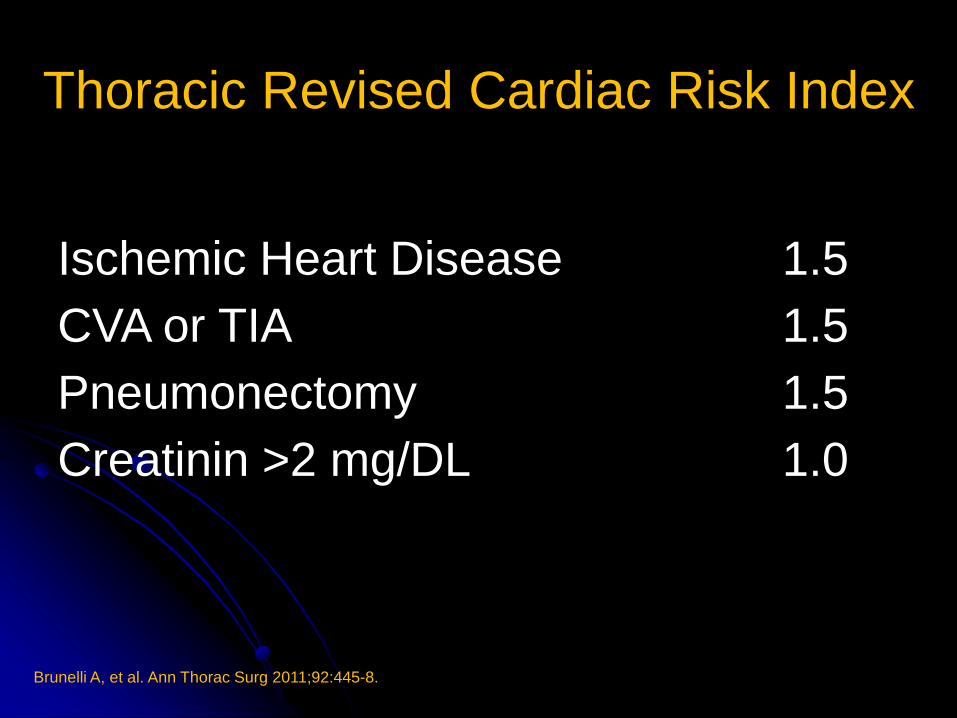
Thoracic Revised Cardiac Risk Index
Ischemic Heart Disease 1.5
CVA or TIA 1.5
Pneumonectomy 1.5
Creatinin >2 mg/DL 1.0
Brunelli A, et al. Ann Thorac Surg 2011;92:445-8.
Brunelli A, et al. Ann Thorac Surg 2011;92:445-8.
.
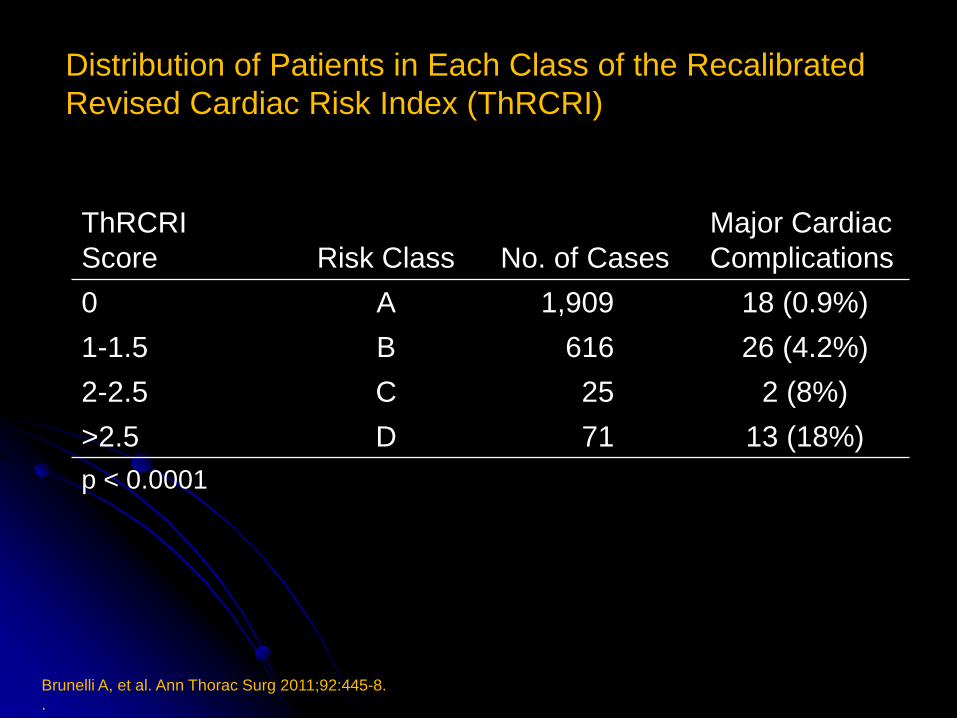
ThRCRI
Score
Risk Class
No. of Cases
Major Cardiac
Complications
0 A 1,909 18 (0.9%)
1-1.5 B 616 26 (4.2%)
2-2.5 C 25 2 (8%)
>2.5 D 71 13 (18%)
p < 0.0001
Distribution of Patients in Each Class of the Recalibrated
Revised Cardiac Risk Index (ThRCRI)
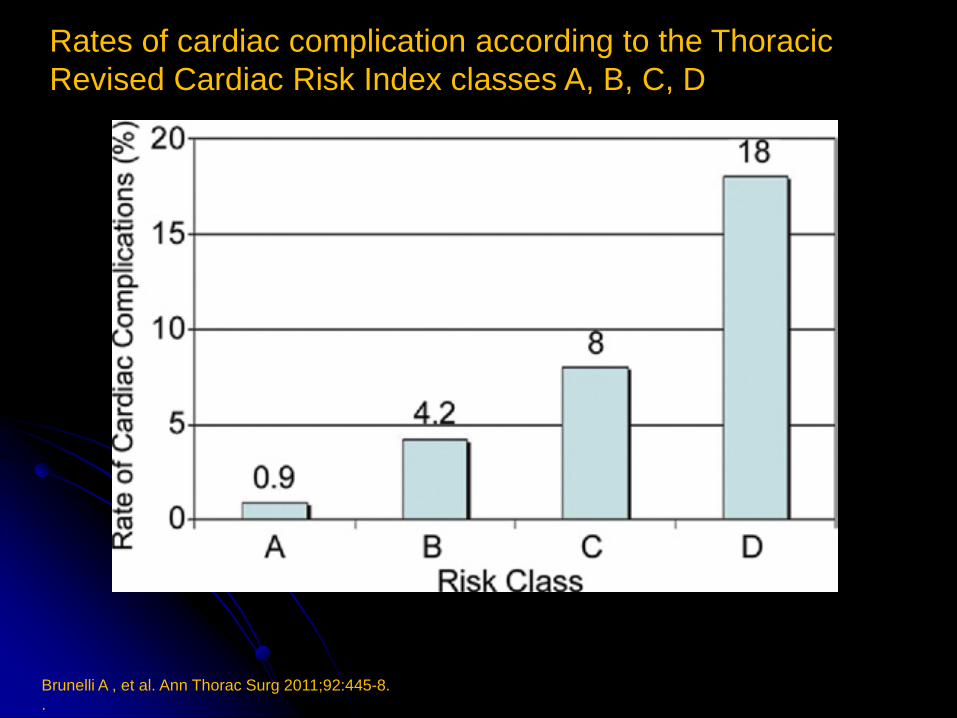
Brunelli A , et al. Ann Thorac Surg 2011;92:445-8.
.
Rates of cardiac complication according to the Thoracic
Revised Cardiac Risk Index classes A, B, C, D
Vascular Study Group of
New England(VSG-CRI)

Bertges, et al. J Vasc Surg 2010;52(3):674-83.
Vascular Surgery Group Cardiac Risk Index (VSG-CRI) scoring
system and predicated risk of adverse cardiac events

Surgical Mortality Probability
Model

ASA PS Classification
ASA PS Definition
I A normal healthy patient
II A patient with mild systemic disease
III A patient with severe systemic disease
IV A patient with severe systemic disease that
is a constant threat to life
V A moribund patient who is not expected to
survive without the operation
Glance LG, et al. Ann Surg 2012;255:696-702.

S-MPM Scoring System for Estimating Risk of 30-Day
Mortality After Noncardiac Surgery
Glance LG, et al. Ann Surg 2012;255:696-702.
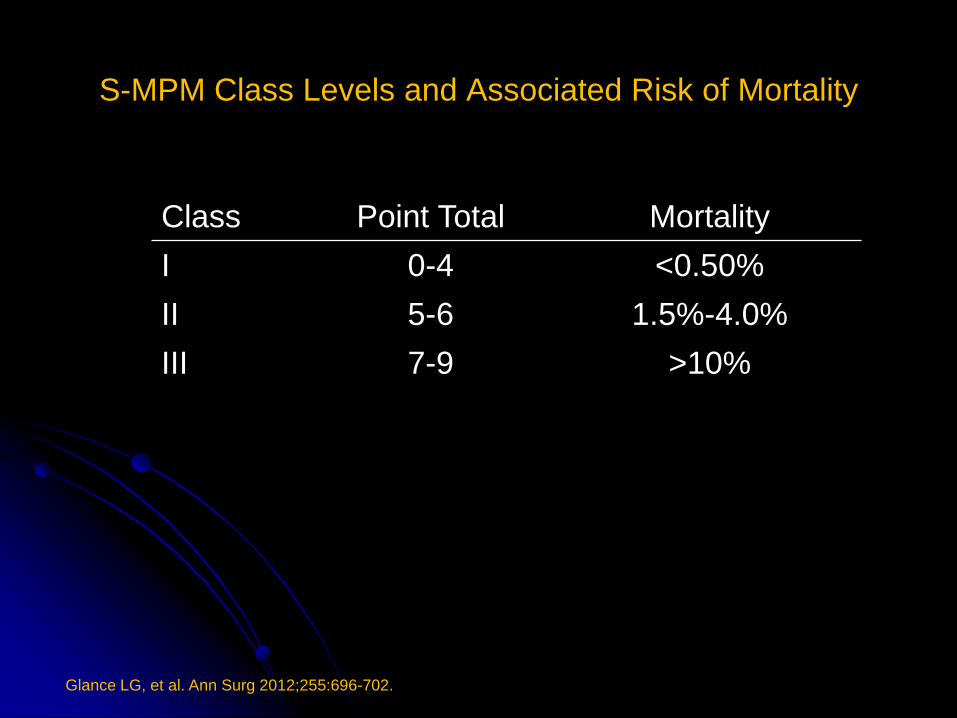
S-MPM Class Levels and Associated Risk of Mortality
Class Point Total Mortality
I 0-4 <0.50%
II 5-6 1.5%-4.0%
III 7-9 >10%
Glance LG, et al. Ann Surg 2012;255:696-702.

Risk Calculator for Prediction
of Cardiac Risk After Surgery

Calculator to Predict the risk of
myocardial infarction or cardiac arrest
(MICA)
Type of surgery
Functional status
Abnormal creatinine
American Society of Anesthesiologists class
Increasing age
The MICA risk calculator is available at www.surgicalriskcalculator.com
Gupta PK, et al. Circulation 2011;124:381-387.

Clinical Recommendations

CCS ACC/
AHA ESC HFSA

CCS ACC/AHA ESC HFSA

Definition
Something that provides direction or
advice as to a decision or course of
action;
A detailed plan or explanation to guide
you in setting standards or determining a
course of action
Collins English Dictionary http://www.thefreedictionary.com/guideline
Definition
Systematically developed statements to assist
practitioner and patient decisions about
appropriate health care for specific clinical
circumstances1
To assist health care providers in clinical
decision making by describing a range of
generally acceptable approaches2
1. Institute of Medicine. Washington, DC: National Academy PR; 1992
2. Hunt S, et al. Circulation 2005;112:1825-52.

Electrocardiogram

Recommendations for Preoperative Resting
12-Lead ECG
Class I
1. Patients with at least 1 clinical risk factor who are
undergoing vascular surgical procedures.
2. patients with known CHD, peripheral arterial disease,
or cerebrovascular disease who are undergoing
intermediate-risk surgical procedures.
Fleisher LA, et al. Circulation 2009;120:e169-e276.

Recommendations for Preoperative Resting
12-Lead ECG
Class III
1. Preoperative and postoperative resting 12-lead
ECGs are not indicated in asymptomatic persons
undergoing low-risk surgical procedures.
Fleisher LA, et al. Circulation 2009;120:e169-e276.

Feely MA, et al. Am Fam Physician 2013;87(6):414-8.
Suggested algorithm for performing preoperative
electrocardiography

Echocardiography
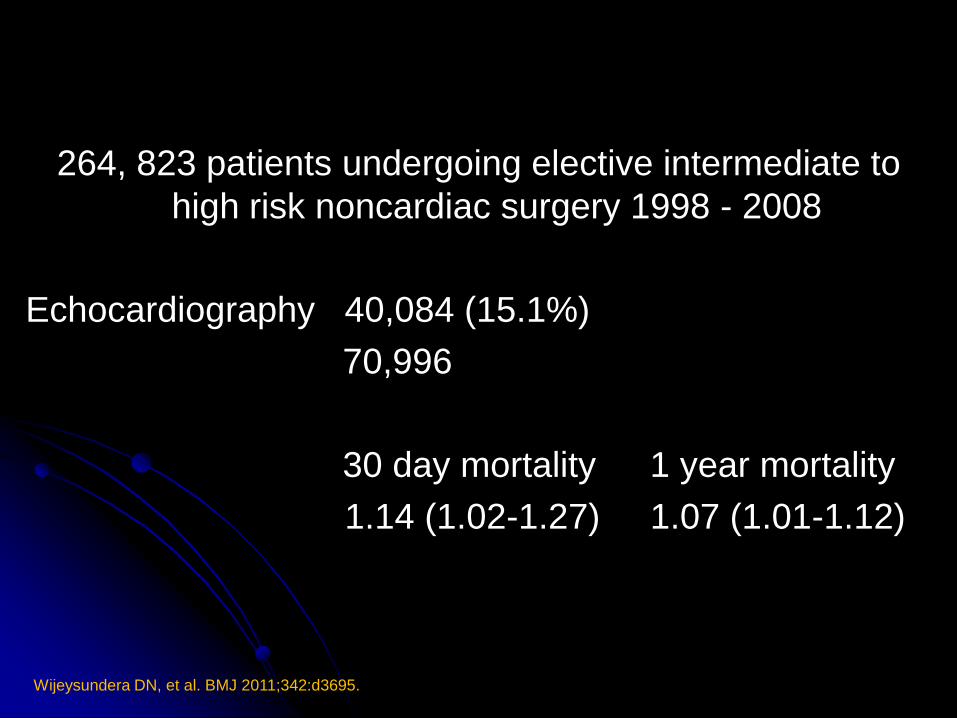
Wijeysundera DN, et al. BMJ 2011;342:d3695.
264, 823 patients undergoing elective intermediate to
high risk noncardiac surgery 1998 - 2008
Echocardiography 40,084 (15.1%)
70,996
30 day mortality 1 year mortality
1.14 (1.02-1.27) 1.07 (1.01-1.12)

Recommendations for Preoperative Noninvasive
Evaluation of LV Function
Class IIa
1. It is reasonable for patients with dyspnea of unknown
origin.
2. It is reasonable for patients with current or prior HF
with worsening dyspnea or other change in clinical
status if not performed within 12 months.
Fleisher LA, et al. Circulation 2009;120:e169-e276.

Recommendations for Preoperative Noninvasive
Evaluation of LV Function
Class IIb
1. Reassessment of LV function in clinically stable
patients with previously documented cardiomyopathy is
not well established.
Class III
1. Routine perioperative evaluation of LV function in
patients is not recommended.
Fleisher LA, et al. Circulation 2009;120:e169-e276.

Stress Testing
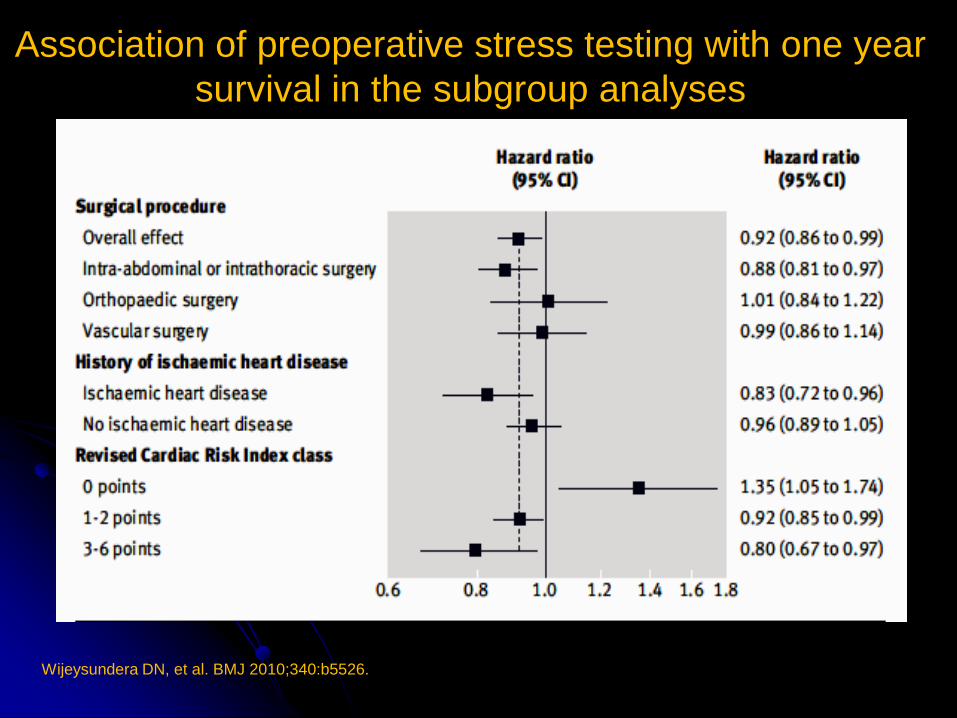
Wijeysundera DN, et al. BMJ 2010;340:b5526.
Association of preoperative stress testing with one year
survival in the subgroup analyses
Active Cardiac Conditions for Which the Patient
Should Undergo Evaluation and Treatment Before
Noncardiac Surgery
Fleisher LA, et al. Circulation 2009;120:e169-e276.
Unstable coronary symptoms
Decompensated HF (NYHA functional
class IV: worsening or new-onset HF)
Significant arrythmias
Severe valvular disease

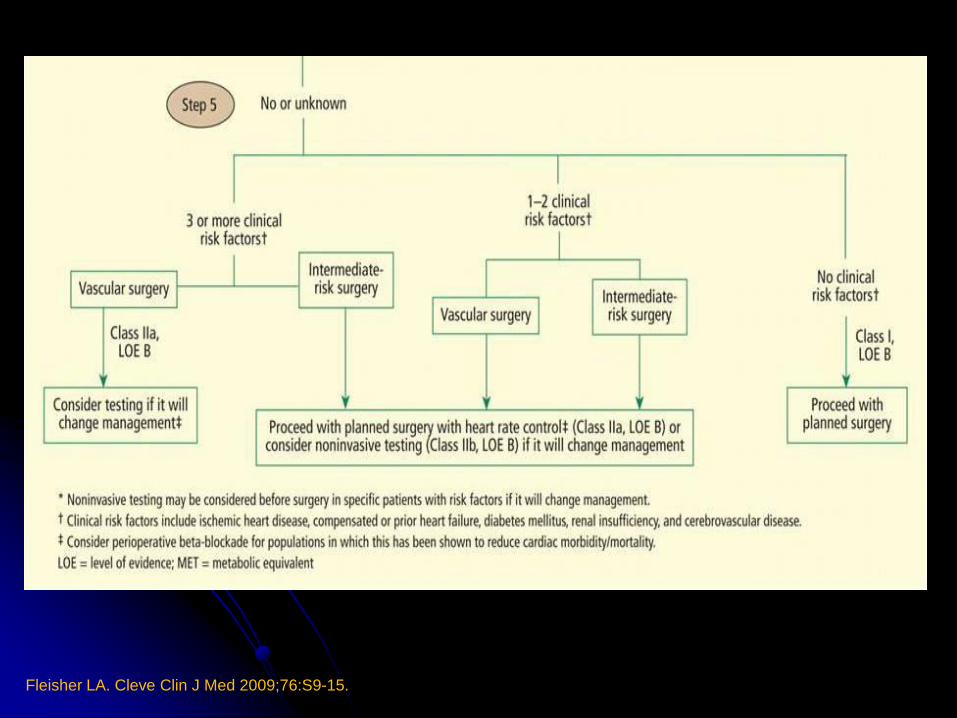
Recommendations for Noninvasive Stress Testing
Before Noncardiac Surgery
Class I
1. Patients with active cardiac conditions.
Class IIa
1. 3 or more clinical risk factors and poor functional
capacity (less than 4 METs) who require vascular
surgery is reasonable if it will change management.
Fleisher LA, et al. Circulation 2009;120:e169-e276.
Recommendations for Noninvasive Stress Testing
Before Noncardiac Surgery
Class IIb
1. may be considered for patients with at lease 1 to 2 clinical
risk factors and poor functional capacity (less than 4
METs) who require intermediate risk or vascular surgery if
it will change management.
Class III
1. Noninvasive testing is not useful for patients with no
clinical risk factors undergoing low or intermediate-risk
noncardiac surgery.
Fleisher LA, et al. Circulation 2009;120:e169-e276.

McFalls EO, et al. NEJM 2004;351:2795-2804.
Long-Term Survival among Patients Assigned to Undergo
Coronary-Artery Revascularization or No Coronary-Artery
Revascularization before Elective Major Vascular Surgery

American College of Cardiology (ACC)/ American
Heart Association (AHA) 2007 Guidelines
Open Vascular Surgery Required
Emergent Proceed with planned procedure Yes
No
Active Cardiac Condition Class I: Non-Invasive Stress Testing
Class I: Coronary Revascularization indications
same as in patients not undergoing surgery
Known Functional Capacity
< 3 Clinical Risk Factors Class I: No Further Testing
Class I: Continue β-blocker if currently prescribed
Class IIa: Consider Non-Invasive Stress Testing
Yes
No
No Yes
No

Biomarkers
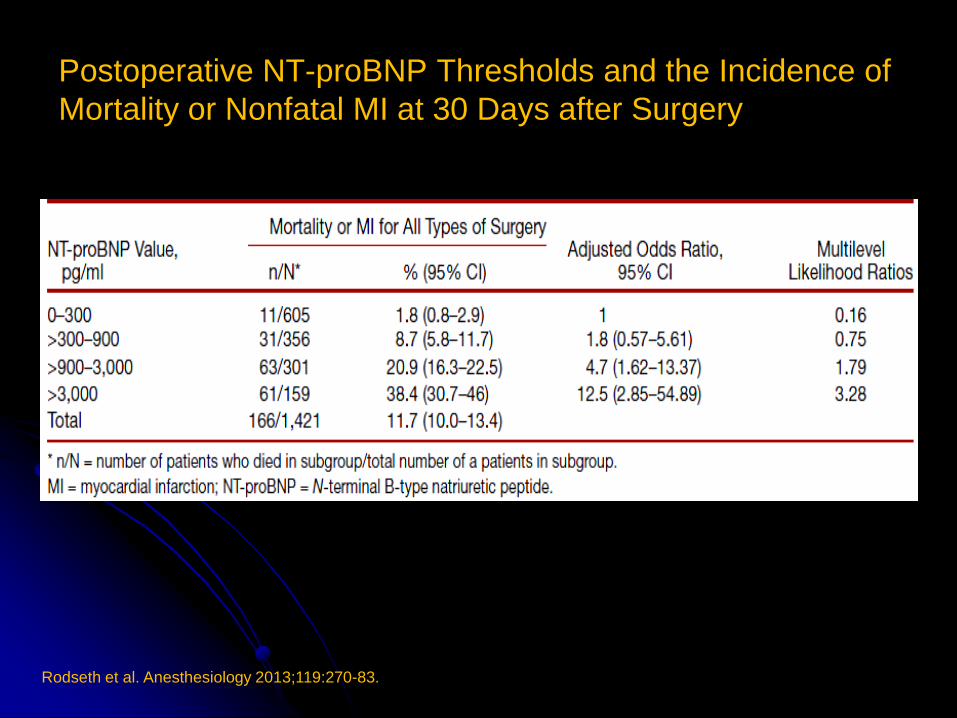
Postoperative NT-proBNP Thresholds and the Incidence of
Mortality or Nonfatal MI at 30 Days after Surgery
Rodseth et al. Anesthesiology 2013;119:270-83.
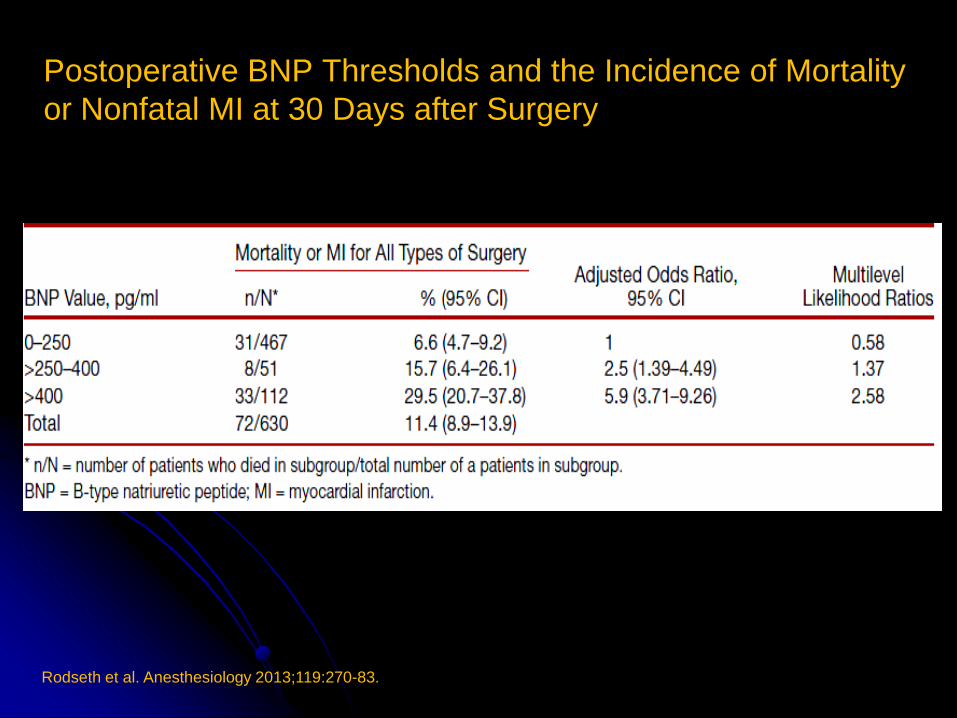
Postoperative BNP Thresholds and the Incidence of Mortality
or Nonfatal MI at 30 Days after Surgery
Rodseth et al. Anesthesiology 2013;119:270-83.
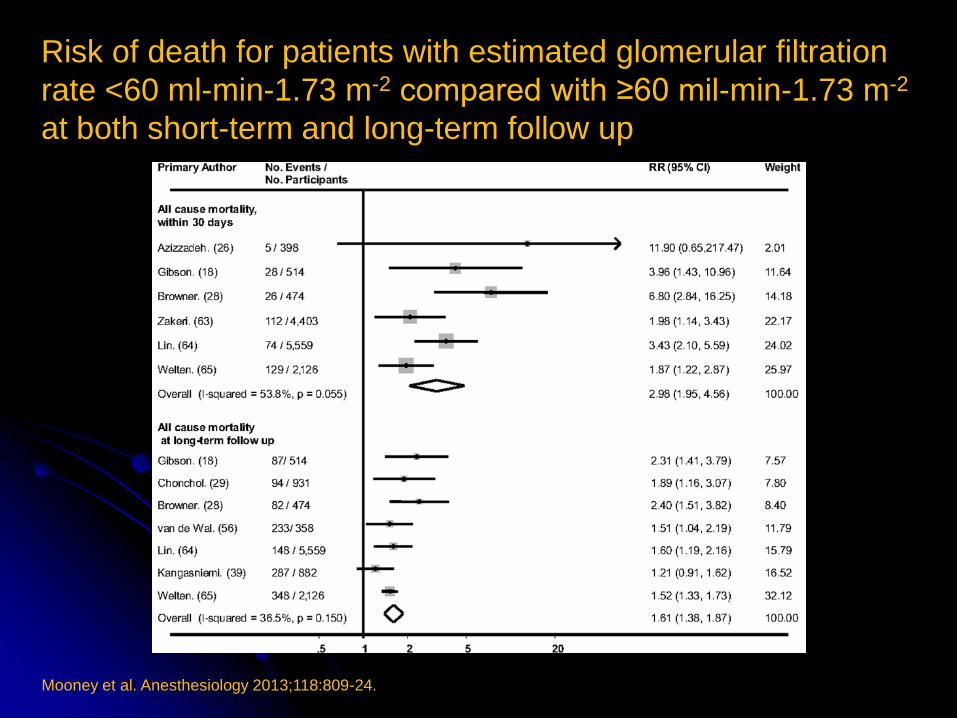
Risk of death for patients with estimated glomerular filtration
rate <60 ml-min-1.73 m-2 compared with ≥60 mil-min-1.73 m-2
at both short-term and long-term follow up
Mooney et al. Anesthesiology 2013;118:809-24.

Kaplan-Meier estimates of 30-Day mortality based on peak
Troponin T values
The Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION)
Study Investigators. JAMA 2013;307:2295-2304.
15,133 noncardiac surgery (2007 – 2011)
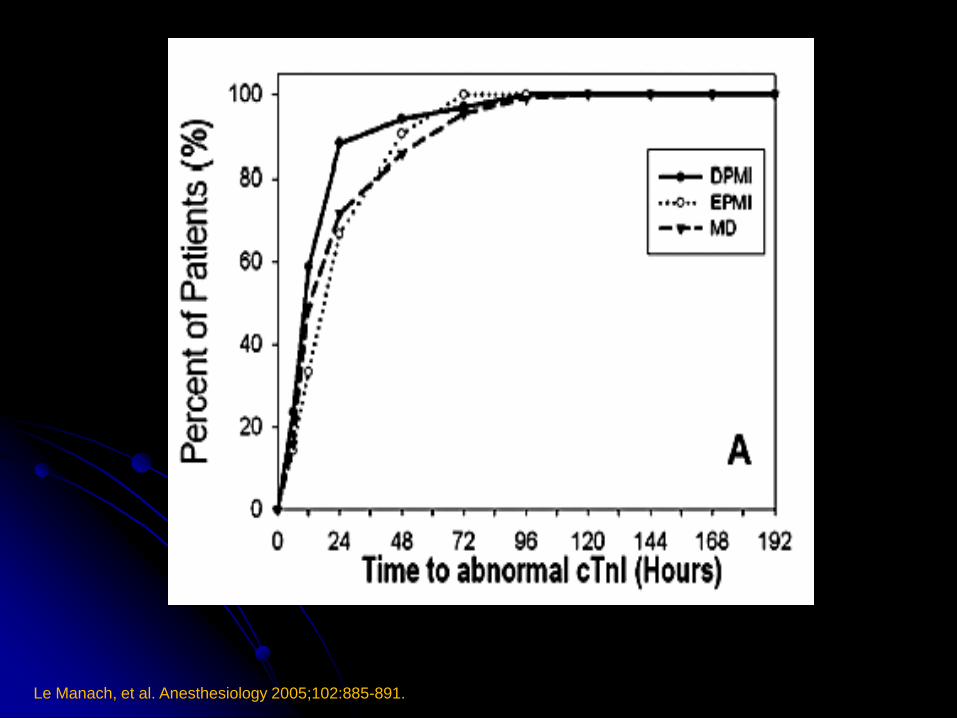
Le Manach, et al. Anesthesiology 2005;102:885-891.
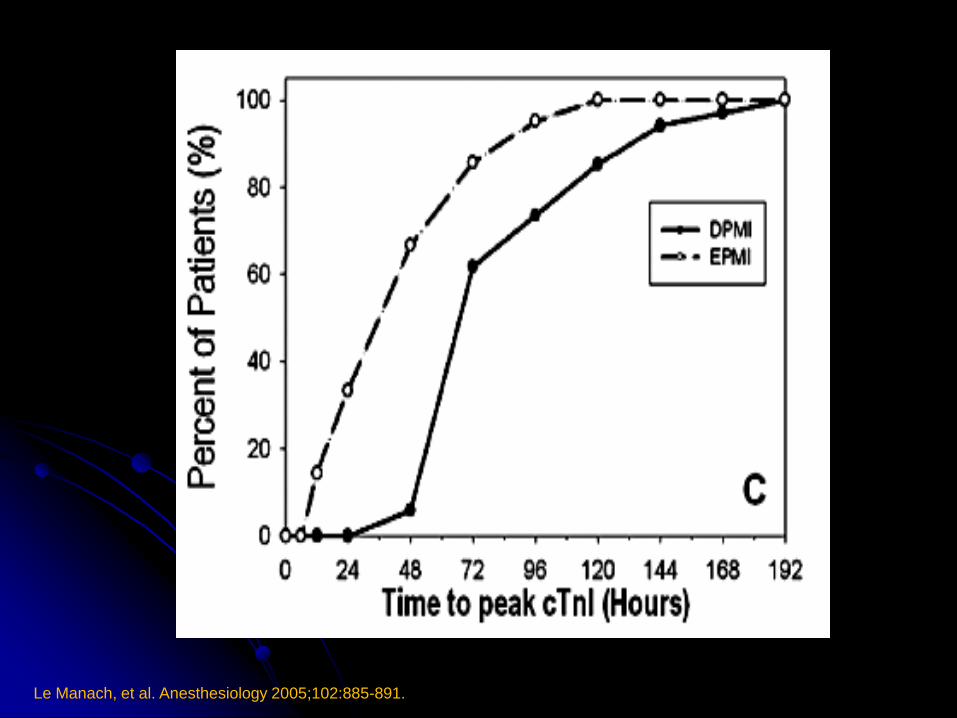
Le Manach, et al. Anesthesiology 2005;102:885-891.
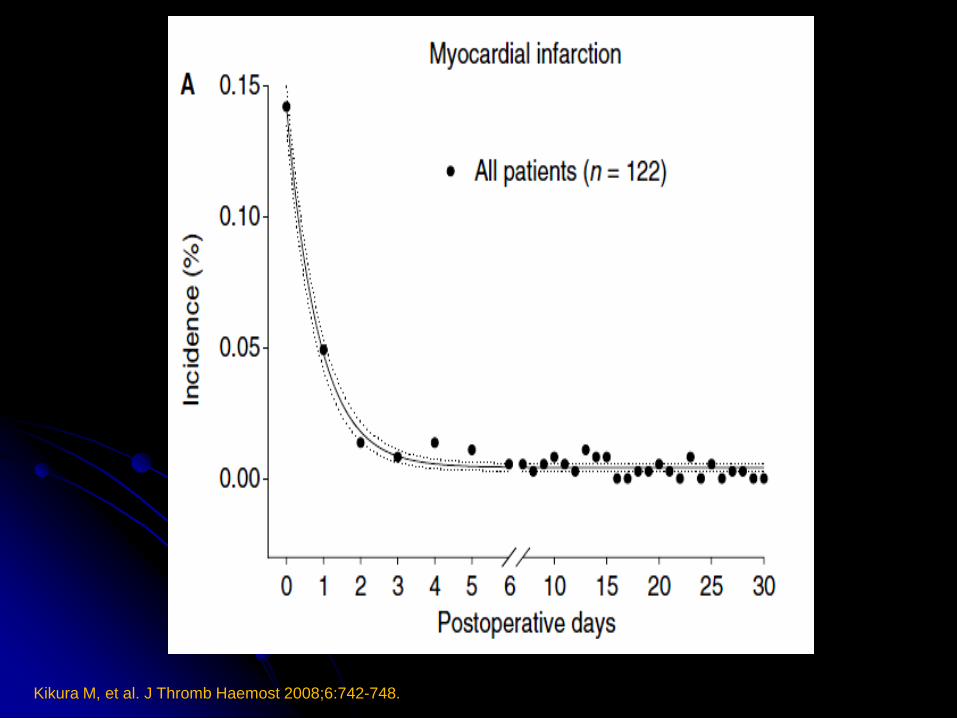
Kikura M, et al. J Thromb Haemost 2008;6:742-748.

Kikura M, et al. J Thromb Haemost 2008;6:742-748.

Statins
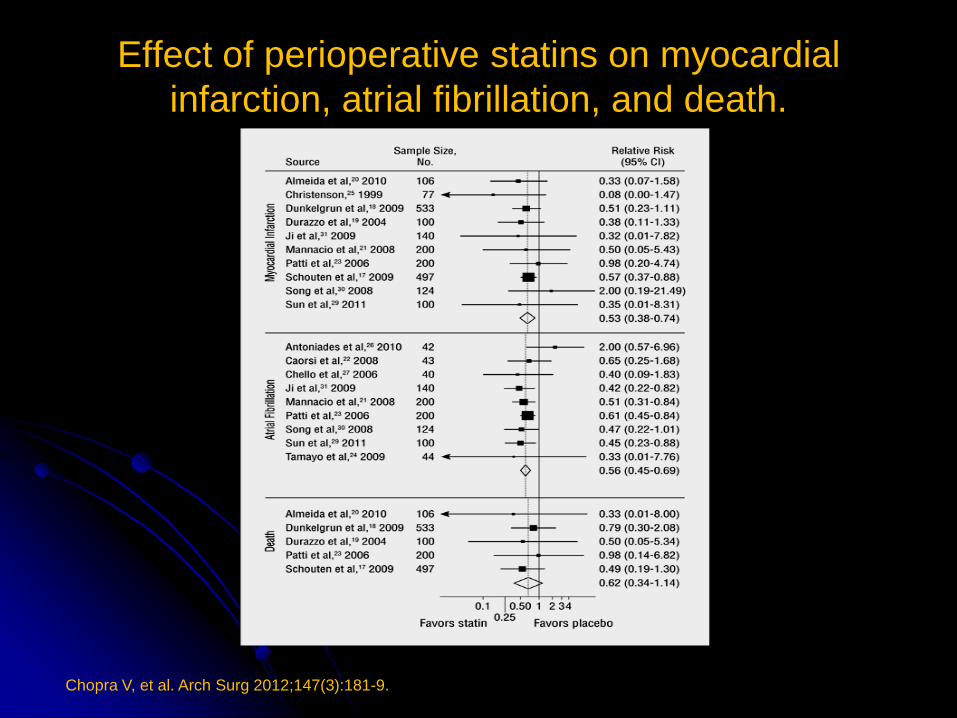
Effect of perioperative statins on myocardial
infarction, atrial fibrillation, and death.
Chopra V, et al. Arch Surg 2012;147(3):181-9.
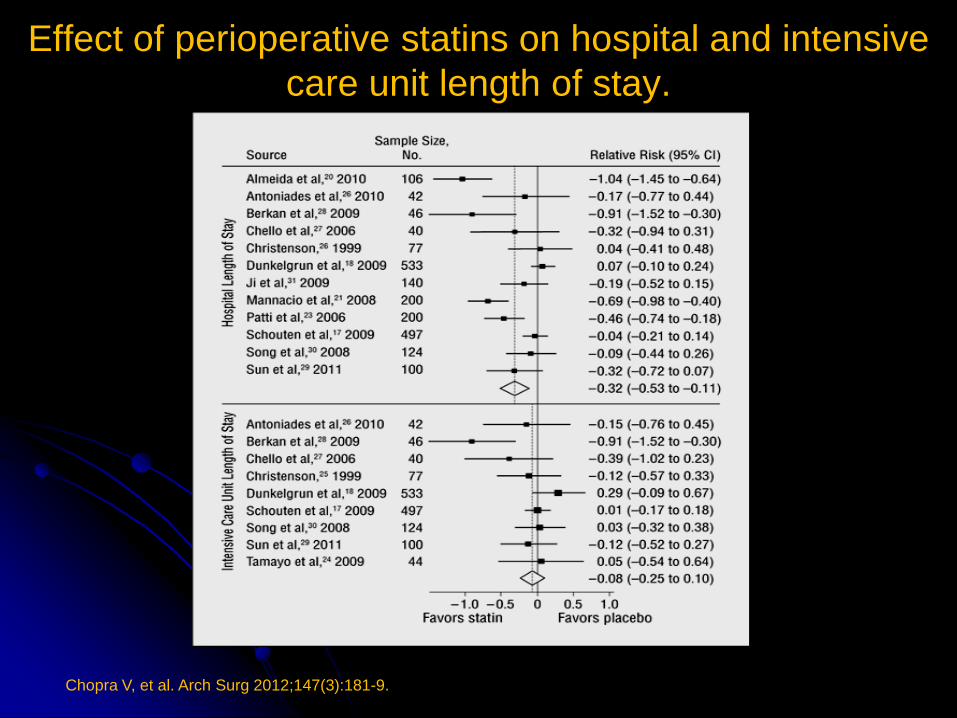
Effect of perioperative statins on hospital and intensive
care unit length of stay.
Chopra V, et al. Arch Surg 2012;147(3):181-9.
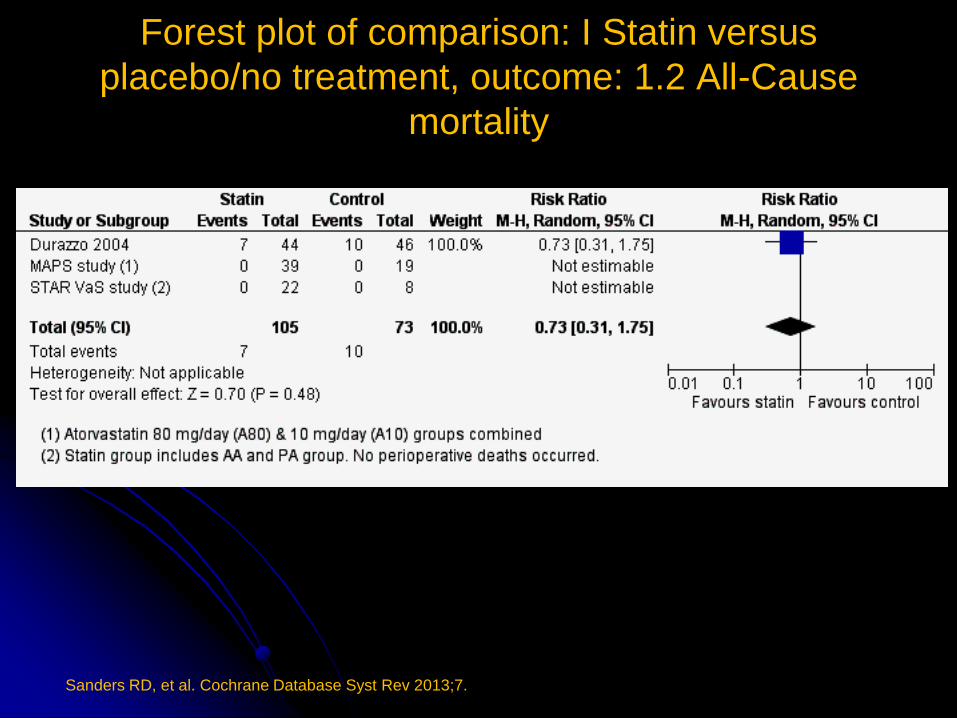
Forest plot of comparison: I Statin versus
placebo/no treatment, outcome: 1.2 All-Cause
mortality
Sanders RD, et al. Cochrane Database Syst Rev 2013;7.
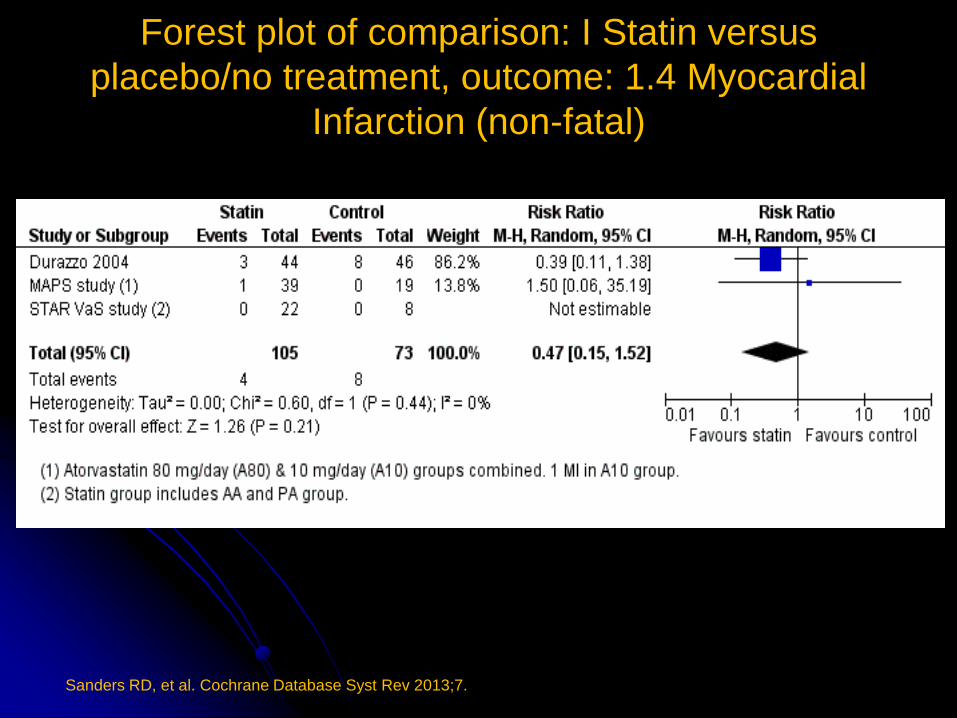
Forest plot of comparison: I Statin versus
placebo/no treatment, outcome: 1.4 Myocardial
Infarction (non-fatal)
Sanders RD, et al. Cochrane Database Syst Rev 2013;7.
PCI
Singla S, et al. JACC 2012;60:2005-2016.
The highest-risk period for ST after PCI with
either BMS or DES following NCS is the first 4
weeks. Therefore, it seems reasonable to
withhold NCS, if possible, for at least 4 weeks
after PCI.
Fleisher LA, et al. Circulation 2009;120:e169-e276.
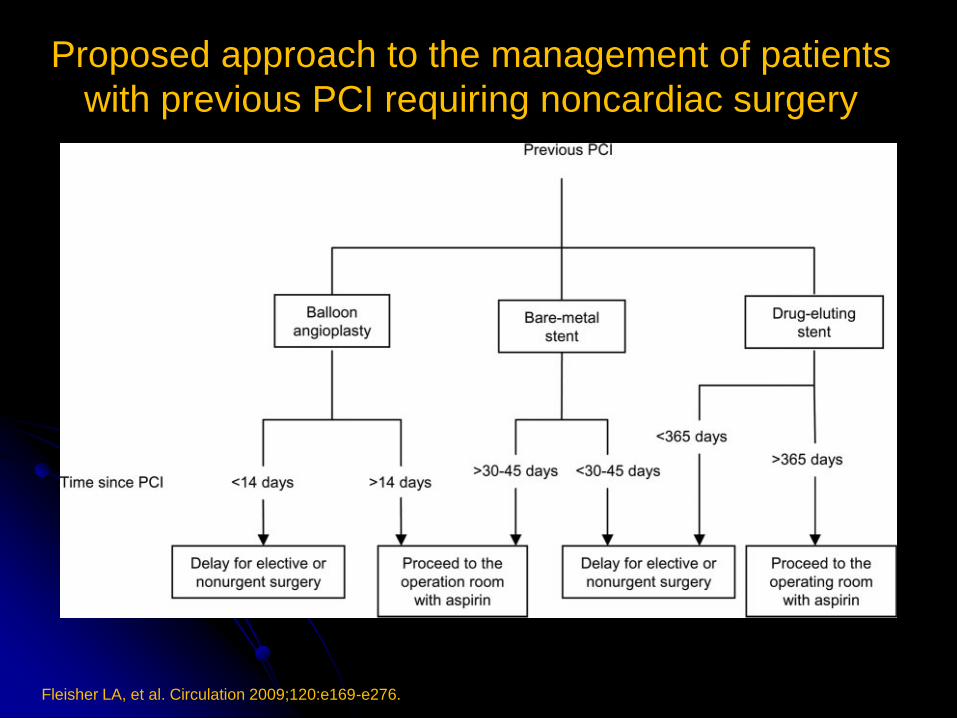
Proposed approach to the management of patients
with previous PCI requiring noncardiac surgery
Fleisher LA, et al. Circulation 2009;120:e169-e276.
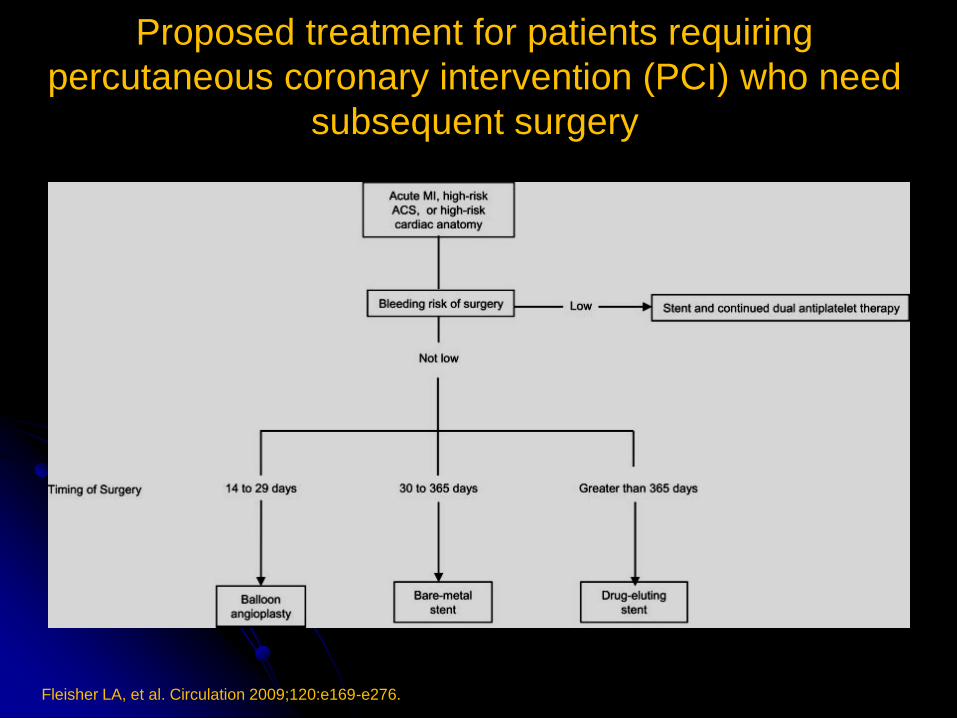
Proposed treatment for patients requiring
percutaneous coronary intervention (PCI) who need
subsequent surgery
Perioperative Hypertension

No link between perioperative complications with
either preexistant hypertension or an elevated
blood pressure
Types of surgery: CABG, AA, CEA, PVS,
intraperitoneal or intrathoracic
Perioperative cardiac complications are
associated with hemodynamic lability (>20%
change in mean BP)

Consider lowering the dose of ACE
inhibitors or AR antagonist 24 hours ( at
least 10 hours) before surgery

Perioperative Beta Blockers
Perioperative Ischemic Evaluation Study (POISE) Group. Lancet 2008;371:1839-47.
8,351 patients with, or at risk of, atherosclerotic
disease received extended-release metoprolol
succinate (n=4174) or placebo (n=4177)
started 2-4 h before surgery and continued
for 30 days.
Perioperative Ischemic Evaluation Study (POISE) Group. Lancet 2008;371:1839-47.
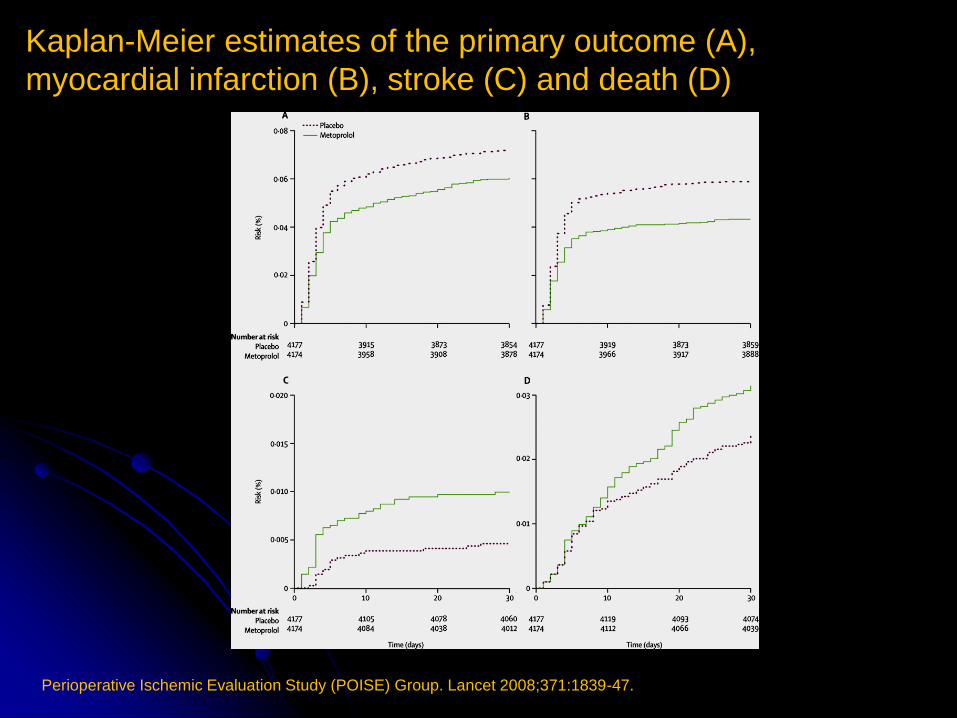
Kaplan-Meier estimates of the primary outcome (A),
myocardial infarction (B), stroke (C) and death (D)
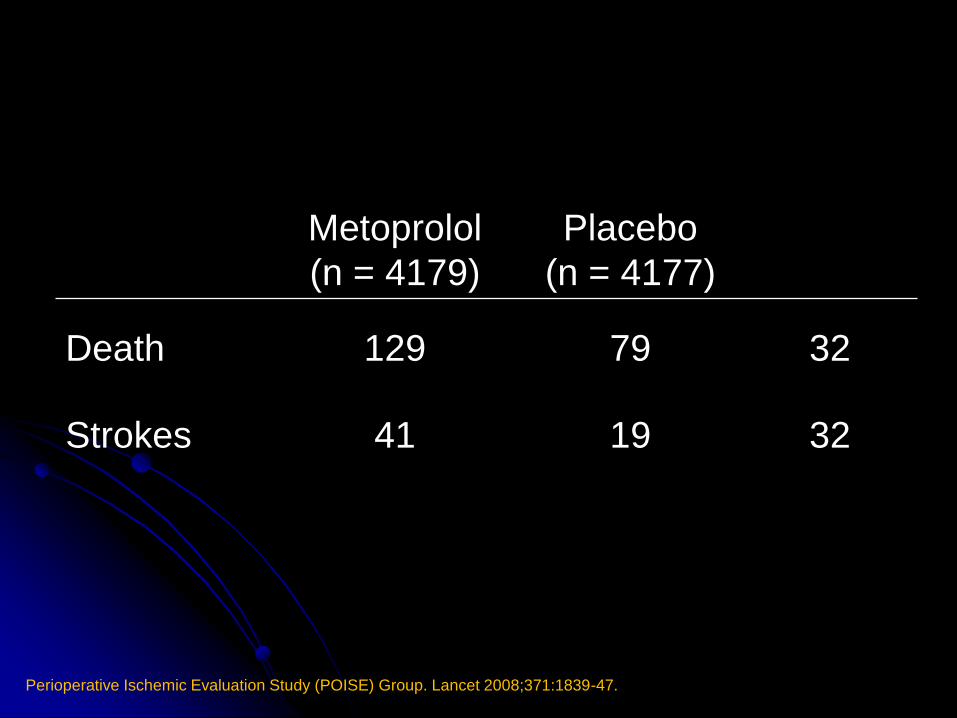
Metoprolol
(n = 4179)
Placebo
(n = 4177)
Death 129 79 32
Strokes 41 19 32
Perioperative Ischemic Evaluation Study (POISE) Group. Lancet 2008;371:1839-47.

Perioperative Ischemic Evaluation Study (POISE) Group. Lancet 2008;371:1839-47.
.
Meta-analysis of β-blocker trials in patients undergoing non-
cardiac surgery
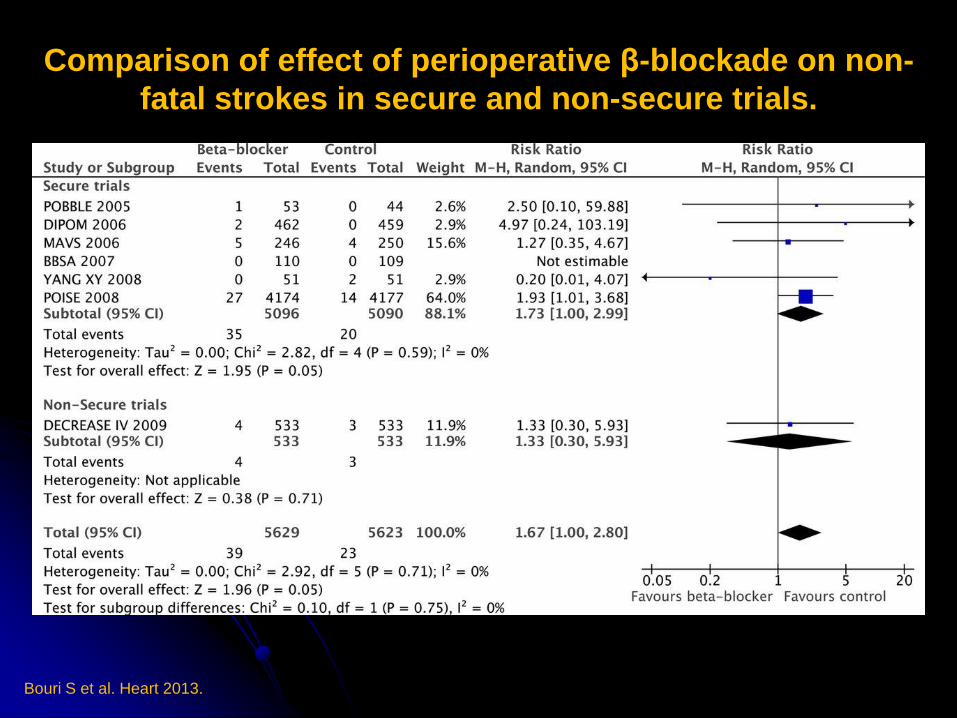
Comparison of effect of perioperative β-blockade on non-
fatal strokes in secure and non-secure trials.
Bouri S et al. Heart 2013.

Meta-analysis of nine secure randomised controlled trials
showing a significant increase in mortality with
perioperative β-blockade.
Bouri S et al. Heart 2013.
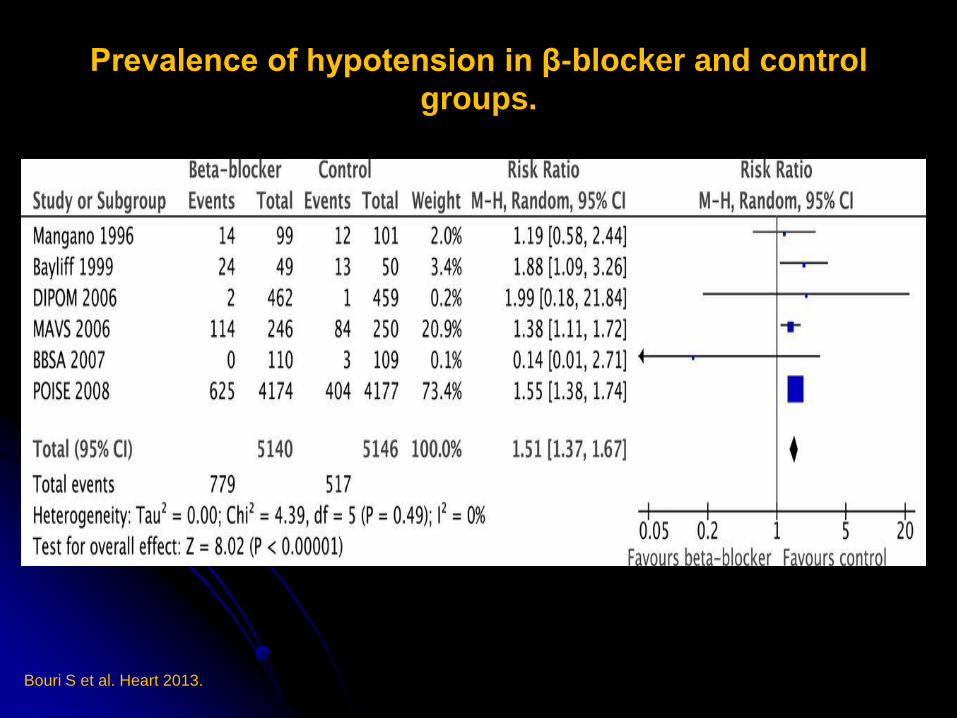
Prevalence of hypotension in β-blocker and control
groups.
Bouri S et al. Heart 2013.
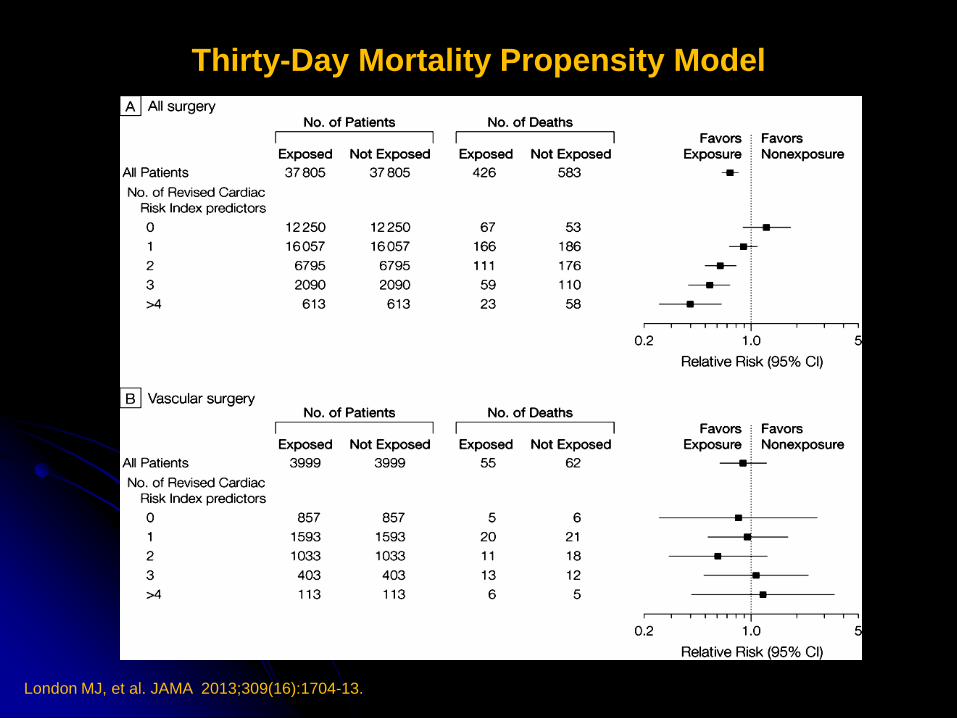
Thirty-Day Mortality Propensity Model
London MJ, et al. JAMA 2013;309(16):1704-13.

Beta Blockers
28,263 adults with IHD who underwent noncardiac
surgery 2004 - 2009
MACE Mortality
Heart Failure 22% 18%
MI within 2 years 46% 20%
MI 2 – 5 years 29% 26%
MI > 5 years 35% 33%
No MI or HF 44% 30%
Anderson C et al. Annual Congress of the European Society of Cardiology. September 18, 2013.
Summary of ACC/AHA Guideline Recommendations
Beta-Blocker Medical Therapy
Class I Beta-blockers should be continued in patients
undergoing surgery who are receiving beta-
blockers to treat angina, symptomatic
arrhythmias, hypertension, or other ACC/AHA
class I guideline indications
Class III Routine administration of high-dose beta-
blockers in the absence of dose titration is not
useful and may be harmful to patients not
currently taking beta-blockers who are
undergoing noncardiac surgery

Fleisher LA. Cleve Clin J Med 2009;76:S9-15.
Fleisher LA. Cleve Clin J Med 2009;76:S9-15.

Medical Consultant
Provide informed clinical judgment based on
knowledge, experience and the individual
patient’s data to optimize short and long term
outcomes.